guideline for the commissioning, prescribing, and … · guideline for the commissioning,...
TRANSCRIPT
Guideline for the Commissioning, Prescribing, and Supply of Bone Morphogenic Protein
Version no: 1.0 Issue Status: Approved Ratified by: Drugs & Therapeutics Committee Date of Ratification: 20th January 2014 Policy Authors: Mr Pritesh Bodalia, Deputy Chief Pharmacist Mr Lester Wilson, Consultant, Spinal Surgical Unit Mr David Goodier, Consultant, Limb Reconstruction Policy Owner: Mr Matthew Shaw, Medical Director Review Frequency: 2 yearly Last Review: December 2013 Next Review: December 2015
POLICY AWARENESS
People who need to know this policy in detail All clinical staff
People who need to have a broad understanding of this policy
All clinical staff
People who need to know this policy exists All clinical staff
CHANGE CONTROL DETAILS
Date (dd/mm/yy) Version Description Reason for changes
19th December 2013 1.0 New Policy New Policy
Location: RNOH web

Page 2 of 21
Table of Contents
1. Introduction ........................................................................................................................................ 3
2. Aims and Objectives........................................................................................................................... 3
3. Bone Morphogenic Product (BMP) products ...................................................................................... 4
3.1. Dibotermin alfa (InductOs; rhBMP-2) ........................................................................................... 4
3.2. Eptotermin alfa (Osigraft; rhBMP-7) ............................................................................................ 4
4. Approved indications for BMP ............................................................................................................ 5
4.1. Dibotermin alfa (InductOs; rhBMP-2) for spinal surgery............................................................... 5
4.1.1. Revision Spinal Surgery .......................................................................................................... 5
4.1.2. Primary Spinal Surgery (high-risk) ........................................................................................... 5
4.2. Dibotermin alfa (InductOs; rhBMP-2) for long-bone surgery ........................................................ 6
4.2.1. Long-bone Surgery .................................................................................................................. 6
4.3. Eptotermin alfa (Osigraft; rhBMP-7) for long-bone surgery .......................................................... 7
4.3.1. Long-bone Surgery .................................................................................................................. 7
5. Areas not covered within the commissioning agreement .................................................................... 7
6. Commissioning Documents ................................................................................................................ 8
7. Evaluation Criteria .............................................................................................................................. 8
8. Contacts ............................................................................................................................................. 9
9. References ......................................................................................................................................... 9
Appendix 1 – NCL JFC Approval Letter for Dibotermin Alfa ..................................................................... 10
Appendix 2 – NCL JFC Approval Letter for Eptotermin Alfa ..................................................................... 12
Appendix 3 – NECL CSU Business Case Approval Letter for BMP ......................................................... 14
Appendix 4 – Prior Approval Form for BMP ............................................................................................. 17
Appendix 5 – BMP Proforma for Data Collection: Spinal Surgery ............................................................ 18
Appendix 6 – BMP Proforma for Data Collection: Long-Bone Fusion ...................................................... 20
Page 3 of 21
1. Introduction The Royal National Orthopaedic Hospital NHS Trust (Stanmore, UK) is the largest orthopaedic hospital in the UK and regarded as the leader in the field of orthopaedics both in the UK and world-wide. The Trust provides a comprehensive range of unique services including being one of the largest Spinal Deformity Units in Europe. Referrals to this service come from throughout the UK and internationally with the unit (comprising of 10 established orthopaedic surgeons) having a world-renowned reputation for their pioneering work. The Trust also undertakes complex limb reconstruction surgery. The lead surgeon for the Spinal Surgery Unit is Mr Lester Wilson. The principal surgeon undertaking complex limb reconstruction surgery is Mr David Goodier. The standard intervention for fusion of bone (spine and long-bone) is traditionally regarded as autogenous bone graft (commonly using the iliac crest).
Osteogenic proteins, more commonly referred to as Bone Morphogenic Protein (BMP), are produced naturally in the body and aid formation of new bone tissue. There are currently two synthetic BMP products licensed within the UK; dibotermin alfa (InductOs; rhBMP-2) and eptotermin alfa (Osigraft; rhBMP-7). They are both excluded from the National Tariff as of April 2009 and are therefore commissioned by Clinical Commissioning Groups (CCGs) as Payment by Results (PbR) excluded drugs. Two common referral themes seen by the Spinal Surgery Unit and the Limb Reconstruction Unit are: 1) Patients who have undergone previous surgery which has resulted in non-union, 2) Patients with high-risk disease and / or poor bone quality who have failed conservative
treatment and who will not be operated on at other centres. The use of Bone Morphogenic Protein (rhBMP-2 and rhBMP-7), a synthetic osteoinductive bone growth factor, licensed as a substitute for autogenous bone graft has been crucial to the success of complex surgeries at RNOH.
2. Aims and Objectives The aim of this guideline is to clarify to clinicians, nurses, pharmacists, commissioning and management the local arrangements for the correct commissioning, prescribing and supply pathway for Bone Morphogenic Protein. The objective of this guideline is to provide a clear framework for RNOH staff with respects to access to Bone Morphogenic Protein. This document provides the necessary guidance for staff to follow to meet the above aim. The recommendations within this guideline will evolve as local commissioning arrangements change.

