haematolymphoidcase presentations –part #2 · • if in doubt, perform cd30 ihc • high index of...
TRANSCRIPT
Haematolymphoid case presentations – part #2
Dr Chris van VlietConsultant Anatomical Pathologist
Lead Pathologist Oncology FISH sectionPathWest QEII, Perth

Case #1
• 15M, presented with abdominal pain ?appendicitis
• Respiratory failure ?ARDS• Intubated and ventilated, followed by venovenous ECMO
• Bilateral inguinal lymphadenopathy noted
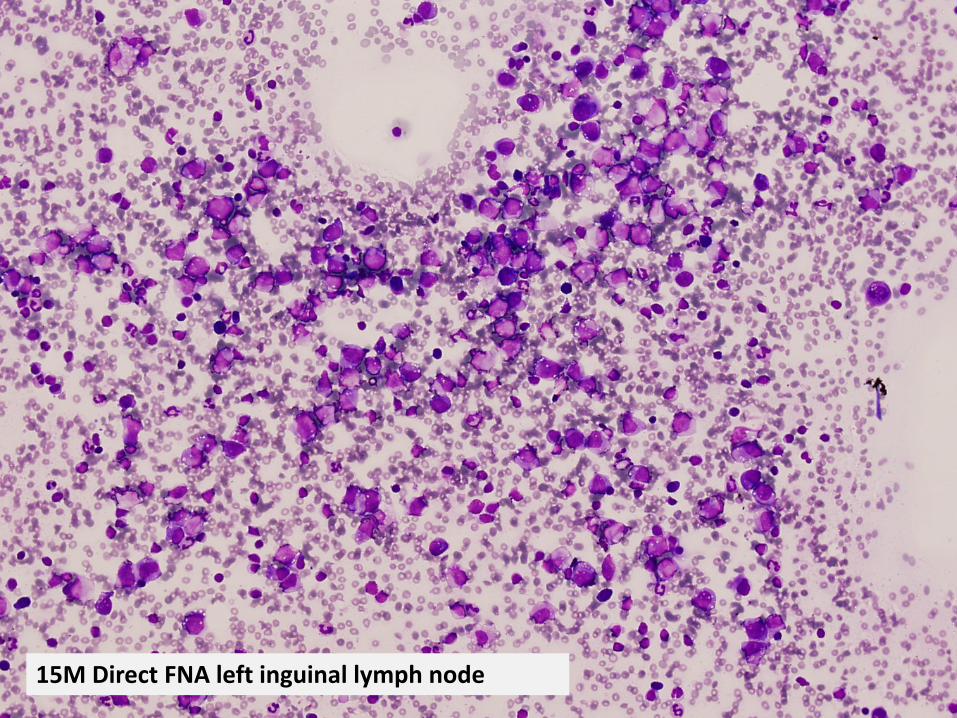
15M Direct FNA left inguinal lymph node


Paediatric lymphomas: ddx
• Hodgkin lymphoma• Burkitt lymphoma• Diffuse large B‐cell lymphoma• Lymphoblastic lymphoma• ALK+ anaplastic large cell lymphoma• (Myeloid sarcoma)• (Exclude EBV infection!)



Vysis ALK FISH break apart FISH probe
Clinical course
• ALK+ anaplastic large cell lymphoma • CHOP chemotherapy• Remained on ECMO for 6 weeks but made a full recovery and remains in remission
Cytologic diagnosis of lymphomas
• Many lymphomas can be diagnosed accurately using a multiparameter approach:– Cytomorphology– Immunophenotyping– Molecular testing – ideally unique to malignancy– Involvement of haematologists– Use WHO terminology
• E.g. SLL/CLL, Mantle cell, ALCL, lymphoblastic

Cytologic diagnosis of lymphomas –the pros
• Improved cytomorphology• Safe, quick and cost effective• Ideal for difficult to reach organs• Good representation of tumours cells (NB molecular testing)
• Multiple lesions/repeat testing
Cytologic diagnosis of lymphomas –the cons
• Sampling issues – low/high grade• Hodgkin lymphoma, PTCL• Many trials require a histologic diagnosis• Loss of archival tissue for reclassification & research

