head injury pathway - tameside and glossop … hospital nhs foundation trust head injury pathway...
TRANSCRIPT

Head Injury Rehabilitation Pathway
3.0 (final)
Head Injury management - multidisciplinary document
Version: 3.0 Authorised by: NSF-long term conditions local
implementation group Date authorised: March 2013 Next review date: March 2015 Document author: Nicki Hatton/NSF-LTC working group

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 2 of 26
Check the Intranet for the latest version

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 3 of 26
Check the Intranet for the latest version
VERSION CONTROL SCHEDULE Head injury rehabilitation pathway Version : 2.0 final
Version Number Issue Date Revisions from previous issue
0.1 (draft) Sept 2007
0.2 (draft) 0.3(draft) 0.4 (draft)
April 2008 April 2008 July 2008
1.0 (final) Jan 2009 Reformatted, ratified and uploaded
2.0 (final) Feb 2011 Reviewed and revised document
3.0 (final) March 2013 Reviewed and revised document

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 4 of 26
Check the Intranet for the latest version
INDEX/ TABLE OF CONTENTS INTRODUCTION ........................................................................................................ 5 PURPOSE .................................................................................................................. 5 Scope ......................................................................................................................... 6 Definitions ................................................................................................................... 7
POLICY STATEMENT ................................................................................................ 7 MEDICAL MANAGEMENT ......................................................................................... 9 Admission to ward………………………………………………………………………….10 Team input…………………………………………………………………………………..12 Guidance on neurological observations………………………………………………….13 Family involvement…………………………………………………………………………14 ASSESSMENTS AND CARE PLANS - to be used as required…………………………. Cognitive assessment and management……………………………………………..15 Daily routine/activity of daily living assessment and management……………..17 Behaviour/anxiety/depression management and assessment………………...…19 Physical functioning/pain assessment and management…………………………21 Communication assessment/Miscellaneous……………………………….…...…...23 Discharge planning…………………………………………………………………………24 Policy Development & Consultation .......................................................................... 25 Monitoring ................................................................................................................. 25 EQUALITY AND DIVERSITY ................................................................................... 25
REFERENCES ......................................................................................................... 25 BIBLIOGRAPHY ....................................................................................................... 25
Review ...................................................................................................................... 25
TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 5 of 26
Check the Intranet for the latest version
INTRODUCTION This pathway has been developed to improve the management and quality of care for head injured patients whilst in Tameside Hospital Foundation Trust. This has been developed as a method to improve compliance with the National Service Framework for long term conditions and other relevant guidelines. The pathway will be used with any patients presenting with the following conditions:
Traumatic brain injury (requiring hospital admission for management rather than observation)
Anoxic brain injury
Sub-arachnoid haemorrhage
Post-neurosurgical
Primary brain tumours
Encephalitis
If additional help or support is required regarding the use of the pathway contact: Nicki Hatton MSc MCSP Clinical Specialist – Neurological Physiotherapist Ext 4122 bleep 1743 [email protected]
PURPOSE
This document will provide a framework for the management of the above patients in addition to standard care. It will commence as the patient is admitted to the ward from A&E, ITU or neurosurgical centre.
The pathway will outline best practice based on current guidelines to facilitate the effective management of this group of patients.
Management of this group of patients can be complex and varied – professional judgement should always be applied. The pathway has been designed to incorporate the ‘head injury team’ so that assessment findings and management strategies can be documented.
The pathway highlights the need for specific care plans pertinent to head injury management. These should be written initially by the member of staff who triggers the care plan.
The document should be used by all staff – supporting documentation and additional assessments will be located in the supplementary information file.
A supplementary information file will be located on each ward where head injured patients are likely to be.
The document should be filed in the medical case notes when the pathway is completed.

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 6 of 26
Check the Intranet for the latest version
SCOPE The document is intended to be used by all staff and can be filled in by any health professional (there will be sections that require specific documentation from the head injury team). The relevant documents should be written on and then placed in the care plan section of the nursing kardex. The ICP will be used on whichever ward the patient is placed on. The head injury team will be responsible for ensuring that all parts of the pathway are completed – ward based staff should complete any documents that they are competent to do. Duplication should be minimised therefore sections of this pathway should be used in preference to existing notes where possible. The pathway does not have to be completed chronologically.
