health effects refractory ceramic fibres: scientific...
TRANSCRIPT

Occupational and Environmental Medicine 1995;52:433-440
Health effects of refractory ceramic fibres:scientific issues and policy considerations
L R Glass, R C Brown, J A Hoskins
AbstractObjectives-To review the scientific liter-ature on the health effects of refractoryceramic fibres (RCFs). The adverseeffects of exposure to asbestos has led toconcern about the potential for otherfibrous materials to cause diseases. Forthis reason the human populations mostheavily exposed to synthetic mineralfibres have been examined for anyadverse effects and many types of fibrehave been studied in animal experiments.One type of man made vitreous fibres(MMVFs), refractory ceramic fibres(RCFs), are principally used in thermalinsulation at high temperatures-up to14001C. As manufactured RCFs exist in aglassy, non-crystalline (sometimes calledamorphous) state, they have variouscompositions, physical properties, andsized fibres.Methods-All reports on the healtheffects of RCFs available up to the end of1994 have been examined and the scien-tific literature reviewed although all pub-lications have not necessarily beenreferenced.Conclusions-In recent inhalation experi-ments conducted with both rats andhamsters at the Research and ConsultingCompany, Geneva, at the highest dosetested (30 mg/ml) there was an increasedincidence of tumours in both species.Lower doses were only examined in therat and at these doses there was no signif-icant excess of lung tumours.Epidemiological investigations of work-ers engaged in the manufacture ofceramic fibres have shown a small excessof pleural plaques. This phenomenon isbeing further investigated but could bedue to confounding exposures. The popu-lations available for study are small andtheir exposures fairly short, but it is con-sidered prudent that they should remainunder surveillance for some time tocome. This is despite the fact that presentexposures in the ceramic fibre industryare low (< 1 f7ml) and are being reduced.
(Occup Environ Med 1995;52:433-440)
Keywords: man made vitreous fibres; tumours; rodentinhalation; epidemiology
The health effects of exposure to amphiboleasbestos are universally accepted although
there is no clear consensus about chrysotile, aserpentine mineral and the commonest typeof asbestos. It is prudent that other fibrousmaterials are examined for any effects similarto those caused by the natural materials andman made vitreous fibres continue to be stud-ied. Most of the extensive experimental workand the epidemiological investigations ofexposed workers have failed to detect anyclear evidence of pathogenesis. In this paperthe results of such research on one type offibre-refractory ceramic fibre (RCF)-arereviewed. We think this is particularly timelyas most of the data are not readily availableand appear only in private reports or reportsawaiting publication.The pathogenicity of fibres is related to
their size, morphology, and durability in tis-sue,' and differences, especially in the durabil-ity in tissues, make it possible that differenttypes of man made fibre pose substantiallydifferent levels of human risk. The terms usedto describe different classes of fibres are oftenimprecise. The term ceramic fibre has beenused for materials with very different physicalproperties and chemical compositions includ-ing crystals or whiskers of silicon nitride, sili-con carbide, or potassium titanate andpolycrystalline alumina or zirconia fibres.These crystalline fibres are not further dis-cussed in this review. The RCFs that form thebulk of ceramic fibres are vitreous aluminosili-cates manufactured as wools and are mostlyused for high temperature insulation. Theyare high alumina silica glasses more closelyrelated to other glasses than they are to crys-talline materials from which they must be dis-tinguished. Due to the random (spinning orblowing) processes used in manufacture of allthe insulation wools (including RCFs) thesecontain fibres with diameters and lengths thatvary both within individual products andbetween different product types.
History, applications, and properties ofrefractory ceramic fibresThe RCFs are made either by melting a com-bination of alumina and silica (Al203 andSiO,) in roughly equal proportions, or bymelting calcined kaolin. The melt is allowedto pass as a fine stream through a port in thebottom of the furnace where it is then actedon by a high velocity air jet or allowed to flowonto a series of spinning wheels. Other oxidessuch as zirconia (ZrO,), boric oxide (BO0), ortitania (TiO,) are sometimes added to themelt to alter the temperature resistance or
The CarborundumCompany, 625 BuffaloAvenue, PO Box 337,Niagara Falls, NY14302 0337, USAL R GlassMRC Toxicology Unit,Hodgkin Building,University of LeicesterR C BrownJ A HoskinsCorrespondence to:Dr R C Brown, MRCToxicology Unit, HodgkinBuilding, University ofLeicester, PO Box 138,Lancaster Road, LeicesterLE1 9HN.Accepted 5 April 1995
433 on 23 M
ay 2018 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.52.7.433 on 1 July 1995. Dow
nloaded from

Glass, Brown, Hoskins
Table 1 Physical properties of refractory ceramic fibresProperty Value
Softening point (0C) 1740-1800Refractive index 1-55-1-57Density (g/cm') 2-6-2-7Elastic modulus (Gpa) 80-100Non-fibrous particulate
shot (weight %) 40-60Diameter Variable, dependent upon
manufacturing process
other properties of the resulting fibre. Table 1shows the physical properties of some RCFsand table 2 shows the chemical formulation ofthree representative types.
Experimental RCFs were first produced inthe early 1940s and commercial productionbegan in the 1950s. The energy crises of the1970s stimulated their use as they were recog-nised as a cost effective and energy efficientsubstitute for hard brick refractories. Theiruse as high temperature insulation can reduceenergy consumption by more than 50% com-pared with alternative products.2 The RCFsare used as insulation in furnaces and similarplant, at temperatures up to 1400'C and alsohave uses in "advanced composites" and forfire protection. Specialist uses for RCFsinclude the heat shields on aircraft (both com-mercial and military), tanks, and cruise mis-siles, and in the heat resistant tiles on theexterior of the space shuttle. Production ofRCFs represents less than 2% of the overallMMVF market. As, unlike other MMVFssuch as glass fibre and rockwool, they arerarely used in consumer products there is nopossibility of significant exposure of the gen-eral public.When RCF is exposed to temperatures in
excess of 10000C, it can devitrify with the for-mation of mullite, a crystalline aluminium sili-cate, and silica, in the form of fl-cristobalite.'In a furnace this reaction occurs only at thehot inner surface of the lining and most of itsthickness remains in the glassy state.
