health effects attributed to mold
TRANSCRIPT

Heath EffectsAttributed To Mold
Harriet A. Burge, Ph.D.
Will begin at 9:00 a.m. (PST). Participants will be in listen only mode.
Download the PDF of this presentation (case sensitive): http://www.emlab.com/m/media/mold-health-effects-webinar.pdf
Continuing Education Units (CEUs)
To receive a certificate of attendance, you mustcomplete the survey after thewebinar:
•Click on the survey link in the “Thank you” email (sent 1 hour after this webinar).
•Complete survey by this Friday, January 22, 2016.
•You will receive an email in 2-3 weeks with instructions when your certificate is ready.
Copyright © 2016 EMLab P&K. All rights reserved.2

Outline
1. The immune system and how it relates to fungal disease
2. Infection3. Hypersensitivity
a. Allergiesb. Hypersensitivity pneumonitis
4. Toxicity
Copyright © 2016 EMLab P&K. All rights reserved.3

Immune System
Evolved to prevent infection
Plays a fundamental role in hypersensitivity
diseases Is damaged by some toxins
Copyright © 2016 EMLab P&K. All rights reserved.4

Immune System (cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.5
• Development of all cells of the immune system begins in the bone marrow with a blood-forming stem cell
• Two broad categories of immune responses: the innate immune system and the adaptive immune system
• Central to both categories: the ability to distinguish our own tissues (that need protection) from foreign invaders (that need to be attacked)

Innate Immune Responses
Copyright © 2016 EMLab P&K. All rights reserved.6
• Rely on cells that require no additional “training” to do their jobs. These cells include neutrophils, monocytes, natural killer (NK) cells and a set of proteins termed the complement proteins.
• Innate responses to infection occur rapidly and reliably. Even infants have excellent innate immune responses.

Adaptive Immune Responses
Copyright © 2016 EMLab P&K. All rights reserved.7
• Involve T-cells and B-cells, two cell types that require “training” or education to learn not to attack our own cells.
• The advantages of the adaptive responses are their long-lived memory and the ability to adapt to new germs.

Cells of the Immune System
• A. Bone marrow: most of the cells of the immune system are produced here as immature or stem cells.
• B. Stem cells: have the potential to differentiate and mature into the different cells of the immune system.
• C. Thymus: An organ located in the chest that instructs immature lymphocytes (white blood cells) to become mature T- lymphocytes.
Copyright © 2016 EMLab P&K. All rights reserved.8

Cells of the Immune System (cont’d)
• D. B-Cells: These lymphocytes differentiate into plasma cells that produce immunoglobulins (antibodies).
• E. Cytotoxic T-cells: lymphocytes that mature in the thymus and are responsible for killing infected cells.
• F. Helper T-cells: lymphocytes that “help” other T-cells and B-cells to perform their functions.
Copyright © 2016 EMLab P&K. All rights reserved.9

Cells of the Immune System (cont’d)
• I. Neutrophils (Polymorphonuclear PMN Cell): rapidly ingest microorganisms and kills them.
• J. Monocytes: develop into macrophages when they migrate to tissues.
Copyright © 2016 EMLab P&K. All rights reserved.10

Immunoglobulins (Antibodies)
Copyright © 2016 EMLab P&K. All rights reserved.11
• Proteins that bind specifically to a particular substance—an antigen.
• All antibodies have the same overall structure
• Each antibody molecule has a unique structure that enables it to bind specifically to its corresponding antigen.
• Antibodies are produced by plasma cells in response to infection, immunization, or allergen exposure.

Antibodies
The two arms of the Y- shaped antibody molecule contain the variable regions that form the two identical antigen-binding sites.
The stem or constant region engages the effector mechanisms that antibodies activate to eliminate pathogens or release symptom-causing chemicals.
Copyright © 2016 EMLab P&K. All rights reserved.12

Copyright © 2016 EMLab P&K. All rights reserved.13

Infection – Colonization
Copyright © 2016 EMLab P&K. All rights reserved.14
• An infection occurs when a microbe enters the body and begins to reproduce.The microbe must:– Survive and multiply under local conditions (e.g. of
temperature and pH) to establish itself in its new habitat
– Successfully compete against the established indigenous microbial flora
– Resist local defense mechanisms
• Once established on a body surface, an organism is said to have colonized that site.

Infection
• The invading microbe may– Remain dormant
– Directly damage cells, or
– Immune system can cause symptoms such as fever, as it tries to rid your body of the invader.
Copyright © 2016 EMLab P&K. All rights reserved.15
Infection – Host Response
Copyright © 2016 EMLab P&K. All rights reserved.16
• Usually begins with an inflammatory reaction, followed by a humoral or cell-mediated immune response.
• Damage occurs due to swelling, increased fragility of tissues, formation of pus, scarring or necrosis.
• Chronic intracellular infection may cause formation of fibrous nodules and a state of latency from which acute infection can be re-established at a much later stage.
Classification of Mycoses
• The clinical nomenclatures used for the mycosesare based on the– (1) Site of the infection,
– (2) Route of acquisition of the pathogen, and
– (3) Type of virulence exhibited by the fungus.
Copyright © 2016 EMLab P&K. All rights reserved.17