IMPLEMENTATION The care pathway will be commenced as the patient is admitted to the ward (this could be any ward under the care of any consultant). The pathway describes best management and what factors need to be assessed – it will be the responsibility of the peripatetic head injury team to ensure that all aspects of the pathway are completed. If parts of the pathway can’t be completed due to a lack of suitably trained staff this will be documented. There is huge variability in the frequency and severity of patients admitted to Tameside Hospital Foundation Trust, the previous document (version 1.0) has been used on occasions, however due to its format much of the document was unused particularly if the patient presented with only a small number of neurological symptoms. The new version has been designed to allow only the documents that are required to be in the kardex (from page 14 onwards). The head injury team will place the relevant documents in the kardex as they are filled in. The head injury team will be responsible for in-situ training as the need arises on the relevant wards. It is not envisaged that there will be a financial implication associated with the pathway – the aim is to reduce duplication, enhance team working and provide more co-ordinated care. Head Injury team: This team has been developed to provide ward based staff with additional advice and support in the management of head injured patients. The team will be peripatetic and virtual – ie provide input wherever the patient may be within the hospital and will constitute members of staff from existing services. The team will facilitate the use of the pathway and will be responsible, in liaison with ward staff, for developing multi-disciplinary goals, treatment plans and discharge coordination. The first point of referral will be: Nicki Hatton – Clinical Specialist Physiotherapist Extension – 4122, bleep 1743 Telephone referrals will suffice – following initial assessment the other head injury team members will be notified.

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 7 of 26
Check the Intranet for the latest version
DEFINITIONS A glossary of commonly used terms and abbreviations will be located in the head injury resource file.
ROLES AND RESPONSIBILITIES The ICP will be completed by ward based and head injury team staff – each individual will be responsible to their own manager. The filling in of the ICP will be monitored by the head injury team and audited at a later stage.
POLICY STATEMENT This document should commence on admission to the ward. It outlines what needs to be assessed and what symptoms may be present. The pathway is available on the intranet or via a member of the head injury team and supplementary information will be located in the head injury resource file. Advice from the head injury team will aim to provide more evidence based, guideline compliant treatment and management. Rehabilitation should commence as early as possible and be multidisciplinary. This should take into account the cognitive, perceptual, physical, behavioural and social aspects of head injury management – the pathway aims to facilitate this process. The ICP will be used until the patient is discharged or transferred – regular reassessment and formulation of care plans should occur throughout the patient’s stay.
TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 8 of 26
Check the Intranet for the latest version
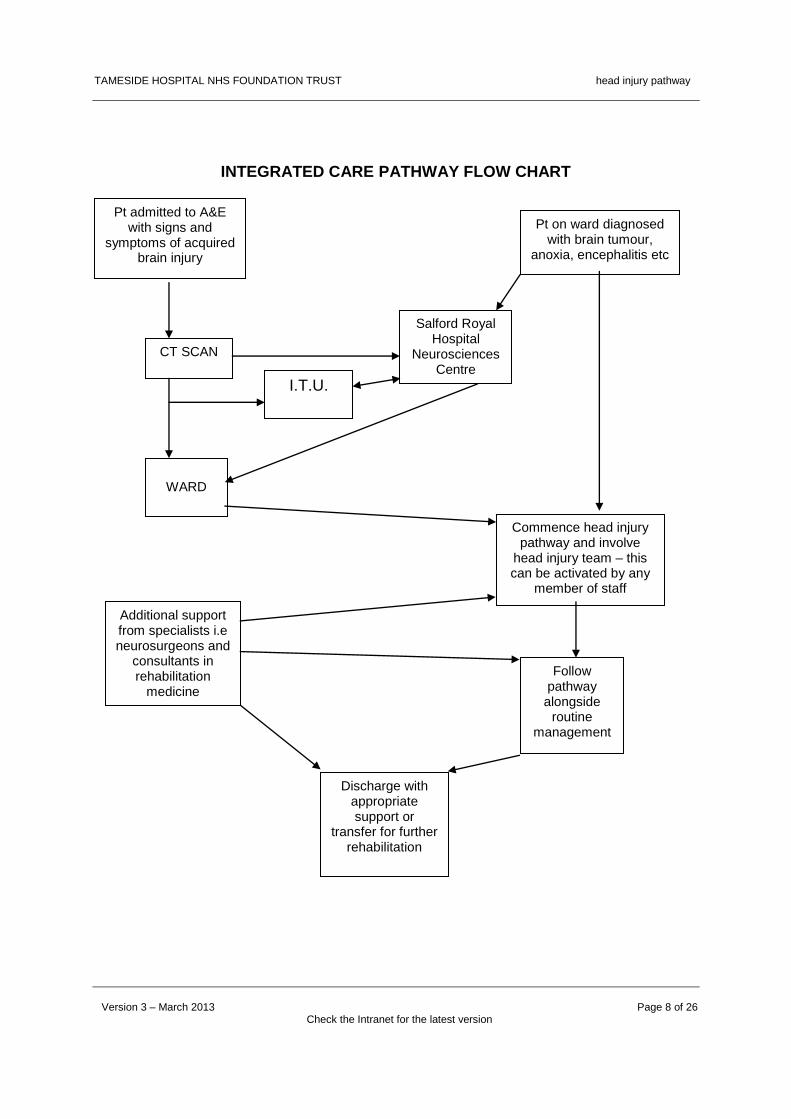
INTEGRATED CARE PATHWAY FLOW CHART
Pt admitted to A&E with signs and
symptoms of acquired brain injury
Pt on ward diagnosed with brain tumour,
anoxia, encephalitis etc
CT SCAN
Salford Royal Hospital
Neurosciences Centre
I.T.U.