Properties of fibres related to theireffects on healthIt is now generally accepted that the effects offibre exposure are related to three main vari-ables-namely, dose, fibre length, and diame-ter and the persistence of fibres oncedeposited in the body.
Differences in persistence could determinethe differences between the health effects ofamphibole and chrysotile asbestos4 as
Table 2 Weight (%/6) comparison of typical refractory ceramic fibresConstituent Kaolin basedfibre High purity fibre Zirconia grade fibre
SiO2 49 5-53-5 48-5-54 47 5-50AI,03 43-5-47 45-5-50 5 35-36ZrO2 01 02 15-17TiO2 2 0-02 0 04Fe2O, 1 < 0 2 < 0-05Cr2O, < 0 03 < 0-01 < 0-01MgO <0-1 <0-01 0-01CaO < 0.1 < 0 05 < 0-05Na2O 0 5 0-2 < 0-3K20 < 0-01 < 0-01 < 0-01
chrysotile is cleared more rapidly from thelungs. Differences in durability between dif-ferent man made fibres could mean that dif-ferent fibres pose different levels of hazard.
Although the importance of durability iswidely, but not universally, accepted there ismuch more agreement about the role of fibredimension or morphology. The role of dimen-sion is perhaps the "central dogma" of fibretoxicology with both length and diameterbeing important. As the least fibre diameter isthe main determinant of respirability-that is,the capacity of a fibre to penetrate to the distalregions of the lung-it may also determinebiological activity once deposited. The lengthof the fibres is also of importance as firstshown by Gardner (quoted by Vorwald et al)in the 1930s in a series of inhalation experi-ments with mineral fibres where chrysotileconsisting mainly of short fibres produced lessasbestosis than longer chrysotile fibres.5
Injection or implantation of mineral fibresinto the pleural or peritoneal cavities has eluci-dated the role of dimension particularly indetermining the ability of a fibre to causemesothelioma.$-" The effect of fibre size hasalso been shown after inhalation exposureespecially by Davis et al who used three sam-ples of amosite asbestos with very differentfibre lengths.'2 1" In a particularly dramaticdemonstration of the role of length Wagnerreported that shortening the fibres of erionitedestroyed the extreme carcinogenicity of thiszeolite mineral.'4 Long fibres are also moreactive in various in vitro systems where clear-ance, deposition, and respirability cannot beplaying a part.'5 The role of fibre dimension asa determinant of activity in humans is moredifficult to show but Lippmann has suggestedthat asbestosis, lung cancer, and mesothe-lioma are related to different sized fibres.'6
Thus, long fibres are more biologicallyactive and fibre diameter affects respirability,the final disposition of fibres in the body, andbiological activity. The actual dimensions offibres responsible for disease or the exact rela-tion between activity and size remain uncer-tain.
Finally, exposure is rarely to fibres alone-some contamination with respirable non-fibrous particulates is inevitable even inexperimental systems. Few experimental stud-ies have considered the effects of such mix-tures. In the case of humans, exposure isalways to complex mixtures including, forexample, tobacco smoke and in this case thereis a well established synergistic interactionbetween asbestos and cigarette smoking.'7
Results of studies on RCFsANIMAL EXPERIMENTSCeramic fibres have been examined by injec-tion or implantation by several authors, andthe data is in agreement with the generalfinding that inocula of long thin fibres cancause tumours after injection into bodycavities.78 18 ' As a consequence of the lackof specificity of these methods mostauthors reject the production of tumours by
434 on 23 M
ay 2018 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.52.7.433 on 1 July 1995. Dow
nloaded from
Health effects of refractory ceramic fibres: scientific issues and policy considerations
placement into cavities as being predictive ofhuman hazard.Y22 Only inhalation exposure
simulates the normal route of exposure inhumans and is the most relevant means forhazard identification and risk assessment ofnovel fibres. Unfortunately, inhalation bioas-says are costly, complex, and time consumingalthough such studies are essential if theresults of animal experiments are to produceresults that are scientifically defensible. Thefirst inhalation experiments with any fibresthat produced clear positive carcinogeniceffects were reported by Gross et al who hadexposed rats to chrysotile asbestos.2' Gross etal had previously examined RCF in rats anddetermined that the effect was comparablewith exposure to an inert dust.24 In a secondRCF inhalation experiment Davis andcoworkers exposed 48 Wistar rats to aerosolsthat contained 95 ceramic fibres/ml, in awhole body exposure for seven hours a day,five days a week for 12 months.25 Eightrats developed pulmonary tumours of whichthree were carcinomas. Unusually there wasone peritoneal mesothelioma, a finding ofunknown relevance.The third experiment with ceramic fibres
was carried out by Smith and coworkers whoexposed both Osborne-Mendel rats andSyrian Golden hamsters to 200 f/ml for sixhours a day, five days a week for two years.'9No excess of tumours was found in the ratsand little, if any, fibrosis. In the hamstersthere was no fibrosis but one animal devel-oped a pleural mesothelioma.The above investigations used only indus-
trial ceramic fibres milled or ground to reduceoverall fibre length. The aerosols producedcontained material that was not respirable byrodents and fragments of the glassy ball"shot" that makes up about 50% by weight ofthese materials. In normal use this shot wouldnot fragment and these contaminants wouldnot make up part of any workplace RCFaerosol. The amount and size of the fibres inthe lungs of the exposed animals was notreported. To compensate for the limitations ofthese earlier experiments a series of investiga-tions were commissioned by the RCF indus-try and carried out at the Research andConsulting Company, Geneva. The RCF
materials used in the Research andConsulting Company experiments were cho-sen to reflect the range of compositions towhich humans might be exposed. These were:a kaolin based fibre; a "high purity fibre",made from alumina and silica; a zirconia fibre,containing 15% zirconia; and the kaolin fibre,heated to simulate a devitrified, "after use"fibre.The RCF used in these experiments was
isolated from the bulk material so as toremove the shot and maximise the content offibres able to be respired by rodents. Sizeselection was carried out with a proprietarymethod that involved chopping the fibre, siev-ing, and grinding the shortened fibre, and twowater elutriation size separation steps. Nearly 1tonne of each commercial product had to beprocessed to provide the material used in theexperiments. This material represented about1 %, by mass, of the "as manufactured" prod-uct. The experimental fibre was "lofted" in agenerator that did not further break the fibresand the animals were exposed in a nose onlysystem in which the aerosol was notrebreathed. With these methods lung burdenwas maximised in relation to exposure26 andpresumably this also maximised the potentialfor lung damage.
