guru ravidas ayurved university, · pdf fileguru ravidas ayurved university, punjab ... hours...
TRANSCRIPT
1
Guru Ravidas Ayurved University, Punjab
Proforma for Inspection Faculty of Homoeopathy
for BHMS
Inspectors 1)
2)
Date of Inspection / Time of Inspection
Name of the College / Institute / Principal
With Complete address, Office / Resi /
Cell & E-mail Address
Status of Payment of previous affiliation fee
i) Details of outstanding affiliation fee (Year wise) :Rs……………………………..
ii) Payment of affiliation fee for the year
Continuation / Extension affiliation is sought : Paid / Not paid
iii) Reasons for non-payment of above affiliation Fee :………………………………...
(i) Name of the Management / Society /
Trust
(ii) If private, then date of registration of
Society / Trust with registration No.
Whether
(i) Allowed by the State Govt.
(ii) (a) Present status of affiliated (b) Provisional (c) Year (attach a letter of affiliating body) Permanent
(i) Name of Course -
allowed / running –
(ii) Course wise intake capacity -
(iii) Actual No. of Admissions made in 1-year of Year Admitted Vacant
course for last 3 sessions –
Criteria of Admission course wise :
2
(i) Student – bed ratio :
(ii) Student – peripheral dispensary ratio:
(iii) What – option given among (i) & (ii) if it is Prior to 12.09.02 :
(iv) Mention Attached Hospital & Peripheral
Centres Where Internship training is
imparted along with name of depts. in it.
6. Eligibility Qualification (coursewise)
7. (i) Admission Procedure (coursewise)
(Merit / Admission test / Counselling)
(ii) Authority regulating admissions
8. Coursewise Fee Structures
BHMS
1) Payment Seat
2) Free Seat
3) NRI Quota
4) Any other (including SC / ST/ OBC/ etc.)
M.D. (Hom)
Regular
External
5) Hostel charges
09. i) Details of Apex Body of College / Instt.
(see regulation 3 of H (M.S.E.) Amendment Regulations, 2002).
ii) How frequency Apex Body meets
iii) Details of recommendation of Apex Body in last one year
10. Accommodation :-
1. Ownership of land
(owned / lease / rent )
(Attach attested documents copies)
2. Total area of land for College
(for college/ hospital / hostel / Qtrs. Separately for hospital including open land) for hostel
for Quarters
Open land for play ground
Herbartum land
3
3. Covered Area
(i) For college
(ii) For Hospital
(iii) For Staff Quarters
(iv) Hostels Male
Female
11 A) # Teaching departments maintained for (Give Brief Description of covered area or area marked for)
: Anatomy with Dissection hall+Museum+Department Library Sq. Area…….
: Physiology / Biochemistry – Laboratory+Museum+Departmental Sq. Area…….
Library
: Pharmacy + Laboratory + Herbgarden+ Department Library = Sq. Area…….
: Pathology Laboratory + Museum +Department Library = Sq. Area…….
: P.S. M. – Museum + Department Library = Sq. Area ……
: F.M.T. – Museum + Department Library = Sq. Area…….
: Medicine & Paediatrics + Department Library = Sq. Area…….
: Surgery including E.N.T. & Eye + Department Library = Sq. Area…….
: Obst. / Gynaecology + Department Library = Sq. Area…….
: Materia Medica & Therapeutics + Department Library = Sq. Area…….
: Organon of Medicine / Philosophy + Department Library = Sq. Area…….
: Homoeo. Repertory + Department Library = Sq. Area…….
B) Class rooms : --------C) Seminar room:----------D) Administrative Sq. Area ……
Block -------------- (sitting capacity in each class room) =
E) Auditorium -------------- F) Library ----------------------= Sq. Area…….
(including office of librarian, Reading Room for students & Sq. Area…….
Staff separately) = 12. Payscale Adopted for employees of all categories to be enclosed ------------------------
Approved BY-------------------
Mode of payment By Cheque / Cash / Bank Transfer in Payees Accounts -------------
Whether C.P.F. / G.P.F. deducted, if so since when -------------- and with whom
deposited --------------
Whether Income Tax deducted (at source from salary) & deposited regularly
(Yes / No) -----------
4
Copy of appointment order of principal, teachers and hospital staff including Full
Time and Guest Faculty be asked during inspection, verified-------------------------------
Copies of audited / unaudited Annual Accounts of the College & attached
Homoeopathic Hospital as well as of management since last inspection or for last
year be examined (to corroborate information in respect of points 10 to 12 above)
and appended. The Zerox attested copies essential.
Annual budget (Plan) Rs. -------------------- (Non - Plan) Rs. -------------------for current session.
Annual expenditure during last year ---------------------------------------------------------------
Capital Investment (Headwise) for current session -------------------------------------------- for last year -----------------------------------------------------
Pay of Staff and Establishment of last 12 months
(Separately cadrewise)
1) -----------------------------------------------------------------------------------------------------------
2) -----------------------------------------------------------------------------------------------------------
3) -----------------------------------------------------------------------------------------------------------
4) -----------------------------------------------------------------------------------------------------------
5) -----------------------------------------------------------------------------------------------------------
6) -----------------------------------------------------------------------------------------------------------
7) -----------------------------------------------------------------------------------------------------------
8) -----------------------------------------------------------------------------------------------------------
9) -----------------------------------------------------------------------------------------------------------
10)-----------------------------------------------------------------------------------------------------------
11)-----------------------------------------------------------------------------------------------------------
12)-----------------------------------------------------------------------------------------------------------
Medicine & Stores (of last 12 months) Expenditure -------------------------------------------
Diet Expenditure (of last 12 months) --------------------------------------------------------------
Non – recurring contingency (of last 12 months) -----------------------------------------------
Budget estimates for next year ----------------------------------------------------------------------
Ambulance, if provided – (monthly expenditure & income of it)-----------------------------
(year make and in whose name is the Registration of Vehicle)
5
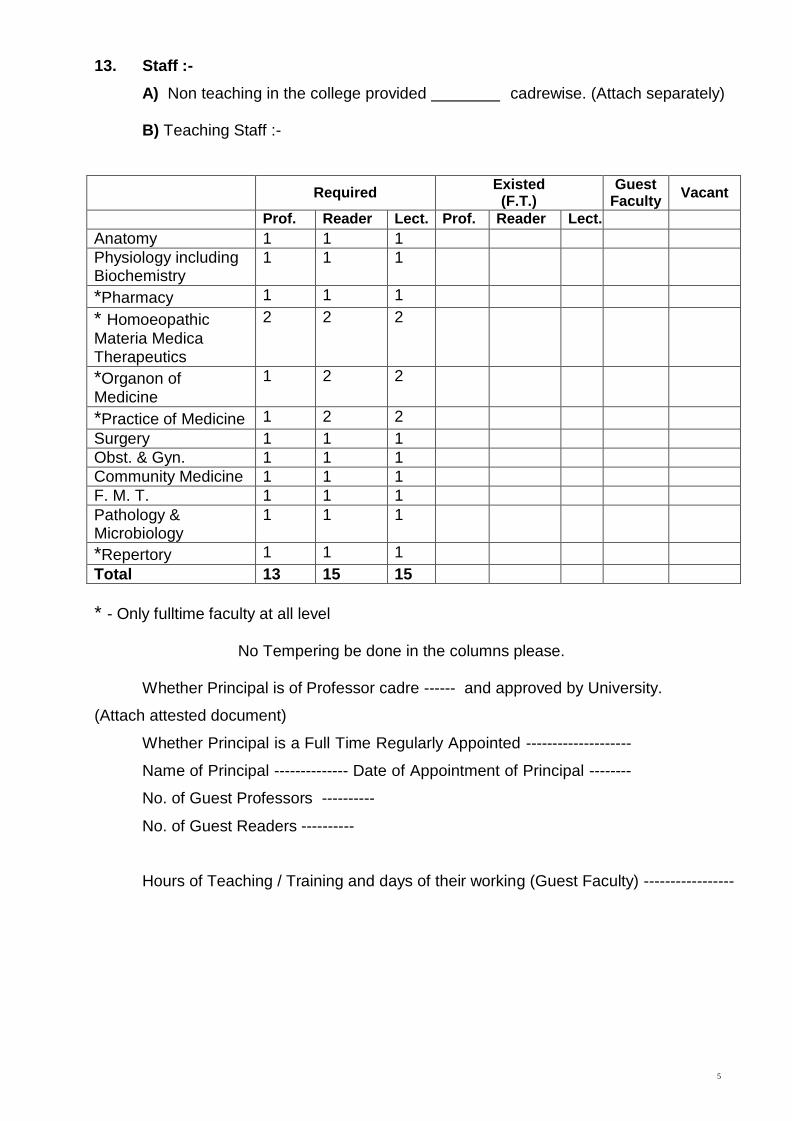
13. Staff :-
A) Non teaching in the college provided
cadrewise. (Attach separately)
B) Teaching Staff :-
Required Existed (F.T.)
Guest Faculty
Vacant
Prof. Reader Lect. Prof. Reader Lect.
Anatomy 1 1 1
Physiology including Biochemistry
1 1 1
*Pharmacy 1 1 1
* Homoeopathic
Materia Medica Therapeutics
2 2 2
*Organon of Medicine
1 2 2
*Practice of Medicine 1 2 2
Surgery 1 1 1
Obst. & Gyn. 1 1 1
Community Medicine 1 1 1
F. M. T. 1 1 1
Pathology & Microbiology
1 1 1
*Repertory 1 1 1
Total 13 15 15
* - Only fulltime faculty at all level
No Tempering be done in the columns please.
