guide to billing — cms-1500 form (02/2012) …/media/files/pdf/cms1500... · guide to billing —...
TRANSCRIPT
GUIDE TO BILLING — CMS-1500 FORM (02/2012) PCS/MLTC CLAIMS


GUIDE TO BILLING — PCS/MLTC CLAIMSCMS 1500 ForM (02-12) ............................................................................................................ 1
CMS 1500 ForM FIELDS 1 through 24E DESCrIptIon anD uSE ......................2
CMS 1500 ForM FIELDS 24F through 33b DESCrIptIon anD uSE ................3
CorrECtLY CoMpLEtED CMS 1500 ForM (02-12) .....................................................4
bILLIng tIpS ..................................................................................................................................5
SErVICES grID .............................................................................................................................6


1
APPROVED OMB-0938-1197 FORM 1500 (02-12) PLEASE PRINT OR TYPE
CMS 1500 FORM (02-12)
1
2 3 4
5 6 7
9 10
17
21
24a
1a
9a
9d
17b
24b 24c24d
24e 24f24g
25 26 27 28 29 30
31 32 33
32a 32b
2
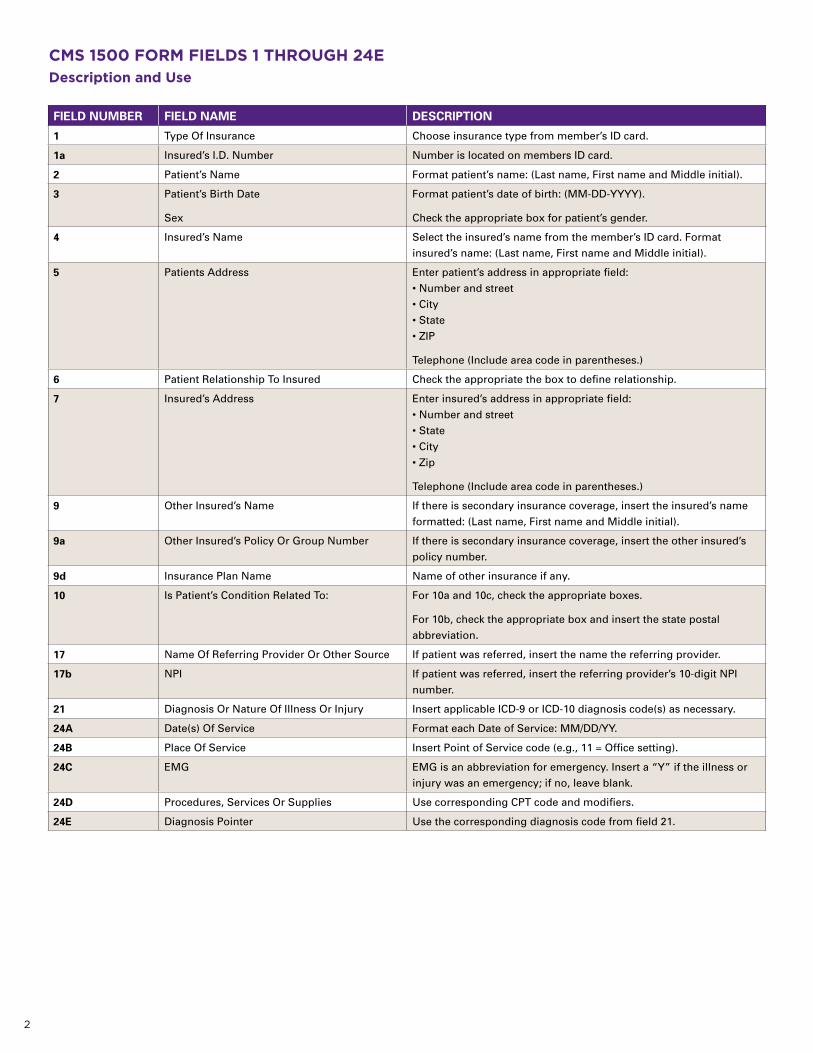
CMS 1500 FORM FIELDS 1 ThROUGh 24EDescription and Use
FIELD NUMBER FIELD NAME DESCRIPTION
1 Type Of Insurance Choose insurance type from member’s ID card.
1a Insured’s I.D. Number Number is located on members ID card.
2 Patient’s Name Format patient’s name: (Last name, First name and Middle initial).
3 Patient’s Birth Date
Sex
Format patient’s date of birth: (MM-DD-YYYY).
Check the appropriate box for patient’s gender.
4 Insured’s Name Select the insured’s name from the member’s ID card. Format insured’s name: (Last name, First name and Middle initial).
5 Patients Address Enter patient’s address in appropriate field:• Number and street • City • State • ZIP
Telephone (Include area code in parentheses.)
6 Patient Relationship To Insured Check the appropriate the box to define relationship.
7 Insured’s Address Enter insured’s address in appropriate field:• Number and street • State • City • Zip
Telephone (Include area code in parentheses.)
9 Other Insured’s Name If there is secondary insurance coverage, insert the insured’s name formatted: (Last name, First name and Middle initial).
9a Other Insured’s Policy Or Group Number If there is secondary insurance coverage, insert the other insured’s policy number.
9d Insurance Plan Name Name of other insurance if any.
10 Is Patient’s Condition Related To: For 10a and 10c, check the appropriate boxes.
For 10b, check the appropriate box and insert the state postal abbreviation.
17 Name Of Referring Provider Or Other Source If patient was referred, insert the name the referring provider.
17b NPI If patient was referred, insert the referring provider’s 10-digit NPI number.
21 Diagnosis Or Nature Of Illness Or Injury Insert applicable ICD-9 or ICD-10 diagnosis code(s) as necessary.
24A Date(s) Of Service Format each Date of Service: MM/DD/YY.
24B Place Of Service Insert Point of Service code (e.g., 11 = Office setting).
24C EMG EMG is an abbreviation for emergency. Insert a “Y” if the illness or injury was an emergency; if no, leave blank.
24D Procedures, Services Or Supplies Use corresponding CPT code and modifiers.
24E Diagnosis Pointer Use the corresponding diagnosis code from field 21.

