hackensack(university(medical(group(|(urology( · from southern new jersey via the new jersey...
TRANSCRIPT

! !
Hackensack(University(Medical(Group(|(Urology(360(Essex(Street,(Suite(403(((Ι(((Hackensack,(NJ(07601(((Ι(((551F996F8090((((Ι((((www.urologynj.com(
IHOR!S.!SAWCZUK,!M.D.,!F.A.C.S.!• Professor & Chairman • Chief, Urologic Oncology John Theurer Cancer Center • Executive VP & Chief Medical Officer
RAVI!MUNVER,!M.D.,!F.A.C.S.!• Associate Professor & Vice Chairman • Chief, Minimally Invasive & Robotic Urologic Surgery • Urologic Oncology & Kidney Stones !KEVIN!R.!BASRALIAN,!M.D.,!F.A.C.S.!• Attending MICHAEL!DEGEN,!M.D.!• Clinical Assistant !DEBRA!FROMER,!M.D. • Assistant Professor • Chief, Center for Bladder, Prostate & Pelvic Floor Health MICHELLE!KIM,!M.D. • Assistant Professor • Chief, Prostatic Disorders and Pelvic Tumors HARRY!P.!KOO,!M.D.,!F.A.A.P.,!F.A.C.S. • Professor • Chief, Pediatric Urology DAVID!SHIN,!M.D. • Assistant Professor • Chief, Center for Sexual Health & Fertility •Men’s Health RICHARD!WATSON,!M.D.,!F.A.C.S. • Professor • Chief, Ambulatory Urology ALAN!N.!!LEIPSNER,!MPH,!MBA,!FACHE!• Administrative Director Urology Academic Affairs Medical Library !!!!!
Dear(Patient,((Thank(you(for(choosing(Hackensack(University(Medical(Group(|(Urology.((We(look(forward(to(meeting(you(and(providing(you(with(the(highest(quality(urological(care.((In(addition(to(our(physicians,(nurses(and(clinical(assistants,(who(will(look(after(your(medical(needs;(our(administrative(staff(is(here(to(help(you(with(scheduling,(billing,(and(other(nonFclinical(issues.((Please(take(a(few(minutes,(prior(to(your(first(visit,(to(complete(and(review(the(following(information(related(to(our(practice.((Doing(so,(will(enable(us(to(serve(you(as(efficiently(as(possible.((
Office&hours&by&appointment&To&schedule&an&appointment&please&call&(551)&996<8090&
&(Included(in(this(packet(for(your(review(and(completion(are(the(following:(
• Registration(Form(• New(Patient(Information(Form(• Questionnaire(s)(• Directions(&(Map(
(In(addition,(we(ask(that(you(bring(the(following(to(your(appointment:(
• Completed(Forms(• Drivers(license(or(legal(form(of(picture(ID(• Insurance(Card(• Insurance(coFpay(• List(of(medications(and(allergies(• Any(and(all(radiology(films(&(reports(–(Please(provide(any(radiology(images((e.g.(XFRay,(
MRI,(Cat(Scan,(and/or(Ultrasound),(or(study(results(relating(to(your(visit((While(under(the(care(of(our(physicians(if(you(need(to(renew(a(prescription,(please(call(your(pharmacy(or(fill(out(the(online(prescription(renewal(form,(found(on(our(website,(urologynj.com.((Please(note(HackensackUMG(|Urology(has(a(noFshow(policy.((Kindly(cancel(or(reschedule(your(appointment(at(least(24(hours(in(advance.((If(a(patient(is(scheduled(for(an(appointment(and(does(not(cancel(or(reschedule,(a(letter(will(be(sent(to(the(patient(charging(them($25.((For(billing(questions(contact(your(billing(representative(within(the(department(at(551F996F8626.((For(all(billing(inquiries(and(details(on(your(statement(please(contact(HackensackUMG’s(Billing(Office(at((866)(571F9238.((Our(goal(is(to(provide(you(with(exceptional(service(and(state(of(the(art(patientFcentered(medical(care(in(an(environment(that(is(sensitive(to(your(needs.((Please(let(us(know(how(we(are(doing(or(how(we(may(improve(our(service(and(do(not(hesitate(to(call(us(if(you(have(any(questions.((Thank(you(again(for(choosing(HackensackUMG(|(Urology(and(we(look(forward(to(meeting(you.(

!