Case #2
• 10F, headaches• CT head: left retro‐orbital sphenoid bone lesion

CT guided FNA left retro-orbital tumour


S100 CD1a
CD68 BRAF VE1

Sanger squencing: BRAF V600E mutation
BRAF c.1799T>A, p.Val600Glu (or V600E) mutation
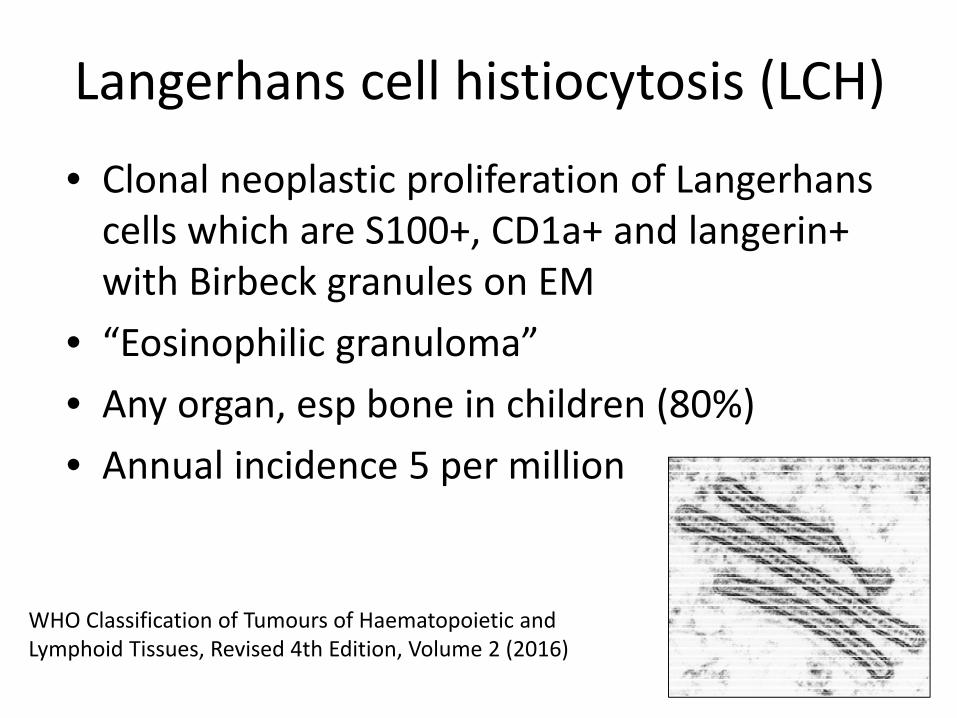
Langerhans cell histiocytosis (LCH)
• Clonal neoplastic proliferation of Langerhans cells which are S100+, CD1a+ and langerin+ with Birbeck granules on EM
• “Eosinophilic granuloma”• Any organ, esp bone in children (80%)• Annual incidence 5 per million
WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, Revised 4th Edition, Volume 2 (2016)