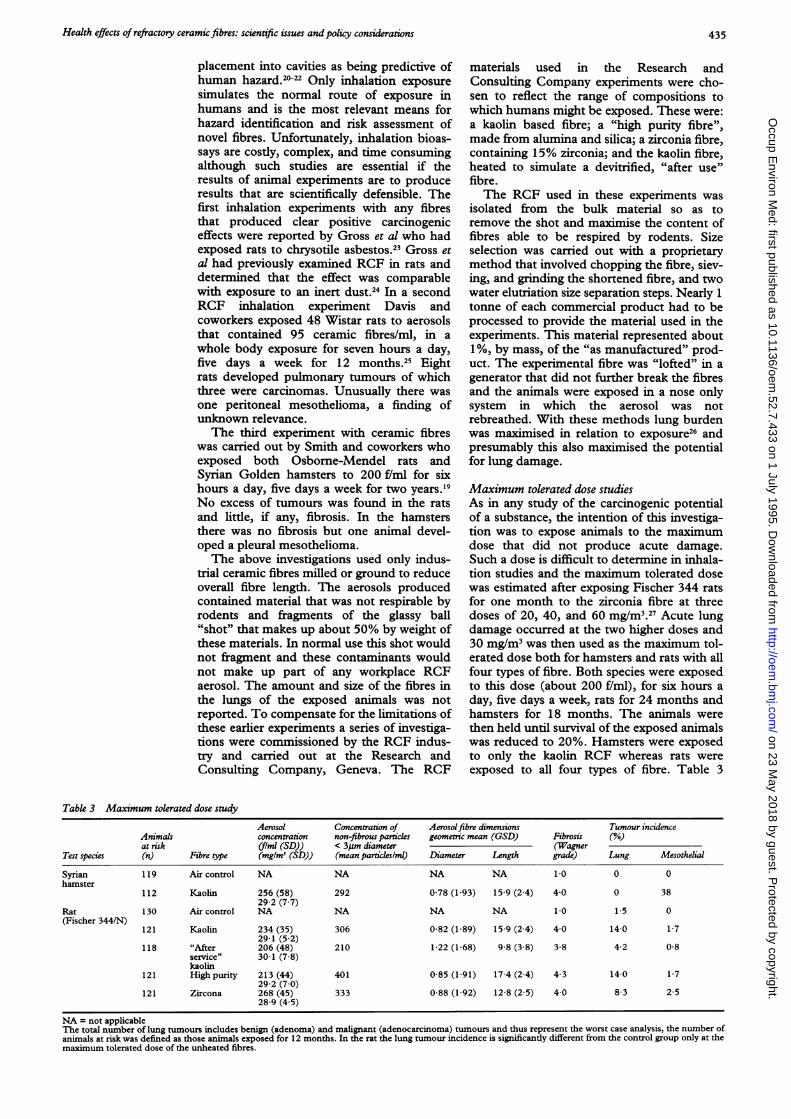
Maximum tolerated dose studiesAs in any study of the carcinogenic potentialof a substance, the intention of this investiga-tion was to expose animals to the maximumdose that did not produce acute damage.Such a dose is difficult to determine in inhala-tion studies and the maximum tolerated dosewas estimated after exposing Fischer 344 ratsfor one month to the zirconia fibre at threedoses of 20, 40, and 60 mg/M3.27 Acute lungdamage occurred at the two higher doses and30 mg/m3 was then used as the maximum tol-erated dose both for hamsters and rats with allfour types of fibre. Both species were exposedto this dose (about 200 f/ml), for six hours aday, five days a week, rats for 24 months andhamsters for 18 months. The animals werethen held until survival of the exposed animalswas reduced to 20%. Hamsters were exposedto only the kaolin RCF whereas rats wereexposed to all four types of fibre. Table 3
Table 3 Maximum tolerated dose studyAerosol Concentration of Aerosolfibre dimensions Tumour incidence
Animals concentration non-fibrous particles geometric mean (GSD) Fibrosis (%/0)at risk (f/ml (SD)) < 3um diameter (Wagner
Test species (n) Fibre type (mg/M3 (SD)) (mean particles/ml) Diameter Length grade) Lung Mesothelial
Syrian 119 Air control NA NA NA NA 1 0 0 0hamster
112 Kaolin 256 (58) 292 0-78 (1-93) 15-9 (2 4) 4-0 0 3829-2 (7-7)
Rat 130 Air control NA NA NA NA 1.0 1-5 0(Fischer 344/N)
121 Kaolin 234 (35) 306 0-82 (1-89) 15-9 (2 4) 4 0 14-0 1-729-1 (5-2)
118 "After 206 (48) 210 1-22 (1-68) 9-8 (3-8) 3-8 4-2 0-8service" 30-1 (7 8)kaolin
121 Highpurity 213 (44) 401 0-85 (1-91) 17-4 (24) 4-3 14-0 1-729-2 (7-0)
121 Zircona 268 (45) 333 0-88 (1-92) 12 8 (2-5) 4 0 8-3 2-528-9 (4-5)
NA = not applicableThe total number of lung tumours includes benign (adenoma) and malignant (adenocarcinoma) tumours and thus represent the worst case analysis, the number ofanimals at risk was defined as those animals exposed for 12 months. In the rat the lung tumour incidence is significantly different from the control group only at themaximum tolerated dose of the unheated fibres.
