grudhrasi kc034 gdg
Post on 19-Oct-2014
1.975 views
DESCRIPTION
Evaluation of the Efficacy of Punarnavadiguggulu & Mahamashadi Taila Kati Basti in the Management of Gridhrasi (Sciatica) By Dr. Gavisiddanagouda. G. Patil, Department of Kayachikitsa, Post graduate studies and research center D.G. MELMALAGI AYURVEDIC MEDICAL COLLEGE, Gadag - 582 103TRANSCRIPT

Evaluation of the Efficacy of Punarnavadiguggulu
& Mahamashadi Taila Kati Basti in the
Management of Gridhrasi (Sciatica)
By
Dr. Gavisiddanagouda. G. Patil
Dissertation Submitted to the Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore.
In partial fulfillment of the requirements for the degree of
AYURVEDA VACHASPATHI M.D. (KAYA CHIKITSA)
In
KAYACHIKITSA
Under the guidance of
Dr. V. VARADA CHARYULU, M.D. (Ayu)
And co-guidance of
Dr. RAGAVENDRA. V. SHETTER, M.D. (Ayu)
Post graduate department of Kayachikitsa, Shri D. G. Melmalagi Ayurvedic Medical College, Gadag – 582103.
2006.
Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore.
1

DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation / thesis entitled
“Evaluation of the Efficacy of Punarnavadiguggulu & Mahamashadi
Taila Kati Basti in the Management of Gridhrasi (Sciatica).” is a bonafide
and genuine research work carried out by me under the guidance of DR. V.
VaradaCharyulu, M.D. (Ayu), Professor and H.O.D, Post-graduate department
of Kayachikitsa and co-guidance of Dr. Ragavendra. V. Shetter, M.D.(Ayu), Post
graduate department of Kayachikitsa.
Date: Signature of Scholar
Place: Gadag Dr.Gavisiddanagouda. G. Patil
2

CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “Evaluation of
the Efficacy of Punarnavadiguggulu & Mahamashadi Taila Kati Basti in
the Management of Gridhrasi (Sciatica).”is a bonafide research work done
by Dr. Gavisiddanagouda. G. Patil in partial fulfillment of the requirement
for the degree of Ayurveda Vachaspathi. M.D. (Kayachikitsa).
Date:
Place: DR. V. VaradaCharyulu, M.D. (Ayu).
Professor & H.O.D
Post graduate department of Kayachikitsa.
3

CERTIFICATE BY THE CO- GUIDE
This is to certify that the dissertation entitled “Evaluation of
the Efficacy of Punarnavadiguggulu & Mahamashadi Taila Kati Basti in
the Management of Gridhrasi (Sciatica).”is a bonafide research work done
by Dr. Gavisiddanagouda. G. Patil in partial fulfillment of the requirement
for the degree of Ayurveda Vachaspathi. M.D. (Kayachikitsa).
Date: Dr. RAGAVENDRA. V. SHETTER,
M.D. (Ayu)
Place: Assistant Professor, Post graduate Department of Kayachikitsa
4

ENDORSEMENT BY THE H.O.D AND PRINCIPAL OF
THE INSTITUTION
This is to certify that the dissertation entitled “Evaluation of
the Efficacy of Punarnavadiguggulu & Mahamashadi Taila Kati Basti in
the Management of Gridhrasi (Sciatica).” is a bonafide research work
done by Dr. Gavisiddanagouda. G. Patil under the guidance of DR. V.
VaradaCharyulu, M.D. (Ayu), Professor and H.O.D, Postgraduate department of
Kayachikitsa and co-guidance of Dr. Ragavendra. V. Shetter, M.D.(Ayu),
assistant professor Post graduate department of Kayachikitsa.
DR. V. VaradaCharyulu, M.D. (Ayu) Dr. G. B. Patil.
Professor & H.O.D, Principal.
Post graduate department of Kayachikitsa.
5

COPYRIGHT
Declaration by the candidate
I hereby declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall have the rights to preserve, use and disseminate
this dissertation / thesis in print or electronic format for academic / research
purpose.
Date: Signature of Scholar
Place: Gadag
Dr.Gavisiddanagouda. G. Patil
© Rajiv Gandhi University of Health Sciences, Karnataka.
6

Acknowledgement
“Many hands make light work”. I take this opportunity to mention my deep gratitude to
several personalities who have helped me in the successful completion of this work.
I express my obligation to my honorable Guide Dr. V. Varadacharyulu M.D (Ayu),
H.O.D., P.G. Department of Kayachikitsa, P.G.S&R, D.G.M.A.M.C, Gadag for his
critical suggestions and expert guidance for the completion of this work.
I am extremely grateful and obliged to my co-guide Dr. Ragvendra.V.Shettttar, Asst.
Professor, P.G.S.&R, D.G.M.A.M.C, Gadag for his guidance and encouragement at every
step of this work.
I express my sincere gratitude to Dr. K. S. R. Prasad M.D (Ayu), Professor for their
sincere advices and assistance.
I express my deep gratitude to Dr .G.B Patil, Principal, D.G.M.A.M.C, Gadag, for his
encouragement as well as providing all necessary facilities for this research work.
I express my sincere gratitude to Dr. G. Purushothamacharyulu M.D. (Ayu), Dr.M.C.Patil
M.D (Ayu), Dr. Mulgund M.D (Ayu) and Dr. Santhosh. N.Belavadi MD (Ayu) and other
PG staff for their constant encouragement.
My modest gratitude to Dr. S.D.Yerageri, R.M.O. D.G.M.A.M.C.&H, Gadag, Dr. U.V.
Purad, Dr. K. S. Paraddi, Dr. S.H. Redder, Dr. S. A. Patil and other undergraduate
teachers for the their support in the clinical work. I thank to Shri.Nandakumar
(Statistician), Shri. V.M. Mundinamani (Librarian), Shri. Sureban, Shri Syavi, Shri. B.S.
Tippanagoudar (lab technician), Shri. Basavaraj (X-ray technician) and other hospital and
office staff for their kind support in my study.

I express my sincere thanks to my colleagues and friends Dr. B. L. Kalmat, Dr.
Venkareddy, Dr. Uday Kumar, Dr. Ratna Kumar, Dr. S. C. Sarvi, Dr. Krishna. J, Dr.
Umesh, Dr. Ashok. Akki, Dr. Ashok. M. G, Dr. Shekar Sharma, Dr. Shivaleela, Dr. K.
M. Angandi, Dr. Sulochana, Dr. Sanjeeva, Dr.Niraj kumar, Dr. Prasanna Joshi, Dr.
Vijaylakshmi, Dr. Veena. J, Dr. Manjunath. Akki, Dr. Suresh. N. Hakkandi, Dr. Ashwini
Dev, Dr. Vijay Hiremath, Dr. L.R.Biradar, Dr. Santhosh.L.Y, Dr. Satish. R, Dr.
Sharnbasappa Angadi, Dr. Anand H, Dr. Rudrakshi. D, Dr. Anitha, Dr. Jagadisha and
other post graduate scholars for their support.

LIST OF ABBREVIATIONS USED
A S – Ashtanga Sangraha
A H – Ashtanga Hridaya
Aru. – Arunadatta
A.T – After treatment
B.T – Before Treatment
B.P – Bhavaprakasha
B.R – Bavarajeeyam
Bh.S – Bhela Samhita
Ca.S – Charaka Samhita
Chi. – Chikitsa Sthana
Chak. – Chakrapani
Dal. – Dalhana
S.L.R - Straight leg raising
Gang. – Gangadhara
K.S – Kashyap Samhita
M.N – Madhav Nidana
Ni. – Nidana Sthana
N.S – Not Significant
SU.S – Sushruta Samhita
Sa.S – Sharangadhara Samhita
Sha.S – Shareera Sthana
Su. – Sutra Sthana
Si. – Siddhi Sthana
Vi. – Vimana Sthana
Y.R. – Yoga Ratnakara
List of tables Page no.
1. Table showing Lakshanas of Gridhrasi by different acharyas. 26 2. Table showing Vyavachhedaka Nidana of Gridrasi 28 3. Table showing the line of treatment of Gridrasi by different 31
Acharyas. 4. Table showing the clinical features of sciatica. 47 5. Table showing the differential diagnosis in sciatica 55 6. Table showing the properties of ingredients of Mahamasadi taila 80 - 83 7. Table showing the properties of ingredients of Dashmoola 84 8. Table showing the Demographic data related to Evaluation of 86

Punarnavadi guggulu in Gridrasi 9. Table showing the Demographic data related to 87
Evaluation of Mahamasadi taila Kati basti in Gridrasi. 10. Table Showing the Pain related chief complications 88
of patients in the study. Group A 11. Table Showing the Pain related chief complications 89
of patients in the study. Group B 12. Table Showing the Distribution of patient according 90
to age & sex among groups 13. Table Showing the Distribution of patient according 91
to occupation 14. Table Showing the Distribution of patient according 92
to Economical status 15. Table Showing the Distribution of patient according 93
to Religion 16. Table Showing the Distribution of patient according to Diet 94 17. Table Showing the Distribution of patient according 95
to type of Gridrasi 18. Table Showing the Distribution of patient according 96
to affected to leg of Sciatica 19. Table Showing the Distribution of patient according to Agni 97 20. Table Showing the Distribution of patient according to Koshta 98 21. Table Showing the Distribution of patient according to 99
Position of work in patients 22. Table Showing the Distribution of patient according to 100
Habits in patients. 23. Table Showing the Distribution of patient according to 101
Prakriti of patients 24. Table Showing the Distribution of patient on the basis 102
of age of the patient. 25. Table Showing the Distribution of patient according to 103
Chronicity of the disease among groups 26. Table Showing the Showing the incidence of range of 104
SLR in the patients 27. Table Showing the Change in the Lumbar movement in 105
the patients of group A 28. Table Showing the Change in the Lumbar movement in 106
the patients of group B 29. Table Showing the Showing the incidence of Walking time 108
in the patients 30. Table Showing the Master Chart of Subjective Parameter 109
of Group- A 31. Table Showing the Master Chart of Subjective Parameter 110
of Group- B 32. Table Showing the Master Chart of Objective Parameter 111
of Group- A 33. Table Showing the Master Chart of Objective Parameter 112
of Group- B 34. Table Showing the Statistical Assessment of Individual 113
Study Group – A (Objective Parameter) 35. Table Showing the Table Showing the Statistical Assessment 113
of Individual Study Group – B (Objective Parameter)

36. Statistical Assessment of Individual Study Group – A 113 (Objective Parameter)
37. Statistical Assessment of Individual Study Group – B 113 (Objective Parameter)
38. Table Showing the Statistical Assessment of Comparative study 114 of Group – A with Group – B, After Treatment. (Objective Parameter)
39. Statistical Assessment of Comparative study of 114 Group – A with Group – B, After Treatment. (Objective Parameter)
40. Table Showing the Statistical Assessment of Individual 116 Study Group – A (Subjective Parameter)
41. Table Showing the Statistical Assessment of Individual 115 Study Group – B (Subjective Parameter)
42. Table Showing the Statistical Assessment of Comparative 115 study of Group – A with Group – B, After Treatment. (Subjective Parameter)
43. Table Showing the Showing the Overall assessment 118 List of Chart, Figures, Photographs & Graphs Page no.
1. Showing figure of Straight leg raising test 50 2. Photo showing ingredients of Punarnavadi guggulu 3. Photo showing of procedure of Katibasti 4. Photo showing the Sacral plexus (posterior view) 5. Graph Showing the Distribution of patient according to age
& sex among groups 90 6. Graph Showing the Distribution of patient according to 91
occupation 7. Graph Showing the Distribution of patient according to 92
Economical status 8. Graph Showing the Distribution of patient according to Religion 93 9. Graph Showing the Distribution of patient according to Diet 94 10. Graph Showing the Distribution of patient according to 95
type of Gridrasi 11. Graph Showing the Distribution of patient according to 96
affected to leg of Sciatica 12. Graph Showing the Distribution of patient according to Agni 97 13. Graph Showing the Distribution of patient according to Koshta 98 14. Graph Showing the Distribution of patient according to Position 99
of work in patients 15. Graph Showing the Distribution of patient according to 100
Habits in patients. 16. Graph Showing the Distribution of patient according to 101
Prakriti of patients 17. Graph Showing the Distribution of patient on the basis of 102
age of the patient. 18. Graph Showing the Distribution of patient according to 103
Chronicity of the disease among groups 19. Graph Showing the Showing the incidence of range of 104
SLR in the patients 20. Graph Showing the Change in the Lumbar movement 106

in the patients of group A 21. Graph Showing the Change in the Lumbar movement 107
in the patients of group B 22. Graph Showing the Showing the incidence of Walking time 108
in the patients 23. Graph Showing the Showing the Overall assessment 118
TABLE OF CONTENTS Page no.
1. Introduction 1 - 3 2. Objectives 4 3. Literary review
a. Historical review of Gridrasi in ayurveda 5 - 37 b. Historical review of Gridrasi in modern science 38 - 59
4. Methodology 60 - 84 5. Observations and results 85 - 118 6. Discussion 119 - 129 7. Conclusion 130 - 132 8. Summary 133 - 135 9. Bibliography 136 - 152 10. Annexure

INTRODUCTION
INTRODUCTION
Health is the supreme foundation of virtue, wealth, enjoyment and salvation.
Diseases are the destroyers of health. Ayurveda is one such system, which prevailed 5000
years ago, which has its chief objects – preservation of health and prevention of disease.
And so this gifted science was considered the most advanced and scientifically proven in
those days and still continues it’s shining. A constant re-examination or re-evaluation of
every theory or fact is therefore, the very essence of science. Aacaarya Caraka says,
“Pa eekshaam abhiprasamsanti kusalaah”r 1
In a normal daily life, living without ambulation is almost impossible for any
human being, from the time immemorial to ultramodern life. Though the movements of
legs are so important, these are the most neglected parts of the body and vulnerable to
many diseases. The most common disorder, which affects the movement of leg
particularly in most productive period of life, is low back pain, out of which 40% of
persons will have radicular pain and this comes under the umbrella of Sciatica syndrome.
Such presentations were common in olden period too and ancient science of life named it
as Gridhrasi. It is considered as Soola Pradhaana Vaatavyaadhi. Ample description is
available in Bhrhatrayee and later treatises as well. Many researches were also conducted
on this disease still the complete cure of this is still a mirage
The physical strain of modern life, adoption of erect posture & lack of physical
exercise made a civilized human liable to backache. Backache is a national personal &
clinical problem because it is experienced by most of the population at some time & is
drain to national sources. It is a personal problem & also clinical problem as it is often
difficult to diagnose & treatment measures are conflicting & often unrewarding. It is a
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
1

INTRODUCTION
problem because of severity of pain, its persistence, its disabling effects the fear of its
origin & apprehension about future. Changing of life style of modern human being has
created several disharmonies in his biological system. As the advancement of busy,
professional and social life, improper sitting posture in offices, factories, continuous and
overexertion, jerking movements during traveling and sports – all these factors create
undue pressure to the spinal cord and play an important role in producing low backache
and sciatica.
According to Ayurveda simple freedom from disease is not health. For a person,
to be healthy he should be mentally and spiritually happy. An imbalance in Doshic
equilibrium is termed as ‘Roga’. Among Tridosha, Vata is responsible for all Cheshta and
all the diseases. As having the properties of locomotor, its dynamic entity, its intensity
and majority of its specific disorder in number more importance and attention is given to
the Vata Dosha.
A variety of Vatavyadhi described in Charaka Samhita are divided into
Samanyaja and Nanatmaja group. Gridhrasi comes under 80 types of Nanatmaja
Vatavyadhi though, occasionally there is Kaphanubandha. The name itself indicates the
way of gate shown by the patients due to extreme pain just like a Gridhra (vulture), it is
clear that this disease not only inflicts pain but also causes difficulty in walking, which is
very much frustrating and embracing to the patient. It disturbs the daily routine and
overall life of the patient.
As the medical science recognized the severity, a medicament, which relieve the
pain, improves the functional ability, restore from functional disability and controls the
condition with cost effectiveness is the need of the century.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
2

INTRODUCTION
The term Gridhrasi and sciatica of modern medicine can be termed synonymous
as much as they refer to the same singular presentation – pain along the course of leg
irrespective of etiological variations.
Now the whole scientific world has high hopes in Ayurveda as capable to provide
proper and safer methods of management in disorders where the efforts with modern
medicine have failed to achieve the desired results. Already the efficacy of the Ayurvedic
drugs and techniques has gained global popularity in musculo-skeletal disorders like
rheumatoid arthritis. Sequential administration of the Snehana, Svedana, Basti,
Siraavyadha and Agnikarma are lines of treatment of Gridhrasi as expounded in the
Ayurvedic literature.2, 3, 4 Apart from these procedures, the Samana line of treatment that
includes oral administration of medicine is of utmost importance as the administration is
very easy and also effective. But only few of research works have been carried out in
relation to the Samana treatment. Many herbal and herbo-mineral combinations are
described in Ayurveda and their therapeutic effect in Gridhrasi is yet to be explored.
Punarnavadi guggulu is one such herbo-mineral combination mentioned in the
Vangasena, prescribed by eminent scholars since many decades for a wide range of
diseases including Gridhrasi.
By looking at the individual herbal and mineral constituents, it appears that this
combination should be very proficient in combating the Gridhrasi.
As the local Samprapti Sthanasanshraya is having quiet major importance in
Gridhrasi local simultaneous Sneha Sweda procedures called Kati Basti has been selected
for the present study.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
3

Objectives
Objectives
Gridhrasi is a common entity encountered in clinical practice. It is one of the
Vataja Nanatmaja Vyadhi classified by Charaka5 .The term Gridhrasi and Sciatica of the
modern science can be considered synonymous in as much as they refer to singular
similar presentation. Back pain (Sciatica) is as much a part of the human condition as the
common cold. In fact, eight out of ten adults will experience an acute episode of back
pain at some point in their lifetime. Back pain is the second most common cause of
missed workdays due to illness and the most common cause of disability.6
Back Pain is a human condition with 60 % to 80% of the world’s population
experiencing pain at sometime in their lives.7 Pain along the course of leg irrespective of
the etiological variations i.e., pain in the sciatic nerve which is felt in the back of the
thigh, leg and foot.8 The disease ranges from simple back ache to severe complications
like deformities and ultimately cripples the patient. Scientific world has conducted
extensive studies on NSAID’s analgesics and other physiotherapies, but could not find a
suitable medication or technique, which is safe and effective.9 so the present study is
undertaken.
Objectives of the study:
1. To evaluate the role of Punarnavadi guggulu in Gridhrasi.
2. To evaluate the efficacy of Kati basti with Mahamasadi thaila.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
4

Historical Review
Historical Review
Ayurveda is the ancient medical science; History is a part of description of
any object. It is the footstep or a story from where the object comes. The origin
and progressive development of any disease is incomplete without considering its
historical background. In this way before going in detail about the Gridhrasi, an
attempt has been made to trace the reference regarding Gridhrasi in particular and
Vata Vyadhi in general. For the total coverage of historical aspect, it has been
divided in 4 parts as below:
• Vedic Period
• Pauranika Period
• Samhita Period
• Sangraha Period
Vedic period:
The Vedas are considered as the oldest recorded knowledge in our culture.
Ayurveda is the upaveda of Atharvaveda. The references of vatavyadhi are found
in Atharvaveda only. The word ‘Vatakrita’10 is used for vatavyadhi. But there is
no any specific mentioning of Gridhrasi.
Pauranika Period:
In Garuda Puraana, 11 healths related subjects are described in details. A
separate chapter is available as Vaatavyaadhi Nidaana and Gridhrasi is described
as an entity there.
Agni Puraana12 also holds identical description.
Samhita period:
Caraka Samhita:
Caraka Samhita is the first and foremost treatise, which elaborates Vaata,
Vaatavyaadhi and Gridhrasi completely. The role of Vaata Dosha in health and
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
5

Historical Review
disease is described in the first chapter itself. In 12th chapter, Vaatakalaakaleeya
of sutrasthana, Charaka has described detail about Vaata, its normal functions and
both intrinsic and extrinsic factors for its aggravation. In 17th Kiyantasiraseeya
chapter the two modes of morbidity of Vaata i.e., Caya and Prakopa as well as
different courses of Doshas in the pathogenesis of disease are described. In 20th
chapter Mahaarogadhyaaya, of Sootrasthaana, 80 types of Vaataja Naanaatmaja
Vikaaras are mentioned. Where Gridhrasi is also mentioned along with other
diseased conditions involving the legs like Paada soola, Paada bhramsa,
Paadasuptataa, Vaatakhuddataa, Oorusaada etc. In 28th chapter of Cikitsa Sthaana,
Acharya Charaka described five varieties of Vaata and etiology of its morbidity
along with its clinical features. The description of morbidity of Vaata included the
different clinical manifestation according to the site of involvement. The unique
pathogenesis of vaata vitiation due to the obstruction to its passage or functioning
is elucidated in full detail. Also the elaborate description of treatment of
imbalance of Vaata. This chapter also includes the complete description of certain
common Vaatavyaadhees in regards its etiology, pathogenesis, general principles
of treatment as well as treatment in particular.
In Caraka, at different places references related to Gridhrasi are available,
In Caraka Sootra Sthaana 5th chapter Maatraaseeteeya Adhyaaya, Paadaabhyanga
is indicated in Gridhrasi.13
In Caraka Sootra Sthaana 14th chapter Svedaadhyaaya Gridhrasi is said to be
treated by Svedana procedure.14
Two distinct clinical varieties of Gridhrasi is mentioned in 19th chapter of
Sootrasthaana entitled Ashtodareeya Adhyaaya.15
An elaborate description of symptomatology16 and treatment17 of Gridhrasi is
given in the 28th chapter of Cikitsa Sthaana.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
6

Historical Review
Sushrut Samhita:
In Saareera Sthaana, Susruta has described the structure of Prushta, Paada
and its joints. He clearly mentioned in Marma Saareera that trauma to Kukundara
Marma leads to sensory and motor loss of lower limbs and leads to disability
(Vaikalyataa).
Susruta has given much importance by allotting the first chapter of
Nidaana Sthaana itself for Vaatavyaadhees. He described the clinical features of
Gridhrasi in the same chapter. He portrayed some allied conditions like Khanja,
Pangu, Kalaayakhanja etc. but classifications not made. In Bhagna Nidaana
chapter he made many original observations pertaining to Sandhimukta
(dislocation or herniation) Kaandabhgna (fracture). His description pertaining to
classification, clinical features, prognosis etc, of Sandhimukta suits for lumbar
disc prolapse that is responsible for majority of sciatica cases.
He described identical treatment for Gridhrasi, Khanja, Pangu,
Vaatakantaka, Paadadaaha, Paadaharsha, Dhamaneegata Vaataroga etc, which is
Siraavyadha along with general measures of Vaataroga. It appears that Dhamani
indicates nerves in this context and stressed the adaptation of general Vaataroga
therapies for Gridhrasi.
In Sushrut Samhita, the description of Gridhrasi is found at following places.
In Vatavyadhi nidan- Symptomatology and pathogenesis have been described.
The symptom ‘Sakthikshepa nigraha’ has been described for the first time, which
can be correlated to the SLR test in Modern medicine. 18
In Mahavatavyadhi chikitsitam – Siraveda is described as chikitsa for Gridhrasi 19
In Siravyadhavidhi Sharira – The site of siravedha in Gridhrasi is indicated.20
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
7

Historical Review
Bhela Samhita:
The description of Vaata its normal and morbid states in Bhela Samhita
are almost analogous to Caraka Samhita in many respects.
He described the association of destruction or Heenaanga (degeneration?) and
Adhikaanga (osteophytes?) with Vaata Rogas.
In this chapter basti and raktamokshana chikitsa are described for Gridhrasi. 21
Kashyapa samhita:
In Kaasyapa Samhita there is no specific chapter for Vaata Vyaadhi
Cikitsa. However the general aspects of Vaata and its aetiopathogenesis are
discussed in Sootrasthaana in similar lines as that of Caraka.
In this samhita, Gridhrasi is considered one among 80 types of vatavikaras, but no
details are described. 22
SANGRAHA PERIOD:
Ashtanga Samgraha:
After Charaka and Sushruta, the next importance is given to Ashtanga
Sangraha.
In Doshabhediya adhyaya – Gridhrasi is included under 80 types of vatavikaras.23
In Siravyadhavidhirnama adhyaya – The site of siravedha in Gridhrasi has been
indicated.24
In Vatavyadhi Nidan – Gridhrasi is described with its symptoms. 25
Ashtang Hridaya:
In Siravyadhavidhi adhyay, Site for siravedha in Gridhrasi has been mentioned. 26
In Vatavyadhi Nidan – Symptomatology and pathogenesis of Gridhrasi is
described which is similar to that of Ashtang Samgraha. 27
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
8

Historical Review
Maadhava Nidaana:
Maadhavakara described Vaata Vyaadhees in 4 chapters i.e., Vaata
Vyaadhees, Vaatarakta, Oorusthambha and Aamavaata, a pattern that had been
adopted by many of his subsequent authors. Gridhrasi finds place in the chapter of
Vaatavyaadhi Nidaana. He described the varieties of Gridhrasi i.e., Vaataja and
Vaatakaphaja more elaborately. In chapter VataVyadhi Nidana, some specific
symptoms of two types of Gridhrasi has been highlighted i.e. Dehasya Pravakrat28
(Sciatic scoliosis) in Vataja type, Mukhapraseka and Bhaktadvesha in Vata-
kaphaja type.
Chakradatta:
This text deals with treatment part only. Cakrapaanidatta, the author of
this tretise & main commentator of Charaka samhitha, gives some herbal
preparation Snehana Chikitsa, Basti Chikitsa and Sashtra Chikitsa described in
detail under the heading of Vatavyadhi Chikitsa in the book Chakradatta.29 While
commenting on Caraka he made the following important observations pertaining
to Vaata in general with special reference to Gridhrasi. In the description of
Gridhrasi Cikitsa in Caraka, Cakrapaani commeted “Antara Kantaraangulyo Sira
Vastyagni Karma Ca”.30 He commented basing on the above that, Siraavyadana to
be performed in between Kandara and Anguli.
Gangaadhara:
Gangaadhara one of commentator of Charaka Samhita made some
importance observations particularly in Gridhrasi Cikitsa. He has taken into
consideration a Pathaantara of Caraka in the particular context i.e., “An ara
Kandaraangulyo Sirovastyagnikarma Ca”.
t
31 He indicated Sirovasti in Gridhrasi
and Agnikarma.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
9

Historical Review
Dalhana:
Dalhanaacaarya made some observations pertaining to Gridhrasi while
commenting on Susruta samhita as follows: -
He considered Gridhrasi naadi as Kandara stated by Susruta. He termed it
as Mahaasnaayu that runs from lumbar region to Gulpha. He mentioned that
Gridhrasi is termed as “Randhrini”32 by lay people. While commenting on
Gridhrasi Cikitsa he indicated Sonita Mokshana is to be performed only after
adopting general therapies of Vaata disorders.33
Indu: 34
Indu mentioned in his Sasilekha Vyaakhyaa on Ashtaanga Sangraha that
in Gridhrasi the symptoms are alike to Visvaaci. If pain and restriction of
movement occurs in the upper limb the disease is called Visvaaci and similar
presentation in lower limb termed as Gridhrasi.
Arunadutta:35
Arundatta in his Sarvanga Sundari commentary on Ashtanga Hridaya
defined clearly that due to Vata in Kandara the pain is produced at the time of
raising leg straight and it restricts the movement of thigh. This is an important
clinical test nowadays for the diagnosis of Sciatica, known as SLR.
Gadanigraha: 36
Vaidya Sothala had mentioned at the introduction of Vaata Rogaadhikaara
that Vaatavyaadhees leads to all other disorders. He described Vaatavyaadhees in
four separate chapters i.e., Vaatavyaadhi, Vaatarakta, Oorusthambha and
Aamavaata.
In this text, treatment part of Gridhrasi has been explained at two places.
In 4th chapter Prayoga Khanda termed as gutikadikara.37
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
10

Historical Review
In 14th chapter of Kayachikitsa Khanda named as Varogadhika describes Basti
chikitsa & Raktamokshana.38
Saarangdhara Samhita:
Saarangdhara mentioned Gridhrasi in 7th chapter of Purvakarama &
counted under 80 types of Vata Nanatmaja Vyadhi.39 He mentioned that the
disorder of Carana i.e., legs are forty-two like Vaataraktaja etc. Aadhamalla
commenting on varieties of disorders of Paada stated that these are Paadasuptataa,
Paadastambha, Paadaharsha, Padasphurana etc. But total forty-two varieties were
described neither by Saarangdhara nor by the commentators. Saarangdhara
appears to be one of the earliest authors to include Rasoushadhas also for the
treatment of various disorders.
Bhaavaprakaasa:
Bhaavamisra told the symptoms and treatment of Gridhrasi including the
disease in eighty types of Vaatavikaaras. Here he has told to give Shodana
Chikitsa before giving Samana Chikitsa, which will give more beneficial results.40
Even he has told to take Go- Mutra with Eranda thaila for the duration of one
month, which will cure the disease with out fail.41
Vangasena Samhita:
Vangasena followed Maadhavakara in description Nidana and Cakradatta
in describing Cikitsa. In this text, its line of treatment has been more clearly
explained by mentioning that Deepana, Pachana, Vamana, Virechana, Basti and
Siravedha should be done in Gridhrasi. Vangasena has indicated Punarnavadi
Guggulu42 in the treatment of Gridhrasi, which is selected for the study, & even
he mentioned Mahamasadi thaila43 for Gridhrasi, which is taken for Kati basti in
the present study.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
11