LCH: new developments
• BRAF V600E mutations in ̴50% LCH• Tends to occur in younger pts• Not assoc with disease site or stage• Therapeutic target – vemurafinib• MAP2K1 muta ons in ̴20%• Rare: ARAF, PIK3CA
Badalian-Very et al. Blood 2010;116(11):1919-1923.Brown et al. Blood 2014;124(10):1655-1658.Emile et al. Blood 2016;127(22):2672-2681.
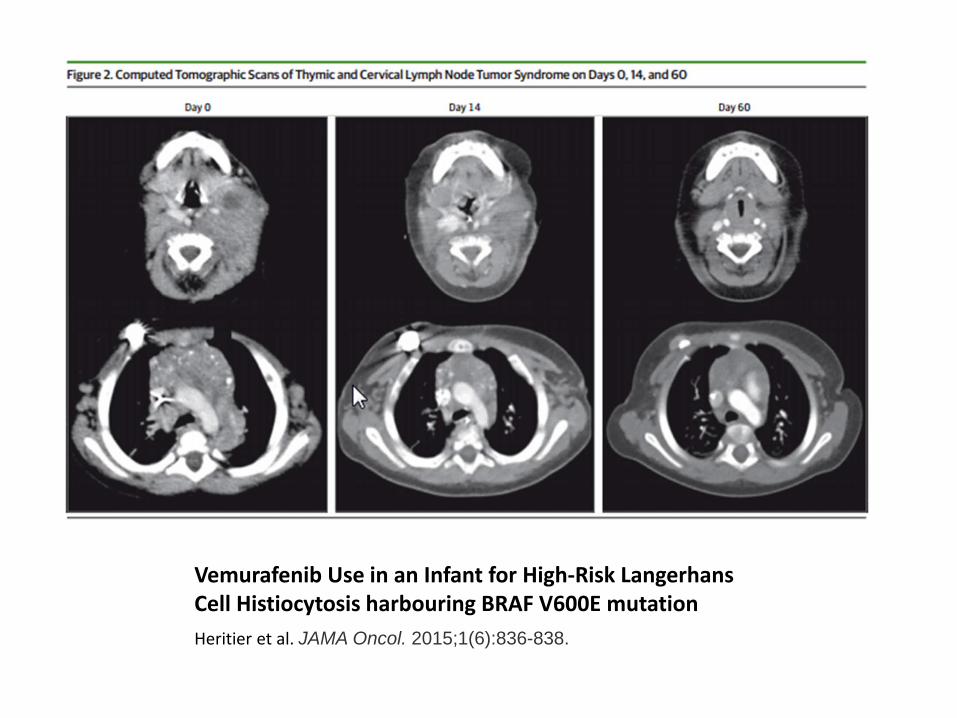
Vemurafenib Use in an Infant for High‐Risk Langerhans Cell Histiocytosis harbouring BRAF V600E mutationHeritier et al. JAMA Oncol. 2015;1(6):836-838.
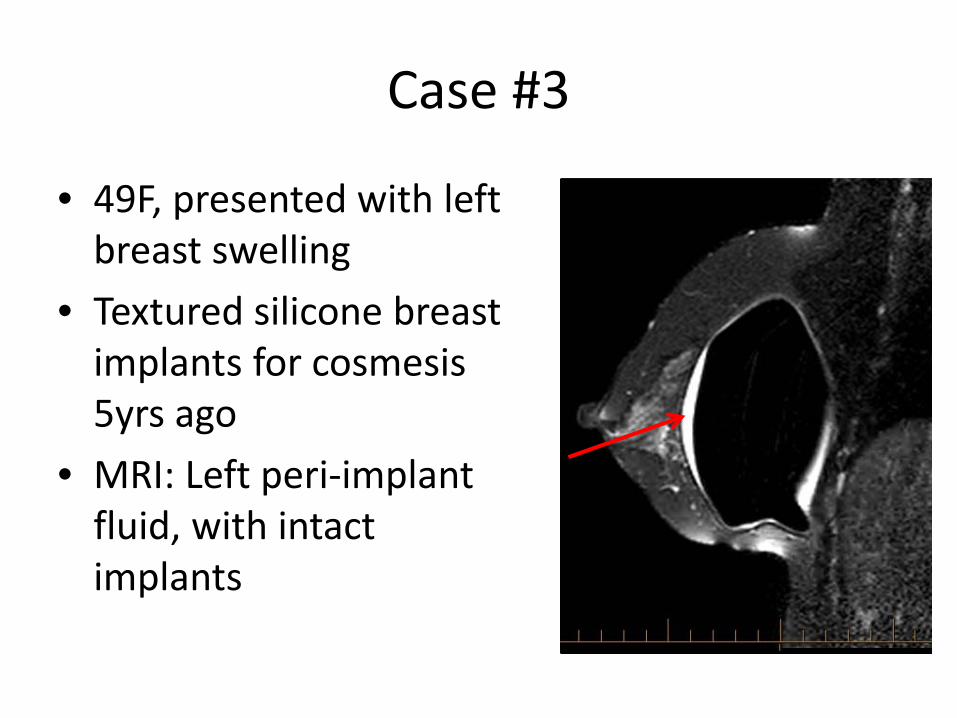
Case #3
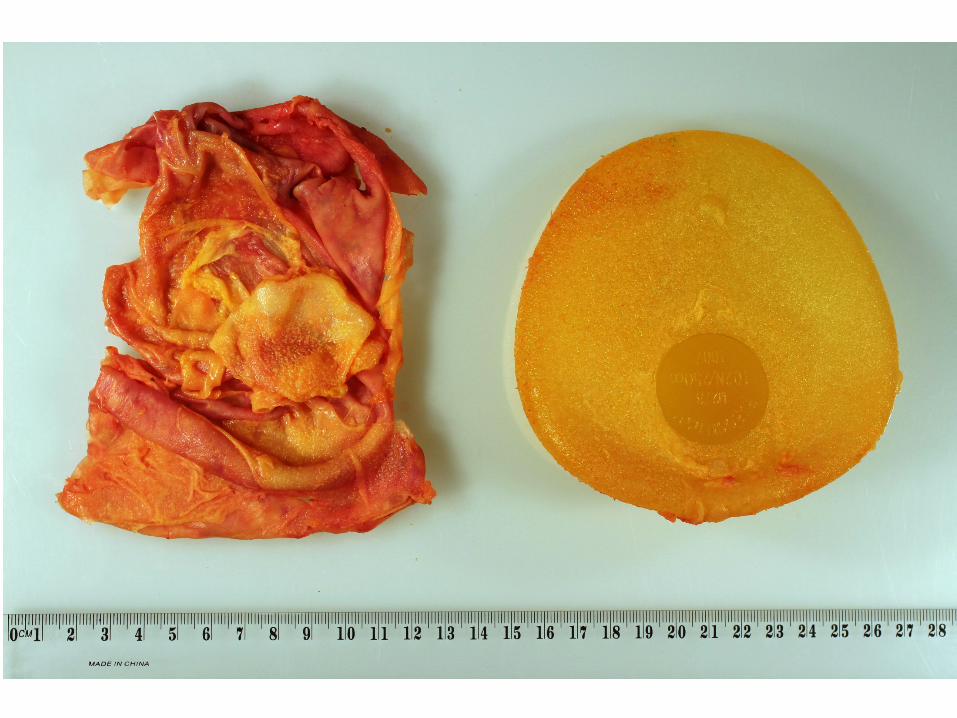
• 49F, presented with left breast swelling
• Textured silicone breast implants for cosmesis5yrs ago
• MRI: Left peri‐implant fluid, with intact implants