435
on 23 May 2018 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.52.7.433 on 1 July 1995. D
ownloaded from

Glass, Brown, Hoskins
Table 4 Multidose study of kaolin fibre in F344 rats
Aerosol Concentration of Aerosolfibre dimensions Tumour incidenceAnimals at concentration non-fibrous particles geometric mean (GSD) Fibrosis (%)risk (f/ml (SD)) < 3um diameter (Wagner(n) (mg/iM3 (SD)) (mean particles/ml) Diameter Length grade) Lung Mesothelial
132 NA NA NA NA 1 0-8 0126 162 (37) 156 0-82 (1-99) 13-8 (24) 4-2 1-6 0
16-5 (1-1)128 91 (34) 141 0-80 (203) 13-9 (25) 4 0 3-9 0-8
8-8 (0 7)125 36 (17) 51 0-80 (206) 13-5 (2-6) 3-2 1-6 0
3 0 (0 4)
Footnotes as for table 3.
summarises the properties of the aerosols usedand the results.A sample of chrysotile asbestos (the
National Institute for Environmental andHealth Studies (NIEHS) intermediate lengthsample) was included in the study; this was ashort fibre with an arithmetic mean length ofonly 2-2 gum (median 0 9 gim) and was used at10 mg/m3. One rat in this group developed amesothelioma. Hamsters had not previouslybeen exposed to this sample of chrysotile.
Forty two of the hamsters exposed to thekaolin RCF were found to have mesothelialtumours after initial microscopic examinationat postmortem examination and review ofroutine lung sections. These tumours weresmall and did not affect survival. Some inter-stitial and pleural fibrosis was also found. Nomesothelial tumours were seen in the animalsexposed to the chrysotile asbestos and nohamsters developed lung tumours.5830
Rats exposed at 30 mg/M3 of the variouschemically different RCFs developed a signifi-cant increase in lung tumours and a fewmesotheliomas were also found in each RCFgroup, but these pleural tumour rates werenot significant. The RCF exposure alsocaused lung and pleural fibrosis but less thanwas seen after exposure to chrysotile. All otherlesions were consistent with expectationsbased on the types, strains, and ages of theanimals in this study.29 31 32
Multidose studyThe study was extended by exposing threeadditional groups of rats to different concen-trations of the kaolin RCF (3, 9, and 16mg/M3, corresponding to about 25, 75, and115 f/ml, table 4). Animals exposed to 16mg/M3 developed pleural and parenchymalfibrosis; at 9 mg/M3 there was mild parenchy-mal fibrosis, whereas at the lowest dose therewere no irreversible effects. There was noexcess of lung tumours at any of these doses;one rat in the 9 mg/M3 group developed amesothelioma.29 3 Table 4 shows the prop-erties of the aerosols used and a summary ofthe results.
Significance of the RCF experimentsThe results from the maximum tolerated dosestudies indicate that exposure to extremelyhigh concentrations of specially processedRCF can produce fibrosis and mesotheliomasin hamsters and fibrosis and lung tumours inrats. Lower doses of fibres were not tested in
hamsters but these produced no excess lungtumours in rats. The sample of chrysotile had,in a previous inhalation experiment at thesame exposure, caused lung tumours in about20% of exposed rats28 and this compares withan incidence of rat lung tumours of 18-8% inthe maximum tolerated dose study. Theabsence of mesotheliomas was predictable asthis fibre is very much shorter than the RCFsand it was not expected to induce significantnumbers of this tumour.
Hamsters do not readily develop lungtumours but are apparently sensitive to thepleural effects of the long (ceramic) fibres. Itis regrettable that only the kaolin RCF hasbeen examined at one dose in this species.Other long fibres should also be tested in thisspecies as a means to understand the nature ofthe, so far, unique mesothelioma response.This is a new finding and suggests that ham-sters might be useful in studies of this tumour.Most of the mesothelial lesions were micro-scopic, had no effect on life span, may nothave been malignant, and probably would nothave been detected in other studies with lesssensitive detection protocols. The relevanceand nature of these lesions are being furtherreviewed.The data from the Research and
Consulting Company studies of RCF havebeen used in a model of pulmonary deposi-tion, retention, and clearance.35 3 This modelsuggests that exposures at the maximum toler-ated dose may have been too high and that thelung burdens could have overwhelmed theclearance mechanisms of the lung. Thisoverload condition has been found afterextreme exposures to non-fibrous particulatesand can induce lung tumours that seem tohave no equivalent in exposed humans.38A0Differences in deposition and clearance mayalso explain the differences between rats andhamsters and help in quantitative risk assess-ments of RCF.41A3The histological appearance of the lungs
and the existence of a no effect level in the ratis consistent with the possibility that the lungtumours at the maximum tolerated dose wereproduced by an epigenetic mechanism medi-ated by cytotoxicity followed by a consequentregenerative cell proliferation.283' 34
Despite the precautions used in preparingthe fibres the aerosol used in the Research andConsulting Company studies contained non-fibrous, respirable particulate and this couldhave contributed to any reduction of clearance
436 on 23 M
ay 2018 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.52.7.433 on 1 July 1995. Dow
nloaded from

Health effects of refractory ceramic fibres: scientific issues and policy considerations
or affected the response to fibres by anothermechanism. Davis and coworkers havereported that with asbestos and quartz mix-tures incidence of mesothelioma was higherthan that due to asbestos alone.44 It was sug-gested that exposure to a non-fibrous particu-late can exacerbate the effects of fibres.Clearly the interaction between fibres andnon-fibrous particles in the lungs of exposedanimals requires much more investigation.The Research and Consulting Company
experiments have also provided informationon the durability of RCFs, which had alreadybeen shown to be much less durable thanasbestos both in vivo and in vitro.i46 Suchcomparisons are complicated by other factors;for example Bellman et al reported thatalthough all the man made fibres, includingRCFs, were cleared from the lung the num-bers of chrysotile fibres increased due to lon-gitudinal splitting. These authors alsoreported that ceramic fibres were less solublethan other MMVFs. In the Research andConsulting Company experiments the overallclearance of those ceramic and glass fibreslonger than 5 ym occurred at similar rates. Insupport of the rapid clearance of RCFs pre-liminary evidence indicates that RCFs inhuman lungs are altered in both chemistryand structure.48 Any hazard posed by humanexposure to RCF would be dramaticallyreduced if the fibres are dissolving and beingweakened and then experiencing a comminu-tion by fragmentation although this might notoccur rapidly enough to reduce the hazard torodents.
Extrapolations between results in animalexperiments and human risk are confoundedby the issue of fibre durability. Fibre dissolu-tion is a physical phenomenon, presumablyoccurring at the same speed in man and ani-mals whereas biological responses are likely torelate to lifespan. Thus, even for the sameexposure laboratory animals are more likely toshow adverse responses than humans. In ani-mals fibres can persist at the point of deposi-tion for a period that is a substantial part ofthe life span causing a sustained insult thatcould result in a compensatory hyperplasia.Such fibres might not persist for a largeenough fraction of a human's life, to causethis type of chronic wounding.
