growth and growth hormone therapy in children...
TRANSCRIPT

………………..……………………………………………………………………………………………………………………………………..
Growth and Growth Hormone Therapy in Children with CKD ADC 2016
John D Mahan, MD Professor of Pediatrics Nationwide Children’s/the Ohio State University
College of Medicine

………………..……………………………………………………………………………………………………………………………………..
Overview Background
•Growth in Patients with CKD •Causes of Growth Failure in CKD
Growth Assessment and Evaluation for Growth Hormone Treatment in Children with CKD
Growth Hormone Therapy in Children with CKD: Benefits, Risks
Guidelines for Evaluating the Growth Response to rhGH Therapy
2
Growth: the Paramount Concern!

………………..……………………………………………………………………………………………………………………………………..
1. Growth is one of the MOST important issues that children with CKD confront!

………………..……………………………………………………………………………………………………………………………………..
What Concerns Children and Parents About Living with CKD*?
Percent (%)
Reynolds JM Arch Dis Child. 1995;73:36-42.
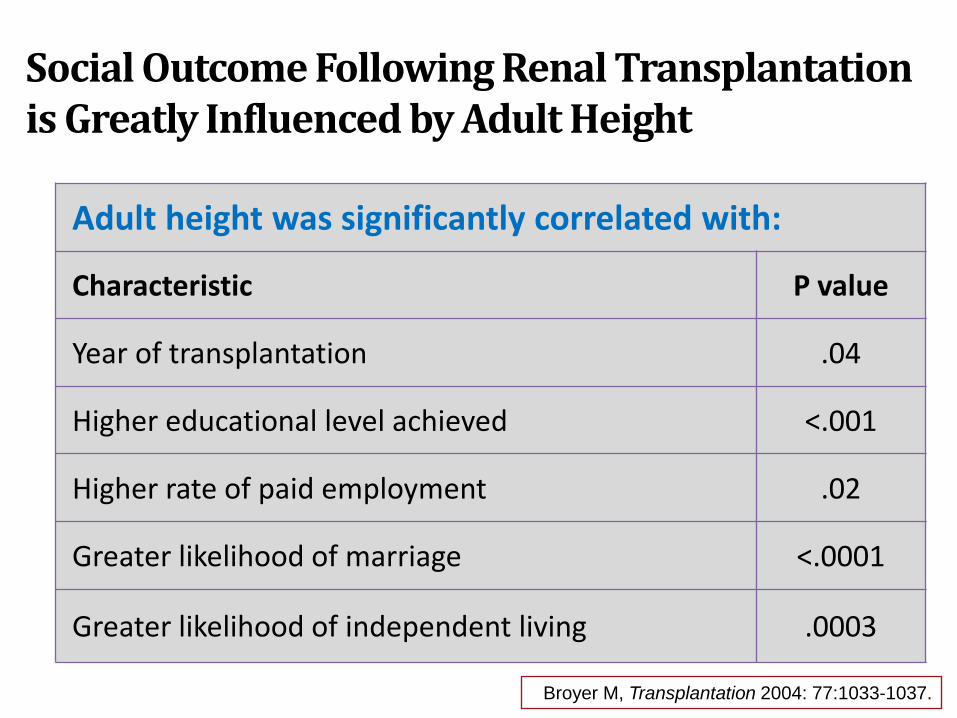
Social Outcome Following Renal Transplantation is Greatly Influenced by Adult Height
Adult height was significantly correlated with:
Characteristic P value
Year of transplantation .04
Higher educational level achieved <.001
Higher rate of paid employment .02
Greater likelihood of marriage <.0001
Greater likelihood of independent living .0003
Broyer M, Transplantation 2004: 77:1033-1037.

Height Dissatisfaction - Impacts Quality of Life
Mean adult height SDS score: –1.56 ± 1.55 Height satisfaction correlated significantly with height SDS score (r = 0.42; P = .006) Quality of life correlated significantly with height satisfaction (r = 0.41; P = .008)
0
5
10
15
20
25
30
35
40
Perc
ent o
f ind
ivid
uals
di
ssat
isfie
d w
ith a
dult
heig
ht
Adults with childhood-
onset ESRD
Healthy age-matched
controls Rosenkranz J, Pediatr Nephrol 2005;20:1288-1294.

………………..……………………………………………………………………………………………………………………………………..
Growth Patterns in Patients with CKD
Child Without CKD
Child With CKD
Height
Birth Puberty
Adapted from Betts et al. Br Med J. 1974;2:189-193.

Growth in Patients with CKD
8
Patient 1 Patient 2

Furth S, Pediatrics 2002
Surv
ival
(%)
100
90
80
70
60
50
40
30 1 2 3 0
Years
Growth Failure in Children with CKD is Associated with Poorer Survival
Age >1, Z > -2.5
Age > 1, Z<-2.5
Age 0-1, Z > -2.5
Age 0-1, Z < -2.5
Height in 2,306 patients with CKD – NAPRTCS At initiation of dialysis - 1992-2001

Furth S.. Pediatr Nephrol 2002
Days
Sur
viva
l (%
)
100
95
90
85
80
75
1000 750 500 250 0 1250 1500 1750 2000
Severe growth failure
Moderate growth failure
Normal growth
Growth Failure in Children on Dialysis is Associated with Poorer Survival
1,112 patients < 18 yo ESRD – USRDS Tanner Stage I to IV, ht data Jan-Dec 1990

………………..……………………………………………………………………………………………………………………………………..
2. The factors that can lead to poor growth in children with CKD include important modifiable and non-modifiable issues!