Page 4 of 21
3. Bone Morphogenic Product (BMP) products
3.1. Dibotermin alfa (InductOs; rhBMP-2)
Dibotermin alfa (InductOs) is an osteoinductive protein which when carried on an absorbable collagen sponge (matrix) can induce new bone at the site of implantation. It binds to receptors on the surface of mesenchymal cells and causes cells to differentiate into cartilage- and bone-forming cells. The differentiated cells form trabecular bone as the matrix is degraded, with vascular invasion evident at the same time. The bone formation process develops from the outside of the implant towards the centre until the entire implant is replaced by trabecular bone. InductOs is available as a licensed product within the UK as a 12mg unit dose for:
Single-level (L4-L5 or L5-S1) anterior lumbar spine fusion as a substitute for autogenous bone graft in adults with degenerative disc disease who have had at least 6 months of non-operative treatment for this condition.
Treatment of acute tibia fractures in adults, as an adjunct to standard care using open fracture reduction and intramedullary undreamed nail fixation.
The use of InductOs has been commissioned for a number of off-label indications as described below.
3.2. Eptotermin alfa (Osigraft; rhBMP-7)
Eptotermin alfa (Osigraft) is an osteoinductive and osteoconductive protein which initiates bone formation through the induction of cellular differentiation in mesenchymal cells, recruited to the implant site from bone marrow, periosteum and muscle. The collagen matrix is insoluble, and provides an appropriate bio-resorbable scaffold for the anchorage dependent cell proliferation and differentiation processes induced by the active substance. The matrix is also osteoconductive and it allows bone in-growth into the defect area from the surrounding healthy bone. Osigraft is available as a licensed product within the UK as a 3.3mg unit dose for:
Treatment of non-union of tibia of at least 9 months duration, secondary to trauma, in skeletally mature patients, in cases where previous treatment with autograft has failed or use of autograft is unfeasible.
The use of Osigraft has been commissioned for a number of off-label indications as described below.

Page 5 of 21
4. Approved indications for BMP
4.1. Dibotermin alfa (InductOs; rhBMP-2) for spinal surgery
The conventional dose of 2mg is applied per vertebrae; therefore in the majority of cases one unit should be prescribed. On rare occasions for patients undergoing scoliosis surgery it may be necessary for two units to be supplied. Prescribing of InductOs for spinal surgery is restricted to the following Consultants within the Spinal Surgery Unit: Mr Wilson, Mr Casey, Mr Rezajooi, Mr Shaw, Mr Gibson, Mr Molloy, Mr Tucker, Mr Lehovsky and Mr Noordeen.
4.1.1. Revision Spinal Surgery
4.2.1.1. For treatment where non-union is identified, of at least 6 months duration, in skeletally mature patients with degenerative disease, in cases where previous autograft treatment has failed and / or use of further autograft is unfeasible [Restricted to Consultants within the Spinal Surgery Unit]
4.1.2. Primary Spinal Surgery (high-risk)
4.1.2.1. For use as a substitute to autogenous bone graft in skeletally mature patients with degenerative disease who have had at least 6 months non-operative treatment and the use of autograft is unfeasible or clinically unsuitable due to one or more of the following factors:
4.1.2.1.1. Pars Interarticularis defects Patients who have suffered an acute fracture and a quick and efficient fusion is required due to the fracture being in a critical load bearing location. The fracture will have occurred due to loading and unloading of the affected spinal vertebral regions through physical activity e.g. athletes and manual labour.
4.1.2.1.2. Osteoporotic bone
Patients with osteoporosis (have poor bone quality) and therefore have poor bone healing properties to be used for grafting. The use of instrumentation and screws would grip poorly and loosen early, compromising the fixation necessary to encourage bone healing. The use of synthetic bone would speed up the process of bone healing to a ‘normal’ rate and minimises the risk of surgical fixation failure. In some cases, the use of instrumentation may be avoided entirely.
4.1.2.1.3. Metabolic bone disease (such as Rheumatoid Arthritis)
The same principles apply here as for osteoporotic bone.
4.1.2.1.4. Repairs secondary to lytic spondylolisthesis
Elderly patients with nerve compression in the neuroforamen. The use of BMP enables the surgeon to avoid the cost and morbidity of using an interbody cage which presents additional risks.