Patient!Information!
!
Date:&____________________________& SSN#:&________________________&
Last&Name:&_______________________& First&Name:&____________________&
Date&of&Birth:&______________________& Gender:& &Male& &&&&&&&Female&
Address:&_________________________________________________________&
City:&____________________________& State:&_______& Zip:&___________&
Special&Living&Arrangements:! &�&None&&&&&&&�&Assisted&Living&&&&&�&Nursing&Home&
Home&Phone:&_____________________& Cell&Phone:&____________________&
EFmail&Address:&___________________________________________________&
Race:& American&Indian/Alaska&Native& Asian& African&American/Black&& Native&Hawaiian/Pacific&Islander& White/Caucasian& &Ethnicity:& Central/South&American& Cuban& Mexican& Puerto&Rican&& Other&Hispanic/Latino& NonFHispanic/Latino&
Preferred&Language:&________________& Marital&Status:!_________________&
Employment:!�&Employed&&�&Medical&Disability&�&SelfFEmployed&&�&Retired&&�&Unemployed&
Employer:&____________________&Employer&Address:&___________________&
Emergency&Contact:&_____________________&Relation:&__________________!
Address:&______________________________&Phone&#&___________________!
Pharmacy&Name:&________________________&Phone&#&__________________&
How&did&you&hear&about&us:&__________________________________________&
Primary!Physician!Information!
NAME:!__________________________________________________________&
ADDRESS:!______________________________________________________&
PHONE!#:!_______________________________________________________&
&
_____________________________________& &&&&&&&&&&_________________&Patient’s&Signature& & & & & & Date&

!
!
Insurance!Information!
Primary!Insurance!
Name&of&Policy&Holder/Guarantor:&_______________________&DOB:&________&
Relationship&to&Patient:&______________________&SSN#:&_________________&
Policy&Holder/Guarantor’s&Address:&____________________________________&
Status:&!Employed&&&&Medical&Disability&&&&&&&&&&&SelfFEmployed&&&&&&&&&&&&&Retired&&&&&&&&&&&&Unemployed&
Employer:&____________________&Employer&Address:&__________________&
Insurance&Company:&_______________________________________________&
Insured’s&Policy/&ID&#:&____________________&Group&#:&__________________&
Insurance&Co.&Address:&_______________________&Phone&#:&______________&
&&&&&&&&&&&&Name&of&Lab&Determined&by&Insurance:&______________________________________&
FFFFFFFFFFFFFF&DO&YOU&HAVE&ANY&ADDITIONAL&INSURANCE?&&&Yes&&&No&FFFFFFFFFFFFFF&
IF&YES,&PLEASE&COMPLETE&THE&FOLLOWING:&
Secondary!Insurance!
