health-seeking behavior of rwandan women
TRANSCRIPT

Sot. .Sci. Med. Vol. 37, No. II, pp. 1285-1292, 1993 Printed m Great Britain. All rights reserved
0277-9536/93 $6.00 + 0.00 Copyright 0 1993 Pergamon Press Ltd
HEALTH-SEEKING BEHAVIOR OF RWANDAN WOMEN
JOANNE CSETE
Department of Nutritional Sciences, University of Wisconsin, Madison, WI 53706. U.S.A
Abstract-The responses of Rwandan women in a highland region to their own and their children’s illness episodes are examined. Over 85% of diarrhea cases from monthly morbidity recalls were treated by health-center visits, use of Western medicine, or no treatment. Factors such as the age of the child at the time of the illness, previous child death in the household, and the women’s control of various categories of household expenditures exert some influence on health-seeking behavior, according to results of cross-tabulations. Women at the highest altitudes tend to respond less actively to children’s diarrhea, possibly because of the relative difficulty of their journey to the health center. Recommendations are offered for policy and further study.
Key words-health-seeking behavior, Rwanda, household survey, traditional cures, altitude
INTRODUCTION
In the highlands of Rwanda (Central Africa), most household-level decisions involving cash or in-kind expenditures are made by the man of the household [I]. Decisions on the course of action to follow when a young child is ill, however, are exceptional as the child’s mother commonly has considerable, if not the principal, decision-making authority in this circum- stance. Women are constrained in this decision- making not only by the level of resources at their disposal for health expenditures for children’s illness (which may be determined by their husbands) but also by such factors as distance to health-care providers and the availability of medicines for use in the home. They are further guided by their own health beliefs and experiences as well as by the health status of the child at the time of the illness episode. Health-seeking behavior of women in response to illness episodes of their young children has been little studied in Rwanda.
In his work in Mexican farming communities, Young [2, 31 develops formal models of treatment choice and other responses to illness based in large part on the responses of rural dwellers to questions about hypothetical illness episodes. He justifies his supposition that illness episodes, as recurring house- hold problems, evoke predictable and patterned responses by the high predictive power of his model when applied to actual illness episodes. Young’s model led to the identification of four factors as principal determinants of initial treatment choice [2, p. 1 lo]: seriousness of the illness, knowledge (of the care-seeker) of the illness and its remedy, degree of confidence in folk remedies for this illness, and expenses associated with the health-care alternatives. Young is critical of what he calls the “thick descrip- tion” approach of Janzen [4] and Turner [5], who reject the establishment of a clear decision-making
pattern in favor of an approach that uses individual illness episodes to highlight the complex interactions among social status, medical beliefs, and economic constraints that underlie health-seeking behavior.
Without explicitly entering into this method- ological debate, other studies, including a number from Africa, examine the association of a number of household-level factors with health-related decision- making outcomes. Some of these works suggest that while distance from the health-care provider is an important determinant of parents’ responses, its importance may sometimes be modified by c ler factors. Stock [6] showed, for example, that, regdrd- less of distance to the facility, households in the Kano State of Nigera had a high rate of utilization of Western health facilities for such diseases as tuber- culosis where the expectation of cure from Western medicine was high. Expectations abou’ the quality of care of a given healer or facility also muted the effect of distance.
A few studies have considered the relationship of social and economic factors to health-seeking behavior in developing countries. Okafor [7] found educational attainment was positively related to more frequent use of Western-type health providers in rural Nigeria, though the important- of the relationship between education and income level was not explored using multivariate methods. In this sample, the more highly educated groups also had a more disdainful attitude toward traditional medicine.
Several such studies focus on the use of Western- type facilities and cures, possibly because in many settings this use is associated with greater record- keeping and is thus more easily verifiable. Colson’s useful work [8] on factors leading to use of traditional and Western medicine in a Malay village is an exception. Like Stock, he concludes that it is often the nature of the disease more than any characteristic of the population or household that determines whether
1285

1286 JOANNE CSETE
Western or traditional health services are sought first. Uyanga [9], working in Nigeria, and Mwabu [IO] in Kenya also assert the importance of the stage of the illness in the determination of the type of healer sought. A study from Bangladesh [I I] suggests the importance of current health status of the child and the child’s sex as determinants of seeking Western medical care.