Historical Review
Yogaratnakara: 44
In Yogaratnakara symptomatology and classification of Gridhrasi has been
mentioned under Vatavyadhi Nidana. Few preparations have also been described
which are useful in Gridhrasi.
Basavaraajeeyam: 45
He explained many Lakshanas of Vaata along with specific Rasoushadhi
prescription for the treatment.
He included Kalaaya Khanja, Gridhrasi, Visvaaci, Khalli, Pangu, Khanja
and Oorusthambha in the list of Balavattara Vaata disorders.
PREVIOUS RESEARCH WORKS DONE AT VARIOUS INSTITUTES
JAMNAGAR –
• Arya M.P.S. (1965) : Vatavyadhi – Gridhrasi (sciatica).
• Nair P.R. (1968) : Gridhrasi Chikitsa with Rasa Taila Eranda and Rasna –
I.A.S.R., Jamngar.
• Notani H.G. (1979) : Snigdha Sweda Ka Vata Shamana Prabhava Ka
Adhyayana Gridhrasi mein Kati Basti Ke Paripekshya mein, I.P.G.T.&
R.A, Jamngar..
• Srikant U. (1984) : Studies on some systemic effect of Basti w.s.r. to
Gridhrasi Vishwachi and Pakshaghata, I.P.G.T. & R.A., Jamnagar.
• Moradia Ghanashyama (1990) : A comparative study on the role of
Shodhana and Shamana therapies of Gridhrasi, I.P.G.T. & R.A., Jamnagar.
• Shridhar Bairy T. (1997) : Phytochemica and pharmacotherapeutic
evaluation of Parijata (N. arbortristis Linn.) w.s.r. to its effect on
Gridhrasi, I.P.G.T. & R.A., Jamnagar.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
12

Historical Review
• R. Shahi (2002) : A comparative study on Aetiopathogenesis of Gridhrasi
and its management by Rasna Guggulu along with Shodhana Therapy,
I.P.G.T. & R.A., Jamnagar.
AHMEDABAD –
• Pradeep S. Nandgaonkar (1991) : The management of Gridhrasi (sciatica)
with Sephalika Ghanavati (N. arbortristis Linn), G.A. Ayu. College.
• Urmila S. Bedekar (1995) : A comparative study of Nirgundi Patrapinda
sweda and Basti Chikitsa in the management of Gridhrasi (Sciatica) , G.A.
Ayu. College.
JAIPUR:
• Sharma Loknatha (1975) : Gridhrasi Roga Ka Naidanika evam
Chikitsatmaka Adhyayana (Rasna Prayoga), NIA Jaipur.
• Sharma R. M. (1981) : A clinical study of Gridhrasi and trial of Eranda
Paka, NIA Jaipur..
• Mishra Murlidhara (1986) : A pharmacological study of Sephalika w.s.r.
to Gridhrasi, NIA Jaipur.
• Pandya Surendra Kumar (1986) : A pharmacological study of Sephalika
w.s.r. to Gridhrasi, NIA Jaipur.
• Varma R. K. (1992) : Gridhrasi Roga par Agnikarma Ki Karmukta, NIA
Jaipur.
B.H.U. –
• Pandey Pradyuman (1973) : Gridhrasi Evam Amavata Mein Bhallataka Ka
Prabhava, B.H. U. Varanasi.
MYSORE –
• Gokaranakor D. J. (1983) : Gridhrasi and its management with Shuddha
Guggulu - G.C. I.C, Mysore.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
13

Historical Review
• Shridhr B. S. (1991) : Managemnt of Gridhrasi w.s.r. to Basti- G.C.I.M.
Mysore.
TRIVENDRUM –
• Pillai Muralidharana K. (1978) : Clinical study on Gridhrasi w.s.r. o
Virechana – G. A. College, Trivendrum.
LUCKNOW –
• Arora R. L. (1982) : A role of Sephalika Patra Kwatha on Gridhrasi.
HARIDWAR –
• Sunil Kumar (1983) : Clinical study of Sephalika decoction in case of
Gridhrasi – R. S. College, Hridwar.
VIJAYAWADA –
• Rao M. K. (1986) : A clinical trial of Prijata in Gridhrasi – Dr. N.R.S.G.
Ayu. College, Vijayawada.
RAJPUR –
• Lalchand (1987) : Clinical effect of Sephalika on Sciatica – A. Ayu.
College, Rajpur.
HYDERABAD –
• Narasimnachari T. (1987) : A study of the effect of Chaturbija in Gridhrasi
– A. Ayu. College, Hyderabad.
Vyutpatti of Gridhrasi:
The word Gridhrasi is in feminine gender46 which is derived from the
Dhaatu “Gridhu” that means to covet, desire, and strive after greedily on eager
for. By the rule of “Susudhadhri Dhibhyah Krammam” as well as by adding
“Run” Pratyaya i.e., Grudh + Krun followed by Lopa of “K” and “N” the word
Grudh + Ru i.e., “Grudhr” is derived. This word is also formed in another
grammatical method as “Grudhr+ So Atonupasargah” – Adding “Kah” Pratyaya
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
14

Historical Review
leads to Gridhra + So + Ka, further by Lopa of ‘O’ and ‘K’ and ‘Sha’ is replaced
by ‘S’a’ by the rule ‘Dhaatvaadeshu Sah Sah’ to get the word Gridhraus. Finally
for this word Gridhraus which is in female gender by adding ‘DisPratyaya the
word ‘Gridhrasi’ is derived. Gridhra refers to the bird Vulture.
It is opined that, in this disease the patients gait becomes altered as his
legs becomes tense and slightly curved due to pain resembling walk of the
vulture, hence the name Gridhrasi is given.
Gridhra means vulture. Vulture is fond of meat & has a particular fashion of
eating meat. It pierces its beak deeply in the flesh & then draws it forcefully,
causing severe pain. The pain in Gridhrasi is also of the same kind, hence the
name.
Niruktti of Gridhrasi:
Following are the niruktti of Gridhrasi-
• Gridhramapisyati, ‘Syati-as-Kshepana’. 47
i i
i
• “Oorusandhau Vaatarogah” 48
• “Gr dhraam va Syaati Gacchati”. 49
The disease Gridhrasi is said to cause an abnormal throwing action in the affected
leg. The Sanskrit word Syaati in Gridhrasi means throwing action. By this
abnormality the gait of the patients is said to resemble the gait of bird vulture and
hence the name Gridhrasi to this unique illness.
“Gr dhyati Maamsamabhikankshati Satatam Iti. Grudh+Krun. Gridhro
Maamsalolupa Manushyatam. Syati Peedayati Nashyati vaa”
The above reference from Sabdakalpadruma50 states that, the word Gridh
refers to a person who is crazy of eating meat. The word Syaati in Sanskrit means
to cause suffering. Thus the word Gridhrasi applies to an illness that mostly
attacks the persons who are greedy of consuming meat.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
15

Historical Review
Paribhaasha of Gridhrasi:
As described by Aacaarya Caraka Gridhrasi is a Vaatavyaadhi
characterized by Stambha (stiffness), Ruk (pain), Toda (pricking pain) and
Spandana (frequents switching). These symptoms initially affects Sphik (buttock)
as well as posterior aspect of Kati (waist) and then gradually radiates to posterior
aspects of Ooru (thigh), Jaanu (knee), Jangha (calf) and Paada (foot).51
Paryaaya of Gridhrasi:
Following are the Paryaaya of Gridhrasi.
1. Ringhinee -by Vacaspatimisra52
The word Ringhinee means the disease that cause to creep or crawling or
that makes a person to go slowly. More over according to the Sabdakalpadruma
this term refers to Skhalana meaning displacement.
2. Randhrinee -by Dalhana53
This term is used by Dalhana while commenting on Susruta, indicates
weak point or rupture.
3. Radhina -by Aadamalla & Kaasiraama54
Aadhamalla and Kaasirama use this term in their Deepika and
Goodhaartha Deepika commentary on Saarangdhara Samhita. It indicates
pressing, compressing or destroying.
NIDAANA:
The Nidaana factors of Vaatavyaadhi in general are also the Nidaana of
the Gridhrasi, as the exclusive Nidaana of Gridhrasi is not elaborated. These vata
disorders are caused by almost the same vata prakopaka nidanas, but the different
diseases are due to the samprapti vishesh of the vitiated vayu. Caraka55 and
Bhaavaprakaasa56 clearly mention the causative factors of Vaatavyaadhi, but in
Susruta Samhita, Ashtaanga Sangraha and Ashtaanga Hridaya etc. the causes of
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
16

Historical Review
Vaatavyaadhi have not been clearly described. In addition to this, in Caraka
Samhita, Ashtaanga Sangraha and Ashtaanga Hridaya, the root cause of
Vaatavyaadhi is mentioned as either Dhaatu Kshaya or Maargaavarana.57, 58,59
The nidana mentioned in the context of vatavyadhi holds good to all types of
vatavyadhis. So, nidana can be classified under following subheading.
1. Swaprakopaka Nidana
2. Margavarodhaka Nidana
3. Marmaghatakara Nidana
4. Dhatukshayakaraka Nidana
1. Swaprakopaka nidana
a. Aharaja nidana – Excess and continuous intake of rooksha, laghu, sheeta and
rasas like katu, tikta, kashaya, and irregular food habits, insufficient diet,
exclusive diet, repeated intake of diet, intake of dried leafy vegetables, dried food
articles, cereals like varaka, kodrava, nishpava, pulses like syamaka, mudga,
kalaya, chanaka, harenu cause vata aggravation. 60
b. Viharaja nidana – Excessive or improper activities of an individual leads to
vata vitiation e.g. exercise, walking, swimming, riding on vehicles, ratrijagarana,
ativyavaya, prapatana, bharavahana, ativyayama, balavat vigraha.61
c. Kalaja nidana – Excessive exposure to air, cloudy atmosphere, rainy season and
part of summer, day, night and digestion and in old age vata vitiates.62
d. Psychological factors – Worry, grief, anger, fear, anxiety, and timidity are
mental factors. These causes vata prakopa as vata is said to be controller and
conductor of mind.63
2. Margavarodhaka nidana
Vatavyadhi manifests due to vataprakopa by dhatukshaya or
margavarodha. 64 The vegadharana and udeerana bhavas causing provocation of
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
17

Historical Review
sthanika dosha, 65 the obstruction by amadosha due to hypo functioning of agni
comes under this aspect of nidana. Kapha vitiating factors should also be
considered here as vatakaphaja Gridhrasi, causing obstruction in the normal
movement of vata.
3. Marmaghatakara nidana
Lifting of heavy weights habitual use of uncomfortable bed and
seat, fall from heights etc causes injury to katiprishtavamsha and
kukundaramarma resulting in the loss of functioning of lower limbs. 66
4. Dhatukshayakaraka nidana
The diminutions of dhatus owing to various etiological factors are also
considered as dhatukshaya increases rookshata then provoke vata.67
Samprapti:
To treat a disease, the complete knowledge of its pathogenesis is must.
The word ‘Samprapti’ means ‘Samyak Prapti of Roga’ that is the proper
understanding of the disease process. The process of manifestation of the disease
by the morbid doshas, which are circulating all over, the body is known as
Samprapti, Jati or Agati.68According to Acharya Sushrut ‘Dosha-dushya
sammurchhana janitovyadhi’. A proper understanding of Sampraapti is vital in
the planning of the treatment of any disease, since Cikitsa as enunciated in
Ayurvedic texts is nothing but Sampraapti Vighatana. 69
Charkacharya has described six types of ‘Samprapti’ namely Sankhya,
Vidhi, Vikalpa, Prudhnya, Bala, Kala. 70 Sushruta has described Samprapti
process in six stages Sanchaya, Prakopa, Prasara, Sthanasanshraya, Vyakti and
Bheda known as Satkriyakala. During Sthansanshraya Avastha the vitiated Dosha
are said to have reached to particular Sthana and get obstructed here and
intimately mix with and vitiate one, two or more Dushyas in that particular
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
18

Historical Review
portion of body. This is the reason that though Nidana of all the Vatavyadhi are
same but only due to the Samprapti Vishesha of disease Vata can produce so
many Vata disorders. If vitiated Vata is accumulated in Katu and lower
extremities by Srotosanga it produces Gridhrasi. Gridhrasi is Shoolapradhana
Vatavyadhi as Shula (pain) can not be produced without involvement of Vata
Dosha. On the basis of symptomatology given in classics, the probable Samprapti
of Gridhrasi can be treated out as below –
Samprapti ghatak:
Dosha : Vata – Apana and Vyana vayu, Kapha.
Dushya : Kandara, asthi, majja, rasa, rakta, mansa, sira, snayu.
Agni : Jatharagni
Ama :Jatharagnimandyajanita
Udbhavasthana : Pakwashaya
Samcharasthana : Rasayani
Adhisthana : Prishtha,kati, sphik
Srotas : Asthi, majja, rasa, rakta, mansa, meda
Srotodushti : Sanga
Rogamarga : Madhyam
Vyakti : Sphik, kati, prishtha, uru, janu, jangha, pada.
Bheda : Vataj and Vatakaphaj
Swabhav : Chirkari
Poorvaroopa:
Poorvaroopa are indications of impending diseases. They occur prior to
complete manifestation of disease and may suggest the forthcoming illness.71
These Purvarupa usually are exhibited during the stage of ‘Sthana Samshraya’ of
the ‘Shadkriyakala’ These Purvarupa usually are exhibited during the stage of
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
19

Historical Review
‘Sthana Samshraya’ of the ‘Shadkriyakala.’72At that time when Dosha-Dushya-
Sammurcchana takes place, some specific sign and symptoms are observed in
particular disease which may be clear or not, they are termed as Purvarupa. The
poorvarupas which can predict the following disease alone are called samanya
poorvarupa, where as those which can predict the forthcoming disease along with
the predominant dosha concerned is called vishesha poorvarupa. According to
Madhukosh, poorvarupa are the symptoms which are exhibited clearly because of
having less severe causative factors, being mild or less in number and having
avarana of doshas .73
Gridhrasi being a vatavyadhi, the samanya poorvarupa of vatavyadhi are
the poorvarupa of Gridhrasi. Charak has mentioned that Avyakta lakshana are the
poorvarupa of vatavyadhi .74 While clarifying the word ‘Avyakta’ Chakrapani
states that few mild symptoms can be considered as poorvarupa.75 Thus, the
symptoms of Gridhrasi such as ruk, toda, spandana, stabdhata, tandra, arochaka
etc. when manifested slightly can be called as poorvarupa of Gridhrasi.
Roopa:
Complete manifestation of the disease is called as Rupa. 76 Roopa appears
in the Vyaktaavastha i.e., fifth Kriyaakaala of the disease. While decribing
Gridhrasi, Acharya Charak has listed ruk, toda, stambha and muhuspandana as the
cardinal symptoms. 77 To be more precise about the track of pain, Chakrapani says
that the pain starts at sphik and then radiates to kati, prishtha, uru, janu, jangha
and pada in order. Whereas Aacaarya Sus’ruta and Aacaarya Vaagbhat’a have
added Sakthyutkshepanigraha to the cardinal signs. 78,79,80 Some signs and
symptoms like Dehasyaapi Pravakrataa, Jaanu Ooru Sandhi Spurana etc, are
specially categorized as Vaatika Lakshanas in Bhaavaprakaasa, Maadhava
Nidaana and Yogaratnaakara. 81,82 Other lakshanas like Tandra, Gaurava, Arocaka,
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
20

Historical Review
Mukhapraseka, Bhaktadwesha etc, have been stated as symptoms of Vaatakaphaja
Gridhrasi by Aacaarya Caraka. Similar references are available in textbooks like
Maadhava Nidaana, Bhaavaprakaasa and Yogaratnaakara.
Considering all the clinical manifestations of Gridhrasi, it may be sub divided into
two distinct categories
1. Saamaanya Lakshanas
2. Vis’esha Lakshanas
1. Saamaanya Lakshanas:
These clinical manifestations are seen in both Kevala Vaataja and
Vaatakaphaja type of Gridhrasi. Following are the Saamaanaya Lakshana of
Gridhrasi.
Ruk:
‘Ruk Satatam Soolam’83
‘Ruk Soolam’84
‘Ruja Vedana.’85
In Gridhrasi Ruk or Soola i.e., pain is one of the prime symptoms and is
felt throughout the lower limb, pain starts from Sphik region and radiates till the
Paada. Non radiating pain felt at sites like, Kati, Ooru, Jaanu, Jangha and Paada
region is also considered as the symptom of Gridhrasi.86 This typical radiating
pain involving the legs is suggestive of sciatica syndrome modern parlance where
pain is felt along the course of the sciatic nerve.
Toda:
‘Todah Soocivyadhanavat Vyadhaa’87
‘Toda Vicchinna Soolam’88
Intermittent pain similar to the feeling of pinprick is known as Toda, the
site of Toda is similar to the site of Soola i.e., from buttock to heal.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
21
Historical Review
Stambha:
‘Stambha Niscalakaram’89
‘Stambha Baahu Ooru Jangha Deenaam Sankochanaadhya Bhaavah’90
‘Stambha Nishkriyatvam’91
Stambha refers to the stiffness or rigidity felt at the thigh and legs and is
another symptom of Gridhrasi. As the movement of the legs worsen the pain, stiff
muscles prevent this and there by manifesting as the symptom Stambha. The
restriction to move the legs also affects the gait of the patient, as his steps are
short, cautious and slow.
Sakthnaaha Kshepam Nigrahanyat:
‘Kshepam Prasaaranam Tam Nigrahanyat Avarudhyaat Ityarthah’92
The movement Kshepana refers to extension. Patient of Gridhrasi is
unable to extend his legs as extending the legs worsens the pain. Aacaarya
Vaagbhat’a opines that it is the Utksepana i.e., lifting of the legs is affected in
Gridhrasi. Further the commentator Arunadutta very clearly defines this symptom
as ‘Paada Udharane Asakti’ 93 expressing the inability of the patient to elevate the
legs. As the extension of the legs worsens the pain patient prefers to assume the
flexed position of the legs.
Muhu Spandana:
‘Spandana Spuranam’94
‘Spandanam Hi Kincit Calanam’95
Sphurana refers to the fasciculation. Fasciculation may be present in lower
extremities in patients of Gridhrasi. To be more precise this symptom is seen in
the muscle supplied by the sciatic nerve.
Few of the symptoms of Gridhrasi are exclusively mentioned In
Basavaraajeeyam. These symptoms include Sopha, Kara Paada Vidaaha Krit,
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
22

Historical Review
Sveda, Moorcha, Bhrama and Trishna. Some of these symptoms are indicative of
vitiation of Pitta Dosha in Gridhrasi.96
2. Visesha Lakshanas:
The unique symptoms of Gridhrasi that indicate either Vaataja or
Vaatakaphaja Gridhrasi are described as Visesha Lakshana. It is evident that the
predominance of Vaata Dosha or Vaatakapha Dosha in the Sampraaptti of
Gridhrasi leads to the manifestation of Visesha Lakshana.
Vaataja Gridhrasi:
Here the Sampraaptti of the Gridhrasi is characterized by the sole
involvement of Vaata Dosha. Evidently there will not be association of Kapha
Dosha in the Sampraapti. Following are the Visesha Lakshana of Vaataja
Gridhrasi.97,98,99,100
Dehasya Vakrata:101
Maadhava described this symptom which means that patient of Gridhrasi
acquires a particular posture due to pain. It may be lateral and forward bending of
body. The patient of Gridhrasi keeps the leg in flexed position and tries to walk
without much extension in the affected side. Hence the whole body is tilted on the
affected side and he assumes the bending posture or limping. This gait is also
typical in Gridhrasi.
Stabdata Brisam: 102
The severe degree of stiffness is seen in patient suffering from Vaataja
Gridhrasi.
Sphuranam:
‘Sphuranam Gatra Dese Swalpa Calanam’103
‘Sphuranam Punah Punah Calanam’104
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
23

Historical Review
The symptom of fasciculation in Kati, Ooru, Jaanu and Jangha are similar
to the Spandana or Muhuspandana is characteristic of Vaataja Gridhrasi.
Suptata:
The patient experiences varied degree of parasthesia or sensory loss in the
affected limb.
Vaatakaphaja Gridhrasi:
Involvement of Kapha Dosha in the Sampraaptti of Gridhrasi cause the
below mentioned unique features.105, 106,107,108
Vahni Maardava:
Sluggishness of the Jatharaagni resulting in impairment of both
Abhyavaharana as well as Jarana Sakti
Tandra:
t
“Tandrayaantu Prabhodhito Api Klamayati Nidrabheda”109
This occurs due to Kapha and Tama Dosha, manifests as a feeling of
drowsiness or inability of sense organs to grasp their respective objects followed
with yawning or even fatigue without doing any labour.110, 111
Mukha Praseka:112
Mukhapraseka means excessive salivation in mouth is due to Kapha in
associated with Aama.
Bhaktadvesha:
‘Dveshamayati Yo Jan u Bhaktadvesha Sa Ucchate’113
Secondary to the sluggishness of Jaatharaagni and Kaphadusti patient of
Gridhrasi develops aversion towards food. Association of Aama is also contended
in the causation of this aversion towards food.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
24

Historical Review
Arocaka:
‘Arocakaastu Prarthite Apyupayogasamaye Anannaabhilaasha’114
‘Aruci Prarthita Anna Bhakshana Asamarthyamucchyte’115
It is a subjective symptom where patient fails to appreciate the taste in the
mouth irrespective of state of appetite. In comparison to the role of Vaata Dosha
involvement of Kapha Dosha has much to with the manifestation of Arocaka,
because the seat of Bodhaka Kapha is Jiwha which does Rasa Bodhana.
Gaurava:
‘Aardra Charmavanaddham Mivetyartha’116
Patient feels heaviness particularly in the lower limb or limbs.
Gaurava is the feeling of heaviness of the body in general or lower
extremities particular. Needless to say this symptom is due to the morbid Kapha
Dosha.
Staimityam:
‘Staimityam Gatranaam Nirutsaahatvam’117
Inertness of the body, feeling of freezing sensation in the affected lower
limb. Staimitya means timidness or frozen sensation. Due to Kapha vitiation
patient feels as if his lower extremities are covered with wet cloth.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
25

Historical Review
Table no. 1- Lakshanas of Gridhrasi:
No Lakshana C.S. S.S. A.S. A.H. M.N B.P Y.R. V.S. General 1 Ruk + - - - + + + + 2 Toda + - - - + + + + 3 Stambha + - - - + + + + 4 Spandana + - - - + + + + 5 Parshnipratyangul
i vedana - + + + - - - -
6 Sakthikshepa nigraha
- + + + - - - -
Vataj 1 Dehasya
pravakrata - - - - + + + +
2 Janusandhisphurana
- - - - + + + +
3 Jangha sandhisphurana
- - - - - + + +
4 Urusandhisphurana
- - - - + + + +
5 Katisandhisphurana
- - - - + - +
6 Suptata - - - - - - + 7 Stabdhata - - - - + + - + Vatakaphaj 1 Tandra + - - - + + + + 2 Gaurav + - - - + + + - 3 Arochak + - - - + + + + 4 Mukhapraseka - - - - + + + + 5 Bhaktadwesha - - - - + + + + 6 Agniandya - - - - + + + + 7 Staimitya - - - - - - + -
Upasaya, anupasaya:
Upasaya are the medicines, diets and regimens, which brings about
happiness either by acting directly against the cause of the disease or it may
produce such effect on the disease indirectly. It is essential to know the
Saadhyaasaadhyataa of a disease before the treatment & even to differentiate to
come to an accurate diagnosis. Caraka says, “A physician who can distinguish
between curable and incurable diseases and initiate treatment in time with the full
knowledge about the various aspects of the therapeutics can certainly accomplish
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
26

Historical Review
his object of curing the disease.118 When identical symptoms having two or more
disease are meet hostilely (or encountered) in such conditions, disease could be
best differentiated by adopting Upasaya & Anupasaya.
Upasaya for Gridhrasi has not been mentioned particularly. But, if there is
uncertainty as whether the disease is Oorusthambha or Gridhrasi, to differentiate
these two we can adopt Upasaya. If symptoms aggravate on the application of oil,
then we can consider it to be Oorusthambha and if the symptoms alleviate we can
consider it as Gridhrasi. The Nidaana mentioned for Vaatavyaadhi, Gridhrasi are
considered as Anupasaya.
Saapeksha Nidaana:
Every disease has its own cardinal signs and symptoms. But certain
diseases have resemblance in their clinical signs and symptoms. For the correct
line of treatment it is very important to make the accurate diagnosis of a particular
disease and differentiate from other similar disorders. Hence it is essential for a
physician to make differential diagnosis of the disease. Gridhrasi, also presents
with a clear picture of shifting pain in lower limbs radiating from sphik, kati,
prishtha and affecting uru, janu, jangha and pada in order.
‘sakthiutkshepanigraha’ is mentioned as a cardinal sign by Sushrut and Vagbhat.
But certain other symptoms such as stambha, toda, sphurana, ruk etc. are also
found in some other disease. Diseases like urustambha, khalli kalaykhanja,
vatakantaka can make confusion with Gridhrasi.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
27

Historical Review
Table no. 2- Vyavachhedaka Nidana:
Sl. No.
Lakshanas Gridhrasi Uru-stambha
Kalay-khanja
Vata kantak
Khalli Pada-harsha
Amavata
1 Sphikpoorvakatikramat vedana
+ - - - - - -
2 Stambha + + - - - - - 3 Ruk + + - + + - + 4 Toda + + - + - - - 5 Muhu spandana + - - - - - - 6 Sakthiutkshepa
nigraha + - - - - - -
7 Janu sphuran + - + - - - - 8 Dehasyapravakr
ata + - + - - - -
9 Kati sandhi sphurana
+ - + - - - -
10 Stabdhata + + - - - - - 11 Parshni vedana + - - + - - - 12 Difficulty in
walking + - - + - - -
13 Sandhi mukta - - + - - - - 14 Supti + - - - - + -
Sadhya – Asadhyata:
While mentioning the importance of sadhyasadhyata Charak mentions,
‘The physician who knows the differential diagnosis between the curable and the
incurable among diseases and begins treatment in time with full knowledge of the
case obtains success in his effort with certainty. But if he fails in the same he will
suffer loss of money and will tarnish his learning and fame’. 119 The separate
prognosis of Gridhrasi is not mentioned in the classics. Hence the general
principles of Sadhyasadhyata can be applied to Gridhrasi. Sadhyasadhyata of a
disease depends on various factors such as involvement of dosha, dushya, number
of premonitory and monitory symptoms, prakruti, bala and age of the patient,
sthana and kala of the vyadhi, presence of upadravas and also the qualities of
Chatushpada
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
28

Historical Review
Pathya – Apathya:
According to Ayurveda, various diseases are caused by the sanchay,
prakopa etc. of the three humours i.e. tridoshas. In person who indulges in
pathyakara ahara and vihara, the dosha sanchay doesn’t occur to such an extent as
to cause dreadful diseases. 120 Various Acharyas praise the importance of pathya.
Gridhrasi, being a vatavyadhi, the pathyapathya mentioned for vatavyadhies
should be followed. The pathya can be considered as to the ahara, aushadhi and
vihara. Ahara, vihara and aushadhi having properties opposite to vata and have
vataghna effects should be taken as pathya for vatavyadhi.
Pathya Ahara:
The patient should consume Ahara dravyas having Madhur, Amla and Lavana
rasa, Snigdha, Ushna guna and Brihana property. 121,122 Chakradatta, Bhaishajya
ratnavali and Yogaratnakar have the description of pathyapathya in details. It can
be presented here as under.123
Anna varga: Rakta shali, purana shashtika shali, kulatha, maasha, godhum, navin
tila, lavana.
Dugdha varga: Dugdha, ghrita, dadhi, matsyandika, dadhikurchika.
Shaka varga: Patola, shigru, vartaka, lashuna, tambula
Phala varga: Dadima, parushaka, badar, draksha, jambira
Mansa varga: Gramya, anupa, audaka mansa, Chataka, Kukkuta, Barhi, Tittira,
Nakra Mansa.
Drava Varga: Taila, vasa, majja, yusha, mansarasa, sura, naladambu
Aushadha: Prasarini, gokshur, neem, kshirkakoli.
Pathya Vihara:
Snigdha swedana, abhyanga, basti, shirobasti, shirahsneha, snaihik dhuma, sneha
nasya, sneha gandusha, sukhoshna parisheka, samvahana are the upakramas to be
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
29

Historical Review
followed . Also patient should reside at a place where direct wind is avoided and
sunlight is present. Patient should use soft beds and abstinence should be
followed.
Apathya Ahara:124
Chanak, kalaya, shyamak, nivar, kangu, mudga, rajmashak, all trina dhanyas,
katthilaka, nishpavabija, bimbi, kasheruka etc. should be avoided. Also tadag,
tatini jala, sheetambu, viruddhanna. Dravyas having kashaya, katu, tikta rasa
should not be consumed by a patient having vatavyadhi.
Apathya Vihara:
Indulgence in sex, excessive riding on vehicles, excessive walking,
sleeping on hard beds should be avoided. Chinta, ratrijagarana, vegavidharana,
shrama, vaman and upavasa should be avoided.
Chikitsa:
The treatment of the disease is called Chikitsa. The first and the foremost
principle to be adopted in the treatment of each and every disease is to avoid the
Nidana of the disease i.e. Nidana Parivarjana as said by acharya Sustruta. 125
Chikitsa is the couteraction of ruja. (Amarkosha). It is the process of breaking
down the pathogenesis of a disease. Diseases are caused due to vitiated doshas
involving dhatus etc. The process, which establishes equilibrium in these body
elements, is Chikitsa. 126 Gridhrasi being a Vatavyadhi, the general treatment of
Vatavyadhi is applicable to Gridhrasi also. Charak has advised dravyas having
madhur, amla, lavana, snigdha, ushna properties and upakramas like snehana,
swedana, asthapana and anuvasana basti, nasya, abhyanga, utsadana, parisheka
etc. 127 Vagbhat has stated that sneha, sweda, mruda samshodhana along with
madhur, amla, lavana dravyas. Veshtana, trasana, madya, sneha siddha with
deepan and pachan drugs, mansarasa and anuvasana basti pacify the vata. 128 In
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
30