Name&of&Policy&Holder/Guarantor:&_______________________&DOB:&________&
Relationship&to&Patient:&______________________&SSN#:&_________________&
Policy&Holder/Guarantor’s&Address:&____________________________________&
Status:!�&Employed&&�&Medical&Disability&�&SelfFEmployed&&�&Retired&&�&Unemployed&
Employer:&____________________&Employer&Address:&__________________&
Insurance&Company&Address:&________________________________________&
Insured’s&Policy/&ID&#:&____________________&Group&#:&__________________&
Insurance&Co.&Address:&_______________________&Phone&#:&______________&
&
PLEASE&PROVIDE&INSURANCE&CARDS&AND&PICTURE&ID&TO&FRONT&DESK&
MAKE&CHECKS&PAYABLE&TO&“HUMG”&
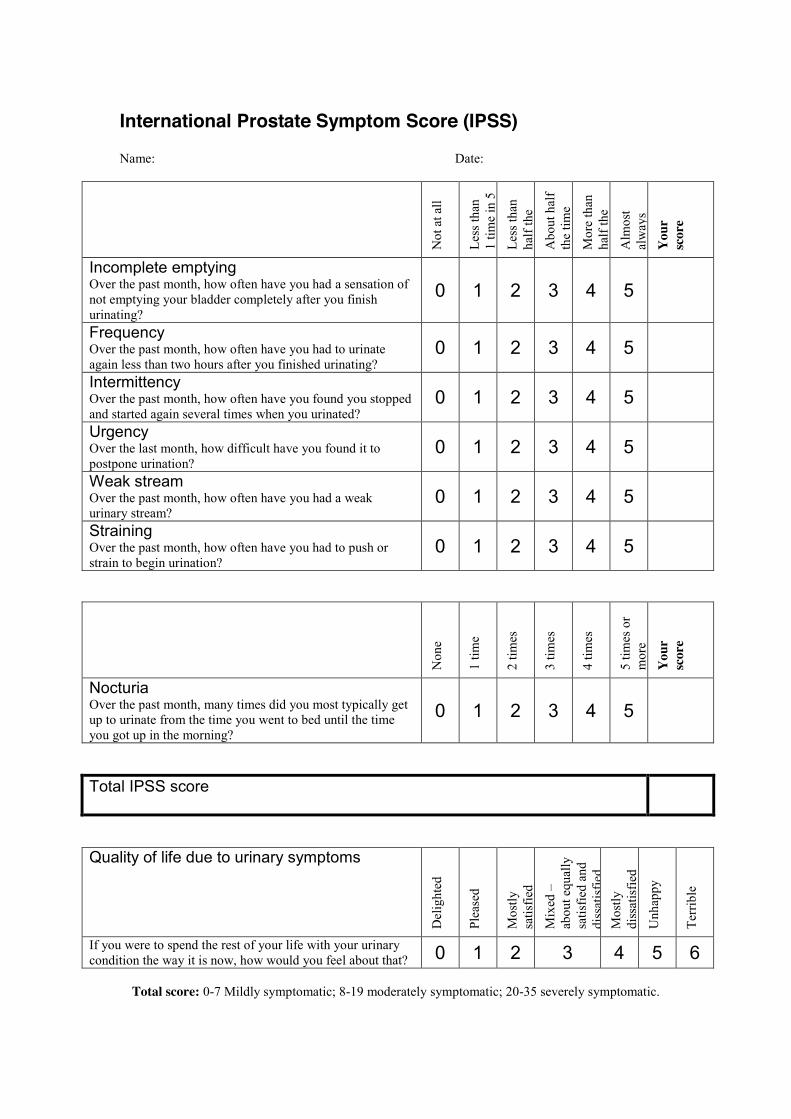
International Prostate Symptom Score (IPSS) Name: Date:
Not
at a
ll
Less
than
1
time
in 5
Less
than
ha
lf th
e tim
e A
bout
hal
f th
e tim
e
Mor
e th
an
half
the
time
Alm
ost
alw
ays
You
r sc
ore
Incomplete emptying Over the past month, how often have you had a sensation of not emptying your bladder completely after you finish urinating?
0 1 2 3 4 5
Frequency Over the past month, how often have you had to urinate again less than two hours after you finished urinating?
0 1 2 3 4 5
Intermittency Over the past month, how often have you found you stopped and started again several times when you urinated?
0 1 2 3 4 5
Urgency Over the last month, how difficult have you found it to postpone urination?
0 1 2 3 4 5
Weak stream Over the past month, how often have you had a weak urinary stream?
0 1 2 3 4 5
Straining Over the past month, how often have you had to push or strain to begin urination?
0 1 2 3 4 5
Non
e
1 tim
e
2 tim
es
3 tim
es
4 tim
es
5 tim
es o
r m
ore
You
r sc
ore
Nocturia Over the past month, many times did you most typically get up to urinate from the time you went to bed until the time you got up in the morning?
