hayley cosh, rd abbott nutrition adult clinical nutriton · 2018-04-05 · scope of the wound...
TRANSCRIPT
HEALING FROM THE INSIDE OUT: THE ROLE OF NUTRITION AND WOUNDS
Hayley Cosh, RDAbbott Nutrition Adult Clinical Nutriton
1

DISCLOSURE STATEMENT
• Support for this program is provided by Abbott Nutrition
• This program is not intended for continuing education
credits for any healthcare professional
2

• Highlight key issues in today’s healthcare environment related to wounds
• Discuss principles of nutrition therapy and updated NPUAP Guidelines
for prevention and treatment
• Review updated data on the use of HMB, arginine and glutamine in
wound healing
PROGRAM AGENDA
3

TODAY THERE ARE NEW CONCERNS IN HEALTH CARE
• Stage 3 and 4 pressure injuries that
occur after admission to a
healthcare facility are not
reimbursed by CMS1
• 76% of 30-day readmissions have
been identified as potentially
preventable; more than half of the
nation’s hospitals — a total of 2,597
will be penalized this year2,3
• Patient lawsuits are increasingly common in both acute and long-
term settings with judgments as high
as $312 million in a single case4
1. http://www.qualityforum.org/Topics/SREs/List_of_SREs.aspx#sre3 Accessed 8/9/2016,
2. http://khn.org/news/more-than-half-of-hospitals-to-be-penalized-for-excess-readmissions/, Accessed 8/9/2016.
3. http://njhimss.org/images/documents/whitepapers/Solving-Preventable-Readmissions-White_Paper.pdf. Accessed 8/9/2016.
4. Legal issues in the Care of pressure Ulcer Patients. http://www.medline.com/media/mkt/pdf/research/Wound-Skin-Care/Legal-issues-in-care-of-pressure-ulcer-patients.pdf. Accessed 8/9/2016.
4

SCOPE OF THE WOUND PROBLEM1
• Types of chronic wounds
in the US are pressure
injury, diabetic ulcer,
venous ulcer, arterial
ulcer, sickle cell ulcer,
burns, traumatic wounds,
and surgical wounds
• 6.5 million patients in the
US are affected
• $25 billion is the current
annual cost of chronic
non-healing wounds in the US
1. Sen CK, et al. Wound Repair Regen. 2009;17(6):763–771.
Stage 1 Stage 2
Stage 3 Stage 4
5
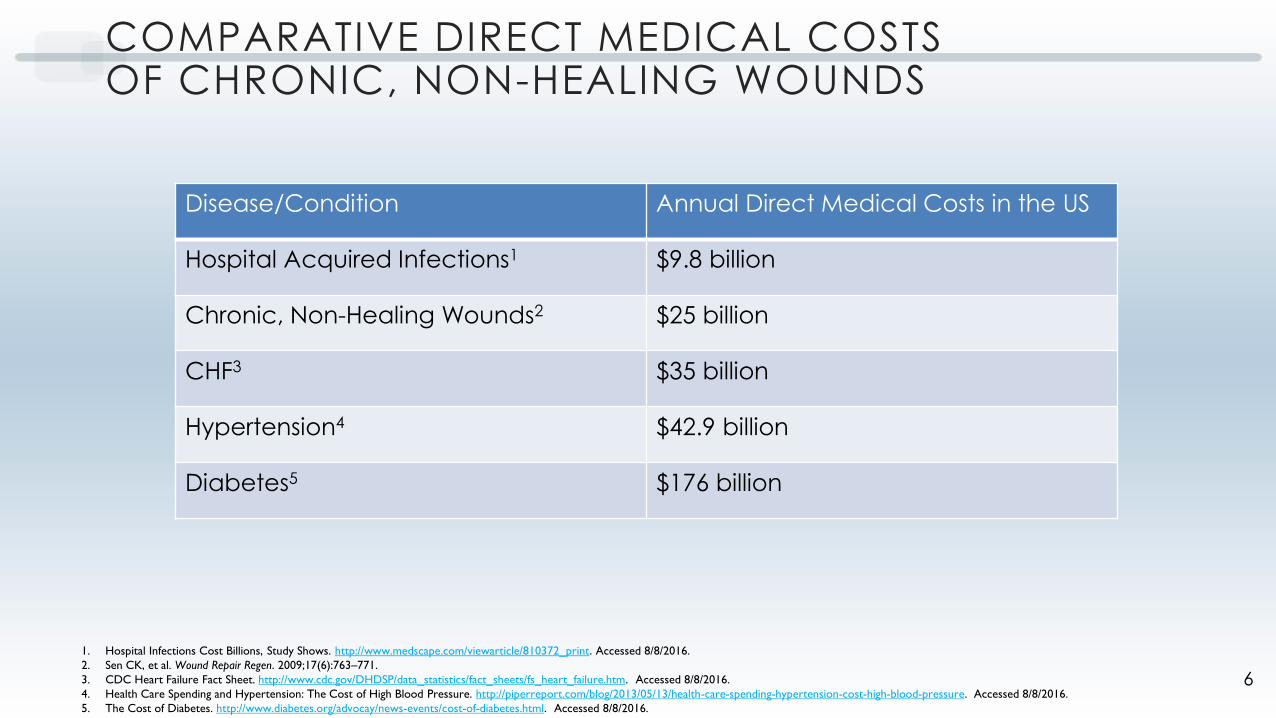
COMPARATIVE DIRECT MEDICAL COSTS OF CHRONIC, NON-HEALING WOUNDS
Disease/Condition Annual Direct Medical Costs in the US
Hospital Acquired Infections1 $9.8 billion
Chronic, Non-Healing Wounds2 $25 billion
CHF3 $35 billion
Hypertension4 $42.9 billion
Diabetes5 $176 billion
1. Hospital Infections Cost Billions, Study Shows. http://www.medscape.com/viewarticle/810372_print. Accessed 8/8/2016.
2. Sen CK, et al. Wound Repair Regen. 2009;17(6):763–771.
3. CDC Heart Failure Fact Sheet. http://www.cdc.gov/DHDSP/data_statistics/fact_sheets/fs_heart_failure.htm. Accessed 8/8/2016.
4. Health Care Spending and Hypertension: The Cost of High Blood Pressure. http://piperreport.com/blog/2013/05/13/health-care-spending-hypertension-cost-high-blood-pressure. Accessed 8/8/2016.
5. The Cost of Diabetes. http://www.diabetes.org/advocay/news-events/cost-of-diabetes.html. Accessed 8/8/2016.
6