………………..……………………………………………………………………………………………………………………………………..
Variables That Can Contribute to Growth Failure in CKD*
12 *Growth hormone indicated for CRI patients only, i.e., patients with GFR<75 mL/min/1.73m3.
Mahan et al. Pediatr Nephrol. 2006;21:917-930.
Age of onset of CKD Primary renal disease Calorie deficiency and abnormal protein metabolism Metabolic acidosis Renal osteodystrophy (CKD – Mineral Bone Disorder) Delayed puberty
Other comorbidities Urinary sodium loss Urine concentrating defect Glucocorticoid therapy
Abnormal GH/IGF-I axis

………………..……………………………………………………………………………………………………………………………………..
Patient AC
AC - boy born at 39 weeks gestation • Birth weight: 3030 g • Birth length: 47 cm • Prune belly syndrome (renal
dysplasia) He was polyuric and required
calcitriol, NaHCO3, sodium polystyrene sulfonate, and Sim PM 60/40 formula

Patient AC: Growth Chart 0-36 months

Patient AC: Growth and Renal Status
Age (yr)
Wt (kg)
Wt SDS
Ht (cm)
Ht SDS
Wt/Ht %tile
Cr (mg)
GFR (mL/min/1.73 m2)
Birth 3.03 –0.87 47 –1.11 74 1.9 11.1
0.5 5.4 –3.57 58.5 –4.26 42 1.5 17.5
0.9 8.84 –1.27 71 –1.42 53 1.0 31.9
1.9 11.2 –0.99 82 –1.16 43 1.0 45
2.9 12.9 –0.92 87.1 –2.06 60 1.1 43.5
3.7 15 –0.36 94.6 –1.38 73 1.3 40
4.5 16.9 –0.13 100.5 –1.09 79 1.4 39.5

Patient AC: Growth Chart 2-9 yrs
Midparental height

What Do We Know About Growth Failure in CKD?
Non-Modifiable Younger age at onset of renal disease More significant uremia Tubulo-interstitial disorders Glucocorticoid therapy
Modifiable Excessive water and sodium loss Calorie deficiency and abnormal protein metabolism Metabolic acidosis Renal osteodystrophy (CKD-MBD) Gonadotropin abnormalities
Growth Failure May Occur at Any Level of CKD (GFR) Growth Does Not Typically Improve with Dialysis Growth Failure is Related to Multiple Factors:
Kaskel F. Kidney Int 2003 Tonshoff B. J Nephrol 1995

What Else Have We Learned About Growth Failure in CKD?
Breakthrough! CKD is a Growth Hormone/IGF-1 Resistance State
Growth Hormone Therapy Improves Growth in Children with CKD

Physiology of the GH/IGF-I Axis
Normal Physiology
CKD Physiology
GH – Growth Hormone ALS – Acid Labile Subunit IGFBP – Insulin-like Growth Factor 1 (IGF-1) Binding Protein
Janjua H. Adv Chronic Kid Dis 2011

………………..……………………………………………………………………………………………………………………………………..
Key GH-IGF-1 Pathophysiologic Points
1. GH and IGF-I levels are not reduced in patients with CKD [increased pulses of GH release and reduced renal GH clearance]
2. CKD = reduced responsiveness to endogenous GH and IGF-I •GH resistance reflects
•Defect in post-receptor GH activated JAK2 STAT pathway [leads to blunted IGF-1 response to GH]
•Decreased density of GH receptors in tissues [bone] [as indicated by decreased levels of GHBP]
•IGF-I resistance related to increased circulating IGFBP-1,2,4,6 = up to 50% reduction in bioavailable IGF-I
3. Increased IGFBP-3 proteolysis leads to reduction in IGF-I circulating in IGF-I/ALS/IGFBP-3 complex–therefore reduced IGF-I receptor activation and reduced feedback to the hypothalamus and pituitary

………………..……………………………………………………………………………………………………………………………………..
Multiple Factors Cause GH Resistance in CKD
Mehls O 2008

………………..……………………………………………………………………………………………………………………………………..
GH-IGF-1 Axis in Children with CKD: CKiD
26 - short stature – no rGH Rx 206 - normal height – no rGH Rx. 34 [18 short, 16 normal Ht on rGH RX

………………..……………………………………………………………………………………………………………………………………..
3. The modifiable factors that can lead to poor growth in children with CKD must be addressed in a determined manner!