Page 6 of 21
Pedicle screws would usually be inserted and distracted into rods thus widening the nerve channel. The use of synthetic bone would speed up the process of bone healing before the screws break or loosen which would otherwise result in recurrent symptoms.
4.1.2.1.5. Scoliosis
In degenerative or adult scoliosis, multi-level vertebral fixation is required. This form of surgery results in enormous mechanical stress to the spine applied through the instrumentation in order to correct the shape. The use of synthetic bone is required as there will not be sufficient quantity of autogenous bone available as well as speeding up the process of bone healing before the instrumentation breaks or loosen which would otherwise result in non-union and recurrent symptoms.
4.1.2.1.6. Sacro-iliac
This is a highly-specialist form of orthopaedic surgery performed by a select few Consultants within the UK. As the sacro-iliac joint is the largest joint in the body and receives an enormous amount of stress through the instrumentation used there is a race between bone healing and instrumentation failure. The use of synthetic bone would speed up the process of bone healing before the instrumentation breaks or loosen which would otherwise result in non-union and recurrent symptoms. [Restricted to Mr Wilson only]
4.2. Dibotermin alfa (InductOs; rhBMP-2) for long-bone surgery
InductOs is commissioned for the treatment of long-bone fractures in patients with Grade IIIB fractures (i.e. more severe cases) as an adjunct to standard care using open fracture reduction and intramedullary nail fixation in whom there is substantial risk of non-union. It is restricted to patients treated with undreamed intramedullary nails. Prescribing of InductOs for limb reconstruction is restricted to the following Consultants within the Limb Reconstruction Unit: Mr Calder, Mr Goodier, Mr Hashemi-Nejad and Prof Marsh.
4.2.1. Long-bone Surgery
4.3.1.1. For treatment where non-union is identified, of at least 9 months duration, in cases which have been assessed for bone autograft AND found to be unsuitable for such procedure.
4.3.1.2. Non-union locations include:
a) Tibia b) Fibula c) Femur d) Ulna e) Radius f) Humerus g) Clavicle
Page 7 of 21
4.3. Eptotermin alfa (Osigraft; rhBMP-7) for long-bone surgery
Osigraft is commissioned for the treatment of non-union of tibia of at least 9 months duration, secondary to trauma, in skeletally mature patients, in cases where previous treatment with autograft has failed or use of autograft is unfeasible Prescribing of Osigraft for limb reconstruction is restricted to the following Consultants within the Limb Reconstruction Unit: Mr Calder, Mr Goodier, Mr Hashemi-Nejad and Prof Marsh.
4.3.1. Long-bone Surgery
4.3.1.3. For treatment where non-union is identified, of at least 9 months duration, in cases which have been assessed for bone autograft AND found to be unsuitable for such procedure.
4.3.1.4. Non-union locations include:
h) Tibia i) Fibula j) Femur k) Ulna l) Radius m) Humerus n) Clavicle
5. Areas not covered within the commissioning agreement The use of BMP is not commissioned via the prior approval pathway for the indications below. Any requests which fall within these criteria will require submission of an IFR.
Use in skeletally immature individuals (i.e. paediatrics)
Sequential use (i.e. repeat dose if used before) due to the possible development of antibody production.
Closed long-bone fractures

