have the evaluation and treatment of acute appendicitis changed with new technology?
TRANSCRIPT

ABDOMINAL EMERGENCIES 0039-6109/97 $0.00 + .20
HAVE THE EVALUATION AND TREATMENT OF ACUTE
APPENDICITIS CHANGED WITH NEW TECHNOLOGY?
Robert T. Wilcox, MD, and L. William Traverso, MD
INTRODUCTION: HAS TECHNOLOGY AIDED THE EXPERIENCED CLINICIAN?
Has new technology changed how we approach and treat a patient with possible appendicitis? Certainly we assume that newer technology connotes better outcomes, but have the results of diagnosis and treat- ment followed this assumption? New technology could lower the rate of delayed diagnosis, thereby providing decreased morbidity. De- pending on the expense of the new technology, the costs might also decrease. The goal of surgical treatment is removal of an inflamed appendix prior to perforation, with a minimal number of negative ap- pendectomies. This goal assumes that perforation is due to prolonging the interval between onset of symptoms and surgical treatment. It also assumes that perforation means increased morbidity and length of stay. The degree to which the diagnosis of appendicitis is delayed may be due to patient-controlled versus physician-controlled factors and remains a debated issue.58, 64 In addition, perforation may occur sooner in young or elderly patients.
Inherent in the evaluation of new technology applied to appendicitis is how new tests like ultrasonography or laparoscopy can avoid a misdiagnosis (false negative or false positive) or provide an earlier
From the Department of General Surgery, Virginia Mason Medical Center, Seattle, Wash- ington
SURGICAL CLINICS OF NORTH AMERICA
VOLUME 77 * NUMBER 6 * DECEMBER 1997 1355
1356 WILCOX & TRAVERSO
disposition of appendicitis (true positive). Of course, all of this benefit should be acquired for a reasonable cost. A population-based observa- tional study during the 1980s from Ontario, Canada, showed that perfo- ration rates increased as the rate of histologically confirmed acute appen- dicitis increased.hs Why? We assume that new tests can detect an increasing number of true-positive cases. This outcome can be accom- plished by avoiding a test that does not ”undercall” a disease and yield a false-negative result. With appendicitis, false-negative tests may result in delayed diagnosis and an increased perforation rate, particularly in the very young or very old. New tests have to be carefully evaluated because they are intended to assist and not replace a surgeon’s judgment and clinical examination. The latter helps to moderate the hazard of a highly sensitive test that avoids undercall but has the potential for “overcall.” The result of overcall is the removal of more normal appendi- ces at operation. Clearly a balance of acceptable rates for normal appen- dices and perforation may be changed for the better by new technology. The purpose of this article is to estimate these changes. It is not surpris- ing that modern studies conclude that the clinical examination by an experienced surgeon is most important.
Studies have attempted to address the issue of decreasing the perfo- ration and complication rate while subjecting a minimum number of patients to unnecessary surgery. Wen and Naylor68 hypothesized that the rate of histologically confirmed appendicitis cases (diagnostic accuracy) would be increased with no associated increase in morbidity with the use of ”modern” 1980s imaging, broad-spectrum antibiotics, and the then-limited use of diagnostic laparoscopy. During the decade of 1981 to 1991 and using 27,189 cases of acute appendicitis as the admitting diagnosis, the diagnostic accuracy rate in Ontario increased in female patients from 71.7% in 1981 to 75.3% in 1991 (statistically significant), with no increased accuracy rate in male patients. Other studies have focused on confirming the more important historical and physical exami- nation findings with subsequent diagnostic scoring systems, evaluating the usefulness of laboratory and imaging studies, and the use of diagnos- tic laparoscopy. Although none of these modalities has been shown to be effective to the exclusion of the careful examination and clinical acumen of an experienced surgeon, the wide range of diagnostic accu- racy between institutions (rates in Ontario ranged from 50% to 96.7Y0)~* warrants a review of more recent studies of useful adjuncts to the surgeon’s clinical impression, particularly in high-risk patients and those with equivocal clinical presentation.
The introduction of laparoscopic surgery has not only had an impact on the diagnosis of appendicitis, but it is also the major change in the 1990s with regard to treatment. Recent studies have focused on whether or not laparoscopic appendectomy should be the procedure of choice for acute appendicitis. Other issues in the treatment of acute appendicitis include nonoperative treatment, the management of complicated appen- dicitis, and earlier discharge after treatment of appendicitis.

HAVE THE EVALUATION AND TREATMENT OF ACUTE APPENDICITIS CHANGED? 1357
EVALUATION
Factors Leading to Delay in Diagnosis
Central to the question of whether new technology will change the approach to acute appendicitis is whether it produces improved out- comes. Many studies have found that perforation rates correlate with time from onset of symptoms to treatment. Delays occurring due to unclear diagnosis could be shortened by using technologic advances and lead to lower perforation rates. If delay is due to late patient presenta- tion, perforation rates could be improved by patient education rather than improved diagnostic tools. Additionally, delays due to lack of consideration of appendicitis in the differential diagnosis may be im- proved by either health care provider education or improved diagnos- tic testing.