3
CMS 1500 FORM FIELDS 24F ThROUGh 33BDescription and Use
FIELD NUMBER FIELD NAME DESCRIPTION
24F $ Charges Insert dollar amount.
24G Days or Units Insert number of units being billed.
25 Federal Tax I.D. Number Insert Tax ID or Social Security Number. Check the appropriate box.
26 Patient’s Account No. Insert the patient’s account number.
27 Accept Assignment Check the appropriate box. If yes, make sure the insured or the person authorized to answer on insured’s behalf has signed the form in field 13.
28 Total Charge Enter total amount from all claim lines.
29 Amount Paid Dollar amount received from any other insurance.
30 Balance Due Insert amount expected after subtracting payments from other insurances.
31 Signature Sign the doctor’s name and insert date the claim is completed for submission.
32 Service Facility Location Information Insert the address where the services were rendered.
32a NPI Leave blank.
32b Blank Provider NPI numbers are not location specific; leave blank.
33 Billing Provider Info & Ph # Insert billing provider’s name, address and telephone number.
33a NPI Leave blank.
33b Blank Insert billing provider’s NPI number.

4
CORRECTLY COMPLETED CMS 1500 FORM (02-12)
APPROVED OMB-0938-1197 FORM 1500 (02-12) PLEASE PRINT OR TYPE
X 12345678
Smith, Mary A 06 28 74
123 Main Street Apartment 4
John R. Smith
Anytown
123 Main Street Apartment 4
NY Anytown NY
15678-9012 845 555-6666 15678-9012 845 555-6666
X
X
X
X
11 15 72 X
X
John Q Doctor, MD 2345678901
788.33
12 21 2013 T4527
A4554
A4927
00000P1234567890
987654321 X
Happy Town Medical Services 987 West South Street Ste 6
Happy, NY 15432-1098
845 555-6666
0006571005
X
12 21 2013
12 21 2013
12 21 2013
12 21 2013
12 21 2013
00000P1234567890
00000P1234567890
Happy Town Medical Services 987 West South Street Ste 6
Happy, NY 15432-1098
12
12
12
$12 00
$20 00
$17 00
1
1
1
09201965DBS X $49 00
Signature on file