The Rwandan highlands, where the present study was conducted, are characterized by high population density, intense cultivation of steep hillsides, and a rugged mountainous terrain. There are no villages; rather, small farms dot the hillsides. There are markets weekly at designated sites, usually in the valleys or foothills. In the study site from which data are reported here, the principal health facility, a small hospital with an outpatient clinic, was located near a market area.
In this setting, a routine health center visit costs about U.S.SO.50 plus the cost of prescribed medi- cines, which may run as high as several dollars. A number of prescription medicines are available in local markets, often at a considerable discount from the health-center price. Forma1 consultation with traditional healers in response to some conditions can be very costly-up to U.S.$50, an enormous sum for these households-but various traditional medicines can be obtained at low cost.
Little ethnomedical research has been done in Rwanda to inform a complete classification of local disease perceptions [ 121. In general, most diseases are named and recognized by their principal symptoms. A generic classification of diarrhea] disease from the Kinyarwanda guhirwn (to have diarrhea) is recog- nized throughout Rwanda. Guhitwu inzoka, to have diarrhea caused by intestinal worms, is also recog- nized. Other commonly reported ailments include cough (inkorortz); fever (umuliro), which stands on its own as an illness but may also accompany other illnesses: and vomiting (ukuruka). An exception to the naming of an illness by its symptom is uburozi
or ‘poisoning’. Incidents of ‘poisoning’ of a family member, said to occur through ingestion of food that has been tampered with. are often regarded to be acts of retribution against the family. In the study region. a number of plant species growing locally were taken to be sources of poison. It was often said that the antidotes were available from the provider of the poison.
In this paper, the responses of women in this region to episodes of a variety of illnesses among their children under age 6 and to their own illnesses are examined. In particular, the association between health-seeking behavior and a number of maternal and household characteristics is considered.
Some 143 women and their 303 children under age 6 from Giciye Commune. Rwanda were selected at
random for this study, which is part of a larger study on links between agriculture and nutrition [see 13 and 141. (The author lived for I5 months in the study area.) The population of Giciye Commune at the time of the study was about 54,000. Only four of the Commune’s I3 sectors were included in the survey for logistical reasons; these four sectors had a total population of approx. 16,000, of which about 3000 were children under age 5 and about 4100 were women aged 1840. Approximately 215 households were included in the survey, but results are reported here only for those in which at least one child under age 6 was present.
In a IO-month period (JanuaryyOctober 1986). women were asked five times to recall the illness episodes of their pre-school children over the last week and three times to recall illness episodes of the past month. The five weekly recalls coincided with the anthropometric data collection (every two months during the study period), and the monthly recalls coincided with the long rainy season, the long dry season, and the second (shorter) rainy season. During both the monthly and the weekly recalls, women recounted the duration of each episode in days and the treatments they sought in a free-response format. Women were encouraged to report more than one treatment response for each illness episode but very few did so; thus, only the first treatment responses are reported here. The point in the course of the illness episode at which treatment was sought was not reported.
Heights and weights of children were measured concurrent with the weekly morbidity recalls. Socio- economic, demographic, agricultural, and dietary data were collected in a three-round household survey concurrent with monthly morbidity recalls. Agricultural questions changed with each round to reflect the activities of the season. Two of the three rounds included detailed questions on household expenditures to enable a seasonal comparison 01 expenditure patterns. In other respects. question- naires for the three rounds were similar. Data analysis was performed on a micro-computer using SPSS/PC+ (Chicago, IL).
Unfortunately, distances from these households to the health facilities they used were not measured. All households lay within an g-km radius of a health center or hospital with out-patient services. Since the principal health facility for most of the households in the survey was located on a road (unpaved) running through the foot of the mountains. persons living at the highest altitudes may have had the most arduous journey to this facility. Altitude of the homes was measured.
RESULTS
The households of all of the study subjects drew their livelihood principally from small-scale agri- culture (mean landholding per household = approx.