Several studies have questioned the cause for delay in treatment of acute appendicitis, with varied results. Causes of delay include late initial contact of health care by the patient, delayed request for surgical consultation, or delay between surgical referral and operative treatment. Concern regarding the latter two possibilities has increased with in- creased numbers of patients enrolled in "managed care" health plans. Concern has focused on possible delay associated with the "gate-keeper" model, disincentives for early surgical referral, and decreased motivation for early surgical intervention by surgeons. These concerns have been addressed by several studies that have been unable to demonstrate a clear association between health maintenance organizations and in- creased perforation rate.2, &
Cause of the delayed diagnosis was addressed by Von Titte and colleagues, who studied 40 patients with known delay of 72 hours or greater. They attributed delay to physician-controlled factors in 62.5% of their cases. Perforation was noted in 90%, and major complications were noted in 60% of patients with delays in their diagnosis." Con- versely, a study by Temple et a158 found that patients with perforation waited an average of 2.5 times longer before first presentation to medical care. They also found that patients with perforated appendicitis were treated faster after presentation than patients without perforation, which was attributable to shorter evaluation times by surgeons. They conclude that rupture is due to factors controlled primarily by the patient and should therefore not be used as a quality assurance meas~rement .~~ Another study reported equal responsibility of physicians and patients for delay in treatment.I8 The conflicting nature of these reports leads to the conclusion that the problem of delayed diagnosis should continue to be addressed with patient education, education of health care provid- ers who have the initial patient contact, and continuing education of surgeons regarding pertinent features of appendicitis. This should be accompanied by studies evaluating where the delay is occurring in various patient populations and then appropriate interventions based on identified deficiencies.

1358 WILCOX & TRAVERSO
History/Physical Examination
Despite advances in other diagnostic modalities, appendicitis re- mains a diagnosis based primarily on history and physical examination. Equivocal cases should continue to be followed by repeated examination by an experienced individual, even in the presence of negative imaging and laboratory studies. A recent meta-analysis of studies reporting the clinical usefulness of various signs and symptoms in adults with appen- dicitis underscored the importance of right lower quadrant pain, rigidity, and pain migration from the periumbilical area to the right lower quad- rant. Appendicitis was noted to be less likely with a history of previous similar pain, absence of right lower quadrant pain, and absence of classic pain migration. The presence of vomiting before pain made the diagnosis of appendicitis unlikely. Notably, the absence of anorexia, nausea, and vomiting had little impact on the likelihood of appendici- tis.66 Rebound tenderness varied too widely among studies to accurately assess the effect of a positive test.66
Although knowledge of classic findings is important, patients most benefitted by surgical evaluation and possible further imaging are those who lack a classic picture of appendicitis. The groups most likely to present with an atypical history include the same groups that are at the highest risk for perforation and subsequent morbidity and mortality.21, 28
The extremes of age have been shown not only to have higher perfora- tion rates but also to perforate earlier than other age groups.28, One should have a high index of suspicion with few clinical signs in these groups, and both early surgical consultation and a thorough diagnostic evaluation should be advocated.
In a study evaluating clinical assessment alone in diagnosing appen- dicitis, accuracy ranged from 83% to 97%, with values correlating with the surgeon’s experien~e.~~ In comparing these results with ultrasonogra- phy, the authors concluded that clinical examination remains the pri- mary modality for diagnosis of acute appendicitis. Studies comparing the surgeon’s clinical impression with laboratory or imaging studies have reportedly shown superiority of the latter.I9, 65 These studies were flawed in that they compared the surgeon’s initial impression with the laboratory or imaging study, with the decision to operate being based upon repeated physical examination. In other words, in all cases the physician’s judgment was ultimately 100% sensitive. The study was a better description of the utility of these tests if the pretest probability of appendicitis was high enough to warrant admission and repeated physi- cal examination.
Computer Models Aiding in Diagnosis
The classic clinical signs listed above, in addition to laboratory studies that are likely to be abnormal in acute appendicitis, have led to both clinical and computer-aided algorithms as diagnostic aids. Weighted
HAVE THE EVALUATION AND TREATMENT OF ACUTE APPENDICITIS CHANGED? 1359
scores are assigned based upon clinical features that add to or detract from the likelihood of appendicitis. The goal is to separate patients who have a high likelihood of appendicitis and in whom early surgical treatment is warranted from those who may be safely observed or discharged. These algorithms focus clinicians on findings that have historically been important features. We urge caution with this kind of approach. For example, a score is only as good as the data used to arrive at the score, and the data are influenced by clinical judgment and experience (whether or not a physical finding exists). Secondly, scores based on large numbers of features common to most cases of appendici- tis do not take into account subtle findings that may be discerned by the experienced surgeon. Algorithms may neglect subtle but pertinent features of a given case. Lastly, those patients who are at the highest risk of complications of a perforated appendix, the old and the very young, have a decreased classic response to appendicitis and thus may score lower.12, 45
Ohmann et a140 evaluated the performance of 10 different diagnostic scoring systems for acute appendicitis. The scoring systems were applied to a data base of 1254 patients to compare the patient’s scoring results with the published data. The authors believed that an adequate scoring system should fulfill the following criteria: a negative appendectomy rate of less than 15%, a perforated appendix rate of less than 35%, a missed perforation rate of less than 15%, and a missed appendicitis rate of less than 5%. The Alvarado score3 was the only scoring system that fulfilled all four of these criteria.40 The Alvarado score was assessed prospectively as to accuracy in preoperative diagnosis of acute appendi- citis in a separate study. A high score was found to be an easy and satisfactory aid to early diagnosis of acute appendicitis in children and men but had a high false-positive rate in women.26
Although these diagnostic scores focus attention on pertinent clini- cal features, they have not been shown to be as accurate as an experi- enced surgeon’s clinical impression. They should be reserved for nonsur- geons and possibly to describe groups of patients in regard to their clinical features in studies. Each patient should be individually evaluated and pertinent findings on examination given credence regardless of a patient’s overall diagnostic score. A high diagnostic score should not be ignored, but problems with these scores are more likely to come from patients with low scores and subtle signs of disease. The utility of these tests needs to be evaluated on those patients at increased risk of complications and those likely to present with subtle signs-the young and the old.