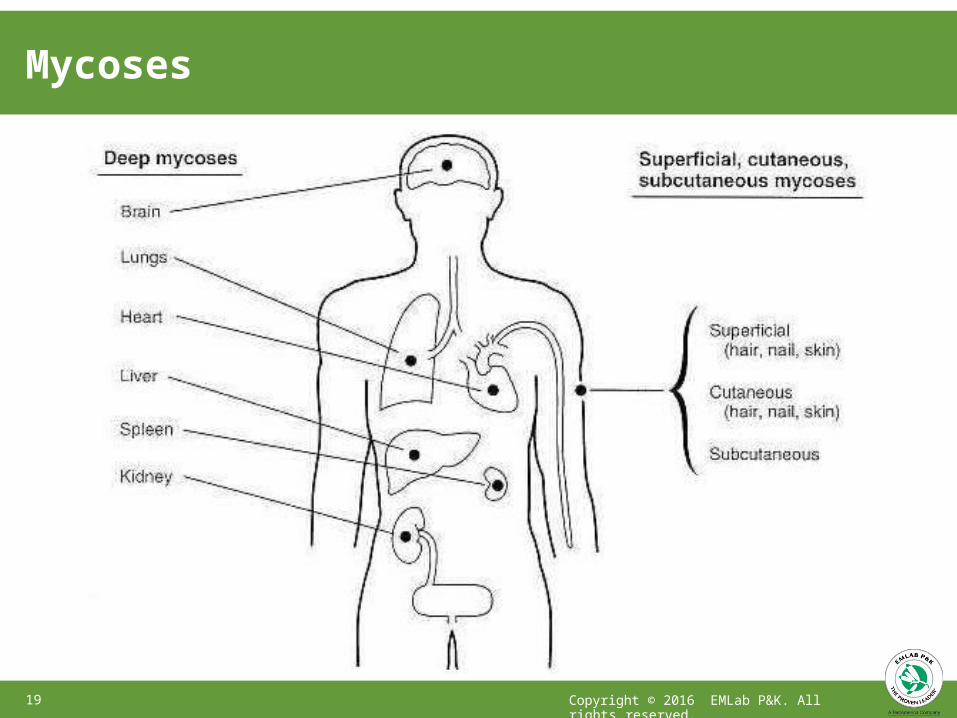
Classification Based on Site of Infection
• Superficial,• Cutaneous,• Subcutaneous,• Systemic (deep) infections
depending on the type and degree of tissue involvement and the host response to the pathogen.
Copyright © 2016 EMLab P&K. All rights reserved.18
Mycoses
Copyright © 2016 EMLab P&K. All rights reserved.19

Classification Based on Route ofAcquisition
• Exogenous or endogenous routes of entry– Airborne, cutaneous or percutaneous.
– Endogenous infection involves colonization by a member of the normal flora or reactivation of a previous infection.
Copyright © 2016 EMLab P&K. All rights reserved.20

Classification Based on Virulence
Copyright © 2016 EMLab P&K. All rights reserved.21
• Primary pathogens can establish infections in normal hosts.
• Opportunistic pathogens cause disease in individuals with compromised host defense mechanisms.
• The primary pathogens have relatively well-defined geographic ranges; the opportunistic fungi are ubiquitous.

Fungal Infections
• All require living spores for disease
• Virulent agents do not grow indoors and disease depends on disturbance of outdoor reservoirs
• Skin agents are probably not airborne
• Opportunistic agents common in the environment
Copyright © 2016 EMLab P&K. All rights reserved.22

Primary (Virulent) Mycoses
• Able to cause infection in a normal host– Coccidioides immitis– Histoplasma capsulatum– Blastomyces dermatitidis– Paracoccidioides brasiliensis (South America)
Copyright © 2016 EMLab P&K. All rights reserved.23

Virulent Infections
Copyright © 2016 EMLab P&K. All rights reserved.24
• Histoplasmosis (Histoplasma capsulatum)– Wet soil enriched with bird droppings
– Soil disturbance necessary for dissemination
– Endemic in the Mississippi valley
• Blastomycosis (Blastomyces dermatididis)– Similar to Histoplasma
• Coccidioidomycosis (Coccidioides immitis)– Dry desert soils
– Sandstorms

Virulent Fungal Infection
Copyright © 2016 EMLab P&K. All rights reserved.25
• Traveling to an area where the causative fungus is common raises the risk for this infection.
• Serious infections occur in those with a weakened immune system due to:
– Anti-tumor necrosis factor (TNF) therapy– Cancer– Chemotherapy– Glucocorticoid medications (prednisone)– Heart-lung conditions– HIV– Organ transplant– Pregnancy (especially the first trimester)

Histoplasma capsulatum
Copyright © 2016 EMLab P&K. All rights reserved.26
• Etiologic agent of the most common respiratory fungal infection affecting humans.
• Lives in the soil, usually in association with large amounts of bird or bat droppings.
• Widely distributed throughout the subtropial and tropical zones of the world. In North America, H. capsulatum is particularly associated with the Mississippi and Ohio River valleys.

Histoplasma capsulatum (cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.27
• Exists in soil in a mycelial form• Tuberculate macroconidia (8 to 14µm in diameter)
and microconidia (2-5 µm in diameter) are formed in the soil
• Microconidia are likely the major source of infection due to their small size, making them readily airborne with soil disturbance, and able to penetrate to the small airways of mammalian lungs by inhalation.
Histoplasma capsulatum (cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.28
• In the body, H. capsulatum converts to a yeast form.• Lung infection can occur after inhalation of airborne,
microscopic fungal spores when soil is disturbed.• Many people who inhale the spores do not get sick.• Symptoms of histoplasmosis are similar to
pneumonia, and the infection can sometimes become serious if it is not treated.
Histoplasmosis
Copyright © 2016 EMLab P&K. All rights reserved.29
• Between 50% and 80% of people who live in areas where Histoplasma capsulatum is common in the environment will show evidence of having been exposed to the fungus at some point in their lifetime. In these areas, 10% to 25% of HIV-infected people will develop disseminated histoplasmosis.
• There is a PCR assay for detection of H. capsulatum in soil. Previously, soil suspensions had to be inoculated into mice and (after 6 weeks or so) the liver and spleen cultured.

Blastomyces dermatitidis (Blastomycosis)
Copyright © 2016 EMLab P&K. All rights reserved.30

Blastomyces dermatitidis (cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.31
• Although long thought to be restricted to the North American continent, cases have been diagnosed in Africa, Asia and Europe in recent years.
• Clinical and epidemiological evidence indicates that humans and lower animals contract blastomycosis from some source in nature.
• However, the natural habitat of B. dermatitidis has yet to be clearly delineated, despite some reports of its isolation from soil.

Blastomycosis
Copyright © 2016 EMLab P&K. All rights reserved.32
• A true systemic (endemic) mycosis.• Occurs mainly in immunocompetent hosts• Acquired by inhalation and usually remains a
lung infection.• Cutaneous infection occurs with direct inoculation
of the fungus into the skin.• Dissemination to other organs and systems
may occur, especially in immunocompromised hosts.