………………..……………………………………………………………………………………………………………………………………..
Modifiable Factors Associated with Growth Failure in CKD: Treatment Aspects
Modifiable Factor Treatment 1. Malnutrition (Cachexia) Provision of 100-120% RDA
calories - Kari 2. Salt and Water Wasting Supplemental Na/H2O 3. Acidosis Alkali – McSherry 4. Anemia Improved growth associated
with Hb>11 - Boehm 5. CKD-Mineral Bone Disorder
(Renal Osteodystrophy) Better growth with Rx – Chesney
6. Gonadotropic Hormone Abnormalities
?
7. GH/IGF-1 Resistance Distinct Benefit from rhGH Rx – Fine, Mehls

………………..……………………………………………………………………………………………………………………………………..
Nutrition and Growth in CKD
• 101 infants (1986-1998); 1 and 5 year survival - 87 and 78% • Supplemental feeding as soon as growth was subnormal;
81 started enteral feeds at ages 0 to 4.5 years. • 46% gastrostomy • 22% Nissen
• Mortality highest in yr 1 • Length in normal range by 1 year of age • Weight gain better than height gain Kari JA. Kidney Inter 2000; 57:1681–1687.

………………..……………………………………………………………………………………………………………………………………..
Growth in Children on Dialysis (NAPRTCS)
26

………………..……………………………………………………………………………………………………………………………………..
Growth in Children After Transplantation NAPRTCS
27

………………..……………………………………………………………………………………………………………………………………..
Growth in Children After Transplantation NAPRTCS
28

………………..……………………………………………………………………………………………………………………………………..
Growth in Children After Transplantation NAPRTCS
29

………………..……………………………………………………………………………………………………………………………………..
4. CKD is a state of GH and IGF-1 resistance – in some children recombinant GH will be necessary to achieve good growth.

Algorithm for Evaluation and Treatment of Growth Retardation in Children with CKD: Overview
31 Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
Short stature or declining height velocity in CKD 2-5
GH therapy assessment
YES NO
Assess and treat poor growth
Continue therapy
Start GH therapy
Monitor GH therapy
IS GROWTH ADEQUATE?
Assess and correct: Dose, metabolic status,
nutrition, compliance
Continue GH therapy
Consider consult
Discontinue GH therapy if necessary*
Reinitiate GH therapy if reason for discontinuation
resolved
IS GROWTH VELOCITY IMPROVED?
YES NO
YES
NO
Is Growth Adequate?

………………..……………………………………………………………………………………………………………………………………..
Evaluation of Growth in Children with CKD
32 Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
A candidate for treatment of growth retardation should have •CRI (CKD) with GFR<75 mL/min/1.73m3 •Height SDS<-1.88 (3rd Percentile) or Ht Velocity SDS<-2
First, a practitioner should assess and optimally treat modifiable factors that may contribute to poor growth
•Acidosis •Insufficient nutrition/fluids •Salt-wasting •Renal osteodystrophy (CKD-MBD) •Hypothyroidism
Determine whether the growth velocity improves following these treatments
Growth Calculator: www.nutropin.com
………………..……………………………………………………………………………………………………………………………………..
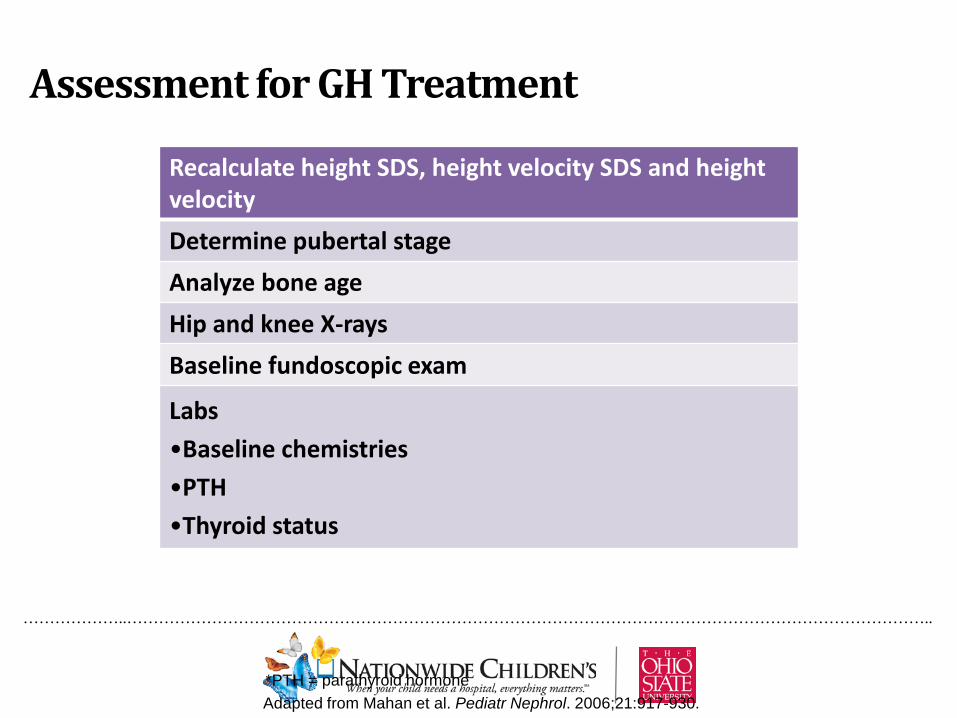
Assessment for GH Treatment
33 *PTH = parathyroid hormone Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
Recalculate height SDS, height velocity SDS and height velocity Determine pubertal stage Analyze bone age Hip and knee X-rays Baseline fundoscopic exam
Labs •Baseline chemistries •PTH •Thyroid status