Page 8 of 21
6. Commissioning Documents For all BMP requests which meet the above criteria, the Consultant (or their Specialist Registrar) is required to complete the ‘Prior Approval Application for BMP’ and section 1 of the ‘BMP Proforma for Data Collection.’ Both of these documents can be obtained from RNOH Commissioning Department (email [email protected]).
A copy of the Prior Approval Application can be viewed in Appendix 4.
A copy of the BMP Proforma for Data Collection (Spinal Surgery) can be viewed in Appendix 5.
A copy of the BMP Proforma for Data Collection (Long-Bone Fusion) can be viewed in Appendix 6.
Once complete, the forms should be sent to Pharmacy via email to the Chief / Deputy Chief Pharmacist. The forms will be verified and forward on to RNOH Commissioning for onward transmission to the relevant CCG. It is expected that the CCG will return a decision for funding approval within 2 weeks of receipt as per Business Case Approval by NECL CSU (Appendix 3).
7. Evaluation Criteria The use of BMP within the above commissioning parameters will require documentation of baseline data (as described above) as well as the undertaking of continual assessment for all patients’ long term recovery using validated outcome measures (as per section 2 of the ‘BMP Proforma for Data Collection.’)
A copy of the BMP Proforma for Data Collection (Spinal Surgery) can be viewed in Appendix 5.
A copy of the BMP Proforma for Data Collection (Long-Bone Fusion) can be viewed in Appendix 6.
These data will be used to conduct a comprehensive evaluation of BMP use at RNOH in order to report on its efficacy, safety and cost-effectiveness in the local patient population.

Page 9 of 21
8. Contacts Pharmacy Mr Pritesh Bodalia Deputy Chief Pharmacist [email protected] Ext. 5410 Mr Ashik Shah Chief Pharmacist [email protected] Ext. 5410 Commissioning
Mr Sebastian Buchmann Commissioning Assistant [email protected] Ext. 5579
9. References
1. North Central London Joint Formulary Committee. Application for dibotermin alfa (March 2013).
2. North Central London Joint Formulary Committee. Application for eptotermin alfa (April 2013).
3. North East and Central London Commissioning Support Unit. Business case submission for BMP use at RNOH (December 2013).

Page 10 of 21
Appendix 1 – NCL JFC Approval Letter for Dibotermin Alfa

Page 11 of 21

Page 12 of 21
Appendix 2 – NCL JFC Approval Letter for Eptotermin Alfa
Page 13 of 21

Page 14 of 21
Appendix 3 – NECL CSU Business Case Approval Letter for BMP
Individual Funding Request Team Clifton House
75 -77 Worship Street
London EC2A 2DU
Tel: 020 3688 1274
[email protected] Ashik Shah, Chief Pharmacist Lesley Macleod, Head of Commissioning Royal National Orthopaedic Hospital NHS Trust Brockley Hill Stanmore Middlesex HA7 4LP
17th December 2013 Dear Ashik and Lesley Re: Bone Morphogenic Protein Business Case Many thanks to you both for providing an update on the business case for Bone Morphogenic Protein (BMP) by the deadline. I can confirm that the case was discussed in detail by the Service Development Review Group on 12th December. The Review Group was led by Barnet Clinical Commissioning Group (CCG) as the lead commissioner for your trust. The recommendations from this Review Group, together with details of the process followed and rationale for decision-making, will be shared with associate CCGs in the expectation that they will agree with the recommendations made in their own commissioning decisions. The Review Group was able to use the details of your papers to further understand the clinical pathway and associated costs for the procedure. It also considered the East of England policy on BMP when reaching its decision. The meeting agreed the following for the range of conditions considered: Spinal Surgery The Review Group agreed to fund the use of BMP for secondary revision of spinal fusion surgery as outlined in your business case. The evidence for cost-effectiveness was not compelling but it was agreed that cost-savings and improved effectiveness of spinal fusion are likely to be realised. The use of BMP for primary spinal fusion surgery for patients at high risk of pseudoarthrosis will also be funded. The following caveats to this approval will apply:
RNOH will seek prior approval for the proposed use of BMP from the Individual Funding Request (IFR) Service at NELCSU (or other such equivalent bodies outside of the NELCSU CCG area). This will utilise a specific form for BMP (Appendix 1), which will