Coccidioides immitis (Valley Fever)
• This fungus resides in soil• Spores become airborne with disturbance (e.g., wind)
Copyright © 2016 EMLab P&K. All rights reserved.33

• Coccidioides is thought to grow best in soil after heavy rainfall and then disperse into the air most effectively during hot, dry conditions.
• Climate change may be affecting the number of Valley fever infections, as well as the geographic range of Coccidioides.
Coccidioides immitis (Valley Fever) cont’d
Copyright © 2016 EMLab P&K. All rights reserved.34

Coccidioides immitis (Valley Fever) cont’d
Copyright © 2016 EMLab P&K. All rights reserved.35
• Symptoms are flu-like, nonspecific and often difficult to diagnose.
• Most people who breathe in the spores don’t get sick. Usually, people who get sick will get better on their own within weeks to months, but some people will need antifungal medication.
• Immunocompromised people are at higher risk for severe illness.
• Responsible for laboratory related infections where the agent is handled.

Opportunistic Infections
Copyright © 2016 EMLab P&K. All rights reserved.36
• Are a serious issue for the immune compromised:– AIDS
– Organ transplants
– Chemotherapy
– Bone marrow transplants
• Not normally an issue for people with competent immune systems

Opportunistic Mycoses
• Candida albicans• Aspergillus• Zygomycetes (Rhizopus, Rhizomucor,
Absidia, Mucor sp.• Cryptococcus neoformans and C. gattii
Copyright © 2016 EMLab P&K. All rights reserved.37

Candida albicans
Copyright © 2016 EMLab P&K. All rights reserved.38
• Candida is a resident organism in the human body.• Infections are of endogenous origin (not
environmental)• Illnesses:
– Thrush (mouth or throat)
– Yeast infection (genital area)
– Diaper rash (baby’s bottom)
– Invasive candidaisis (bloodstream)

Candida albicans (cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.39
• Thrush– Infants and the elderly
– Chemotherapy patients
– Patients with immunosuppressive disease
• Diaper rash– Not always caused by Candida– Can occur in any baby if bottom remains wet

Candidiasis or Candidemia
Copyright © 2016 EMLab P&K. All rights reserved.40
• You are more likely to get this invasive type of infection if you:– Are in the hospital's intensive care unit (ICU)
– Have had recent surgery
– Have a central line (catheter)
– Have a weakened immune system

Candida Infection on The Internet
Copyright © 2016 EMLab P&K. All rights reserved.41
• Some people with unexplained symptoms and having a little information about Candida believe that systemic candida infection has caused many different symptoms both physical and psychological.
• Unfortunately, a few physicians have supported thisopinion.
• The key term is “believe.” There is no evidence for such associations.

Aspergillus Infection
• All animals and many plants have highly efficient mechanisms to prevent themselves being infected by Aspergillus, and it is usually only when those mechanisms are defective in some way that Aspergillus can grow within the body.
• Thus, this is a true opportunisticinfection
Copyright © 2016 EMLab P&K. All rights reserved.42
Invasive Aspergillosis
Copyright © 2016 EMLab P&K. All rights reserved.43
• Invasive aspergillosis (true Aspergillus infection) is an important medical concern in immunocompromised patients
• It is an airborne disease• The number of living spores required to initiate an
infection is unknown, and probably varies with the individual’s immune status.
• Millions of spores can be inhaled with no infection occurring in normal people.

Aspergillus Infection (cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.44
• Inhaled conidia germinate into invading hyphae that penetrate the respiratory epithelium.
• Aspergillus traits, including the production of pigment, antioxidants, proteases, adhesins, siderophores, and mycotoxins, are implicated as potential virulence factors.
• These factors interact in the patient with depressed immunity to allow infection to occur.

Aspergillosis In General
Copyright © 2016 EMLab P&K. All rights reserved.45
• Invasive aspergillosis– Invasive infection
• Aspergilloma– colonization of “holes” in the lung parenchyma forming
Aspergillus balls
• Allergic bronchopulmonary aspergillosis– Colonization of the mucous lining the lungs of asthmatics.
• Only invasive aspergillosis can be accurately calledan infection.

Zygomycetes
Copyright © 2016 EMLab P&K. All rights reserved.46
• Orders Mucorales and Entomophthorales include human pathogens
• Entomophthorales infection is very rare• Members of the Mucorales that cause
human disease:– Rhizopus (most common)
– Mucor, Rhizomucor, Absidia, Apophysomyces, Saksenaea, Cunninghamella, Cokeromyces, and Syncephalastrum have also been causal agents.

Zygomycosis
Copyright © 2016 EMLab P&K. All rights reserved.47
• The spores are transmitted by– inhalation,
– a variety of percutaneous routes,
– ingestion of spores.
• Opportunistic: Host risk factors include– Diabetes mellitus, neutropenia, sustained
immunosuppressive therapy, chronic prednisone use, iron chelation therapy, broad-spectrum antibiotic use, severe malnutrition, and primary breakdown in the integrity of the cutaneous barrier such as trauma, surgical wounds, needle sticks, or burns.

Cryptococcus neoformans
Copyright © 2016 EMLab P&K. All rights reserved.48
• C. neoformans v. grubii and v. neoformans have a worldwide distribution and are often found in soil that has been contaminated by bird excrement.
• C. neoformans has been recovered from the ruins of Chernobyl and may be able to use radiation as an energy source.
• Cryptococcus is a basidiomycete belonging to the order Tremelliales (jelly fungi). Basidiospores are formed during a brief mycelial stage, and are aerosolized, leading to possible inhalation exposure.

Cryptococcum neoformans
Copyright © 2016 EMLab P&K. All rights reserved.49
• C. neoformans is an opportunistic fungus.Normal healthy people are rarely infected.
• Infections are usually pulmonary, although with severe immunosuppression such as in AIDS patients, meningioencephalitis can occur.
• Pulmonary cryptococcosis can be treated withantifungal drugs.
• Central nervous system infections are very difficult to treat and are often fatal.
Cryptococcus gattii
Copyright © 2016 EMLab P&K. All rights reserved.50
• Cryptococcus gattii, formerly known as Cryptococcus neoformans var gattii, is a tropical species, only recently reported in northeastern North America.
• According to the CDC, from 2004 to 2010, 60 cases were identified in the U.S.: 43 in Oregon, 15 from Washington, and one each from Idaho and California.
• About 52% of these were in immunocompromisedpatients.