COMPARATIVE DIRECT MEDICAL COSTS OF CHRONIC, NON-HEALING WOUNDS
Disease/Condition Annual Direct Medical Costs in the US
Hospital Acquired Infections1 $9.8 billion
Chronic, Non-Healing Wounds2 $25 billion
CHF3 $35 billion
Hypertension4 $42.9 billion
Diabetes5 $176 billion
1. Hospital Infections Cost Billions, Study Shows. http://www.medscape.com/viewarticle/810372_print. Accessed 8/8/2016.
2. Sen CK, et al. Wound Repair Regen. 2009;17(6):763–771.
3. CDC Heart Failure Fact Sheet. http://www.cdc.gov/DHDSP/data_statistics/fact_sheets/fs_heart_failure.htm. Accessed 8/8/2016.
4. Health Care Spending and Hypertension: The Cost of High Blood Pressure. http://piperreport.com/blog/2013/05/13/health-care-spending-hypertension-cost-high-blood-pressure. Accessed 8/8/2016.
5. The Cost of Diabetes. http://www.diabetes.org/advocay/news-events/cost-of-diabetes.html. Accessed 8/8/2016.
7

PRESSURE INJURY CAN INCREASE LENGTH OF STAY AND HOSPITAL READMISSIONS1
1. Lyder CH et al. J Am Geriatr Soc 2012; 60(9):1603-8.
• 51,842 hospitalized fee-for-service Medicare patients (1/1/2006 to 12/31/2007)
• Data extracted from the Medicare Patient Safety Monitoring System (MPSMS)
• 4.5% developed at least one new PI during their
hospitalization
• LOS for those who developed a PI was 11.2 days vs
4.8 days for those who did not
• Odds ratio for readmission for those who developed a PI was 1.33 (p<0.001)
8

COSTS FOR STAGE 4 HOSPITAL ACQUIRED PRESSURE INJURY1
• A retrospective chart analysis of patients with stage 4 PI
(19 pts – 11 acute care, 8 community acquired)
• Costs included both treatment and secondary complications
• $127,185 during one hospital stay
• $124,327 for community acquired
1. Brem et al. Am J Surg 2001:200 (4): 473-477.
Stage 4
9

AVERAGE COST ASSOCIATED WITH STAGE 4 PRESSURE INJURY1
Cost Component Average Cost/Episode ($)
Hospital Accommodation 94,915.85
Laboratory 2,519.55
Radiology 4,529.49
Operating Room Services 5,575.50
Pathology 1,826.82
Ancillary Services 11,591.89
Consultation Services 1,991.27
Miscellaneous 700.50
TOTAL COST 127,185.00
1. Brem et al. Am J Surg 2001:200 (4): 473-477.
10
TRANSITIONS OF CARE
Hospital
Acute Post Care
Home
11