Laboratory Studies
Adjunctive laboratory studies have been found to be useful in the diagnosis of acute appendicitis. An easily obtainable, inexpensive laboratory study with rapid results and adequate sensitivity would
1360 WILCOX & TRAVERSO
obviate the need for imaging studies to rule out the diagnosis of appen- dicitis. Laboratory studies demonstrated to be helpful thus far represent nonspecific acute phase reactants elevated secondary to acute inflamma- tion. C-reactive protein (CRP), total white blood cell (WBC) count, and differential have been evaluated. Gurleyik et all9 compared serum CRP measurements with the surgeon's clinical impression in a prospective study of 108 patients suspected of having appendicitis on clinical grounds. Ninety patients were confirmed to have appendicitis histologi- cally, and a normal appendix was found in 18. The false-negative rate of CRP was 3%, and the false-positive rate was 11%. Sensitivity was found to be 93.59'0, specificity 80%, and accuracy 91%. C-reactive protein levels were recommended to be used routinely. Serial analysis of CRP and WBC count was also found to be useful. With appendicitis, CRP values have been found to continue to rise, whereas WBC values de- creased on repeated testing.I4
Caldwell and Watsons studied the use of peritoneal aspiration cytol- ogy as a diagnostic aid. The value of a positive test was found to be 95%, and a negative test had a predictive value of 94%. It was reported to be a useful diagnostic test. Although helpful, it is also invasive and carries an undefined risk. The use of these tests has been suggested as part of an algorithm for the diagnosis of acute appendicitis without any imaging study, although no report of diagnostic accuracy with this algorithm was reported.8
imaging
The goal of an imaging study as a diagnostic aid in acute appendici- tis should be to differentiate presence of disease in those with inflamma- tion, without perforation, and with equivocal clinical findings. In addi- tion, it should be quick, relatively noninvasive, and accurate in those groups at highest risk of complication if perforation should occur. It should be free of interobserver variability, easily reproducible, and easily obtained at any hour. Ideally, imaging should reveal inflammation of the appendix when it is located at an anatomically troublesome site to evaluate via clinical examination.
Ultrasonography
Ultrasonography has changed the approach to the diagnosis of acute appendicitis, as evidenced by multiple studies performed over the past 12 years and continued debate regarding its usefulness. Although studies have reported sensitivity and specificity of this imaging mod- ality, as well as comparison with the surgeon's diagnostic impression, the utility of ultrasonography in changing outcomes of acute appendici- tis has not been proven. Opinion varies from recommending this study in all patients with suspicion of acute appendicitis to questioning its use because of the added cost without improved clinical outcome.15, 63 Initial
HAVE THE EVALUATION AND TREATMENT OF ACUTE APPENDICITIS CHANGED? 1361
enthusiasm and perhaps overuse will, it is hoped, change to a more appropriate and clinically useful outcome affecting application of this adjunctive test.
Orr et a142 reviewed the usefulness of ultrasonography using meta- analysis of English language articles published from 1986 to 1994. An overall sensitivity of 84.7% and specificity of 92.1% were reported. More importantly, the study demonstrated the impact of pretest probability of disease upon the accuracy and usefulness of a test. In a group with high prevalence of appendicitis (80%-usually operated upon based on clinical grounds), a negative test result had a negative predictive value of only 59.5%; conversely, in a group with low prevalence of appendicitis (2%-usually discharged home), a positive test had a positive predictive value of only 19.5%. A balanced ”test performance accuracy” was dem- onstrated only in those patients with an intermediate prevalence of appendicitis (40%-usually observed in the hospital). They concluded that ultrasonography is most useful in those with an intermediate proba- bility of disease and should be avoided in patients with high or low likelihood of disease because they are associated with high false-negative and false-positive rates, respecti~ely.~~
Knowing that a diagnostic test has a given sensitivity or specificity is not as important as determining whether the test adds new informa- tion to the clinical picture. In other words, does ultrasonography tell us anything we don’t already know? How does it compare with the clinical evaluation of the surgeon? Answers to these questions have been varied. One study comparing clinical examination and ultrasonography found examination superior but noted that ultrasonography was a useful adjunct in unclear cases.25 Another study compared the surgeon’s initial clinical impression with ultrasonography, finding ultrasonography supe- r i ~ r . ~ ~ It should be noted that the value of both of these modalities is influenced by experience; this study compared the opinions of ultra- sound-dedicated radiology attending physicians with the clinical impres- sions of senior general surgery residents or general surgery staff.25, 63
Additionally, the initial impression was arrived at using the Alvarado scoring ~ys t em.~ The study best represents a comparison of expert ultra- sound examination with the Alvarado score. In concluding, the authors state: “Accuracy of ultrasonography in the diagnosis of appendicitis was statistically superior (p < .OOOl) to that of the surgeon’s clinical impres- sion. However, 24% of the patients with normal ultrasound findings were ultimately found to have appendicitis at operation, emphasizing the point that ultrasonography cannot be relied on to the exclusion of the surgeon’s careful and repeated e~aluat ion.”~~
Comparison of the surgeon’s clinical impression with ultrasound findings should not lead one to consider whether surgical consultation or an ultrasonogram should be obtained; rather, it should lead to early surgical referral and a surgeon’s decision based upon clinical grounds if ultrasonography is warranted. Likelihood of appendicitis in practice carries degrees of certainty for the examiner. Are features that lead to difficult ultrasound diagnosis independent of those that make the clinical
1362 WILCOX & TRAVERSO
diagnosis difficult (i.e., as in children)? Ramachandran et a147 compared the use of ultrasonography in two groups of children. The first group consisted of all children with the possible diagnosis of appendicitis; the second group had ultrasonography only when the diagnosis was equivocal. Sensitivity (88% and 92%, respectively) and specificity (96% and 97%, respectively) were equivalent in the two groups. This study showed that ultrasonography is a useful adjunct when the clinical find- ings are equivocal.