Page 15 of 21
be scrutinised by the IFR Team with sign-off by appropriate CCG. If all criteria are satisfactorily met, then approval will be given. The turnaround time for approval under this process is currently 2 weeks.
We note your assessment of activity levels for the next two years. We will be monitoring activity levels for the use of BMP across all CCGs, not just NELCSU CCGs. If activity levels are more than 10% above predicted levels in any of the categories then we will conduct a review of the usage of BMP.
Long Bones We agree the use of BMP in long bones for the following indications (taken from the East of England policy 2010):
(i) For acute tibial fractures with Grade IIIB fractures (i.e. more severe cases): “dibotermin alfa (InductOs®) is recommended as an adjunct to standard care using open fracture reduction and intramedullary nail fixation in patients in whom there is a substantial risk of non-union. It is restricted to patients treated with unreamed intramedullary nails.”
(ii) Non-union of long bones exceeding nine months which have been assessed for bone
autograft AND found to be unsuitable for such a procedure:
o NB Osigraft® (Eptotermin alfa combined with bovine collagen) should only be considered third-line AND treatment is restricted by named consultants for use in tibial, ulnar, radial, humoral, femoral and clavicular non-union.
Please note that the same prior approval form will be used for spinal surgery and long bone fracture patients. Evaluation We require the continual assessment of all patients’ long-term recovery using validated outcome data. We require that for each patient baseline and follow up scores are recorded using three measures – SF-36, Visual Analogue Score (VAS) assessment of pain and the Oswestry Disability Index (spinal patients only). We require that audits of these outcomes are presented to the IFR Panel at six-monthly intervals (April and October) over the next two years in order to assist the CCGs to confirm continual funding. We will require the separate analysis of secondary fusion patients from primary fusion patients. Timescales We note your application for this funding was made to start in 2013/14. However this decision to fund will not be retrospective for 13/14 but will start from the date of the decision i.e. 12th December 2013. As previously stated, we are unable to agree funding decisions for associate CCGs on their behalf and we will need to notify them of our decision to enable them to plan for the increased expenditure. Please note that both their decision to fund and the timescales of funding may be different from this recommended approach. We wish you luck in your forthcoming research and look forward to seeing your researched published. We would also request that in the event of the research being undertaken but not published, that the results are shared with NELCSU CCGs.
Page 16 of 21
Yours sincerely,
Susan Beecham, Deputy Director Individual Funding Requests, North and East London Commissioning Support Unit Copies to: Tim Baker, Assistant Director of Individual Funding Requests, North and East London Commissioning Support Unit David Culley, Senior Contracts Manager, North and East London Commissioning Support Unit

Page 17 of 21
Appendix 4 – Prior Approval Form for BMP

Page 18 of 21
Appendix 5 – BMP Proforma for Data Collection: Spinal Surgery
Section 1: To complete with the notification form
DEMOGRAPHIC DETAILS
Consultant Name Click here to enter text.
Patient Name Click here to enter text. D.O.B. Click here to enter text.
NHS Number Click here to enter text. Hospital No. Click here to enter text.
SURGERY DETAILS
Type of Surgery Primary ☐ Revision ☐ Use of Cage Yes ☐ No ☐
Approach ALIF ☐ PLIF ☐ TLIF ☐ Type of Cage Click here to enter text.
Levels Single ☐ Multiple ☐
Location
Cervical ☐ C1-2 ☐ C2-3 ☐ C3-4 ☐ C4-5 ☐ C5-6 ☐ C6-7 ☐
Thoracic ☐ T1-2 ☐ T2-3 ☐ T3-4 ☐ T4-5 ☐ T5-6 ☐ T6-7 ☐
T7-8 ☐ T8-9 ☐ T9-10 ☐ T10-11 ☐ T11-12 ☐
Lumbar ☐ L1-2 ☐ L2-3 ☐ L3-4 ☐ L4-5 ☐ L5-6 ☐
Sacro-Iliac Joint ☐
Risk of pseudoarthrosis
THIS SECTION MUST BE COMPLETED FOR PRIMARY SURGERY
Pars Interacticularis ☐ Repairs secondary to lytic spondylolisthesis ☐
Osteoporotic bone ☐ Metabolic bone disease ☐
Scoliosis ☐ Sacro-Iliac ☐
Previous Surgery
THIS SECTION MUST BE COMPLETED FOR REVISION SURGERY
Date Name of Intervention Outcome
Click here to enter text. Click here to enter text. Click here to enter text.
Click here to enter text. Click here to enter text. Click here to enter text.
Click here to enter text. Click here to enter text. Click here to enter text.
BASELINE SCORES
THESE SCORES MUST HAVE BEEN TAKEN WITHIN THE LAST SIX WEEKS
FUNCTION: Oswestry Disability Index (ODI)
Click here to enter text. Date recorded: Click here to enter text.
PHYSICAL / MENTAL STATUS: Short Form 36 (SF-36)
Click here to enter text. Date recorded: Click here to enter text.
PAIN: Visual Analogue Score (VAS)
Click here to enter text. Date recorded: Click here to enter text.