Historical Review
Ashtang Samgraha Hemant ritucharya is indicated in vatavyadies. 129 Similarly
Sushrut has advised shirobasti, shirosneha, snaihik dhumapana, sukhoshna
gandusha for the treatment of vatavyadhies. 130
Specific Treatment of Gridhrasi:
The effective treatment of Gridhrasi can not be unified, as the pathology
involves multiple varying factors. Vitiated Vaata and association of Kapha Dosha
afflicting the Asthi Dhaatu vitiating Snaayu and Kand’ara affecting in the Asthi
produces the illness. Therefore, the procedures mainly aimed at the rectification
of the imbalances of Vaata Dosha as well as Kapha Dosha if associated.
Generally Snehana, Swedana, Vamana, Virechana, Niruha and Anuvasana
Basti, Siravedha, Raktamokshana, Agnikarma and Shastrkarma are advised by
different Acharyas.
The following table shows the line of treatment of Gridrasi by different
Acharyas.:
Table no. 3 showing the line of treatment of Gridrasi by different Acharyas
Treatment Ch. Su. A.H. B.P. Y.R. C.D. Snehana - - - - - + Swedana - - - - - + Vamana - - - + - + Virechana - - - + - + Niruha Basti + - - - - - Anuvasana Basti + - + + + + Siravedha + + + - + + Raktamokshana - - - - - - Agnikarma + - + - + + Shastrakarma - - - - - +
1. Snehana:
Snehana or oleation therapy is used externally and internally in
case of Gridhrasi. Externally snehana may be performed in the form Abhyanga,
Pizhiccil, Avagaaha, Parisheka etc. One should remember that if the Kapha Dosha
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
31

Historical Review
in involved in the pathogenesis as in case of Vaatakaphaja Gridhrasi, Snehana
Cikitsa should be restricted, as this treatment tend to worsen the imbalance of
Kapha Dosha. Taila is said to be best in vatavyadhi as it is having exactly
opposite properties as that of vata. 131 Sneha pacifies vata, brings out softness in
the body and removes malasanga. 132. It acts on sparshanendriya, which is the seat
of vayu. While mentioning the kala of abhyanga, Sushrut has stated that after 900
matras the sneha can reach majjadhatu 133 It signifies the action of sneha on asthi
& majja dhatus, which are involved in Gridhrasi.
2. Swedana:
Snehanapurvak swedana is indicated in nirama vatavyadhies while only
swedana is indicated in samavatavyadhies. Nadi, prastara, sankara etc. are the
various types of sweda. 134 Swedana activates agni, creates komalata, ruchi, clears
srotasas, diminishes tandra 135 Snehanapurvak swedana relieves the symptoms
such as harsha, toda, ruk, shotha, stambha, graha etc. It produces mruduta in the
body. Charak says that proper snehan and swedana can make even dry wood
flexible. 136
In Gridhrasi stambha, ruk, toda etc. are the main symptoms. Snehana and
swedana by virtue of their vatashamak and dhatuposhak properties are useful in
relieving the symptoms.
3. Vamana:
After the Snehana and Svedana, Sodhana is indicated in Gridhrasi.
The authors like Cakrapaani and Bhaavamisra opine that without Sodhana of
body Basti Cikitsa will not give desired effect in patients of Gridhrasi.137 Sodhana
in the form of Vamana is advised in patients suffering Gridhrasi and is specially
preferred in Vaatakaphaja Gridhrasi for evident reasons.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
32

Historical Review
4. Virecana:
Virecana has an important role in Gridhrasi. The doshas, which are not
pacified by snehana and swedana, should be removed from the body. Hence
mrudu virechana is advised for this purpose. 138 Snigdha virechana is advised for
vatavyadhies. The action of Virecana is not only limited to particular site, it has
effects on the whole body. In Vaatavyaadhi most of the authors mentioned Mridu
Virecana.139Oral administration of ‘Erand’a Sneha’ along with milk is ideal for
the Virecana purpose.140 This will help in both Vaata Anulomana as well as
smooth excretion of Mala. The Sneha Virecana clears obstruction in the Srotas
and relieves Vaata vitiation very quickly.141Vatanulomana is necessary for the
vayu obstructed by malas lodged in srotasas. It is to be done by snigdha, amla,
lavana, ushna drugs. 142
5. Basti:
Basti is the best treatment for vata. In patients who are weak or avirechya,
Niruhaa basti is advised for removal of doshas by Acharya charak. 143 Basti is
considered as param vatahara, because it makes the vata to move in its natural
paths and channels. Also it has systemic effect in eliminating doshas from the
body gradually by pakwashaya shodhana. 144. Asthapana basti is srotovishodhan
and malapahara, while anuvasana performs the function of malashodhana and
vatashaman. 145 While explaining the importance of basti, Charak says that there
is no therapeutic procedure comparable to that of basti, in as much as it possesses
rapid and useful properties of cleansing, in addition to its being a quick agent of
impletion and depletion and is unattended with danger 146
KATI BASTI
Literary Katibasti is made up of two words as such – Kati & Basti
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
33

Historical Review
1.Kati: It is a femine gender, in Caraka samhita he as told as
Sariram vatasthaneshvekam |147
i.e. it is the sthana of vata. In Susruta samhita, he as explained the pramana of kati
as, 18 angulis.148
2. Basti: The word Basti is having the meaning of
“Vas Nivase”149
“Vas Aachhadane”
“Vas Surabhikarane”150.
Here the word “Vas Aachhadane” holds good for Kati Basti. The word meaning is
“to cover” “that which surrounds” or “Aavaranam”. Hence “Dharana” or
maintainence of certain substances in the Kati Pradesha for a stipulated time may
be considered as Basti.
The word ‘Vas Nivase’ means, “to reside”. Specifically this holds good
for Niruha or Anuvasana or Uttara Basti. But in case of Kati Basti when oil is
retained for certain time it may also be considered for the definition.
Kati basti is a unique procedure, where both Snehana & Swedana, i.e.
Snehayukta swedana is done. The bassti is performed in the katipradesha so it is
called as katibasti. It is adopted procedure of Shirobasti, there is no any direct
reference of katibasti in any classics. It is the modified procedure of shirobasti. In
this procedure oil is used for the purpose of treatment, hence this may be
considered under the type of drava sweda. In case of Caraka Samhita Sankara ,
Prastara , Pariseka etc 13 types of Sweda are told.151 In the view of above said
sweda types, kati basti can put in the form of Avagaha. Avagaha means
immersion. In case of katibasti immersion/ covering of the kati region with oil
may force us to consider it as avagaha sweda. While dealing with the Drava
sweda Cakradatta mentioned it is useful in case of Vataja disorders & Kaohayukta
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
34

Historical Review
Vataja disorders.152 For the severe condition of gridrasi (sciatica) and osteo-
arthritis of the hip, a disease condition characterized by severe pain radiating
down the leg, a combination of shamana (palliative) and shodhana (eliminatory)
measures is necessary if a relapse is to be avoided.153
According to different types of classifications Kati Basti may be put under
following groups:
I According to Agni Bheda: it is Saagni sweda
II. According to Sthaana Bheda: Ekaanga Sweda
III. According to Guna Bheda: Snigdha Sweda
IV. According to Roga And Rogi Bala: Madyama Sweda
V. According to Taapaadi 4 Bhedas: Drava Sweda
VI. According to Sankaraadi 13 types: Avagaaha
While defining Swedana it has been said that Ruk, Stambha, Gaurava, Sheeta are
reduced. Katibasti also does the samething. While dealing with the Samyak
Sweda Lakshanas 154 and uses of Swedana certain things are quoted 155,156. All of
them are not exactly fitting into the context of Kati Basti.
Few of them may be summarized as below.
1. Induces Twak MardaVaata and Twak Prasaadana.
2. Restoration of functions of Sandhi by removing Stambha.
3. Reduces Gaurava and Tandra.
4. Reduces Seeta quality locally.
5. Induces Swedana locally.
Among Samyak and Asamyak Sweda Lakshanas following may be attributed to
Kati Basti.
Samyak:
S’ula Uparama
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
35
Historical Review
Seeta Uparama
Stambha Nigraha
Gaurava Nigraha
Mardhava
Sweda Srava
Vyadhiharatwa
Laghutwa
Ati Sweda :
Pitta Prakopa
Ati Sweda
Asamyak:
No S’ula Uparama
Feeling of coldness
Stambha
Gaurava
Procedure of Katibasti:
Poorva Karma:
The patient was advised to avoid Vaatakara Aahara and Vihara.
The Taila was made into lukewarm indirectly by placing it in a vessel containing
water.
Oushadha:
Mahamasadi taila
Upakarana:
Table, vessels, spoon, gas stove, wheat floor, cotton, water.
Pradhana Karma:
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
36

Historical Review
The patient was made to lie prone position on the table and Kati Pradesha
is exposed. Meanwhile sufficient quantity of masha floor was taken and made into
dough by adding required quantity of water. The dough was made into a shape of
circular ring corresponding to the area of tenderness in the lumbo-sacral region.
The inner and outer walls of the circular ring were properly sealed over the skin
so as to prevent the leakage of the Taila from the circular ring. Before pouring the
oil first check the heated oil by immersing our finger to rule out the temperature
into it. Then the heated Taila was poured in little amount to check the tolerance of
heat by the patient. According to the tolerance of the lukewarm oil, it is slowly
poured inside the circular ring with a help of a spoon. Constant temperature of the
oil was maintained inside the circular ring by rotating the oil with a finger. Once
the temperature of the oil is decreased, it was replaced with lukewarm oil again.
The procedure was continued till the patient attains Samyak Swinna Lakshanas or
upto 30 to 45 minutes. The procedure is done for 14 days in increasing order of
time i.e. initially kati basti is started with 30 minutes, then increased by 5 minutes
per day upto 45 minutes, then maintained for 7 days & decreased the time by 5
minutes per day upto 30 minutes of procedures i.e. for 14th day.
Paschat Karma:
After the procedure, oil was completely removed out from the
circular ring with the help of a cotton or spoon. The dough ring was also removed
from the back. Mild massage over the area was done. Then the patient was
advised to take lukewarm water bath after 15 to 20 minutes.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
37

Historical Review
MODERN REVIEW OF SCIATICA157
Due to the dynamics of the human spine, lumbar disc syndrome and
accompanying complaints of sciatica are long-standing afflictions of our species.
Although Greco–Roman physicians eruditely described this ailment, their uneven
diagnostic and therapeutic acumen hampered an understanding of the disorder for many
centuries. It was not until 1934, with the landmark publication of Mixter and Barr, 14 that
the herniated lumbar disc was shown to be a major cause of sciatica. This reflects only
one of many scientific discrepancies that have surrounded the concept of sciatica as a
distinct clinic pathological entity. Although quadrupeds can have disc problems, it is
probable that human’s upright posture and relative longevity have exposed our species to
a special, unwelcome affinity for lumbar disc syndrome and associated sciatica
Increasing axial somatic weight bearing, long periods of standing and walking, and the
additive stresses associated with running, bending, weight lifting, or merely jumping, can
exact a toll on the spinal column, resulting in substantial degenerative sequelae.
Anatomy And Physiology of Sciatic Nerve:
The parts affected in Gridrsi are kati, prishta (lumbo-sacral region) posterior
aspect of uru, janu, jangha and pada region.
24 asthisandhis, slightly movable constitutes lumbo-sacral region.158 The
bones of katiprushta pradesha are firmly united by mamsarajju (ligaments).159 60 peshis
are situated in prishtabhaga and each 5 peshis are situated in buttocks.160 The union of 5
sacral vertebrae, trika, the seat of avalambaka kapha and kati is one among the vata
sthanas.161,162 The lower limbs are considered as one karmendriya 163,164 and the motor
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
38

Historical Review
functions are carried by 100 peshis, 150 snayus, 2 koorchas, 2 kandaras, 30 asthis and 17
asthisandhis situated in each limb. 165
Katikatharunamarma (asthi), kukundaramarma (sandhi) and nitamba (asthi) are
situated in the shroni (pelvis), below the pelvis and on the hip region respectively.166
Sciatica nerve or Gridhrasi nadi / snayu167
The sciatic nerve is the largest and longest nerve in the human body, about as big
around as a thumb (2 cm) at its largest point. The nerve arises from the sacral plexus,
which is situated largely anterior to the sacral and formed by the ventral rami of the
spinal nerves L4 – L5 and the 1st, 2nd and 3rd (S1, S2, S3) sacral spinal nerves. Thus, the
five nerves group together on the front surface of the piriformis muscle (in the buttocks)
and become one large nerve – The Sciatic Nerve. This nerve travels then down the back
of each leg, branching out to innervate specific regions of the leg and the foot. Though
the two main divisions of sciatic nerve i.e. the tibial nerve (medial popliteal) and the
common peroneal nerve (lateral popliteal) are bound together by common sheath of
connective tissue, they are separable upto the sacral plexus because of its different root
value.
Root Value:
The tibial part of the sciatic nerve derives its fibers from the ventral division of
the ventral rami of L4 – L5 and S1, S2, S3 whereas the common peroneal part of the sciatic
nerve derives its fibers from the dorsal division of the ventral rami of L4, L5, S1 and S2.
Course And Relation:
1. In The Pelvis:
The nerve lies in front of the piriformis, under cover of its fascia.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
39

Historical Review
2. In The Glueteal Region:
The sciatic nerve enters the gluteal region through greater sciatic foramen (below
the piriformis). It runs downwards with a slight lateral convexity, passing between the
ischial tuberosity and the greater trochanter. It has a following relation in the gluteal
region.
Superficial (Posterior): Gluteal maximus and sometimes the posterior cutaneous nerve of
the thigh.
Deep (Anterior): i) Body of the ischium and nerve to the quadratus femoris; ii) Tendon of
the obturator internus with the gemelli; iii) Quadratus femoris, obturator externus, and
ascending branch of the medial circumflex femoral artery; iv) The capsule of the hip joint
which lies deep to the forementioned muscles and v) the upper, transverse fibers of the
adductors magnus.
Medial: i) Inferior gluteal nerve and vessels, ii) Sometimes the posterior cutaneous nerve
of the thigh.
3. In The Thigh:
The sciatic nerve enters the back of the thigh at the lower border of the gluteus
maximum, and runs vertically downward upto the superior angle of the popliteal fossa (at
the junction of the upper 2/3rd and lower 1/3rd of the thigh) where it terminates by
dividing into the tibial and the common peroneal nerve. It has the following relations in
the thigh.
Superficial (Posterior): The sciatic nerve is crossed by the long head of the biceps
femoris.
Deep (Anterior): The nerve lies on the adductor magnus.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
40

Historical Review
Medial: The posterior cutaneous nerve of the thigh, the semi-membranous and the semi-
tendinosus.
Lateral: Biceps femoris.
The division into tibial and common peronneal takes place usually at knee or at any point
between the pelvis and the lower 3rd of the thigh.
Tibial Nerve (Medial Popliteal Nerve): This is the longer terminal branch of the sciatic
nerve. It supplies the skin of the lateral and posterior part of the lower 1/3rd of the leg. It
runs downward through the popliteal fossa, lying first on the lateral side of the popliteal
artery, then posterior to it and finally medial to it. The popliteal vein lies in between the
nerve and artery throughout its course. The nerve enters the posterior compartment of the
leg by passing beneath the soleus muscle.
Its branches are as below:
Medial Planter: It supplies the abductor hallusis, flexor digitorum brevis and flexure
hallucis brevis muscles; skin over medial 2/3rd of planter surface of the foot.
Lateral Planter: It supplies remaining muscles of a foot not supplied by medial planter
nerve. Skin over lateral 3rd of planter surface of food.
Common Peroneal Nerve (Lateral Popliteal Nerve): This is the smaller terminal branch of
the sciatic nerver arises in the lower 3rd of the thigh. It runs downward through the
popliteal fossa, closely following the medial border of the biceps muscle. It leaves the
fossa by crossing superficially the lateral head of the gastro nemius muscle. It then passes
behind the head of the fibula, winds laterally around the neck of the bone; pierce the
peroneus longus muscle and divides in two terminal branches.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
41

Historical Review
Superficial peroneal nerve: It supplies the peroneus longus and pernoneus brevis muscles;
skin over distal 3rd of anterior aspect of leg and dorsum of foot.
Deep peroneal nerve: It supplies tibialis anterior, extensor hallucis longus, peroneus
tertius and extensor digitorum longus and brevis muscles; skin on adjacent side of great
and second toes.
Sciatic Nerve Injury
Complete lesion of this nerve is very rare and will cause complete paralysis of
hamstring muscles and all the muscles below the knee. Subtrachanteric fracture of femur
or posterior dislocations of the hip are most common cause of incomplete lesion of this
nerve. Common peroneal part of this nerve is most often affected than the medial tibial
part in injury to the sciatic nerve.
1. Common Peroneal Nerve (Lateral Popliteal):
This nerve supplies the extensor and peroneal groups of muscles of the leg as also
through its musculo-cutaneous branch it supplies the anterior and lateral aspect of the leg
and whole of the foot and toes except the skin between the great and second toe which is
supplied by its deep peroneal nerve. So, injury to this nerve will result in the foot drop
and talipes equinovarus deformity. The patient will be unable to dorsiflex and evert the
foot. The sensory loss will affect the anterior and lateral aspect of the leg, dorsum of the
foot and toes.
2. Tibial Nerve (Medial Popliteal):
This nerve is rarely injured except in open wounds. This nerve supplies the
muscles of the calf e.g., the soleus, the gastronemius, the popliteus, the plantaris, the
tibialis posterior, the flexor digitorum longus and the flexor hallucis longus. Through
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
42

Historical Review
sural nerve it supplies the lateral part of the leg and sole and through plantar nerve it
supplies the sole. So, injury to this nerve will make the patient unable to plantar flex his
ankle with loss of sensation of the whole of the sole. Thus, this deformity is known as
talipus calcaneovalgus or claw foot.
Sciatica
Sciatic – (Si-at’ik) (Mediv L – Sciaticus, a corrupt form of Gr- Ischiodicus from –
ischion, the hip joint, ISHI) which means,
Affecting the hip or the sciatic nerve
Of or belonging to the ischium or hip (The Oxford English Dictionary)
Sciatica is an extremely painful condition that often accompanies low back pain
and can affect either one or both lower extremities. Sciatica commonly refers to pain that
radiates along the sciatic nerve and is typically felt in the rear, down the back of the leg
and possibly to the foot. Sciatica is one of the most common forms of pain caused by
compression of the spinal nerves, and the leg pain often feels much worse than the back
pain.
Irritation of the fourth and fifth lumber and first sacral roots, which form the
sciatic nerve, causes pain that extends mainly down the postero and anterolateral aspects
of leg and into the foot termed sciatica.168 (Harrison’s Principles of Internal Medicine)
Causes of Sciatica169
I. True Sciatica Neuritis –
1. Leprosy
2. Polyartritis nodosa
3. Nerve injury due to injections or trauma
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
43

Historical Review
4. Post – herpetic neuralgia
II. Mechanical pressure on nerves or roots or referred pain –
1. In the spinal cord –
a. Tumors of cauda equina
b. Arachnoiditis
c. Rarely thrombosis
d. Hemorrhage or infection irritating meninges of the cord
2. In the cord space –
a. Protruded intervertebral disc
b. Extramedullary tumors
3. In the vertebral column –
a. Arthriris
b. Tuberculosis
c. Spondylolisthesis
d. Ankylosing spondylitis
e. Primary bone tumors
f. Secondary carcinoma
4. In the back –
a. Fibrositis of posterior sacral ligaments
b. Compression where the nerve leaves the pelvis in those who lie immobile on a
hard surface for long time (a form of Saturday night palsy)
5. In the thigh & buttock –
a. Fibrositis
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
44

Historical Review
b. Sacro – sciatic band
c. Hip joint or sacroiliac joint disease
d. Neurofibroma
e. Hemorrhage within or adjacent to nerve sheath in blood dyscrasias &
anticoagulant therapy
f. Misplaced therapeutic injection
6. In the pelvis –
a. Sacroiliac arthritis or strain
b. Hip disease
c. Infection of prostate or female genital tract
d. Rectal impactions
e. Tumors of lumbo –sacral plexus
Pathology
Pressure or irritation on the sciatica nerve in the spinal area results in the sciatica
syndrome. These mechanical irritations are mainly due to pathological changes in the
intervertebral disc of lumbosacral region. Intervertebral disc is the part, which contains
maximum strains and having more movements. It has annulus fibrosus – outer casing and
nucleus pulposus – inner softer jelly. As disc age, they fragment, dissociate and collapse
of gradual diminution in the concentration of hyaluronic acid. Initially this starts in the
nucleus pulposus, resulting in the central annular lamellae buckling inward while the
external concentric bands of the annular fibrosis bulge outwards, resulting in increased
mechanical stress at cartilaginous end plates at the vertical body lip.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
45

Historical Review
Degenerative changes can also affect the facet joints that lie behind and on
either side of vertebral canal and are known as oesteoarthritic changes spondylosis and
usually occur together. Extra bony growth on the vertebrae called osteophytes, may
present can press on nerve roots causing pain and irritation. As a disc degenerates it can
herniate back into the spinal canal. The weakest spot in a disc is directly under the nerve
root, and a herniation in this area puts direct pressure on the nerve which causes pain to
radiate all the ways down the patients leg to the foot.
Yet another pathological change will be lumbar spondylitis where
inflammation of the vertebral joint inturn leads to pain along the nerves. Mechanical
pressure over the nerve will happen in other changes the lumbar spinal stenosis, isthemic
spondylolisthesis causing sciatic syndrome. 170
Clinical features of sciatica 171
The characteristic feature of sciatic syndrome is that the pain originates in
lumbosacral region radiating downwards form buttock, posterolateral aspect of thigh and
the calf to the outer aspect / border of foot. Usually gradual onset but can be sudden also.
So pain is felt in the back, the buttock, the thigh, the leg and the foot - together or as
involvement of few areas.
The pain may immediately follow an injury such as strain or a fall or there
may be latent interval of 4 days or even weeks. After 2-3 days of pain in the lumbar
spine, the pain radiates down the back of one leg form buttock to ankle and sometimes to
the foot.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
46

Historical Review
Table 11
Table no. 4- Showing the clinical features of sciatica
Disc
level
Root Sensory
loss
Motor weakness Reflex
loss
Pain distribution
L3-
L4
L4
Medial calf
Quadriceps (knee
extension), thigh
adduction, tibialis
anterior (foot
dorsiflexion)
Knee
Knee medial calf
L4-
L5
L5
Lateral calf,
dorsum of
foot
Peroneii (foot eversion),
Tibialis anterior (foot
dorsiflexion), Gluteus
medius (hip abduction),
Toe dorsiflexion
Hamstring
Lateral calf, dorsal
foot, posterolateral
thigh, and
buttocks.
L5-
S1
S1
Plantar
surface of
foot lateral
aspect of
foot
Gastronemus / soleus
(foot planter flexion)
abductor hallucis (toe
flexors), gluteus
maximus (hip extension)
Ankle
Bottom foot,
posterior calf,
posterior thigh,
and buttocks.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
47

Historical Review
Symptoms - Different types of sciatica pain:172
Sciatica from L4 nerve root (usually the L3-L4 level)
The patient may have reduced knee-jerk reflex. Symptoms of sciatica stemming
from this level of the lower back may include: pain and/or numbness to the medial lower
leg and foot; weakness may include the inability to bring the foot upwards (heel walk).
Sciatica from L5 nerve root (usually the L4-L5 level)
The patient may have weakness in extension of the big toe and potentially in the
ankle called foot drop. Symptoms of sciatica originating at this level of the lower back
may include: pain and/or numbness to the top of the foot, particularly in the web between
the great toe (big toe) and the second toe.
Sciatica from S1 nerve root (the L5-S1 level)
The patient may have reduced ankle-jerk reflex. Symptoms of sciatica originating
at this level of the spine may include: pain and/or numbness to the lateral or outer foot;
weakness that results in difficulty raising the heel off the ground or walking on the
tiptoes.
Pressure on the sacral nerve roots from sacroiliac joint dysfunction
Symptoms may include: a sciatica-like pain or numbness that is often described as
a deep ache, inside the leg more so than a linear, well-defined geographic area of pain
numbness found in true sciatica.
Pressure on the sciatic nerve from the piriformis muscle
This pressure on the sciatic nerve can tighten and irritate the sciatic nerve called
piriformis syndrome. Symptoms of piriformis syndrome may include: a sciatica-like pain
and/or numbness in the leg, usually more intense above the knee, which usually starts in
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
48

Historical Review
the rear rather than the low back, often sparing the low back of symptoms or signs.
Piriformis syndrome can mimic the signs and symptoms of sciatica pain from a disc
herniation and is part of the differential diagnosis of possible causes of sciatica.
Clinical Diagnosis173
History
A detailed history regarding the nature, character of pain, its distribution, mode of
onset, chronicity, aggravating factors etc. should be taken. Also history of trauma,
infectious diseases, personal history, past medical history, any associated diseases and
also family history, obstetric history and occupational history should be inquired.
General examination
Any clues for systemic diseases should be looked for e.g. fever etc. They help for
differential diagnosis as well as treatment decisions.
Musculoskeletal Examination
Gait : The patient of sciatica has a very typical limping gait while walking.
Posture : The shape of the lumber spine is altered and the mobility is restricted. The
spinal mobility is checked by the ability to bend forwards. There may be loss of normal
lordosis. Te muscular spasm produces list to one or other side on standing, known as
sciatic scoliosis.
Tenderness : Local tenderness and presence of trigger points in the back and limb should
be identified. The following signs are helpful to confirm the diagnosis of sciatica.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
49

Historical Review
• Straight leg raising test (SLR)
There is no universal agreement about
the correct way to perform the straight
leg raising test. One method is that
when the patient is in the horizontal
position, on a counch or on the floor,
asks him to do straight leg raising.
Another method is to support the heel
in the cupped hand of the
examiner and having explained the method
to the patient, gently lift the heel from the cou
Normally the leg can be raised up to 80o - 90o w
rests on the pelvis to limit pelvic rotation. The ele
complains of pain, which is due to stretching of
assessed using goniometer. The patient is asked ab
although a little uncomfortable for the patient,
lifting the leg to the maximum permitted level.
This test is most useful diagnostically to asse
prognostically to assess the results of treatment. C
disc herniation and suggests a poor prognosis.
• Lasegue test : It elicits pain in the leg or back, whe
the knee is slightly flexed, the hip further flexed an
Evaluation Of The Efficacy Of PunarnavadigugguluBasti In The Management Of Gridhrasi (Sciatica)
Straight leg raising test. After the limb has beenraised to the position which produces pain (1), dorsiflexion at the ankle (2) exacerbates that
nch with the knee still extended.
ithout any pain. The opposite hand
vation is stopped when the patient
the affected root, and the angle is
out the site of that pain. However,
better repeatability is obtained by
ss the severity of the pain and
rossed leg pain is pathognomic of a
n at the limit of straight leg raising
d the knee then extended.
& Mahamashadi Taila Kati 50

Historical Review
• Bragaad’s test : At maximum straight leg raising, the foot is dorsiflexed to see if
tension on the posterior tibial nerve increases the sensation of pain. In the same
position, the limb is extremely rotated, relaxing the sacral plexus and then internally
rotated, increasing root tension, the experience of pain is recorded.
• Bow-string test: At the limit of straight leg raising, the knee is first flexed and then
extended and the tibial nerve compressed at the popliteal fossa with the examining
fingers of one hand, the ‘bow string test’.
• Sciatic Nerved Stretch Test: At the limit of SLR; increasing the pressure on the
irritated sciatic nerve by sharply dorsiflexing the foot producing extra pain.
• Naffziger’s Sign: Pain in the lower part of the back and legs on pressure over the
jugular vein.
Femoral nerve stretch test, sitting test, popliteal compression test, knee-jerk and ankle
jerks are also useful test for diagnosis of a disease. All the above mentioned tension signs
are generally present when a lower lumber or sacral root is involved in the pathological
process of pain. They are marked with acute root involvement from a disc protrusion, but
mild or absent with nerve root irritation from long standing degenerative change.
Also pelvic rotation and testing of sacroiliac joints by pressure on two anterior superior
iliac spines should be done.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
51

Historical Review
Neurological Examination
• The knee, ankle and plantar reflexes should be examined and they should be
symmetrical on both the sides.
• The motor power of selected muscles i.e. extensor hallucis longus (L5 or S1),
peronei (S1), quadriceps (L4 and 5) should be recorded.
• Wasting of muscles of the leg especially quadriceps should be measured.
• The sensation should be recorded by using a sharp pin. Areas of numbness,
hypoasthesias should be marked.
Others
• The dorsalis pedis and ant. tibial arteries should be palpated because claudication
pain can be confused with the redicular pain.
• Palpation of the abdomen is also mandatory, as an abdominal mass may explain
the cause of pain.
• Rectal examination should be carried out and in women vaginal examination also.
All the above signs have got some clinical value but it is not always that one or more of
them may be present and the diagnosis has to be confirmed by other measures.
Investigations
Laboratory investigations
• Urine examination for sugar etc.
• Complete blood count (C.B.C.), Erythrocyte sedimentation rate (E.S.R.) These are
especially helpful in screeing for infection or myeloma.
• Rheumatoid factor for rheumatoid arthritis, serum calcium, phosphorus, uric acid,
alkaline phosphatase in suspected hyperparathyroidism, malignancy, osteoporosis,
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
52

Historical Review
Paget’s disease and acid phosphate in suspected case of metastatic carcinoma of
prostate.
• Immunoglobulin electrophoresis is useful in diagnosis of multiple myeloma,
lymphomas and connective tissue disorders.
• Cerebrospinal fluid examination for the diagnosis of disease of the central nervous
system and spinal cord.
Other Diagnostic Techniques
• Plain radiographs : No assessment of spine is complete without radiographs.
Many causes of sciatic pain are associated with bony changes visible in
radiographs Roentgenograms of lumber spine (L4,L5,S1) in anteroposterior,
lateral and oblique planes gives differential diagnosis of narrowing of disc space,
spondylolisthesis, sclerosis of vertebral bodies, disc herniations, prolapse etc.
• Myelography : Myelography is radiography after injection of an opaque
substance into the lumber spinal subarachnoid space, usually at the L2-L3 level.
The purpose is to outline the spinal cord and nerve root in order to demonstrate
pathological lesions such as lesions or fissuring of annulus, cyst on sacral nerve
roots etc. It is obviously contraindicated if lumber puncture is contraindicated
Epidurography can be done for the diagnosis of intraspinal lesions not visualized
by conventional myelography. Discography may be done by injecting contrast
medium directly into the intervertebral disc but it is pain-provocating, carrying
risk of damage and infection. Also it is difficult to interprete.
• C.T. Scan : An important advance in radiological investigation of post fossa and
spinal lesions, from syringomyelia to lesions of the lumbosacral nerve roots and
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
53

