hat subcommittee for grossing standardization. brian adley carey august rasheed hammadeh mike...
TRANSCRIPT
GROSSING STANDARDIZATIO
N RECOMMENDATIO
NSHAT subcommittee for grossing
standardization
HAT SUBCOMMITTEE FOR GROSSING STANDARDIZATION: Brian Adley Carey August Rasheed Hammadeh Mike Mihalov Adaora Okonkwo
BACKGROUND Workforce/budget reduction across the
healthcare industry including ACL: especially in histology
Workload>>>manpower, leading to delayed slide turnaround time, poor slide quality, mislabeling, ect
POSSIBLE SOLUTIONS1. Increase the workforce: not likely to happen, beyond MDP pathologists’ control
2. Standardize/limit number of blocks submitted on larger cases (specifically breast, colon, lung, prostate, uterus), within MDP pathologists’ control
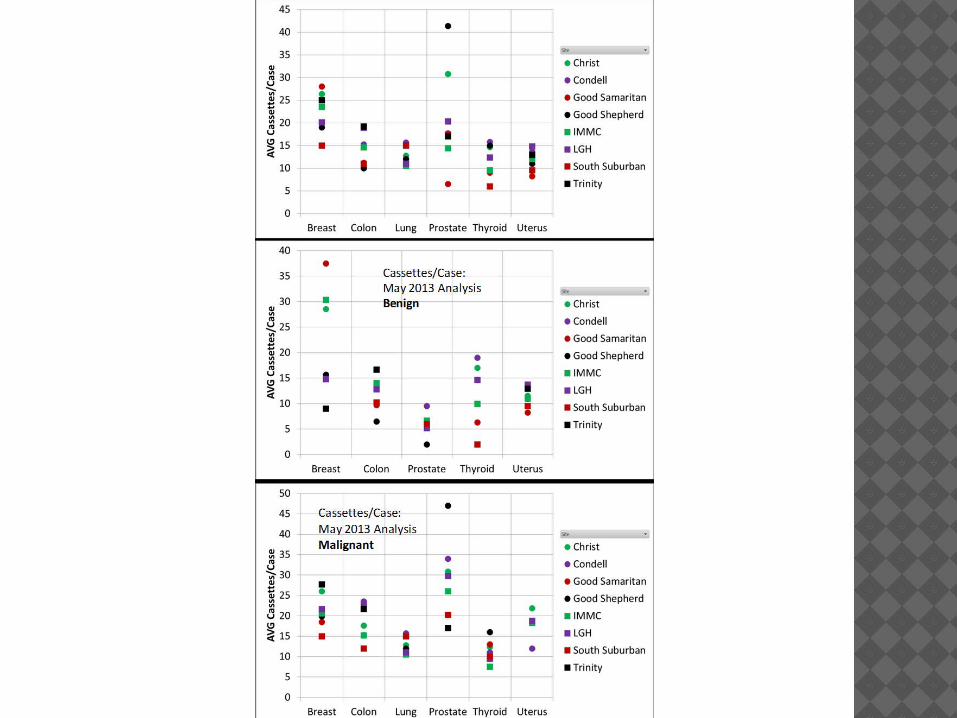
SUBCOMMITTEE GOAL: The goal of the committee was to come
up with data driven recommendations for the appropriate number of blocks per large case for accurate diagnosis and staging when applicable (specifically for colon, prostate, lung, uterus and breast)
Any additional blocks that did not add pertinent/diagnostic information were eliminated (we no longer have the luxury to submit 40-50 blocks on these cases in today’s environment)
REFERENCES Lester, 3rd edition Indiana University Grossing Manual (on line) Silverberg SG. The Endometrium Pathologic Principles and
Pitfalls, Arch Pathol Lab Med 2007;131:372-382. Eusher ED,Bassett R, Malpica A.Lymph Node Counts in
Endometrial Cancer: Expectations Versus Reality. Am J Surg Pathol 2011;35:913-918.