Health-seeking behavior of Rwandan women I287
Table I. Description of sample households
Mean SD
Altitude of homestead (m) 2317 351 No. persons per household 6.17 2.04 Age, fathers of pre-schoolers (yr) 38.8 12.2 Age, mothers of pre-schoolers (yr) 33.9 10.9 % household members c age 6 yr 40.7 14.7 % household members < age 13 yr 52.2 15.5
Percentage % female-headed % in which mother of pre-schoolers is
7.0
one of several wives % nuclear family only living in house,
26.8
i.e. parent(s) and their child(ren) only 83.0
0.75 hectares). Some characteristics of the households are described in Table 1. The households lay at altitudes ranging from 2090m (6860 ft) to 2700m (8860ft) above sea level. At lower altitudes within this range, the staple food crops cultivated (and consumed) are sweet potatoes and beans and at higher altitudes white potatoes and peas. Sorghum is widely cultivated, particularly as a constituent of beer, and is harvested once a year at the beginning of the year.
The high percentage of sample households that are nuclear families-that is, a parent or parents and their child or children only-may reflect the scarcity
of land in the region, which does not allow for support of an extended family. (The percentage of young children in these households compared to that of the general population is high because these households are selected from the full sample because they include pre-school children.) In polygynous arrangements, which are present in about 27% of the households, the wives of a given man do not live in the same household.
The nutritional status of young children is better in this high-rainfall region than Rwandan national averages [15] but still precarious. One quarter of the children in the sample are stunted (< 90% of the NCHS median height for age; see Ref. [16]), and about 15% deficient in weight for age (< 80% of NCHS median).
Women’s responses to the illness episodes of their children under age six are summarized in Table 2, which is based on the monthly morbidity recalls. Results from the weekly recalls were similar. Women’s health-seeking responses may vary with the duration of the child’s illness episode. Results are therefore shown for all illness episodes and for subset of episodes that lasted longer than five days. (Five days is an arbitrary period but, in the opinion of the Rwandan interviewers, represents an approxi-
Table 2. Treatment responses by illness and illness duration for children (monthly recall, rounds combined)
All episodes Episodes of > 5 days
Treatment “0. % “0. %
A. Diarrhea Health center Western medicine Traditional medicine No treatment Other
Total
B. Fewr Health center Western medicine Traditional medicine No treatment Other
Total
C. Cough, cold Health center Western medicine Traditional medicine No treatment Other
50
43 I6 49
I65
45 34
5 50
I35
49 40
8 62
30.3 26.1 9.7
29.7 4.2
100.0
33.3 25.2
3.7 37.0
0.7
100.0
30.4 47 33.6 24.8 35 25.0
5.0 8 5.7 38.5 48 34.3
I.2 2 1.4
46 36.8 32 25.6 IO 8.0 30 24.0
7 5.6
Gz- 100.0
40 40.4 27 27.3
4 4.0 27 27.3
I 1.0
99 100.0
- ___ Total I61 100.0 140 loo.0
D. Poisoning--all rounds (monthly and weekly recalls) Western medicine I 9.1 Traditional medicine (purchased) 8 72.7 Traditional medicine (other) 2 18.2