CHARACTERISTICS OF “AT RISK” PATIENTS1
• Underlying medical condition(s)
• e.g. diabetes, renal disease, arterial disease
• Bedfast or immobile
• Incontinent
• Lack of sensory perception
• Nutritional compromise
• e.g. malnutrition, dehydration, underweight or overweight
1. Braden Risk Assessment Scale. http://www.bradenscale.com/images/bradenscale.pdf. Accessed 8/9/2016.
12
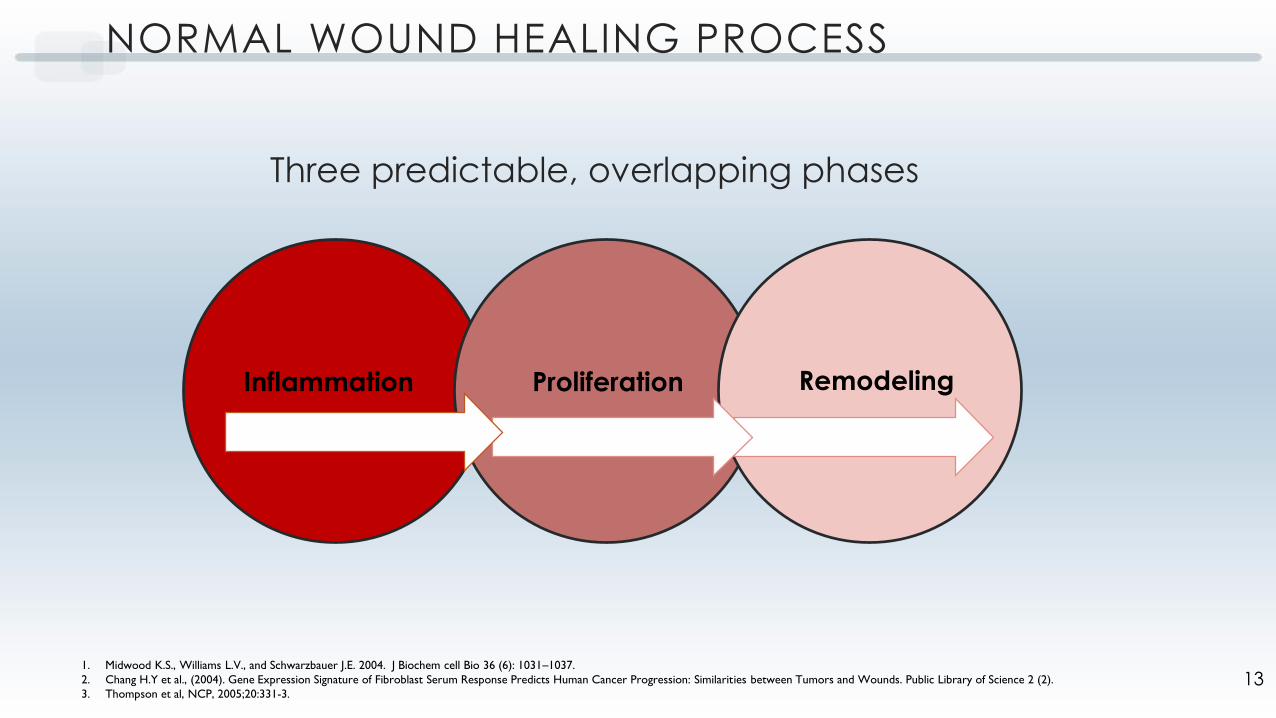
NORMAL WOUND HEALING PROCESS
Three predictable, overlapping phases
1. Midwood K.S., Williams L.V., and Schwarzbauer J.E. 2004. J Biochem cell Bio 36 (6): 1031–1037.
2. Chang H.Y et al., (2004). Gene Expression Signature of Fibroblast Serum Response Predicts Human Cancer Progression: Similarities between Tumors and Wounds. Public Library of Science 2 (2).
3. Thompson et al, NCP, 2005;20:331-3.
Inflammation Proliferation Remodeling
13