Few studies have addressed whether the increasing use of ultraso- nography as a diagnostic tool has resulted in improved outcomes. Possi- ble benefits of ultrasonography include decreased percentage of negative operations and decreased length of time between presentation and surgi- cal treatment in patients who would otherwise have been observed with serial examinations. In women of childbearing age, ultrasonography may be invaluable in defining presence or absence of pelvic pathology leading to abdominal pain as well as preventing complications of infertil- ity if diagnosis could occur prior to appendiceal perforation. Studies to date have not shown remarkable improvements in these areas with the use of ultrasonography. One study reported a decreased laparotomy rate of only 5%, which they believed was due to the limited influence of negative ultrasound findings on the decision of whether or not to operate.63
Ford and colleague^'^ addressed the question of improved outcome with increased use of ultrasonography by comparing a ”pre-ultrasound year” of 1986 with 1989, when ultrasonography was increasingly used. During this period, the group of surgeons remained the same, patient groups were reportedly not statistically different, and diagnostic accu- racy rates significantly decreased (from 85.6% to 77.0%). Additionally, there was no difference in complications, perforation rate, or hospital length of stay. Of note, 66% of ultrasonograms were ordered by nonsur- geons before consultation. A total of 325 ultrasonograms were per- formed, with 252 patients undergoing appendectomy, of whom 118 had received ultrasound studies. They conclude that ultrasonography increases costs without improving outcome. They also comment that surgical consultation costs less than ultrasonography at their hospital; therefore, it would be cost effective to obtain surgical consultation and allow the surgeon to decide if ultrasonography is ~ar ran ted . ’~
Improvements in the diagnosis or exclusion of appendicitis using ultrasonography are continuing, which makes a definitive answer re- garding its usefulness difficult. Several recent improvements include color Doppler ultrasonography to detect hyperemia in the wall of the appendix32 and increased visualization of the normal appendix.51 Pre- viously, a nonvisualized appendix was considered a negative examina- tion, which may have led to lower negative predictive values.51 Demon- stration of a normal appendix with lack of hyperemia in the appendiceal walls may lead to a high enough negative predictive value that unneces- sary laparotomy could be avoided. Additionally, availability of ultraso-

HAVE THE EVALUATION AND TREATMENT OF ACUTE APPENDICITIS CHANGED? 1363
nographers may be less of an issue in the future as surgeons become increasingly adept at ultrasonography of the abd~men.~, 71
Ultrasonography has changed clinical practice over the past decade and will likely continue to be a valued tool for clinically equivocal cases in the future. It will be most helpful in those groups in which early diagnosis and operative management are essential to reduce complica- tions-the very young and the older patient. It will also be of assistance in ruling out pelvic disease in women of childbearing age. To avoid unnecessary costs and delay, the decision regarding ultrasonography should be left to the surgical consultant.
Computed Tomography
Computed tomography (CT) has been advocated as the imaging test of choice in diagnosing acute appendicitis. In a study comparing CT with ultrasonography, Balthazar and colleagues5 conclude that CT is the test of choice except in children or women in their first trimester of pregnancy. This study showed improved evaluation of the extent of inflammation, improved diagnosis of alternate intra-abdominal disease, and a higher rate of demonstration of a normal appendix with CT scan. Higher sensitivity, accuracy, and negative predictive value were seen with CT scan. However, CT scan is associated with greater cost, expo- sure to ionizing radiation, and exposure to contrast agents. Several studies have used unenhanced helical CT to avoid both delay and need for patients to be exposed to contrast agents. These studies have revealed similar results to those studies evaluating CT scans with intravenous contrast.31, 33
The approach to evaluating patients with acute appendicitis via diagnostic imaging may change when improved outcomes have been demonstrated. As mentioned previously, this has not been clearly dem- onstrated. To evaluate this question, two time periods were compared- one before and one after widespread use of these techniques. Although the second group had a statistically greater number of CT, ultrasound, barium enema, and laparoscopic studies performed, there was no differ- ence in perforation rate, negative appendectomy rate, time between presentation and operation, or length of ho~pitalization.~~ Further study needs to be performed to identify those patients in whom preoperative imaging will improve outcome.
Diagnostic Laparoscopy
Several authors have advocated the use of laparoscopy as a diagnos- tic modality in the evaluation of a patient suspected of having acute appendicitis.lO, 41 Although directly visualizing the appendix might be a valid method of determining acute inflammation, patients with a normal appendix would be exposed to the risks and costs of general anesthesia and diagnostic laparoscopy. A note of caution is derived from the study
1364 WILCOX & TRAVERSO
of Grunewald and Keating,I7 who showed histologic inflammation in appendices that appeared uninflamed to the surgeon.
Diagnostic laparoscopy should be viewed as an invasive procedure requiring general anesthesia and having risks similar to appendectomy. For this reason it is not preferred as a diagnostic tool. During ”diagnostic laparoscopy” for suspected acute appendicitis, if no other pathology is identified, the appendix should be removed regardless of gross appear- a n ~ e . ~ This both rules out inflammation by pathologic examination and makes the diagnosis of acute appendicitis less likely if the patient com- plains of similar pain in the future.