Total II 100.0
E. Other illness--all rounds (monthly and weekly recalls) Health center 24 27.6 23 30.3 Western medicine 24 27.6 20 26.3 Traditional medicine 9 10.3 9 I I.8 No treatment 29 33.3 23 30.3 Other I I.1 I 1.3
~ ____ _____ Total 87 100.0 76 100.0
I288
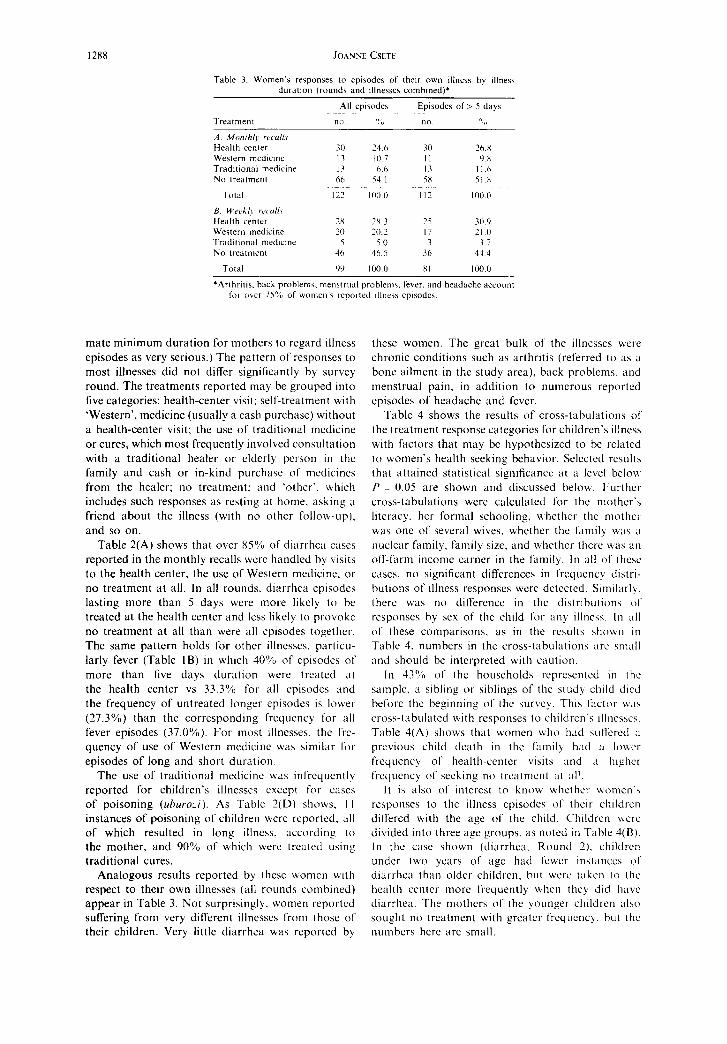
Table 3. Women’s responses 1” episodes of their own illness by illness
duration (rounds and illnesses combined)*
All episodes Epiwdes of > 5 days
“(3 ” ,I “” ” I,
A. ,Monrh/~ reudl\
Health center 30 24 6 30 26 X
Western medicme 17 IO 7 II YX
Tradmonal medune 13 hh 13 I I 6 No treatment 66 54 I 5x 51.X
TOlLi 122 IO0 0 II? I no 0
B. U&/~ I<‘( O/l\
Health center 7x 2X.3 25 30.‘)
Western medicine 20 20.2 I7 ?I .(I Traditmnal meduns 5 5.0 3 17
No treatmenl 46 4h S 36 44.4
Total YY 100.0 XI 100.0
‘Arthritis. back problem?, mena~rual problem\, fever. and headache account
for over 75% of women‘s reported illness epwdes.
mate minimum duration for mothers to regard illness episodes as very serious.) The pattern of responses to most illnesses did not differ significantly by survey round. The treatments reported may be grouped into five categories: health-center visit; self-treatment with ‘Western’, medicine (usually a cash purchase) without a health-center visit; the use of traditional medicine or cures, which most frequently involved consultation with a traditional healer or cldcrly person in the family and cash or in-kind purchase of medicines from the healer; no treatment: and ‘other’. which includes such responses as resting at home. asking a friend about the illness (with no other follow-up). and so on.
Table 2(A) shows that over 85% of diarrhea casts reported in the monthly recalls wcrc handled by visits to the health center, the use of Western medicine. or no treatment at all. In all rounds. diarrhea episodes lasting more than 5 days were more likely to be treated at the health center and less likely to provoke no treatment at all than were all episodes together. The same pattern holds for other illnesses, particu- larly fever (Table IB) in which 40% of episodes of more than five days duration were treated at the health center vs 33.3% for all episodes and the frequency of untreated longer episodes is lower (27.3%) than the corresponding frequency for all fever episodes (37.0%). For most illnesses. the frc- quency of use of Western medicine was similar fat episodes of long and short duration.
The use of traditional medicine was infrequently reported for children’s illnesses except for cases of poisoning (uhuro~i). As Table 2(D) shovvs, I I instances of poisoning of children wcrc reported, all of which resulted in long illness. according to the mother, and 90% of which were treated using traditional cures.
Analogous results reported by these women with respect to their own illnesses (all rounds combined) appear in Table 3. Not surprisingly. women reported suffering from very different illnesses from those of their children. Very little diarrhea was reported by
these women. The great bulk of the illnesses were chronic conditions such as arthritis (referred to as a bone ailment in the study area). back problems. and menstrual pain, in addition to numerous reported episodes of headache and fever.