WARD
Commence head injury pathway and involve
head injury team – this can be activated by any
member of staff
Additional support from specialists i.e neurosurgeons and
consultants in rehabilitation
medicine
Follow pathway alongside
routine management
Discharge with appropriate support or
transfer for further rehabilitation

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 9 of 26
Check the Intranet for the latest version
MEDICAL MANAGEMENT
Any medication prescribed
complies with current
guidance – see supplementary
file
Document frequency of neurological observations
and what to do if condition
deteriorates
Pt managed in ward setting with head
injury team input
Additional advice re medical management
obtained from Consultant in Rehab
Medicine of Neurosurgeon
Regular review, check epilepsy status and drug management
Refer to other consultants as required
eg PEG, ENT etc
Regular team meetings and
discussion with family to update
on condition
Discharge, referral to tertiary centre or
specialist community team
Patient assigned to appropriate
consultant
Additional advice obtained from SRFT
Neurosciences Centre as required
Medical assessment form completed
TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 10 of 26
Check the Intranet for the latest version
ADMISSION TO WARD This is to be completed by nursing staff on admission to ward – refer to supplementary information file located on the ward for additional information.
Date Signature
Document diagnosis and give a brief outline of presenting condition on admission to the ward:
Outline where patient had been treated prior to admission to ward:
Ensure that the patient has been referred to the Head Injury Team: Contact Nicki Hatton – Physiotherapy Dept (x 4122 or bleep 1743) Date of referral:
Name: ___________________ DOB: ___________________ Unit no: ___________________ NHS no ___________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 11 of 26
Check the Intranet for the latest version
ADMISSION TO WARD – CONTINUED:
Date Signature
Commence neurological observation chart: Ensure that staff know how frequently to perform observations: Glasgow Coma Scale score on admission to ward: Eyes: /4 Verbal: /5 Motor: /6 Total: /15
Follow TGH swallowing care plan: Perform swallow screen if appropriate: Date completed: Document reasons if not completed:
Complete nutritional screening tool and commence appropriate care plan – refer to supplementary information file for additional advice with regard to head injured patients.
Commence epilepsy monitoring. It is important to monitor all head injured patients as patients can develop epilepsy some time after initial onset.
Commence falls assessment/pathway as part of routine patient management – document in the care plan any head injury specific reasons for falls eg visuo-perceptual deficit, reduced judgement and safety awareness etc.
Name: ___________________ DOB: ___________________ Unit no: ___________________ NHS no ___________________
TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 12 of 26
Check the Intranet for the latest version
TEAM INPUT
WARD BASED STAFF:
DESIGNATION NAME CONTACT DETAILS
NAMED NURSE
PHYSIOTHERAPIST
OCCUPATIONAL THERAPIST
DIETICIAN
SOCIAL WORKER
HEAD INJURY TEAM MEMBERS:
DESIGNATION NAME CONTACT DETAILS
SPECIALIST NURSES:
PHYSIOTHERAPIST
OCCUPATIONAL THERAPIST
S.A.L.T.