TREATMENT
Open Versus Laparoscopic Approach
The most recent technology applied to the evaluation and treatment of appendicitis has been the use of laparoscopy. As laparoscopic chole- cystectomy has become the standard of care, surgeons have applied laparoscopy to a wide variety of surgical diseases. Debate regarding the usefulness of laparoscopic appendectomy continues. Supporters of the laparoscopic approach report decreased wound infection rate, less post- operative pain, decreased hospital stay, better cosmetic result, and sooner return to normal activity. Greater visualization of the entire abdominal cavity to identify alternative pathology is also a reported benefit in cases of a normal appendix at the time of operation. Those who favor the open approach point to studies showing no difference in length of hospital stay, complications, duration of postoperative pain, or return to normal activity in the face of greater costs and operative time associated with the laparoscopic approach.
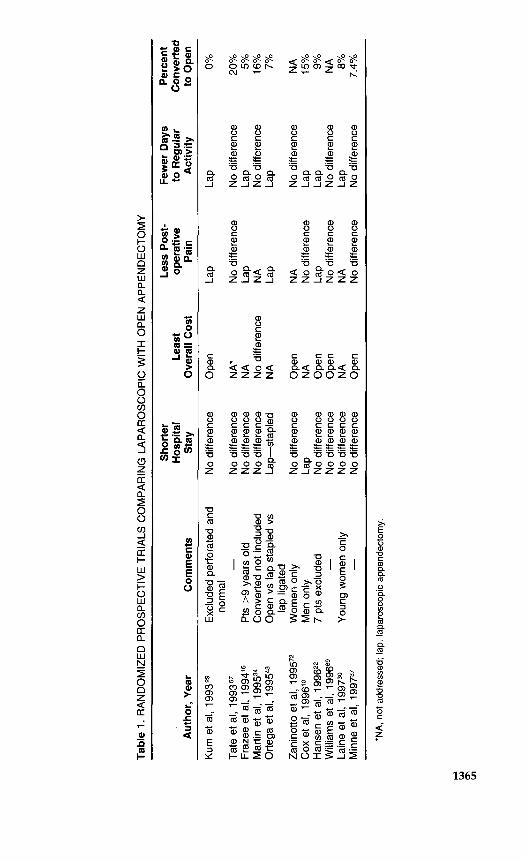
Table 1 shows results of recent prospective randomized trials com- paring laparoscopic and open appendectomy. These studies vary in their support of the laparoscopic approach, but several generalizations may be made. Although shorter hospital stay has been a reported benefit, individuals with open appendectomies are being discharged earlier, leading to a decreased benefit of the laparoscopic approach. Hospital length of stay appears to be related largely to pathologic stage of disease rather than to operative approach. Secondly, only one study has found similar costs for the two procedure^.^^ Most studies conclude that laparo- scopic technique leads to significantly higher total cost. The area in which laparoscopic technique appears to have the greatest possible benefit is decreased postoperative pain and more rapid return to regular activity. Duration of postoperative narcotic consumption was generally used as a guide for postoperative pain. Note that return to regular activity can be influenced by many patient or doctor variables. The most recent study revealed no difference in time to return to normal
In response to the increased cost and operative time with little improvement in outcome, proponents of the laparoscopic approach
Tabl
e 1.
RA
ND
OM
IZE
D P
RO
SP
EC
TIV
E T
RIA
LS C
OM
PA
RIN
G L
AP
AR
OS
CO
PIC
WIT
H O
PE
N A
PP
EN
DE
CTO
MY
_
__
__
~
__
__
__
__
_
__
__
_
Sho
rter
Le
ss P
ost-
Fe
wer
Day
s P
erce
nt
Ho
spit
al
Leas
t op
erat
ive
to R
egul
ar
Con
vert
ed
to O
pen
Act
ivity
A
utho
r, Y
ear
Com
men
ts
Sta
y O
vera
ll C
ost
Pai
n
Kum
et a
l, 19
9329
Tate
et a
l, 19
9357
Fr
azee
et a
l, 19
9416
M
artin
et a
l, 19
9534
O
rtega
et a
l, 19
9543
Zani
notto
et a
l, 1 9
9572
C
ox e
t al,
1996
lO
Han
sen
et a
l, 1 9
9622
W
illia
ms
et a
l, 19
9669
La
ine
et a
l, 19
9730
M
ime
et a
l, 19
9737
Exc
lude
d pe
rfora
ted
and
Pts
>9
year
s ol
d C
onve
rted
not i
nclu
ded
Ope
n vs
lap
stap
led
vs
lap
ligat
ed
Wom
en o
nly
Men
onl
y 7
pts
excl
uded
norm
al -
You
ng w
omen
onl
y -
No
diffe
renc
e
No
diffe
renc
e N
o di
ffere
nce
No
diffe
renc
e La
p-st
aple
d
No
diffe
renc
e
No
diffe
renc
e N
o di
ffere
nce
No
diffe
renc
e N
o di
ffere
nce
Lap
Ope
n
NA
* N
A
No
diffe
rei
NA
Ope
n N
A
Ope
n O
pen
NA
O
pen
Lap
Lap
Lap
NA
N
o di
ffere
nce
Lap
No
diffe
renc
e N
A
No
diffe
renc
e
No
diffe
renc
e
ice
N
A
Lap
No
diffe
renc
e La
p N
o di
ffere
nce
Lap
Lap
Lap
No
diffe
renc
e La
p N
o di
ffere
nce
No
diffe
renc
e
0%
20% 5%
16%
7%
NA
15
%
9%
NA
8%
7.4%
"A,
not a
ddre
ssed
; lap
, lap
aros
copi
c ap
pend
ecto
my.