THE CHRONIC, NON-HEALING WOUND PROCESS
1. Midwood K.S., Williams L.V., and Schwarzbauer J.E. 2004. J Biochem cell Bio 36 (6): 1031–1037.
2. Chang H.Y et al., (2004). Gene Expression Signature of Fibroblast Serum Response Predicts Human Cancer Progression: Similarities between Tumors and Wounds. Public Library of Science 2 (2).
3. Thompson et al, NCP, 2005;20:331-3.
Wound gets stuck in the inflammatory phase
Inflammation Proliferation Remodeling
14
Intrinsic
• Systemic disease
• Perfusion/oxygenation
• Infection process
• Nutrition/hydration
• Medications
• Age
Extrinsic
• Mobility
• Wound bed environment
• Bacterial burden
• Soft tissue/bone infection
• Devitalized tissue
Nutrition/hydration is one of the most modifiable factor affecting wound healing
FACTORS AFFECTING WOUND HEALING
15

RELATIONSHIP BETWEEN LOSS OF LEAN BODY MASS (LBM) AND WOUNDS1
1. Nutrition, Anabolism, and the Wound Healing Process: An Overview. ePlasty. 2009;9:65-94. Available at http://www.medscape.com/viewarticle/711879. Accessed 7/30/2016.
Wound healing ceases
Risk of new wound development
Risk of wound development
LBM loss of >10%
Wound healing is
Impaired
LBM loss of >20%
16
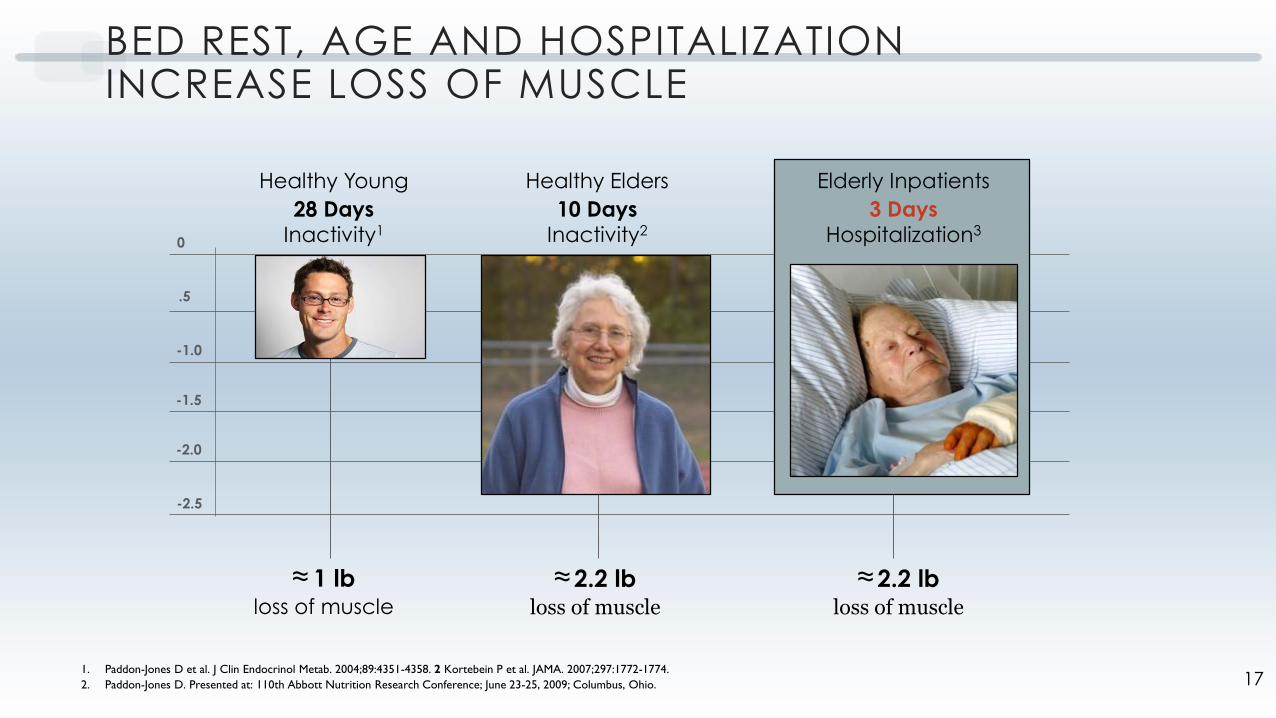
BED REST, AGE AND HOSPITALIZATION INCREASE LOSS OF MUSCLE
≈ 1 lbloss of muscle
≈ 2.2 lbloss of muscle
≈ 2.2 lbloss of muscle
0
.5
-1.0
-2.5
-2.0
-1.5
Healthy Young
28 Days Inactivity1
Healthy Elders
10 Days Inactivity2
1. Paddon-Jones D et al. J Clin Endocrinol Metab. 2004;89:4351-4358. 2 Kortebein P et al. JAMA. 2007;297:1772-1774.
2. Paddon-Jones D. Presented at: 110th Abbott Nutrition Research Conference; June 23-25, 2009; Columbus, Ohio.
Elderly Inpatients
3 Days Hospitalization3
17