Historical Review
cauda equina, has been the combination of CT scan with myelography using a
non-ionic water soluble medium such as iohexol. Reconstruction techniques can
be used to outline the spinal cord and nerve roots with a precision hitherto
impossible.
• MRI : MRI has several advantage over CT scanning in the assessment of cervical
and lumbosacral spines. No ionising radiations involved and intradural soft
tissue lesions can be visualized without the need for intrathecal contrast.
• Procaine Injection Test : Disappearance of the pain following local injection of
procaine or lidocaine into the tender spot is both diagnostic and therapeutic of
fibrositic pain.
• EMG: Electromyographic studies help to confirm the presence of impaired nerve
functions. Selective muscle degeneration can be identified and can suggest the
nerve root responsible.
• Nerve conduction tests support a diagnosis of peripheral nerve entrapment of the
common peroneal nerve at the neck of the fibula and of the post tibial nerve in
tarsal tunnel syndrome.
• Radionuclide Bone Scanning : Bone scanning is currently used to investigate a
wide range of spinal disorders, both benign and malignant. It is a highly sensitive
method for demonstrating bone disease, often providing an earlier diagnosis and
demonstrating more lesions than are found on X-ray.
• Aortic arteriography, intravenous pyelography and barium enema may be
necessary to find out aortic aneurysm or pelvic or rectal pathology.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
54

Historical Review
Differential diagnosis 174
Differentiation in sciatica is made on the basis of variety of
aetiopathological events, which cause compression over nerve roots or sciatic nerve.
Table No: - 5
Showing the differential diagnosis in sciatica
No Disease / condition
Age In
yrs.
Location of pain
Quality of pain
Aggravating / relieving factors
Signs
1.
Back strain
20-40
Low back, buttock posterior thigh
Ache, spasm
Increased with activity or bending
Local tenderness, limited spinal motion.
2.
Acute disc herniation
30-40
Low back to lower leg
Sharp, shooting or burning pain, parasthesia in leg.
Decreased with standing; increased with bending or sitting
Positive SLR test, weakness, asymmetric reflexes.
3.
Spondylolisthesis
Any age
Back, posterior thigh
Ache
Increased with activity a bending
Exaggeration of lumbar curve, palpable ‘step off’ tight hamstring
4.
Ankylosing spondylitis
15-40
Sacro iliac joints, lumbar spine
Ache
Morning stiffness
Decreased back motions, tenderness over sacroiliac joints.
5.
Infections
Any age
Lumbar spine, sacrum
Sharp pain, ache
Varies
Fever, percussive tenderness; may have neurologic abnormalities or decreased motion.
6.
Malignancy
>50
Affected bone(s)
Dull ache, throbbing pain, slowly progressive
Increased with recumbency or cough
May have localized tenderness neurologic signs or fever.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
55

Historical Review
Treatment: 175
The treatment is of two types –
1. Conservative Treatment
2. Surgical Treatment
Conservative Treatment
It is important to know and convey to the patient that the pain in the lower back is
very common. It can be related to certain activities, poor posture, physical stress, or
psychological stress. 90% of back pain patients improve within 4-6 weeks. Reassure
patient that 70% of acute patients will improve within 2 weeks and 90% of acute patients
will improve within 4 weeks.
Rest –
(a) Bed rest (supine position) with pillow under the knees/ Semi fowler position for 2-3
days.
(b) Modification of activities: No lifting of weights or bending forwards.
(c) Braces – Reminds the patients to be cautious, increases intra-abdominal pressure,
which in turn supports the lumbar spine. Simple abdominal corset may be used
temporarily. Discontinue as soon as possible as it encourages muscle wasting.
(d) Traction is not recommended anymore as a means of treatment. However may help
restricting the patient to the bed and to relieve musle spasm. Commonly used techniques
are:
(1) Continous traction in the hospital
(2) Intermittent in the physical therapy
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
56

Historical Review
The amount of weight required to affect the disc space is at least 25% of the body weight.
It is important to add counter-traction.
(e) Analgesics – Non-narcotics & Narcotics.
Non-narcotics: acetaminophen, ibuprofen, diclofenac, piroxicam, etoricoxib etc.
Narcotic analgesics. Codeine, propoxyphene, tramadol, morphine.
Muscle relaxants are sometimes helpful for a few days but can cause drowsiness.
Antidepressants: Are helpful but need to be mentioned for side effects and drug
interactions.
Cold and hot therapies – ice packs, superficial heat (packs/ infra red), deep (Ultrasonics
and SWD).
Injections – Epidural cortisone- It is a combination of a long –acting steroid with an
epidural anesthetic ,is a method of symptomatic treatment of leg and back pain from
discogenic diseases. Fluoroscopy control enhanced success rate. Not proved to be
effective in the treatment of acute radicular pain – useful in the management of chronic
pain of spinal stenosis. Minimum of 6 weeks of conservative treatment is recommended
for lumbar degenerative conditions.
Activity Recommendations to prevent recurrence:
Patients with acute low back pain should be advised to stay active and continue ordinary
daily activity within the limits permitted by the pain. For patients with chronic back pain,
there is evidence that exercise therapy is effective. A gradual return to normal activities is
more effective and leads to more rapid improvement. Continue routine activity while
paying attention to correct posture. Patients with acute low back problems may be more
comfortable if they temporarily limit or avoid specific activities known to increase
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
57

Historical Review
mechanical stress on the spine, especially prolonged unsupported sitting, heavy lifting
and bending or twisting the back especially while lifting.
Low stress aerobic exercise can prevent debilitation due to inactivity during the
first month of symptoms and thereafter may help to return patients to the highest level of
functioning appropriate to their circumstances. Aerobic (endurance) programs, which
minimally stress the back (walking, biking, or swimming), can be started during the first
2 weeks for most patients with acute low back problems. Conditioning exercise for trunk
muscles (especially back extensors) gradually increased, are helpful for patients with
acute low back problems, especially if symptoms persist. During the first 2 weeks these
exercises may aggravate the symptoms since they mechanically stress the back more than
endurance exercise. These exercises should not be forced in the face of increased pain.
Surgical disc removal*- Indications for Surgery 176
Mandatory and Urgent indication-
Cauda Equina syndrome with neurologicalinvolvement.
Elective indication-
• Failure of conservative treatment, trial of at least six weeks.
• Progressive or severe neuro-motor deficit.
• Persistent neuro-motor deficit > 4-6 weeks of conservative treatment
• Chronic Sciatica with positive SLR 4-6 weeks
*Disc surgery is not a cure, only provides symptomatic reliefof leg pain, it does not
restore the normal state.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
58

Historical Review
Active exercise is important for sciatica relief 177
Although it may seem counterintuitive, exercise is usually better for healing sciatic pain
than bed rest. Patients may rest for a day or two after their sciatica flares up, but after that
time period, inactivity will usually make the pain worse. Without exercise and
movement, the back muscles and spinal structures become deconditioned and less able to
support the back. The deconditioning and weakening can lead to back injury and strain,
which causes additional back pain. Exercise is also important for the health of the spinal
discs. Movement helps exchange nutrients and fluids within the discs to keep them
healthy. Many sciatica exercises focus on strengthening the abdominal and back muscles
in order to give more support for the back. Stretching exercises for sciatica target muscles
that cause pain when they are tight and inflexible. When patients engage in a regular
program of gentle strengthening and stretching exercises, they can recover more quickly
from a flare up of sciatica and can help to prevent future episodes of pain.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
59

MAHAMASADI TAILA Table no. 6 - showing the properties of ingredients of Mahamasadi taila Sl. No
Name Latin name Rasa Virya Vipaka Guna Doshaghnata Karma & Rogaghnata
1 Masha193 Phaseolus mungo
Madhura Ushna Madura Guru,Snigdha
Vata shamaka Shoolahara, balya, pakshagata, gridrasi
2 Dugda 194 Madhura Sheeta Madura Snigdha Tridosahara Brimhana, Vrishya,Balya. Vataroga, Swasa, Kasa, Pandu, Daha.
3 Tila taila195 Sesamum indicum
Madhura,Katu,Tikta, Kashaya
Ushna Madura Guru Vatanashaka Vrana,Shotha, Kushta,Vata vyadhi.
4 ChagaMamsa196
Madhura Naatisheeta
NaatiguruNaati snigda
Tridosahara Bruhmana, raktapittahara, peenasahara.
5 Manjista197 Rubia cardifolia
Madhura Tikta
Ushna Katu Guru Kapha pittanashaka
Kushta, Raktatisara, Raktaja vikara
6 Chaya198 Piper retrofractum
Katu Ushna Katu
Laghurooksha
Kaphavatha shamak
Deepana, pachana, krimignha
7 Chitraka199 Plumbago zeylanica
Katu Ushna Katu
Laghurooksha teekshna
Kaphavatha shamak
Deepana, pachana, krimignha,shothahas (yakritplecharoga) jeernapratishyayahara
80

8 Katphala200 Myrica esculenta
Kashaya, Tikta, Katu
Ushna Katu Laghu,Tikshana
Kapha Vatahara
Shootahara, Krimigna, Shoolahar, pakshagata, gridrasi
9 Shunti201 Zingiber officinale
Katu Ushna Madura Laghu,Snigdha, Guru
Kapha-vata hara
rochana, rakta shodhaka, srotovishodhaka
10 Marica202 Piper nigrum
Katu Ushna Katu Laghu,Teekshna
Kapha-vata hara
krimigna, deepana, pachana
11 Pippali203 Piper longum
Katu Anushnasheeta
Madura Laghu,Snigdha, Teekshna
Kapha-vata hara
mridu rechaka, kushtagna, deepana, yakrit uttejaka
12 Pippalimula204 Root of Piper longum
Katu Anushna MaduraSheeta
Laghu Snigdha
Kapha Vataghna
Deepana, Truptighna, Vatanulomana, Mridu rechana, Rasayana, Balya
13 Rasna205 Pluchea lanceolata
Katu Ushna Katu Guru Kaphavatashamaka
Vedanasthapana Amapachana Rasayana
14 Amalaki206 Emblica officinalis
Amlapradhanapancharasa lavana rahita
Sheeta Madura GuruRuksha Sheeta
Tridosha hara Rochana, deepana anulomana rasayana
15 Gokshura207 Tribulus terrestris
Madhura Sheeta Madhura Guru,Snigdha
Vata-Pitta shamaka
Ashmarinashana, Mutrala, Bastishothahara
16 Athmagupta208 Mucuna prurita
Madhura, Tikta
Ushana Madhura Guru,Snigdha
Vatashamaka Brumana, shoolahara
81

17 Eranda209 Ricinus cumminus
Madhura, Katu, Kashaya
Ushna Madhura Snigdha,Teekshna,Sookshm
Kapha-Vata shamaka
Mutravishodhaka
Shothahara, Krimigna
18 Shataavha210 Anethumsowa
Katu Tikta
Ushna Katu Laghu Ruksha Teekshna
Kaphavata Shamaka
Rochana, deepana, pachana anulomana shothahara
19 Saindhavalavana211
Madhura,Lavana
Sheeta Madhura Laghu,
Snigda,
Sukshma
Tridosha Shamaka
Deepana,Pachana,Rechana,Ruchikara, Hridya,
Chakshushya
20 Vida212 Kshara
Katu
Ushna Katu Ushna,
Tikshna,Suksma,
Vyavahi
Deepana,
Rochana, Vatanulomana, Hridya
21 Suvacchal213 Katu Ushna Katu Vishada Laghu
Sukshma
Pachana,RochnaBhedana, Hridya Vatanulomana
22 Ashwaghanda214 Withania somnifra
Katu, Tiktha, Kashaya
Ushna Madhura Laghu,Snigda
Kaphavata shamaka
Balya, Hridroga, Ksaya, Shoosa
23 Amruta215 Tinospara cardifolia
Tikta Kashaya
Ushna Madhura GuruSnigdha
Tridosha shamaka
Vedanasthapana, Trishnanigrahana anulomana, jwaragna rasayana
24 Yavani216 Trachyspermum ammi
Katu, Tiktha Ushna Katu Laghu,Ruksh,Thikshna
Kaphavatahara Deepaniya, Hrudya,Shoola hara
82

25 Vacha217 Acorus calamus
Katu Tikta
Ushna Katu LaghuTeekshna
Kapha Vata shamaka
Raktabhara shamaka, Vatahara, Medhya, Nidrajanana, Manovikara hara
26 Shati218 Hedychium spicatium
Katu, Tikta, Kashaya
Ushna Katu LaghuTeekshna
Kapha Vata shamaka
Vatahara, Medhya, Nidrajanana, Manovikara hara
27 Amalaki219 Emblica officinalis
Lavanavarjita pancharasa (Amlpradhan)
Sheeta Madhura Guru Ruksha Sheeta
Tridoshahara (Pitta shamaka)
Hridya,Shonitasthapana, Rasayana, Mutrala
28 Mudgaparni220 Phaseblus trilobus
Madura, Tikta Sheeta Madhura Laghu, Rookha
Vata pittagna Vataroga,Shota, Deepaneeya & Grahi
29 Masaparni221 Teramnus labialis
Madura, Tikta Sheeta Madhura Laghu, Rookha
Vata pittagna Vatanuloma, Deepaneeya, Shoota
30 Jeevanti222 Leptadenia reticulata
Madura, Sheeta Madhura Laghu,Rookha
Vata pittagna Vatanuloma, Rasayana
31 Maduka223 Glycyrhiza glabra
Madura, Sheeta Madhura Guru,snighda
Vata pittagna Vatanuloma,Nadi daurbalya
83

Dashmoola – Table no. 7 - showing the properties of ingredients of Dashmoola No. Name Latin name Rasa Virya Vipaka Guna Doshaghnata Karma & Rogaghnata 1. Bilwa224 Aegle marmelos Kashaya,
Tikta Madhur Ushna Katu Laghu,
Ruksha Vata, Kapha Balya, dipan, pachana
2. Gambhari225 Gmelina arborea Tikta, Kashaya, Madhur
Ushna Madhur Guru Tridoshashamak Deepan, pachan,medhya, shothahara, shoolahara
3. Patala226 Stereospermum suaveolens Tikta, Kashaya
Ushna Katu Laghu,Ruksha
Tridoshashamak Shothahara, shwasa,aruchi, hikka
4. Agnimanth227 Premna integrifolia Tikta, Katu Kashya, Madhur
Ushna Katu Laghu,Ruksha
Kaphavatashamak Deepan, pachan,shothahara, anulomana
5. Shyonaka228 Oroxylum indicum Tikta, Kashaya
Sheeta Katu Laghu,Ruksha
Tridoshashamak Deepan, grahi, kasa, atisara, aruchi
6. Shalaparni229 Desmodium gangeticum Madhur, Tikta
Ushna Madhur Guru,Snigdha
Tridoshashamak Vrushya, brihana,rasayana, shothahara, jwara, daha
7. Prishniparni230 Uraria picta Madhur, Tikta
Ushna Madhur Laghu,Snigdha
Tridoshashamak Deepan, Vrushya, Daha, Jwara, Shwasa.
8. Brihati231 Solanumindicum Katu, Tikta Ushna Katu Laghu,Ruksha, Tikshna
Kaphavatashamak Grahi, pachan, shoola, shwasa, kushtha
9. Kantakari232 Solanum xanthocarpum Tikta, Katu Ushna Katu Laghu, Ruksha
Kaphavatashamak Sara, deepan, pachan kasa, shwasa, parshwashoola
10. Gokshura233 Tribulus terrestris Madhura Sheeta Madhur Guru, Snigdha
Vatapittashamak Balya, deepan, ashmari, prameha, shwasa, kasa.
84

Methodology
Methodology
Ayurveda is a science with ageless concrete fundamentals and with a
holistic approach. Some centuries ago, Ayurveda was the main stream in the
society. Various factors such as the attack on India by foreigners etc. made
Ayurveda to lag behind in the race. It became alternative system of medicine. But
now, people have started realizing advantages of it over other systems of
medicine. Efforts are being made to rejuvenate this science. For revival and
progress of any science, research is an essential practice. Research is the process
of finding out the old hidden facts and from old theories and concepts, also
discovering new facts.
The therapeutic measures, drugs and procedures of Ayurveda have
remained in the practice since long on the basis of methodology prevalent in
ancient times. This is the time that the rationality of Ayurvedic therapeutic
approach is explained on modern scientific lines. Clinical trial is a way of
research and its best method to evaluate any drug or line of treatment. The trial is
a carefully designed experiment with the aim of solving unrewarding problems
conducted on scientific line and is the only way to achieve the objectives.
Research Approach.
Experimentation is the most powerful research approach. In the
present study, the objectives are to ‘Evaluate the efficacy of Punarnavadi guggulu
in the management of Gridhrasi with special reference to Sciatica’ & to ‘Evaluate
the efficacy of Mahamasadi taila kati basti in the management of Gridhrasi with
special reference to Sciatica’. The efficacy can be determined by finding out the
difference between the baseline data and after follow up data.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
60

Methodology
Source of data:
a. Patients suffering from Gridhrasi will be selected from PG S&R PG O.P.D
of DGM Ayurvedic medical college and hospital by pre-set inclusion and
exclusion criteria.
b. Trial Drug: Orally - Punarnavadi guggulu, & Katibasti – Mahamasadi taila
c. Method of collection of Data:
1. Study Design: The study design set for the present study is ‘Prospective
clinical trial’. The study was done in double group.
2. Sample Size: A minimum of total 30 patients of Gridhrasi disease will be
the sizes, which are made of 2 groups.
a. Group A: A minimum of 15 patient of Gridhrasi disease will be
treated by PUNARNAVADI GUGGULU orally.
b. Group B: A minimum of 15 patient of Gridhrasi will be treated by
Mahamasadi.thaila Kati basti.
3. Selection Criteria :
Patients suffering from Gridhrasi were selected from the Post-
graduation and Research Center OPD of D.G.Melmalagi Ayurvedic Medical
College Hospital, Gadag. The criteria for inclusion and exclusion are as follows.
a. Inclusion Criteria:
1. Presence of clinical features of Gridhrasi.
2. Patient with back pain radiating to thigh, foot.
b. Exclusion Criteria:
1. Patient below 18 and above 60 years of age.
2. Patient with other systemic disorders and malignancy.
3. Degenerative disorders with marked deformity.
4. Pregnant women and lactating mother.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
61
Methodology
5. History of major trauma causing fractures.
6. Patient of Cauda equina syndrome and other Surgical
Emergencies.
4.Posology:
1. Punarnavadi guggulu taken orally : 3 grams in divided
doses.
Anupana : Hot water
2. Katibasti by Mahamasadithaila : qs
5.Study Duration:
• 30 - days medicine given orally and follow-up for 30 days
• 14 - days of kati basti and follow-up for 30 days.
6.Data Collection
Patients selected were thoroughly examined by both subjective
and objective parameters. Detailed history and physical examination findings
were noted. Laboratory and radiological investigations such as a complete blood
count, ESR, RBS, Urine routine along with X-ray AP and Lateral views of
lumbosacral regions were done, to exclude and include in the study.
7.Assessment of Result:
Subjective and objective parameters of base line data to post medication
data comparison are used for assessment of results.
i. Subjective Parameters:
As designated in the classical ayurvedic and modern texts.
Method of assessment of Grading:
The assessment of results, by observing the severity of symptomatology.
The severities of the symptoms are assessed before and after the treatment.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
62

Methodology
Grading of parameters:
The results were evaluated by observing subjective and objective
parameters by grading method. The grading was done in the following manner.
SUBJECTIVE PARAMETERS:
A) Ruk (pain) -
The grading for the pain was given on the basis of Visual Analogue Scale
(VAS)178. Scale of 0 to 10, with 10 indicating most severe pain (visual analogue
scale, VAS).
Scale
No Pain 0 1 Mild, annoying pain 2 3 Nagging, Uncomfortable, 4 Troublesome pain 5 Distressing, miserable pain 6 7 Intense, dreadful, horrible pain 8 9 Grade 0 - No pain - No Pain
Grade 1 - Trival pain - Mild, annoying pain
Grade 2 - Mild pain - Nagging, Uncomfortable, Troublesome
pain Grade 3 - Moderate pain - Distressing, miserable pain
Grade 4 - Severe pain - Intense, dreadful, horrible pain
B) Sthambha (Stiffness)
Grade 0- No stiffness
Grade 1- With up to 25% impairment in the range of movement of joints. Patient
can perform daily routine work without any difficulty.
Grade 2 – With 25-50% impairment in the range of movement of joints. Pt has
moderate to severe difficulty in performing daily routine.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
63

Methodology
Grade 3 – With 50-75% impairment in the range of movement of joints. Pt has
moderate to severe difficulty in performing daily routine.
Grade 4 – With more than 75% impairement in the range of movements of the
joints patient totally unable to perform daily routine.
C) Toda (Piercing pain)
Grade 0- Absent
Grade 1 – Mild, occasionally in a day
Grade 2 – Moderate, after movement, daily frequent not persistent.
Grade 3 – Moderate, after movement, daily frequent and persistent.
Grade 4 – Severe, persistent
Objective Parameters:
1. SLR Test: is assessed as positive at 00 to 900 with pain, negative at 900 (without
pain)
Grade 0 - up to 900 with out pain.
Grade 1 - up to 900 with pain.
Grade 2 - can be raised more than 400 with pain.
Grade 3 - cannot be raised more than 400 with pain.
2. Movements of lumbar spine:
1. Forward Flexion :Assessed by measuring the distance between the tip
of middle finger and floor in cms.
2. Rt. Lat Flexion :Assessed by measuring the distance between the tip
of right middle finger and floor in cms
3. Left Lat flexion :Assessed by measuring the distance between the tip
of left middle finger and floor in cms.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
64

Methodology
3. Walking time - to cover 21 meters
Grade 0 - upto 20 sec
Grade 1 - upto 21-30 sec.
Grade 2 - upto 31-40 sec
Grade 3 -upto 41-50 sec.
Grade 4 - upto 51-60 sec.
9. Investigation for Exclusion:
3. X-ray of lumbo-sacral region with anterior-posterior and lateral
views
4. Hb%
5. Total WBC count
6. Differential count
7. Erythrocyte sedimentation rate
8. RBS
9. Urine routine examination
10. Overall assessment
Good relief - 100% relief
Marked response - more than 75% relief in signs and symptoms.
Moderate response - 50-75% relief in signs and symptoms.
Mild response - Below 50% relief in signs and symptoms
Not relief - No relief.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
65

Methodology
Drug Review
PUNARNAVADI GUGGULU
Punarnava179
Latin name : Boerhaavia diffusa
Family : Nyctagineae
Synonyms : Punarnava, Shothaghni
Gana : Ca-Vayah sthapana, Kasahara, Anuvasanopaga
Su- Vidarigandadi
Rasa : Madhura, Tiktha, Kashya
Guna : Laghu, Ruksha
Virya : Ushna
Vipaka : Madhura
Doshaghnata : Tridoshahara
Parts used : Moola, Beeja, Panchanga
Karma : Dipaneeya, balya,
Rogaghnata : Shootagna, Pandu, Shoolahara
Chemical Composition:
Punarnavine, Patassium nitrate, Sulphur, Chloride, Nitrate
Action and Uses:
It is bitter, Stomatic, laxative, diuretic, expectorant, diaphoretic & emetic.
Root is purgative, anthelmintic & febrifuge. Juice of the leaves is used in hepatic
disorders of jaundice, with honey.
Eranda180
Latin name : Ricinus communis
Family : Euphorbiaceae
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
66

Methodology
Synonyms : Urubuka, Gandharvahasta, Vatari, Snehaprada.
Gana : Ch.: Bhedaniya, Swedopaga, Angamarda prashamana,
Madhurskandha.
Su : Vidarigandhadi, Adhobhagahara, Vatasamshaman.
Rasa : Madhur, Kashay, Katu
Guna : Guru, Snigdha, Tikshna, Sukshma
Virya : Ushna
Vipaka : Madhur
Prabhav : Vatahara
Doshaghnata : Vatakaphaghna
Karma : Dipan, Vrushya, Shoolaghna, Shothaghna, Adhobhagadoshahara.
Rogaghnata : Vatarakta, Gulma, Hridroga, Jirnajvara, Gridhrasi, Pakshaghata.
Chemical Composition:
Castor oil consists of the glycerides of ricinolecis, isoricinoleic, stearic and
dihydroxy-stearic acids (Wallis 1967)
Action and Uses:
Root and root bark is recommended as a fabrifuge, purgative in nervous
diseases, rheumatic affections such as lumbago and sciatica. (Pharmacognosy-
CCRAS) Banerjee et al (1978) have also reported that apart from its purgative
action, the plant possesses efficacy in chronic rheumatic affections. After oral
administration, it is converted into ricinoleic acid by the pancreatic lipase, which
irritates the bowel, stimulates the intestinal glands and muscular coat to cause
purgation. It acts in 4 to 5 hrs causing liquid stools without gripping pain.
Use of erandtaila in vatavyadhies specially katishla, prishthashoola,
Gridhrasi, Sandhishoola is praised by the Acharyas. Erandtaila with its snigdha,
guru and ushna guna pacifies vata and thus vatavyadhies. With its tikshna,
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
67
Methodology
sukshma guna, katu, rasa and ushna virya it mitigates kapha dosha. Also when
vata is vitiated due to avarana of kapha, in such conditions also erand taila is
useful as it does both the functions i.e. removes the avarana and pacifies vata.
Erandtaila scrapes out the tridoshas as well as malas accumulated in pakwashaya
by sransana karma. Erand taila is both snigdha and ushna, thus has pachan and
snehanakarma. It is seen that most of the substances which perform the pachan
karma are not snigdha but erandtaila is utilized for both virechana and amapachan
property.
Neurons are made up of myelin sheath, 65% to 85% water, 16.5% grey
matter, 30% white matter. The grey matter consists of nucleoproteins. These
proteins are fatlike substances and are more abundant in non-medullated. In view
of Ayurveda, these are noting but substances having snigdha, guru, picchila etc.
gunas. Defeciency of these nucleoproteins may lead to demyelination. Such
degenerative changes in sciatic nerve cause sciatica. Hence administration of
snigdha dravyas like errand taila may provide nourishment to nervous tissue,
establishing the equilibrium of neucleoproteins. Thus process of demyelination
can be checked.
So, erandtaila is helpful in breaking down the pathology of Gridhrasi in
view of both Ayurvedic and modern medicine.
Shunthi181
Latin name : Zingiber officinale
Family : Zingiberaceae
Gana : Ch.: Truptighna, Arshoghna, Deepaniya, Shoolaprashamana,
Sheetaprashamana,Trishna Nigrahana.
Su.: Pippalyadi, Trikatu
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
68

Methodology
B.P. Panchkola, Shadushana
Synonyms : Vishwa, Nagar, Shrungavera, Katubhadra
Rasa : Katu
Guna : Laghu, Snigdha
Virya : Ushna
Vipaka : Madhur
Doshaghnata : Kaphavataghna
Part Used : Dried Vhizome
Karma : Pachan, Ruchya, Shothaghna, Shoolaghna,Anulomana.
Chemical Composition:
Camphene, Phellandrene, Zingiberine, Cineol and borneol, ginerol.
Gingerin is the active principle. Other resins and starch, K-Oxalate are also
present (M.M.)
Action and Uses:
It is aromatic, carminative, stimulant to the gastrointestinal tract and
stomachic. It removes viscid matter, strengthens memory, and removes
obstruction in the vessels. It is used is nervous diseases, incontinence of urine.
Shudda Guggulu182
Latin name : Commiphora mukul
Family : Burseraceae
Synonyms : Guggulu, Devagupta, kaushika, Pura, Mahishaaksha, Palmkasa,
Kumba, Ullukhala
Gana : Su - Eladigana
Rasa : Tiktha, Katu
Guna : Laghu, Ruksha, Vishada, Suksma, Sara, Sugandhi - Purana
Guggulu
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
69

Methodology
Snigda – Pichila – Naveena Guggulu
Virya : Ushna
Vipaka : Katu
Prabava : Tridosha hara
Doshaghnata : Tridosha hara
Parts used : Niryasa
Karma : Vedanastapaka, Rasayaniya
Rogaghnata : All Vata vikaras.
Chemical Composition:
Volatile oil, Gum – resin & Bitter principle
Action and Uses:
It acts as dipanam, ruksham, balyam, rasayanam, vrishyam,
bhagnasanthana karam. It is used in vranam, apachi, arasa, granti, skin diseases &
in vata vikaras.
Trivruth choorna183
Latin name : Operculina turpethum
Family : Convolvuaceae
Synonyms : Nishota, Trivruth, Triputa, Tribandi, Sarala, Suvaha, Rechani
Gana : Ca – Bedaniya
Su – Adobagahara, Syamadi
Rasa : Tikta, Katu
Guna : Laghu,Ruksha,Teekshna
Virya : Ushna
Vipaka : Katu
Doshaghnata : Kapha-Pittahara
Parts used : Bark of root
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
70
Methodology
Karma : Bhedana,Rechana,Lekhana,Jwaragna,Shothahara
Rogaghnata : Anaha, Vibhanda, Arasa’s, Udararoga, etc,.
Chemical Composition:
Turpethin, vol.oil, glycosoides
Action and Uses:
As it is rechaka it used in Virechanakarma, it relives Jeerna anaha,
Vibhanda, & used in the diseases as Aras’s, Udara roga, Amavata, Vatarakta,
Shoota etc,.
Nikumba choorna184
Latin name : Baliospermum monantum
Family : Euphorbiaceae
Synonyms : Danti, Udumbara, Erandaphala, Shigra, Nikumba, Pratyakshani
Gana : Ca – Virecana, Mulini, Mulasava
Su - Adobhagahara
Rasa : Katu
Guna : Guru,Teekshna
Virya : Ushna
Vipaka : Katu
Doshaghnata : K-P
Parts used : Leaves,Seedf,Root
Karma : Teekshnavirechaka,Shothahara,Jwaragna,Ashmarinashana
Rogaghnata : Shootahara, Shoolahara,
Action & Uses:
By doing lepa of Dantimula, it relives Shoota, Shoola etc,. The oil of beeja
is used as abhyanga in Vata vyadhi.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
71