Whether Principal is of Professor cadre ------ and approved by University.
(Attach attested document)
Whether Principal is a Full Time Regularly Appointed --------------------
Name of Principal -------------- Date of Appointment of Principal --------
No. of Guest Professors ----------
No. of Guest Readers ----------
Hours of Teaching / Training and days of their working (Guest Faculty) -----------------
6
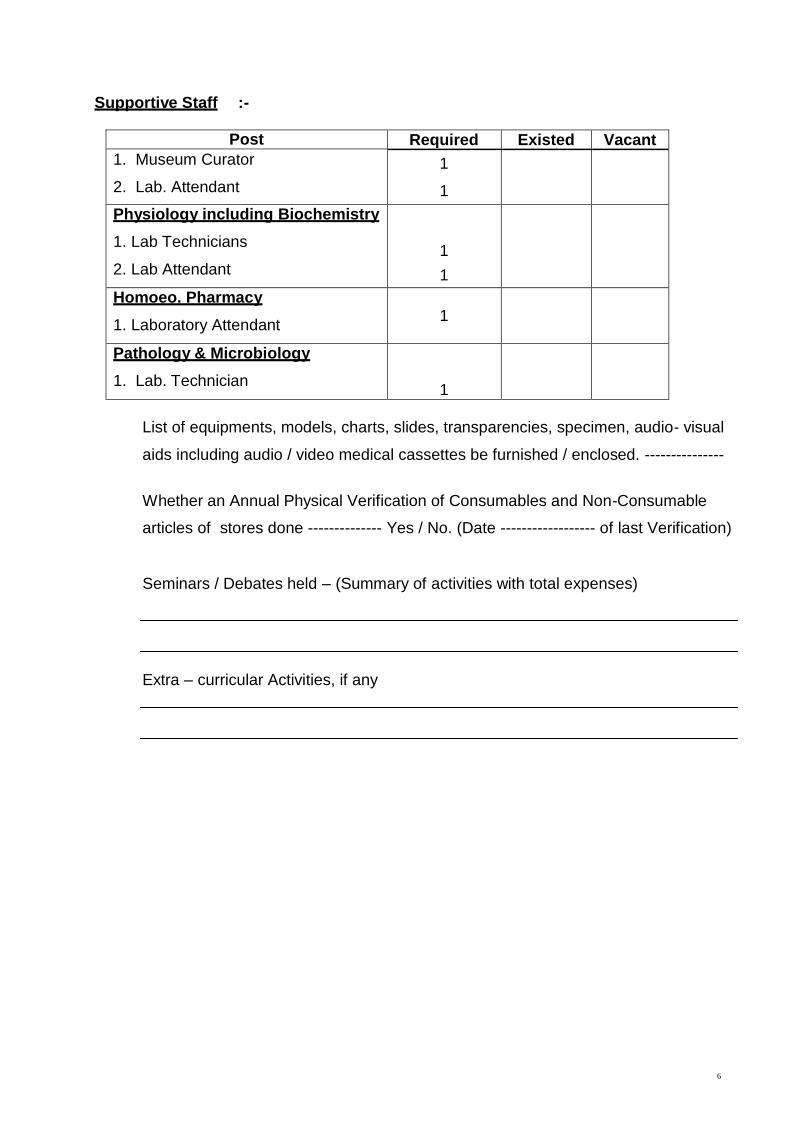
Supportive Staff :-
Post Required Existed Vacant
1. Museum Curator
2. Lab. Attendant
1
1
Physiology including Biochemistry
1. Lab Technicians
2. Lab Attendant
1
1
Homoeo. Pharmacy
1. Laboratory Attendant
1
Pathology & Microbiology
1. Lab. Technician
1
List of equipments, models, charts, slides, transparencies, specimen, audio- visual
aids including audio / video medical cassettes be furnished / enclosed. ---------------
Whether an Annual Physical Verification of Consumables and Non-Consumable
articles of stores done -------------- Yes / No. (Date ------------------ of last Verification)
Seminars / Debates held – (Summary of activities with total expenses)
Extra – curricular Activities, if any
7
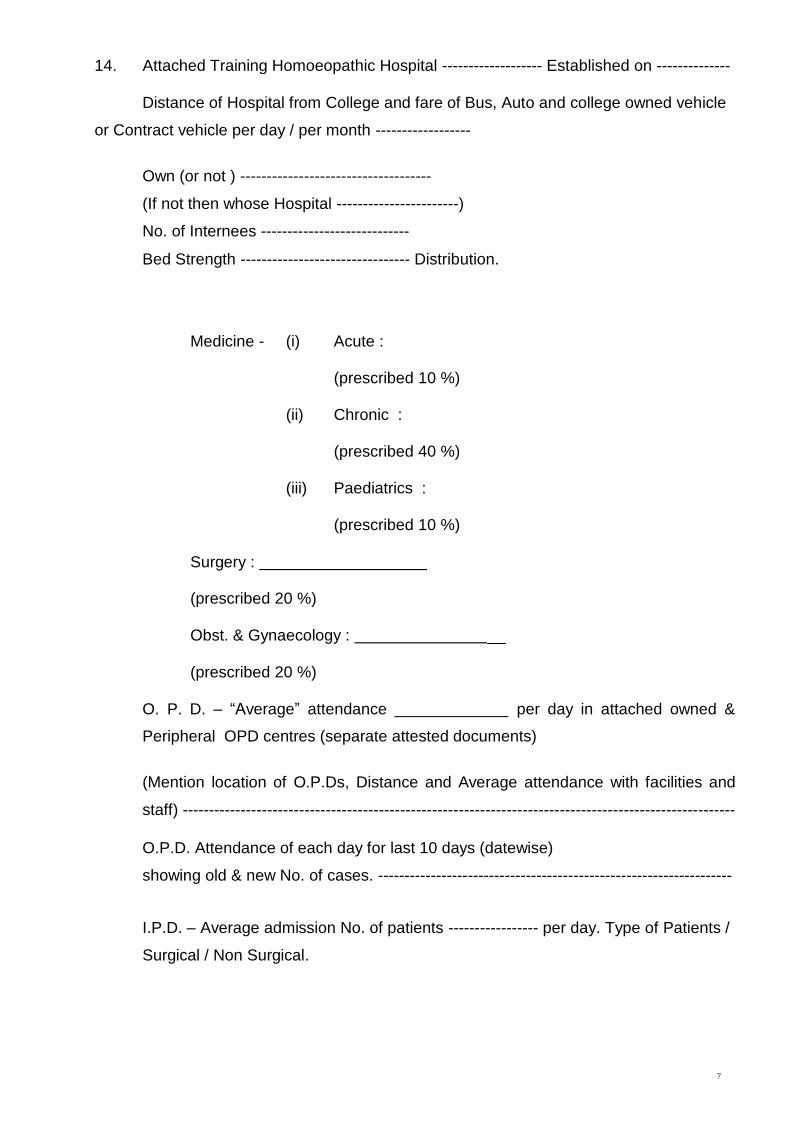
14. Attached Training Homoeopathic Hospital ------------------- Established on --------------
Distance of Hospital from College and fare of Bus, Auto and college owned vehicle
or Contract vehicle per day / per month ------------------
Own (or not ) ------------------------------------
(If not then whose Hospital -----------------------)
No. of Internees ----------------------------
Bed Strength -------------------------------- Distribution.
Medicine - (i) Acute :
(prescribed 10 %)
(ii)
Chronic :
(prescribed 40 %)
(iii)
Paediatrics :
(prescribed 10 %)
Surgery :
(prescribed 20 %)
Obst. & Gynaecology :
(prescribed 20 %)
O. P. D. – “Average” attendance per day in attached owned &
Peripheral OPD centres (separate attested documents)
(Mention location of O.P.Ds, Distance and Average attendance with facilities and
staff) --------------------------------------------------------------------------------------------------------
O.P.D. Attendance of each day for last 10 days (datewise)
showing old & new No. of cases. -------------------------------------------------------------------
I.P.D. – Average admission No. of patients ----------------- per day. Type of Patients /
Surgical / Non Surgical.
8
Average discharge No. of patients --------------------- per day.