Table 4 shows the results of cross-tabulations of the treatment response categories for children’s illness with factors that may be hypothesized to be r&ted to women’s health seeking behavior. Sclccted results that attained statistical significance at a level below P = 0.05 are shown and discussed below Further cross-tabulations were calculated for the mother’s literacy. her formal schooling, whether the mother vvas one of several wives. whether the family wxs a nuclear family. family size, and whcthcr thcrc was an off-farm income earner in the family. In all of thcsc cases, no significant differences in frcqucncy Jistri- butions of illness responses were detected. Similarly. there was no difference in the distributions ot responses by sex of the child for any illness. In alI
of these comparisons, as in the results shown in Table 4. numbers in the cross-tabulations arc small and should bc interpreted with caution.
In 43% of the households rcprcscntcd in the sample. a sibling or siblings of the study child died before the beginning of the survey. This litctor was cross-tabulated with responses to children’s illncsscs. Table 4(A) shows that women aho had suffered ;I previous child death in the family had ;I lower frequency of health-center visits and a highct frcqucncy of seeking no trcatmcnt at ~tl’.
It is also of interest to know whether womcn‘~ responses to the illness cpisodcs of their children differed with the age of the child. Children \hct-c divided into three age groups. as noted in Table 4(B). In the case shown (diarrhea, Round 2). children
under two years of age had fewer tnstances 01
diarrhea than older children, but were taken to the
health center more frequently when they did have diarrhea. The mothers of the younger children also sought no treatment with grcatcr frequency. hut the numbers here are small.

Health-seeking behavior of Rwandan women 1289
Women’s control of categories of expenditures other than those associated with the health of their children may be reflected to some degree in patterns of their health-seeking behavior. This connection is considered in Table 4(C). The measure of women’s control of food expenditures used in Table 4(C) is an estimate from the household survey of the value of food-related transactions under the women’s control during the survey period divided by the number of adults equivalents in the household. This continuous indicator was recoded into a two-level categorical variable around its mean for this cross-tabulation. Women with a higher degree of control over food expenditures made somewhat more frequent health- center visits on their children’s behalf. They also had somewhat higher frequencies of seeking no treatment and somewhat lower frequencies of use of Western medicine for fever and ‘other’ illness episodes.
As noted above, vertical distance (i.e. altitude) may be an important determinant of accessibility of health services in this setting. The continuous altitude vari- able is recoded into three categories for the cross- tabulations shown in Table 5. The significance of the P-values of the comparisons in both parts of the table is due in large part simply to the greater incidence of diarrhea and fever in the children living at higher altitudes. Health-center visits were less frequent
in Round I for the children in the highest-altitude group who suffered diarrhea, but the same pattern
was not found for fever (all rounds). In both cases, mothers in the highest-altitude group had a higher frequency of seeking no treatment than those at lower altitudes.
The results in Tables 4 and 5 suggest the need for mulitivariate analysis of these health-care decisions, but the numbers of cases reported of the various illnesses are generally small, and the decision-making outcome is categorical. To address these problems, a continuous dependent variable was calculated as the proportion of children’s diarrhea episodes (because diarrhea was the most frequently reported illness) to which some active response was made (that is, one minus the proportion for which no treatment was sought). A number of independent variables were tested for their simultaneous associations with this outcome, including mother’s control of food pur- chases and other expenditures, mother’s literacy, mother’s age at the time of her first pregnancy (thought by some observers to be a positive indicator of the ‘progressiveness’ of women if not also of their social class), child’s age and sex, total expenditures of the household during a given period (indicating in- come status), number of persons in the household, whether the household had suffered the death of a
Table 4. Frequemes of treatment choms for children by selected factors of interest: cross. tabulations
A. Treatment choice for fever vs sIbline death in the “ast Cweeklv recall. Round 11
Treatment
No illness” Health center Western medicine No treatment
Total
No death Post ambling death no. C-01. % no. Cal. %
155 X6. I 109 88.6 15 8.3 2 1.6 4 2.2 I 0.X 6 3.3 II 8.9
180 100.0 I23 100.0
x’= 10.9; df= 3; P = 0.01
B. Treatment choice for diarrhea by age of child at beginning of survey (montly recall, Round
2)
O---24 months 2548 months t 48 months
No illness XI 75.0 80 x7.9 93 91.2 Health center I2 I I.1 2 2.2 3 2.9 Western medicine 7 6.5 4 4.4 4 3.9 Traditional medicine I 0.9 2 22 I I.0 No treatment 7 6.5 3 3.3 I 1.0
Total I08
12 = 19.1; Af= IO; P = 0.04.