Yin H,Mittal K. Incidental Findings in Uterine Prolapse Specimen Frequency and Implications. Int J Gynecol Pathol 2003;23:26-28.
Iremashvili V. et al. Partial Sampling of Radical Prostatectomy Specimens. Am J Surg Pathol 2013;37:219-225.
www.pathnet.medsch.ucla.edu/.../get.asp https://www.pathology.med.umich.edu/Resident/
Cutting_Manual/Breast http://grosspathology.sites.uchicago.edu/page/lumpectomy
COLON1. Neoplastic (16-18 cassettes) Site CassettesLesion 3-4* (x2 - deepest penetration; x1 w adjacent NL; x1 - w distal marg) Both margins (inked) 1LNs approx 5 (NON-bisected - up to 3 per cassette)Appendix (if applicable) 1Other 5-7 (additional lesions: polyps, diverticuli)*Certain lesions like villous adenomas will require more extensive sampling
COLON2. Diverticulitis (5 cassettes)Site CassettesBoth Margins including NL 1Diverticuli/perforation3Other 2 (polyp, LNs, etc)
COLON3. IBD (16-18 cassettes)Site CassettesDiseased tissue UC - x10 (1 per 10 cm); Crohn's - x5 of diseased areaBoth margins 2 (separate cassettes)Additional lesions 2-3Readily identifiable LN2-3
PROSTATECTOMY If < or = to 35 g, submit entire prostate
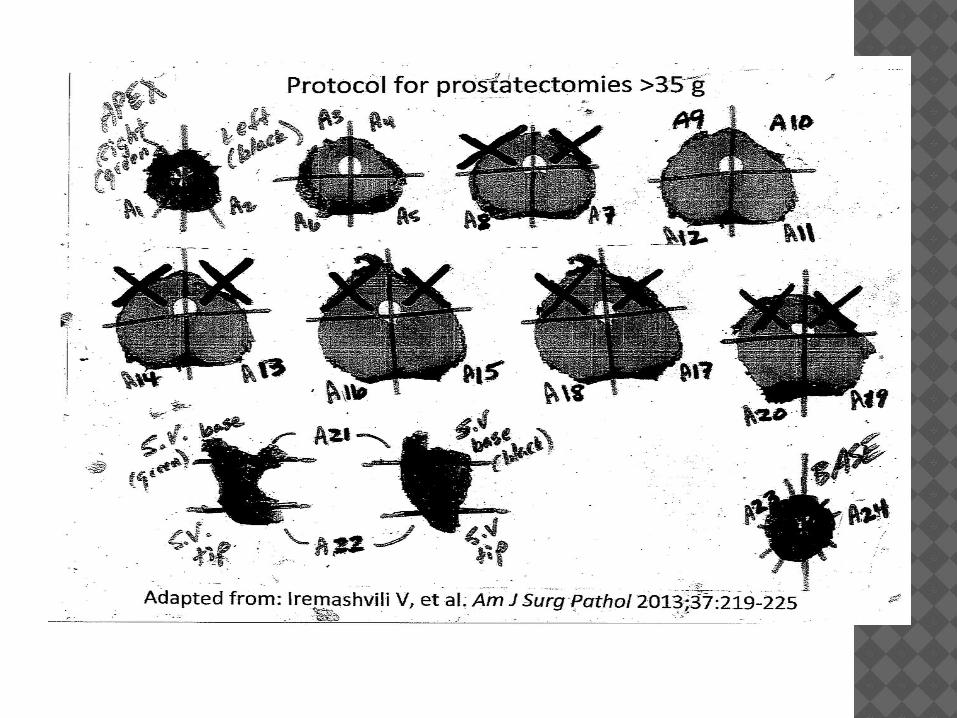
and base of both seminal vesicles If greater than 35 g, follow protocol
proposed by Iremashvili V et al. (AJSP 2013;37:219-225):
TURP First 10 g: 5 cassettes >10 g (1 cassette per additional 10 g)
UTERUS1.MORCELLATION HYSTERECTOMY-up to 8 blocks 2.MYOMECTOMY-up to 5 blocks (look for most abnormal)
UTERUS3.SIMPLE HYSTERECTOMY FOR BENIGN DISEASE-up to 10 (if no adnexae); up to 12 (if adenxae present)-Anterior+posterior cervix, Anterior+posterior endomyometrium, 3 sections of leiomyomata if they appear typical (one section of the largest, 2 other random sections)-Fallopian tube and ovary section submitted in same cassette
UTERUS4.HYSTERECTOMY FOR ENDOMETRIAL CANCER-up to 20 blocks-Anterior+posterior cervix, Anterior+posterior LUS,4 Anterior+posterior endomyometrium with tumor (divide tissue as needed to demonstrate full thickness, which would result in 4 more cassettes),Left+right parametria,2 sections leiomyomata,1 section R ovary and tube, 1 section L ovary and tube
UTERUS5.HYSTERECTOMY FOR COMPLEX ATYPICAL HYPERPLASIA (ie, no definitive diagnosis of cancer)-up to 20 blocks-Same as hysterectomy for cancer, but need to strip and submit entire endometrium. To accomplish this, take sections of endometrium with endomyometrial junction and submit multiple samples in each cassette.