At worst the rate at which material may begiven to an animal can be such as to over-whelm the clearance and dissolutionprocesses. Consequently the results of animalexperiments might overestimate the possibil-ity of any effect of exposure to fibres at work-place concentrations in humans. Theseconsiderations are additional to the more gen-eral criticisms of animal carcinogenicity bioas-says that involve extremely high doses.49 50
INVESTIGATIONS ON HUMAN POPULATIONSEXPOSED TO RCFSThese investigations have concentrated onworkers in the manufacturing plants as theyare probably the cohort with the heaviestexposure. Many of the plants involved have
also manufactured hard refractories and mayhave used asbestos and so care must be takenin the attribution of any effect to RCFs alone.
European Ceramic Fibre Insulation Association(ECFA) ceramic fibre morbidity study(1986-1989)This investigation of the health of over 650employees in the manufacture of RCF did notidentify any evidence of lung disease in thosewho had never smoked. Lung function tests ofcurrent and ex-smokers showed effects onsmall airways that were consistent with theirsmoking habit. The possibility of a relationbetween duration of exposure to RCF anddecreased lung function was also raised, butjudged to be of no clinical significance.Symptoms of dry cough and breathlessnesswere also found but could not be attributed toRCF exposure.5' A second European study isto be undertaken in the near future.
Preliminary United States radiographic study(1986)Examination of chest x ray films of 214 cur-rent employees who worked in two RCF man-ufacturing plants showed no effectsattributable to RCF exposure. The findingsfrom the x ray films were reported to be con-sistent with those found in similar surveys ofother factory workers not exposed to fibres.52
American industry studies (1987-present)Lockey and coworkers conducted a longitudi-nal pulmonary morbidity study of UnitedStates workers in the manufacture of RCF orRCF products. This cohort (n = 742) repre-sents 98-5% of the exposed population.Exposure was classified only as either RCFexposed (production workers) or unexposed(non-production workers). In the exposedgroup the only measures of exposure wereduration and time since first employment inproduction. Thirty per cent of the cohort hadbetween 10 and 20 years of exposure and 4%more than 20 years.
There was a decrease of between 2% and3% in forced vital capacity and forced expira-tory volume in one second. These effects werecorrelated with smoking history and with theduration of exposure. These changes were notclinically significant and similar decrementshave been found in manual workers withexposure to other dusty environments.5354
Pleural plaques were identified by at leasttwo of three qualified B reader radiologists inposterioanterior x ray films of 2-4% of theproduction employees. There was no evidenceof interstitial fibrosis and no excess of lungcancer; no mesotheliomas were reported.53 55-58
In a more detailed study of current and for-mer employees at two of the plants, a com-plete medical history was taken and bilateraloblique angle x ray films of the chest were alsotaken. Permission was sought from employeeswho required thoracic surgery and at post-mortem examination for any tissue taken tobe examined for the presence of fibres anddisease.
437
on 23 May 2018 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.52.7.433 on 1 July 1995. D
ownloaded from

Glass, Brown, Hoskins
As in the wider survey, there was anincrease in the prevalence of respiratory symp-toms in current and former production workerscompared with non-production workers.Although the symptoms seemed to correlatewith increased duration of employment inproduction, the prevalence of the symptomswas similar to that found in other people whohave worked in other dusty environments andthus were not specific for exposure to ceramicfibres.
Spirometric findings were again dependenton the smoking habits of the employee. Incontrast with non-smokers, smokers had anadditional job related small reduction in somemeasures of respiratory function. This decre-ment in lung function was associated withduration of employment in a production job,cumulative exposure to RCF, and smokinghistory. Again these effects did not reach clin-ical significance. TiMs population is continu-ing to be monitored to ascertain if the declinein lung function continues and if there is anysensitive subgroup.
Pleural plaques were found in 0-9% of non-production workers (2/214) and productionworkers with less than 10 years of RCF expo-sure (1/117), in 2 8% ofworkers with 10 to 20years exposure (7/248), and in 12-5% ofworkers with more than 20 years of exposure(9/72). These crude incidence figures clearlyrequire correction for age. Minimal or nochanges were found in lung parenchymal tis-sue. Of the 652 workers for whom chest x rayfilms were available three (0A46%) had bor-derline parenchymal changes a prevalencesimilar to that found in other working popula-tions.A case-control study is being carried out in
this group in an attempt to ascertain if theincidence of pleural plaques can be attributedto previous exposure to asbestos. Cases andcontrols have been interviewed with a spe-cially structured questionnaire designed toprovide information on all exposures toasbestos. At present there remains some rela-tion between exposure to RCF and the devel-opment of pleural plaques that must beinvestigated further.The number and causes of deaths in the
cohort was consistent with that in the generalpopulation. In particular no excess risk oflung cancer was found (3 5 expected; 4observed). Again there were no mesothe-liomas.59
These studies are being extended foranother five years.
Relevance of the epidemiological investigationsOver 80% of the workers exposed during themanufacture of RCF in both Europe and theUnited States have been included in thesestudies. These investigations have maximisedthe likelihood of identing any adverse effectalthough the size of the study population isless, and exposures shorter, than that of othercohorts with occupational exposure to dustsor fibres. It would be difficult to increase thesize of the cohort and it presumably repre-sents workers with the greatest exposure to
RCF. The aggregated evidence from all thesestudies does not show an adverse health effectfrom exposure to RCF but does warrantextension of the surveys. To date the mainfinding is the presence of pleural plaques in afew former and current workers. It is generallyheld that pleural plaques are benign and, par-ticularly in the absence of asbestosis, are mostappropriately recognised as indicators ofexposure to asbestos.60
Current exposures to RCFPreliminary estimates indicate that there areno more than 33 000 people in the UnitedStates and 25 000 in Europe who could beexposed to these materials. These occupa-tional exposures can be limited and areamenable to a high level of control, indeedboth engineering controls and improved workpractices are being implemented.6' There arefew consumer applications, and those thereare usually involve fibre that is enclosed orencapsulated so that any potential for expo-sure of the general public is minimal.