0 1 2 3 4 5
Total IPSS score
Quality of life due to urinary symptoms D
elig
hted
Plea
sed
Mos
tly
satis
fied
Mix
ed –
ab
out e
qual
ly
satis
fied
and
diss
atis
fied
Mos
tly
diss
atis
fied
Unh
appy
Terr
ible
If you were to spend the rest of your life with your urinary condition the way it is now, how would you feel about that? 0 1 2 3 4 5 6
Total score: 0-7 Mildly symptomatic; 8-19 moderately symptomatic; 20-35 severely symptomatic.

International Index of Erectile Function (IIEF) Questionnaire Please circle the appropriate numbers below
Patient Name _______________________________________ Today’s Date ___________________________
1. How often were you able to get an erection during sexual activity?
0 no sexual activity
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
2. When you had erections with sexual stimulation, how often were your erections hard enough for penetration?
0 no sexual activity
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
3. When you attempted sexual intercourse, how often were you able to penetrate (enter) your partner?
0 did not attempt
intercourse
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
4. During sexual intercourse, how often were you able to maintain your erection after you had penetrated (entered) your partner?
0 did not attempt
intercourse
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
5. During sexual intercourse, how difficult was it to maintain your erection to completion of intercourse?
0 did not attempt
intercourse
1 extremely difficult
2 very difficult
3 difficult
4 slightly difficult
5 not
difficult
6. How many times have you attempted sexual intercourse?
0 no attempts
1 one to two attempts
2 three to four
attempts
3 five to six attempts
4 seven to ten
attempts
5 eleven + attempts
7. When you attempted sexual intercourse, how often was it satisfactory?
0 did not attempt
intercourse
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
8. How much have you enjoyed sexual intercourse?
0 no intercourse
1 no
enjoyment
2 not very
enjoyable
3 fairly
enjoyable
4 highly
enjoyable
5 very highly enjoyable
9. When you had sexual stimulation or intercourse, how often did you ejaculate?
0 no sexual
stimulation/ intercourse
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
10. When you had sexual stimulation or intercourse, how often did you have the feeling of orgasm or climax?
0 no sexual
stimulation/ intercourse
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
11. How often have you felt sexual desire?
1 almost never
2 a few times
3 sometimes
4 most times
5 almost always
12. How would you rate your level of sexual desire?
1 very low/ none at all
2 low
3 moderate
4 high
5 very high
13. How satisfied have you been with your overall sex life?
1 very
dissatisfied
2 moderately dissatisfied
3 about equally satisfied and dissatisfied
4 moderately
satisfied
5 very
satisfied