O. P. D. patients admitted on each day in last 7 days date wise & No. of discharged patients on these days
1) -----------------------------------------------------------------------------------------------------------
2) -----------------------------------------------------------------------------------------------------------
3) -----------------------------------------------------------------------------------------------------------
4) -----------------------------------------------------------------------------------------------------------
5) -----------------------------------------------------------------------------------------------------------
6) -----------------------------------------------------------------------------------------------------------
7) -----------------------------------------------------------------------------------------------------------
8) -----------------------------------------------------------------------------------------------------------
9) -----------------------------------------------------------------------------------------------------------
10)-----------------------------------------------------------------------------------------------------------
Medical camps held – (Summary of activities with details of fees for patients) –
---------------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------------------
Brief information –
(a) Radiology / ultrasound ------------------------------
(b) Physical Medicine and Rehabilitation ------------------------------
(c) Yoga & Naturopathy practice Facility ------------------------------
(d) Operation Theatres ------------------------------
(e) Dental Clinic ------------------------------
(f) Psychiatry Clinic ------------------------------
9
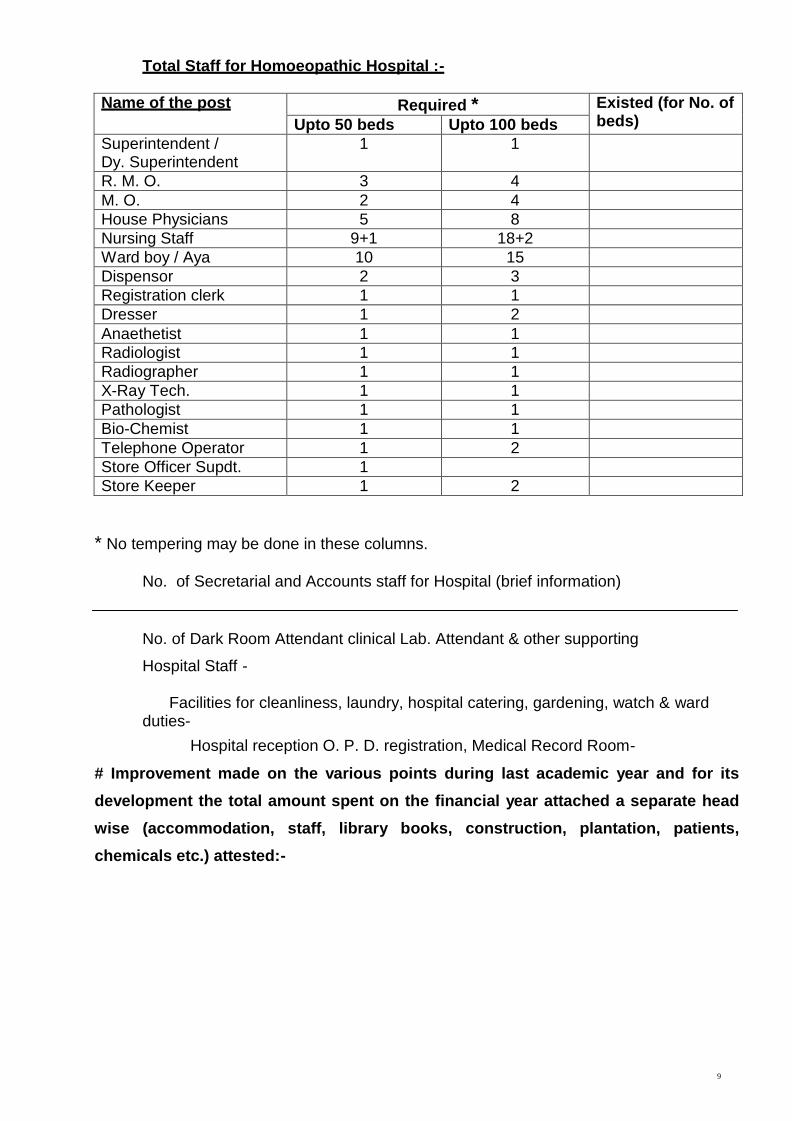
Total Staff for Homoeopathic Hospital :-
Name of the post Required * Existed (for No. of
beds) Upto 50 beds Upto 100 beds
Superintendent / Dy. Superintendent
1 1
R. M. O. 3 4
M. O. 2 4
House Physicians 5 8
Nursing Staff 9+1 18+2
Ward boy / Aya 10 15
Dispensor 2 3
Registration clerk 1 1
Dresser 1 2
Anaethetist 1 1
Radiologist 1 1
Radiographer 1 1
X-Ray Tech. 1 1
Pathologist 1 1
Bio-Chemist 1 1
Telephone Operator 1 2
Store Officer Supdt. 1
Store Keeper 1 2
* No tempering may be done in these columns.
No. of Secretarial and Accounts staff for Hospital (brief information)
No. of Dark Room Attendant clinical Lab. Attendant & other supporting
Hospital Staff -
Facilities for cleanliness, laundry, hospital catering, gardening, watch & ward duties-
Hospital reception O. P. D. registration, Medical Record Room-
# Improvement made on the various points during last academic year and for its
development the total amount spent on the financial year attached a separate head
wise (accommodation, staff, library books, construction, plantation, patients,
chemicals etc.) attested:-
10
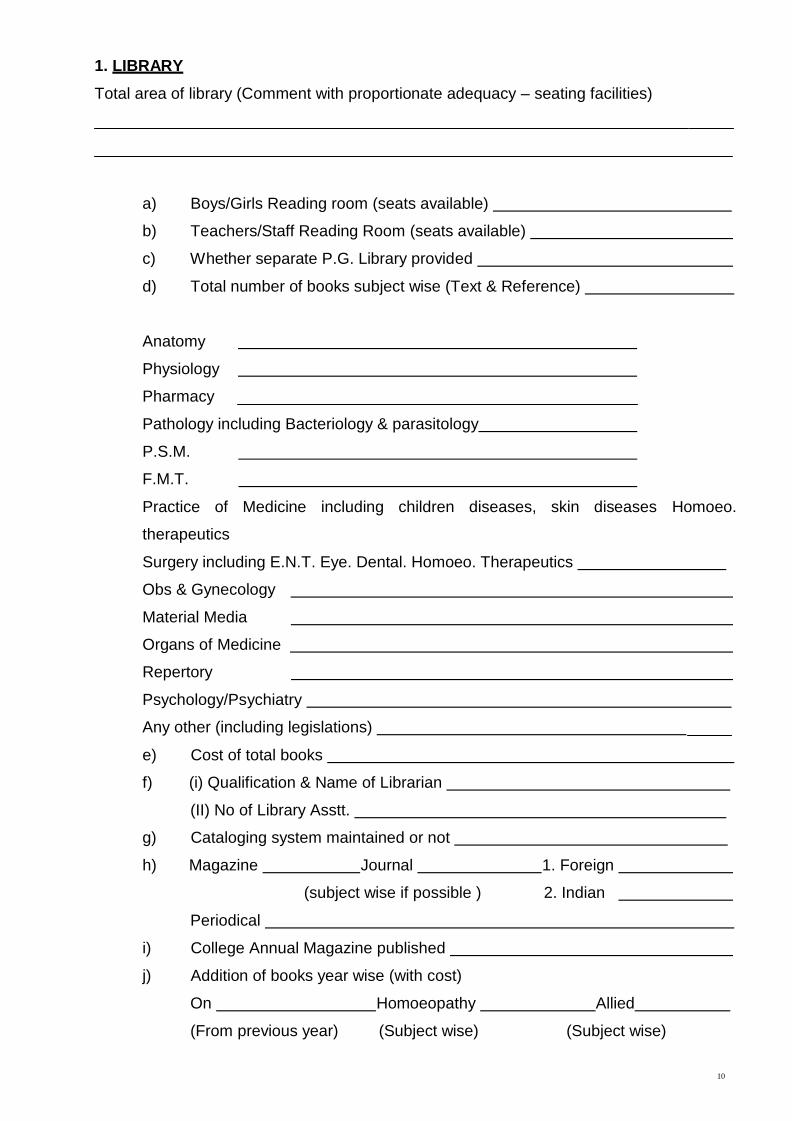
1. LIBRARY
Total area of library (Comment with proportionate adequacy – seating facilities)
a) Boys/Girls Reading room (seats available)
b) Teachers/Staff Reading Room (seats available)
c) Whether separate P.G. Library provided
d) Total number of books subject wise (Text & Reference)
Anatomy
Physiology
Pharmacy
Pathology including Bacteriology & parasitology
P.S.M.
F.M.T.
Practice of Medicine including children diseases, skin diseases Homoeo.
therapeutics
Surgery including E.N.T. Eye. Dental. Homoeo. Therapeutics
Obs & Gynecology
Material Media
Organs of Medicine
Repertory
Psychology/Psychiatry
Any other (including legislations)
e) Cost of total books
f) (i) Qualification & Name of Librarian
(II) No of Library Asstt.
g) Cataloging system maintained or not
h) Magazine Journal 1. Foreign
(subject wise if possible ) 2. Indian
Periodical
i) College Annual Magazine published
j) Addition of books year wise (with cost)
On Homoeopathy Allied
(From previous year) (Subject wise) (Subject wise)
11
k) Daily issue of books to students- U.G.
P.G.