Methodology
Guduchi185
Latin name : Tinospora cordifolia
Family : Menispermaceae
Synonyms : Amrita, Madhuparni, Chhinna, Rasayani
Gana : Ch - Vayasthapana, Dahaprashaman, Trishnanigrahana,
Stanyashodhan, Truptighna.
Su.:Guduchyadi, Patoladi, Aragvadhadi, Kakolyadi,
Vallipanchmoola
Rasa : Tikta, Kashaya
Guna : Laghu, Snigdha
Virya : Ushna
Vipaka : Madhur
Doshaghnata : Tridoshashamak
Parts used : Stem
Karma : Rasayan, Dipan, Balya, Samgrahi
Rogaghnata : Jvara, Pandu, Kushtha, Vatarakta, Krimi
Chemical Composition:
Giloin, a glycoside, Gilenin a non-glycoside and Gilosterol are found in
stem. Presence of bitter principles of columbin, chasmonthin and palmarin in the
drug has been reported (Chopra et al 1958). Tinosporin, tinosporic acid and
tinosporal have been reported in the stem. (Anon 1976)
Action and Uses:
Guduchi is considered as bitter tonic, astringent, diuretic and a potent
aphrodisiac. Its use has been indicated in heart diseases, hypertension and
rheumatoid arthritis.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
72

Methodology
The drug has been observed to relax smooth muscles of intenstine, uterus and
inhibit constrictor response of histamine and acetylcholine on smooth muscles
(Gupta et al, 1967). The drug has proved to be effective as antirheumatic and
diuretic as well as having anti-inflammatory properties. (Rai and Gupta, 1966).
The drug is reported to possess one fifth of the analgesic effect of sodium
salicylate.
Trikatu
Maricha186
Latin name : Piper nigrum
Family : Piperaceae
Synonyms : Maricha, Vellaja, krushna, Ushana, Suvruta
Gana : Ca – Dipaniya, Sulaprasamana, Krumigna, Sirovirecana
Su – Pippalyadi, Tryushana
Rasa : Katu
Guna : Laghu, Teekshna
Virya : Ushna
Vipaka : Katu
Doshaghnata : Kapha-Vathara
Parts used : Black pepper
Karma : Deepana,Pachana,Krimigna,Kushtagna,Jwaragna
Rogaghnata : Agnimandya, Ajeerna, Switra, Kilasa, Pama, etc
Chemical Composition:
Piperine,Piperidine,Chavicin,Lignin,Gum Volatile oil
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
73

Methodology
Action and Uses:
Pepper is acrid, pungent, hot, carminative, also used as Dipaniya.
Externally it is rubefacient & stimulant to the skin & resolvent. It acts on Swasam,
Soolam, Krimi, etc,.
Pippali187
Latin name : Piper longum
Family : Piperaceae
Synonyms : Pippali, Trikana, Tikshnatandula, Maghadhi, Vaidehikana
Gana : Ca - Kasahara, Hikkanigrahana, Sirovirechana, Vamana,
Truptigna, Dipaniya, Shoolaprashama
Su – Pippalyadi, Urdvabaghahara, Sirovirecaniya
Rasa : Katu
Guna : Laghu,Snigdha,Teekshna
Virya : Anushna shita
Vipaka : Madhura
Doshaghnata : Kapha-Vathara
Parts used : Fruit, Leaves, Root, bark
Karma : Pachana,Medhya,Triptigna,Kasahara,Rakta shodhaka
Rogaghnata : Vatahara, Shoolahara, Kasahara, Swasa hara, Kustagna
Chemical Composition:
Embelicacid,Tannin,Christembine,
Action and Uses:
Infusion is stimulant, carminative & alterative tonic also aphrodisiac,
diuretic, vermifuge & emmenagogue. Root is stimulant.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
74
Methodology
Chitraka188
Latin name : Plumbago zeylanica
Family : Plumbaginaceae
Synonyms : Chitraka, Agni - shikha
Gana : Ca – Dipaniya, Truptigna, Sulaprasamana, Bedaniya, Arasogan,
Lekaniya, Katukaskanda
Su – Pippalyadi, Mustadi, Amalakyadi, Mushkadi, Varunadi,
Aragvadaadi
Rasa : Katu
Guna : Laghu,Rukshna,Teekshna
Virya : Ushna
Vipaka : Katu
Doshaghnata : Kapha-Vathara
Parts used : Root
Karma : Deepana,Pachana,Grahi,Kantya,Twachya,Shothahara,Vajikar
Rogaghnata : Slipada, Switra, Vatavyadhi, Ajeerana, Udarashoola, Krimigna
Chemical Composition:
Plumbagin, Protinage
Action and Uses:
Root increases the digestive power & promotes the appetite.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
75

Methodology
Saindhav Lavana189
Latin name : Sodium chloride
Rasa : Lavana, Madhur
Virya : Sheeta
Vipaka : Madhur
Guna : Laghu, Snigdha, Sukshma
Doshaghnata : Tridoshaghna
Karma : Dipan, Pachan, Ruchya, Vrushya, Hridya.
Chemical Composition:
Sodium Chloride : 62.85 %
Calcium Chloride : 0.53 %
Magnesium Chloride : 0.43 %
Sodium Bicarbonate : 0.74 %
Insoluble matter : 30.34 %
Action and Uses:
It is mainly used in aruchi, ajirna, vibandha and agnimandya. In small doses it is
highly carminative, stomachic and digestive. In large doses it is cathartic, in still
larger doses it is emetic. Saindhav plays the role of carrier and helps to act the
basti at deep level. It also helps in the pratyagama of basti in proper time.
Bhallathaka190
Latin name : Semecarpus anacardium
Family : Anacardiaceae
Synonyms : Bhallataka, Bhallatamu, Agnimukhi, Arushkara
Gana : Ca – Kustagna, Dipaniya, Mutrasangraniya
Su – Nyagrodaadi, Mustadi
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
76

Methodology
Rasa : Katu,Tikta,Kashaya
Guna : Laghu,Snigdha,Teekshna
Virya : Ushna
Vipaka : Madhura
Doshaghnata : Kapha-Vata
Parts used : Fruit
Karma : Kushtagna,Shothahara,Medhya,Vajikara,Swedajanana, Hrudya
Utyaja,
Rogaghnata : It is a best Rasayana. Shota, Kusta, Krimi, Gulma, Gridrasi, etc,.
Chemical Composition: Bhilawanol, Semecarpol
Action and Uses:
Juice of the pericarp & the oil are powerful escharotics. Oil is a powerful
antiseptic & cholagogue. Kernel is a good nutritive food, also appetizer, digestive
& carminative.
Vidanga191
Latin name : Embelia ribes
Family : Myrsinaceae
Synonyms : Vidanga, Vrishanasana, Chitra – tandula, Janthunashana
Gana : Ca – Krimigna, Truptigna, Shirovirecana
Su – Surasaadi, Pippalyadi
Rasa : Katu Kashaya
Guna : Laghu,Ruksha,Teekshna
Virya : Ushna
Vipaka : Katu
Doshaghnata : Kapha-Vatahara
Parts used : FruitLeaves RootBark
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
77

Methodology
Karma : Anulomana,Deepana,Pachana,Krimigna,Kushtagna,
Rogaghnata : Shoolahara, Krimigna, Kustagna,etc.
Chemical Composition:
Embelicacid,Tannin,Christembine, Crystalline compounds of embolic acid
with Soda, Potash & Ammonia are obtained.
Action and Uses:
Fruits or dried berries (Seeds) are carminative, anthelmintic, stimulant &
alterative. Pulp is purgative. Fresh juice is cooling, diuretic & Laxative. So these
are used as shoolahara, krimigna etc.
Makshika dhatu192
Sanskrit name : Makshika
English name : Chalcopyrite
Rasa : Madhura, Tiktha
Guna : Snigdha, Guru
Virya : Sheeta
Dosagnata : Tridosha
Rogaghnata : Madhumeha, Pandu, Kustha, Jeerna jwara, etc.
Method of preparation of guggulu
Punarnava moola, Erandamoola & Shunti are made into yavakuta churna
and its kwatha is prepared. This kwatha is taken into lohapatra & sodhita guggula
is added and boiled over mandagni. While heating contents are stirred properply,
when guggulu completely gets dissolved in the above kwatha, little by little
eranda taila is added & stirred when the mass begins to solidify, add fine powder
of the prakshepaka dravyas and mixed well uniformly. The mass is then
transferred to a vessel with gritha lipta & then guggulu of 500mg are made.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
78

Methodology
Method of preparation of taila
Masa & dasamula are prepared in to yavakuta curna & dissolved in
mentioned quantity of water in a kasaya patra and kept as it is for one night &
next day these contents are reduced into 1/4th quantity over madhyamagni
according to kwtha vidhi. Kwatha is filtered & kept ready. Ajamamasa is
collected & mixed with mentioned quantity of water till it gets reduced to 1/4th
part then mamsa ras is filtered and kept ready. Murchita tila taila is taken in a
sneha patra & heated over madhyamagni then already prepared kwatha is added &
mixed well, after that cows – milk is added. While adding kwatha etc.
dravadravyas. Kalka of above mentioned drugs are to be added and mixed well,
then taila is prepared according to tailapaka vidhi. After attaining paka pariksa,
sneha patra has to be taken out from the fire & taila is filtered immediately and
obtained taila is preserved.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
79

Results
Observation and Results
In the present clinical study subjective and objective changes were
considered for the assessment of Ayurvedic management of Gridhrasi (Sciatica)
with Punarnavadi guggulu taken orally & Mahamasadi taila kati basti. Thirty
patients were selected for the study, and were divided into two groups viz. in
group A, 15 patients were administered with Punarnavadi guggulu taken orally &
in group B, 15 patients were given kati basti with Mahamasaditaila. All the
patients were assessed before and after the treatment. Both subjective and
objective changes were recorded according to the guidelines of proforma of case
sheet.
The data were collected as follows: -
1. Demographic data
2. Data related to etiological factors, type and duration of chief complaints.
3. Data related to subjective and objective parameters before and after
treatment.
4. Data related to incidence of disease.
5. Statistical analysis and assessment for response.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
85

Table No. 8 Demographic data related to Evaluation of Punarnavadi guggulu in Gridrasi.
Sex Religion Occupation Eco. status Diet Vyasana Prakriti ResponseSl.
OPD Age
M F 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
1 3827 24 + + + + + + + +
2 3160 41 + + + + + + + +
3 3967 60 + + + + + + + +
4 4095 40 + + + + + + + + +
5 4090 55 + + + + + + + +
6 4164 30 + + + + + + + +
7 4238 55 + + + + + + + +
8 4242 42 + + + + + + + +
9 4508 40 + + + + + + + +
10 4495 50 + + + + + + + +
11 4646 24 + + + + + + + +
12 4675 43 + + + + + + + +
13 72 36 + + + + + + + + +
14 226 54 + + + + + + + + +
15 439 42 + + + + + + + +
1 – Hindu, 2 – Muslim, 3 – Christian, 4 – Sedentary, 5 – Active, 6 – Labour, 7 – Poor, 8 – Middle class, 9 – Highclass, 10 – Vegetarian, 11 – Mixed, 12 – Smoking, 13 – Tobacco, 14 – Alcohol, 15 – None, 16 – Vatapitta, 17 – Vatakapha, 18 – Kaphapitta, 19 – Marked response, 20 – Moderate response, 21 – Mild response.
86

Table No. 9 Demographic data related to Evaluation of Mahamasadi taila Kati basti in Gridrasi.
Sex Religion Occupation Eco. status Diet Vyasana Prakriti ResponseSl.
OPD Age
M F 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
1 3867 65 + + + + + + + + +
2 3972 41 + + + + + + + +
3 4094 59 + + + + + + + +
4 4181 45 + + + + + + + +
5 4201 28 + + + + + + + +
6 4664 55 + + + + + + + +
7 4611 35 + + + + + + + +
8 59 45 + + + + + + + +
9 81 65 + + + + + + + +
10 4728 35 + + + + + + + +
11 669 20 + + + + + + + +
12 962 55 + + + + + + + +
13 1008 30 + + + + + + + +
14 1030 33 + + + + + + + +
15 1238 45 + + + + + + + +
1 – Hindu, 2 – Muslim, 3 – Christian, 4 – Sedentary, 5 – Active, 6 – Labour, 7 – Poor, 8 – Middle class, 9 – Highclass, 10 – Vegetarian, 11 – Mixed, 12 – Smoking, 13 – Tobacco, 14 – Alcohol, 15 – None, 16 – Vatapitta, 17 – Vatakapha, 18 – Kaphapitta, 19 – Marked response, 20 – Moderate response, 21 – Mild response.
87

Table No. 10
Showing the Pain related chief complications of patients in the study. Group A On set Variety Nature Relieving factors Site Pain at Sl.No
A B C D E F G H I J K L M N O P Q R S T
1 + + + + + + +2 + + + + + + + +3 + + + + + + + +4 + + + + + + + + + +5 + + + + + + +6 + + + + + + + + + +7 + + + + + + + +8 + + + + + + + +9 + + + + + + + +10 + + + + + + + +11 + + + + + + + +12 + + + + + + + +13 + + + + + + + +14 + + + + + + + +15 + + + + + + + + A – Sudden, B – Gradual, C – Acute, D – Chronic, E – Local, F – General, G – Radiating, H – Rest, I – Pain relievers, J – Pressure, K – Lumbodorsal, L – Lumbar, M – Lumbo sacral, N – Spik, O – Kati, P – Prushta, Q – Uru, R – Janu, S – Jangha, T – Pada.
88

Table No. 11
Showing the etiological factors and chief complications of patients in the study. Group B
On set Variety Nature Relieving factors Site Pain at Sl.No
A B C D E F G H I J K L M N O P Q R S T
1 + + + + + + + +2 + + + + + + + +3 + + + + + + + +4 + + + + + + + +5 + + + + + + + +6 + + + + + + + +7 + + + + + + + +8 + + + + + + + +9 + + + + + + +10 + + + + + + + +11 + + + + + + + +12 + + + + + + + +13 + + + + + + + +14 + + + + + + + +15 + + + + + + + + A – Sudden, B – Gradual, C – Acute, D – Chronic, E – Local, F – General, G – Radiating, H – Rest, I – Pain relievers, J – Pressure, K – Lumbodorsal, L – Lumbar, M – Lumbo sacral, N – Spik, O – Kati, P – Prushta, Q – Uru, R – Janu, S – Jangha, T – Pada.
89

Results
Table no. 12- Distribution of patient according to age & sex among groups.
Group A Group B Age in Yrs
No. of Patient
%
M % F % M % F %
20-29 4 13.33% 1 6.66% 1 6.66% 1 6.66% 1 6.66% 30 -39 6 20% 1 6.66% 1 6.66% 1 6.66% 3 20% 40 -49 10 33.33% 2 13.33% 4 26.66% 0 0% 4 26.66% 50 -59 7 23.33% 2 13.33% 2 13.33% 3 20% 0 0% 60 -69 3 10% 1 6.66% 0 0% 2 13.33% 0 0% Above chart shows most of the patients were of age group of 40 – 49 yrs is of 10
(33.33%) in number. In that female patients were predominant in study i.e. 4
(26.66%) in group A & 4 (26.66%) in group B. Minimum number of patients
were of age groups of 60 – 69 yrs is of 3(10%) in number. In that 1(6.66%)
patient is male of Grade A & 2(13.33%) is in Group B.
Sex
7 7
8 8
6.57
7.58
8.5
No. of Patient No. of Patient
Group A Group B
No.
of P
atie
nt
MaleFemale
Age of the patient
1 1 1 11 1 1
32
4
0
4
2 23
01
0
2
0012345
No. of Patient No. of Patient No. of Patient No. of Patient
Male Female Male Female
Group A Group B
Num
ber o
f pat
ient
20 – 29 30 – 39 40 – 49 50 – 59 60 – 69
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
90

Results
Table no. 13 Distribution of patient according to occupation.
Group A Group B Occupation
No. of Patient % No. of Patient %
Sedentary 2 13.33% 2 13.33% Active 11 73.33% 12 80% Labour 2 13.33% 1 6.66% Others 0 0% 0 0%
Table shows among 15 patients in Group A, maximum are active 11(73.33%),
minimum 2(13.33%) was sedentary & rest 2(13.33%) are labours. In Group B
maximum patient were active 12(80%), minimum were labour 1(6.66%) & rest
2(13.33%) were Sedentary.
Distribution of patient according to occupation.
2
11
20
2
12
1 00
5
10
15
Sedentary Active Labour Others
Occupation
Num
ber o
f pa
tient
Group A No. of Patient Group B No. of Patient
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
91

Results
Table no.14 Distribution of patient according to Economical status
Group A Group B Economical status
No. of Patient % No. of Patient %
Poor 2 13.33% 1 6.66% Middle class 13 86.66% 14 93.33% High class 0 0% 0 0%
Among 15 patient in Group A, maximum patient belongs to middle class,
13(86.66%) whereas no patients were of higher class & only 2(13.33%) patient
were of poor class. In Group B maximum patient belongs to middle class,
14(93.33%), where as no patient were of higher class & only 1(6.66%) were of
poor class.
Distribution of patient according to Economical status
2 1
13 14
0 00
5
10
15
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f pat
iient
Poor Middle class High class
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
92

Results
Table no. 15 Distribution of patient according to Religion
Group A Group B Religion
No. of Patient % No. of Patient %
Hindu 13 86.66% 14 93.33% Muslim 2 13.33% 1 6.66%
Christian 0 0% 0 0% Others 0 0% 0 0%
Among 15 patient in Group A maximum patient belongs to Hindu, 13(86.66%)
where as 2(13.33%) patients were of Muslim, Christians & other religions were
not reported in present study. In Group B maximum patient belongs to Hindu,
14(93.33%), where as 1(6.66%) patient is of Muslim, Christians & other religions
were not reported in present study.
Distribution of patient according to Religion
13 14
2 10 00 00
5
10
15
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f pa
tient
s
Hindu Muslim Christian Others
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
93
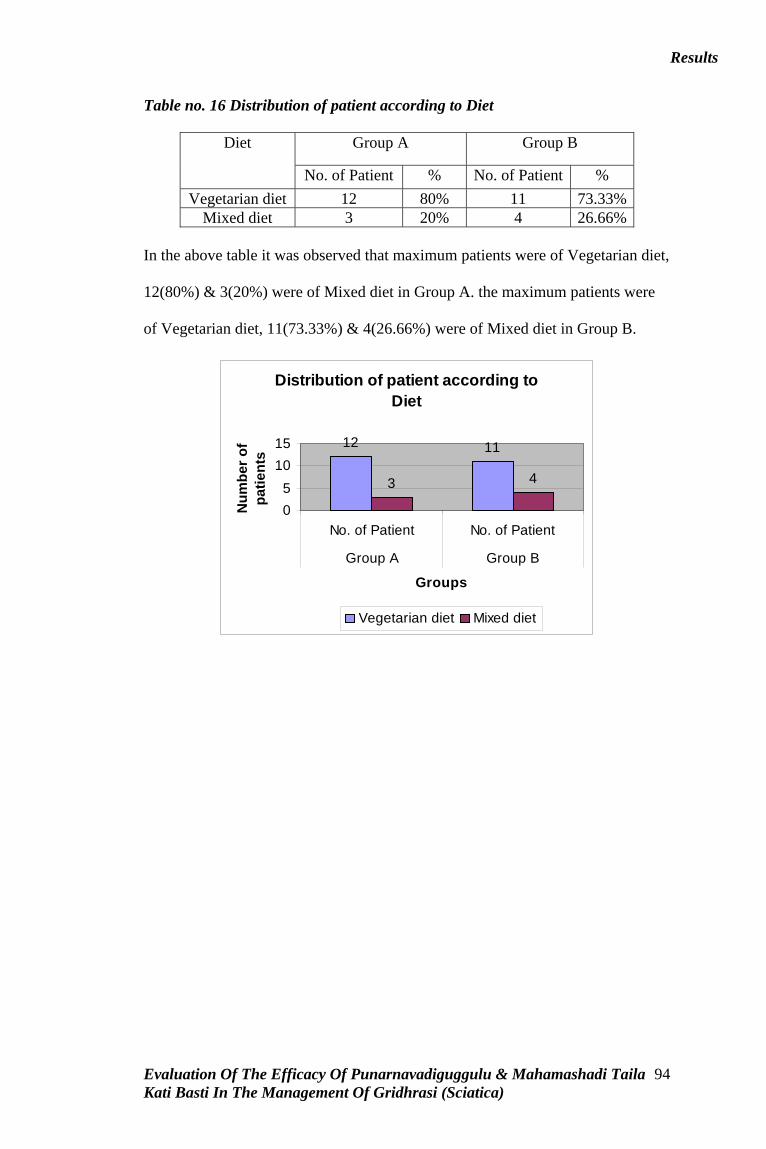
Results
Table no. 16 Distribution of patient according to Diet
Group A Group B Diet
No. of Patient % No. of Patient %
Vegetarian diet 12 80% 11 73.33% Mixed diet 3 20% 4 26.66%
In the above table it was observed that maximum patients were of Vegetarian diet,
12(80%) & 3(20%) were of Mixed diet in Group A. the maximum patients were
of Vegetarian diet, 11(73.33%) & 4(26.66%) were of Mixed diet in Group B.
Distribution of patient according to Diet
12 11
3 4
05
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f pa
tient
s
Vegetarian diet Mixed diet
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
94

Results
Table no.17 Distribution of patient according to type of Gridrasi
Group A Group B Type of Gridhrasi
No. of Patient % No. of Patient %
Vataja 10 66.66% 4 26.66% Vatakaphaja 5 33.33% 11 73.33%
In the above table it was observed that maximum patients were of Vataja types,
10(66.66%) & 5(33.33%) is of Vatakaphaja in Group A. the maximum patient
were of Vatajakaphaja, 11(73.33%) & 4(26.66%) is of Vataja in Group B.
Distribution of patient according to type of Gridrasi
10
45
11
05
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pa
tient
s
Vataja Vatakaphaja
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
95
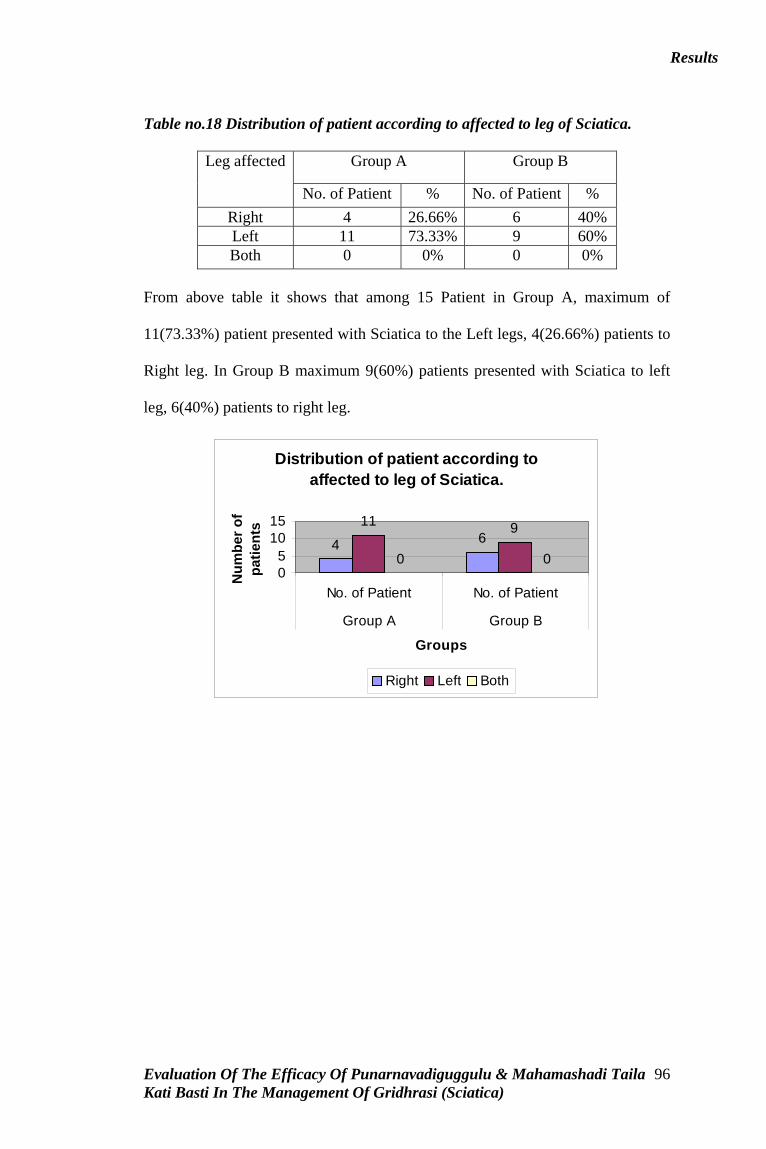
Results
Table no.18 Distribution of patient according to affected to leg of Sciatica.
Group A Group B Leg affected
No. of Patient % No. of Patient %
Right 4 26.66% 6 40% Left 11 73.33% 9 60% Both 0 0% 0 0%
From above table it shows that among 15 Patient in Group A, maximum of
11(73.33%) patient presented with Sciatica to the Left legs, 4(26.66%) patients to
Right leg. In Group B maximum 9(60%) patients presented with Sciatica to left
leg, 6(40%) patients to right leg.
Distribution of patient according to affected to leg of Sciatica.
4 611 9
0 005
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f pa
tient
s
Right Left Both
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
96
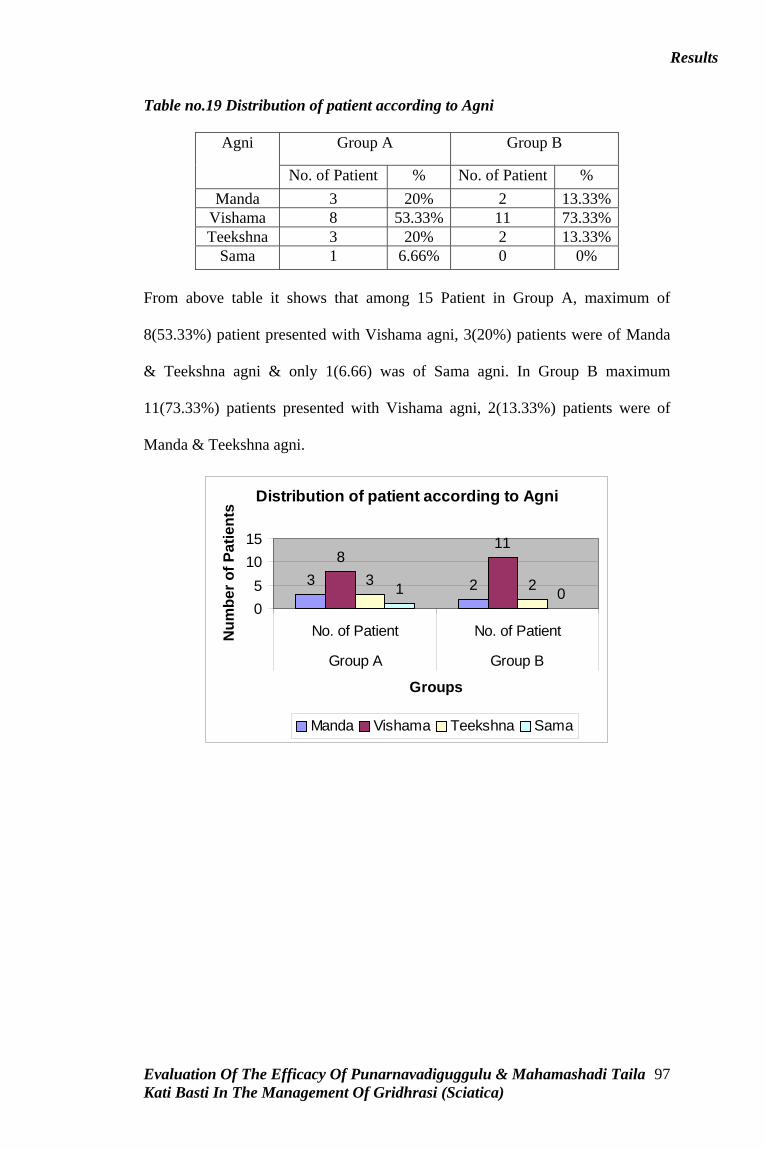
Results
Table no.19 Distribution of patient according to Agni
Group A Group B Agni
No. of Patient % No. of Patient %
Manda 3 20% 2 13.33% Vishama 8 53.33% 11 73.33% Teekshna 3 20% 2 13.33%
Sama 1 6.66% 0 0%
From above table it shows that among 15 Patient in Group A, maximum of
8(53.33%) patient presented with Vishama agni, 3(20%) patients were of Manda
& Teekshna agni & only 1(6.66) was of Sama agni. In Group B maximum
11(73.33%) patients presented with Vishama agni, 2(13.33%) patients were of
Manda & Teekshna agni.
Distribution of patient according to Agni
3 2
811
3 21 005
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pat
ient
s
Manda Vishama Teekshna Sama
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
97

Results
Table no.20 Distribution of patient according to Koshta
Group A Group B Koshta
No. of Patient % No. of Patient %
Mridu 1 6.66% 1 6.66% Madhya 4 26.66% 8 53.33% Kroora 10 66.66% 6 40% Sama 0 0% 0 0%
From above table it shows that among 15 Patient in Group A, maximum of
10(66.66)% patient presented with Kroora kostha, 4(26.66%) patients were of
Madhya kostha, 1(6.66) was of Mridu kostha. In Group B maximum 8(53.33%)
patients presented with Madhya kosta, 6(40%) patients were of Kroora kostha &
1(6.66%) wass of Mridu kostha.
Distribution of patient according to Koshta
1 14
8106
0 005
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pa
tient
s
Mridu Madhya Kroora Sama
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
98