CD30
ALKTIA1
CD4
Clinical course:
• Breast implant‐associated associated anaplastic large cell lymphoma
• Stage 1E disease• Capsulectomy and removal of implant performed
• No further chemo‐ or radiotherapy• Patient remains disease‐free at 5 years

Schematic representation of breast implant-associated anaplastic large cell lymphoma. https://www.fda.gov/

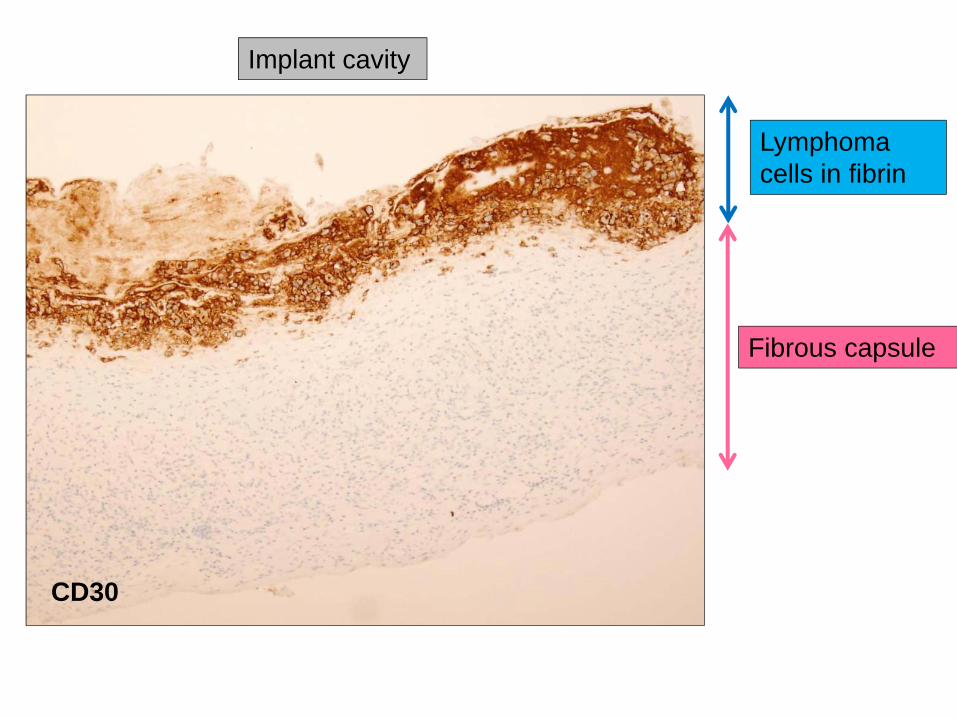
Lymphoma cells in fibrin
Fibrous capsule
Breast tissue
Implant cavity
Images courtesy of Dr Ming Chai
Lymphoma cells in fibrin
Fibrous capsule
CD30
Implant cavity