NUTRITION FOR PREVENTION AND TREATMENT OF PRESSURE ULCERS1
Selected Recommendations from NPUAP 2014 Guidelines
Nutrition Screening: • Screen nutritional status at admission to a health care setting
Care Planning:• Develop an individualized nutrition care plan
• Follow relevant and evidence-based guidelines on nutrition
Energy Intake: • Provide individualized energy intake.
• Provide 30 to 35 calories/kg body weight
Protein Intake: • Provide adequate protein
• Offer 1.25 to 1.5 grams protein/kg body weight daily for adults
Hydration:
• Provide and encourage adequate daily fluid intake for hydration
Vitamins and Minerals:• Provide/encourage a balanced diet that includes good sources of vitamins and minerals.
• Provide/encourage vitamin and mineral supplements when dietary intake is poor
1. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Emily Haesler (Ed.).
Cambridge Media: Osborne Park, Western Australia; 2014. 18

2014 NPUAP CLINICAL PRACTICE GUIDELINES FOR ENERGY1
“Offer high protein mixed oral nutritional
supplements and/or tube feeding, in addition to
the usual diet, to individuals with nutritional risk and
pressure ulcer risk because of acute and chronic
disease, or following a surgical intervention.”
- Strength of Evidence: A
1. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Emily Haesler (Ed.).
Cambridge Media:Osborne Park, Western Australia; 2014. 19

NUTRITION FOR TREATMENT OF WOUNDS1
Selected Recommendations from NPUAP 2014 Guidelines
Nutrition Screening: • Screen nutritional status at admission to a health care setting
Care Planning:• Develop an individualized nutrition care plan
• Follow relevant and evidence-based guidelines on nutrition
Energy Intake: • Provide individualized energy intake.
• Provide 30 to 35 calories/kg body weight
Protein Intake: • Provide adequate protein
• Offer 1.25 to 1.5 grams protein/kg body weight daily for adults
Hydration:
• Provide and encourage adequate daily fluid intake for hydration
Vitamins and Minerals:• Provide/encourage a balanced diet that includes good sources of vitamins and minerals.
• Provide/encourage vitamin and mineral supplements when dietary intake is poor
1. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Emily Haesler (Ed.).
Cambridge Media:Osborne Park, Western Australia; 2014. 20

2014 NPUAP CLINICAL PRACTICE GUIDELINES FOR TREATMENT OF PRESSURE ULCERS1
1. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Emily Haesler, ed. Osborne Park, Western
Australia: Cambridge Media; 2014.
“When an adult patient with a pressure ulcer
Category/Stage III or IV or multiple pressure ulcers
cannot meet nutritional requirements with
traditional high-calorie and protein supplements,
supplement with high protein, arginine and micronutrients.”
- Strength of Evidence: B
21

INTRODUCING JUVEN®: TARGETED NUTRITIONAL THERAPY
HMB
Glutamine
Arginine
Week 2Juven clinically shownto support wound healing in as little as 2 weeks
Week 0
Week 1
22

B-HYDROXY- B-METHYLBUTYRATE (HMB)1-4
1. Nissen SL, Abumrad NN. J Nutr Biochem. 1997;8:300-11
2. Wilson. Nutr Metab. 2008;5:1
3. Eley HL et al. Am j Physiol Endocrinol Metab. 2008;295:E1409-26
4. Deutz NE et al. Clin Nutr. 2013 ;32:704-12.
• 85 human clinical trials over the past 30 years
• Metabolite of amino acid leucine
• Occurs naturally in human muscle cells
• Found in small amounts in many foods (e.g., avocado, grapefruit, catfish)
• Inhibits intracellular protein degradation in muscle and supports intracellular protein synthesis in muscle by:
• Reducing the inflammatory response
• Protecting muscle from breakdown
• Protecting muscle from stress-related damage
23

EFFECT OF HMB ON MUSCLE MASS AND STRENGTH DURING BED REST1
1. Deutz NE et al. Clin Nutr. 2013 Oct;32(5):704-12
• Objective:
• To investigate the effect of HMB on muscle mass
and strength that occur during 10 d bed rest
• To investigate the effect of HMB (+ exercise) on muscle recovery
following the bed rest period
• Study Design:
• Randomized, double-blinded, controlled study
• Healthy elderly subjects (60 to 77 yrs; Average= 68 yrs)
• Ca-HMB (3 gm/d) versus Control
• 24 subjects (20 women; 4 men)
• Outcomes:
• Decline in muscle mass and function
24

