Haematological Emergencies Pieter de Witt 18 Oct 2014
Overview � Malignant spinal cord compression
� Hypercalcaemia
� Superior Vena Cava syndrome
� Neutropaenic fever
� Extreme Cytosis
Malignant Spinal Cord Compression
MSCC Spinal cord
MSCC Importance / Urgency � Neurological status at Rx
initiation � Most important prognostic
factor
MSCC Clinical presentation � Pain
� Motor findings
� Sensory findings
� Bladder and Bowel dysfunction
� Ataxia
Presenter
Presentation Notes
Severe local back painSensory – less common complaint Progressively increases in intensityAscending numbness and parasthesia Worse with recumbency - venous pressure vs diurnal variation in endo steroidsSensory level or Saddle sensory loss Pain only with movement suggests – instabilityLhermitte’s phenomenon Alleviation with corticosteroids suggests significant neural compression Lumbosacral more radicular pain - spreads down leg, with Valsalva / movement Thoracic - symmetrical band-like wraps anteriorly Abrupt worsening of pain suggests compression fracture Motor Weakness:Upper limb - extensors Lower limb – flexors Reflexes: Brisk, upgoing plantars Cauda Equina – LMN lesions in lower limbs
MSCC Imaging � Plain X-rays
� Magnetic Resonance Imaging – preferred
� CT Myelography
� Image the whole spine Multi-level deposits are present in 1/3 of patients with MSCC
MSCC Management � Goals � Pain control � Preservation or improvement of neurological
� Supportive management � Pain control � Bed rest � Anticoagulation � Prevent constipation � Pressure care
Presenter
Presentation Notes
Glucocorticoids – +/- all patients (vasogenic oedema) Limited documented beneftt High dose (Dexa 96mg/day) vs Low dose (Dexa 16mg/day) Some evidence for improved outcomes BUT higher adverse events Choice of definitive treatment depend on: Spinal stability – Spine Instability Neoplastic Score (SINS) Degree of spinal cord compression Radiosensitivity of the tumour
MSCC Prognostic factors � Neurological status prior to therapy � Histology
� Extent of disease � Visceral or bony metastasis
� Aggressiveness of the tumor � Interval between initial diagnosis and MSCC < 15mo
Presenter
Presentation Notes
Many Haematological disorders are potentially curable
MSCC Key points � Early recognition
� Image the whole spine
� Potentially curable condition
Hypercalcaemia
Presenter
Presentation Notes
Common: 20-30% of people with cancer - Breast Ca, Lung Ca, Myeloma
Hypercalcaemia Causes � Hyperparathyroidism – most common
Higher incidence of above conditions to occur in the same patient
� Other rare causes…
> 90%
Presenter
Presentation Notes
1 Osteolytic metastasis – local osteolysis3. Vitamain D Osteoclast activity >> osteoblast activity - +/- 100% of Hodgkin’s lymphoma, 1/3 of NHL NOT A DIRECT TUMOUR EFFECT- Extrarenal production of 1,25 dihydroxy Vit D by malignant lymphocytes, macrophages *Breast Ca- Increased GIT absorption >> increased bone resorption Locally produced PTHrP without systemic elevation in PTHrP- Usually responds to corticosteroids RANKL and Cytokines *Myeloma Osteoclasts – IL6, RANKL, Osteoprotegerin, IL3, Macrophage Inhibitory Protein !a 2. PTHrP Most common cause in NON-metastatic solid tumours (Squamous) and NHL Serum PTH levels are usually very low Similar findings as in Hyperparathyroidism Measurements - Tumour marker, predict poorer response to bisphosphonates, high PTHrP associated with shorter median OS times
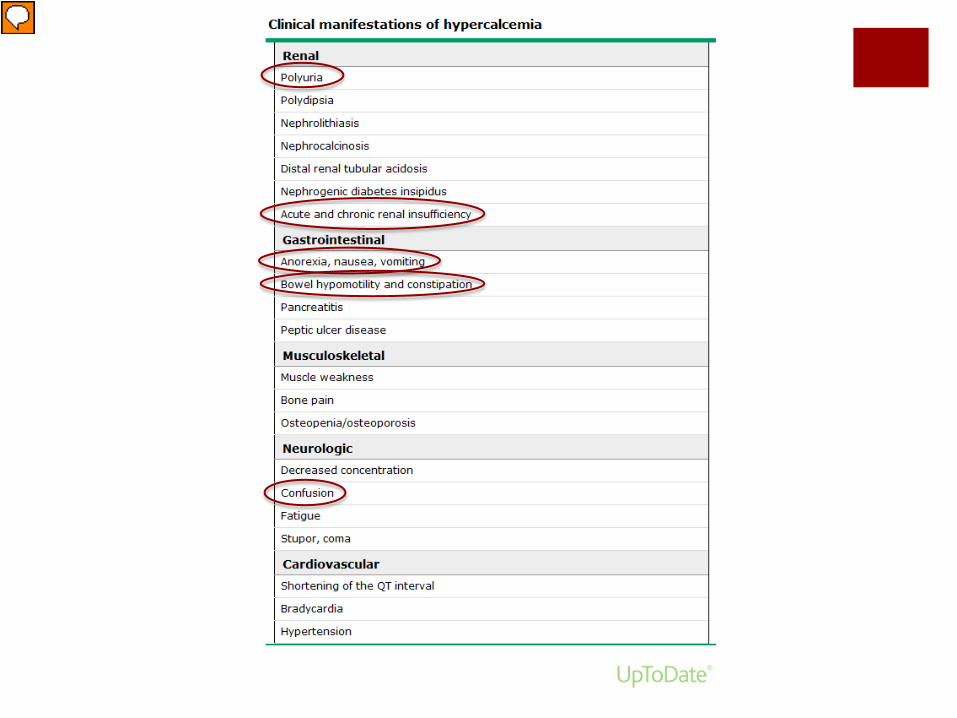
Hypercalcaemia Clinical presentation � Depends on: � Degree of hypercalcaemia � Rate of onset � Individual sensitivity