Breast implant ALCL: background
• 1962: 1st silicone breast implants inserted• 1997: 1st case report of ALCL in association with silicone implant
• 2011: 1st US FDA safety communication• 2016: Recognised by WHO classification as a provisional entity
• 2018: 594 cases worldwide, 73 Australian
Keech et al. Plast Reconstr Surg. 1997;100:554–555.Swerdlow SH et al. Blood 2016;127(20):2375‐2390https://www.plasticsurgery.org/ (accessed 13/9/2018)https://www.tga.gov.au/ (accessed 13/9/2018)
Breast implant ALCL
• Silicone and saline filled implants implicated• Post breast cancer recon & cosmetic• Risk: 1‐in‐1,000 and 1‐in‐10,000• Most cases 3 and 14 years after the implant• All patients exposed to textured implants
– US mostly smooth– Australia/Europe mostly textured
Brody GS et al. Plast Reconstr Surg. 2015 ;135(3):695‐705.Deva AK. Plast Reconstr Surg. 2017;139(5):1051‐1052. https://www.tga.gov.au/ (accessed 13/9/2018)

Breast implant ALCL: Biofilm
• Bacterial biofilm implicated –activates T lymphocytes
• Ralstonia sp.• ?Similar model to H. pylori and MALT lymphoma
• 14‐point intraoperative plan to reduce contamination
Hu H et al. Plast Reconstr Surg. 2016 Jun;137(6):1659‐69.

Laurent C et al. Ann Oncol. 2016;27(2):306‐314.
Seroma/effusion
Mass (+/‐ effusion)

Solid tumour progression hypothesis
Lymph node invasion
Luminal side of capsule Breast
tissue
Lymphoma cell
Fibrin layer
Thickened capsule
with mass
1
2
3 4
Courtesy of Drs Miles Prince and Mark Clemens

Breast implant ALCL: treatment
Clemens MW et al. Plast Reconstr Surg. 2018 Apr;141(4):586e‐599e.
• Capsulectomy + removal of the breast implant• Mass forming disease +/‐ nodal involvement require additional chemotherapy.