To teachers_
l) Rules of library maintained Yes/No
m) Annual Physical verification done on
n) Book Bank facility
o) Computer facilities (with internet)-
p) Whether copying facilities available
Any publication teaching staff
Remarks:-
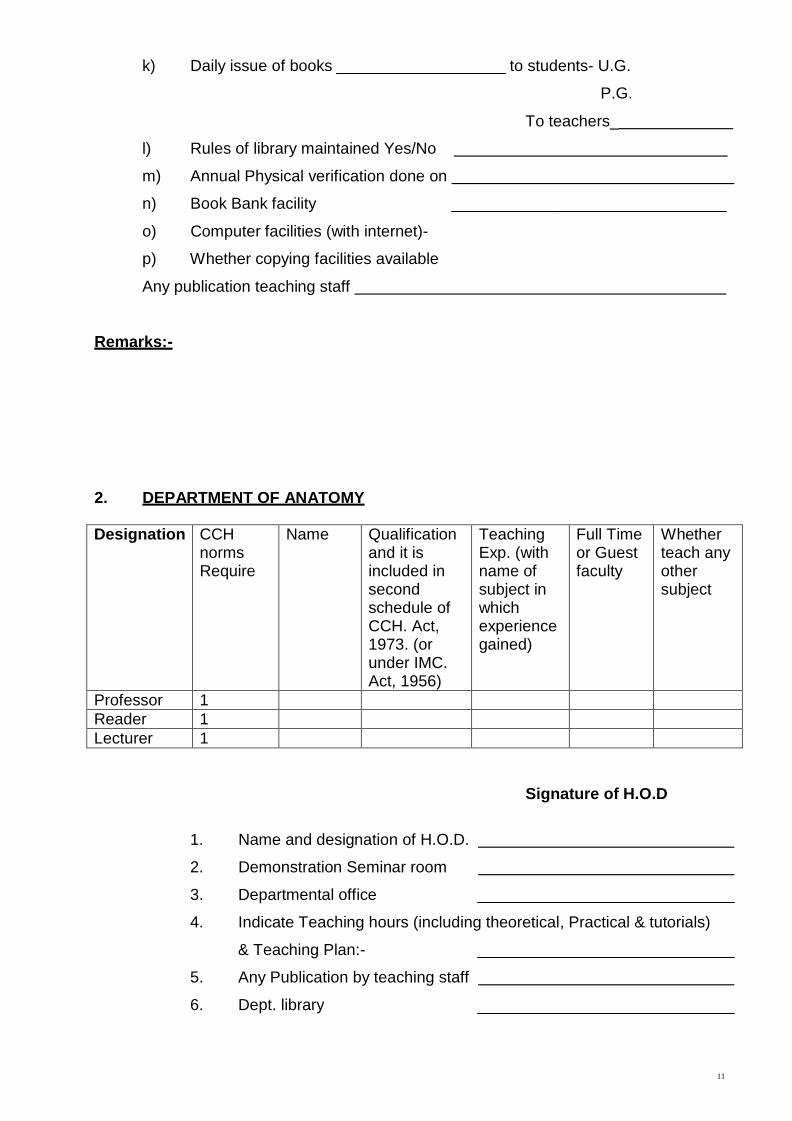
2. DEPARTMENT OF ANATOMY
Designation CCH norms Require
Name Qualification and it is included in second schedule of CCH. Act, 1973. (or under IMC. Act, 1956)
Teaching Exp. (with name of subject in which experience gained)
Full Time or Guest faculty
Whether teach any other subject
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D
1. Name and designation of H.O.D.
2. Demonstration Seminar room
3. Departmental office
4. Indicate Teaching hours (including theoretical, Practical & tutorials)
& Teaching Plan:-
5. Any Publication by teaching staff
6. Dept. library
12
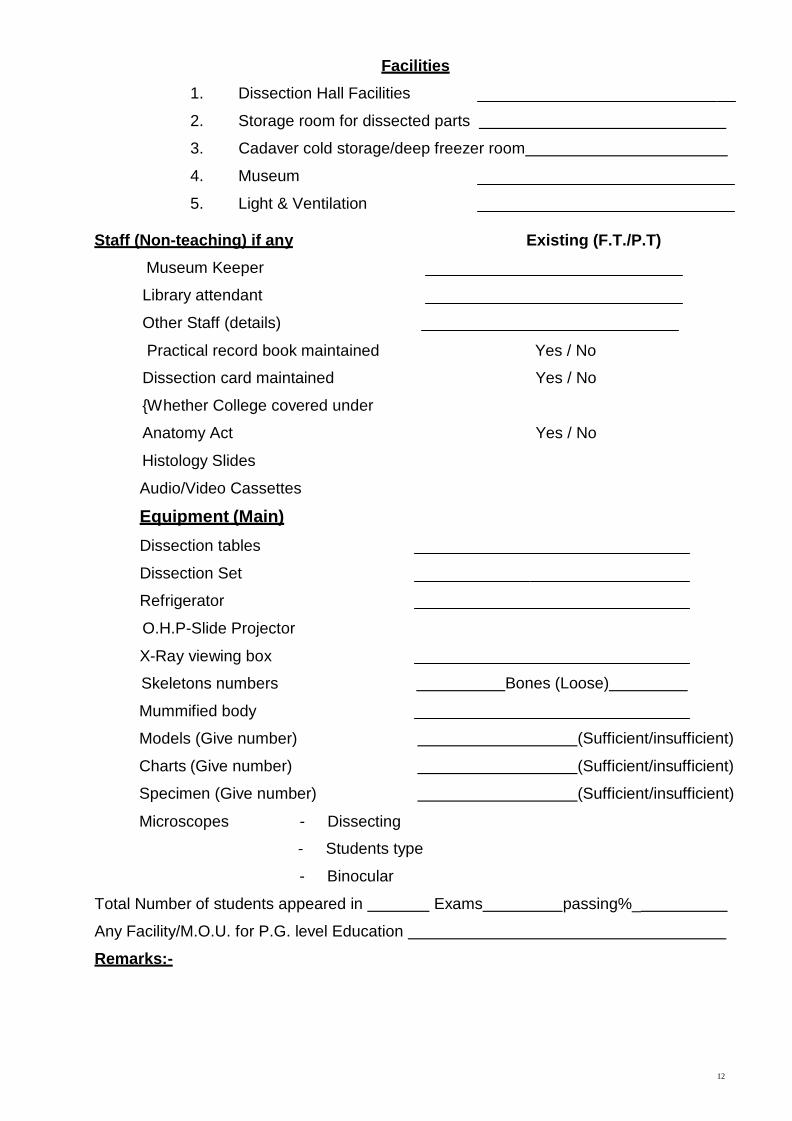
Facilities
1. Dissection Hall Facilities
2. Storage room for dissected parts
3. Cadaver cold storage/deep freezer room
4. Museum
5. Light & Ventilation
Staff (Non-teaching) if any Existing (F.T./P.T)
Museum Keeper
Library attendant
Other Staff (details)
Practical record book maintained Yes / No
Dissection card maintained Yes / No
{Whether College covered under
Anatomy Act Yes / No
Histology Slides
Audio/Video Cassettes
Equipment (Main)
Dissection tables
Dissection Set
Refrigerator
O.H.P-Slide Projector
X-Ray viewing box
Skeletons numbers
Mummified body
Models (Give number)
Charts (Give number)
Specimen (Give number)
Microscopes - Dissecting
Bones (Loose)
(Sufficient/insufficient)
(Sufficient/insufficient)
(Sufficient/insufficient)
- Students type
- Binocular
Total Number of students appeared in Exams passing%_
Any Facility/M.O.U. for P.G. level Education
Remarks:-
13
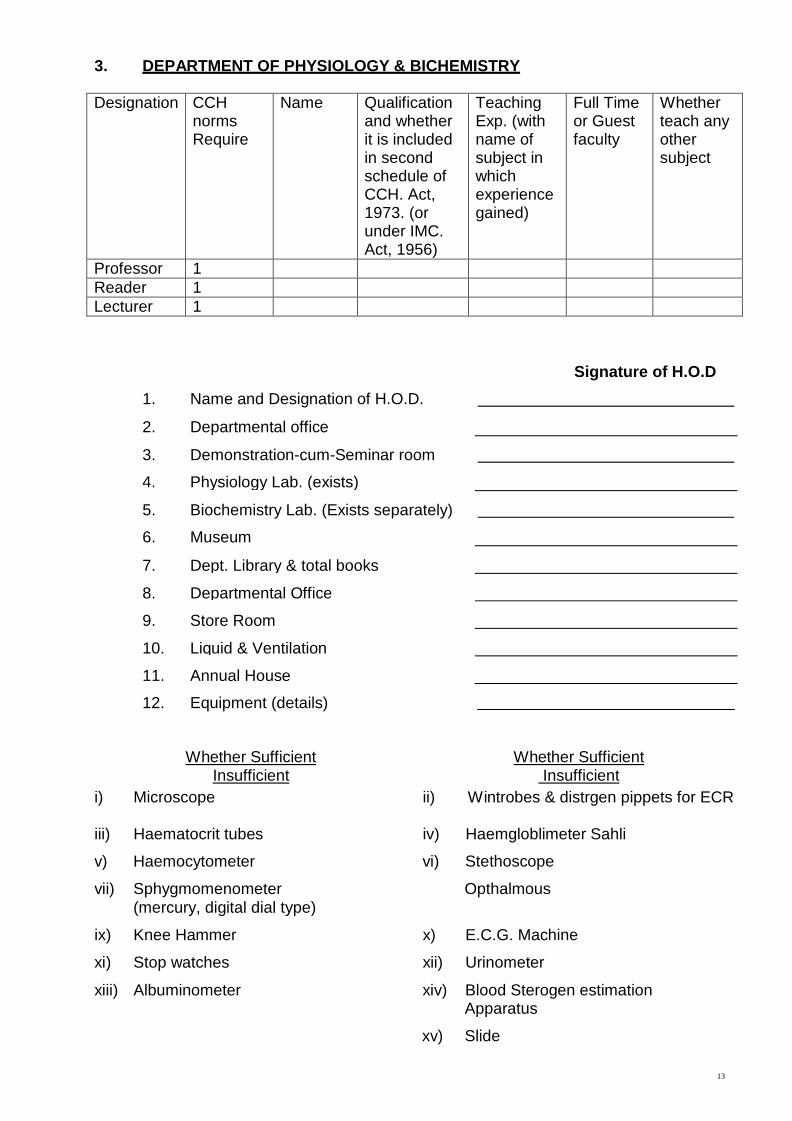
3. DEPARTMENT OF PHYSIOLOGY & BICHEMISTRY
Designation CCH
norms Require
Name Qualification and whether it is included in second schedule of CCH. Act, 1973. (or under IMC. Act, 1956)
Teaching Exp. (with name of subject in which experience gained)
Full Time or Guest faculty
Whether teach any other subject
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D
1. Name and Designation of H.O.D.
2. Departmental office
3.