………………..……………………………………………………………………………………………………………………………………..
Growth Hormone Therapy in CKD
34
• Evaluation • Authorization/Insurance approval • GH Dose:
• 0.35 mg/kg/wk; • divided into daily SC injections
• Patient education

Considerations for GH Administration in CKD
Chronic ambulatory peritoneal dialysis patients should receive their injections in the evening, at the time of the overnight exchange
Chronic cyclic peritoneal dialysis patients should receive injections in the morning after dialysis
Hemodialysis patients should receive their injections at bedtime or at least 3 to 4 hours after treatment to avoid the possibility of hematoma formation from heparin use
Usually recommended to administer in the evening
35

………………..……………………………………………………………………………………………………………………………………..
Growth Hormone Therapy in CKD: Ongoing
36
Adapted from Mahan. Ped Nephrol 2006;21:917-930.
Monitoring growth response/safety - every 3-4 months •Height, weight, height velocity OFC* (until 3 years of age) •Pubertal stage Nutritional intake •Fundoscopic exam Labs (chemistries, PTH) •Bone age, hip and knee X-rays (every year)
Adjusting GH doses as needed Encouraging compliance/measuring IGF-1 levels Consider pubertal dosing if growth response lags during puberty
• 125-200 % of standard dose • If limited time until epiphyseal closure • If IGF-1 response is not large (large = > 3-4 times normal)

Vimalachandra DV, et al. J Pediatr 2001
WMD (95% CI Random) Study
Treatment n
Control n
Weight %
WMD (95% CI Random)
Favors control Favors treatment
Maxwell 1998 Pubertal
Maxwell 1998 Prepubertal
Guest 1998
Fine 1994
Powell 1997
Total (95% CI)
4
9
41
55
30
139
3
6
44
27
14
94
–2 –1 0 1 2
3.4
6.7
19.7
24.4
45.8
100
0.60 (-0.81, 2.01)
0.90 (-0.08, 1.88)
0.30 (-0.21, 0.81)
1.10 (0.66, 1.54)
0.80 (0.56, 1.04)
0.77 (0.51, 1.04)
Effect of rhGH Rx on Height SDS in Children with CKD: A Meta-Analysis

Improved Growth After rhGH Treatment in Children with CKD
38 38 38 Fine R. J Pediatr. 1994;124:374-382.
**P<0.00005 compared to placebo.
Gro
wth
Rat
e (c
m/y
r)
Children with CKD who receive rhGH therapy have better growth rates than placebo-treated children.
**

Sample Size Growth Hormone • Boys = 32 • Girls = 6
Control • Boys = 31 • Girls = 19
Children with Poor Growth Treated with GH Experience Significant Height Prepubertal Gains
39 39
*P<0.001 rhGH vs. non-rhGH.
Haffner D. NEJM. 2004;343:923-930.
Prep
uber
tal H
eigh
t Gai
n (c
m)
Children with CKD who receive GH therapy show a significant improvement in prepubertal height gain.
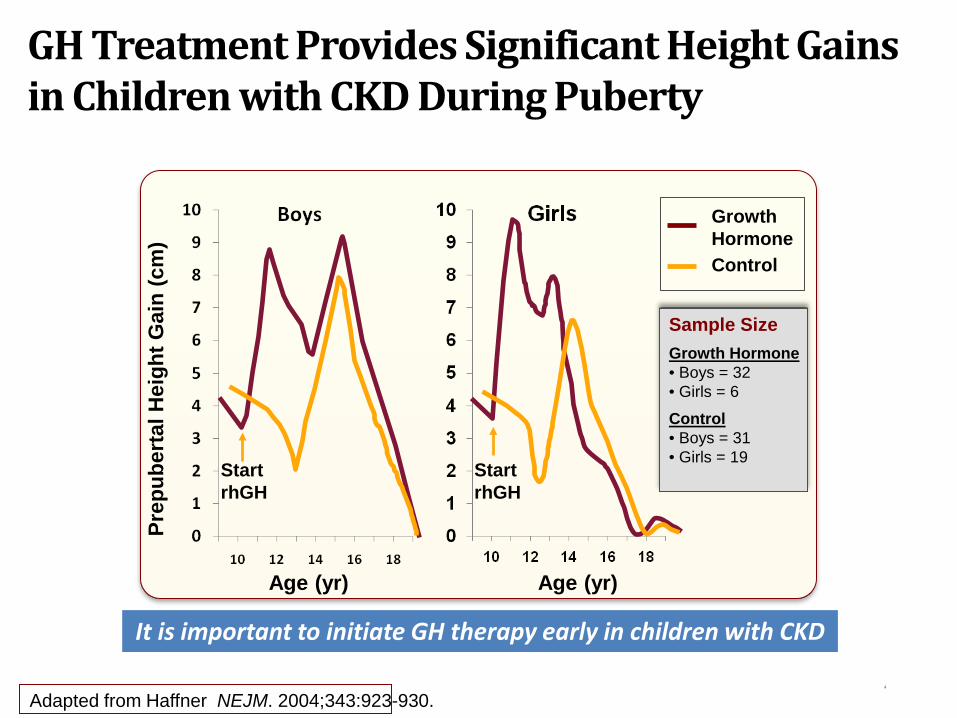
GH Treatment Provides Significant Height Gains in Children with CKD During Puberty
40 40 40 Adapted from Haffner NEJM. 2004;343:923-930.
Prep
uber
tal H
eigh
t Gai
n (c
m)
Sample Size Growth Hormone • Boys = 32 • Girls = 6
Control • Boys = 31 • Girls = 19
Growth Hormone Control
Age (yr) Age (yr)
Start rhGH
Start rhGH
It is important to initiate GH therapy early in children with CKD