UTERUS7.RADICAL HYSTERECTOMY FOR CERVICAL CANCER-up to 20 blocks-4 Full thickness cervix with tumor, 4 entire vaginal margin, 2 parametrial margins, Anterior+posterior LUS, Anterior+posterior endomyometrium, 3 sections leiomyomata or other endometrial lesions such as polyp, Left tube and ovary, Right tube and ovary
UTERUS8.HYSTERECTOMY FOR HSIL OR MICROINVASIVE CARCINOMA-up to 25 blocks-12 coned cervix (more than one section per cassette), Anterior +posterior LUS,Anterior+posterior endomyometrium, 3 leiomyomata or other endometrial lesions such as polyp,1 paracervical tissues (use different colors of ink to denote left and right), Left tube and ovary, Right tube and ovary
UTERUS6.LYMPH NODE DISSECTION FOR ENDOMETRIAL CANCER-Only submit the dissected lymph nodes. There is no reason to submit all of the fat. Just say no.
LUNGLung, wedge resection for tumor:Tumor<5 cm (6-8 total blocks): - 3 blocks for tumor (may include 2 small sections of tumor in each), one block also include pleura.- 1-2 block for parenchyma near tumor- 1-2 block for parenchyma away from tumor- 1-2 block margin of resection near tumor (if needed).- Tumor >5 cm (8-10 total blocks): -one section of tumor/cm (may put 2 section in one block).- 1-2 block for parenchyma near tumor- 1-2 block for parenchyma away from tumor- 1-2 block margin of resection near tumor (if needed).
LUNGLung, Lobectomy:Lung, lobectomy for tumor, no prior wedge (12-14 total blocks): 1 block margin of main bronchus. 1 block margin of hilar vessels. 1 block parenchymal margin if applicable. 1-3 block hilar lymph nodes. 3 blocks of lung parenchyma, including any
abnormal area 2 blocks from parenchyma near tumor. 3 blocks for tumor (may include 2 small
sections of tumor in each), one block also include pleura.
LUNGLung, lobectomy for tumor, with prior wedge (8-10 blocks): 1 block margin of main bronchus. 1 block margin of hilar vessels. 1 block parenchymal margin if
applicable. 1-3 block hilar lymph nodes. 3 blocks of lung parenchyma, including
any abnormal area 2 blocks parenchyma near tumor.
LUNGLung, pneumectomy for tumor (14-16 total blocks): 1 block margin of main hilar bronchus. 1 block margin of hilar vessels. 1 block parenchymal margin if applicable. 1-3 block hilar lymph nodes. 3 blocks of lung parenchyma, including any
abnormal area, for each lobe 2 blocks parenchyma near tumor. One section of tumor/cm (may put 2 section
in one block). 1-2 blocks from interlobar fissure if needed.