Skin Infections
• Microsporum, Epidermophyton, and Trichophyton– Athlete’s foot
– Ringworm
– Jock itch
Copyright © 2016 EMLab P&K. All rights reserved.51

Infection – Cutaneous
Copyright © 2016 EMLab P&K. All rights reserved.52
• Microsporum, Epidermophyton, and Trichophyton• Dermatophytes cause infections of the skin, hair
and nails, obtaining nutrients from keratinized material.
• Dermatophytes generally do not penetrate into living tissue, but remain in the keratinized layer of the skin
• Common name for these infections includeringworm, jock itch, athlete’s foot, and others
• Transmission is through direct contact with infectedpeople and shed fungal materials.

Copyright © 2016 EMLab P&K. All rights reserved.53
Hypersensitivity
Copyright © 2016 EMLab P&K. All rights reserved.54
• Immune responses to innocuous antigens that lead to symptomatic reactions upon re-exposure– Hypersensitivity: The state of heightened reactivity
to antigen.
– Hypersensitivity reactions are classified by mechanism:
• Type I reactions involve IgE antibody triggering of mast cells;
• Type II reactions involve IgG antibodies against cell surface or matrix antigens;
• Type III reactions involve antigen:antibody complexes;
• Type IV reactions are T cell-mediated.

Type I Hypersensitivity – Allergy
Copyright © 2016 EMLab P&K. All rights reserved.55

Mast Cells
Copyright © 2016 EMLab P&K. All rights reserved.56
• Large cells found in connective tissues throughout the body, most abundantly in the submucosal tissues and the dermis.
• Contain large granules that store mediator molecules including histamine.
• Have high-affinity Fcε receptors (FcεRI) that allowthem to bind IgE monomers.
• Antigen-binding to this IgE triggers mast-cell degranulation and mast-cell activation,
• Producing a local or systemic immediate hypersensitivity reaction.

Ports of Antigen (Allergen) Entry
• Intravenous:– General release of histamine
• Intradermal– Local release of histamine
• Inhalation, upper airway– Local release of histamine
• Inhalation, lower airway– Local release of histamine
• Gastrointestinal– Local release of histamine– Diffusion into blood stream
Anaphylaxis
Wheal and flare
Allergic rhinitis
Asthma
Diarrhea, vomiting Urticaria, anaphylaxis
Copyright © 2016 EMLab P&K. All rights reserved.57

Type I Hypersensitivity – Allergic Diseases
• Diseases– Allergic rhinitis (hay fever)
– Asthma
– Anaphylaxis
– Eczema (atopic dermatitis)
– Allergic bronchopulmonary aspergillosis
Copyright © 2016 EMLab P&K. All rights reserved.58

Exposure To Fungal Allergens
Copyright © 2016 EMLab P&K. All rights reserved.59
• Exposure to fungal allergens is high, and sensitization is common (at least 10% of the population)
• As with most allergens, low doses over a long period of time are likely needed for sensitization.Higher doses for symptoms.
• Fungal sensitivity predisposes the patient to severe asthma.

Outdoor Aerosol
Copyright © 2016 EMLab P&K. All rights reserved.60
Most fungal allergen exposure occurs outdoors
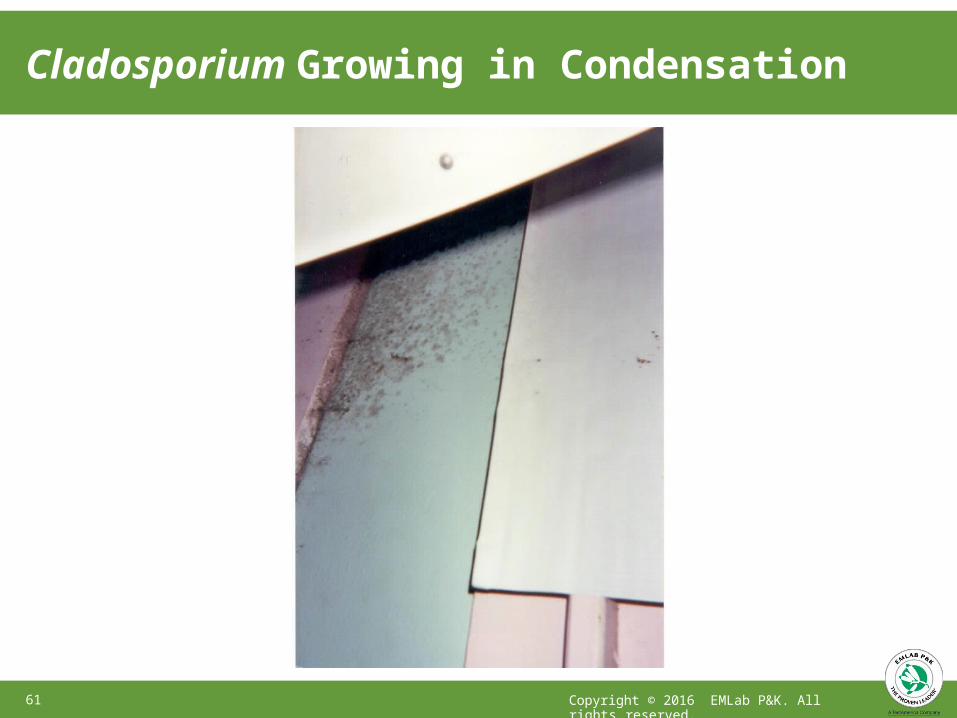
Cladosporium Growing in Condensation
Copyright © 2016 EMLab P&K. All rights reserved.61

Fungal Colonization
Copyright © 2016 EMLab P&K. All rights reserved.62
• Diseases– Allergic bronchopulmonary aspergillosis (mycosis)– Allergic Fungal Sinusitis
• Background– ABPA: fungus colonizes mucous in the lung; Symptoms
caused by immune response to the fungus– AFS: Fungus colonizes mucous in sinuses; Sinuses fill with
fungal hyphae and thick mucous produced in response to the fungal allergens
– Risk depends on having chronic asthma or rhinitis– Only a few fungi are involved

Evidence for Allergic Reactions
Copyright © 2016 EMLab P&K. All rights reserved.63
• Asthma:– There is extensive evidence to
document that exposure to fungi can precipitate asthma attacks, and may be involved in the initial development of asthma in some circumstances.
• Childhood asthma studies
• Work related asthma studies

Interesting Point
• Asthma attack related to fungi on mouth guard (Glass et al., 2007)– If mouth guard is used only at
school, the school environment could be blamed
– If mold is found in a building, the tendency is to blame the mold for symptoms
– Important to consider other possibilities, especially if only one person is affected.
Copyright © 2016 EMLab P&K. All rights reserved.64