Page 19 of 21
Section 2: To complete as part of monitoring
INTRA-OPERATION DETAILS
Date of Surgery Click here to enter text.
BMP Dose Click here to enter text.
Operative Time Click here to enter text.
Precise Grafting Volume
Click here to enter text.
Precise Grafting Technique
Click here to enter text.
Cage Size Click here to enter text.
Blood Loss Click here to enter text.
POST-OPERATION DETAILS
Early Complications
Wound Swelling/ Inflammation
Choose an item.
Wound Leakage
Choose an item.
Radiculitis
Choose an item.
Systemic Symptoms of Allergy
Choose an item.
Back Pain
Choose an item.
Late Complications
Bone Lysis
Choose an item.
Pseudoarthrosis
Choose an item.
Cage Subsidence
Choose an item.
Heterotrophic Bone
Choose an item.
Excessive Bone
Choose an item.
Length of Stay in Hospital
Click here to enter text.
FOLLOW-UP
Fusion Verified
Imaging performed by: Choose an item.
6 months Choose an item. 12 months Choose an item. 18 months Choose an item.
24 months Choose an item. 36 months Choose an item. 48 months Choose an item.
FUNCTION: Oswestry Disability Index (ODI)
6 months: Click here to enter text. 12 months: Click here to enter text.
24 months: Click here to enter text. 48 months: Click here to enter text.
PHYSICAL / MENTAL STATUS: Short Form 36 (SF-36)
6 months: Click here to enter text. 12 months: Click here to enter text.
24 months: Click here to enter text. 48 months: Click here to enter text.
PAIN: Visual Analogue Score (VAS)
6 months: Click here to enter text. 12 months: Click here to enter text.
24 months: Click here to enter text. 48 months: Click here to enter text.