Results
Table no.21 Distribution of patient according to Position of work in patients.
Group A Group B Position of work
No. of Patient % No. of Patient %
Sitting 13 86.66% 13 86.66% Standing 12 80% 10 66.66% Stooping 2 13.33% 0 0% Squatting 0 0% 0 0%
From above table it shows that among 15 Patient in Group A, maximum of
13(86.66)% patient presented with sitting position, 12(80%) patients were
presentment with standing position, 2(13.33) was presentment with Stooping
position. In Group B maximum 13(86.66%) patients presented with Sitting
position, 10(66.66%) patients were presented with Standing position.
Distribution of patient according to Position of work in patients.
13 1312 102 00 0
05
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pa
tient
s
Sitting Standing Stooping Squatting
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
99

Results
Table no.22 Distribution of patient according to Habits in patients.
Group A Group B Types of Habits
No. of Patient % No. of Patient %
Smoking 5 33.33% 1 6.66% Tobacco 4 26.66% 2 13.33% Alcohol 0 0% 0 0%
None 9 60% 13 86.66%
From above table it shows that among 15 Patient in Group A, maximum of
9(60%) patient were not having any habits, 5(33.33%) patients were having of
Smoking habits, 4(26.66%) were having Tobacco eating habits. In Group B
maximum of 13(86.66%) patients were not having any habits, 2(13.33%) were
having Tobacco eating habits, & 1(6.66%) was having Smoking habits.
Distribution of patient according to Habits in patients.
51
4 20 0
913
05
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pa
tient
s
Smoking Tobacco Alcohol None
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
100

Results
Table no.23 Distribution of patient according to Prakriti of patients.
Group A Group B Prakriti
No. of Patient % No. of Patient %
Vatapitta 7 46.66% 7 46.66% Vatakapha 6 40% 6 40% Kaphapitta 2 13.33% 2 13.33%
From above table it shows that among 15 Patient in Group A & Group B,
maximum of 7(46.66)% patient were of Vatapitta prakriti, 6(40%) patients were
patient were of Vatakapha prakriti & 2(13.33%) patient were of Kaphapitta
prakriti.
Distribution of patient according to Prakriti of patients.
7 76 6
2 2
02468
No. of Patient No. of Patient
Group A Group BGroups
Num
ber o
f Pa
tient
s
Vatapitta Vatakapha Kaphapitta
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
101

Results
Table no. 24 Distribution of patient on the basis of age of the patient.
Group A Group B Age in years
No. of Patient % No. of Patient %
20 – 29 2 13.33% 2 13.33% 30 – 39 2 13.33% 4 26.66% 40 – 49 6 40% 4 26.66% 50 – 59 4 26.66% 3 20% 60 – 69 1 6.66% 2 13.33%
From above table it shows that among 15 Patient in Group A, maximum of
6(40%) patient were of 40 – 49years of age, 4(26.66%) patients were of 50 –59
years of age, 2(13.33%) were of 20 – 29years & 30 –39 years of age. In Group B
maximum of 4(26.66%) patient were of 40 – 49years & 30 – 39 years of age,
3(20%) patients were of 50 –59 years of age, 2(13.33%) were of 20 – 29years &
60 – 69 years of age.
Distribution of patient on the basis of age of the patient
2 224
644 3
1 2
02468
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pa
tient
s
20 – 29 30 – 39 40 – 49 50 – 59 60 – 69
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
102

Results
Table no.25 Distribution of patient according to Chronicity of the disease among groups.
Group A Group B Duration in months
No. of Patient % No. of Patient %
Up to 1 5 33.33% 5 33.33% 2 – 6 3 20% 5 33.33% 7 – 11 1 6.66% 0 0% 12 – 16 3 20% 3 20% 17 – 21 1 6.66% 1 6.66% 22 – 26 2 13.33% 0 0%
27 – 31 0 0% 0 0% 32 – 36 0 0% 1 6.66%
From above table it shows that among 15 Patient in Group A, maximum of
5(33.33%) patient were of acute i.e., Up to 1 month chronicity of the disease,
3(20%) patient were of 2 – 6 months & 12 - 16months of chronicity of the
disease, 2(13.33%) patient were of 22 –26 months of chronicity of the disease &
1(6.66%) patient were of 7 - 11 months & 17 – 21 months of chronicity of the
disease. In Group B, maximum of 5(33.33%) patient were of acute i.e., Up to 1
month & 2 – 6 months of chronicity of the disease, 3(20%) patient were of 12 -
16months of chronicity of the disease, & 1(6.66%) patient were of 17 - 21 months
& 32 – 36 months of chronicity of the disease.
Distribution of patient according to Chronicity of the disease among groups
5 53
5
10
3 31 1
200 00
1
0246
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber
of P
atie
nts
Up to 1 month 2 – 6 months7 – 11 months 12 – 16 months17 – 21 months 22 – 26 months
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
103

Results
Table no. 26 Showing the incidence of range of SLR in the patients.
Group A Group B SLR range in degrees
No. of Patient % No. of Patient %
Grade 0 0 0% 0 0% Grade 1 3 20% 0 0% Grade 2 4 26.66% 11 73.33% Grade 3 8 53.33% 4 26.66%
From above table it shows that among 15 Patient in Group A, maximum of
8(53.33%) patient were at grade 3, 4(26.66%) patients were grade 2, 3(20%) were
at grade 1. In Group B maximum of 11(73.33%) patients were at grade 2,
4(26.66%) were at grade 3.
Showing the incidence of range of SLR in the patients
0 03
04
118
4
05
1015
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pa
tient
s
Grade 0 Grade 1 Grade 2 Grade 3
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
104

Results
Table no.27 Change in the Lumbar movement in the patients of group A.
Forward flexion Rt. Lateral flexion Lt. Lateral flexion
Difference in cms
No. % No. % No. % 0 – 5 cms 11 73.33% 11 73.33% 13 86.66% 6 – 10 cms 4 26.66% 4 26.66% 2 13.33% 11 – 15 cms 0 0% 0 0% 0 0% 16 – 20 cms 0 0% 0 0% 0 0% 21 – 25 cms 0 0% 0 0% 0 0% 26 – 30 cms 0 0% 0 0% 0 0% 31 – 35 cms 0 0% 0 0% 0 0% 36 – 40 cms 0 0% 0 0% 0 0% 41 – 45 cms 0 0% 0 0% 0 0% 46 – 50 cms 0 0% 0 0% 0 0%
Forward flexion –
Among 15 patients of group A, 4(26.66%) of patients had increased in
forward flexion of 6 – 10 cms & 11(73.33%) of patient had increased in forward
flexion of 0 – 5 cms.
Right lateral flexion –
Among 15 patients of group A, 4(26.66%) of patients had increased in
Right lateral flexion of 6 – 10 cms & 11(73.33%) of patients had increased in
Right lateral flexion of 0 – 5 cms only.
Left lateral flexion –
Among 15 patients of group A, 13(86.66%) of patients had increased in
Left lateral flexion of 0 – 5 cms only & 2(13.33%) of patients had increased in
Left lateral flexion of 6 – 10 cms only.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
105
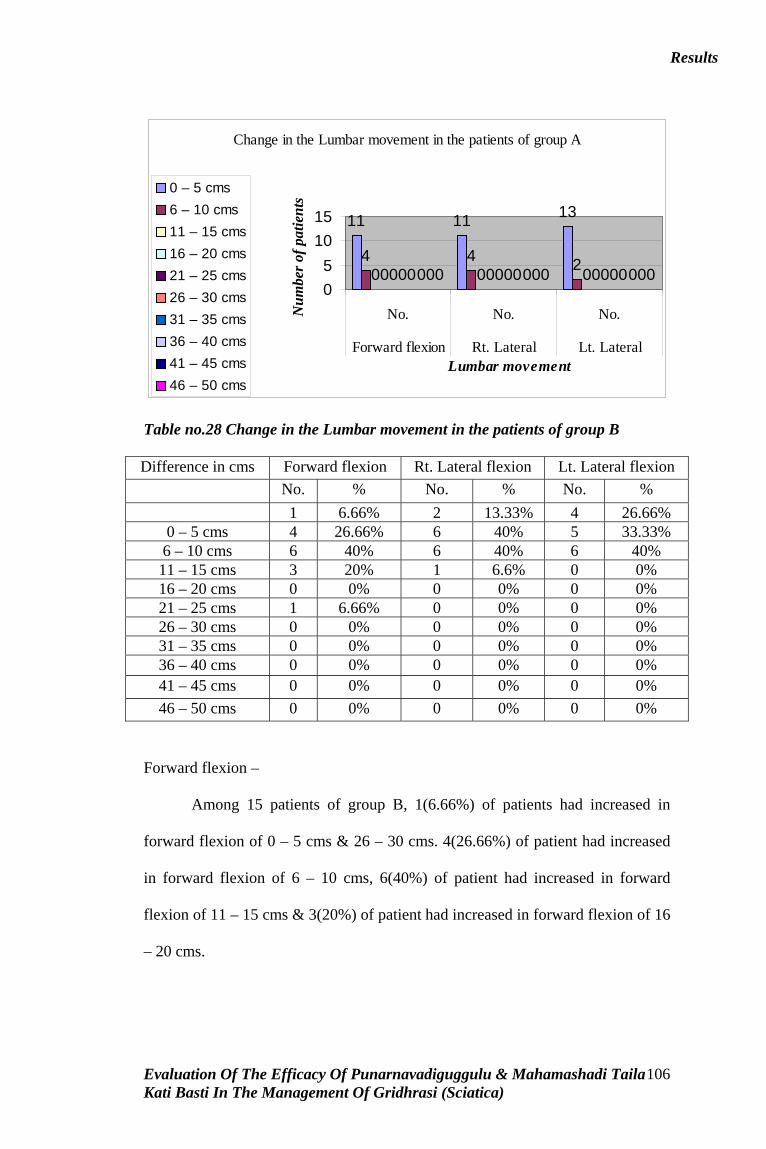
Results
Change in the Lumbar movement in the patients of group A
11 11 13
4 4 20 0 00 0 00 0 00 0 00 0 00 0 00 0 00 0 005
1015
No. No. No.
Forward flexion Rt. Lateral Lt. LateralLumbar movement
Num
ber o
f pat
ient
s
0 – 5 cms6 – 10 cms11 – 15 cms16 – 20 cms21 – 25 cms26 – 30 cms31 – 35 cms36 – 40 cms41 – 45 cms46 – 50 cms
Table no.28 Change in the Lumbar movement in the patients of group B Difference in cms Forward flexion Rt. Lateral flexion Lt. Lateral flexion
No. % No. % No. %
1 6.66% 2 13.33% 4 26.66% 0 – 5 cms 4 26.66% 6 40% 5 33.33% 6 – 10 cms 6 40% 6 40% 6 40% 11 – 15 cms 3 20% 1 6.6% 0 0% 16 – 20 cms 0 0% 0 0% 0 0% 21 – 25 cms 1 6.66% 0 0% 0 0% 26 – 30 cms 0 0% 0 0% 0 0% 31 – 35 cms 0 0% 0 0% 0 0% 36 – 40 cms 0 0% 0 0% 0 0% 41 – 45 cms 0 0% 0 0% 0 0%
46 – 50 cms 0 0% 0 0% 0 0%
Forward flexion –
Among 15 patients of group B, 1(6.66%) of patients had increased in
forward flexion of 0 – 5 cms & 26 – 30 cms. 4(26.66%) of patient had increased
in forward flexion of 6 – 10 cms, 6(40%) of patient had increased in forward
flexion of 11 – 15 cms & 3(20%) of patient had increased in forward flexion of 16
– 20 cms.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
106

Results
Right lateral flexion –
Among 15 patients of group B, 2(13.33%) of patients had increased in
Right lateral flexion of 0 – 5 cms & 6(40%) of patients had increased in Right
lateral flexion of 6 – 10 cms & 11 – 15cms & 1(6.66%) of patients had increased
in Right lateral flexion of 16 – 20 cms.
Left lateral flexion –
Among 15 patients of group B, 4(26.66%) of patients had increased in
Left lateral flexion of 0 – 5 cms, 5(33.33%) of patients had increased in Left
lateral flexion of 6 – 10 cms & 6(40%) of patients had increased in Left lateral
flexion of 11 – 15cms.
Change in the Lumbar movement in the patients of group B
1 244
6 56 6 6
31 00 0 01 0 00 0 00 0 00 0 00 0 0
02468
No. No. No.
Forward flexion Rt. Lateralflexion
Lt. Lateralflexion
Lumbar movement
Num
ber
of P
atie
nts 0 – 5 cms
6 – 10 cms11 – 15 cms16 – 20 cms21 – 25 cms26 – 30 cms31 – 35 cms36 – 40 cms41 – 45 cms46 – 50 cms
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
107

Results
Table no.29 Showing the incidence of Walking time in the patients.
Group A Group B Walking time in Grade
No. of Patient % No. of Patient %
Grade 0 2 13.33% 1 6.66% Grade 1 2 13.33% 4 26.66% Grade 2 8 53.33% 5 33.33% Grade 3 3 20% 5 33.33% Grade 4 0 0% 0 0%
From above table it shows that among 15 Patient in Group A, maximum of
8(53.33%) patient were at grade 2, 2(13.33%) patients were grade 1 & grade 0,
3(20%) were at grade 3. In Group B maximum of 5(33.33%) patient were at grade
2 & grade 3, 4(26.66%) patients were grade 1, 1(6.66%) were at grade 0.
Showing the incidence of Walking time in the patients
2 124
8
53
5
0 002468
10
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pat
ient
s
Grade 0Grade 1Grade 2Grade 3Grade 4
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
108

Table no. 30 MASTER CHART – SUBJECTIVE PARAMETER – GROUP- A
Ruk Sthambha Toda Spandana Ayama Gourava Suptata Shosha Vibhandha DahaSl. No
O.P.D B A B A B A B A B A B A B A B A B A B A
1 3827 3 2 0 0 2 2 - - - - + - + + - - - - - -2 3160 3 2 0 0 2 1 - - - - - - + - - - + - - -3 3967 4 2 0 0 0 0 - - - - - - + + - - - - - -4 4095 3 2 1 1 0 0 - - - - - - - - - - + - - -5 4090 2 1 0 0 2 1 - - - - - - + + - - - - - -6 4164 3 2 0 0 3 2 - - - - - - - - - - - - - -7 4238 3 2 2 2 0 0 - - - - - - - - - - + - - -8 4242 2 1 0 0 1 0 - - - - - - - - - - + - - -9 4508 2 1 1 0 0 0 - - - - + - - - - - + - - -10 4495 3 2 2 2 0 0 - - - - - - - - - - + - - -11 4646 4 3 0 0 2 1 - - - - - - - - - - + - - -12 4675 3 2 2 2 2 1 - - - - + - - - - - + - - -13 72 2 1 0 0 2 2 - - - - - - - - - - - - - -14 226 2 1 1 1 0 0 - - - - + - - - - - + - - -15 439 3 3 3 3 2 2 - - - - + - + + - - + - - -
109

Table no. 31 MASTER CHART – SUBJECTIVE PARAMETER – GROUP- B
Ruk Sthambha Toda Spandana Ayama Gourava Suptata Shosha Vibhandha DahaSl. No
O.P.D B A B A B A B A B A B A B A B A B A B A
1 3867 3 1 0 0 2 1 - - - - + - + - + + - - - -2 3972 4 2 2 2 2 1 - - - - + - + - + + + - - -3 4094 3 1 0 0 0 0 - - - - + - - - - - + - - -4 4181 3 1 2 0 2 1 - - - - + - + - - - + - - -5 4201 3 0 0 0 3 0 - - - - + - - - - - + - - -6 4664 3 1 2 0 2 0 - - - - + - + - - - + - - -7 4611 3 1 1 0 1 0 - - - - - - - - - - + - - -8 59 2 0 1 0 1 0 - - - - + - - - + + + - - -9 81 3 0 2 0 0 0 - - - - + - + - - - + - - -10 4728 4 1 3 0 0 0 - - - - + - - - - - + - - -11 669 3 0 2 0 0 0 - - - - + - - - - - - - - -12 962 3 0 3 1 0 0 - - - - + - + + - - - - - -13 1008 3 1 0 0 2 0 - - - - - - - - - - - - - -14 1030 3 1 2 1 1 0 - - - - + - - - - - + - - -15 1238 3 0 0 0 1 0 - - - - - - - - - - - - - -
110

Table no.32 MASTER CHART – OBJECTIVE PARAMETER – GROUP- A
S.L.R Movement of Lumbar spine Movement of Hip Walking time
Sl. No.
O.P.D Rt. Left 1 2 3 4 5 6 7 8 9a 9b 10a
10b
11
B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A1 3827 2 1 28 25 42 33 40 35 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 35 242 3160 3 2 30 26 42 36 40 36 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 40 203 3967 3 2 29 26 45 43 40 36 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 31 224 4095 3 2 30 20 41 38 45 40 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 25 205 4090 3 2 29 25 42 40 40 38 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 32 256 4164 3 3 28 23 45 38 39 33 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 46 407 4238 3 2 30 28 40 38 41 40 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 50 408 4242 1 0 15 8 40 36 41 38 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 20 209 4508 1 0 15 5 35 30 35 30 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 22 2010 4495 2 2 25 20 32 25 34 28 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 33 2611 4646 3 3 25 20 32 28 32 28 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 34 3012 4675 2 2 15 10 23 20 24 21 1 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 31 2513 72 2 1 40 37 41 39 40 38 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 33 2514 226 1 0 0 0 15 15 15 15 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 20 2015 439 3 3 45 40 48 46 45 43 1 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 42 38
1 – Forward flexion, 2 – Right Lateral flexion, 3 - Left Lateral flexion, 4 – Extension, 5 – Rotation, 6 – Flexion, 7 – Abduction, 8 – Adduction, 9 – Rotation in flexion: a) Internal rotation, b) External rotation, 10 – Rotation in Extension: a) Internal rotation, b) External rotation, 11 - Extension
111

Table no.33 MASTER CHART – OBJECTIVE PARAMETER – GROUP- B
S.L.R Movement of Lumbar spine Movement of Hip Walking time
Sl. No.
O.P.D
Rt Lt 1 2 3 4 5 6 7 8 9a 9b 10a
10b
11
B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A1 3867 2 1 15 5 35 25 36 27 1 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 41 302 3972 3 2 45 40 48 46 45 43 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 45 303 4094 2 0 8 0 20 15 20 15 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 20 154 4181 2 1 20 10 30 20 30 20 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 31 205 4201 2 0 25 10 30 15 31 17 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 41 286 4664 3 1 30 20 40 28 41 30 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 33 237 4611 3 1 25 10 30 20 30 21 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 25 158 59 2 0 25 12 33 25 30 24 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 28 209 81 3 1 32 15 40 28 39 25 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 35 2610 4728 2 0 30 15 40 28 41 36 1 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 42 2811 669 2 0 15 5 23 13 24 14 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 22 1612 962 2 1 32 13 40 28 39 24 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 41 2913 1008 2 0 28 10 37 27 41 30 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 31 1914 1030 2 0 20 7 38 25 34 29 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 23 1515 1238 2 1 36 9 38 20 34 19 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 35 20
1 – Forward flexion, 2 – Right Lateral flexion, 3 - Left Lateral flexion, 4 – Extension, 5 – Rotation, 6 – Flexion, 7 – Abduction, 8 – Adduction, 9 – Rotation in flexion: a) Internal rotation, b) External rotation, 10 – Rotation in Extension: a) Internal rotation, b) External rotation, 11 - Extension
112

Table no.34 Statistical Assessment of Individual Study Group – A (Objective Parameter)
Sl.No Parameters Mean S.D S.E t- value P - value RemarksS.L.R Right 0.5 0.577 0.149 3.355 <0.05 H.S 1
S.L.R Left 0.724 0.467 0.120 6.058 <0.001 H.S
2 Forward flexion
4.733 2.685 0.693 6.83 <0.001 H.S
3 Right Lateral flexion
3.866 2.477 0.638 6.059 <0.001 H.S
4 Left Lateral flexion
3.4666 1.807 0.466 7.437 <0.001 H.S
5 Extension 0.666 0.487 0.125 5.328 <0.001 H.S 6 Rotation 0.1333 0.351 0.090 1.481 >0.05 N.S 7 Walking
time 6.6 4.95 1.279 5.16 <0.001 H.S
Table no.35 Statistical Assessment of Individual Study Group – B (Objective Parameter)
Sl.No Parameters Mean S.D S.E t- value P - value Remarks S.L.R Right 1.666 0.516 0.133 12.52 <0.001 H.S 1
S.L.R Left 1.666 0.5 0.129 12.29 <0.001 H.S
2 Forward flexion
13.666 5.367 1.385 9.867 <0.001 H.S
3 Right Lateral flexion
10.6 3.794 0.979 10.827 <0.001 H.S
4 Left Lateral flexion
9.266 4.078 1.053 8.8 <0.001 H.S
5 Extension 0.533 0516 0.133 4.00 <0.01 H.S 6 Rotation 0.133 0.351 0.090 1.47 >0.05 N.S 7 Walking time 6.6 4.95 1.279 5.16 <0.001 H.S
Table no.36 Statistical Assessment of Individual Study Group – A (Objective Parameter)
Sl.No Parameters Mean S.D S.E t- value P - value Remarks1 V.A.S 1.6 0.828 0.213 7.511 <0.001 H.S
Table no. 37 Statistical Assessment of Individual Study Group – B (Objective Parameter)
Sl.No Parameters Mean S.D S.E t- value P - value Remarks1 V.A.S 3.933 0.961 0.248 15.858 <0.001 H.S
113

Table no 38 Statistical Assessment of Comparative study of Group – A with Group – B, After Treatment. (Objective Parameter)
Sl.No Parameters Group Mean S.D S.E P.S.E t- value P - value
Remarks
A 2.0 1.414 0.365 S.L.R Right B 0.5 0.547 0.141
0.391 1.278 >0.05 N.S
A 1.545 0.934 0.241
1
S.L.R Left
B 0.666 0.707 0.182
0.302 2.91 <0.02 H.S
A 20.866 11.15 2.879 2 Forward flexion
B 12.066 9.098 2.349
3.716 2.368 <0.02 H.S
A 33.666 8.582 2.216 3 Right Lateral flexion B 24.2 7.97 2.059
3.024 3.13 <0.01 H.S
A 33.266 1.977 1.977 4 Left Lateral flexion B 24.93 2.045 2.045
2.844 2.931 <0.01 H.S
A - - - 5 Extension
B 0.0666 0.258 0.0666
0.0666 1.000 >0.05 N.S
A - - - 6 Rotation B 0.0666 0.258 0.0666
0.0666 1.000 >0.05 N.S
A 26.33 7.333 1.894 7 Walking time
B 22.26 5.787 1.494
2.412 1.687 >0.05 N.S
Table no 39 Statistical Assessment of Comparative study of Group – A with Group – B, After Treatment. (Objective Parameter)
Sl.No Parameters Group Mean S.D S.E P.S.E t- value P - value
Remarks
A 3.733 2.016 0.52 1 V.A.S
B 2.2 1.32 0.341
0.624 2.46 <0.05 H.S
114

Table no 40 Statistical Assessment of Individual Study Group – A (Subjective Parameter)
Sl.No Parameters Mean S.D S.E t- value P - value
Remarks
1 Ruk 1.0 0.377 0.097 10.309 <0.001 H.S
2 Sthamba 0.0666 0.258 0.066 1.000 >0.05 N. S
3 Toda 0.4 0.507 0.1309 3.055 <0.01 H.S
Table no 41 Statistical Assessment of Individual Study Group – B (Subjective Parameter)
Sl.No Parameters Mean S.D S.E t- value P - value
Remarks
1 Ruk 2.4 0.507 0.130 18.461 <0.001 H.S
2 Sthamba 1.0 1.0 0.258 3.875 <0.01 H.S
3 Toda 0.933 0.883 0.228 4.093 <0.01 H.S
Table no 42 Statistical Assessment of Comparative study of Group – A with Group – B, After Treatment. (Subjective Parameter)
Sl.No
Parameters Group Mean S.D S.E P.S.E t- value
P - value
Remarks
A 1.733 0.593 0.153 1 Ruk
B 0.666 0.617 0.159
0.22 4.806 <0.001 H.S
A 0.733 1.032 0.266 2 Sthamba
B 0.266 0.593 0.153
0.306 1.526 >0.05 N.S
A 0.8 0.861 0.222 3 Toda
B 0.2 0.414 0.106
0.246 2.439 <0.05 H.S
Table
To compare the mean effect of 2 groups, the analysis is done by using un
paired t – test by assuming that the mean effect of 2 groups is same after the
treatment. From the analysis the objective parameter forward flexion, right lateral
flexion, left lateral flexion & VAS shows highly significant & other parameter
shows non – significant. In the parameter SLR, right leg which shows not
significant the analysis done by using 4 patients in group A & 6 patients in group
115

B, those have symptoms. In SLR of left leg the analysis done for 11 patients in
group A and 9 patients in group B those have the symptoms of the parameter
which shows highly significant. By comparing p value & t value. (Table III)
In the subjective parameters, the Ruk and Toda shows highly significant,
but Sthamba shows non significant.
To know the effect of drug individually the analysis done by using paired t
test by assuming that drug is not responsible for changes in the observation before
& after the treatment. Over all the group B shows more highly significant in all
the objective parameter except extension, where as the Rotation shows not
significant in both the groups. The parameter VAS shows more highly significant
in group B with more mean & more variation.
In subjective parameters in group B shows highly significant but in the
parameter Sthambha is not significant in group A. There is a much highly
significant in parameter Ruk, Toda & Sthamba in group B with more mean &
more variation. By comparing p value, t value, mean & standard deviation. (From
table I & II)
Individual Parameter
Objective parameter –
In group B the parameter SLR right & left shows more net mean effect
with less variation.
In group B the parameter Forward flexion shows more net mean effect
with more variation.
The parameter right lateral flexion in group B is having more net mean
effect with more variation.
The parameter left lateral flexion in group B is having more net mean
effect with more variation.
116

The parameter extension in group B is shows less net mean effect with
less variation.
The parameter rotation in both groups is shows same net mean effect with
same variation.
In the parameter, walking time in both groups shows same net mean effect
with same variation.
In group B the parameter, VAS shows more net mean effect with more
variation.
Subjective parameter –
The parameter Ruk in group B shows more net mean effect with more
variation.
The parameter Sthambha in group B shows more net mean effect with
more variation.
The parameter Toda in group B shows more net mean effect with more
variation.
117

Table no 43 Showing the Overall assessment
Group A Group B Response
No. of Patient % No. of Patient %
Good relief 0 0% 0 0% Marked response
0 0% 10 66.66%
Moderate response
3 20% 5 33.33%
Mild response 12 80% 0 0% Not relief 0 0% 0 0%
The above table shows the assessment of result among groups. In group A,
12(80%) patient have got mild response, 3(20%) patient have got moderate
response. In group B, 10(66.66%) patients have got marked response &
5(33.33%) patient have got moderately relieved.
Showing the over all assessment
0 00
10
35
12
00 00
5
10
15
No. of Patient No. of Patient
Group A Group B
Groups
Num
ber o
f Pat
ient
s
Good Marked Moderate Mild Not relief
118

Discussion
Discussion
Main intention of any research is to re-examine the established facts in modern
light, clarify the doubts and filling in the lacunas. The study process starts with forming
of the hypothesis, detailed planning of research, at prefinal stage clubbing the
observations and results on which certain conclusions can be drawn. This section titled
‘discussion’ analyzes and contemplates the observations made during project and results
obtained post therapeutically on the selected problem, Gridhrasi.
In human body, the lumber spine is the site of most expensive orthopedic problem
for the world’s industrialized countries. It is the seat of miracles. The central nervous
system as well as autonomic nervous system work through the spine and the entire
nervous system dependant upon the spine. So the diseases affecting lumber spine are
handled very carefully. Gridhrasi is such a disease having its origin in Pakvashaya and
seat in Sphika and Kati i.e. lumber spine. In classics, Gridhrasi is included under 80 types
of Nanatmaja Vata Vikara under the heading of Vatavyadhi as a separate clinical entity
There is no need to state that modern medical treatment has its own limitation in
managing this type of disease. Modern medical treatment either conservative or surgical
and is highly symptomatic and with troublesome side effects. This suggests special need
of an ayurvedic management for this type of conditions.
As the number of patients suffering from this disease are increasing day by day.
Ayurvedic physician should also make effort continuously to find out effective remedy
for the patients of Gridhrasi from Ayurvedic classics.
Gridhrasi is one of the Nanatmaja Vatavyadhi and occasionally Kapha is also
associated with the Vata Dosha and produce Vata-kaphaja type of Gridhrasi. So, the
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
119