Polyuria – Nephrogenic Diabetes Insipidus Impaired urinary concentration in the distal convoluted tubule & collecting duct Downregulation of Aquaporin 2 channels, deposition of Calcium in the medulla Calcium sensing receptors Dehydration – Polyuria with anorexia, nausea and vomiting
Hypercalcaemia Management
AIMS Identify and treat the cause Lower serum calcium
Hypercalcaemia Management
Targets
1. Dilute 2. Excrete 3. Influx 4. Remove
Presenter
Presentation Notes
Saline diuresisCalcitonin 200-300 ml/hr or U-output of 100-150ml/hr- Increase renal excretion of calcium, decrease release from bone (inhibiting osteoclasts) +/- diuretics - Relative weak agent but works rapidly (and only for 48hrs) Usually sufficient for mild hypercalacaemia, rarely fully corrects moderate to severe hypercalcaemia- Used in combination with saline diuresis BisphosphonatesGallium nitrate – inhibit osteoclast activity Adsorbs to bone hydroxyapatite – inhibits osteoclast mediated bone resorptionDialysis Pamidronate or Zolidronic acid are preferred agentsCalcimimetics Effect only after 48-72 hrs Careful in renal dysfunction Repeated doses – risk of osteonecrosis of the jaw Glucocorticoids – esp in lymhpoid malignancies - Decrease Vitamin D production – less GIT absorption of calcium
Infective causes Syphilitic Thoracic Aortic Aneurysms Fibrosing Mediastinitis Malignant causes Non-small cell lung cancer – 50% most common Small cell lung cancer – 25% Non-Hodgkin lymphoma – 10% Hodgkin’s lymphoma – rare cause of SVC syndrome despite common presentation with mediastinal lymphadenopathy Benign causes - Intravascular device related thrombosis
SVC Syndrome Clinical manifestations
Presenter
Presentation Notes
Rapidity of onset of signs and symptoms depend on rate of SVC obstructionImaging Malignancy = weeks to months- Majority have an abnormal CXR – mediastinal widening, pleural effusions Fibrosing mediastinitis = years- Ultrasounds – useful to exclude thrombosis - CT or MR – more appropriate investigations Venous pressure increase due to obstruction Lead to the formation of collaterals Interstitial oedema of face, neck & arms – usually most striking Head fullness – exacerbated by bending forward or lying down Narrowing of upper respiratory tract – DYSPNOEA, stridor, hoarseness, cough, dysphagia Cerebral oedema – headache, confusion, coma Hemodynamic compromise usually related to mass effect on the heart rather than SVC obstruction
Malignant SVC Syndrome Management
� PAST – was considered a potential life-threatening medical emergency requiring immediate Radiotherapy
� NOT ANYMORE,…. UNLESS � Stridor � Central airway obstruction or � Laryngeal oedema
� Coma from cerebral oedema
Stent placement and Radiotherapy
Presenter
Presentation Notes
Not emergency RT anymore 1. Deferring Rx until a full diagnostic work-up has been done – NO hazard for most patient PROVIDED the evaluation is efficient and the patient is clinically stable 2.. Radiotherapy may obscure the histological diagnosis Stent placement without radiotherapy might be considered during diagnostic work-up
Malignant SVC Syndrome Management
� Principles � Diagnose and treat the underlying cause � Alleviate symptoms
Presenter
Presentation Notes
Supportive care:Chemotherapy – Treatment of choice Elevate the head ?- Response is usually rapid (Not in NSCLC – stent) Catheter-related thrombosis - remove the vascular catheter +/- AnticoagulationRadiotherapy Glucocorticoids- Most malignancies causing SVC syndrome are RT sensitive Lymphoma & Thymoma - Benefits of RT are usually only temporary NOT in NSCLC After RT esp with laryngeal oedemaEndovascular stents Diuretics – unclear benefit- Rapid symptom palliation - Thrombotic occlusion NOT a contraindication for stent placement