CLINICAL PSYCHOLOGIST
CONSULTANTS:
OTHERS INVOLVED:
OTHER USEFUL CONTACTS: Consultant neurosurgeon/neurologist: Name: Contact number: Consultant in Rehabilitation Medicine: Name: Contact number: Community neurological rehabilitation team – 366 2323 Selbourne House, Hyde Specialist neuro rehab nurse – 366 2323 Headway – 0808 800 2244 (National), 07733 320049 (Local) BASIC (Brain and spinal injury charity) – 0870 750 0000 Neurocare centre – 0161 707 6441
Name: _____________________ DOB: _____________________ Unit no: _____________________ NHS no _____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 13 of 26
Check the Intranet for the latest version
GUIDANCE ON NEUROLOGICAL OBSERVATIONS
Mild/minor head injury: GCS 13-15 Moderate head injury: GCS 9-12 Severe head injury: GCS < 9 The Glasgow Coma Scale should be recorded as separate parameters. Eye: / 4 Verbal: / 5 Motor: / 6 The GCS should be monitored every 30 minutes until there is a score of 15 then every 60 minutes for 4hours and then 2 hourly. If GCS drops obtain a medical review (assess ABG’s, electrolytes and recent drug administration). If no cause can be found repeat CT scan. If this is abnormal seek a neurosurgical review. Other indications for review include the development of agitation, abnormal behaviour, severe increase in headache and/or persistent vomiting or new neurological signs. Regular contact should be maintained with the neurosurgeon and/or consultant in rehabilitation medicine as required.

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 14 of 26
Check the Intranet for the latest version
j FAMILY INVOLVEMENT
To be completed by named nurse or head injury team member.
Date Signature
Ward based staff or head injury team member should make contact with the patients family and arrange to meet: Date of meeting:
Distribute patient information leaflet (available on intranet; headinjurypatientinfoleaflet) and additional support leaflets available from Headway (headway.org.uk/Factsheets) Details:
Document if family members require further information/support: Detail intervention required:
Are family members able/willing to take an active role in the patients care/rehabilitation? Give details:
Note any relevant factors that may influence rehabilitation eg social circumstances, previous drug/alcohol problems, psychiatric history, previous physical deficits etc.
The following sections should be placed in the pathway if deemed relevant by a member of the head injury team – please refer to these assessments and care plans for advice and guidance regarding the management of each individual patient.
Name: _____________________ DOB: _____________________ Unit no: _____________________ NHS no_____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 15 of 26
Check the Intranet for the latest version
COGNITIVE ASSESSMENT AND MANAGEMENT
Post-traumatic amnesia (PTA) is a clinical feature often apparent after a traumatic head injury even in patients who may not have lost consciousness. Symptoms may include disorientation, confusion, agitation and restlessness. Patients will have limited short term memory, may not recognise people, could be disinhibited or act out of character. PTA may last weeks or months. Points to consider:
Does the patient require orientation strategies or memory aids.
Ensure consistency of information, try to minimise personnel involved in care.
Outline level of supervision required.
Do not constantly correct patient if they are delusional.
Patients behaviour may be affected for other reasons: eg infection, pain, alcohol withdrawal, medication.
If patient requires sedation benzodiazepines such as lorazepam should be used.
Avoid haloperidol and chlorpromazine.
Use Trust mental health pathway for further guidance if required.
Date Outline initial cognitive symptoms patient presents with. Signature
Brief outline of neurological OT assessment:
Date Assessment Recommendations Signature
Memory
Attention
Executive function
Information processing
Name: ___________________ DOB: ___________________ Unit no: ___________________ NHS no ___________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 16 of 26
Check the Intranet for the latest version
COGNITIVE MANAGEMENT CARE PLAN
Can be completed and added to by any member of staff.
Date Signature
Outline the main areas of difficulty for the patient with regard to their cognitive deficit.
Name: _____________________ DOB: _____________________ Unit no: _____________________ NHS no_____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 17 of 26
Check the Intranet for the latest version
DAILY ROUTINE/ACTIVITIES OF DAILY LIVING ASSESSMENT AND MANAGEMENT
Many patients with head injury have difficulty structuring their time and even if physically capable they may struggle with everyday tasks. Routine, consistency of approach and an awareness that over-stimulation can be detrimental are key factors in management. Points to consider:
Is an orientation board with time, location etc required?
The patient may lack initiation, be distractable and have a poor sleep routine – these factors should be considered in the care plan.
Assess whether the patient can constructively occupy their time – if not, a plan should be devised taking into account of patients likes and dislikes and usual routine.