Page 20 of 21
Appendix 6 – BMP Proforma for Data Collection: Long-Bone Fusion
Section 1: To complete with the notification form
DEMOGRAPHIC DETAILS
Consultant Name Click here to enter text.
Patient Name Click here to enter text. D.O.B. Click here to enter text.
NHS Number Click here to enter text. Hospital No. Click here to enter text.
SURGERY DETAILS
Location Tibia ☐ Ulna ☐ Radia ☐ Humerus ☐ Femur ☐ Clavicle ☐
Previous Intervention
OSIGRAFT is commissioned for third-line treatment only
Immobilisation ☐ Corticotomy ☐
External fixator ☐ Ultrasonic bone growth stimulator ☐
Osteotomy ☐ Autograft ☐
BASELINE SCORES
THESE SCORES MUST HAVE BEEN TAKEN WITHIN THE LAST SIX WEEKS
FUNCTION: Short Musculoskeletal Function
Assessment Click here to enter text. Date recorded: Click here to enter text.
PHYSICAL / MENTAL STATUS: Short Form 36 (SF-36)
Click here to enter text. Date recorded: Click here to enter text.
PAIN: Visual Analogue Score (VAS)
Click here to enter text. Date recorded: Click here to enter text.
Page 21 of 21
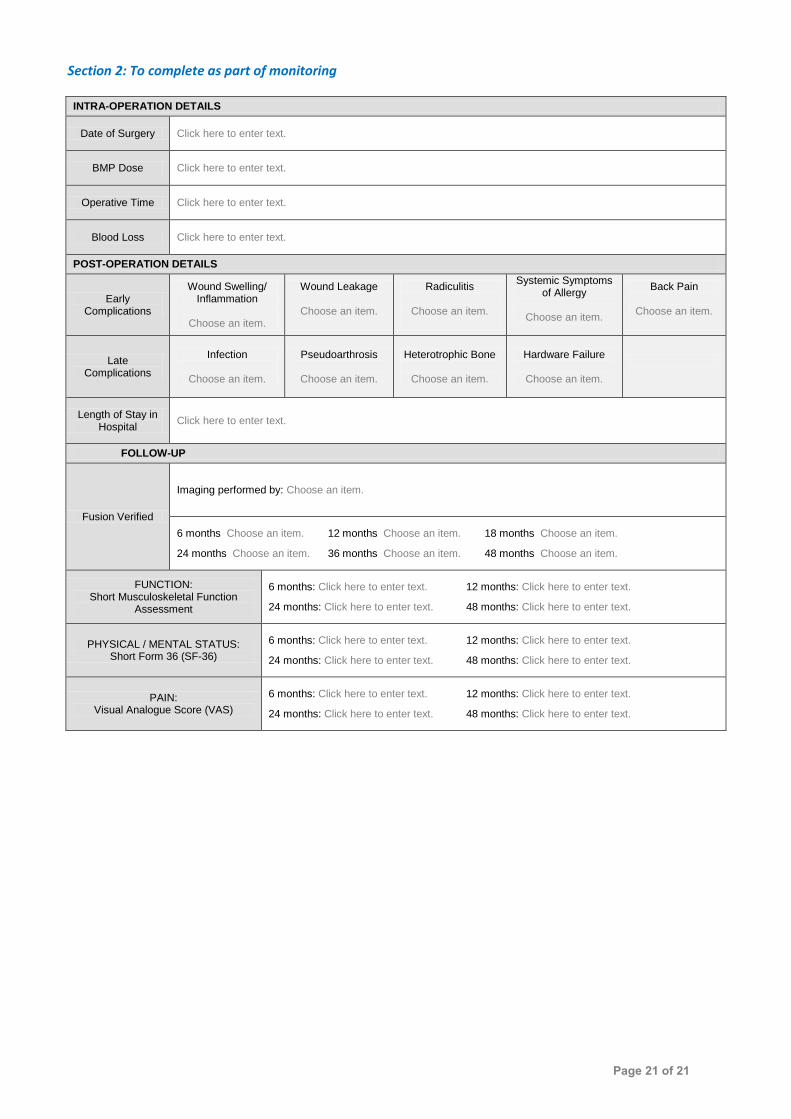
Section 2: To complete as part of monitoring
INTRA-OPERATION DETAILS
Date of Surgery Click here to enter text.
BMP Dose Click here to enter text.
Operative Time Click here to enter text.
Blood Loss Click here to enter text.
POST-OPERATION DETAILS
Early Complications
Wound Swelling/ Inflammation
Choose an item.
Wound Leakage
Choose an item.
Radiculitis
Choose an item.
Systemic Symptoms of Allergy
Choose an item.
Back Pain
Choose an item.
Late Complications
Infection
Choose an item.
Pseudoarthrosis
Choose an item.
Heterotrophic Bone
Choose an item.
Hardware Failure
Choose an item.
Length of Stay in Hospital
Click here to enter text.
FOLLOW-UP
Fusion Verified
Imaging performed by: Choose an item.
6 months Choose an item. 12 months Choose an item. 18 months Choose an item.
24 months Choose an item. 36 months Choose an item. 48 months Choose an item.
FUNCTION: Short Musculoskeletal Function
Assessment
6 months: Click here to enter text. 12 months: Click here to enter text.
24 months: Click here to enter text. 48 months: Click here to enter text.
PHYSICAL / MENTAL STATUS: Short Form 36 (SF-36)
6 months: Click here to enter text. 12 months: Click here to enter text.
24 months: Click here to enter text. 48 months: Click here to enter text.
PAIN: Visual Analogue Score (VAS)
6 months: Click here to enter text. 12 months: Click here to enter text.
24 months: Click here to enter text. 48 months: Click here to enter text.