In the industry a lack of exposure data,changes in the methods of exposure assess-ment, and poor record retention make itextremely difficult to reconstruct historicalexposures; however, these were certainlyhigher than those of today, which are mostlybelow 1 f/ml.62 63 Thus the concentrations thatproduced lung tumours in the ResearchConsulting Company animal studies wereover 200 times higher than the typical indus-trial human exposures. Further, measurementof the bivariate size distribution of fibres fromselected occupational settings,63 suggests thatthe animals were exposed to a much higherconcentration of the thin long fibres thoughtto be responsible for the production of disease.
Discussion and conclusionsAny estimate of the degree of hazard posed bya substance requires knowledge of that sub-stance, the environment in which exposurecan occur, the exposed population, and theduration and frequency of the exposure. Tounderstand these issues for RCF their manu-facturers have undertaken the design andcompletion of the health studies already dis-cussed as part of a formal product stewardshipprogramme.
Adverse effects can be produced in rodentsexposed to high concentrations of an RCFparticulate aerosol, although the relevance ofthis to human hazard requires further analy-sis. This must take account of the facts thatfibre dissolution occurs in calendar timealthough the production of disease occurs inphysiological time; ceramic fibre is far lessdurable in the lung than chrysotile, the leastdurable asbestos mineral.4647 The naturalminerals can also split longitudinally produc-ing more fibres, although vitreous fibresincluding RCFs do not.
All the biases intrinsic in animal studiesmean that hazard is likely to be overestimatedrather than underestimated and the occur-rence of tumours in animals induced only by
438
on 23 May 2018 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.52.7.433 on 1 July 1995. D
ownloaded from

Health effects of refractory ceramic fibres: scientific issues and policy considerations
very high doses may have little relevance tohumans. It also seems likely that at the highestexposures the animals' lungs were over-loaded-a condition that can result in lungtumours in rodents whatever type of particle isinhaled.38 The mesotheliomas found in ham-sters in the Research and ConsultingCompany study were microscopic and not lifethreatening and their exact histopathology iscurrently being reviewed. Any comparisonwith mesotheliomas in humans and thesesmall compact lesions, especially their use inquantitative risk assessment, requires investi-gation. There is certainly a case for supportingthe common assertion that further work needsto be done.
Epidemiological investigations haveincluded morbidity and mortality studies incohorts from manufacturing establishmentsthat are assumed to represent the most heavilyexposed population. To date there is no evi-dence that exposure to RCF can cause anyrespiratory disease. As no workers have beenexposed over a full working life it may besome time before definitive human studiescan be undertaken.
Despite these uncertainties there are con-tinuing efforts to control exposure to RCFsand so reduce any risk61626465 It is probablethat current exposures are so low and are stillbeing reduced that human disease will notdevelop and so the human relevance of theanimal results will never become clear. It iscertainly true that extrapolation from suchexperiments that used extreme doses of ahighly refined fibre fraction isolated frommore complex bulk materials will never besimple.
Finally, it must be emphasised that theobjective of these studies and control mea-sures is to capture the undoubted benefits ofRCFs to industry and the environment whilecontrolling any risks at all stages of manufac-ture, use, and disposal.
1 International Agency for Research on Cancer. Man-mademineral fibres and radon. IARC Monogr Eval CarcinogRisks Hum 1988;43.
2 Everest Consulting Associates. Cost impacts of a potentialban on refractory ceramic fibre for furnace related applica-tions; technical and economic analysis. Submitted to theUnited States Environmental Protection Agency(USEPA), Washington DC: Refractory Ceramic FibreCoalition (RCFC), 1992.
3 Brown RC, Hoskins JA, Sara EA, Evans CE, Young J,Laskowski JJ, et al. The effects of heating and devitrifica-tion on the structure and biological activity of alumi-nosilicate refractory ceramic fibres. Ann Occup Hyg1992;36:1 15-29.
4 Mossman BT, Bignon J, Corn M, Seaton A, Gee JBL.Asbestos: scientific developments and implications forpublic policy. Science 1990;247:247-301.
5 Vorwald AJ, Durkan TM, Pratt PC. Experimental studies ofasbestosis. American Medical Association Archives ofIndustrial Hygiene and Occupational Medicine 1951;3:1-43.
6 Pott F. Some aspects of the dosimetry of the carcinogenicpotency of asbestos and other fibrous dusts. Staub-Reinholt Luft 1978;38:486-90.
7 Pott F, Roller M, Ziem U, Reiffer F-J, Bellmann B,Rosenbruch M, Huth F. Carcinogenicity studies on nat-ural and man-made fibres with the intraperitoneal test inrats. In: Bignon J, Peto J, Saracci R, eds. Non-occupa-tional exposure to mineral fibres. Lyon: InternationalAgency for Research on Cancer, 1989;173-9. (IARC SciPubl No 90.)
8 Pott F, Roller M, Rippe RM, Germann P-G, Bellman B.Tumours by the intraperitoneal and intrapleural routesand their significance for the classification of mineral
fibres. In: Brown RC, Hoskins JA, Johnson NF, eds.Mechanisms in fibre carcinogenesis. Nato Asi seriesA life sci-ences. Vol 223. New York: Plenum Press, 1991:547-65.
9 Stanton MF, Layard M, Tegeris A, Miller E, Kent E.Carcinogenicity of fibrous glass: pleural response in therat in relation to fibre dimension. J7 Nat Cancer Inst1977;58:587-603.
10 Stanton MF, Layard M, Tegeris A, Miller E, May M,Morgan E, Smith A. Relation of particle dimension tocarcinogenicity in amphibole asbestos and other fibrousmaterials. J Nad Cancer Inst 1981;67:965-75.
11 Stanton MF, Wrench C. Mechanisms of mesotheliomainduction with asbestos and fibrous glass. Y Nat CancerInst 1972;48:797-821.
12 Davis JMG, Addison J, Bolton RE, Donaldson K, JonesAD, Smith T. The pathogenicity of long versus shortfibre samples of amosite asbestos administered to rats byinhalation and intraperitoneal injection. British Journal ofExperimental Pathology 1986;67:415-30.