Children with CKD Who Receive GH Rx Have Better Final Adult Height Than Those Who Do Not
41 41 41
rhGH effectively improves Final Height in CKD RTx patients, without affecting kidney function
Gil S. Ped Nephrol 2012
Red initial height (IH) (rhGH) Black IH (control) Green final height (FH) (rhGH) Blue FH (control)
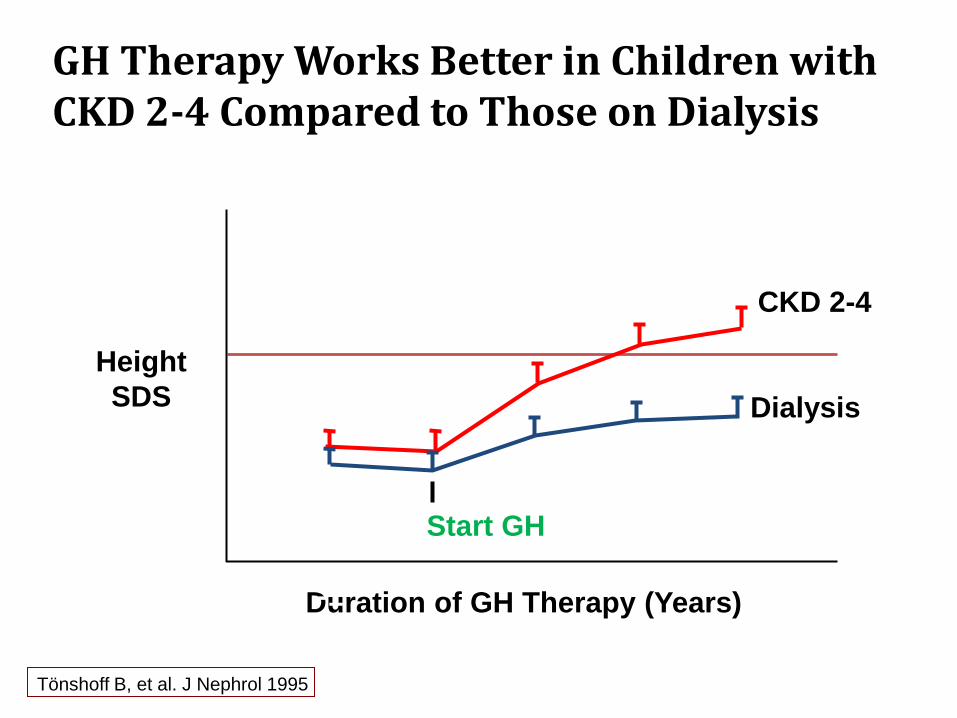
Height SDS
Duration of GH Therapy (Years)
-1
-3
-4
-5
Dialysis
CKD 2-4
Start GH
-2 -1 4
0
GH Therapy Works Better in Children with CKD 2-4 Compared to Those on Dialysis
Tönshoff B, et al. J Nephrol 1995

First Year Height Velocity in CKD: Assure Appropriate Growth Response
Height Velocity During Year 1 of Growth Hormone Treatment and Pretreatment Height Velocity:
Prepubertal Naïve Patients with Chronic Kidney Disease
Mean Height Velocity + 1*SD
Mean Height Velocity
Mean Height Velocity – 1 *SD
Mean PreTreat Height Velocity
Mean Height Velocity – 2 *SD
Baseline Age (yr)
Hei
ght V
eloc
ity (c
m/y
r)
NCGS GH RX in CKD Curves
Mahan JD. Ped Nephrol. 25:1125-30, 2010.

Age at Baseline
Year
1 H
eigh
t Vel
ocity
(cm
/yr) ISS Males
CKD
Year 1 Height Mean Velocity ± 1 SD in ISS Males and CKD Males
Mean Height Velocity + 1*SD
Mean Height Velocity
Mean Height Velocity – 1 *SD
ISS CKD
NCGS

………………..……………………………………………………………………………………………………………………………………..
Predicting Response to GH Rx in Children with CKD
Results: Annualized height velocity (cm/year) during first year of GH Rx best predicted by:
age at start weight SDS underlying renal disorder (hereditary kidney disorder) GFR (at baseline) GH dosage Model explained 37% of variability of growth response (SE = 1.6 cm) Age = most important predictor of growth response (20.3% of
variability) followed by weight SDS at start Only 27.2% of variability of 2nd year response predicted by 1st year
response and GFR Mehls O, J Clin Endocrinol Metab. 2010;95:686-92. 2010.