BREASTMastectomies (Segmental, Simple and Modified Radical): 14 - 16 Blocks should be submitted as follows: 4 cassettes of tumor - Include closest inked
margin if possible. Representative closest margins For lesions < 2 cm, submit entirely. Up to 5 cassettes of biopsy cavity if no tumor is
present - including to the deep margin Nipple, areola, skin. Sections of additional suspicious lesions and
concurrent disease processes. 1 representative section from each quadrant.
BREASTProphylactic mastectomies, 9-10 blocks 1 cassette for nipple, lesion (if present), 2 cassettes for each quadrant.
BREAST For post-treatment tumor beds, submit
entirely if <5cm. If more than 5 cm, submit 2
representative sections per cm of tumor bed or per hospital protocol if indicated.
Nipple, areola, skin. Sections of additional suspicious lesions
and concurrent disease processes. 1 representative section from each
quadrant.
BREASTLumpectomy for palpable mass: Approx 15 cassettes Lumpectomies should be entirely
submitted if small (< 5 cm), with sequential relationship to surgical margin.
For well-circumscribed lesions, benign (fibroadenomas), 1 section per cm
If mass is predominantly DCIS on NCB with/without focal microinvasion, submitting the entire lumpectomy is required to exclude a larger size of invasive carcinoma.
BREASTLumpectomies >5cm (15-20 cassettes): Submit a perpendicular section of the
mass/lesion with each margin if close to mass/lesion.
If the margins are distant from the mass/lesion, then submit representative-shave sections (2 cassettes per margin)
Both discrete or ill-defined masses/lesions should have flanking sections submitted on both sides of the greatest dimension measurement.
BREASTLumpectomy for microcalcifications (no biopsy or biopsy benign): Submit entire specimen in sequential sections if
specimen is < 5 cm. In larger specimens (> 5 cm), sample the area of
the wire tip and representative adjacent tissue. If clip is found, 2-4 blocks surrounding clip, relation
of suspicious area to close margins, 1 block perpendicular to each margin.
For multiple lesions, sampling each lesion individually, sections from normal-appearing areas in-between the lesions.
In cases where gross examination and initial sections do not show histologic abnormality, all the fibrous foci should be submitted.
BREAST MARGIN RE-EXCISIONS Unorientated flat portions of tissue are laid flat in a cassette (shave
margin) and submitted entirely. Oriented (inked) specimens are serially sectioned perpendicular to new
margin, and submitted in a manner to examine the new margin. Small re-excisions (4-5 cassettes) can be submitted in toto.
Larger re-excisions can be representatively sampled with 4 representative blocks.
For re-excisions following invasive carcinoma, status of gross residual disease is evaluated with its relationship to different excision margins; in the absence of gross disease, the specimen should be representatively sampled (q2 or q3 levels).
For re-excisions following a diagnosis of in situ carcinoma, the specimen may need to be more widely sampled to detect residual disease and/or associated invasive carcinoma.
Complete re-excision of cavity created by a prior lumpectomy are inked with respect to orientation, and serially sectioned as in a lumpectomy. The blood-filled biopsy cavity should be entirely submitted, in particular with respect to new margins to evaluate the residual disease and status of surgical margins. Submit alternate sections or every third levels (submit q2 or q3 levels) if large (> 5 cm).
BREASTGynecomastia, 2 - 4 blocks 2 cassettes of breast parenchyma If lesion present, additional cassettes.Breast Reduction, 2 - 4 blocks 1 cassette of breast parenchyma & skin If lesion present, 2 cassettes If a breast cancer history is present - 4 cassettesBreast duct Sequentially submit the entire specimen (anterior to
posterior) mention which cassettes contain the lesion.
Breast Prostheses and Capsule, 1 - 2 blocks 1 or 2 sections of fibrous “capsule” that is submitted with implant(s).
BREASTAxillary Lymph node dissections: At least 10 lymph nodes, if less, re-examine and submit additional
tissue.
Thank you for your attention!