13 Davis JMG, Jones AD. Comparisons of the pathogenicityof long and short fibres of chrysotile asbestos in rats.British Journal of Experimental Pathology 1988;69:717-37.
14 Wagner JC. Biological effects of short fibres. In:Proceedings of the VIIth International PneumoconiosisConference. Cincinnati: US Department of Health andHuman Services, 1990. (DHSS (NIOSH) Publ No90-108, part II.)
15 Petruska JM, Mossman BT, Brown RC, Hoskins JA.Mechanism of action of mineral fibres as studied by invitro methods. In: Liddell D, Miller K, eds. Mineralfibresand health. Boca Raton: CRC Press, 1991:303-19.
16 Lippman M. Asbestos exposure indices. Environ Res1988;46:86-106.
17 Saracci R. Asbestos and lung cancer: an analysis of the epi-demiological evidence on the asbestos-smoking interac-tion. IntJrCancer 1977;20:323-31.
18 Wagner JC, Berry G, Timbrell V. Mesotheliomas in ratsafter inoculation with asbestos and other materials. BrJCancer 1973;28:173-85.
19 Smith DM, Ortiz LW, Archuleta RF, Johnson NF. Long-term health effects in hamsters and rats exposed chroni-cally to man-made vitreous fibers. Ann Occup Hyg1987;32:731-54.
20 World Health Organisation. Validity of methods for assessingthe carcinogenicity of man-made fibres. Lyon: executivesummary of a WHO consultation, 1992.
21 Hesterberg TW, Vu V, Chase GR. Use of animal modelsto study man-made fibre carcinogenesis. In: Brinkly B,Lechner J, Harris C, eds. Cellular and molecular aspects offibre carcinogenesis. Cold Spring Harbor, NY: ColdSpring Harbor Laboratory, 1991:183-205.
22 McClellan RO, Miller FJ, Hesterberg TW, Warheit DB,Bunn WB, Kane A, et al. Approaches to evaluating thetoxicity and carcinogenicity of man-made fibres: sum-mary of a workshop held November 11-13, 1991,Durham, North Carolina. Reg Toxicol Pharmacol 1991;16:321-64.
23 Gross P, De Treville RTP, Tolker EB, Kaschak M,Babyak MA. Experimental asbestosis: the developmentof lung cancer in rats with pulmonary deposits ofchrysotile asbestos dust. Arch Environ Health 1967;15:343-55.
24 Gross P, Westrick ML, Shrenk HH, McNerney JM. Theeffect of synthetic ceramic fibre dust upon the lungs ofrats. American Medical Association Archives of IndustrialHealth 1956;13:161-6.
25 Davis JMG, Addison J, Bolton RE, Donaldson K, JonesAD, Wright A. The pathogenic effects of fibrous ceramicmaterial aluminium silicate glass administered to rats byinhalation and peritoneal injection. In: Biological effects ofman-made mineral fibres. Proceedings of a WHOIARCConference, Copenhagen, April 20 to 22, 1982. Vol 2.Geneva: WHO/IARC 1984,303-11.
26 Bernstein DM, Drew R, Kuschner M. Experimentalapproaches for exposure to sized glass fibers. EnvironHealth Perspect 1980;34:47-57.
27 Glass LR, Mast RW, Chevalier J, Hesterberg TH,Anderson R, McConnell EE, Bernstein DM. Sub acute(28 day) nose only inhalation study of size selectedrefractory ceramic fibre (RCF) in male fischer 344 rats.The Toxicologist 1993;13:34.
28 McConnell EE, Mast RW, Hesterberg TW, Chevalier J,Kotin P, Bernstein DM, et al. Chronic inhalation toxicityof a kaolin based refractory ceramic fibre (RCF) in syr-ian golden hamsters. Inhalation Toxicology 1995 (inpress).
29 Bunn WB, Bender JR, Hesterberg TW, Chase GR,Konzen JL. Recent studies of man-made vitreous fibres,chronic animal inhalation studies. J Occup Med 1993;35:101-13.
30 Mast RW, McConnell EE, Glass LR, Hesterberg TW,Anderson R, Bernstein DM. Inhalation oncogenicity ofkaolin refractory ceramic fibre (RCF) in hamsters-finalresults. The Toxicologist 1992;12:377.
31 Mast RW, McConnell EE, Anderson R, Chevalier J, KotinP, Berstein DM, et al. Studies of the chronic toxicity(inhalation) of four types of refractory ceramic fibre inmale fischer 344 rats. Inhalation Toxicology 1995 (inpress).
32 Glass LR, Mast RW, Hesterberg TH, Anderson R,McConnell EE, Bernstein DM. Inhalation oncogenicityof refractory ceramic fibre (RCF) in rats-final results.The Toxicologist 1992;12:377.
439
on 23 May 2018 by guest. P
rotected by copyright.http://oem
.bmj.com
/O
ccup Environ M
ed: first published as 10.1136/oem.52.7.433 on 1 July 1995. D
ownloaded from

Glass, Brown, Hoskins
33 Mast RW, McConnell EE, Glass LR, Hesterberg TW,Thevenaz P, Chevalier J, Anderson R. A multiple dosechronic inhalation toxicity study of kaolin refractoryceramic fibre (RCF) in male Fischer 344 rats. TheToxicologist 1993;13:43.
34 Mast RW, McConnell EE, Hesterberg TW, Chevalier J,Kotin P, Thevenaz P, et al. A multiple dose chronicinhalation toxicity of size selected kaolin refractoryceramic fibre (RCF) in male fischer 344 rats. InhalationToxicology 1995 (in press).
35 Yu CP, Asgharian B, Abraham JL. Mathematical model-ling of alveolar clearance of chrysotile asbestos fibersfrom the rat lungs. Journal of Aerosol Science 1990;21:587-94.
36 Yu CP, Asgharian B. A kinetic model of alveolar clearanceof amosite asbestos fibers from the rat lung at high lungburdens. Journal ofAerosol Science 1990;21:21-7.
37 Yu CP, Asgharian B, Pinkerton KE. Intrapulmonarydeposition and retention modelling of chrysotile fibers inrats. Yournal ofAerosol Science 1991;22:757-63.