Type III and IV Hypersensitivity
Copyright © 2016 EMLab P&K. All rights reserved.65
• Hypersensitivity pneumonitis (also called allergic alveolitis) is caused by a combination of type III and IV hypersensitivity responses
• Exposure to antigen leads to production of specific IgG molecules. These are called precipitating antibodies.
• Re-exposure to antigen leads to formation of antigen/antibody complexes that deposit in the alveoli (small sacs in the lung.
• This is the Type III response

Hypersensitivity Pneumonitis
Copyright © 2016 EMLab P&K. All rights reserved.66
In addition:• Early response to the antigen leads to an increase
in neutrophils and mononuclear cells in the alveoli and small airways.
• These cells release proteolytic enzymes, prostaglandins, and leukotrienes. The production and release of interleukins, cytokines, growth factors, and various other mediators from T lymphocytes and macrophages play important roles in hypersensitivity pneumonitis pathogenesis.
Pathophysiology
Copyright © 2016 EMLab P&K. All rights reserved.67
• The subacute, or intermittent, form:– Produces well-formed granulomas, bronchiolitis with or
without pneumonia, and interstitial fibrosis
– This type (stage) can often be reversed by eliminating exposure
• Chronic forms:– Display chronic interstitial inflammation and alveolar
destruction (honeycombing)
– There is no good treatment for this form, and continuingexposure can lead to death
Acute Symptoms
• Fever• Chills• Fatigue• Breathlessness• Chest tightness• Cough
Copyright © 2016 EMLab P&K. All rights reserved.68

Exposures Leading To HypersensitivityPneumonitis
Copyright © 2016 EMLab P&K. All rights reserved.69
• Acute HP– Intense exposure to small particle organic dusts including
small fungal spores.
• Chronic HP– Low level exposure to small particle antigens over a long
period.

Antigens Leading To HP
Copyright © 2016 EMLab P&K. All rights reserved.70
• Compost HP• Malt worker lung• Peat moss HP
AspergillusAspergillus clavatusMonocillium sp,
CompostMoldy barley
Penicillium citreonigrum Peat moss• Suberosis Penicillum frequentans Moldy cork dust
• Maple bark HP Cryptostroma corticale Moldy wood bark
• Wood pulp worker lung Alternaria species Moldy wood pulp
• Wood trimmer lung Rhizopus species Moldy wood trimmings
• Tree cutter lung Penicillium (3 species)Paecilomyces sp. Aspergillus niger Rhizopus sp.Aspergillus sp.
Wood chips from living maple and oak tree
• Dry rot HP Merulius lacrymans Moldy rotten wood
• Sequoiosis Graphium species, Moldy wood dust

Antigens Leading To HP (Cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.71
• Japanese summer-type HP
• Cheese washer lung
Trichosporon cutaneum
Pencillum casei
Damp wood and mats
Cheese casingsP.roqueforti
• Tobacco worker lung Aspergillus sp. Moldy tobacco
• Greenhouse HP Aspergillus sp. Penicillium sp. Cryptostroma corticale
Moldy soil
• Esparto grass HP Aspergillus fumigatus Moldy esparto(used to produce ropes, canvas, sandals, mats, baskets, and paper paste)• Soy sauce brewer lung Aspergillus
oryzaeFermentation starter for soy sauce

Copyright © 2016 EMLab P&K. All rights reserved.72
Toxic Fungal Metabolites
Copyright © 2016 EMLab P&K. All rights reserved.73
• Toxic mainly to bacteria: Antibiotics• Toxic mainly to plants: Phytotoxins• Toxic to the animal kingdom and produced by
macrofungi (mushrooms): Mushroom toxins
• Toxic to the animal kingdom and produced by microfungi: Mycotoxins

Toxicosis Classification of Mycotoxins
Copyright © 2016 EMLab P&K. All rights reserved.74
• Classification schemes tend to reflect the training of the person doing the categorizing.– Clinicians: classification by organ affected
• hepatotoxins, nephrotoxins, neurotoxins, immunotoxins, etc
– Cell biologists: mechanism of action• teratogens, mutagens, carcinogens, and allergens
– Organic chemists: chemical structure• lactones, coumarins
– Et cetera

Acute vs. Chronic Toxicosis
Copyright © 2016 EMLab P&K. All rights reserved.75
• Acute toxicity– Adverse effects of a substance that result either from a
single exposure or multiple exposures in a short space of time (usually less than 24 hours).
• Chronic toxicity– Prolonged (repeated) exposure to a substance
– Prolonged internal exposure because a substance remains in the body for a long time
• Doses required for acute toxicity are generally muchhigher than those for chronic toxicity.

Is A Disease Caused By Mycotoxin Exposure?
Copyright © 2016 EMLab P&K. All rights reserved.76
• Anecdotal evidence: Suspicion that mycotoxins have caused symptoms
• Animal studies: Documentation that effects CAN occur in animals
• Epidemiology: Association between exposure anddisease; Dose/response information
• Biological monitoring: Measurement of toxins or their metabolites or adducts in body fluids

Anecdotal Evidence
Copyright © 2016 EMLab P&K. All rights reserved.77
• Many anecdotal reports of mycotoxin associated illness in the lay press– None supported by unbiased data
– (Unfortunately) the courts accept these as indicating better than a 50/50 chance of a cause/effect relationship
• A few anecdotal reports in the peer reviewedliterature indicating the possibility of an association– Most admit that the association is not documented
– The courts accept these as well

Animal Studies
Copyright © 2016 EMLab P&K. All rights reserved.78
• Many reports of animal studies of mycotoxin effects.• Most seek to document mechanisms of action• Those attempting dose/response effects use very
high doses (much higher than would be expected from environmental exposure except by ingestion.
• Many of these studies are very well done, andindicate that mycotoxins are, in fact, toxic.
• They do not establish a connection betweenexposure and disease.

Epidemiological Studies
Copyright © 2016 EMLab P&K. All rights reserved.79
• Several epidemiological studies associate chronic mycotoxin exposure with cancer. These are all occupational.
• One epidemiological study reported associations between Stachybotrys on walls of infant bedrooms and pulmonary bleeding in the infants.
• The epidemiology in this study was improperly done, and the same organization (CDC) published an analysis of the former study, saying that the conclusions were not justified.