Discussion
drugs having Vatahara, Shulahara and Srotoshodhaka properties may be very useful in
the treatment of Gridhrasi.
Discussion part is divided into four sections.
1. Discussion on Gridhrasi and Sciatica.
2. Discussion on Clinical study & Observation.
3. Discussion on probable mode of action of Punarnavadi guggulu in Gridhrasi
4. Discussion on probable mode of action of Mahamasaditaila kati basti in Gridhrasi
Discussion on Gridhrasi and Sciatica.
Gridrasi is one of the Nannatmaja vyadhi of vata vyadhi. The pain starts from
Spik, and radiates to down to leg, which is a classical condition in Gradrasi & even
Sciatica.
Sciatica, a clinical entity that is described in modern science, has a striking
resemblance to the symptomatology of Gridrasi. It can be better compared through a
discussion made from the shareera (Anatomy) to the Roopa(clinical presentation) of the
diseases.
On a closer look into the shareera, the parts, which are affected in the Gridhrasi
disease, are Spik, kati prishta pradesa, kandaras of parshni and angulis, kukundara
marma, katikatharunamarma and the Gridhrasi snayu / nadi. While discussing the modern
aspect, the anatomical structures, which are affected in Gridhrasi disease, are lumbar
vertebrae, intervertebral joints, lumbo-sacral plexus and sciatic nerve.
A better comparision can be made from the review of Nidana, The
swaprakopakara nidanas, marmaghatakara nidans and margavarodhaka nidanas
eventually leads to dhatukshaya and there by producing vataja type of Gridhrasi in the
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
120
Discussion
body. Another type is the vatakaphaja Gridhrasi where the margavarodha janya nidana
bhavas can be considered because the presenting complaints include tandra, gourava, and
aruchi along with Gridhrasi shoola. Taking the kaphavrita vata symptoms into
considerations, both the condition go in parallel confirming the margavarodha.
Considering the etiological factors for the sciatica we can find the similar types of factors
responsible for the condition. Avitaminosis, nutritional deficiencies leading to calcium
deficiency were observed to lead inflammation of sciatic nerve resulting to sciatica by
modern scientists. Intake of excessive and heavy fatty meals was observed to lead to
accelerate degenerative process and can be considered as kapha provocation diet. The
posture at work of sitting, stooping, squatting, standing etc are considered as the cause for
sciatica. The psychological factors anxiety, tension, fear etc leads to prolonged
contraction of back muscles. So all these factors can be considered as the swprakopakara
nidana factors of Ayurveda. Trauma is observed to be the single most important causative
factor for disc prolapse. Trauma / abhighata to the marmas are to be interpreted here.
Almost all the patients of Gridhrasi have a history of trauma. Here the term to be
considered much is the abhighata i.e. the acute injuries, fall from the height, heavy
manual works, heavy blow on the low back etc further leads to degenerative changes in
the particular area. Even this can also trigger the condition in degenerated vertebrae also.
The degenerative changes can be correlated with the dhatukshaya features. For this
degeneration to happen all other causative factors are the reason. The lumbar spondylosis,
where marked degeneration of the vertebrae happen, can be considered, which inturn
leads to the disc prolapse causing sciatica.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
121

Discussion
In the samprapthi review, two opinions can be put forward as- Gridhrasi dhamani
and Gridhrasi snayu / nadi. Commenting on to the context Dalhana has considered it as
kandara and termed as Mahasnayu. He has also used the term kandaradwayam indicating
the sciatic nerve of both legs. The mahasnayu starts from gulpha to vitapa. In Vriddha
Vagbhata’s Astanga sangraha, Gridhrasi occurs due to vata sited at snayu. So basing on
these commentaries, the concept of Gridhrasi dhamani can be rejected and the Gridhrasi
snayu / nadi is the apropriate term for the sciatic nerve that also starts from the gulpha to
vitapa on both legs.
Dhamanis are having the property of dhmana (pulse vibrations) as each spurt of
fluid impinges on the wall of arteries and so dhamani is considered as a part of the
circulatory system. Snayus are the nadis that conduct vayu as per vaidyasabdasindhu. It is
also noted that snayu binds the dehamamsa (muscles), asthi (bones), medas (fat tissue)
and strengthens the joint. So by conducting the vayu through out the body, snayu helps in
prasarana, akunchana etc. So here by we can assume that the snayu is more connected to
the musculo-skeletal system and so the sciatic nerve can be considered as Gridhrasi nadi /
snayu.
Vitiated vata especially apana and vyana vayu are involved in the samprapti of
Gridhrasi. Kapha may be the anubandhi dosha. The samprati takes place either by
dhatukshaya or margavarana or due to agantunja causes like abhighata. In dhatukshayaja
samprapti, due to improper nourishment of rasadi dhatus, these dhatu land into kshaya
avastha. Dhatukshaya further vitiates vata causing Gridhrasi. This type of samprapti can
be correlated to the Sciatica caused by degenerative changes. These changes are
osteoporosis, spondylosis etc. which lead to Sciatica.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
122

Discussion
When vayu is obstructed by kapha, ama etc. it gets vitiated leading to
margavaranajanya samprapti of Gridhrasi. Agantuja factors are mentioned as a cause of
Gridhrasi by both the systems of medicine.
Considering the roopa, the similarities in both Gridhrasi and sciatica can be found.
Both have the same singular presentations - pain along the course of leg. The pain over
the spik, kati, prishta etc and can be considered as low backache. When the pain extends
to uru, janu, jangha pada and angulees the roopavastha happens. The same way the
typical sciatic nerve pain is radiating type, where the low backache turns to a radiating
one through the course of sciatic nerve as the prolapsed disc compresses the nerve root.
On the later stages the dehavakratha (scoliosis) and the abnormal sensations like toda,
spandana, ayama etc happens. Further it leads to the impairment in uplifting of the leg
and loss of sensations, which can be termed as sakthi utkshepana nigrahana and suptatha
in turn leads to neurological deficit. This is a clinical sign for the diagnosis of Sciatica
known as SLR in modern science. It also has prognostic value. Regarding the gait of the
patient it will be of limping nature in sciatica, which can be considered as gridhramaiva
syati.
Snehana, Svedana and Mrdu Sodhana are the line of treatment in all
Vaatavyaadhees. Even though, Snaayu and Rakta are involved as Dooshya, Agnikarma
and Siraavyadha are also the chief lines of treatment. These therapeutic measures
disintegrate the union of Dosha and Dooshya. From the Samana point of view, any
medication which soothe the magnitude of pain, improves the functional ability along
with Sampraapti Vighatana is best in patients of Gridhrasi. An added advantage will be
achieved if it can re-establish the Dhaatu equilibrium along with Vaataanulomana.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
123
Discussion
Considering all these aspects, Punarnavadi gugglu having all these therapeutic effects had
been taken for this study.
Discussion on Clinical study & Observation
The patients were selected incidentally from exclusively conducted medical
camps in the premise of Shri .D. G. Melamalagi Ayurvedic Medical College and Hospital
Gadag. Both the types of Gridhrasi were taken. Patients of both sexes were selected for
the clinical study between the age group 18 to 65 years.
In total 30 patients were selected for the study. Two groups were divided of 15
patients for each group, i.e., Group A of 15 patients were treated by Punarnavadi guggulu
orally for 1 month & Group B of 15 patients were treated by Kati basti with Mahamasadi
taila for 14 days. All the patients were subjected to thorough clinical, laboratory and
radiological examinations. There is no drop out in the study and all the 30 patients were
appeared for the assessment of results. The laboratory tests like total blood count,
differential count and ESR were carried out to exclude infections, disorders like
tuberculosis of spine, the RBS was carried out to rule out diabetes, Hb% was carried out
to rule out anemia. The radiology of LS spine is also a diagnostic criteria to exclude the
conditions like severe osteoporosis, fractures, osteophytes etc. But in the present study,
among all the 30 patients, not a single patient has shown the above exclusion conditions.
The straight leg-raising test is a good objective parameter to diagnose the Gridhrasi
disease in western medicine. The authorities of Ayurveda mentioned that kshepana and
utkshepana are the salient features of Gridhrasi disease. The other objective parameters
taken were movements of lumbar spine and walking time. The Hip movement is also one
of the parameter taken to rule out any ristriction of Hip due Hip arthritis.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
124

Discussion
Assessments of response were done both subjectively and objectively. After
recording the baseline data and post treatment data of the factors, ruk, sthamba, & toda in
grading as the subjective parameters and the factors such as straight leg raising test in
degrees, the movements of the spine viz, forward flexion, right and left lateral flexions in
centimeters and walking time in second as the objective parameters, the assessments were
done. The statistical analyses of the subjective and objective parameters were made on
these assessments.
As Gridhrasi is a shoola pradhana vatavyadhi, eventhough the other subjective
parameters are taken for assessment, the effect was more concentrated on ruk (pain).
Among 15 patients of Group A, 53.33% of patients were at grade 3, 13.33% of patients
were at grade 4, 33.33% of patients were at grade 2. After treatment 53.33% patients
were at grade 2, 33.33% patients were at Grade 1 & 13.33% patients were at grade 3.
In 15 patients of Group B, 80% of patients were at grade 3, 13.33% patients were at grade
4, 6.66% patient was at grade 2. After treatment 53.33% patients were at grade !, 40%
patients were at grade 0, i.e., completely the pain was reduced. 6.66% patient was at
grade2. This shows that there was marked variation in the grades of pain in the patients of
both groups. But there was very good response in group B than group A. So in the
statistical analysis the parameters pain showed highly significant with t – value 10.309 in
group A & 18.461 in group B, the corresponding P value < 0.001in both the groups.
The parameter Sthambha shows not significant with t – value 1.00, the corresponding P
value > 0.05 in group A & in group B Sthambha shows highly significant with t value
3.875 & corresponding P value < 0.01.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
125

Discussion
The parameter Toda shows highly significant in both groups with t – value 3.055 in
group A, 4.093 in group B & the corresponding P value < 0.01. Among Ruk, Sthamba &
Toda, in group A Ruk & Toda are significant & Sthamba is not significant. In group B
Ruk is highly significant than Sthamba & Toda.
In group A 5 patients & in group B 12 patients were with symptom Gourava,
which was relived completely. In group A & group B 10 patients were with Vibhanda ,
all were relived completely after treatment. In both groups , Suptata was relieved very
minutely but Shosha was not responded.
Considering the response in some of the individual categories in the duration,
33.33% patients were of acute onset (up to 1month) in both groups. 20% patients were of
group A & 33.33% patients were of group B were of 2 – 6 months of duration.
Regarding the Objective Parameters
In 15 patients of group A, 53.33% of patients were at grade 3, 26.66% of patients
were at grade 2, 20% of patients were at grade 1. after treatment 46.66% of patients were
at grade 2, 20% patients were at grade 3, 13.33% patients were at grade 1, 20% of
patients were at grade 0. In this group 4 patients were affected with right leg & 11
patients were affected with left leg.
In 15 patients of group B, 73% patients were at grade 2, 26.66% of patients were
at grade 3. after treatment 46.66% of patients were at grade 0, 46.66% were at grade 1 &
1 patient was at grade 2. in this group 6 patients were affected with right leg & 9 patients
were affected with left leg.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
126
Discussion
Seeing the statistical analysis, in both group it was highly significant P value <
0.05 in right leg affecting & P value < 0.001 in left leg. But the observation shows group
B is highly significant than group A.
In the parameter Lumbar movement –
In Forward flexion, among 15 patients of Grade A, 26.66% of patients had increased to 6
– 10 cms in flexion, 73.33% of patients increased to 0 – 5 cms only. In group B, 40% of
patients were increased to 11 – 15 cms, 26.66% of patients were increased to 6 – 10 cms,
20% of patients increased to 16 – 20 cms,6.66% of patient increased to 0 – 5 cms & 26 –
30 cms improved. This shows that there was improvement in the forward flexion in both
groups . but there was very good response in group B than group A. In the statistical
analysis the parameter showed highly significant with t value 6.83 in group A & 9.867 in
group B, the corresponding p value < 0.001 in both groups.
In right lateral flexion, in 15 patients of group A, 26.66% patients increased in flexion of
6 – 10 cms & 73.33% patients increased in movement of 0 – 5 cms. In group B, 13.33%
of patients increased in movement of 0 – 5 cms, 40% of patients increased to 6 – 10 cms
& 11 – 15 cms & 6.66% of patient’s increased to 16 -20 cms.
In left lateral flexion, among 15 patients of group A, 86.66% of patients increased of 0 –
5 cms & 13.33% of patients were increased to 6 – 10 cms. In group B, 26.66% of patients
were increased to 0 – 5 cms, 3.66% of patient increased to 6 – 10 cms & 40% of patients
increased to 11 – 15 cms in flexion.
Walking time –
In goup A of 15 patients, 53.33% patients were at grade 2, 13.33% of patients
were at grade 0 & grade 1& 20% of patients were at grade 3. after treatment 46.66% of
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
127

Discussion
patients were at grade 1, 33.33% of patients were at grade 0 & 20% of patients were at
grade 3. In group B of 15 patients 33.33% patients were at grade3 & grade 2, 26.66% of
patients were at grade 1 & 6.66% of patient was at grade 0. After treatment 53.33% of
patients were at grade 0 & 46.66% of patients were at grade 1. This shows that there was
a good variation in the grading of walking time in the patients of both groups. But there
was good response in group B then group A. In the statistical analysis the parameter
walking time showed highly significant with t value 5.16 in group A & group B, the
corresponding p value < 0.001 in the both groups.
In the overall assessment among 30 patients, 8 patients showed moderately
response, 10 patients showed marked response & 12 patients showed mild response. But
seeing the assessment of individual groups, in group A 12 patients showed mild response
& 3 patients showed moderately response, in group B 10 patients showed marked
response & 5 patients showed moderately response.
This shows that group B(Mahamasadi taila katibasti) has highly significant the
group A(Punarnavadi guggulu orally).
The statistical evaluation showed all parameters in Subjective & Objective has
shown highly significant except the parameter Sthmba in group A, Rotation in lumbar
movement in group A & group B.
Discussion on probable mode of action of Punarnavadi guggulu in Gridhrasi
The materials in the nature including the human body as well as drugs are
composed of panchamahabutha. In drug compositions of these mahabuthas are known by
inferred on the basis of their properties like Rasa, Guna, Viryaa, Vipaka, Prabhava etc,
which are inherent in drug on which the pharmacodyanmic depends.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
128
Discussion
Punarnavadi Guggulu described by Acharya Vangasena in Vatarakthaadikara
Adyyaya has been selected for the Shamana in the study. Punarnavadi Guggulu contains
mainly Punaranava, Erandamoola, Sunthi, Guggulu, Eranda taila, Makshika dathu etc,
which possesses Vata-kaphahara, Anulomaka & Shoolahara property as well as anti-
inflammatory, analgesic, muscle relaxant properties & even regenerative properties
which give relief from the disease.
Discussion on probable mode of action of Mahamasaditaila kati basti in Gridhrasi
Mahamasadi taila described by Acharya Vangasena in Vatavyadhadhikara
Adyyaya has been selected for the Kati Basti. Mahamasadi taila contains mainly Masha,
Trikatu, Tila taila, Eranda, Dugda, Chagamamsa, Dasamula, Gokshura, Amalaki etc
drugs which possesses Vata-kaphahara property.
Snehana, Swedana and Mrdu Sodhana are the Principles of treatment in all
Vaatavyadhi. Even though Snaayu and Rakta are involved as Dooshya, Agnikarma and
Siravyadha are also the chief lines of treatment. Mrdu Sodhana in the form of Basti or
mrudu Virechana plays the major treatment of Gridhrasi. From the Samana point of view,
various medication which soothe the severity of pain, improves functional ability is best
in Gridhrasi. An added advantage will be achieved if Snehana and Swedana are done
which relieves Stambha, Gaurava, Seeta and which reduces the intensity of pain.
Considering this aspect Katibasti is adopted for this study.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
129

Conclusion
Conclusion
At the end of the study, following conclusions can be drawn on the basis of observations
made, results achieved and thorough discussions in the present context.
• Historical glimpses reveal that though the knowledge of Sciatica is just two
centuries old for the modern medicine, Ayurveda has concise but exact
description of the disease in the samhitas. The anatomical, pathological, clinical
and even diagnostic aspects of the disease are well covered in our texts.
• Our classics have described vata dosha as the main culprit in the disease
Gridhrasi. Sometimes kapha is the anubandhi dosha. This is supported clinically
as maximum no. of the patients showed vataprakopaka hetus as the cause.
Physical as well as mental stress was observed as the common causes along with
trauma.
• There is no direct reference regarding Nidana and Samprapti of Gridhrasi.
• Gridhrasi can be equated with Sciatica in modern medicine.
• Majority of the patients had dwandwaj prakruti i.e. vatapitta or vatakapha. Also
majority of patients had vishamagni and krura koshtha. All these finding support
the dominance of vata dosha.
• In the present study, majority of the patients suffered from vatakaphaj Gridhrasi
(53.33%) with 46.66% suffering from vataj Gridhrasi.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
130
Conclusion
• In the present study both the therapies were effective in combating the disease.
Major improvement was observed on all signs and symptoms as well as on SLR
in both the groups.
• On comparing the overall effect of the therapies, Kati basti showed more effective
than only Shaman Therapy. This proves the importance of kati basti therapy in the
management of Gridrasi.
• The drugs administered in Guggulu form gave overwhelming response in treating
Gridhrasi. Only shaman therapy cured 3 patients were moderately responded and
12 patients showed Mild improvement. This proves the efficacy of Guggulu
kalpana in mitigating vata and kapha and also potentiating agni.
• Another reason behind the effectiveness of the therapy might be that the
combination was with erand taila. Erand taila effectively conquers vata and kapha
dosha. It clears the srotasas by removing mala and avarana. It conquers the
rukshata of vayu with snigdha guna and also normalizes apana vayu, which is the
main culprit.
• No major adverse or side effects were encountered during this treatment period.
• Preventive aspect and patient’s education play an important role in the
management of Gridhrasi. Proper guidelines about posture etc along with
exercises strengthening the spine are helpful for effective management.
• Allopathic management is far away from the perfect treatment.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
131

Conclusion
Suggestions for future study
Study is better to be conducted on a large sample
Shodana followed by Katibasti.
Katibasti followed by samana yoga.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
132

Summary
Summary
In spite of the spine’s excellent form and function, back pain is a national,
personal and clinical problem: national because it is experienced by most of the
population at some time and is a drain on the nation’s resources, personal because it can
remain a major unresolved dilemma, and clinical because not only is diagnosis difficult,
but methods of treatment are conflicting and often unrewarding. Sciatica is one of the
many conditions causing back pain and pain in the lower limb. This condition causes
great discomfort to the patient and affects his daily routine as it is directly related to the
locomotor system.
It would be a great achievement, if we are able to treat such an agonizing
condition with principles laid by our ancient acharyas. Keeping this view in mind, the
project titled ‘Evaluation of the Efficacy of Punarnavadiguggulu & Mahamashadi Taila
Kati Basti in the Management of Gridhrasi (Sciatica)’ was undertaken.
The present study entitled’ consists of 7 parts.
1. Introduction
2. Objectives
3. Review of literature
4. Methodology
5. Results
6. Discussion
7. Conclusion
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
133

Summary
The introduction consists of the general description of Ayurveda, the incidence of the
disease Gridrasi, brief description of Gridrasi disease with its treatment.
The objectives consist of the need for the study and objectives of the study and
studies conducted on the related topic in the past and recent times.
Review of literature consists of the historical review, vyutpatti and nirukthi of
Gridhrasi. The shareera part deals with both anatomy and physiology related to the
disease Gridhrasi. In the karma review, the procedure, indications and contraindications
etc of kati basti, the drugs used and the probable mode of action of basti are discussed. In
the disease review, nidana, samprapthi, poorvaroopa, roopa, vyavachedaka nidana etc are
elaborated.
Methodology part deals with the preparation of the patients for performing kati basti
& even the method of preparation of the selected medicine Punarnavadi guggulu taken
orally & even the preparation of the Mahamasadi taila for kati basti as said in classic even
it properties are also mentioned. The study design was done on the basis of subjective and
objective parameters with their grading and tests to assess the parameters are explained.
The observations and results are dealt in the result section. The demographic data,
response to treatment and overall response are also dealt. Results are given in the form of
tables along with a short description. The improvements in selected parameters are
statistically analyzed and presented in the form of tables and graphs.
Discussion part is divided into four sections. First section entitled – discussion on
Gridhrasi and Sciatica – deals with the correlation between Gridhrasi and Sciatica
through the anatomical aspect to the roopavastha. The second section discuss about the
Clinical study & Observation. Discussion on clinical study deals with the analysis of
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
134

Summary
clinical response to the treatment with logical interpretation. The third section deals with
the Discussion on probable mode of action of Punarnavadi guggulu in Gridhrasi and
lastly the fourth section deals the probable mode of action of Mahamasaditaila kati basti
in Gridhrasi. Lastly the Conclusion is given on the present study.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica)
135

Bibliography
Bibliography – References
1. Agnivesa, Charakasamhita Vimanasthana, edited by Vaidya Jadavaji Trikamji Acharya, chapter 8 – 18th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 265.
2. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 101th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 621.
3. Susruta, Susrutasamhita Sareerasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 8 – 17th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 381.
4. Vagbatha, Asthangahrudaya Sutrasthana, edited by Achrya Baladeva
Upadyaya, chapter 27 – 15th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 328.
5. Pt. Kashinathshastri and Dr. Goraknath Chathurvedi. Edited, Charaka
Samhita Sutra Sthana, Chapter20, Shloka11, Vidyotini Hindi Commentory 10th Edition Varanasi ; Chaukhambha Samsthana (kasi Sanskrit series ; 1982). Page No 399.
6. By; Peter F Ullrich,jr, MD spine.health.com September 8,1999 (up
dated February28,2001) Assessed on 4th June 2006.
7. Cristopher Haslett, Edwin R Chilvers, Nicholas A Boon, Nicki R Colledge, edited Davidson’s Principles & Practice of Medicine Chapter 20, 19th edition 2002. Church hill Living stone, Edinburge London, New york, Philadelphia, St Louis Sydeny Toronto 2002, Page No. 981.
8. Sir Charles Illingwoth A text book of surgical pathology Nervous system
12th edition, English language book society, London 1975 Page No 140-141.
9. Dr. Pate At, Ogle, Dr AA Low back pain:-Diagnosis and management of
low Back pain, University of Kansas medical center, available from; www.spine.health.com. Assessed on 6th June 2006.
10. Atravaveda Samhitha, edited by Vedamurthy Taponistam Sri
Mansharma achrya Delhi, Parimala publication, 19/60/2, page no. 56.
11. Maharsi Vedavyasa, Garudapurana, edited by Dr. Ramashankar Bhattacharya, chapter 166 – 51st sloka. . Varanasi: Chaukhambha Sanskrit Sansthan; 1998 page no. 199.
12. Maharshi Vedavyasa’s, Agnipurana, edited by Achrya Baladeva
Upadyaya, chapter 285 – 51st sloka Varanasi Chaukhamba Sanskrit Samsthan, 1998 page no. 115
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
136

Bibliography
13. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya Jadavaji Trikamji Acharya, chapter 5 – 92th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 43.
14. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 14 – 22th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 89.
15. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 19 – 3th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 110.
16. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 56th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 619.
17. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 101th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 621.
18. Susruta, Susrutasamhita Nidanasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 1 – 74th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 268.
19. Susruta, Susrutasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 5 – 23rd sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 428.
20. Susruta, Susrutasamhita Sareerasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 8 – 7th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 381.
21. Bhela, Bhelasamhita Chikitsasthana, edited by Prof. Priyavrat Sharma,
chapter 24/44-45th sloka. Varanasi: Chaukhambha Visva Bharti; 2005 page no, 454.
22. Vrddha Jivaka, Kasyapasamhita Sutrasthana, edited by Pandit
Hemaraja Sharma, chapter 27- 21st sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 1976 page no. 41.
23. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 20 – 13th sloka. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 383.
24. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 36 – 9th sloka. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 609.
25. Vrddha Vagbhata, Astangasamgraha Nidanasthana, edited by
K.R.Srikantha Murthy, chapter 15 – 56th sloka. Varanasi: Chaukhambha Orientalia; 1996 page no. 535.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
137

Bibliography
26. Vagbatha, Asthangahrudaya Sutrasthana, edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 27 – 15th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 328.
27. Vagbatha, Asthangahrudaya Nidanasthana, edited by Bhisagacharya
Harisastri paradakara Vaidya, chapter 15 – 54th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 535.
28. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 22 – 54th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
29. Chakrapanidatta, Chakradatta, edited by P.V.Sharma, vatavyadi adyaya
53rd sloka. Varanasi: Chaukhambha Publishers; 1998. p. 189.
30. Agnivesa, Charakasamhita Chikitsasthana Chakrapanidatta commentary, edited by Vaidya Jadavaji Trikamji Acharya, chapter 28 – 101th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 621.
31. Agnivesa, Charakasamhita Chikitsasthana Gangadara commentary,
edited by Kaviraj Naredranath Sengupta & Kaviraj Balachandra Sengupta, chapter 28 – 30th sloka.Varanasi: Chaukhambha Orientalia; 1991 page no. 3404.
32. Susruta, Susrutasamhita Nidanasthana Dalhana commentary, edited by
Vaidya Jadavaji Trikamji Acharya, chapter 1 – 74th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 268.
33. Susruta, Susrutasamhita Chikitsasthana Dalhana commentary, edited
by Vaidya Jadavaji Trikamji Acharya, chapter 5 – 23th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 428.
34. Vrudda Vagbhatta,Ashtangasangraha Chikitsasthana Indu vyakha, Part
2 edited by Dr. D.V.Pandithrao & Vaidya Ayodhya Pandyeya, chapter 23. Delhi: Vangamaya Anusamdhana Akaka; 1998.
35. Vagbatha, Asthangahrudaya Nidanasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 15 – 54th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 535.
36. Sri Vaidya Sodhala, Gadanigraha, edited by Sri Gangasattaya Pandeya,
Vatarogaadikara 352 – 357th sloka. Varanasi: Chaukhambha Sanskrit Series; 1968 page no. 271.
37. Sri Vaidya Sodhala, Gadanigraha Prayoga khanda, edited by Sri
Gangasattaya Pandeya, Vatarogaadikara 352 – 357th sloka. Varanasi: Chaukhambha Sanskrit Series; 1968 page no. 271.
38. Sri Vaidya Sodhala, Gadanigraha Kayachikitsa khanda, edited by Sri
Gangasattaya Pandeya, 147 & 152th sloka. Varanasi: Chaukhambha Sanskrit Series; 1969 page no. 506.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
138

Bibliography
39. Sharangadhara, Sarngadharasamhitha Poorvakhanda edited by Pandit
Parasurama Sasatri, chapter 7 – 108th sloka. Delhi: Chaukhambha Orientalia; 1983 page no. 103.
40. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by Bishakrathna Sri Brhmashanker Misra, chapter 24 sloka 133-135.Varanasi: Chaukhambha Sanskrit Sadana; 1988. p. 243-244.
41. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by Bishakrathna
Sri Brhmashanker Misra, chapter 24 sloka 140.Varanasi: Chaukhambha Sanskrit Sadana; 1988. p. 243-244.
42. Vangasena, Vangasenasamhitha, edited by Kaviraj Sri Shalligramjji
Vaishya, Vatarakthaadhikara Adyyaya Shloka 117-121, Kamaraj Sri Krishnadasa Prakashsena Mumbai, Page no.: 387.
43. Vangasena, Vangasenasamhitha, edited by Kaviraj Sri Shalligramjji
Vaishya, Vatavyadhadhikara Adyyaya Shloka 326-332, Kamaraj Sri Krishnadasa Prakashsena Mumbai, Page no.: 351.
44. Yogaratnakara, Vatavyadhinidana sloka 3-4. edited by Vaidya
Lakshmipatisastry,. Varanasi: Chaukhambha Sanskrit Sansthan; 1988. p. 511 (Kasi Sanskrit series 160).
45. Vaidyavara Basavaraja, Basvarajeeyam Prakarana 6. Shri Govardhana
Sharma, editor. Varanasi: Chaukhambha Vidyabhavan; 1987. p. 93.
46. Amarasimha, Amarakosha, edited by Pundit Vishwanath Jha, Pranishyavarga 5 sloka 21. Delhi: Motilal Banarasi Das; 1979. p. 102.
47. Susruta, Susrutasamhita Nidanasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 1 – 74th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 268.
48. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 101th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 621.
49. Raja Radha Kantadeva, Shabda kalpadrum, Varanasi: Chaukhambha
Sanskrit Series; Part 2, 1967 page no. 103.
50. Raja Radha Kantadeva, Shabda kalpadrum, Varanasi: Chaukhambha Sanskrit Series; Part 2 21st sloka, 1967 page no. 103.
51. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 56th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 619.
52. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 22 – 54th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
139

Bibliography
53. Susruta, Susrutasamhita Nidanasthana Dalhana commentary, edited by Vaidya Jadavaji Trikamji Acharya, chapter 1 – 74th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 268.
54. Sharangadhara, Sarngadharasamhitha Poorvakhanda edited by Pandit
Parasurama Sasatri, chapter 7 – 108th sloka. Delhi: Chaukhambha Orientalia; 1983 page no. 103.
55. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 15 to 18th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 617.
56. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by Bishakrathna
Sri Brhmashanker Misra, chapter 24 sloka 1 – 2 sloka.Varanasi: Chaukhambha Sanskrit Sadana; 1988. p. 227.
57. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 59th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 619.
58. Vrddha Vagbhata, Astangasamgraha Nidanasthana, edited by
K.R.Srikantha Murthy, chapter 15 – 7,8th sloka. Varanasi: Chaukhambha Orientalia; 1996 page no. 242.
59. Vagbatha, Asthangahrudaya Nidanasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 15 – 5 & 6th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 530, 531.
60. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 15, 16th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 617.
61. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 15 to 18th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 617.
62. Vagbatha, Asthangahrudaya Nidanasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 1 – 14 & 15th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 444.
63. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 16th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 617.
64. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 59th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 619.
65. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 17th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 617.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
140
Bibliography
66. Susruta, Susrutasamhita Sareerasthana Dalhana commentary, edited by
Vaidya Jadavaji Trikamji Acharya, chapter 6– 26th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 366.
67. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 59th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 619.
68. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 1 – 10th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 54.
69. VruddaVagbatha, Ashtangasangraha Nidanasthana, edited by
Prof.K.R.Shrikhantamurthy, chapter 1- 11th sloka Varanasi: Chaukhambha Orientalia; 1996. p. 143.
70. Agnivesa, Charakasamhita Nidanasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 1 – 11th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 196.
71. Agnivesa, Charakasamhita Nidanasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 1 – 8th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 194.
72. Susruta, Susrutasamhita Susrutasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 21 – 33th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 106.
73. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 1 – 5, 6th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 32.
74. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 19th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 617.
75. Agnivesa, Charakasamhita Chikitsasthana Chakrapanidatta
commentary, edited by Vaidya Jadavaji Trikamji Acharya, chapter 11 – 12th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 479.
76. Agnivesa, Charakasamhita Nidanasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 1 – 9th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 195.
77. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 28 – 56th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 619.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
141