………………..……………………………………………………………………………………………………………………………………..
5. GH Treatment is Safe and Effective for children with CKD and children Post Renal Transplantation; careful monitoring for complications and appropriateness of growth response is necessary during GH treatment

………………..……………………………………………………………………………………………………………………………………..
Guidelines for Growth Hormone Therapy Discontinuation
47 Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
GH therapy should be discontinued in when: –Achieved 50th percentile for height for age based on mid-parental height –Closed epiphyses –Active neoplasia –Slipped femoral epiphyses –Intracranial hypertension –Noncompliance –Severe hyperparathyroidism (PTH>800 pg/mL – Stage V; >400 pg/mL – Stage II-IV) –At the time of renal transplantation If height velocity remains <2 cm/year over baseline and reason for discontinuation is resolved, GH therapy re-initiation should be considered

Adapted from Bell et al. J Clin Endocrinol Metab. 2010;95:167-177.
Safety: Incidence of Adverse Events in Children with CKD Treated with rhGH
48 48
Targeted Events by Indication Results NCGS CRI Number 54,996 1778 Adverse Events 6.2 10.9 Serious AE 2.4 6.5 Deaths 0.3 1.2 Malignancy* 0.1 0.0 IC Tumor Recurrence 0.3 0.1 Leukemia*† 0.0 0.0 2nd Neoplasm 0.1 0.1 Adrenal Insufficiency† 0.0 0.0 Diabetes Mellitus 0.1 0.2 Intracranial Hypertension 0.1 0.3 SCFE 0.1 0.3 Scoliosis 0.4 0.1 Pancreatitis 0.0 0.0
Data are expressed as percentage. *New onset, no risk factors. †Based on fewer than 15 reports.
3/300 post-renal Tx 1/17 post-liver Tx All 4 on concomitant immunosuppressives

………………..……………………………………………………………………………………………………………………………………..
Safety: Infants with CKD Treated with rhGH
49
Santos CJASN 2010
RCT – open label – 16 infants 29 adverse events: 9 in the rhGH group 20 in the untreated group, *no adverse effects with rhGH Rx

………………..……………………………………………………………………………………………………………………………………..
Safety: Post Transplant Lymphoproliferative Disorder in Patients Treated with rhGH
50
Dharnidharka V. Ped Transpl 2007
PTLD Rates According to rhGH Use During CKD (n = 1647)
No PTLD PTLD Fisher Exact p-value
All cases 1606 (97.5%) 41 (2.5%) 0.009
No rhGH pre-Tx 1217 (98.1%) 23 (1.9%) rhGH pretransplant
389 (95.6%) 18 (4.4%)
• Groups not equal for age, era or post-Tx meds. • The hazard ratio for PTLD development post-transplant, adjusted for transplant era
and age at transplant, was just borderline higher with rhGH use (ratio = 1.88, 95% CI = 1.00–3.55, p = 0.05).
• No data on length of therapy, co-morbidities or specifics of immunosuppression .

………………..……………………………………………………………………………………………………………………………………..
Major Barriers to GH Therapy in Children with CKD
Lack of urgency • That rhGH treatment can be delayed • Short stature perceived as a cosmetic issue Evaluation and documentation • Uncertainty -evaluation, rhGH dosing, monitoring • Reimbursement worries – lack of appropriate
support for reimbursement Patient compliance
51 Mahan et al. Pediatr Nephrol. 2006;21:917-930.
Greenbaum L. Ped Neph 2008

………………..……………………………………………………………………………………………………………………………………..
Patient RP
Boy born at 40 weeks of gestation •Birth weight: 3370 g/Birth length: 47 cm •Joubert’s syndrome with ARPKD
Polyuric and required NaHCO3, calcitriol, anti-hypertensive agents, Epogen.
Required Synthroid for hypothyroidism. Clinical course complicated by reactive airway disease, polyuria;
several admissions for dehydration with gastroenteritis. Delay in sitting and ability to walk noted during first year of life. After repeated attempts to boost caloric intake, he remained near
3rd percentile for weight and below 3rd percentile for height.

Patient RP: Growth and Renal Status
Age (yr)
Wt (kg)
Wt SDS
Ht (cm)
Ht SDS
Wt/Ht SDS
Cr (mg)
GFR (mL/min/1.73 m2)
Birth 3.37 –0.71 47 –1.11 -0.25 1.9 11.1
2.8 10.6 -2.38 85.3 -2.23 -1.45 1.0 47
GH Rx 3.5 11.7 -2.22 89.5 -2.37 -1.25 0.9 57
4.0 11.9 -2.46 89.9 -2.98 -1.15 1.2 41
4.5 13.7 -1.94 96 -2.3 -0.79 1.2 44
5.0 15 -1.73 98.5 -2.38 -0.20 1.1 49
5.5 17.6 -0.94 105.8 -1.48 0.14 1.0 58 Ht velocity
SDS = 7.90!!!