100.0 91 100.0 102 100.0
C. Treatment choice for ‘other’ Illness by woman’s control of food expenditures (monthly recall. all rounds)
Treatment Low control High control
no. Cal. % no. Cal. %
No illness 156 89.7 107 X3.6 Health center I 0.6 X 6.3 Western medicine 9 5.2 4 3.1 Traditional medicine 4 2.3 2 1.6 No treatment 4 2.3 7 5.5
TOVdl 174 100.0 I28 100.0
x2 = 13.0; d/ = 6; P = 0.04. “No illness episodes; figures shown only to show relatwe frequency of illness episodes in
comparison groups.

1290 JOANNE CSETE
Table 5. Freuuenaes of treatment responses bv altitude selected cross-tabulattons
< 2235 m 223&2364 m t 2365 m Treatment no. % no. % no. %
A. Duvrhea (monrhly recoil. Round I)
No illness x7 79. I 76 76.X 62 66.0 Health center II 10.0 II II.1 4 4.3 Western medicine 6 5.5 2 2.0 9 9.6 Traditional medicine 4 3.6 I 1.0 3 3.2 No treatment 2 IX 9 9. I 16 17.0
Total 110 100.0 99 100.0 94 100.0 x’= 26.3; df = IO: P =0.013.
R. Fwer (monthl, recall. all row&)
No illness 78 68.9 72 72.7 44 46.X Health center 9 8.2 7 7.1 I3 13.X Western medicine II IO 0 9 9.1 II I I.7 Traditional medicine I 09 I I .o 2 2.2 No treatment II 10.0 IO IO.1 24 25.5
Total 110 100.0 99 100.0 94 100.0 Y’ = 28.9: (If= 16: P = 0.02
child, whether the house is rectangular (round houses are associated with poverty), and mother’s current age.
The results of evaluating these factors by ordinary least-squares regression appear in Table 6. Altitude was the only independent variable significant at P < 0.05, and its negative coefficient is highly signifi- cant. That is, women at lower altitudes are found to make more active responses to their children’s diarrhea episodes than do women at higher altitudes, as suggested in Table 4. Mother’s control of food expenditures approaches significance in a positive direction if included in the model, echoing Table 3(E). Mother’s literacy would also have P < 0.10 in the model with a positive coefficient. The other factors do not approach significance, but signs of coefficients are as expected. The child’s sex and the mother’s having taken a non-formal course had no significance in the model.
DlSCUSSlON AND RECOMMENDATIONS
Because of the relatively small numbers involved in some of the comparisons shown above, these results
Table 6. Determinanta of active response to children’s diarrhea: multiole reeresston results . -
Dependent variable: Proportion of child’s diarrhea episodes to which some response was made (health center visit or medicine admmtstered)
Independent variables B or [j” Signif.
SelecttYi h,v .S,qw’S’ procedure: Altitude ~0.0005 0.0065 N,JI srkred: Mother’s control of food exp. 0. I378 0.068 Mother is literate 0.1276 0.09 Age of mother’s 1st pregnancy 0.0976 0.22 Age (child) 0.0758 0.32 Total expenditures of household 0.0520 0.49 Number of members of household -0.0419 0.59 Prev. child death in family -0.0357 0.64 Whether house is rectangular 0.0316 0.68 Age (mother) 0.0236 0.76
R’= 4.3%. F (regr) = 7.59. Adj. R* = 3.8%. Signif. F = 0.0065. “Value shown is B for variable ‘Altitude’ and p for other variables
should be interpreted with caution. A much larger sample of children or much higher incidence rates would be more revealing. The grouping of treatments across illnesses addresses this statistical problem to some degree but introduces theoretical problems. The absence of information on the point during the course of the illness at which treatments were sought is another weakness of this data set.