38 Hext PM. Current perspectives on particulate inducedpulmonary tumours. Hum Exp Toxicol 1994;13:700-14.
39 Morrow PE. Dust overloading of the lungs: update andappraisal. ToxicolAppl Pharnacol 1992;113:1-12.
40 Lewis TR, Morrow PE, McClellan RO, Raabe OG,Kennedy GR, Schwartz BA, et al. Establishing aerosolexposure concentrations for inhalation toxicity studies.ToxicolAppl Pharmacol 1989;99:377-89.
41 Yu CP, Zhang L, Oberdoerster G, Mast RW, Glass LR,Utell MJ. Deposition modelling of refractory ceramicfibres in the rat lung. journal ofAerosol Science 1995 (inpress).
42 Yu CP, Zhang L, Oberdoerster G, Mast RW, Glass LR,Utell MJ. Clearance of refractory ceramic fibres (RCF)from the rat lung: development of a model. Environ Res1995 (in press).
43 Yu CP, Ding J, Zhang L, Oberdoerster G, Mast RW,Glass LR, Utell MJ. Deposition and clearance modellingof inhaled kaolin refractory ceramic fibres (RCF) inhamsters-comparison with rat results. Journal ofAerospace Science 1995 (in press).
44 Davis JMG, Jones AD, Miller BG. Experimental studies inrats on the effects of asbestos inhalation coupled with theinhalation of titanium dioxide or quartz. IntJ Exp Pathol1991;72:501-25.
45 Scholze H, Conradt R. An in vitro study of the chemicaldurability of siliceous fibres. Ann Occup Hyg 1987;31:683-92.
46 Hammad Y, Simmons W, Abdel-Kader C, Reynolds C,Wiell H. Effect of chemical composition on pulmonaryclearance of man-made mineral fibres. Ann Occup Hyg1988;32:769-79.
47 Bellman B, Muhle H, Pott F, Konig H, Kloppel H,Spurny K. Persistance of man-made mineral fibres(MMMF) and asbestos in rat lungs. Ann Occup Hyg1987;31:693-709.
48 Sebastien P, Vergnon JM, Blanchard 0, Wastiaux A,Emonot KL. Durability of ceramic fibres in the humanlung: preliminary results. Presented At The 23rdInternational Congress on Occupational Health, September1990. Stockholm: 1990.
49 Ames B, Gold LS. Too many rodent carcinogens: mitoge-nesis increases mutagenesis. Science 1990;249:970.
50 Cohen SM, Ellwein LB. Cell proliferation in carcinogenesis.Science 1990;249:1007-1 1.
51 Trethowan WN, Burge PS, Harrington JM, Calvert I,Rossiter C. Study of the respiratory health of employeesin seven European plants that manufacture ceramicfibres. Occup Environ Med 1995;52:97-104.
52 Horvath EP. Report to Standard Oil. Chest x ray resultsfrom current New Carlisle and Niagara Falls areaemployees. 1986.
53 Lockey J, Lemasters G, Rice C. An industry wide pulmonarymorbidity study of workers manufacturing refractory ceramicfibres and RCF products. Presented at the 23rd InternationalCongress on Occupational Health, September, 1990.Stockholm: 1990.
54 Lockey J, Lemasters G, Rice C, McKay RT, Gartside PS. Across sectional analysis of respiratory health among cur-rent refractory ceramic fibre employees. Submitted tothe Thermal Insulation Manufacturers Association(TIMA).Washington, DC: 1991.
55 Lemasters G, Lockey J, Rice C, et al. Radiographicchanges among workers manufacturing refractoryceramic fibre and products. Ann Occup Hyg1994;18(suppl 1):745-5 1.56 Lockey J. Issues associated with occupational exposure to
refractory ceramic fibres. Presented to the spring meeting ofthe American College of Occupational and EnvironmentalMedicine, May, 1992. Cincinnati: 1992.
57 Lockey J, Lemasters G, Rice C. An industry wide pulmonarymorbidity study ofcurrent andformer workers manufacturingrefractory ceramic fibres and products. Presented at theBOHS 7th International Symposium on Inhaled Particles,Edinburgh, September, 1991.
58 Lockey L, Lemasters G, Rice C. Pleuralplaques-a marker ofexposure to refractory ceramicfibres. Presented at the Society ofEpidemiologic Research, July, 1992. Cincinnati: 1992.
59 LockeyJ, Lemasters G, Rice C, McKay RT, Gartside PS. Aretrospective morbidity, mortality and nested case-controlstudy of the respiratory health of individuals manufacturingrefractory ceramic fiber and RCF products. Submitted to theRefractory Ceramic Fiber Coalition (RCFC), 1993.Washington, DC: 1993.
60 Weiss W. Asbestosis related pleural plaques and lung can-cer. Chest 1993;103:1854-9.61 Barrows GL, Chen SH, Shemanski L. The refractoryceramic fibre coalition's product stewardship program.American Ceramic Society Bulletin 1993;72:28-34.62 Everest Consulting Associates. Report to the OccupationalSafety and Health Administration (OSHA). An analysis ofthe economic feasibility of a 1 flml permissible exposure limit(PEL) for the refractory ceramicfibre industry. Washington,DC: Sponsored by the Refractory Ceramic FibreCoalition (RCFC), 1992.
63 Hori H, Toshiaki H, Fujino A, Yamato H, Ishimatsu S,Oyabu T, Tanaka I. Measurement of airborne ceramicfibres in manufacturing and processing factories. AnnOccup Hyg 1993;37:623-9.
64 Everest Consulting Associates. Waste generation and man-agement in the manufacture, processing and use of refractoryceramicfiber (RCF). Washington, DC: Sponsored by theRefractory Ceramic Fibre Coalition (RCFC), 1994.
65 Breitsman WJ, Maxim LD, Allshouse J, Crankshaw 0,Wrenn C. Refractory ceramic fibre emissions from domesticproduction facilities and related matters: phase Ifinal report.Prepared on behalf of TIMA, Inc for the Office of ToxicSubstances (OTS), Office of Pesticides and ToxicSubstances, US Environmental Protection Agency (EPA).Washington, DC:1992.
440 on 23 M
ay 2018 by guest. Protected by copyright.
http://oem.bm
j.com/
Occup E
nviron Med: first published as 10.1136/oem
.52.7.433 on 1 July 1995. Dow
nloaded from