EFFECT OF HMB ON MUSCLE MASS AND STRENGTH DURING BED REST1
1. Deutz NE et al. Clin Nutr. 2013 Oct;32(5):704-12
Change in Total Lean Mass (Female)K
g
25

3 MAJOR FUNCTIONS OF ARGININE IN WOUND HEALING1
1. Patel JJ, Miller KR, Rosenthal C, Rosenthal MD. Nutr Clin Pract. 2016;31(4):438-444.
Stimulant for
Wound Healing• Protein
biosynthesis
• Enhances IGF-1
• Mediates
growth hormone
Nitric Oxide production
for intracellular signaling• Vasodilates blood
vessels
• Increases vascular
permeability
Support immune function• Is directly
bactericidal
• Used by
macrophages and
leukocytes to
destroy pathogens
Arginine is a Key Amino Acid for Metabolic Pathways:
26

ROLE OF GLUTAMINE IN WOUND HEALING
• Glutamine may become depleted in patients with1:
• Critical Illness
• Increased metabolic demand
• Protein catabolism
• Glutamine is the most abundant amino acid
in the body:
• >20% total circulating Amino acids
• >60% intracellular Amino acids
• Benefits of supplemental glutamine related
to wound healing include3:
• Stimulation of collagen synthesis
• Regulation of nitrogen metabolism in catabolic states
• Immune support
• Gut integrity
1. Manpreet S, Mundi MD, Shah M, Hurt RT. Nutr Clin Pract. 2016;;31(4):445-450.
2. Buhaescu I, Izzedine H, Covic A. Ther Drug Monit. 2006;28(5):577-584.
3. Escobar J, Frank JW, Suryawan A, et al. Am J Physiol Endocrinol Metab. 2005;288(5):E914-E921.
GLUTAMINE
27

EFFECT OF HMB, GLUTAMINE, AND ARGININE ON PROTEIN SYNTHESIS AND DEGRADATION
f=p<0.001 from Control degradation
g=p<0.001 from Cachectic degradation
h=p<0.001 from Glut+ Arg degradation, using one-way ANOVA with Tukey-Kramer Multiple Comparison Test (n=6)
a=p<0.01 and b=p<0.001 from Control synthesis
c=p<0.001 from cachectic synthesis
d=p<0.05
e=p<0.01 from HMB, Arg + Glut synthesis using one-way ANOVA with Tukey-Kramer Multiple Comparison Test (n=6)
Source: Abbott on file28

RECENT JUVEN® PUBLICATIONS
1. Moore M et al. Phase Angle, an Alternative Physiological Tool to Assess Wound Treatment in Chronic Nonhealing Wounds. J Am Col Cert Wound Spec 2011;3:2-7.
2. Sipahi S et al., The effect of oral supplementation with a combination of HMB, arginine and glutamine on would healing: a retrospective analysis of diabetic hemodialysis patients. BMC Nephrology 2013;14:8.
3. Jones M et al., Targeted amino acid supplementation in diabetic foot wounds: Pilot data and a review of the literature. Surgical Infections. 2014;15:708-712.
4. Ogura Y et al., Treatment of pressure ulcers in patients with declining renal function using arginine, glutamine and HMB. J Wound Care 2015;24:478-482.
Study Objective Subjects Duration of Intervention with Juven Outcome with Juven
Use of Bioelectrical
Impedance (BIA) to
measure wound healing
11 patients; ave age -
62.5 years; various
wound types
12 weeks or until the
wound closed
64% of patients had closure
of their wounds
46% healed within 12 weeks
Retrospective examination
of the use of Juven in
healing of diabetic foot
wounds
11 diabetic patients;
ave age 66 years4 weeks
63.6% improved wound
depth (p=0.006)
72.7% improved wound
appearance (p=0.001)
Examined the effect of
Juven on wound healing
Examined 9 subjects with
diabetic foot ulcer FOPR
the effect of Juven on
wound healing
2 weeks
Significantly higher
hydroxyproline content
at wound site +67.8% vs
-78.4% (p=0.03)
Examination of the effect of
Juven on healing pressure
ulcers with Juven
2 cases of elderly patients
with renal dysfunction
and pressure ulcer
case 1 = 113 days;
case 2 = 72 days
Juven improved pressure
ulcer healing with no
effect on renal function.
29