Biological Monitoring
Copyright © 2016 EMLab P&K. All rights reserved.80
• Biological monitoring is commonly done in studies documenting ingestion of mycotoxins. Most of these are focused on whether or not particular populations are routinely exposed to mycotoxins in their food.
• A few studies claim detection of mycotoxins in bodily fluids of people reporting airborne residential mycotoxin exposure. So far, these studies are not convincing, primarily because of bias.

Lower Respiratory Infections
Copyright © 2016 EMLab P&K. All rights reserved.81
• Lower respiratory illness:– There is epidemiological evidence
that children living in damp buildings have an increased incidence of lower respiratory infections.
– These effects are separate from asthma, and don’t depend on sensitivity to the fungi, or to family history of allergies.
– Some hypothesize that mycotoxins are involved, but no good evidence for this connection has appeared.


Anecdotal evidence: word of mouth, case studies
Copyright © 2016 EMLab P&K. All rights reserved.83
Experimental evidence Epidemiological evidence
Logic
“proof”
Types of Evidence

Fungal Irritants
Copyright © 2016 EMLab P&K. All rights reserved.84
• Irritants (volatile organic compounds):– There is some evidence that these
agents cause mucous membrane (eye, nose) irritation, and may lead to headaches.
– Evidence so far is incomplete but there is no indication so far that these effects do not occur.
– Neurological effects probably dueto perception of odors

Evidence for Fungal-Associated Irritant Effects
Anecdotal evidence: word of mouth, case studies
Copyright © 2016 EMLab P&K. All rights reserved.85
Experimental evidence Epidemiological evidence
Logic
“proof”

Fungal Toxins
• Diseases– Cancer– Immunosuppression– Neurological effects– Irritant effects
• Background– All of these effects are related to
ingestion of moldy food.– Cancer requires long term
exposure; exposure cumulative– Other effects are immediate;
exposures not cumulative– Inhalation very unlikely as an
exposure route
Copyright © 2016 EMLab P&K. All rights reserved.86

Fungus Mycotoxins Possible health effectsAlternaria alternata Tenuazoic acid Nephrotoxic,
hepatotoxic, hemorrhagic
Aspergillus flavus,A. parasiticus
Aflatoxins Mutagenic, carcinogenic, hepatotoxic
Aspergillus fumigatus Fumitremorgens,gliotoxin
Tumorgenic, cytotoxic
Cladosporium sp. Epicladosporic acid Immunosuppressive
Fusarium moniliforme Fumonisins Neuro, nephrotoxic and hepatotoxic, carcinogen
Stachybotrys chartarum (atra)
Satratoxins, verrucarins, roridins
Immunosuppressive, hemotoxic, hemorrhagic
Copyright © 2016 EMLab P&K. All rights reserved.87
Mycotoxins

Fungal Toxins – New Information
• New information– Hundreds of publications on
dietary mycotoxins, especially in underdeveloped countries.
– No new publications that provide evidence for airborne mycotoxin exposure.
– Stachybotrys conidia require air speeds 1,000 times higher than those that normally prevail in the indoor environment. (Tucker et al. 2007)
Copyright © 2016 EMLab P&K. All rights reserved.88

Fungal Toxins (cont’d)
• Toxic molds on the web– Many sites on the web claim
that scientists are underreporting the dangers of toxic mold.
– Position papers by major medical organizations are considered “biased”.
– Expert witnesses are considered biased because they are paid for presenting their opinions.
Copyright © 2016 EMLab P&K. All rights reserved.89

Fungal Toxins (cont’d)
• Comments
Copyright © 2016 EMLab P&K. All rights reserved.90
– Medical groups should not rely on reviews for position papers, only the published peer reviewed research literature.
– Courts should not decide scientific relevance of scientific literature. Position papers are consensus documents of experts in the field, and should be considered authoritative.
– Just because scientists are often defense witnesses does not mean they do not know the facts. Experts are hired because they do know the facts. These same experts would be used by the plaintiffs if the facts fit their cases.
– The fact remains that the exposure models are relevant and there is no good evidence for mycotoxin inhalation disease
• Synergistic effects
Copyright © 2016 EMLab P&K. All rights reserved.91
• Biomarkers, and background measurements of each– (note dietary mycotoxins as confounder)
– (sensitivity of the marker)
• Ochratoxin A: 0.011-0.1/A. carbonarius conidium

Evidence for Fungal-Associated MycotoxinEffects (Inhalation)
Anecdotal evidence: word of mouth, case studies
Copyright © 2016 EMLab P&K. All rights reserved.92
Experimental evidence Only for Agriculture
Logic
“proof”

Toxicological References
Copyright © 2016 EMLab P&K. All rights reserved.93
• Eduard W. 2009. Fungal spores: A critical review of the toxicological and epidemiological evidence as a basis for occupational exposure limit setting. CRITICAL REVIEWS IN TOXICOLOGY 39(10): 799-864
• Hardin BD, Robbins CA, Fallah P, Kelman BJ. 2009. The Concentration of No Toxicologic Concern (CoNTC) and Airborne Mycotoxins JOURNAL OF TOXICOLOGY AND ENVIRONMENTAL HEALTH- PART A-CURRENT ISSUES 72(9): 585-598

• Pasqualotto, AC. (Ed.) 2010 Chapter: Ben-Ami R, Kontoyiannis DP, 345-379• Kim et al., Indoor Air 2007; 17: 153–163• Pini et al.,2008• Tucker et al., Indoor Air 2007; 17: 153–163• Burr et al., 2007. Thorax;62:767–772.• Fisk et al., Indoor Air 2007; 17: 284–296• Holck et al., 2007. Basic & Clinical Pharmacology & Toxicology 101, 455-458• Iverson et al., 2007. Eur J Clin Microbiol Infect Dis 26:879–886• Nucci & Anaissie, 2007. CLINICAL MICROBIOLOGY REVIEWS, 695–704• Wang et al., 2007. Pediatr Allergy Immunol : 18: 441–447• Park et al., 2008. Environ Health Perspect 116:45–50.• Glass et al., 2007. Gen Dent. 55(5):4a36-40• Sautour et al., 2007. J Hosp Infect. Dec;67(4):367-73.• Wicklow & Shotwell., 1983. Canadian J Microbiology. 29(1):1-5.
Copyright © 2016 EMLab P&K. All rights reserved.94
General References