The plan should take into account the amount of rest/sleep the patient requires and structured activities should occur for a set amount of time with only one activity at once. Eg TV watching.
Care should be taken to minimise sensory overload ie if people are talking/treating etc then TV/radio should be switched off.
Behavioural outbursts or agitation are often caused because of overstimulation – the patient should be monitored to assess what factors cause this.
Relatives should be instructed about the importance of the above.
Assess whether the patient requires a side room or requires supervision within a larger ward setting taking into account the above factors.
To be completed by occupational therapist following assessment.
Date Signature
Outline the main areas of difficulty for the patient in performing ADL’s (include perceptual and cognitive features alongside physical problems)
Describe the level of assistance/support required and the rationale for this (again include cognitive and perceptual factors)
Name: ____________________ DOB: ____________________ Unit no: ____________________ NHS no ____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 18 of 26
Check the Intranet for the latest version
DAILY ROUTINE/ ADL MANAGEMENT CARE PLAN
Can be completed and added to by any member of staff
Date Signature
Outline the main factors to be considered following assessment.
Name: ____________________ DOB: ____________________ Unit no: ____________________ NHS no ____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 19 of 26
Check the Intranet for the latest version
BEHAVIOURAL
ASSESSMENT/MANAGEMENT
Many patients will display behavioural symptoms that are out of character. It is important that triggers for abnormal behaviour are identified and a plan devised that anticipates potential problems as well as ongoing problems. Points to consider:
Often the patient will not be in control of their actions.
Consider if the patient is withdrawing from drugs/alcohol/ITU
Assess triggers for abnormal behaviour – is it linked to a person, time of day, pain, catheters, constipation, communication difficulties, anxiety, reduced insight etc.
A consistency of approach is vital
Try to minimise child –like or ‘daft’ behaviour even if it is amusing.
Assess the risk of a patient absconding and plan appropriately.
Does the patient require referral to drug/alcohol liaison team or mental health services.
Date Outline main behavioural problems and triggers for these. Signature
ANXIETY/DEPRESSION
Be aware that pts may be at risk of developing post-traumatic stress disorder especially following critical care treatment. Points to consider:
The patient may have flashbacks, recurrent dreams, avoidance of thoughts/feelings/activities associated with trauma, emotional detachment, insomnia and poor concentration.
If anti-depressants are prescribed monitor closely as seizure thresholds can be lowered.
Date Document symptoms associated with anxiety/depression Signature
Name: _____________________ DOB: _____________________ Unit no: _____________________ NHS no ____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 20 of 26
Check the Intranet for the latest version
BEHAVIOURAL/ANXIETY/DEPRESSION
MANAGEMENT CARE PLAN Can be completed and added to by any member of staff
Date Outline the main factors to be considered following assessment. Signature
Name: ____________________ DOB: ____________________ Unit no: ____________________ NHS no____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 21 of 26
Check the Intranet for the latest version
PHYSICAL FUNCTIONING Following head injury some pts may be left profoundly physically disabled or may have no physical deficit. Points to consider:
If a patient is physically able it doesn’t mean that they won’t have other neurological deficits.
Spasms and spasticity may be exacerbated by pain, agitation, bladder and bowel dysfunction, IV lines etc.
Some pts may be able to move all four limbs but may have very poor balance mechanisms.
Patients with poor insight, reduced cognition, perception or impulsivity may be at increased risk of falls if they try to move without having an intact balance mechanism.
Do not force spastic/tight limbs into a position they don’t want to rest in – use pillows, bed etc to provide comfort and support.
To be completed by physio following assessment (use body chart if required)
Date Document main physical symptoms: Signature
PAIN ASSESSMENT
The patient may not be able to express pain or outline symptoms, it may present as agitation or restlessness. Points to consider:
Assume that patient will be in pain unless you can show otherwise, especially following TBI where other trauma has occurred – use all forms of communication to check this.
If patient has spasticity or abnormal postures, these are often painful.
Bladder and bowel dysfunction, IV lines and catheters will all cause pain.
Head injured patients can often experience neurogenic pain – this will require different medication.
Date Document patients description or expression of pain and any triggering factors.