14. How satisfied have you been with your sexual relationship with your partner?
1 very
dissatisfied
2 moderately dissatisfied
3 about equally satisfied and dissatisfied
4 moderately
satisfied
5 very
satisfied
15. How do you rate your confidence that you could get and keep an erection?
1 very low
2 low
3 moderate
4 high
5 very high
SHIM: 2, 4, 5, 7, 15: ___________


Revised 3/21/2013
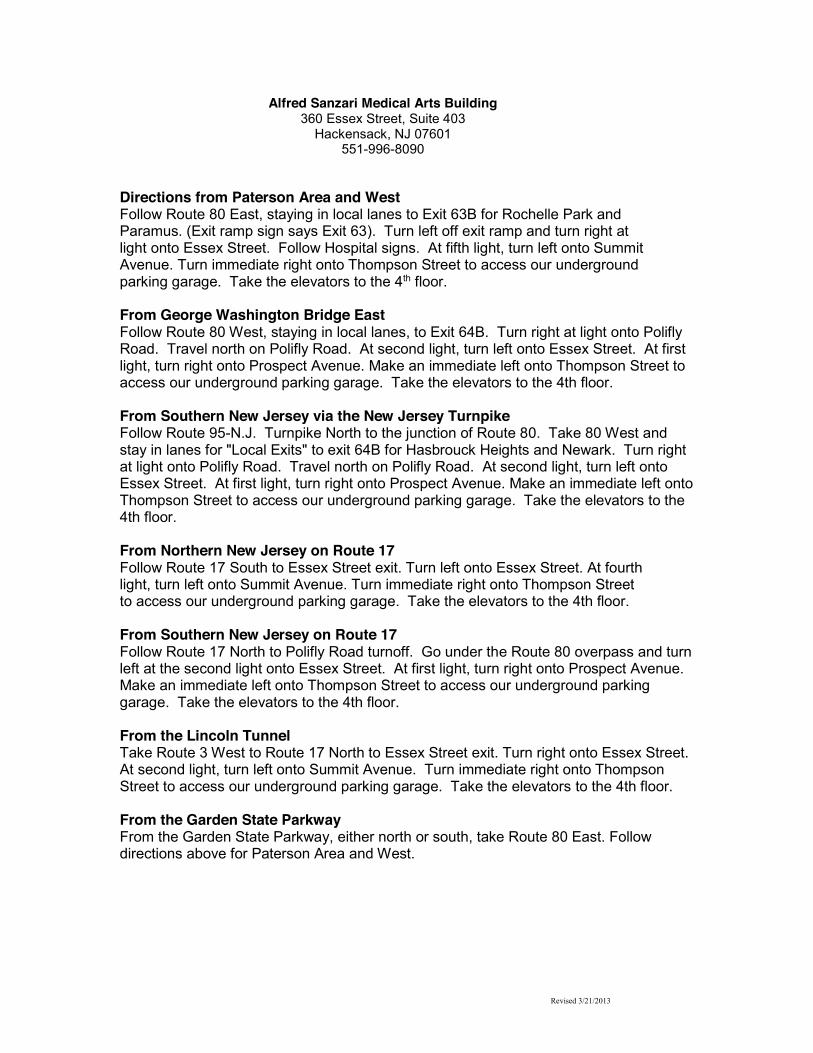
Alfred Sanzari Medical Arts Building 360 Essex Street, Suite 403
Hackensack, NJ 07601 551-996-8090
Directions from Paterson Area and West Follow Route 80 East, staying in local lanes to Exit 63B for Rochelle Park and Paramus. (Exit ramp sign says Exit 63). Turn left off exit ramp and turn right at light onto Essex Street. Follow Hospital signs. At fifth light, turn left onto Summit Avenue. Turn immediate right onto Thompson Street to access our underground parking garage. Take the elevators to the 4th floor.
From George Washington Bridge East Follow Route 80 West, staying in local lanes, to Exit 64B. Turn right at light onto Polifly Road. Travel north on Polifly Road. At second light, turn left onto Essex Street. At first light, turn right onto Prospect Avenue. Make an immediate left onto Thompson Street to access our underground parking garage. Take the elevators to the 4th floor. From Southern New Jersey via the New Jersey Turnpike Follow Route 95-N.J. Turnpike North to the junction of Route 80. Take 80 West and stay in lanes for "Local Exits" to exit 64B for Hasbrouck Heights and Newark. Turn right at light onto Polifly Road. Travel north on Polifly Road. At second light, turn left onto Essex Street. At first light, turn right onto Prospect Avenue. Make an immediate left onto Thompson Street to access our underground parking garage. Take the elevators to the 4th floor. From Northern New Jersey on Route 17 Follow Route 17 South to Essex Street exit. Turn left onto Essex Street. At fourth light, turn left onto Summit Avenue. Turn immediate right onto Thompson Street to access our underground parking garage. Take the elevators to the 4th floor. From Southern New Jersey on Route 17 Follow Route 17 North to Polifly Road turnoff. Go under the Route 80 overpass and turn left at the second light onto Essex Street. At first light, turn right onto Prospect Avenue. Make an immediate left onto Thompson Street to access our underground parking garage. Take the elevators to the 4th floor.
From the Lincoln Tunnel Take Route 3 West to Route 17 North to Essex Street exit. Turn right onto Essex Street. At second light, turn left onto Summit Avenue. Turn immediate right onto Thompson Street to access our underground parking garage. Take the elevators to the 4th floor.
From the Garden State Parkway From the Garden State Parkway, either north or south, take Route 80 East. Follow directions above for Paterson Area and West.

HBF #5005787 Rev. 2/2012
Hackensack University Medical Center Campus Map