General References (cont’d)
Copyright © 2016 EMLab P&K. All rights reserved.95
• Janeway CA Jr, Travers P, Walport M, et al. Immunobiology: Hypersensitivity diseases. Available from: http://www.ncbi.nlm.nih.gov/books/NBK27136/
• http://www.niaid.nih.gov/topics/microbes/documents/microbesbook.pdf

Continuing Education Units (CEUs)
To receive a certificate of attendance, you mustcomplete the survey after thewebinar:
•Click on the survey link in the “Thank you” email (sent 1 hour after this webinar).
•Complete survey by this Friday, January 22, 2016.
•You will receive an email in 2-3 weeks with instructions when your certificate is ready.
Copyright © 2016 EMLab P&K. All rights reserved.96

Thank you for your time!
Copyright © 2016 EMLab P&K. All rights reserved.100
Questions about Mold:[email protected]
All other questions:[email protected]

Appendix
EMLab P&K

EMLab P&K Products
Authorized Distributor for:
Copyright © 2016 EMLab P&K. All rights reserved.99
Buy equipment and supplies for samplingallergens, asbestos, bacteria, mold, fungi, and more
Shop online at www.emlab.com/store
Locations Nationwide to Serve You(Addresses on Following Slides)
WASHINGTON
OREGON
IDAHO
NEVADA
MONTANA
WYOMING
UTAH
ARIZONA
COLORADO
NEW MEXICO
TEXAS
NORTH DAKOTA
SOUTH DAKOTA
NEBRASKA
KANSAS
OKLAHOMA
MINNESOTA
IOWA
MISSOURI
ARKANSAS
LOUISIANA
WISCONSIN
INDIANAILLINOIS
OHIO
KENTUCKY
TENNESSEE
GEORGIA
SOUTH CAROLINA
NEW YORK
PENNSYLVANIA
MICHIGAN
MAINE
WEST VIRGINIA
VIRGINIANORTH
CAROLINA
NEW HAMPSHIRE
VERMONT
MARYLAND
RHODE ISLAND
CONNECTICUTNEW JERSEYDELAWARE
MASSACHUSETTS
HAWAII
Copyright © 2016 EMLab P&K. All rights reserved.100

EMLab P&K Locations Near You
MicroLabs in bold are AIHA Accredited as documented by the
Scope of Accreditation Certificate.
Arizona - Phoenix1501 West Knudsen Drive Phoenix, AZ 85027phone: 800.651.4802fax: 623.780.7695AIHA LAP, LLC EMLAP# 102297
California - San Francisco 6000 Shoreline Ct, Suite 205 So. San Francisco, CA 94080 phone: 866.888.6653fax: 650.624.5371AIHA LAP, LLC EMLAP# 102856
New Jersey - Marlton3000 Lincoln Drive East, Suite A Marlton, NJ 08053phone: 866.871.1984fax: 856.334.1040AIHA LAP, LLC EMLAP# 103005
M I C R O L A B S
L A B O R A T O R I E S
California - San Diego 8304 Clairemont Mesa Blvd. Suite 103San Diego, CA 92111 Phone: 866.465.6653Colorado - Denver4955 Yarrow StreetArvada, CO 80002phone: 800.651.4802
Florida - Ft. Lauderdale6301 NW 5th Way Suite 1410Ft. Lauderdale, FL 33309phone: 877.711.8400
Georgia - Atlanta 6500 McDonough Dr. Suite C-10Norcross, GA 30093phone: 877.711.8400
Illinois - Chicago 1815 West Diehl Rd. Suite 800Naperville, IL 60563phone: 866.871.1984Nevada - Las Vegas 6000 S. Eastern Ave. Suite 5ELas Vegas, NV 89119phone: 866.888.6653
California - Glendale 1010 N. Central Ave. Suite 390Glendale, CA 91202phone: 866.465.6653California - Irvine17461 Derian Ave.Suite 100Irvine, CA 92614Phone: 866.465.6653
California - Sacramento880 Riverside ParkwayWest Sacramento, CA 95605phone: 866.888.6653
Texas - Houston6310 Rothway St.Houston, Texas 77040phone: 800.651.4802
Virginia - Fairfax 3929 Old Lee Highway Unit 91CFairfax, Virginia 22030phone: 866.871.1984
Washington - Seattle 19515 North Creek Parkway N, Suite 100 Bothell, WA 98011phone: 866.888.6653
For the most current list of locations, please visit us at www.emlab.com Contact individual laboratories for service capabilities and scopes of accreditation.
Copyright © 2016 EMLab P&K. All rights reserved.101