Signature
Name: ____________________ DOB: ____________________ Unit no: ____________________ NHS no ___________________
TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 22 of 26
Check the Intranet for the latest version
PHYSICAL FUNCTIONING/PAIN CARE PLAN
Can be completed or added to by any member of staff
Date Outline how physical symptoms and pain are to be managed. Signature
Name: _____________________ DOB: _____________________ Unit no: _____________________ NHS no ____________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 23 of 26
Check the Intranet for the latest version
COMMUNICATION ASSESSMENT/MANAGEMENT
Points to consider:
If the patient is unable to communicate verbally it is imperative that another communication channel is established eg physical gestures, light-writer, communication board.
Some patients will communicate well verbally but confabulate ie have a conversation without any basis in reality.
Some patients may have a very limited vocabulary or expressive/receptive dysphasia.
It can be often difficult to distinguish between speech and language deficit and cognitive deficit.
To be completed by SALT following assessment
Date Outline of main speech deficits Signature
See separate SALT plan for further details.
MISCELLANEOUS:
Date Details of wheelchair/cushion/equipment ordered:
Signature
Details of visual disturbance, dizziness, hearing loss and referral to other clinicians if required.
Describe any other relevant factors pertinent to the management of this patient.
Name: ________________________ DOB: ________________________ Unit no: ________________________ NHS no ________________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 24 of 26
Check the Intranet for the latest version
DISCHARGE PLANNING Use TGH discharge plans in addition to the following pages:
Date Signature
Following team review outline the initial discharge plans and options. Links should be made at the earliest opportunity with tertiary centres such as the Devonshire Centre and with the Consultant in Rehabilitation Medicine if required. Document any referrals made regarding discharge: (Referral letters to be kept in medical notes)
Where is pt to be discharged to?
Outline what equipment should be taken with pt on discharge:
Discontinuation of head injury pathway: Reason:
Name: ______________________ DOB: ______________________ Unit no: ______________________ NHS no______________________

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 25 of 26
Check the Intranet for the latest version
POLICY DEVELOPMENT & CONSULTATION
The protocol/care pathway was initially developed following publication of the National Service Framework for long term conditions in 2005. A local implementation group was developed (Chair – Adrian Griffiths, Lead – Jill Rogalski). From this a working group was developed to implement the key aspects of care outlined in the above document (Chair – Nicki Hatton). The working group process mapped the patient journey and its variables. A wide range of clinicians and the voluntary sector were consulted. The care pathway will be piloted on whichever ward a head injured patient is admitted to and subsequent amendments will be made. Following a review the document was amended in February 2011.
MONITORING Where monitoring has identified deficiencies, recommendations and action plans will be developed and changes implemented accordingly. Progress on these will be reported to NSF-LTC local implementation group.
EQUALITY AND DIVERSITY The Tameside Hospital Foundation Trust is committed to ensuring that, as far as is reasonably practicable, the way we provide services to the public and the way we treat our staff reflects their individual needs and does not discriminate against individuals or groups on any grounds.
REFERENCES Department of Health (2005) National Service Framework for long term conditions.
BIBLIOGRAPHY BSRM/RCP – British Society of Rehabilitation Medicine/Royal College of Physicians (2003). Rehabilitation following acquired brain injury – national clinical guidelines. TARN – Trauma, audit and research network (2006). The management of head injured patients within Greater Manchester. Greater Manchester TBI audit group.
REVIEW This policy will be formally reviewed in February 2015 (2 years after approval/implementation), or earlier depending on the results of monitoring.

TAMESIDE HOSPITAL NHS FOUNDATION TRUST head injury pathway
Version 3 – March 2013 Page 26 of 26
Check the Intranet for the latest version
Equality Impact Assessment Tool
Yes/No Comments
1. Does the policy/guidance affect one group less or more favourably than another on the basis of:
Race No
Ethnic origins (including gypsies and travellers)
No
Nationality No
Gender No
Culture No
Religion or belief No
Sexual orientation including lesbian, gay and bisexual people
No
Age No
Disability - learning disabilities, physical disability, sensory impairment and mental health problems
No
2. Is there any evidence that some groups are affected differently?
Yes The procedure is slightly different to accommodate variations in disability, not all patients require all interventions.
3. If you have identified potential discrimination, are any exceptions valid, legal and/or justifiable?
No Any differences are to maintain patient health and safety. To do what is reasonably practicable to maintain safety.
4. Is the impact of the policy/guidance likely to be negative?
No
5. If so can the impact be avoided? N/A
6. What alternatives are there to achieving the policy/guidance without the impact?
N/A
7. Can we reduce the impact by taking different action?
N/A