Patient RP: Growth Chart 2-20 yrs
Midparental height
RP DOB 3/9/03 3.37 kg 47 cm

3 Years/1 Month
3 Years/4 Months

4 Years/1 Month

5 Years/7 Months
On GH Rx
5 Years/11 Months
………………..……………………………………………………………………………………………………………………………………..
Take Home Messages: Growth is Important!
Growth is a Vital Sign Poor growth deserves our attention Use Height SDS +/or Height Velocity to monitor growth Consider Mid Parental Height Projection
•[Mom’s ht (in) + Dad’s ht (in)]/2 •Add 2.5 in male •Subtract 2.5 in female
Use all available interventions to improve growth: Calories, fluid/Na, alkali, vitamin D, Growth Hormone The earlier GH is used, the better the final adult height

………………..……………………………………………………………………………………………………………………………………..
Conclusions 1. Growth is one of the MOST important medical issues that children
with CKD confront! 2. The factors that can lead to poor growth in children with CKD
include important modifiable and non-modifiable issues! 3. CKD is a state of GH and IGF-1 resistance – in some children
recombinant GH will be necessary to achieve good growth. 4. Children with CKD who demonstrate growth failure should be
evaluated and all modifiable factors addressed – if poor growth persists, GH therapy should be utilized.
5. GH Treatment is Safe and Effective for children with CKD and children Post Renal Transplantation; careful monitoring for complications and appropriateness of growth response is necessary during GH treatment .
6. Successfully optimizing growth in children with CKD really demonstrates your value as pediatric nephrologist!
59
………………..……………………………………………………………………………………………………………………………………..

………………..……………………………………………………………………………………………………………………………………..
References Haffner D, Schaefer F, Nessel R, et al. Effect of GH treatment on the adult height of children with
chronic renal failure. NEJM. 2000;343:923-30. Hokken-Koelga, Mulder P, De Jong R, et al. Long-term effects of GH treatment on growth and
puberty in patients with CRI. Ped Nephrol. 2000;14:701-706. Kari JA, Rees L. Growth hormone for children with chronic renal failure and on dialysis. Ped
Nephrol. 2005;20:618-621. Kaskel F. Chronic renal disease: a growing problem. Kidney Int. 2003; 64(3):1141-1151. Kuizon BD, Salusky IB. Growth retardation in children with chronic renal failure. J Bone Miner Res.
1999; 14:1680-1690. Mahan JD and Warady BA. Assessment and Treatment of Short Stature in Pediatric Patients with
Chronic Kidney Disease: A Consensus Statement. Ped Nephrol. 2006;21:917-930. Mentser MI, Breen TJ, Sullivan EK, et al. GH treatment of renal transplant recipients – A report of
NCGS and NAPRTCS. J Ped. 1997;131:S20-24. North American Pediatric Renal Transplant Cooperative Study. 2008 and 2011 Annual Reports. Renal
transplantation, dialysis, chronic renal insufficiency. Available at: http://spitfire.emmes.com/study/ped/resources/annlrept.
Mahesh S, Kaskel F. Growth hormone axis in chronic kidney disease. Ped Nephrol. 2007;23:41-48. Janjua HS, Mahan JD. Growth in Chronic Kidney Disease. Adv Chronic Kid Dis. 2011; 18:324-331.

………………..……………………………………………………………………………………………………………………………………..
References Postlehwaite RJ, Eminson DM, Reynolds JM, et al. Growth in renal failure: a longitudinal study of
emotional and behavioural changes during trials of GH treatment. Arch Dis Child. 1998;78:222-229.
Roelfsema V and Clark RG. The GH and IGF Axis: Its manipulation for the benefit of growth disorders in renal failure. J Am Soc ephrol. 2001;12:1297-1306.
Schaefer F, Veldhuis JD, Robertson WR, Dunger D, Scharer K. Immunoreactive and bioactive luteinizing hormone in pubertal patients with chronic renal failure. Cooperative Study Group on Pubertal Development in Chronic Renal Failure. Kidney Int. 1994; 45:1465-1476.
Stefanidis CJ, Klaus G. Growth in prepubertal children on dialysis. Ped Nephrol. 2007;22:1251-1259.
Tonshoff B, Kiepe D, Ciarmatori S. Growth hormone/insulin-like growth factor system in children with chronic renal failure. Ped Nephrol. 2005; 20:279-289.
Wuhl E, Schaefer F. Puberty in chronic renal failure. Adv Ren Replace Ther. 1999; 6:335-343. Vimalachandra D, Craig JC, Cowell CT, et al. GH treatment in children with chronic renal failure: A
meta-analysis of randomized controlled trials. J Peds. 2001;139:560-7. Seikaly M, Salhab N, Warady B, Stablein D, Use of rhGH in children with chronic kidney disease:
lessons from NAPRTCS. Ped Nephrol. 2007; 22:1195–1204. Dharnidharka VR, Talley LI, Martz KL, Stablein DM, Fine RN. Recombinant growth hormone use
pretransplant and risk for post-transplant lymphoproliferative disease – a report of the NAPRTCS. Ped Transplant. 2008; 12:689-95.
Mehls O, Wuhl E, Tonshoff B, Schaefer F, Nissel N, Haffner D. Growth hormone treatment in short children with chronic kidney disease. Acta Pæd. 2008;97:1159–1164.