Breast implant ALCL: genetic profile
• Mutations of JAK1 or STAT3 in a subset, similar to other ALCLs
• Leads to JAK/STAT pathway activation
• Targeted therapies?• No DUSP22 or TP63 rearrangements
Blomberry P et al. Haematologica 2016;101(9):e387‐90.Oishi N et al. Blood 2018;132(5):544‐547.Di Napoli A et al. Br J Haematol 2018;180(5):741‐744.
IHC pSTAT3 expression.Blood 2018;132(5):544‐547.
Breast implant ALCL: Approach to dx
• Periprosthetic fluid collections should be aspirated and submitted fresh
• Triage for micro + cytology (including cell block) +/‐ flow cytometry
• Most cases are easy to diagnose• If in doubt, perform CD30 IHC• High index of suspicion, but not all late seromas are due to ALCL
Clemens MW et al. Plast Reconstr Surg. 2018 Apr;141(4):586e‐599e.Chai SM et al. Diagn Cytopathol. 2014 Nov;42(11):929‐38.
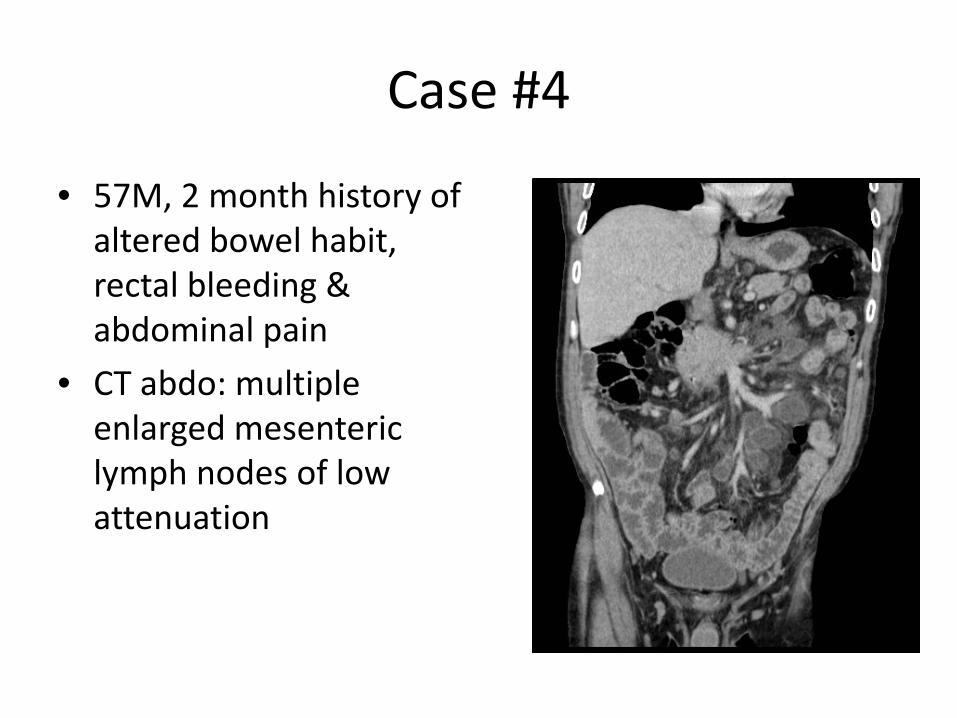
Case #4
• 57M, 2 month history of altered bowel habit, rectal bleeding & abdominal pain
• CT abdo: multiple enlarged mesenteric lymph nodes of low attenuation
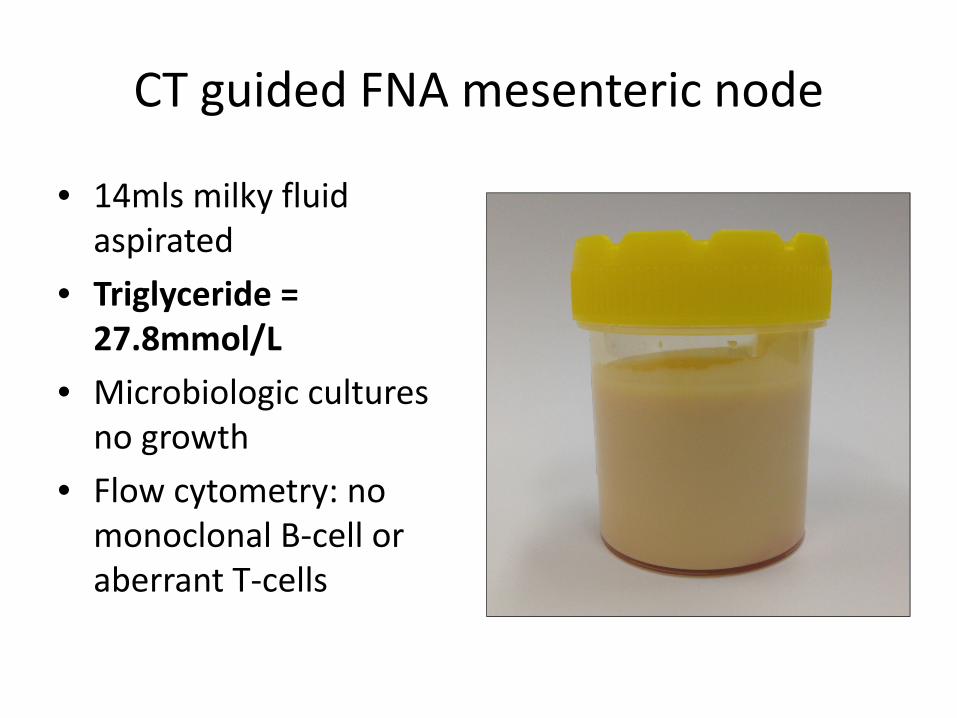
CT guided FNA mesenteric node
• 14mls milky fluid aspirated
• Triglyceride = 27.8mmol/L
• Microbiologic cultures no growth
• Flow cytometry: no monoclonal B‐cell or aberrant T‐cells