Charles, a 62-year-old male, had a 20-year history of diabetes mellitus when he developed a diabetic foot ulcer
with osteomyelitis.
In January, Charles sought medical attention after a crack on the bottom of his foot developed into a lesion.
• Tissue around the lesion was inflamed and necrotic
• Four weeks later, his wound-care team administered a debriding treatment
• Ulcer worsened and Charles developed osteomyelitis
• Charles was treated with IV antibiotics for the next 9 months
JUVEN® CASE STUDY: FOOT ULCER
Wound-care team decided that the ulcer required a second
debridement. After the procedure, wound measured 6.35 cm (L) x 5.08
cm (W) and 2.54 cm (H).
• Physician directed Charles to clean the wound, change the dressing
daily, and take an oral antibiotic (levofloxacin)
• In spite of the debridement, good home care, and adequate
nutrition, the wound continued to worsen
• Consulting physician recommended below-the-knee amputation and
wound-care team recommended hyperbaric oxygen therapy
Overview
August—Before Juven therapy
30

JUVEN® CASE STUDY: FOOT ULCER
Faced with potential amputation and hyperbaric oxygen therapy,
Charles’s doctor suggested that he add 2 packets of Juven to his daily diet.
• Charles mixed 1 packet of Juven with 8–10 oz of water, twice a day
• After 2 weeks, Charles noticed his wound beginning to heal
• Charles continued to take Juven every morning and night for 6 weeks
Wound had reached remodeling phase.
• Charles returned to the wound care center for a follow-up visit
• Ulcer surface had diminished to 3.81 cm (L) x 1.27 cm (W)
October—After 2 weeks of Juven therapy
December—After 14 weeks of Juven therapy
31

NUTRITION THERAPY: A COST-EFFECTIVE INTERVENTION
• Add nutrition interventions to your wound care protocol
• Therapeutic nutrition is a highly cost-effective intervention to help prevent
and treat pressure ulcers
• Brem et al reported cost of
Stage 3/4 PI $127,185.001
• If nutrition therapy costs $5/day,
you could provide nutrition for
25,437 days (69 years) at an equal
cost to treat one pressure injury!
1. Brem et al. Am J Surg 2001:200 (4): 473-477.
CONDITIONCOST FOR
CARE
NUTRITION
COST
(Equivalent)
One Stage
3/4 PI$127,185.00
25,437 days
(69 years)
32

SAMPLE PRESSURE ULCER (PU) PREVENTION AND TREATMENT DECISION TREE WITH STANDING ORDERS
Known Diabetes Mellitus or
hyperglycemia6?
Yes
No
Standing Order7
1. ONS 1- 2 per day8
For example: Patient receives 1
(8oz) Ensure Enlive® or 2 (8oz)
Ensure per day
3. Nutrition Consult
Diagnosis of Diabetes Mellitus or
hyperglycemia present6?
Yes
No Standing Order
No
Standing Order7
1. Diabetes specific meal plan
2. ONS 1-2 per day8
For example: Patient receives 2 (8oz) Glucerna® Shake per day
3. Nutrition Consult
Standing Order for PU
If PU present on admission
or diagnosed, add Juven 2 X day9
Yes
Are one or more facility specific
nutrition screening parameters
present?
1. Low albumin10
2. Low protein intake11
3. Poor dietary Intake12
Yes
No
Standing Order for PU
If PU present on admission
or diagnosed, add Juven 2 X
day9 Reassess
every 24 hours7
No
Are one or more of the following risk
factors present1?
Age (over 50)2
Surgery3
Weight4
Poor skin condition5
Friction/Shear
Oral Nutrition Supplements (ONS) and Juven®
33