Y

1366 WlLCOX & TRAVERSO
point to other reported advantages. Several authors have found de- creased wound infection rates with the laparoscopic approach.22, 29, 43, 50
This is thought to be related to the fact that the inflamed appendix does not contact the wound edges as it is removed from the trocar site or the specimen is retrieved in a sterile container. Additionally, the laparo- scopic approach is associated with improved satisfaction with cosmetic
Finally, the laparoscopic approach has been associated with a greater ability to establish and possibly treat alternative disease- particularly in women of childbearing age.30, 72
Application of the laparoscopic technique to appendectomy should not be considered the ”gold standard.” The postoperative course, mor- bidity, and decreased cost continue to support open appendectomy in the majority of cases. Application of the laparoscopic technique is likely to be of benefit in some patient populations. Women of childbearing age, who, as discussed previously, are more likely to have a normal appendix at the time of operation (up to 40%), benefit from diagnosis and possibly ability to treat pelvic disease that may account for their symptoms. Additionally, the benefits of the laparoscopic approach seen with obese patients undergoing cholecystectomy likely apply to laparo- scopic appende~tomy.~~ Obese individuals who would require larger skin incisions during open appendectomy may benefit from the laparo- scopic approach.24
The Periappendiceal Mass
Appendiceal masses include both phlegmon and periappendiceal abscess. Initial nonoperative treatment of appendiceal phlegmon with antibiotics, with or without drainage for periappendiceal abscess, has been accepted treatment.39 Historically, nonoperative initial management is followed by interval appendectomy to eliminate the possibility of recurrence and rule out other-possibly malignant-causes of a periap- pendiceal mass.39, 46 Recently, alternative suggestions in the management of periappendiceal masses have ranged from early aggressive resection (at the time of initial pre~entation)~~ to conservative initial treatment with interval appendectomy only if symptoms recur.’,
Proponents of aggressive resection at the time of initial presentation argue that primary repair and anastomosis are effective and safe, the need for interval appendectomy with associated risk is eliminated, and total hospital stay and complications associated with conservative treat- ment are likely to be decrea~ed .~~ Those who favor conservative treat- ment followed by interval appendectomy with recurrent symptoms state that a small percentage (0% to 20%) of patients have recurrence, sparing the majority of patients an unnecessary procedure.’, The optimal treat- ment of the appendiceal mass remains unclear, with lack of randomized studies providing conclusive evidence. Cecectomy with primary anasto- mosis is a reasonable approach in those patients who have intra-abdomi- nal masses palpated after they have been ane~thetized.~~ Periappendiceal

HAVE THE EVALUATION AND TREATMENT OF ACUTE APPENDICITIS CHANGED? 1367
masses identified prior to this should be managed according to the surgeon’s judgment. If nonoperative management is decided upon, fur- ther evaluation should occur based upon the patient’s age to rule out other causes of right lower quadrant mass.
Nonoperative Management
Nonoperative management has been suggested as a possibility in patients with acute appendicitis. The treatment of complicated appendi- citis nonoperatively and the suggestion that subsequent interval appen- dectomy is unnecessary have led to the suggestion by some authors that acute appendicitis (not complicated by abscess or phlegmon) may be treated by antibiotics alone. A randomized controlled trial of appendec- tomy versus antibiotic therapy alone for acute appendicitis was reported in 1995 by Eriksson and GranstromI3 to address this question. Forty patients with abdominal pain of less than 72 hours were randomized to antibiotics alone or to surgery. Twenty patients were randomized to intravenous antibiotics for 2 days, followed by an 8-day course of oral antibiotics; the remaining 20 patients were randomized to surgery. In the antibiotic group, 40% required appendectomy (one patient with perforated appendix during treatment, seven required appendectomy within 1 year). In the surgery group, a 15% negative appendix rate was noted. Although these authors conclude that ”conservative treatment” with antibiotics could be justified by the results of this study, the 40% of patients failing antibiotic therapy argue that surgical treatment is the truly ”conservative” management of this disease.
SUMMARY
The evaluation and treatment of acute appendicitis remain essen- tially unchanged for the majority of individuals who present with this disease. Although advancements have been made in laboratory analysis as well as imaging via ultrasonography and CT, nothing can replace careful evaluation by an experienced surgeon. Appendicitis remains a diagnosis based primarily on history and physical examination, with further studies being useful adjuncts in atypical cases-more likely to occur in the very young or very old and most cost effective when ordered by the surgical consultant. Improvement in outcomes has not been demonstrated with routine use of ”new technology.”
The treatment of acute appendicitis continues to be early surgical intervention. Although laparoscopic appendectomy may offer advan- tages in women of childbearing age and in obese individuals, its routine use is not indicated based upon current reports in the literature. Debate continues regarding the optimal treatment of the periappendiceal mass. Further clinical research regarding early operation compared with intra- venous antibiotics with or without drainage, as well as comparison of

1368 WILCOX & TRAVERSO
outcomes with or without interval appendectomy, needs to be per- formed.
With continued research and definition of populations likely to benefit from advances in technology, a more focused application will be possible. This will lead to improved outcomes and decreased overall cost. The issue of delay in treatment, a major determinant of morbidity associated with appendicitis, warrants further evaluation and should be addressed on a population-specific basis. Emphasis should remain on the early clinical diagnosis of acute appendicitis with its associated low morbidity and mortality.