Bibliography
78. Susruta, Susrutasamhita Nidanasthana, edited by Vaidya Jadavaji Trikamji Acharya, chapter 1 – 74th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 268.
79. Vagbatha, Ashtangahrudaya Nidanasthana chapter 15sloka 54.
Prof.K.R.Shrikhantamurthy, editor. Varanasi: Chaukhambha Orientalia; 1996. p. 535.
80. VrudaVagbatha, Ashtangasangraha Nidanasthana chapter 15 sloka 56.
Prof.K.R.Shrikhantamurthy, editor. Varanasi: Chaukhambha Orientalia; 1996. p. 248.
81. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 22 – 56th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
82. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by Bishakrathna
Sri Brhmashanker Misra, chapter 24 sloka 129.Varanasi: Chaukhambha Sanskrit Sadana; 1988 page no. 241.
83. Vagbatha, Asthangahrudaya Sutrasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 49th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
84. Vagbatha, Asthangahrudaya Sutrasthana Hemadri commentary, edited
by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 49th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
85. Susruta, Susrutasamhita Nidanasthana Dalhana commentary, edited by
Vaidya Jadavaji Trikamji Acharya, chapter 5 – 13th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 285.
86. Sri Madhvakara, Madhavanidanam Madhukosha vyaakhya, edited by
Yadunandana Upadhyaya, chapter 22 – 54th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
87. Agnivesa, Charakasamhita Chikitsasthana Yogendranath sen vyakhya,
edited by Vaidya Jadavaji Trikamji Acharya, chapter 7 – 14th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 621.
88. Vagbatha, Asthangahrudaya Sutrasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 49th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
89. Vagbatha, Asthangahrudaya Sutrasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 50th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
90. Vagbatha, Asthangahrudaya Sutrasthana Hemadri commentary, edited
by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 50th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
142
Bibliography
91. Vagbatha, Asthangahrudaya Sutrasthana Hemadri commentary, edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 50th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
92. Susruta, Susrutasamhita Nidanasthana Dalhana vyakha, edited by Vaidya Jadavaji Trikamji Acharya, chapter 1 – 74th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 268.
93. Vagbatha, Asthangahrudaya Sutrasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 54th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
94. Vagbatha, Asthangahrudaya Sutrasthana Hemadri commentary, edited
by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 50th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
95. Vagbatha, Asthangahrudaya Sutrasthana Arunadatta commentary,
edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 12 – 50th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
96. Vaidyavara Basavaraja, Basvarajeeyam Prakarana 6. Shri Govardhana
Sharma, editor. Varanasi: Chaukhambha Vidyabhavan; 1987. p. 93.
97. Sri Madhvakara, Madhavanidanam, edited by Yadunandana Upadhyaya, chapter 22 – 55th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
98. Sri Vaidya Sodhala, Gadanigraha Kayachikitsa khanda, edited by Sri
Gangasattaya Pandeya, 19 – 63rd sloka. Varanasi: Chaukhambha Sanskrit Series; 1969 page no. 486.
99. Yogaratnakara, Vatavyadhinidana sloka 67. edited by Vaidya
Lakshmipatisastry,. Varanasi: Chaukhambha Sanskrit Sansthan; 1988 page no. 407.
100. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by
Bishakrathna Sri Brhmashanker Misra, chapter 24 sloka 129.Varanasi: Chaukhambha Sanskrit Sadana; 1988. p. 241.
101. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 22 – 55th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
102. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 22 – 55th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
103. Vrudda Vagbhatta,Ashtangasangraha Sutrasthana Indu vyakha,
Part 1 edited by Dr. D.V.Pandithrao & Vaidya Ayodhya Pandyeya, chapter 19 – 5th sloka. Delhi: Vangamaya Anusamdhana Akaka; 1998 page no.236.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
143

Bibliography
104. Susruta, Susrutasamhita Chikitsasthana Dalahana vyakha, edited by Vaidya Jadavaji Trikamji Acharya, chapter 1 – 7th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 397.
105. Sri Madhvakara, Madhavanidanam, edited by Yadunandana Upadhyaya, chapter 22 – 56th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
106. Sri Vaidya Sodhala, Gadanigraha Kayachikitsa khanda, edited
by Sri Gangasattaya Pandeya, 19 – 64th sloka. Varanasi: Chaukhambha Sanskrit Series; 1969 page no. 486.
107. Yogaratnakara, Vatavyadhinidana sloka 67 – 70th sloka, edited
by Vaidya Lakshmipatisastry,. Varanasi: Chaukhambha Sanskrit Sansthan; 1988 page no. 407.
108. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by
Bishakrathna Sri Brhmashanker Misra, chapter 24 sloka 129.Varanasi: Chaukhambha Sanskrit Sadana; 1988. p. 241.
109. Susruta, Susrutasamhita Sutrasthana Dalhana vyakha, edited by
Vaidya Jadavaji Trikamji Acharya, chapter 45 – 3th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 196.
110. Susruta, Susrutasamhita Sareerasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 4 – 35th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 358.
111. Vagbatha, Asthangahrudaya Sutrasthana, edited by
Bhisagacharya Harisastri paradakara Vaidya, chapter 9 – 37th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 201.
112. Sri Madhvakara, Madhavanidanam, edited by Yadunandana
Upadhyaya, chapter 22 – 56th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 437.
113. Sri Madhvakara, Madhavanidanam Madhukosha vyakha, edited
by Yadunandana Upadhyaya, chapter 14 – 4th sloka. Chaukhamba Sanskrit Sansthan; 1985 page no. 309.
114. Agnivesa, Charakasamhita Chikitsasthana Chakrapani
commentary, edited by Vaidya Jadavaji Trikamji Acharya, chapter 9 – 20th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 469.
115. Agnivesa, Charakasamhita Chikitsasthana Chakrapani commentary, edited by Vaidya Jadavaji Trikamji Acharya, chapter 16 – 14th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 527.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
144

Bibliography
116. Susruta, Susrutasamhita Sutrasthana Dalhana vyakha, edited by Vaidya Jadavaji Trikamji Acharya, chapter 4 – 55th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 360.
117. Vrudda Vagbhatta,Ashtangasangraha Sutrasthana Indu vyakha,
Part 1 edited by Dr. D.V.Pandithrao & Vaidya Ayodhya Pandyeya, chapter 9 – 39th sloka. Delhi: Vangamaya Anusamdhana Akaka; 1998 page no.144.
118. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 10 – 7th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 66.
119. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 10 – 8th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 66.
120. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 30 – 329th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 649.
121. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 28 – 104th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 621.
122. Susruta, Susrutasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 4 – 21 to 26th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 422.
123. Yogaratnakara, Vatavyadhinidana, edited by Bhisagratna
Brahmasankar Sastri, Varanasi: Chaukhambha Sanskrit Sansthan; 1997 page no. 548.
124. Yogaratnakara, Vatavyadhinidana, edited by Bhisagratna
Brahmasankar Sastri, Varanasi: Chaukhambha Sanskrit Sansthan; 1997 page no. 548.
125. Susruta, Susrutasamhita Uttaratantra, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 1 – 25th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 597.
126. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 16 – 35th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 98.
127. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 20 – 13th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 114.
128. Vagbatha, Asthangahrudaya Sutrasthana, edited by
Bhisagacharya Harisastri paradakara Vaidya, chapter 13 – 1 to 3rd sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 211.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
145

Bibliography
129. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 21 – 3rd sloka. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 395.
130. Susruta, Susrutasamhita Chikitsasthana, edited by Vaidya Jadavaji Trikamji Acharya, chapter 4 – 22 to 26th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 422.
131. Vagbatha, Asthangahrudaya Sutrasthana, edited by
Bhisagacharya Harisastri paradakara Vaidya, chapter 1 – 26th sloka. Varanasi: Chaukhambha Orientalia; 2002 page no. 211.
132. Agnivesa, Charakasamhita Siddhisthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 28 – 101th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 678.
133. Susruta, Susrutasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 24 – 30th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 488.
134. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 28 – 78th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 620.
135. Susruta, Susrutasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 33 – 22nd sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 514.
136. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 28 – 79th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 620.
137. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by
Bishakrathna Sri Brhmashanker Misra, chapter 24 sloka 133-135.Varanasi: Chaukhambha Sanskrit Sadana; 1988. p. 243-244.
138. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 28 – 83rd sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 620.
139. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 28 – 83th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 620.
140. Vrudda Vagbhatta,Ashtangasangraha Chikitsasthana Indu
vyakha, Part 2 edited by Dr. D.V.Pandithrao & Vaidya Ayodhya Pandyeya, chapter 23 – 6th sloka. Delhi: Vangamaya Anusamdhana Akaka; 1998 page no. 238.
141. Bhavamishra, Bhavaprakasha Uttarakhanda, edited by
Bishakrathna Sri Brhmashanker Misra, chapter 24 sloka 133-135.Varanasi: Chaukhambha Sanskrit Sadana; 1988. p. 243-244.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
146

Bibliography
142. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 28 – 85th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 620.
143. Agnivesa, Charakasamhita Chikitsasthana, edited by Vaidya Jadavaji Trikamji Acharya, chapter 28 – 86th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 620.
144. Agnivesa, Charakasamhita Siddhisthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 11 – 18th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 728.
145. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 2 – 15th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 25.
146. Agnivesa, Charakasamhita Siddhisthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 10 – 5th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 724.
147. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 20 – 8th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 113.
148. Susruta, Susrutasamhita Sutrasthana, edited by Vaidya Jadavaji
Trikamji Acharya, chapter 35 – 12th sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 150.
149. Amarasimha, Amarakosha Manushyavarga 6 sloka 73. Pundit
Vishwanath Jha, editor. Delhi: Motilal Banarasi Das; 1976. p. 139.
150. Vagbatha, Asthangahrudaya Sutrasthana, edited by Bhisagacharya Harisastri paradakara Vaidya, chapter 17 – 1st sloka. Varanasi: Chaukhambha Orientalia; 2002 page no.253.
151. Agnivesa, Charakasamhita Sutrasthana, edited by Vaidya
Jadavaji Trikamji Acharya, chapter 14 – 39, 40th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 90.
152. Agnivesa, Charakasamhita Chikitsasthana Chakrapani vyakha,
edited by Vaidya Jadavaji Trikamji Acharya, chapter 14 – 305th sloka. Varanasi: Chaukhambha Sanskrit Sansthan; 2004 page no. 620.
153. India kativasti massage, ayurvedic kerala treatment,
consultation.htm www.cochinayurveedic.com. Accessed on 4th June 2006.
154. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 26 – 22nd sloka. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 474.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
147

Bibliography
155. Susruta, Susrutasamhita Chikitsasthana, edited by Vaidya Jadavaji Trikamji Acharya, chapter 32 – 22nd sloka. Varanasi: Chaukhambha Orientalia; 1980 page no. 514.
156. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 26 – 37th sloka. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 477.
157. Neurosurg Focus 16 (1): Article 6, 2004, Sciatica: a historical
perspective on early views of a distinct medical syndrome Neurosurg. Focus / Volume 16 / January 2004 Available from: www.google.com. Accessed on 6th June 2006.
158. Sushrutha, Sushruthasamhitha Shareerasthana edited by Vaidya
Jadavji Trikamji Acharya chapter 5 sloka 27. Varanasi: Krishnadas Academy; 1980. p. 367.
159. Sushrutha, Sushruthasamhitha Shareerasthana edited by Vaidya
Jadavji Trikamji Acharya chapter 5 sloka 14. Varanasi: Krishnadas Academy; 1980. p. 365.
160. Sushrutha, Sushruthasamhitha Shareerasthana edited by Vaidya
Jadavji Trikamji Acharya chapter 5 sloka 37. Varanasi: Krishnadas Academy; 1980. p. 367.
161. Vagbhata, Ashtangahridaya Suthrasthana edited by
Bhisagacharya Harisastri Paradakara chapter 10 sloka 1. Varanasi: Krishnadas Academy; 2002. p. 174.
162. Vagbhata, Ashtangahridaya Suthrasthana Bhisagacharya
Harisastri Paradakara chapter 12 sloka 14. Varanasi: Krishnadas Academy; 2002. p. 194.
163. Sushrutha, Sushruthasamhitha Shareerasthana edited by Vaidya
Jadavji Trikamji Acharya chapter 1 sloka 4. Varanasi: Krishnadas Academy; 1980. p. 338.
164. Agnivesa, Charakasamhitha Shareerasthana edited by Vaidya
Jadavaji Trikamji Acharya chapter 7 sloka 7. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 337.
165. Sushrutha, Sushruthasamhitha Shareerasthana edited by Vaidya
Jadavji Trikamji Acharya chapter 5. Varanasi: Krishnadas Academy; 1980. p. 363.
166. Sushrutha, Sushruthasamhitha Shareerasthana edited by Vaidya
Jadavji Trikamji Acharya chapter 6 sloka 27. Varanasi: Krishnadas Academy; 1980. p. 374.
167. Chaurasia.B.D, Human Anatomy (vol 2) section 1 chapter 7. 3rd
ed. New Delhi: CBS Publishers and Distributors; 1995. p. 75-77.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
148

Bibliography
168. Harrison’s, Principles of Internal medicene, edited by FaUCI, Breanwald, Isselbacher, Wilson ,Martin, Kasper & Longo, Vol 1 1998, Mc Grawttill health profession division, page no.
169. Golwalla’s Medicine for Students, edited by Dr. Aspi F Golwalla
(M.D) & Sharukh.A.Golwalla, 1999, page no. 483
170. Natarajan.M.Dr, Textbook of Orthopedics and Traumatology chapter 12. 4th ed. Chennai: M.N.Orthopedic Hospital; 2000. p. 147-150.
171. Adams. J.C.Dr, Outline of Orthopedics chapter 10. 13th ed.
London: Churchill Livingston; 2001. p. 200-205.
172. Patel T.A, Ogle A.A, Diagnosis and Management of Acute Low back pain. University of Kansas Medical Center.2002. Available from: www.spine-health.com. Accessed on 6th June 2006.
173. Adams. J.C.Dr, Outline of Orthopedics chapter 10. 13th ed.
London: Churchill Livingston; 2001. p. 172-177.
174. Patel T.A, Ogle A.A, Diagnosis and Management of Acute Low back pain. University of Kansas Medical Center.2002. Available from: www.spine-health.com. Accessed on 6th June 2006.
175. Patel T.A, Ogle A.A, Diagnosis and Management of Acute Low
back pain. University of Kansas Medical Center.2002. Available from: www.spine-health.com. Accessed on 6th June 2006.
176. Patel T.A, Ogle A.A, Diagnosis and Management of Acute Low
back pain. University of Kansas Medical Center.2002. Available from: www.spine-health.com. Accessed on 6th June 2006.
177. Mayoclinic.com tool for healthier lives © 1998-2006 Mayo
Foundation for Medical Education and Research (MFMER). Available from www.sciatica-mayoclinic.com. Accessed on 6th June 2006.
178. A Max India Institution, Max Healthcare Caring for you for life
Low Back ace & Sciatica ppt. Available from www.maxindia.com. Accessed on 6th June 2006.
179. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular
Prakashan, 1996, Vol – 1, page no. 202.
180. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular Prakashan, 1996, Vol – 1, page no. 1065.
181. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular
Prakashan, 1996, Vol – 1, page no. 1308.
182. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular Prakashan, 1996, Vol – 1, page no. 170.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
149
Bibliography
183. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no.420.
184. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular
Prakashan, 1996, Vol – 1, page no. 166. 185. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular
Prakashan, 1996, Vol – 1, page no. 1220. 186. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular
Prakashan, 1996, Vol – 1, page no. 969.
187. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular Prakashan, 1996, Vol – 1, page no. 965.
188. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular
Prakashan, 1996, Vol – 1, page no. 990.
189. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr. Ravidutt Tripathi, chapter 12. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 254.
190. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular
Prakashan, 1996, Vol – 1, page no. 1119.
191. Dr K.M.Nadkarni’s, Indian Matria medica, Bombay Popular Prakashan, 1996, Vol – 1, page no. 478.
192. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 393.
193. Dr. Siddhinandan Mishra’s, Ayurvediya Rasashastra, Varanasi Chaukhambha Orientalia, 1998, page no. 376.
194. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 6. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 99.
195. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 120.
196. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr. Ravidutt Tripathi, chapter 7. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 132.
197. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 800.
198. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 335.
199. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 359.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
150

Bibliography
200. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 575.
201. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 331.
202. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 362.
203. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 275.
204. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 275.
205. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 39.
206. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 758.
207. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 632.
208. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 569.
209. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 58.
210. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 403.
211. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 12. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 254.
212. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 12. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 254.
213. Vrddha Vagbhata, Astangasamgraha Sutrasthana, edited by Dr.
Ravidutt Tripathi, chapter 12. Delhi: Chaukhamba Sanskrit Pratishthan; 2003 page no. 254.
214. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 763.
215. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 761.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
151

Bibliography
216. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 494.
217. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 28.
218. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 292.
219. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 758.
220. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 745.
221. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 747.
222. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 365.
223. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no. 253.
224. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no. 455.
225. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no.225.
226. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no.223.
227. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no.221.
228. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no.469.
229. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no.820.
230. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no.822.
231. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi
Chaukhambha Bharati Academy, 1999, Vol. II, page no.282.
232. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no.283.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
152

Bibliography
233. Prof. P.V.Sharma’s, Dravyaguna Vijnana, Varanasi Chaukhambha Bharati Academy, 1999, Vol. II, page no.632.
Evaluation Of The Efficacy Of Punarnavadiguggulu & Mahamashadi Taila Kati Basti In The Management Of Gridhrasi (Sciatica
153

SPECIAL CASE SHEET FOR GRIDHRASI Post Graduate Research and Studies Centre (Kayachikitsa) Shri. D.G.M.Ayurvedic Medical College, Gadag.
Guide : Dr. Vardhacharula M. D (Ayu) Co-Guide : Dr. R. V. Shettar M. D.(Ayu) P.G.S Scholar : Gavisiddanagouda. Patil
1. Name of the patient : Sl. No.
2. Father’s/Husband’s Name : OPD No.
3. Age : ………... yrs IPD No.
4. Sex : Male/Female Bed No.
5. Religion :
Hindu Muslim Christian Others 6. Occupation :
Sedentary Active Labor Others 7. Economical Status :
Poor Middle class Higher class 8. Address : …………………………. Phone No. …………………………. E- Mail: …………………………. Pin code:
9. Date of Schedule Initiation:
10. Date of Schedule Completion:
11. Result :
Good relief
Marked Response
Moderate Response
Mild Response
Not relief
12. Consent : I here by agree that, I have been fully
educated with the disease and treatment.
Here by satisfied whole-heartedly, and
accept the medical trial over me.
Investigator’s Signature Patient’s Signature
1

1) Chief Complaints a) RUK (Pain)
Onset : Sudden Gradual
Varity : Acute Chronic
Nature : Local General Radiated
At Postural Change : Yes No
Aggravating Factors : Physical Exercise Emotion Exposure to cold Exposure to heat
Any other causes Relieving factors :
Rest Pain relievers Pressure Severity of pain :
Gr.0 Gr.1 Gr.2 Gr.3 Gr.4 Lumbar region :
Lumbodorsal Lumbar Lumbosacral
Leg : Right Left Both
Duration :
b) STHAMBHA(Stiffness) : Present Absent
Site : Thigh Calf Foot
Severity : Gr.0 Gr.1 Gr.2 Gr.3 Gr.4
Relieving factors :
Rest Walking Pain relivers
Time :
Early morning After noon Night Duration :
c) ABNORMAL SANSATIONS :
Toda Spandana Ayama d) GOURAVA(Heaviness) :
Present Absent e) DEHAVAKRATHA :
Scoliosis Khyphoscoliosis Right Right Left Left
2

2.Associated Complaints. a) Numbness :
R. Lower limb
L. Lower limb
Bilateral
b) Wasting (muscular) : Present Absent
R. Lower limb
L. Lower limb
Bilateral
c) Constipation : Present Absent
d) Burning sensation : Present Absent
e) Sleeplessness : Present Absent
Daily ……hrs. 3.History of present illness Mode of onset :
Lifting up weight Trauma Sudden jerk
Part first affected : Spik Janu Kati Jangha Prushta Pada Uru
Direction of spread : Back and outer side of thigh, leg & foot
Sacroiliac joints
R. Lower limb
L. Lower limb
Bilateral
Routine activities affected : Yes No
4. History of past illness Episodes of same illness Yes No Obesity Yes No Tuberculosis Yes No Other Vata Vyadhees Yes No Diabetes Mellitus Yes No Trauma/Fracture involved of lumbar region
Yes No
Others Yes No 5. Treatment History
Modern Ayurvedic Others Relief with previous treatment :
Partially relieved No relief at all 6. Family history – relevant :
Yes No
3

7. Personal HistoryAhara :
Veg Mixed Agni :
Manda Teekshn Vishama Sama
Koshta : Mrudu Madhya Kroora
Mutra pravurti- frequency : Day Night
Vyasana : Smoking Tobacco
chewing Alcohol None
Malapravurthi- frequency : 1 time 2 time More Constipated
Aarthavapravurti : Alpa Ati Vishama Rajonivrutti
History of previous Operation : ……………… Type of Anesthesia :
Spinal General Position during daily working hours :
Standing Sitting Stooping Squatting
Nature of work : Hard manual
Moderate manual
Sedentary
House work Office work Others Nature of field work : i) Work in standing : ………. in hrs ii) Work in bending position : ………. in hrs iii) Traveling in vehicles : ………. in kms Specify type of vehicle :
2 wheelers
4 wheeler
Horse riding
Bullock cart
iv) Type of chair used for sitting : Cushion chair
Hard chair
With back rest
Without back rest
v) Sleeping pattern : Korlon Cotton Zuote Carpet Others
vi) Using pillows :
Moderate High Psychological status :
Anxious Grief Depressed Broody Irritable Normal Angry
4
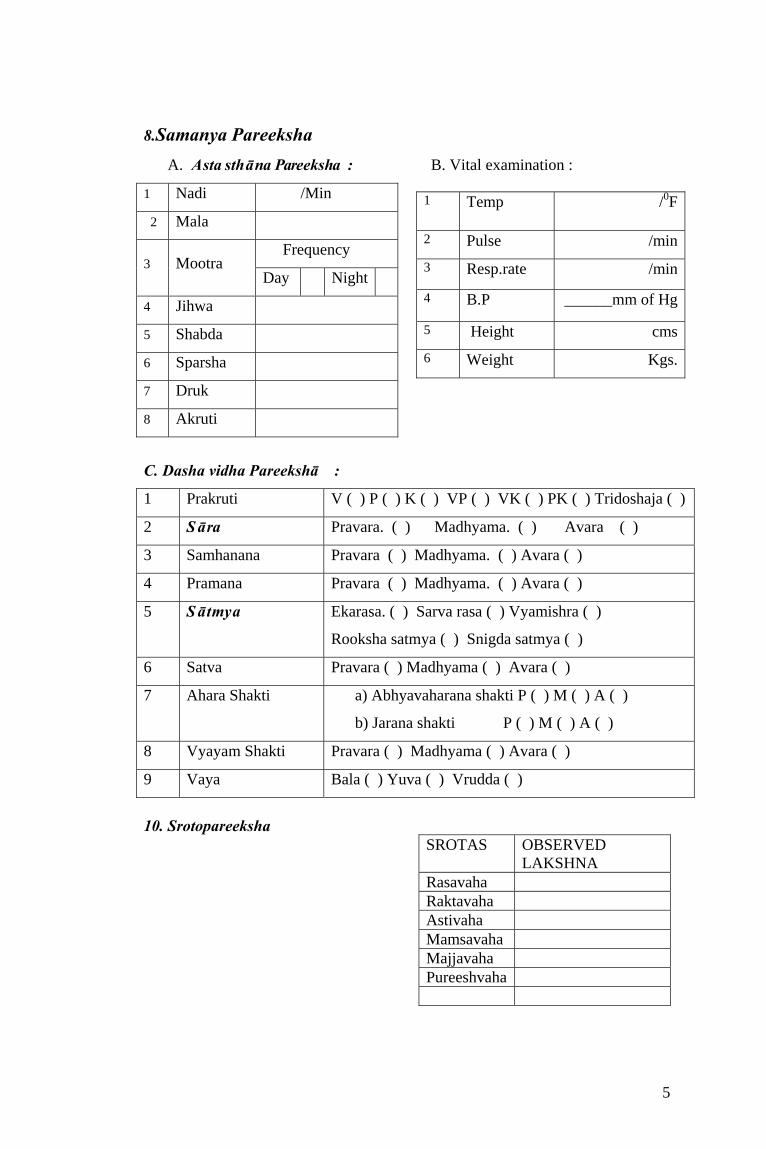
8.Samanya Pareeksha A. Asta sthāna Pareeksha : B. Vital examination :
1 Nadi /Min
2 Mala
Frequency 3 Mootra
Day Night
4 Jihwa
5 Shabda
6 Sparsha
7 Druk
8 Akruti
1 Temp /0F
2 Pulse /min
3 Resp.rate /min
4 B.P ______mm of Hg
5 Height cms
6 Weight Kgs.
C. Dasha vidha Pareekshā :
1 Prakruti V ( ) P ( ) K ( ) VP ( ) VK ( ) PK ( ) Tridoshaja ( )
2 Sāra Pravara. ( ) Madhyama. ( ) Avara ( )
3 Samhanana Pravara ( ) Madhyama. ( ) Avara ( )
4 Pramana Pravara ( ) Madhyama. ( ) Avara ( )
5 Sātmya Ekarasa. ( ) Sarva rasa ( ) Vyamishra ( )
Rooksha satmya ( ) Snigda satmya ( )
6 Satva Pravara ( ) Madhyama ( ) Avara ( )
7 Ahara Shakti a) Abhyavaharana shakti P ( ) M ( ) A ( )
b) Jarana shakti P ( ) M ( ) A ( )
8 Vyayam Shakti Pravara ( ) Madhyama ( ) Avara ( )
9 Vaya Bala ( ) Yuva ( ) Vrudda ( )
10. Srotopareeksha
SROTAS OBSERVED LAKSHNA
Rasavaha Raktavaha Astivaha Mamsavaha Majjavaha Pureeshvaha
5

11. Nidana 1) Swaprakopakara nidana : a) Ahara Guna :
Seeta Rooksha Laghu Rasa :
Katu Tiktha Kashaya Shuskanna :
Yes No Upavasa :
Yes No b) Vihara
Ratrijagarana
Yanam Bharavahana
Vyayama
Pradhavana
Jumping
Pratarana
Walking
c)Manasika : Chinta (worry)
Shoka (grief)
Bhaya (fear)
Krodha (anger)
2) Marmaghatakara nidana : 3) Dhatukshayakaraka nidana : 12. Special Examination
a) Visual analogue scale (VAS)
No Pain 0 1
Mild, annoying pain 2 3
Nagging, Uncomfortable, Troublesome pain
4 5
Distressing, miserable pain 6 7
Intense, dreadful, horrible pain
8 9
6

b) Spinal root examination Root involved Pain Sensory loss Motor weakness Reflex change 2nd Lumbar Front of
mid thigh
Front of mid thigh
Quadriceps Diminished knee jerk
3rd Lumbar Front of lower thigh
Front of lower thigh
Quadriceps Diminished knee jerk
4th Lumbar Side of thigh
Side of thigh Quadriceps Diminished knee jerk
Front of inner thigh
Front of inner thigh
Anterior tibialis
Weak dorsiflexion of foot
5th Lumbar Back of thigh Lateral leg Dorsum of foot to big toe
Back of thigh Lateral leg Dorsum of foot to big toe
Anterior tibialis Weak plantar flexion of big toe
Absent/ Diminished ankle jerk
1st Sacral Base of leg sole and side of foot
Base of leg sole and side of foot
Gastronimus Weak Planter flexion of Big toe and foot
Absent ankle jerk
c) Gait :
Normal Abnormal If abnormal …………………………….type of gait d) Straight Leg Raising (SLR) :
Active Right-Negative /positive At……………..Degrees Left-Negative/Positive At…………….. Degrees Passive Right-Negative/Positive At………………Degrees Left-Negative/Positive At……………….Degrees
e) Reflexes :
7
Knee jerk Leg Absent Diminished Brisk Right
Left Ankle jerks Right Left Babinski’s sign Leg Positive Negative
Right Left

f) Movement of lumbar spine : Type of movements Nil Limited Full Forward flexion Right lateral flexion Left lateral flexion Extension Rotations g) Walking time : Time taken to cover 21 meters Gr.0 Gr.1 Gr.2 Gr.3 Gr.4 h) Movement of hip : Type of movement Nil Limited full Flexion Abduction Abduction Rotation in flexion Internal rotation External rotation
Rotation in Extension Internal rotation External rotation
Extension i) Other Investigations :
Hb% TC
DC P L E M B
ESR
Blood
RBS
Sugar Albumin
Urine
Microscope
X-ray (Lumbosacral) AP & Lat view
13. Treatment Shedule : a. Punarnavadi Guggulu given internally : Date of initiation :
Date of completion :
b. Kati Basti nireekshana : Date of basti initiation :
Date of basti completion :
8

14. Assessment of Results : Chief and Associated Complaints Before 14th Day 30th day After follow up Ruk Sthambha Toda Spandana Ayama Gourava Suptata Shosha Vibandha Daha Assessment of Objective parameter: a) SLR passive Before 14th Day 30th Day After follow up Right Left b) Movements of lumbar spine
i) Forward flexion in cms
ii) Right lateral flexion in cms
iii) Left lateral flexion in cms
Nil Limi Full Nil Limi Full Nil Limi Full Nil Limi Full Ted ted ted ted iv) Extension v) Rotation c) Movement of hip
Nil Limited Full
Flexion Abduction Adduction Rotation in flexion Internal rotation External rotation
Rotation in Extension Internal rotation External rotation
Extension
9

d) Walking time
Before 14th day 30th day After follow up
Gr
.0
Gr
.1
Gr
.2
Gr
.3
Gr
.4
Gr
.0
Gr
.1
Gr
.2
Gr
.3
Gr
.4
Gr
.0
Gr
.1
Gr
.2
Gr
.3
Gr
.4
Gr
.0
Gr
.1
Gr
.2
Gr
.3
Gr
.4
Signature of Scholar Signature of Supervisor
10