………………..……………………………………………………………………………………………………………………………………..
References Garibotto G, Russo R, Sofia A, Ferone D, Fiorini F, Cappelli V, Tarroni A, Gandolfo MT, Vigo E, Valli
A, Arvigo M, Verzola D, Ravera G, Minuto F. Effects of uremia and inflammation on growth hormone resistance in patients with chronic kidney diseases. Kidney Int. 2008.
Mahan JD, Warady BA, Frane J, Rosenfeld RG, Swinford RD, Lippe B, Davis DA. First-year response to rhGH therapy in children with CKD: a National Cooperative Growth Study Report. Ped Nephrol. 2010; 25:1125-30.
Mehls O. Predicting the response to growth hormone treatment in short children with chronic kidney disease. J Clin Endo Metab. 2010; 95:686-92.
Moreno L, Santos F, Neto A, Ariceta G, Vara J, Alonso A, et al.Improvement in growth after one year of growth hormone therapy in well-nourished infants with growth retardation secondary to chronic renal failure: results of a multi-center, controlled, randomized, open clinical trial. Ped Nephrol. 2010;25:790.
Santos F, Moreno ML, Neto A, Ariceta G, Vara J, Alonso A, et al.Improvement in growth after 1 year of growth hormone therapy in well-nourished infants with growth retardation secondary to chronic renal failure: Results of a multicenter, controlled, randomized, open clinical trial. Clin J Am Soc Nephrol. 2010;5 (7):1190–7.
Gil S, Vaiani E, Guercio G, et al. Effectiveness of rhGH treatment on final height of renal-transplant recipients in childhood Ped Nephrol. (2012) 27:1005–1009.
………………..……………………………………………………………………………………………………………………………………..
Information for Patients and Families
National Kidney Foundation http://www.kidney.org/
MAGIC Foundation http://www.magicfoundation.org/www
American Association of Kidney Patients http://www.aakp.org/
Kidney & Urology Foundation of America http://www.kidneyurology.org/
Genentech’s Growth Hormone Site (including Stepping Stones, Understanding Growth in Kidney Disease, etc)
www.nutropin.com

Algorithm for Evaluation and Treatment of Growth Retardation in Children with CKD
65

Algorithm for Evaluation and Treatment of Growth
Retardation in Children with CRI
66 66
Patient Selection GFR<75 mL/min/1.73m3
Ht SDS<-1.88 (3rd Percentile) or Ht Velocity SDS<-2
Treat Contributors to Poor Growth Acidosis, Malnutrition, Salt-wasting,
Osteodystrophy, Hypothyroidism
Continue Current Therapy
YES
Is Growth Velocity Improved?
Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.

Algorithm for Evaluation and Treatment of Growth
Retardation in Children with CRI (Cont’d)
67 67 67 Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
NO
Continue Current Therapy
YES
Baseline Assessment for GH Therapy
Recalculate Ht SDS, ht velocity SDS, and height velocity
Pubertal stage, Bone age, Hip and knee X-rays Funduscopic exam
Chemistries, PTH, Thyroid studies
Is Growth Velocity Improved?

Algorithm for Evaluation and Treatment of Growth
Retardation in Children with CRI (Cont’d)
68 68 68 Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
Start Growth Hormone Therapy 0.05 mg/kg/day SC (0.35 mg/kg/wk)
Monitor Every 3-4 months
Height, weight OFC (until 3 years of age)
Pubertal stage Nutritional evaluation Funduscopic exam Chemistries, PTH
Toxicity Every year Bone age
For symptoms Hip and knee X-rays

Algorithm for Evaluation and Treatment of Growth
Retardation in Children with CRI (Cont’d)
69 69 69 Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
Yes, Growth Adequate
No, Growth Inadequate
Continue GH Rx Adjust dose
every 3-4 months based on weight
Assess & Correct Dose for weight Metabolic status
Nutrition Compliance
Consider Pediatric Endocrinology consult
Adequate Growth
Is Growth Adequate? (Ht velocity 2 cm/yr>baseline)
NO
YES

70 70
Algorithm for Evaluation and Treatment of Growth Retardation in Children with CRI (Cont’d)
70 Adapted from Mahan et al. Pediatr Nephrol. 2006;21:917-930.
If height velocity<2 cm/yr, and reason for discontinuation resolved,
consider reinitiation of GH therapy
Discontinue GH Therapy for Achieved ht goal based on mid-parental ht
and/or 50th percentile for age; Closed epiphyses; Active neoplasia;
Slipped femoral epiphyses; Intracranial hypertension; Non-compliance;
Severe hyperparathyroidism (PTH>900 pg/mL – Stage V; >400 pg/mL – Stage II-IV)