Malignant SVC Syndrome Key Points � NO MORE emergency
Neutropenic Fever Epidemiology � Only 20 – 30% of patients – identifiable infectious source
� Endogenous flora – responsible for 80% of infections
� Bacteria – most frequent infectious cause � Gram negatives (esp Pseudomonas) – most serious � Gram positives � S epidermidis most common (much less virulent) � S aureus & Viridans Streptococci – more serious gram positives
Neutropenic Fever Epidemiology � Fungal infections – esp in high risk patients � Duration of neutropenia � Severity of neutropenia � Prolonged antibiotic use � Number of chemotherapy cycles
Candida – GIT commensal Fever often the sole manifestation Hepatosplenic involvement is common Signs and symptoms often only develop with recovery from neutropenia Albicans = most common; Non-Albicans sp when fluconazole prophylaxis has been used Vascular catheter-related infections Aspergillus – Inhalation of spores Primarily affect the lower respiratory tract Sinusitis, also CNS, bone and skin Mucormycosis Life-threatening rhino-orbital-cerebal, pulmonary and/or disseminated infectons
Neutropenic Fever Management
CRITICAL TO RECOGNIZE !
� Early initiation of empiric systemic antimicrobials � Within 60min of presentation! � Delayed antibiotics – mortality as high as 70%
� Cultures (esp blood) prior to antibiotic initiation
Hyperleukocytosis – WCC > 50 x 109/L (100) Leukostasis – Symptomatic hyperleukocytosis = MEDICAL EMERGENCY Symptoms of decreased tissue perfusion Respiratory and Neurological
Lymphoid vs Myeloid
Presenter
Presentation Notes
Pathophysiology – TISSUE HYPOXIA Increased blood viscosityTHUS High number of abnormal cells- Worsened by red cell transfusions Decreased deformability of the cells- Worsened by diuretics Local hypoxemia High metabolic activity- Lower incidence with CLL Endothelial damage – enzymes and cytokine production- Lower incidence with ALL and CLL In vitro studies: Increased viscosity, AML > 300 ALL > 600 AMLALLCLLCML Hyperleukocytosis10-20%10-30%Significant proportionTypical presentation LeukostasisM4 M5 Microgranular M3Rare (DIC / TLS)Rare (unless > 400)Very uncommon in Chronic stable phase
Leukostasis Clinical presentation
� Pulmonary
� Neurological
� Fever
Presenter
Presentation Notes
Dyspnea and Hypoxia PaO2 falsely low – O2 saturation more accurate measure Visual changes, headaches, dizziness, tinnitus, gait instability, confusion, somnolence, coma - Increased risk of intracranial haemorrhage – persists for at least 1 week after reduction of WCC Fever – 80% of patients - Inflammatory response vs Infection
Hyperleukocytosis Management � Cytoreduction � Chemotherapy � Hydroxyurea - 50-100mg/kg (2 to 4g q12hrly per os) � Leukapheresis
� Supportive care � Blood viscosity � Red cell transfusions, diuretics
� Coagulopathy � Platelet transfusions and DIC
� Tumor lysis prophylaxis � Fluids, Allopurinol
� Prognosis
Presenter
Presentation Notes
Induction chemotherapy – Treatment of choicePrognosis Reduces the WCC substantially within 24 hrs- 1 week mortality 20-40% - Overall prognosis also decreased – biology of tumor and chemoresistance If chemotherapy needs to be delayed If asymptomatic – Hydroxyurea If symptomatic - ?Leukapheresis + Hydroxyurea (no proven benefit) Viscosity Red cell transfusion should be avoided or given slowly over hours Hydration is encouraged, diuretics are discouraged Coagulopathy DIC increases risk of local hemorrhage Maintain platelet count above 20-30 x 109/L for several weeks (risk of ICH persists for weeks after reduction of WCC) – REPERFUSION injury