Demonstration-cum-Seminar room
4. Physiology Lab. (exists)
5.
Biochemistry Lab. (Exists separately)
6. Museum
7.
Dept. Library & total books
8.
Departmental Office
9.
Store Room
10.
Liquid & Ventilation
11.
Annual House
12.
Equipment (details)
Whether Sufficient Insufficient
Whether Sufficient Insufficient
i) Microscope ii) Wintrobes & distrgen pippets for ECR
iii) Haematocrit tubes iv) Haemgloblimeter Sahli
v) Haemocytometer vi) Stethoscope
vii) Sphygmomenometer (mercury, digital dial type)
Opthalmous
ix) Knee Hammer x) E.C.G. Machine
xi) Stop watches xii) Urinometer
xiii) Albuminometer xiv) Blood Sterogen estimation Apparatus
xv) Slide
14
13) Indicate Teaching hours including theoretical Practical & tutorial & Teaching Plan ----------------------------------------------------------------------------------------------------
14) Any Publication by teaching staff ----------------------------------------------------------------------
Staff (non Teaching)
Lab Tech. ----------------------------------------------------------------------------------------------------------
Lab. Attendant ---------------------------------------------------------------------------------------------------
Other Staff details -----------------------------------------------------------------------------------------------
Total number of practicals conducted on human Physiology & Biochemistry during current
session -------------------------------------------------------------------------------------------------------------
Total number of Animal Experiments -----------------------------------(During current session)-
Total candidates appeared in exams. ------------------------------------Passing% --------------------
Any facility/O.U. for P.G. level Education ------------------------------------------------------------------
Signature of H.O.D.
Remarks:-
15
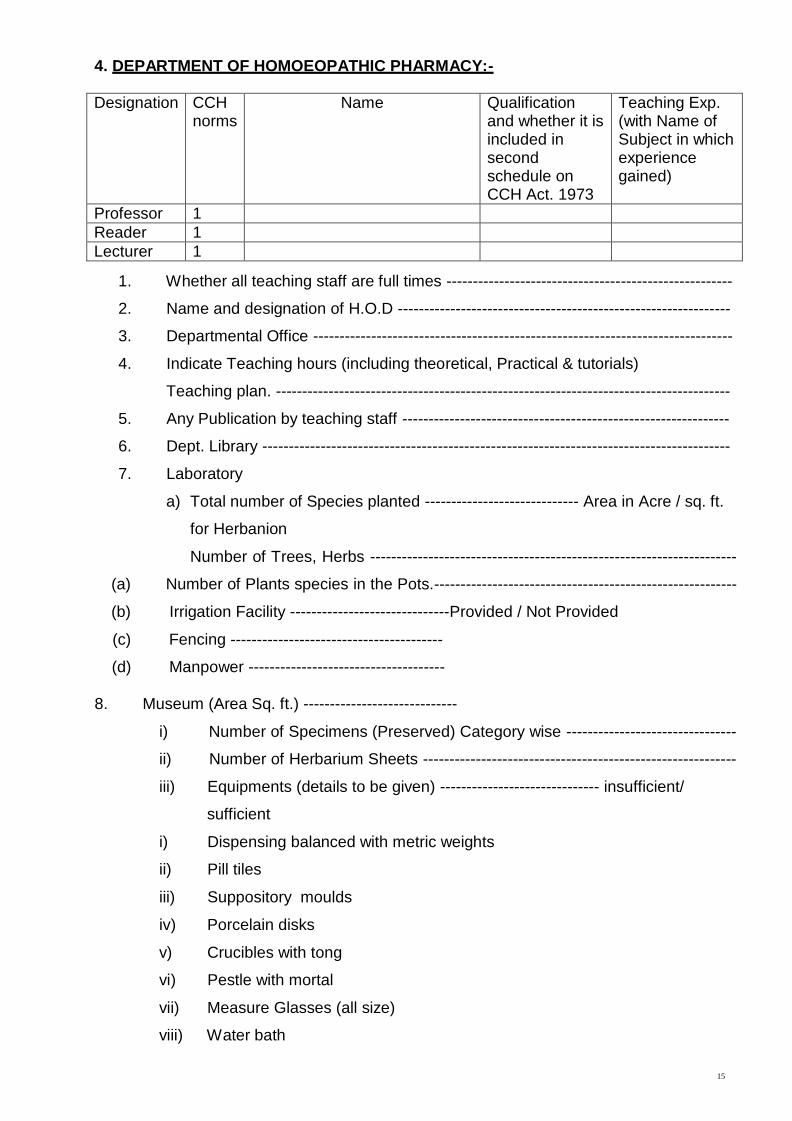
4. DEPARTMENT OF HOMOEOPATHIC PHARMACY:-
Designation CCH
norms
Name Qualification and whether it is included in second schedule on CCH Act. 1973
Teaching Exp. (with Name of Subject in which experience gained)
Professor 1
Reader 1
Lecturer 1
1. Whether all teaching staff are full times ------------------------------------------------------
2. Name and designation of H.O.D ---------------------------------------------------------------
3. Departmental Office -------------------------------------------------------------------------------
4. Indicate Teaching hours (including theoretical, Practical & tutorials)
Teaching plan. --------------------------------------------------------------------------------------
5. Any Publication by teaching staff --------------------------------------------------------------
6. Dept. Library ----------------------------------------------------------------------------------------
7. Laboratory
a) Total number of Species planted ----------------------------- Area in Acre / sq. ft.
for Herbanion
Number of Trees, Herbs ---------------------------------------------------------------------
(a) Number of Plants species in the Pots.---------------------------------------------------------
(b) Irrigation Facility ------------------------------Provided / Not Provided
(c) Fencing ----------------------------------------
(d) Manpower -------------------------------------
8. Museum (Area Sq. ft.) -----------------------------
i) Number of Specimens (Preserved) Category wise --------------------------------
ii) Number of Herbarium Sheets -----------------------------------------------------------
iii) Equipments (details to be given) ------------------------------ insufficient/
sufficient
i) Dispensing balanced with metric weights
ii) Pill tiles
iii) Suppository moulds
iv) Porcelain disks
v) Crucibles with tong
vi) Pestle with mortal
vii) Measure Glasses (all size)
viii) Water bath
16
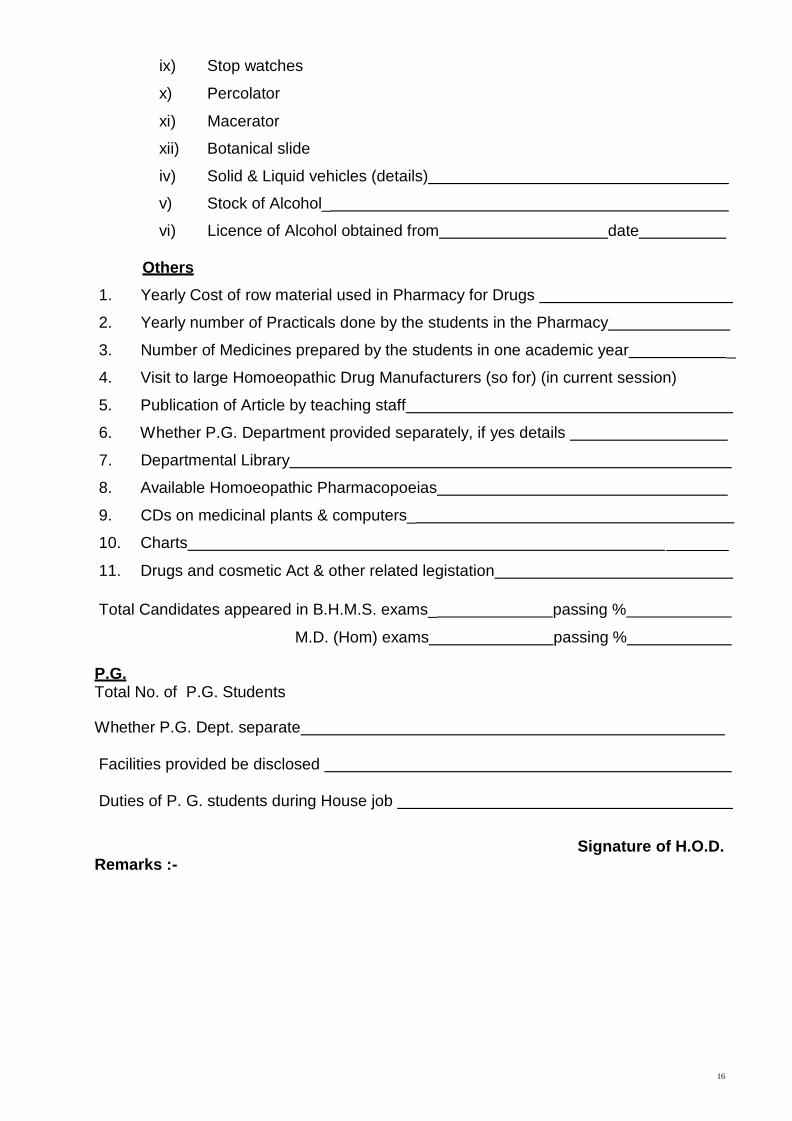
ix) Stop watches
x) Percolator
xi) Macerator
xii) Botanical slide
iv) Solid & Liquid vehicles (details)
v) Stock of Alcohol_
vi) Licence of Alcohol obtained from date
Others
1. Yearly Cost of row material used in Pharmacy for Drugs
2. Yearly number of Practicals done by the students in the Pharmacy
3. Number of Medicines prepared by the students in one academic year _
4. Visit to large Homoeopathic Drug Manufacturers (so for) (in current session)
5. Publication of Article by teaching staff
6. Whether P.G. Department provided separately, if yes details
7. Departmental Library
8. Available Homoeopathic Pharmacopoeias
9. CDs on medicinal plants & computers_
10. Charts
11. Drugs and cosmetic Act & other related legistation
Total Candidates appeared in B.H.M.S. exams_ passing %
M.D. (Hom) exams passing %
P.G. Total No. of P.G. Students
Whether P.G. Dept. separate
Facilities provided be disclosed
Duties of P. G. students during House job
Remarks :- Signature of H.O.D.