Some of the results are nonetheless suggestive of factors that may be of interest to health practitioners and policy-makers in Rwanda. The infrequent use of traditional cures and traditional healers for diseases other than ‘poisoning’ relative to the use of Western- type treatments suggests that (I) there is some expec- tation of cure by Western methods on the part of these women; (2) there is significant under-reporting of the use of traditional treatments in response to the illnesses listed here, or (3) some traditional cures are beyond the financial reach of these women who then fall back on the less desirable Western methods. Women in the study population sometimes expressed the view that persons not from the Giciye area would be unlikely to appreciate their use of traditional cures for certain ailments. For this reason, they may have under-reported the occurrence of ailments for which traditional cures would more readily be sought. Such under-reporting has been uncovered elsewhere in Africa [l7]. Further study of the relative import- ance of traditional and Western responses to some diseases might be of use to health-care providers in this setting.
That frequency distributions of responses differed with longer duration of the illness episode indicates either that women’s responses even to such illnesses as diarrhea were not rapid or that the longer episodes were more severe from the beginning and thus more likely to be treated actively. If the former is the case. it is a matter of some concern. It is also striking that women displayed little or no knowledge of oral rehydration therapy as a first response to diarrhea in their young children. In a setting in which approxi- mately one third of all diarrhea episodes were report-

Health-seeking behavior of Rwandan women 1291
edly left untreated, oral rehydration education might population is very small, skewing the frequency
address an important need. While one may hope that distributions somewhat. That comparisons made
oral rehydration is explained to a mother at a health- with respect to family size were not significant may
center visit made in response to a young child’s not be surprising. The presence in the household of
diarrhea, casual observations indicated that counsel- older children may free the mother to respond ing of women during health-center visits in this area actively to younger children’s illness in spite of the
is often lacking. greater demands of her larger family. The lower frequency of health-center use among
women with a deceased child echoes the finding of Bhardwaj and Paul in Bangladesh [l 11. These authors suggest this result stems from the firmly held belief among certain parents that a seriously ill child should not be exposed to the elements on a trip to the health facility. In the present study, it is likely that certain beliefs about children’s health would be unshaken by the death of one child, particularly if that death entailed no contact with health agents who might suggest new treatment choices. In addition, time constraints or economic barriers to the use of health centers for a household or a woman might be in- tractable over time and, indeed, might be exacerbated by the death of a child in this setting. The lower frequency of health-center use itself may be indicative of other health-related attitudes and practices in the household that are associated with higher infant mortality.
In this setting, establishing a health-care response model based on responses to hypothetical questions, as in Young’s work, would be unwise. Tests of the survey instrument before the first survey round indicated that women would give highly idealized responses to hypothetical questions and, in particu- lar, would not be likely to offer ‘no treatment’ as a response to diarrhea. Where infectious disease is frequently left untreated but there has been enough contact with Western health education to suggest that treatment is the more acceptable practice, Young’s method may be less useful. Indeed, the numeric results presented here simplify long stories about health care recounted in some interviews. Several interviewers felt a ‘thick description’ approach might be best for depiction of these health-seeking behaviors, but time and other constraints did not allow for it to be used.
The altitude results in Table 5 suggest two areas of concern. First, the higher incidence of illness episodes among children in the highest-altitude regions is remarkable. A higher incidence of diarrhea in the highest altitude group was found, particularly during the heavy rainy season. A UNICEF water specialist working in the area considered the drinking water sources of the high-altitude households to be no less safe than those in the lower-altitude areas (C. Massar, personal communication). It is not clear whether the harsher climate of the highest-altitude area may be related to this higher incidence of children’s illness, as is believed by many women in the sample. Secondly, there may be greater reluctance to make the trip to the health center from the high-altitude households, as suggested in Table 5(A). The regression results in Table 6 indicate, however, that it is not only health- center visits but all ‘active’ responses to children’s diarrhea episodes that decline with altitude. Whether this result is related to greater workloads of women at higher altitudes or some other factor is worth examining.
It is not possible with the data at hand to evaluate the importance of various treatment responses to the improvement of child (or maternal) survival in this setting. Duration of illness in a previous period was, however, the most consistent predictor of current nutritional status for both women and children in this study in large multivariate models including many household and maternal social and economic factors as independent variables 114, pp. 229-280, 307-3091. Even in sub-groups for which household food supply was abundant, illness dur- ation had a significant negative association with nutritional status during the survey period. Insofar as nutritional status is an indicator of survival probability, at least for children, these results high- light the importance of response to illness as a key to child survival in this setting.