TestAmerica LocationsFor the most current list of locations, please visit us at www.emlab.com
For your convenience, you can drop off samples for EMLab P&K at these locations.CALIFORNIA - Pleasanton1220 Quarry Ln.Pleasanton, CA 94566phone: (925) 484-1919
CALIFORNIA - San Bernardino 202 E. Airport RoadSuite 140San Bernardino, CA 92408 Phone: (909) 370-4707
CALIFORNIA – W. Sacramento 880 Riverside PkwyWest Sacramento, CA 95605 phone: (916) 373-5600
CONNECTICUT128 Long Hill Cross Rd. Shelton, CT 06484phone: (203) 929-8140
FLORIDA - Jacksonville 8933 Western Way, Suite 1Jacksonville, FL 32256phone: (904) 519-9551FLORIDA - Orlando8010 Sunport Drive, Suite 116Orlando, FL 32809phone: (407) 851-2560
FLORIDA - Pensacola3355 McLemore Dr.Pensacola, FL 32514phone: (850) 474-1001FLORIDA - Tallahassee 2846 Industrial Plaza Dr. Tallahassee, FL 32301phone: (850) 878-3994
FLORIDA - Tampa6712 Benjamin Rd., Suite 100Tampa, FL 33634phone: (813) 885-7427GEORGIA - Atlanta6500 McDonough Drive, Suite C-10 Norcross, GA 30093phone: (678) 966-9991
GEORGIA - Savannah5102 LaRoche AvenueSavannah, GA 31404phone: (912) 354-7858HAWAII - Honolulu99-193 Aiea Heights Dr. Suite 121Aiea, HI 96701phone: (808) 486-5227
ILLINOIS - Chicago2417 Bond Street University Park, IL 60484 phone: (708) 534-5200
ILLINOIS - Elmhurst655 W. Grand Ave., Suite 205Elmhurst, IL 60126phone: (630) 758-0262INDIANA - IndianapolisStutz Business Center212 W. 10th Street, Ste A-205 Indianapolis, IN 46202Phone: (317) 264-9686
INDIANA - Valparaiso 2400 Cumberland DriveValparaiso, IN 46383phone: (219) 464-2389IOWA - Cedar Falls 704 Enterprise Drive Cedar Falls, IA 50613 phone: (319) 277-2401IOWA - Davenport736 Federal St., Suite 2202Davenport, IA 52803phone: (563) 323-7944
LOUISIANA - Baton Rouge6113 Benefit Dr.Baton Rouge, LA 70809 phone: (225) 755-8200MARYLAND - Baltimore5710 Executive Drive, Suite 106Baltimore, MD 21228phone: (410) 869-0085MASSACHUSETTS - Boston240 Bear Hill Rd., Suite 104Waltham, MA 02451phone: (781) 466-6900MASSACHUSETTS - Westfield 53 Southampton RoadWestfield, MA 01085phone: (413) 572-4000
MICHIGAN - Brighton10448 Citation Drive, Suite 200Brighton, MI 48116Phone: (810) 229-2763MINNESOTA - Minneapolis 7204 West 27th Street, Suite 114 St. Louis Park, MN 55426 phone: (800) 593-8519
ALABAMA - Mobile900 Lakeside DriveMobile, AL 36693phone: (251) 666-6633ALASKA - Anchorage2000 W. International Airport Rd., Suite A10Anchorage, AK 99502phone: (907) 563-9200
ARIZONA - Phoenix4625 E. Cotton Center Blvd., Suite 189Phoenix, AZ 85040phone: (602) 437-3340
ARIZONA - Tucson1870 W. Prince Road, Suite 59Tucson, AZ 85705phone: (520) 807-3801CALIFORNIA – Costa Mesa 3585 Cadillac Ave, Suite A Costa Mesa, CA 92626 phone: (714) 258-8610
Copyright © 2016 EMLab P&K. All rights reserved.102

TestAmerica Locations (cont’d)
NEW YORK - Albany 25 Kraft Ave.Albany, NY 12205phone: (518) 438-8140NEW YORK - Buffalo10 Hazelwood Drive, Ste. 106Amherst, NY 14228phone: (716) 691-2600NEW YORK - New York City 47-32 32nd Place, Suite 1141 Long Island City, NY 11101 Phone: (347) 507-0579
NEW YORK - Syracuse 118 Boss Rd.Syracuse, NY 13211phone: (315) 431-0171
NORTH CAROLINA - Charlotte I-85 South Bldg.2858 Queen City Dr., Suite B Charlotte, NC 28208phone: (704) 392-1164
NORTH CAROLINA - Raleigh101-F Woodwinds Industrial CourtCary, NC 27511phone: (919) 380-9919
For the most current list of locations, please visit us at www.emlab.comFor your convenience, you can drop off samples for EMLab P&K at these locations.
OHIO - Cincinnati 11416 Reading RoadCincinnati, OH 45241phone: (513) 733-5700OHIO - Dayton4738 Gateway CircleDayton, OH 45440Phone: (937) 294-6856OHIO - North Canton 4101 Shuffel Street NW North Canton, OH 44720 phone: (330) 497-9396OREGON - Portland 9405 SW Nimbus Avenue Beaverton, OR 97008phone: (503) 906-9200
PENNSYLVANIA - King of Prussia 1008 W. Ninth Ave.King of Prussia, PA 19406 phone: (610) 337-9992
PENNSYLVANIA - Pittsburgh 301 Alpha DrivePittsburgh, PA 15238phone: (412) 963-7058
SOUTH CAROLINA - Charleston 1436-A North Point LaneMt. Pleasant, SC 29464 phone: (843) 849-6550TENNESSEE - Knoxville 5815 Middlebrook PikeKnoxville, TN 37921phone: (865) 291-3000
TENNESSEE - Nashville 2960 Foster Creighton Dr. Nashville, TN 37204phone: (615) 726-0177
TEXAS - Austin14050 Summit Dr., Ste. A100 Austin, TX 78728phone: (512) 244-0855
TEXAS - Beaumont 4400 Lawndale Ave.Groves, TX 77619phone: (409) 540-5302TEXAS - Corpus Christi 1733 N. Padre Island Drive Corpus Christi, TX 78408 phone: (361) 289-2673
MISSOURI - Eureka1699 West Fifth Street, #200Eureka, MO 63025Phone: (314) 302-8354
MISSOURI - Kansas City 601 NW 39th StreetBlue Springs, MO 64015 phone: (800) 276-1286
MISSOURI - St. Louis13715 Rider Trail North Earth City, MO 63045 phone: (314) 298-8566
NEW JERSEY - Edison 777 New Durham Road Edison, NJ 08817phone: (732) 549-3900NEW JERSEY - South Jersey 520 Fellowship Rd., Suite A-106 Mt. Laurel, NJ 08054phone: (856) 222-1990
TEXAS - San Antonio404 E. Ramsey, Suite 208 San Antonio, TX 78216 phone: (210) 344-9751
VERMONT - Burlington30 Community Drive, Suite 11 South Burlington, VT 05403 phone: (802) 660-1990
VIRGINIA - Virginia Beach 5135 Cleveland Street Virginia Beach, VA 23462 phone: (757) 671-1291
WASHINGTON - Richland 2800 George Washington Way Richland, WA 99354phone: (509) 375-3131
WASHINGTON - Spokane 11922 E. 1st Ave.Spokane, WA 99206phone: (509) 924-9200
WASHINGTON - Tacoma5755 8th Street East Tacoma, WA 98424phone: (253) 922-2310
Copyright © 2016 EMLab P&K. All rights reserved.103

107 Copyright © 2016 EMLab P&K. All rights reserved.
When quality and accuracy are critical.
Copyright © 2016 EMLab P&K, a TestAmerica Company
Analytical Services: Fungi, Asbestos, Bacteria, USP <797>, PCR, Allergens & Radon
Phone: (866) 888-MOLD (6653)Email:
[email protected] Web: www.emlabpk.com