CT guided FNA mesenteric node
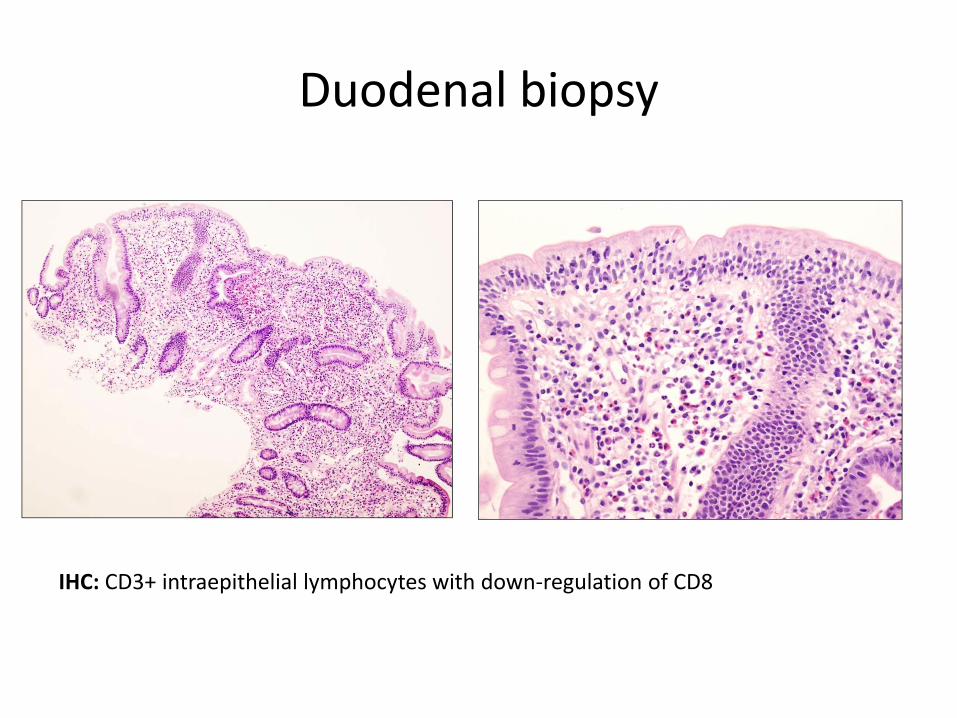
Duodenal biopsy
IHC: CD3+ intraepithelial lymphocytes with down‐regulation of CD8
Clinical course:
• Cavitating mesenteric lymph node syndrome complicating unrecognised coeliac disease
• IgA anti‐tTg = 66 U/ml• Monitored by haematology and gastro teams• Weight gain on gluten‐free diet• Reduction in mesenteric nodes• Alive & well

Cavitating mesenteric lymph node syndrome (CMLNS)
• Rare, poorly understood complication of coeliac disease (CD)
• Diarrhoea, weight loss & hyposplenism• Mortality 50% due to cachexia, infection, lymphoma or DIC
• Exclude enteropathy‐associated T‐cell lymphoma (EATL)
Schwock J et al. Diagn Cytopathol. 2015;43(2):125‐30.Schmitz F et al. Int J Colorectal Dis. 2002;17(3): 192‐8.Howat AJ et al. Histopathol. 1995;27(4):349‐54.

CMLNS arising in the context of EATL
• 55M, presented with massive melaena.
• Emergency surgery for small bowel perforation, milky fluid oozing from lymph nodes
• Jejunum showed EATL & background CD
• Poor response to chemo & died
Case and images courtesy of Drs PriyanthiKumarasinghe and Celia Green
CMLNS: Lessons• It’s so rare the radiologists/clinicians might not have heard of it!
• Rapid on‐site useful even though the cellular yield is not as impressive as the imaging
• Triage for micro, biochem, flow & cell block• Not all patients have known history of coeliac disease
• Further management requires input from gastro & haematology teams

Acknowledgements
• Dr Benhur Amanuel and AP Molecular Pathology Department at PathWest
• Ms Joanne Peverall and the FISH team at PathWest
• Dr Ming Chai• Dr Priyanthi Kumarasinghe• Dr Miles Prince