References
1. Adalla SA: Appendiceal mass: Interval appendicectomy should not be the rule. Br J Clin Pract 50:168, 1996
2. Adolph VR, Falterman KW: Appendicitis in children in the managed care era. J Pediatr Surg 31:1035, 1996
3. Alvarado A: A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med 15:557, 1986
4. Amgwerd M, Rothlin M, Candinas D, et al: Ultrasound diagnosis of appendicitis by surgeons-a matter of experience? Langenbecks Arch Chir 379:335, 1994
5. Balthazar EJ, Bimbaum BA, Yee J, et al: Acute appendicitis: CT and US correlation in 100 patients. Radiology 190:31, 1994
6. Blair NP, Bugis SP, Tumer LJ, et al: Review of the pathologic diagnoses of 2,216 appendectomy specimens. Am J Surg 165:618, 1993
7. Bonanni F, Reed J, Hartzell G, et a1 Laparoscopic versus conventional appendectomy. J Am Coll Surg 179:273, 1994
8. Caldwell MT, Watson RG: Peritoneal aspiration cytology as a diagnostic aid in acute appendicitis. Br J Surg 81:276, 1994
9. Connor TJ, Garcha IS, Ramshaw BJ, et al: Diagnostic laparoscopy for suspected appen- dicitis. Am Surg 61:187, 1995
10. Cox MR, McCall JL, Toouli J, et al: Prospective randomized comparison of open versus laparoscopic appendectomy in men. World J Surg 20:263, 1996
11. Ein SH, Shandling B Is interval appendectomy necessary after rupture of an appendi- ceal mass? J Pediatr Surg 312349, 1996
12. Elangovan S: Clinical and laboratory findings in acute appendicitis in the elderly. J Am Board Fam Pract 9:75, 1996
13. Eriksson S, Granstrom L: Randomized controlled trial of appendicectomy versus antibiotic therapy for acute appendicitis. Br J Surg 82:166, 1995
14. Eriksson S, Granstrom L, Carlstrom A: The diagnostic value of repetitive preoperative analyses of C-reactive protein and total leucocyte count in patients with suspected acute appendicitis. Scand J Gastroenterol 29:1145, 1994
15. Ford RD, Passinault WJ, Morse ME: Diagnostic ultrasound for suspected appendicitis: Does the added cost produce a better outcome? Am Surg 60:895, 1994
16. Frazee RC, Roberts JW, Symmonds RE, et a1 A prospective randomized trial compar- ing open versus laparoscopic appendectomy. AM Surg 219:725,1994
17. Grunewald B, Keating J: Should the 'normal' appendix be removed at operation for appendicitis? J R Coll Surg Edinb 38:158, 1993
18. Guidry SP, Poole GV: The anatomy of appendicitis. Am Surg 60:68, 1994 19. Gurleyik E, Gurleyik G, Unalmiser S: Accuracy of serum C-reactive protein measure-
ments in diagnosis of acute appendicitis compared with surgeon's clinical impression. Dis Colon Rectum 38:1270, 1995
20. Hale DA, Jaques DP, Molloy M, et a1 Appendectomy: Improving care through quality improvement. Arch Surg 132:153, 1997
HAVE THE EVALUATION AND TREATMENT OF ACUTE APPENDICITIS CHANGED? 1369
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
Hale DA, hlalloy M, Pearl RH, et al: Appendectomy: A contemporary appraisal. Ann Surg 225:252, 1997 Hansen JB, Smithers BM, Schache D, et al: Laparoscopic versus open appendectomy: Prospective randomized trial. World J Surg 2017, 1996 Jeffrey RB: In patients with right lower quadrant pain, is sonography or CT the preferred imaging technique for initial evaluation? AJR 164:1547, 1995 Jitea N, Angelescu N, Burcos T, et a1 Laparoscopic appendectomy in obese patients. A comparative study with open appendectomy. Chirurgia (Bucur) 45:203, 1996 John H, Neff U, Kelemen M: Appendicitis diagnosis today: Clinical and ultrasonic deductions. World J Surg 17243,1993 Kalan M, Talbot D, Cunliffe WG, et al: Evaluation of the modified Alvarado score in the diagnosis of acute appendicitis: A prospective study. Ann R Coll Surg Engl 76:418, 1994 Keller MS, McBride WJ, Vane DW: Management of complicated appendicitis. A ratio- nal approach based on clinical course. Arch Surg 131:261, 1996 Koepsell TD, Inui TS, Farewell VT Factors affecting perforation in acute appendicitis. Surg Gynecol Obstet 153:508, 1981 Kum CK, Ngoi SS, Goh I'M, et al: Randomized controlled trial comparing laparoscopic and open appendicectomy. Br J Surg 80:1599, 1993 Laine S, Rantala A, Gullichsen R, et al: Laparoscopic appendectomy-is it worthwhile? A prospective, randomized study in young women. Surg Endosc 11:95, 1997 Lane MJ, Katz DS, Ross BA: Unenhanced helical CT for suspected acute appendicitis. AJR 168:405,1997 Lim HK, Lee WJ, Kim TH, et a1 Appendicitis: Usefulness of color Doppler US. Radiology 201:221, 1996 Malone AJ, Wolf CR, Malmed AS, et a1 Diagnosis of acute appendicitis: Value of unenhanced CT. AJR 160763, 1993 Martin LC, Puente I, Sosa JL, et a1 Open versus laparoscopic appendectomy. A prospective randomized comparison. Ann Surg 222:256, 1995 McCahill LE, Pellegrini CA, Wiggins T, et al: A clinical outcome and cost analysis of laparoscopic versus open appendectomy. Am J Surg 171:533, 1996 McNamara MJ, Pasquale MD, Evans S: Acute appendicitis and the use of intraperito- neal cultures. Surg Gynecol Obstet 177393, 1993 Mime L, Vamer D, Bumell A, et al: Laparoscopic vs open appendectomy. Prospective randomized study of outcomes. Arch Surg 132708, 1997 Nies