Accessibility of options for dealing with disease, then, is of great importance for women and young children in this population. Some recommendations suggested by these results for policy makers concerned with child-survival programs are as follows:
The factors that did not result in significant differ- ences in the regression and cross-tabulations are as meaningful as those that did. The presence of an off-farm income earner (usually a man) in the house- hold, for instance, was not associated with health- seeking behavior patterns. The overall level of household income may be less important with respect to treatment options for the children than is the women’s control of the existing level of income. It is also interesting that formal schooling made no signifi- cant difference in the treatment choices of these women, though the rate of formal education in the
-Oral rehydration therapy and other simple treat- ments not requiring a trip to the health center should be accessible to all women. Information on their use should be part of the curricula of all community agents having frequent contact with households. Others [e.g. 181 have made similar suggestions.
-Literacy courses for women, of which there are many, public and private, in Rwanda, should also include basic information on child survival and on effective responses to and prevention of

1292 JOANNE CSETE
children’s illnesses. Education on vaccination and oral rehydration should be emphasized.
-Planning of health facilities and mobile health 9
services should take into account vertical dis- tance between households and service providers. 10
AcknoM,ludX~n,enrs-The data collection for this paper was supported in Rwanda by the Government of the Federal
, ,
Republic of Germany through the International Food Policy Research Institute (J. von Braun. principal investi- gator for Rwanda project).
12
13
REFERENCES
Ministere du Plan (Republic of Rwanda) EnquLte Nationale SW Ie Budget et la Consommation des Mtinuges. Vol. 2: Structure du Budget des M&ages. 14 (1986). Young J. C. A model of illness treatment decisions in a Tarascan town. Am. Erhnol. 7. 106. 1980. Young J. C. Medical choice in (1 Mexican Gilage. 15 Rutgers University Press, New Brunswick, NJ, 1981. Janzen J. M. Th; Quest for Therapy in Lower Zaire. University of California Press, Berkeley. 1978. Turner VT Drums of4fflicrion. Clarendon Press. Oxford. 16 1968. Stock R. Distance and the utilization of health facilities 17 in rural Nigeria. Sot. Sci. Med. 17, 563, 1983. Okafor S. 1. Factors affecting the frequency of hospital trips among a predominantly rural population. Sot. Sci. Med. 17, 591, 1983. 18 Colson A. C. The differential use of medical resources
in developing countries. J. Hlfh .soc. Behut.. 12, 226. 1971. Uyanga J. The characteristics of patients of spiritual healing homes and traditional doctors in southeastern Nigeria. Sot. Sri. Med. 13A, 323, 1979. Mwabu G. M. Health care decision at the household level: Results of a rural health survey in Kenya. Sot,. Sci. Med. 22, 315, 1986. Bhardwaj S. M. and Paul B. K. Medical pluralism and infant mortality in a rural area of Bangladesh. SW. .Sci. Med. 23, 1003, 1986. Taylor C. C. The concept of flow in Rwandan popular medicine. Sot. Sci. Med. 27, 1343, 1988. von Braun J., de Haen H. and Blanken J. Commercial- ization of agriculture under conditions of population pressure: A study in Rwanda on production. consump- tion, and nutrition effects, and their policy implications. International Food Policy Research Institute report. 1988. Csete J. Determinants of young children’s nutritional status in a Rwandan highland region with special attention to the Gishwati potato scheme. Ph.D dissertation, Cornell University. 1989. Ministere de la Sante Publique et des Alfaires Sociales (Govt. of Rwanda). Resultats de l’enquete sur I’etat nutritionnel des enfants de 0 a 5 ans au Rwanda. Kigali. 1987. National Center for Health Statistics Month/>, C’itul Sfutistics Rep. 25,(3), Suppl. (HRA) 76 1120. 1976. Kloos H., Etea A.. Degefa A.. Aya H.. Solomon B.. Abera K.. Abegaz A. and Belemo G. Illness and health behavior in Addis Ababa and rural Central Ethiopia. Sot. Sci. Med. 25, 1003. 1987. UNICEF/Rwanda Situtrrion Ancr/~sr.v of C‘hi~dren trnd Women in Rwundrr. UNICEF:Rwanda, Kigah. 19X7.