17
5. DEPARTMENT OF PATHOLOGY & MICROBIOLOGY
Designation CCH norms Require
Name Qualification and whether it is included in second schedule of CCH. Act, 1973. (or under I.M.C. Act, 1956)
Teaching Exp. (with name of subject in which experience gained)
Full Time or Guest faculty
Whether teach any other subject
Professor 1
Reader 1
Lecturer 1
1. Name of Designation of HOD
2. Dept. Library
3. Demonstration-cum-Seminar room
4. Museum
5. Departmental Office
6. Laboratory
7. Indicate teaching hours (including theoretical, practical & tutorials)
& Teaching plant
8.
Any publication by teaching staff
9.
Equipment :-
Microtome –Rotatory
Flat cutting
Hot plate
Haemocytometer
Hemoglobinometer
Microscopes
ESR
Centrifugal machine
Auto clave
Incubatory
Slide
18
10. Laboratory Technician
11. Charts 12. Specimen 13. Slide
Students appeared in B.H.M.S. exams_ passed %
Any facility / M.O.U. for P.G. level Education
Remarks:-
6. DEPARTMENT OF COMMUNITY MEDICINE:-
Signature of H.O.D.
Designation CCH
norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973 (of under I.M.C..Act. 1956)
Teaching Exp. (with Name of Subject in which experience gained)
Full Time or Guest faculty
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D.
1. Name and Designation of H.O.D. --------------------------------------------------------------
2. Indicate Teaching hours (including theoretical, practical & tutorials)
Teaching Plan---------------------------------------------------------------------------------------
3. Any publication by teaching staff ---------------------------------------------------------------
4. Museum ----------------------------------------------------------------------------------------------
5. Department Library --------------------------------------------------------------------------------
6. Other details -----------------------------------------------------------------------------------------

19
7. Equipments ------------------------------------------------------------------------------------------
1) Barometer----------------- 2) Filter Berke feid------------ 3) Hydrometer spirit-------
4) Hydrometer Milk--------- 5) Hydrometer water--------------------------------------------
8. Models
9. Charts
10. Specimen------------------ on food substances -------------- Sources of Vitamins------
11. Family planning/Welfare goods-------------- Devices---------- Demography-----------
12. Primary Health Centre ------------------- Nos -------------- Locations----------------------
13. Village adopted with name distance and activities undertaken ------------------------
-----------------------------------------------------------------------------------------------------------
14. Involvement in family planning Programme ------------------------------------------------
15. National Health Policy Programme – if any involvement:-
16. Health Camps ----------------- Organised and conducted on ------------------------- at
Place---------(Amount spent and received on it)
17. Field Visits, --------------------------------------------------
18. Transport facility on such camps by the colleges -----------------------------------------
19. Record maintained by the respective students-------------------------- in the current
precious academic session-------------------------------
20. Concept of immunization taught- Yes/No
21. Information on Homoeopathic propylaxis – Given/ Not given.
22. Total number of students in exams -------------- passing %-------------------------------
Signature of H.O.D.
Remarks:-
20
7. DEPARTMENT OF PRACTICE OF MEDICINE:-
Designation CCH
norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973 (of under I.M.C. Act, 1956)
Teaching Exp. (with Name of Subject in which experience gained )
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D.
1. Whether all teachers full time -------------------------------------------------------------------
2. Name and Designation of H.O.D.---------------------------------------------------------------
3. Indicate Teaching hours (including theoretical, practical & tutorials)
& Teaching Plan------------------------------------------------------------------------------------
4. Any publication by teaching staff ---------------------------------------------------------------
5. Department Library --------------------------------------------------------------------------------
6. Dept. exist in college premises in Hospital premises.
7. Departmental Office –
8. Demonstration – cum – Seminar room -------------------------------------------------------
9. (a) Paediatrics (teaching) (b) skin (teaching)---------- (c) Psychiatry
Others
(i) Clinical Training facility provided, if yes give details-----------------------------------
(ii) Total no. of beds earmarked.
(iii) Portion of Homoeopathy therapeutics covered (No. of classes/methodology)
(iv) Bed side case history recording done on acute and long case ---------------------
(v) Publication of Article by teaching staff ----------------------------------------------------
(vi) (a) Whether P.G. Department provided separately ------------------------------------
(b) If yes, details of teaching, other staff and no of students ------------------------
(c) Facilities provided -------------------------------------------------------------------------
(d) Dissertation topics allocated so far (year wise) ------------------------------------
(e) Name & Qualification of P.G. Students ----------------------------------------------
(f) Work given to P.G. students in House job ------------------------------------------
(vii) No. of students appeared in BHMS/M.D. (Hom) exams -------- passed -----%

21
(viii) (a) No. of visiting consultants in Hospital -------------------------------------------------
(b) House –Physicians (No. & their names with duty roster) ------------------------
and their duty details---------------------------
(c) O.P.D. Performance ---------------------------
(d) Diagnostic facilities.
Signature of H.O.D.
Remarks:-
22
8. DEPARTMENT OF FORENSIC MEDICINE & TOXICOLOGY :-
Designation CCH norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973. (of under I.M.C. Act, 1956 )
Teaching Exp. (with Name of Subject in which experience gained)
Full Time or Guest faculty
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D.
Name and Cadre of H.O.D ---------------------------------------------------------------------------
Departmental Office: ----------------------------------------------------------------------------------
Museum (brief description) ---------------------------------------------------------------------------
Equipment:
1) Weighing Machine ------ 2) Height Measurement -------- 3) Warnier Calipers ------
Weapons (in total) : --------------------
Blunt ------------ Sharp -------- Models --------- Charts --------- Specimens -----------------
Poisonous Substances: ----------- Chemical --------- Organic ------ Inorganic ------------
Facility for Ante/Post mortem examination provided
(brief description) ---------------------------------------------------------------------------------------
Record maintain for 10 cases of Post Mortem examination ------------- Yes/ No.
Whether prescribed – legislations available in Dept. & taught ------------------------------
Hours of teaching demonstration, tutorials and teaching plan ------------------------------
Total No. of Students appeared in exams ------------- passing ----------------------%
Departmental Library ----------------------------------------------------------------------------------
Audio- visual teaching material ---------------------------------------------------------------------
Any publication by teaching staff ------------------------------------------------------------------- Remarks:-
23
9. DEPARTMENT OF SURGERY:-
Designation CCH norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973 (of under I.M.C. Act, 1956)
Teaching Exp. (with Name of Subject in which experience gained)
Full Time or Guest faculty
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D.
1. Name and Designation of H.O.D. --------------------------------------------------------------
2. Other Staff :
3. No. of Beds earmarked :
4. Library Room :
5. Departmental Office :
6. Dept. Whether in College or Hospital :
7. Demonstration Room :
8. Facilities in attached Homoeopathic Hospital for undertaking operation exist or
not:------------------------------------------------------------------------------------------------------
9. No. of operations conducted --------------------------------------------------------------------
(in the given session )
(a) Audiometry Room (in ENT Section)
(b) Dental Surgery (and Prosthetic Dentistry)
10. Whether Homoeopathic Therapeutics taught
(No. of cases/Methodology) ---------------------------------------------------------------------
11. Indicate teaching hours (including theoretical, Practical & tutorials) & teaching
Plan: ---------------------------------------------------------------------------------------------------
12. Equipment list to be verified & attached ------------------------------------------------------
13. Any publication by teaching staff. -------------------------------------------------------------
14. No. of students appeared in BHMS exams -------------------------------------------------
15. Involvement in P.G. level courses ------------------------------------------------------------
16. No. of House Physicians & their duties. ------------------------------------------------------
17. No. of internees ------------------------------------------------------------------------------------ Remarks:
24
10. DEPARTMENT OF Obstetrics & Gynaecology:-
Designation CCH norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973. (of under I.M.C. Act, 1956)
Teaching Exp. (with Name of Subject in which experience gained)
Full Time or Guest faculty
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D.
1. Name and Cadre of H.O.D. ----------------------------------------------------------------------
2. Department set up where total area available --------------------------- sq. ft.
3. Whether Dept. is in College or Hospital -----------------------------------------------------
4. Demonstration Room :
5. Teaching Room :
6. Departmental library provided with total books on Gynaecology ---------------- and
Obstetrics and on therapeutics
7. Clinical training facility :
8. Total no. of beds earmarked :
9. Portion of Homoeopathic therapeutics covered – Yes / No.
(Teaching hours / methodology) :
10. Case recording done by students on acute and chronic cases :
11. Ante natal/ post natal check- up facility available – Yes / No.
12. Total no. of equipments provided in O. T. with full aseptic measures.
13. Laboratory and investigations facility provided :
14. Total no. of labour cases –
15. Child heath care facility existed – Yes / No
16.Whether equipment sufficient – Yes / No
17. Total no. of students appeared in exams ------------------ passing ------------%
18. Indicate teaching hours (including theoretical, practical & tutorial).--------------------
19. Any publication by teaching staff. :
20. Family Welfare clinic :
21. No. of House Physicians & their duties :
22. No. of Internees : Remarks:
25
11. DEPARTMENT OF Homoeopathic Materia Medica :-
Designation CCH norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973. (of under I.M.C Act, 1956)
Teaching Exp. (with Name of Subject in which experience gained)
Professor 2
Reader 2
Lecturer 2
Signature of H.O.D.