C, Bartsch D, Rothmund M: Laparoscopic cholecystectomy in morbid obesity. Indications or contraindications? Chirurg 65:29, 1994 Nitecki S, Assalia A, Schein M: Contemporary management of the appendiceal mass. Br J Surg 3018, 1993 Ohmann C, Yang Q, Franke C: Diagnostic scores for acute appendicitis. Abdominal Pain Study Group. Eur J Surg 161:273, 1995 Olsen JB, Myren CJ, Haahr PE: Randomized study of the value of laparoscopy before appendicectomy. Br J Surg 80:922, 1993 Orr RK, Porter D, Hartman D Ultrasonography to evaluate adults for appendicitis: Decision making based on meta-analysis and probabilistic reasoning. Acad Emerg Med 2:644, 1995 Ortega AE, Hunter JG, Peters JH, et a1 A prospective, randomized comparison of laparoscopic appendectomy with open appendectomy. Laparoscopic Appendectomy Study Group. Am J Surg 169:208, 1995 OToole SJ, Karamanoukian HL, Allen JE, et al: Insurance-related differences in the presentation of pediatric appendicitis. J Pediatr Surg 31:1032, 1996 Paajanen H, Somppi E: Early childhood appendicitis is still a difficult diagnosis. Acta Paediatr 85:459, 1996 Price MR, Haase GM, Sartorelli KH, et al: Recurrent appendicitis after initial conserva- tive management of appendiceal abscess. J Pediatr Surg 31:291, 1996 Ramachandran P, Sivit CJ, Newman KD, et al: Ultrasonography as an adjunct in the diagnosis of acute appendicitis: A 4-year experience. J Pediatr Surg 31:164, 1996

1370 WILCOX & TRAVERSO
48. Ramirez JM, Deus J: Practical score to aid decision making in doubtful cases of appendicitis. Br J Surg 81:680, 1994
49. Rao PM, Rhea JT, Novelline RA, et al: Helical technique for the diagnosis of appendicitis: Prospective evaluation of a focused appendix CT examination. Radiology 202139, 1997
50. Richards W, Watson D, Lynch GW, et al: A review of the results of laparoscopic versus open appendectomy. Surg Gynecol Obstet 177:473, 1993
51. Rioux M: Sonographic detection of the normal and abnormal appendix. AJR 158:773,1992 52. Rossi P, Covarelli P, Mosci F, et al: Ultrasonography in the management of acute
appendicitis. Surg Endosc 10:619, 1996 53. Sanson TG, OKeefe KP: Evaluation of abdominal pain in the elderly. Emerg Med Clin
North Am 14:615, 1996 54. Sarfati MR, Hunter GC, Witzke DB, et al: Impact of adjunctive testing on the diagnosis
and clinical course of patients with acute appendicitis. Am J Surg 166:660, 1993 55. Sayed Hassen AH, Cade RJ: A prospective trial of open versus laparoscopic appendi-
cectomy. Aust NZ J Surg 66:178, 1996 56. Schirmer BD, Schmieg RE Jr, Dix J, et al: Laparoscopic versus traditional appendectomy
for suspected appendicitis. Am J Surg 165:670, 1993 57. Tate JJ, Dawson JW, Chung SC, et al: Laparoscopic versus open appendicectomy:
Prospective randomised trial. Lancet 342:633, 1993 58. Temple CL, Huchcroft SA, Temple WJ: The natural history of appendicitis in adults:
A prospective study. Ann Surg 221:278, 1995 59. Thompson JE Jr, Bennion RS, Schmit PJ, et al: Cecectomy for complicated appendicitis.
J Am Coll Surg 179335, 1994 60. Vallina VL, Velasco JM, McCuloch CS: Laparoscopic versus conventional appendec-
tomy. Ann Surg 218:685, 1993 61. Vargas HI, Averbook A, Stomos MJ: Appendiceal mass: Conservative therapy followed
by interval laparoscopic appendectomy. Am Surg 60:753, 1994 62. Velanovich V, Satava R Balancing the normal appendectomy rate with the perforated
appendicitis rate: Implications for quality assurance. Am Surg 58:264, 1992 63. Verroken R, Penninckx F, Van Hoe L, et al: Diagnostic accuracy of ultrasonography
and surgical decision-making in patients referred for suspicion of appendicitis. Acta Chir Belg 96:158, 1996
64. Von Titte SN, McCabe CJ, Ottinger LW: Delayed appendectomy for appendicitis: Causes and consequences. Am J Emerg Med 14:620, 1996
65. Wade DS, Marrow SE, Balsara ZN, et al: Accuracy of ultrasound in the diagnosis of acute appendicitis compared with the surgeon’s clinical impression. Arch Surg 128:1039, 1993
66. Wagner JM, McKinney WP, Carpenter J L Does this patient have appendicitis? JAMA 276:1589, 1996
67. Walker SJ, West CR, Colmer MR: Acute appendicitis: Does removal of a normal appendix matter, what is the value of diagnostic accuracy and is surgical delay important? AM R Coll Surg Engl 77358, 1995
68. Wen SW, Naylor CD: Diagnostic accuracy and short-term surgical outcomes in cases of suspected acute appendicitis. Can Med Assoc J 152:1617, 1995
69. Williams MD, Collins JN, Wright TF, et al: Laparoscopic versus open appendectomy. South Med J 89:668, 1996
70. Williams MD, Miller D, Graves ED, et a1 Laparoscopic appendectomy, is it worth it? South Med J 87592,1994
71. Williams RJ, Windsor AC, Rosin RD, et al: Ultrasound scanning of the acute abdomen by surgeons in training. Ann R Coll Surg Engl 76:228, 1994
72. Zaninotto G, Rossi M, Anselmino M, et al: Laparoscopic versus conventional surgery for suspected appendicitis in women. Surg Endosc 9:337, 1995
Address reprint requests to L. William Traverso, MD
Department of General Surgery Virginia Mason Medical Center
1100 Ninth Avenue Seattle, WA 98111