Extreme Cytosis Red cells � Definitions � Hct > 48% (♀) or > 52% (♂) � Hb > 16,5 (♀) or > 18,5 (♂)
� Relative polycythemia
� Absolute polycythemia � Primary � Secondary
Erythrocytosis
Presenter
Presentation Notes
Secondary erythrocytosis in response to tissue hypoxia = physiological and probably beneficial BUT Circulation is compromised due to hyperviscosity - ? Hct > 60-65% Impaired alertness, headaches, dizziness, compromised exercise tolerance Increased risk of VTE, strokes, myocardial infarcts Theory behind phlebotomy By reducing the hematocrit, blood viscocity reduces and oxygen delivery improves
Erythrocytosis Management � Control the underlying cause
� Phlebotomies � No clear guidelines with threshold Hct levels � Suggestions: � Considered in hypoxic conditions � Limited phlebotomy � Isovolaemic venesections � Avoid iron deficiency � Iron replacement used cautiously
� Other � Weight loss, smoking cessation, home oxygen
Presenter
Presentation Notes
American College of Cardiology / American Heart Association – Guidelines 2008 Recommended therapeutic phlebotomy for: Symptomatic patients Hb > 20 g/dl Hct > 65% With fluid replacement during phlebotomy Lowering the peripheral vascular resistance you may increase the right to left shunt and worsen the hypoxia Iron deficiency Compromise oxygen delivery AND raise the viscocity for a given level of Hb THUS recurrence of symptoms
Erythrocytosis Key Points � Establish the cause
� Limited clinical guidelines for secondary erythrocytosis
� When in doubt – isovolaemic venesections
Extreme Cytosis Platelets � Definitions � Thrombocytosis > 400 x 109/l � Extreme thrombocytosis > 1000 x 109/l
� Reactive thrombocytosis
� Autonomous thrombocytosis � MPN, MDS, CML, AML
Presenter
Presentation Notes
The severity of the thrombocytosis CANNOT be used to distinguish between reactive and Autonomous causes 280 consecutive patients with extreme thrombocytosis 82% had reactive thrombocytosis and only 18% had Autonomous thrombocytosis Infection – 31% Post splenectomy / hyposplenism – 19% Malignancy - 14% Trauma - 14% Inflammation (non infectious) - 9%
Vasomotor symptoms = irrespective of cause Headache, visual symptoms, dizziness, atypical chest pain, acral dysesthesia, erythromelalgia 280 patients with Extreme thrombocytosis - Rates of significant Thrombosis or Hemorrhage Both 24% in Autonomous vs 1% & 3% respectively in Reactive Splenomegaly – might be helpful if present Repeat testing Patients with Reactive thrombocytosis – frequently have many other vascular risk factors
Extreme thrombocytosis Management � Bleeding
� Platelet dysfunction � Acquired type II VWD � Acquired Factor deficiencies (DIC, Factor V)
� Rx � Stop antiplatelet agents � Rapidly reduce the number of platelets � Platelet apheresis � Pharmacological agents – HU or Anagrelide
� Correct deficiencies
Presenter
Presentation Notes
Predominantly mucocutaneous bleeding Difficult situation GIT or GUT bleeding with high platelets - ? Cause GIT bleeding causing iron deficiency with reactive thrombocytosis Or - MPN with dysfunctional platelets causing GIT bleeding
Extreme thrombocytosis Management � Thrombosis � Rx � Rapidly reduce the number of platelets � Platelet apheresis � Pharmacological agents – HU or Anagrelide