5
BILLING TIPS
• Prior approval is required for these services.
• It is very important to complete the CMS-1500 (02-12) accurately and completely in order to ensure timely and accurate processing of your claims.
• CMS 1500 (02-12) is the correct type of claim form. Please do not use UB-04 or UB-92 forms.
• Electronic billing is preferred. Turnaround time for processing and issuance of payment is generally faster when claims are submitted via EDI (Electronic Data Interchange).
• Submit paper claims on red “drop out” forms and forms should be typed, not handwritten.
• Complete only required fields. Entry in fields that are not required may result in your claim being denied.
• Be sure that the billed services match those that were previously approved or authorized. If the billed service was not previously approved or authorized, the claim will be denied.
• Review your Agreement to verify the types of services for which you have contracted and the amount you should expect to be reimbursed per the contractual agreement.
• Be sure to bill the units as appropriate for each type of service. For example:
• S5120: Home Modifications. Billed in 15 minute increments. One (1) hour of service is equal to four (4) billed units.
• S5161: Emergency Response Service fee. One (1) month of service is equal to one (1) billed unit.
• S5131: Homemaker Service (i.e., bed bug cleaning and extermination). One (1) service is equal to one (1) billed unit.

6
SERvICES GRIDThis list is not complete and is subject to change
CPT/HCPCS CODE DESCRIPTION UNITS BILLED AS PLACE OF SERVICE
A0130 Non-emergency transportation. 1 unit = 1 transport 41 or 40
S5120 Home maintenance. (Can be used for housekeeping and maid services.)
1 unit = 15 minutes 4 units = 1 hour
12: Home
S5121 Chore services for heavy-duty cleaning. 1 unit = 1 date of service 12: Home
S5130 Carpet cleaning; upholstery. 1 unit = 1 day 12: Home
S5131 Homemaker services; bed bug cleaning and extermination.
1 unit = 1 date of service 12: Home
S5150 Unskilled respite care. 1 unit = 15 minutes 4 units = 1 hour
12: Home
S5160 Emergency Response System: Installation. 1 unit = installation 12: Home
S5161 Emergency Response System: Service fee. 1 unit = monthly monitoring 12: Home
S5165 Home modifications. 1 unit = 1 modification 12: Home
S5170 Home delivered meals, including preparation. 1 unit = 1 meal 11: Office 12: Home
T1028 Assessment of home; used for home modifications.
1 unit = 1 assessment 12: Home
92012 92014 92015 92060 Vision/Eyeglasses. 1 unit = 1 date of service 11: Office
V2020
92533-92550 92555-92557 92563-92565 92567-92568 92570-92571 92579, 92585-92588, 92601-92604
Hearing aids. 1 unit = 1 date of service 11: Office
97802 Medical nutrition. 1 unit = 1 date of service 11: Office 12: Home
97803 Medical Nutrition — individual. 1 unit = 1 date of service 11: Office 12: Home
Variable* Podiatry. 1 unit = 1 service 11: Office
Variable* PT/OT/ST. 1 unit = 1 service 11: Office
Variable* DME. 1 unit = 1 item 12: Home P: Purchase S: Supply R: Rental
Note: *Refer to CPT book for listing of codes for this service.


group health Incorporated (ghI), hIp health plan of new York (hIp), hIp Insurance Company of new York and Emblemhealth Services Company, LLC are Emblemhealth companies. Emblemhealth Services Company, LLC provides administrative services to the Emblemhealth companies.
EMb_pr_bro_18850_CMS1500-MLtC-billingguide 6/14
55 Water Street, new York, new York 10041-8190 | www.emblemhealth.com