1. Name and Cadre of H.O.D. ----------------------------------------------------------------------
2. Whether all teachers on full time basis :
3. Department Office :
4. Department Library :
5. Department Museum containing various Drug Specimen/Substances, Articles,
case report and specimens for the use of teaching purposes.
6. Indicate Teaching hours (including theoretical, Practical & tutorials) & teaching
plan--------------- Any publication by teaching staff
7. Practical bed side clinics – and case demonstration & tutorial classes – were
held year wise ---------------------------------------------------------------------------------------
8. Stress on homoeopathic therapeutics --------------------------------------------------------
No. of charts --------------------- Audio- visual materials-------------------------------------
9. Any publication, seminars, Debate and group discussions – organized and
conducted.
Discussion Room :
10. Total number of students appeared in BHMS /M.D. (Hom)-------- passing %
computers & accessories & programmes-----------------------------------------------------
(i) Whether P. G. dept. provided separately –
(ii) If yes, details of teaching & other staff –
(iii) Dissertation topics allocated so far (year wise)
(iv) Worked allotted to P.G. students during House job.
Total number of students appeared in BHMS / M.D. (Hom.) -------- passing -------- % Remarks :
26
12. DEPARTMENT OF Organon of Medicine :-
Designation CCH norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973. (of under I.M.C. Act, 1956)
Teaching Exp. (with Name of Subject in which experience gained)
Professor 1
Reader 2
Lecturer 2
Signature of H.O.D.
1. Name and Cadre of H.O.D. ---------------------------------------------------------------------
2. Whether all teachers on full time basis :
3. Teaching Programme (No. of lectures on introductory part) :
4. History of Medicine, Principle and Philosophy on applied aspects of Organon
(including Kent’s and Stuart’s Close Essay taught)
5. Indicate Teaching hours (including theoretical, Practical & tutorials) & teaching
plan -------------- Any publication by teaching staff------------------------------------------
6. Maintenance of Clinical records on cases by students and interns term- wise :
7. Department Library
No. of charts ---------------------------- Audio- visual materials------------------------------
8. Any paper publications, scientific seminars, Debate and group discussions-
Organized and conducted.
9. Publication of Article by teaching staff :
10. computers & accessories & programmes ---------------------------------------------------
(i) Whether P.G. Department provided separately -
(ii) If yes, details of teaching & other staff –
(iii) Dissertation topics allocated so far (year wise)
(iv) Work allocated to P. G. students during House job.
Total number of students appeared in BHMS / M.D. (hom.) --------- passing --------%
Remarks :
27
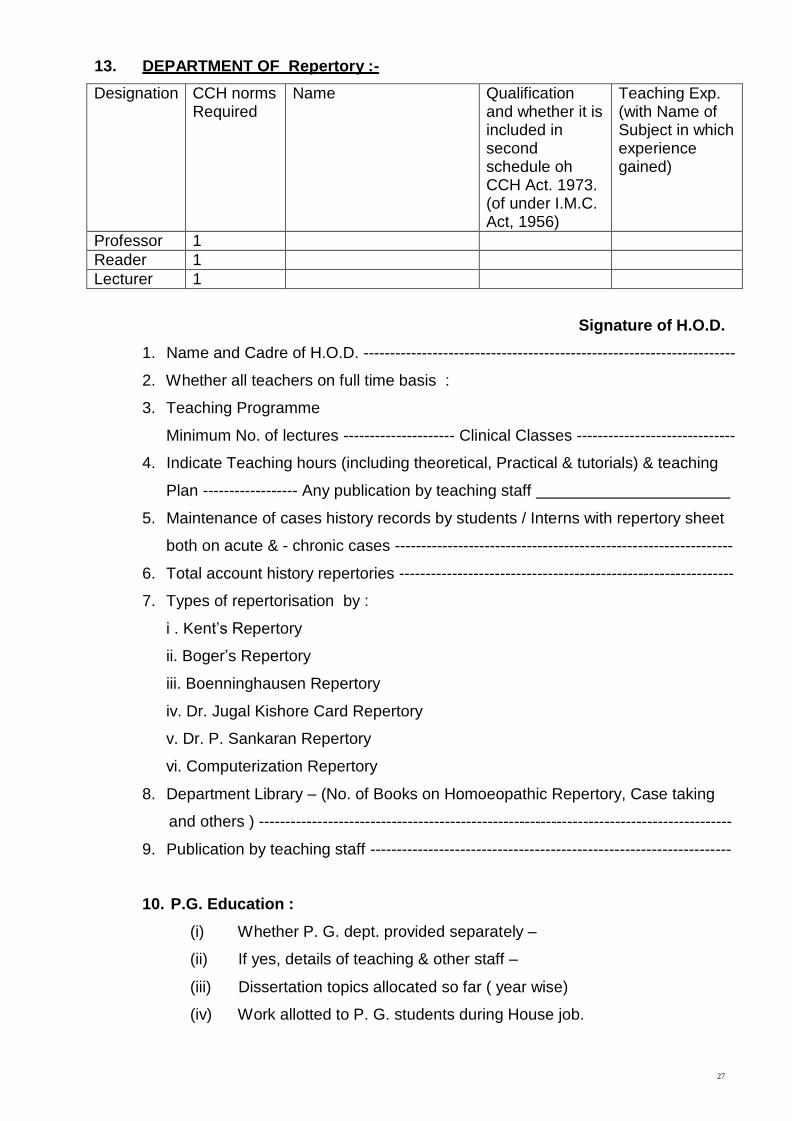
13. DEPARTMENT OF Repertory :-
Designation CCH norms Required
Name Qualification and whether it is included in second schedule oh CCH Act. 1973. (of under I.M.C. Act, 1956)
Teaching Exp. (with Name of Subject in which experience gained)
Professor 1
Reader 1
Lecturer 1
Signature of H.O.D.
1. Name and Cadre of H.O.D. ----------------------------------------------------------------------
2. Whether all teachers on full time basis :
3. Teaching Programme
Minimum No. of lectures --------------------- Clinical Classes ------------------------------
4. Indicate Teaching hours (including theoretical, Practical & tutorials) & teaching
Plan ------------------ Any publication by teaching staff
5. Maintenance of cases history records by students / Interns with repertory sheet
both on acute & - chronic cases ----------------------------------------------------------------
6. Total account history repertories ---------------------------------------------------------------
7. Types of repertorisation by :
i . Kent’s Repertory
ii. Boger’s Repertory
iii. Boenninghausen Repertory
iv. Dr. Jugal Kishore Card Repertory
v. Dr. P. Sankaran Repertory
vi. Computerization Repertory
8. Department Library – (No. of Books on Homoeopathic Repertory, Case taking
and others ) -----------------------------------------------------------------------------------------
9. Publication by teaching staff --------------------------------------------------------------------
10. P.G. Education :
(i) Whether P. G. dept. provided separately –
(ii) If yes, details of teaching & other staff –
(iii) Dissertation topics allocated so far ( year wise)
(iv) Work allotted to P. G. students during House job.
28
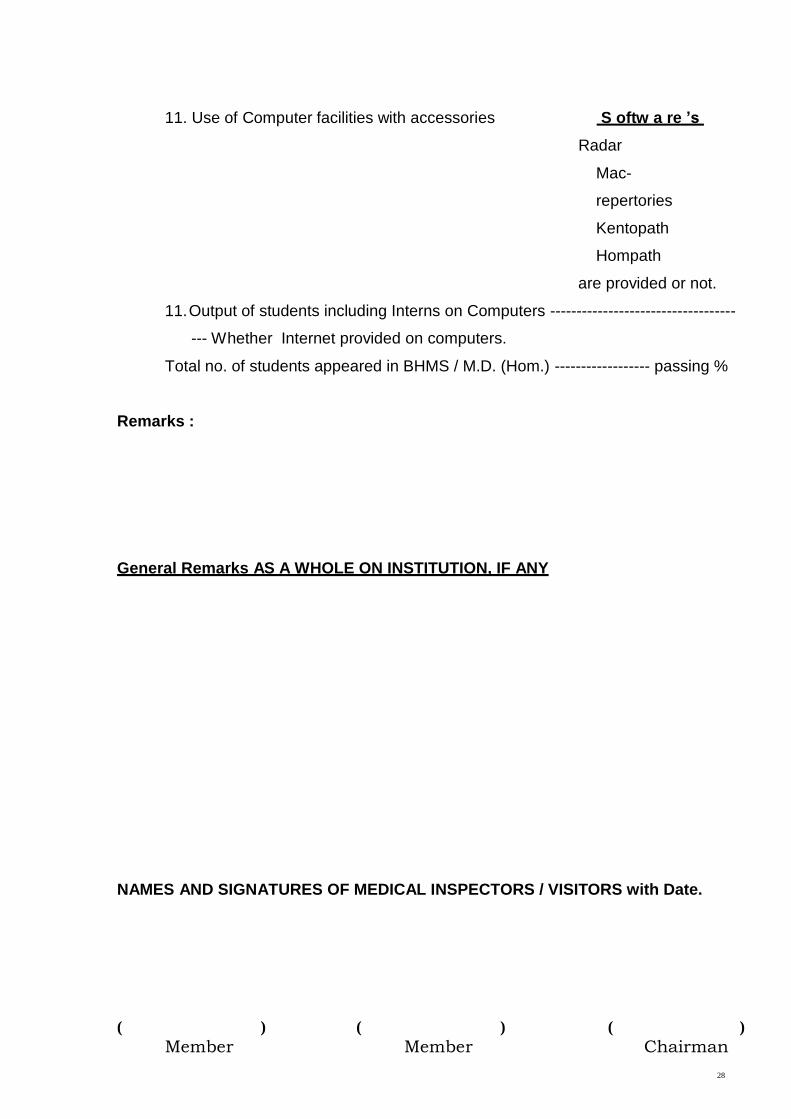
11. Use of Computer facilities with accessories S oftw a re ’s
Radar
Mac-
repertories
Kentopath
Hompath
are provided or not.