1. Risk factors. A simple prediction rule based on 5 hospital patient characteristics may help identify those at increased risk for pressure ulcer development. Age over 50, particularly age over 75, weight on admission of less than 119 lbs. and greater than 209 lbs., abnormal appearance of skin, potential for friction and shear, and surgery in the coming week were all independent predictors of PU development. Formula for calculation of risk can be found in Schoonhoven, 2006.
2. Age. Up to 55% of patients admitted to the hospital are malnourished, particularly older individuals (McWhirter, 1994; Weekes, 1999). Older individuals have a variety of risk factors for malnutrition including polypharmacy, social isolation, depression, medical conditions, poor diet, socioeconomic factors, and dependency. Age over 50 increases risk of developing a PU (Schoonhoven, 2006).
3. Surgery. Surgical patients are at increased risk for PU development. 49% of cardiac surgery patients develop pressure ulcer in the operating room (Frankel, 2007) and 66% of orthopedic surgery patients develop PU (Versluysen, 1986). Even well-nourished patients can experience adverse outcomes if postoperative nutrition is delayed (Huckleberry, 2004). One study showed that even in patients with no risk for PU development before surgery (Braden Pressure Ulcer Risk Assessment Scale), 54.8% were observed to have a Stage I pressure ulcer within 6 days post-op. A study of 161 elderly surgical IUC patients examined risk factors for development of PU. Incidence of PU in this study was 40% and risk factors included: redness of the skin, duration of surgery, fecal incontinence and diarrhea, use of steroids and decreased total protein and albumin 1 DAY POST-OP (Versluvsen, 1986).
4. Weight. Underweight and low BMI are known risk factors for PU development. However, overweight creates risk for PU as well. Schoonhoven et al found that patients who weighed over 209 lbs had 2.2 x the risk compared to those who weighed between and 209 lbs. Those patients who weighed 119 lbs or less had 1.3 x the risk as those who weighed between 119 and 209 lbs. Underweight patients are at risk due to bony prominences placing stress on the skin. The condition is under-recognized and under-treated and can lead to decreased strength and mobility and diminished organ function. Overweight patients are at risk due to extra tissue causing stress/friction of the skin. Malnutrition under-recognized in this group and they have a greater risk for hyperglycemia, reduced circulation, and inability to reposition. Braunschweig et al found that upon admission, patients with severe malnutrition (assessed by SGA) were on the high end of normal weight (mean BMI 23.5) and at discharge, patients with severe malnutrition were overweight (mean BMI 25.7).
5. Skin condition. Characteristics include dry (particularly dry sacral skin) or unhealthy, thin skin. The skin is largest organ in the body and plays important role in preserving fluid balance, sensation, and body temperature (Scoonhoven, 2006).
6. Diabetes Mellitus/hyperglycemia. Diabetes increases risk of PU by 60% (Resnick, 2008). 4.2 million hospitalizations occur annually among people with diabetes, 1.5 million hospitalizations occur with significant hyperglycemia and no history of diabetes. Nutritional factors that increase risk include dehydration (can compromise skin integrity) and PEM (decreases collagen synthesis increases loss of lean body mass). Hyperglycemia causes tissue ischemia (decreased microcirculatory function) increasing the risk of poor skin condition (Fromy, 2005).
7. Standing orders. An immediate practice change may be necessary to efficiently provide supplemental nutrition for patients to reduce development of PU. In a pilot for the “SKIN” PU prevention program at Ascension Health, researchers found that 87% of the time a nutritional consult had been ordered for patients with PU, but were carried out only 35% of the time. This lead to medical-staff-approved standing orders for dietitians. Due to this comprehensive program, PU incidence was reduced to >1% with no new Stage III or IV PU (Gibbons, 2006).
8. Oral nutrition supplements (ONS). In a randomized, prospective multi-center trial of 672 acute care, older patients, 200 kcal supplements 2x day were shown to decrease the incidence of PU development (Bourdel-Marchesson, 2000) A meta-analysis of 15 studies of elderly, post-surgical, hospitalized patients showed that ONS of 250-500 kcal/day significantly reduced risk of developing pressure ulcer by 25% compared to routine care (Stratton, 2005). The ESPEN 2006 guidelines for geriatrics give ONS an “A” rating, stating that ONS, particularly high protein ONS, can reduce the risk of developing pressure ulcers (Vulkert, 2006).
9. Juven. Juven has been clinically shown to help build lean body mass and support healing (May, 2002; Clark, 2000; Williams, 2002)
10. Albumin. Interstitial edema due to low albumin can decrease nutrient passage to damaged tissue (Wells, 1994). 75% of patients with serum albumin below 3.5 md/dl develop pressure ulcers (Holmes, 1987). Even patients admitted to a hospital who screen as adequately nourished can experience declines in nutritional status during their stay. Braunschweig et al found that 38% of patients admitted with normal nutrition status (assessed with SGA) declined in nutritional status.
11. Low protein intake. Protein intake < 93% of RDA is associated with PU development whereas protein intake of >119% is associated with no PU (Bergstrom,1992).
12. Poor dietary intake. Defined as persistently poor appetite, meals being held, or a prescribed diet of less than 1100 kcal or 50 g protein/day, shown to predict PU development (Berlowitz, 1989)
Pressure Ulcer (PU) Prevention and Treatment Decision
Tree for Standing Orders Support and References
34

TAKE ACTION
• Revisit nutrition care planning for
prevention and treatment of wounds
including:
• Nutrition screening
• Aggressive nutrition therapy
• Nutrition education at discharge
• Implement a treatment protocol for
wounds
• Early nutrition intervention
• Standing orders
• Discharge recommendations
35

DISCUSSION AND QUESTIONS
The team approach to treatment:• We must all work together
to communicate
the nutrition message
161760/September 2016 36