11. Output of students including Interns on Computers -----------------------------------
--- Whether Internet provided on computers.
Total no. of students appeared in BHMS / M.D. (Hom.) ------------------ passing %
Remarks :
General Remarks AS A WHOLE ON INSTITUTION, IF ANY
NAMES AND SIGNATURES OF MEDICAL INSPECTORS / VISITORS with Date.
( ) ( ) ( )
Member Member Chairman
29
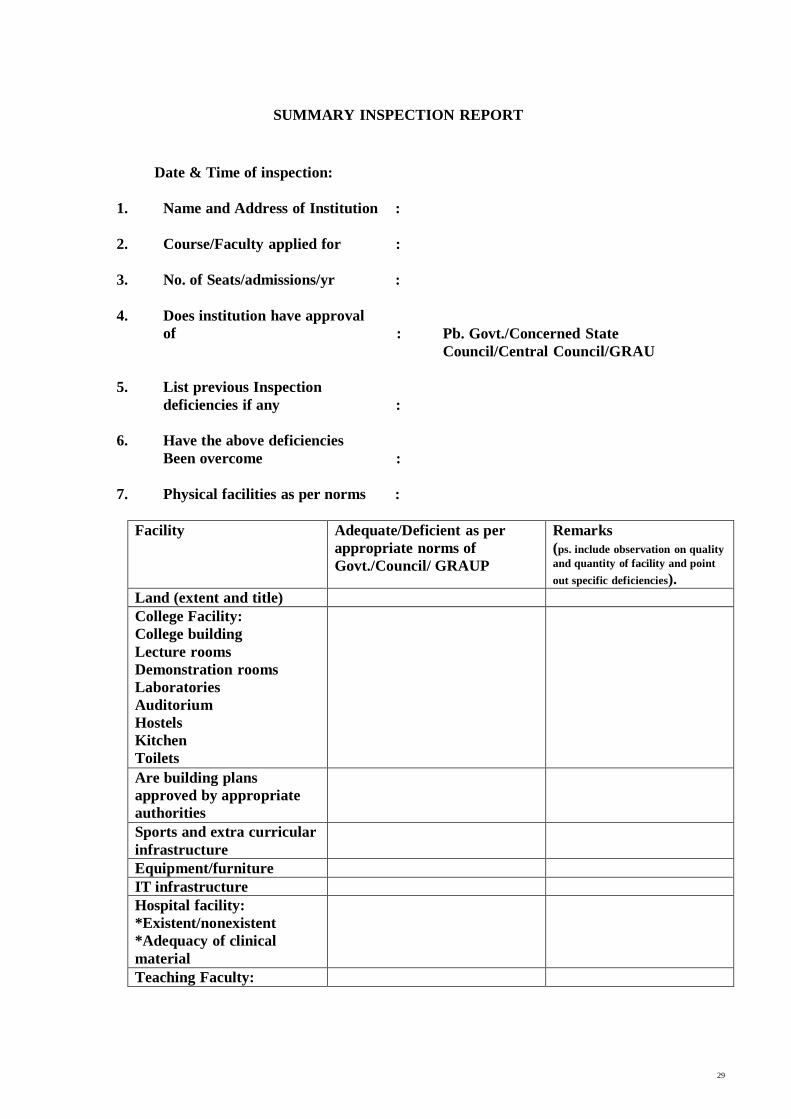
SUMMARY INSPECTION REPORT
Date & Time of inspection:
1. Name and Address of Institution :
2.
Course/Faculty applied for :
3.
No. of Seats/admissions/yr :
4.
Does institution have approval
of :
Pb. Govt./Concerned State
Council/Central Council/GRAU
5.
List previous Inspection
deficiencies if any :
6.
Have the above deficiencies
Been overcome :
7.
Physical facilities as per norms :
Facility Adequate/Deficient as per
appropriate norms of
Govt./Council/ GRAUP
Remarks
(ps. include observation on quality
and quantity of facility and point
out specific deficiencies).
Land (extent and title)
College Facility:
College building
Lecture rooms
Demonstration rooms
Laboratories
Auditorium
Hostels
Kitchen
Toilets
Are building plans
approved by appropriate
authorities
Sports and extra curricular
infrastructure
Equipment/furniture
IT infrastructure
Hospital facility:
*Existent/nonexistent
*Adequacy of clinical
material
Teaching Faculty:
30
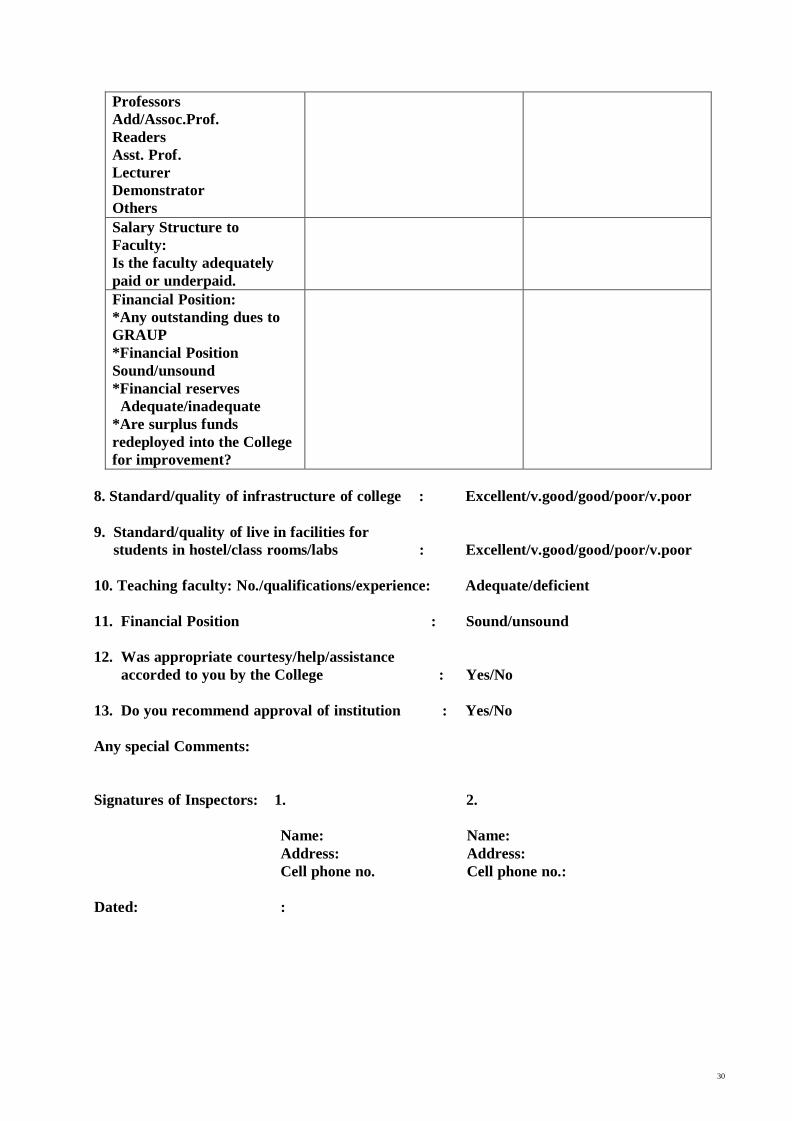
Professors
Add/Assoc.Prof.
Readers
Asst. Prof.
Lecturer
Demonstrator
Others
Salary Structure to
Faculty:
Is the faculty adequately
paid or underpaid.
Financial Position:
*Any outstanding dues to
GRAUP
*Financial Position
Sound/unsound
*Financial reserves
Adequate/inadequate
*Are surplus funds
redeployed into the College
for improvement?
8. Standard/quality of infrastructure of college : Excellent/v.good/good/poor/v.poor
9. Standard/quality of live in facilities for
students in hostel/class rooms/labs : Excellent/v.good/good/poor/v.poor
10. Teaching faculty: No./qualifications/experience: Adequate/deficient
11. Financial Position : Sound/unsound
12. Was appropriate courtesy/help/assistance
accorded to you by the College : Yes/No
13. Do you recommend approval of institution : Yes/No
Any special Comments:
Signatures of Inspectors: 1. 2.
Name: Name: Address: Address:
Dated:
Cell phone no.
:
Cell phone no.: