great poster
DESCRIPTION
how to make scientific posterTRANSCRIPT

The Anatomy of a Great Poster
Richard Gerkin, M.D.
Bridget Stiegler, D.O.

Introduction:
Syphilis is often described as the great masquerader due
to its diverse manifestations. A high level of suspicion is
needed to identify rare presentations of this disease.
Case:
H.N. is a 30 year old Caucasian male that presented to
the emergency room with a two day history of worsening
headache and vision loss described as a “black blob” to his
superior and temporal visual fields on the right.
Bilateral vision changes began three months prior.
Ophthalmology work up revealed macular edema and a MRI
demonstrated thickening of the right optic nerve sheath
that was consistent with optic neuritis, with no evidence of
multiple sclerosis. He was evaluated by neurology who
diagnosed the patient with migraines. He continued with
waxing and waning visual disturbances over the three
months preceding this visit, that always resolved in
between episodes. For completeness an RPR was drawn
during his neurology evaluation and was noted to be 1:64.
The patient did not receive treatment due to lack of follow-
up. The patient denied penile lesions or subsequent
rashes. Social history revealed both male and female
sexual partners. The rest of the review of systems was
negative.
Physical Exam:
Vital Signs: 98.6 69 102/55 18
General: Alert and oriented
HEENT: Pupils equally round, 2.5mm. Normal pupil
reflexes. No Marcus-Gunn pupils . No retinal lesions on
fundoscopic exam. Extra ocular motion intact and
symmetric bilaterally.
Visual Fields: Right eye “curtain loss” of the upper and
lower nasal regions with spread to upper temporal region.
Visual acuity:
OD: 20/800
OS: 20/30
Skin: no rashes
GU: no penile lesions
Neuro: Sensory intact bilaterally
DTRs: ¾ in upper and lower extremities
Strength: 5/5 in upper and lower extremities
Pertinent Labs:
WBC: 6.5 K/ul
RPR 1:64
MHA-TP : Reactive
HIV: Non-reactive
Lumbar puncture: Clear, colorless fluid
9 WBCs/cmm, 83% lymphocytes, 13% mononucleocytes,
no organisms
VDRL – nonreactive
negative for aspergillosis, coccidiodomycosis, histoplasmosis
Anti-Cardiolipin antibody – negative
Studies:
Repeat MRI of brain and face: no evidence of multiple sclerosis
Transthoracic Echocardiogram with bubble study: normal LV function
with no right to left shunt
Hospital Course:
The patient underwent repeat MRI, ophthalmology and neurology
evaluations and was diagnosed with central retinal artery
occlusion, optic neuritis, and syphilis. Cardiolipin studies and an
echocardiogram were done to rule out embolic causes of central
retinal artery occlusion. The unifying diagnosis of ocular syphilis
explains all presenting symptoms and is consistent with the
history of bilateral symptoms. The patient was treated with a
fourteen day course of IV penicillin. On day seven he noted
improving vision in his right eye. On discharge he had resolution
of symptoms. No further visual deficit was noted.
Follow-up visual acuity:
Discussion:
Syphilis rates had been on the decline during the 1990s but have
increased over the last six years. The rising incidence has been
related to homosexual intercourse.
Syphilis is defined as early syphilis (previously described as
primary), secondary, and early latent, and late syphilis (previously
tertiary). Late syphilis can appear at any time from one to thirty
years after primary infection. The most common manifestations
of late syphilis are gummas, cardiovascular complications and
neurosyphilis. Neurosyphilis occurs in 5-10% of cases of late
syphilis. A rare form of neurosyphilis, ocular syphilis, can
presents with a wide range of symptoms. Ocular symptoms can
also present during secondary syphilis but with a different
presentation. Venous and arterial occlusive events, as in this
case, only present during late stage syphilis. In all instances, all
structures of the eye can be involved.
An RPR greater then 1:32 increases the likelihood of
neurosyphilis by ten fold. CSF-VRDL can be diagnostic but has a
very low sensitivity, being reactive in only thirty percent of cases
and, therefore, does not exclude neurosyphilis. Ocular syphilis
must be diagnosed early and with rapid intervention of IV
penicillin vision loss can be reversed.
References:
Anthony Aldave, MD, Julie King MD, Emmett Cunningham MD. Ocular syphilis. Current Opinion in
Ophthalmology. 2001;12:433-441.
CDC Guidelines. National Surveillance Data for Chlamydia, Gonorrhea, and Syphilis. Trends in
Reportable Sexually Transmitted Diseases in the United States, 2004.
FAR
OD: 20/30
OS: 20/20
NEAR
OD: 20/30
OS: 20/20
Syphilis in the
United StatesCases reported Rate per 100,000
Primary and
secondary7980 2.7
Neurosyphilis 833 0.3
Total 33401 11.5
Arizona Total 974 9.1
Secondary Syphilis Late Syphilis
Anterior
Segment
Blepharitis
Conjunctivitis
Iritis
Episcleritis
Scleritis
Interstitial keratitis
Lens dislocation
Episcleritis
Scleritis
Uveitis
Posterior
Segment
Chorioretinitis
Vitritis
Neuroretinitis
Retinal detachment
Vasculitis
Chorioretinitis
Venous and Arterial
Occlusions
Macular edema

Case Report: A 39year-old female presents to an outside hospital with complaints of nausea and tinnitus after ingesting
more than 400 tablets of 325mg Aspirin. An initial salicylate level was 75 mg/dl 4 hours after ingestion. The ABG at that
time was: pH 7.47, PCO2 23, HCO3 16 . The patient was admitted to the intensive care unit and started on a bicarbonate
infusion with the plan to repeat the salicylate level in 6 hours. However, 3 hours later, a toxicology consult was requested
secondary to the development of confusion, hallucinations, and diaphoresis. A stat salicylate level at that time was 121
mg/dl, and transfer to our facility for dialysis was recommended. Vital signs upon arrival at 1:30AM were: HR 153, RR 44,
BP101/53, Temp. 101.7°. The patient was diaphoretic, delirious, and agitated. On arrival, the patient was given 3 amps of
NaHCO3 IV push and the bicarbonate drip was increased to 500cc/hr while a femoral hemodialysis catheter was placed.
An initial ABG revealed a pH 7.5, pCO2 19, and HCO3 of 18. The anion gap was 24. A repeat salicylate level was
obtained upon arrival and dialysis was initiated. The arrival salicylate level was reported at 152 mg/dl. One hour into
dialysis the patient’s BP fell to 80/40, which was unresponsive to aggressive fluid resuscitation. Norepinephrine was
required for the next 8 hours for blood pressure support. After 12 hours of continuous hemodialysis, the patient was
asymptomatic with normal vital signs and a clear mental status. The salicylate level was of 15 mg/dl at that time, and no
rebound occurred. The CK rose mildly peaking at 3673 IU/L. The patient was transferred to an inpatient psychiatric facility
2 days later.
Conclusion: To our knowledge, this represents one of the highest salicylate levels reported in a patient who survived
without morbidity. This case emphasizes the importance of aggressive treatment and frequent clinical and laboratory
assessments early in the course of salicylate toxicity.
Background: Salicylate toxicity carries a high risk of morbidity and mortality unless recognized early and treated
aggressively. We report a case of severe salicylate toxicity with an excellent outcome despite having one of the highest
salicylate levels ever reported in a survivor.

What to Expect• Purpose
• Elements
• Arrangement
• Research Poster
• Case Presentation Poster
• Construction
• Presentation
• Judging/Evaluation

• Why would you take the time to enter a research or case presentation poster?
• Why wouldn’t you?
• What makes a poster great?• Upon first impression?• After reading?
• What makes a poster irritating?
• What elements are important when judging a poster?

Purpose
• To communicate medical/scientific research
• To illustrate key points in a visually stimulating
and aesthetically pleasing manner
• To represent yourself and your work to peers
and colleagues
• To participate meaningfully in a scientific meeting
or conference

Elements
• Easy for evaluators to read, clean and uncluttered
• Well planned and meets the guidelines set forth
by ACP and other professional societies
• Attracts viewer’s attention, grabs a second look
• Concisely communicates results of investigation

Arrangement
Timing
• The viewer is able to glean the message in 3-5 minutes
• The viewer is able to read the text in 10 minutes
Organization
• Organized in sections similar to a scientific article or oral presentation
• Describes and represents findings of either a scientific research project or a clinical case

Construction
• Use a template/software program• Internet search “poster template”
• Embrace the rough draft process• 1st draft at least one month prior to conference• Multiple considerations
• Font: ≥ 72 point title, ≥ 20 point text• Word count, prose style, grammar, fluidity,
figure clarity, spelling
• Print rough draft on letter sized paper to assess layout challenges

Research Poster
• Title
• Introduction
• Materials and Methods
• Results
• Discussion
• Conclusion
• References
• Acknowledgements

Research Poster• Title; 2 lines or less
• ≥ 72 pt. type, legible at 25 feet• Clear, concise, direct
• Intro; 200 words or less• Define the issue• Establish the purpose of your work• Justify your experimental approach• Provide a clear hypothesis
• Materials and Methods; approximately 200 words• Use figures and tables to illustrate experimental design• Use flowcharts to summarize timing of events• Include photograph or labeled drawing • Outline statistical plan

Research Poster, continued
Results; approximately 200 words• Provide qualitative/descriptive results• Present analyses that specifically address the hypothesis• Refer to charts or images
Discussion; approximately 300 words• Remind the viewer of the hypothesis• Discuss if/why results were conclusive• Point out relevance of findings to other published work • Discuss limitations of the work• Highlight future directions of the research

Research Poster, continued
Conclusion; approximately two sentences
• Concise summary
• Reminds viewer of relevance
References
• Approximately 5-10 citations
• Standard format
Acknowledgement
• Assistance and financial support

Case Presentation Poster
• Title
• Introduction
• History of Present Illness
• Hospital Course
• Family History
• Social History
• Labs, Images, Studies• Discussion
• Conclusion
• References

Case Presentation Poster• Introduction – briefly introduce the type of
condition/disease process – pathogenesis, etiology, microbiology, epidemiology if relevant
• HPI – as in a classic academic history and physical. Age of patient, important past medical history, presenting complaint, events leading to presentation
• Hospital Course - pertinent positive and negative findings on physical exam, work up and treatment plan, involvement of consultants, clinical progress

Case Presentation Poster• Family History
• Social History
• Pertinent Labs/Images• Visual additions attract and inform viewers more
effectively than text• Details on graphs and photos should easily be
viewed from six feet away• If you include a photo, add a thin gray or black
border• If possible use digital, high quality photographs as
many web images have poor printing resolution


Elution Performance of Surgeon-Mixed and Commercially Pre-Mixed
Low Dose Antibiotic Loaded Bone Cement1Nugent, M T; 1Kaul, H; 1,2MacLemore, R; 1Economopoulos K; 1,2McLaren A C (A,B); 2Vernon, B (A,B)
1-Banner Good Samaritan Medical Center, Phoenix, AZ, 2-Arizona State University, Center for Interventional Biomaterials, Tempe, AZ
Introduction: In 2003 the FDA approved low dose
antimicrobial loaded bone cement (AL-PMMA). Published
data on surgeon mixing compared to pre-mixed
preparations report that commercially pre-mixed
preparations have better elution characteristics in two
studies [1,2] and worse elution in a third[3]. Neither study
evaluated how evenly the antimicrobial was dispersed in
the cement.
Research Question: Does surgeon-mixed antimicrobial
loaded bone cement have inferior elution characteristics
compared to commercially pre-mixed formulations?
Hypothesis: Elution of antimicrobials is less and the
antimicrobial is less evenly distributed for surgeon-mixed
low-dose AL-PMMA than for commercially pre-mixed low-
dose AL-PMMA.
Results: The total cumulative weight of recovered
antimicrobial at 30 days (Graph 1) did vary from one
cement to another, but no single mixing method was
consistently different from another or from the premixed
formulation.
The COV was not different for any mixing method (Graph
2). Therefore no meaningful difference in distribution of
antimicrobial in a batch of AL-PMMA was seen for any
mixing method
Discussion: The average elution of antimicrobial from
low-dose AL-PMMA was not different for any mixing
method including commercial premixed formulations.
Also, based on COV of elution of antimicrobial from
individual test cylinders we did not find a meaningful
difference between the antibiotic distribution in low-dose
AL-PMMA using any mixing method. Simply mixing the
monomer in the polymer is sufficient to distribute the
antibiotic in low-dose AL-PMMA.
Conclusion: Surgeon mixed low-dose antimicrobial
loaded bone cement is not inferior in elution to
commercially premixed antibiotic loaded bone cement.
10 test specimens (6mm x 12mm cylinders, ASTM F 451-
99 ) were made from each of the five cements using each
of the four mixing methods and the respective premixed-
formulation using a Teflon mold. All batches of low-dose
AL-PMMA were polymerized in a bowl without vacuum and
introduced into the mold in the dough phase.
Specimens were eluted in deionized water, completely
exchanging the eluant on days 1, 3, 7, 15,and 30. The
eluate was assayed for antibiotic concentration using the
Kirby Bauer disc diffusion bioassay.
Materials and Methods:Five AL-PMMA preparations:
1)Simplex P 1 gram tobramycin (Stryker)
2)Palacos R +G G500 mg gentamicin (Biomet)
3)Smart Set HVG 1 gram gentimicin (Depuy)
4)Cobalt G 500 mg gentamicin (Biomet)
5)Cemex G 1 gram rentamicin (Exactec)
Four surgeon-mixing methodologies:
1)suspension of antibiotic powder in monomer
2) no mixing of antibiotic and polymer
3) hand stirred antibiotic powder into polymer
4) commercial mixing bowl to mix antibiotic powder
into polymer
Graph 2
Figure 1: Experimental setup showing
representative elution vials and bioassay plate
1. Lewis G. Biomaterials. 2005; 26: 4317-25
2. Neut D Acta Orthop Scand 2003; 74(6): 670-676
3. Balsamo LH CORR 2007; 462: 195-199
(Figure 1). Data was analyzed using ANOVA.
Coefficient of Variance was calculated for the
specimens from each mix to determine the
distribution of antimicrobial throughout the batch
Graph 1
A. Research or institutional support has been received from OREF , Arizona State
University and Banner Health;
B. Miscellaneous non-income support (PMMA and antibiotics) have been received from
Biomet, DePuy, Exactec and Stryker.
0
5
10
15
20
25
30
35
40
Pre Mix Suspension No-Mix Hand-Stirred Bowl-Mix
Mixing Method
Coe
ffic
ient
of Var
ianc
e (%
)
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Pre Mix Suspension No-Mix Hand-Stirred Bowl-Mix Machine Mix
Mixing Method
Antibi
otic
Rel
ease
(µg)
Cemex
Cobalt
PalacosC
PalacosS
Simplex
SmartSet

Brucellosis As the Cause of Recurrent Fevers
Introduction Case
Lindsay Alaishuski, MD and Jason Leubner, MSIVDepartment of Family Medicine Banner Good Samaritan Hospital
Human brucellosis is a rare but potentially life
threatening zoonotic disease of bacterial origin. While
widespread in the Middle East, this infection is rare to
the United States, with approximately 100 reported
cases each year. Transmission occurs via direct contact
with or consumption of milk from infected goats,
sheep, or cattle. Brucellosis is a multisystem disease
with many nonspecific symptoms including fever,
malaise, myalgias, and weight loss. Maternal infection
with Brucella during pregnancy can lead to significant
morbidities such as spontaneous abortion, intrauterine
fetal demise and preterm labor. We report a case of
recurrent fevers in pregnancy due to undiagnosed
brucellosis, possibly leading to preterm delivery.
A 17 year-old Gravida 2, Para 1 Hispanic
woman had an uneventful first trimester of
pregnancy. A first trimester ultrasound was done in
Mexico, and prenatal labs were normal with the
exception of anemia. At 23 weeks gestation,
unexplained fevers and panctyopenia prompted a
hospitalization where a CT scan showed bilateral
pneumonia and axillary lymphadenopathy.
Appropriate antibiotics were given and fevers
resolved. Patient was readmitted at 28 weeks
gestation for nightly fevers, myalgias, and elevated
inflammatory markers. Consultation and workup by
hematology/oncology and infectious disease did not
reveal a fever source. Antibiotics were again given
and symptoms resolved.
With similar symptoms and new onset
hypotension, patient was admitted at 32 weeks
gestation. Emergent c-section was performed for
non-reassuring fetal heart tracings. Nightly fevers
persisted after delivery. Postpartum labs revealed
transaminitis and continued panctyopenia.
Hepatosplenomegaly was seen on abdominal CT
scan. With extensive serologic testing pending, it
was discovered that patient spent time on a farm in
Mexico in her early pregnancy, during which she
consumed unpasteurized dairy products. Empiric
doxycylcine was begun, and prompt resolution of
fevers occurred. Patient was discharged in stable
condition on a six week course of rifampin and
doxycycline. Exhaustive infectious serologic testing
resulted in positive Brucella IgM titers. Given the
patient’s dietary and travel history, serologic findings
and antibiotic response, the diagnosis of brucellosis
was supported. Four months postpartum, febrile
symptoms again recurred and were once again
responded well to the doxycylcine/rifampin regimen.
Diagnosis of brucellosis is mainly made from
detailed history, serologic testing and blood cultures.
Antepartum antbiotics can be protective against
spontaneous abortion. Prognosis is generally excellent,
but relapse, even after appropriate antibiotic therapy,
may occur in 10% of patients.
In a patient with the appropriate history, the
diagnosis of brucellosis should be entertained when
evaluating a fever of unknown origin. While rare in the
United States, travel to endemic areas should raise
clinical suspicion for Brucella infection.
in an Ante-, Peri-,and Post-partum Woman
1st Trimester 2nd Trimester 3rd Trimester Peripartum Postpartum
•Healthy
•Normal Ultrasound in Mexico
•Prenatal labs: Anemia
•Healthy
•Normal Ultrasound in Mexico
•Prenatal labs: Anemia
28 weeks: Nightly fevers and myalgias
•Labs: Elevated ESR, CRP, and LDH
•Labs: Continued pancytopenia, transaminitis
•CT abd/pelvis: Hepatosplenomegaly
•Serology: + Brucella IgM titers
4 months postpartum: Fevers return
•CT abd/pelvis: Prominent spleen and inguinal lymphadenopathy
•Azithromycin/ ceftriaxone given & fevers resolve
32 weeks: Fevers, hypotension, and tachycardia
•Emergent C-section for non-reassuring FHTs
•Empiric doxycycline & fevers resolve
•Doxycycline/ rifampin & clinical improvement
Features of Brucellosis Percentage
of Cases
Our
Patient
Signs and Symptoms
Malaise 90
Sweating 84.4
Arthralgia 81.9
Fever 79.8
Myalgia 49.2
Vomiting 21.7
Hepatomegaly 21.3
Discussion
Images from Pappas G, et al. ―The new global map of human brucellosis‖ Lancet Infect Dis. 2006; 6: 91-99.

The Presentation• Know your poster inside and out, be able to present a synopsis
without reading from the poster (two minutes or less)
• Maintain eye contact with the judges during your evaluation
• Brainstorm potential questions ahead of time
• Practice presenting to multiple people, request that they ask you questions
• Be prepared to discuss any tests or laboratory findings that are inconsistent
• Know the limitations of your study type
• Be well versed on both sides of concepts that may be controversial
• Know your references; do not list a reference that you have not read

Judging and Evaluation
• Who will be judging your poster• Attending physicians, unfamiliar with author
• What kind of questions you will be asked• Preparation is key, anticipate questions
• Have friends and colleagues tell you what their questions would be
• Any style of question is possible
• Breakdown of points system
• Example judging sheet

Value Anchor Explanation
1 Outstanding Virtually flawless, with negligible weaknesses
2 Excellent Very strong, but with some minor weaknesses
3 Very Good Strong, but with some moderate weaknesses
4 Good Weak, but with some moderate strengths
5 Acceptable Very weak, with some minor strengths
6 Unacceptable Inadequate
Rating Scale
Area Description
Presentation Was the content logically arranged, easy to read,
clearly written, and visually effective?
Significance Does the study help to understand and/or
improve human health?
Rationale Were the reasons for the study clear? Was the
study justified?
Research Design Was the study designed to clearly and directly
answer the research question?
Analysis/Interpretation Was the analysis proper and did the conclusions
flow from the research question and data?
Originality Was the approach to the research question unique
and original?
Content Areas: Research Poster

Area Description
Presentation Was the content logically arranged, easy to read,
clearly written, and visually effective?
Significance Does the report help to understand and/or improve
human health?
Discussion Did the poster effectively “mine” all available
information from the case?
Originality Were the choice and approach to the case unique
and original?
Content Areas: Case Report


A VERA-cious Cause of Cirrhosis Elise Barney, DO, ACP Associate
Department of Internal Medicine, Banner Good Samaritan Medical Center
Carl T. Hayden VA Medical Center, Phoenix, AZ
CaseThe patient was a 40 year-old previously healthy Native-American woman who presented to the emergencydepartment with diffuse abdominal pain and ascites.An extensive workup was done and she wasdiagnosed with cirrhosis. The etiology of her cirrhosis wasunclear at that time and she was discharged from thehospital. She returned to the emergency departmentseveral months later with recurrent severe abdominal pain.CT of the abdomen showed small intrahepatic IVC and twoportal venous phase enhancing hepatic nodules,suspicious for regenerative/Budd-Chiari nodules (Figure 1).
Learning Points Budd-Chiari syndrome (BCS)
results from hepaticoutflow obstruction from either thrombosis of the hepaticveins or the inferior vena cava. Diagnosis of BCS is made by
dopplerultrasonography Myeloproliferative disorders
account for ~ 50% ofcases of Budd-Chiari syndrome, polycythemia vera beingthe most common. Major WHO criteria for the
diagnosis of PV includeHg level of >18.5 in men or > 16.5 in women, a sustainedincrease of > 2 g/dL from baseline, an elevated red cellmass, and the presence of a JAK2V617F mutation. ~ 95% of patients with PV will
carry the JAK2tyrosine kinase V617F mutation, causing cytokine-independent activation of JAK-STAT and other pathways inerythropoietin-receptor signaling (Figure 4).
Laboratories were significant for a hemoglobin of 11.8 with RBCof 5.05, platelets 213, MCV 71, hypochromia, albumin 2.7, AST39, ALT 23, total bilirubin 2.0 and PT 18.8. Abdominal dopplerultrasound revealed an inferior vena cava thrombus (Figure 2).
References
1.Menon K.V., Shah V, Kamath PS. The Budd-Chiari Syndrome. N Eng J Med 2004; 350:578-85.
2.Campbell PJ, Green AR. The Myeloproliferative Disorders. New England J Med 2006; 355:2452-66.3.Vannucchi AM, Guglielmelli P, Teffer A. Advances in Understanding and Management of Myeloproliferative Neoplasms. CA Cancer J Clin 2009; 59: 171-191.4.Valla D.C.. Thrombosis and Anticoagulation in Liver Disease. Hepatology 2008; 47: 1384-1391.5.Kralovics R, Passamonti F, Buser AS et al. A Gain-of-Function Mutation of JAK2 in myeloproliferative Disorders. New England Journal of Medicine 2005; 352: 1779-90
Figure 1. White arrow shows Budd-Chiari nodule in left
hepatic lobe. Yellow arrow shows narrowed intrahepatic IVC.
As many as 40% of BCS patients without clear etiology are carriers of the JAK2 V617F mutation. Without treatment, 50% die from thrombotic events within 18 months of diagnosis. Anticoagulation is controversial but low-dose aspirin is recommended in all patients.
Figure 4. In Panel A, in the absence of ligand, the erythropoietin receptor (EPOR) binds JAK2 as an
inactive dimer, leading to signaling through pathways made up of Janus kinases and signal transducers and
activators of transcription (JAK–STAT). In cells with the V617F mutation, the signaling is increased, even in the
absence of erythropoietin. In Panel B, the JAK2 protein binds to multiple cytokine receptors —EPOR,
thrombopoietin receptor (MPL), and others that are important for hematopoietic stem-cell biology and
differentiation. In Panel C, the development of homozygosity for the V617F mutation involves an initial point
mutation followed by mitotic recombination of chromosome 9p between the JAK2 locus and the centromere.
Figure 2. Image A shows flow in IVC by doppler but elevated velocities, with
peak of 279 cm/sec. Image B shows 1.8 cm echogenic thrombus in proximal IVC.
Hypercoaguable workup was negative. The etiology of her Budd-Chiari was unclear at the time and the patient was discharged home. During a third hospitalization for recurrent thrombosis, further workup revealed a JAK2 V617F mutation to be homozygous positive with a tumor load of 2093. Upon review of her records, it was noted that she had an elevated RBC of 7 and hemoglobin of 17.5 one year prior. A Transjugular Intrahepatic Portosystemic Shunt (TIPS) was performed with hepatic venography (Figure 3) and the patient was discharged home with outpatient Transplant Clinic follow-up.
Figure 3. Image A shows a normal hepatic venogram of the right
hepatic vein with no collateral circulation between the tributaries of the hepatic vein. Image B shows venography from a patient with Budd-Chiari in which the right hepatic vein is not visualized and instead, there is a rich collateral circulation between the tributaries of the hepatic vein and the liver capsule, forming a "spider's web.” Image C shows our patient with tiny occluded hepatic veins and significant collaterals. Image D shows the anatomic causes of Budd-Chiari syndrome along with the typical radiographic finding of enlarged caudate lobe.
A
D
C
B
A B
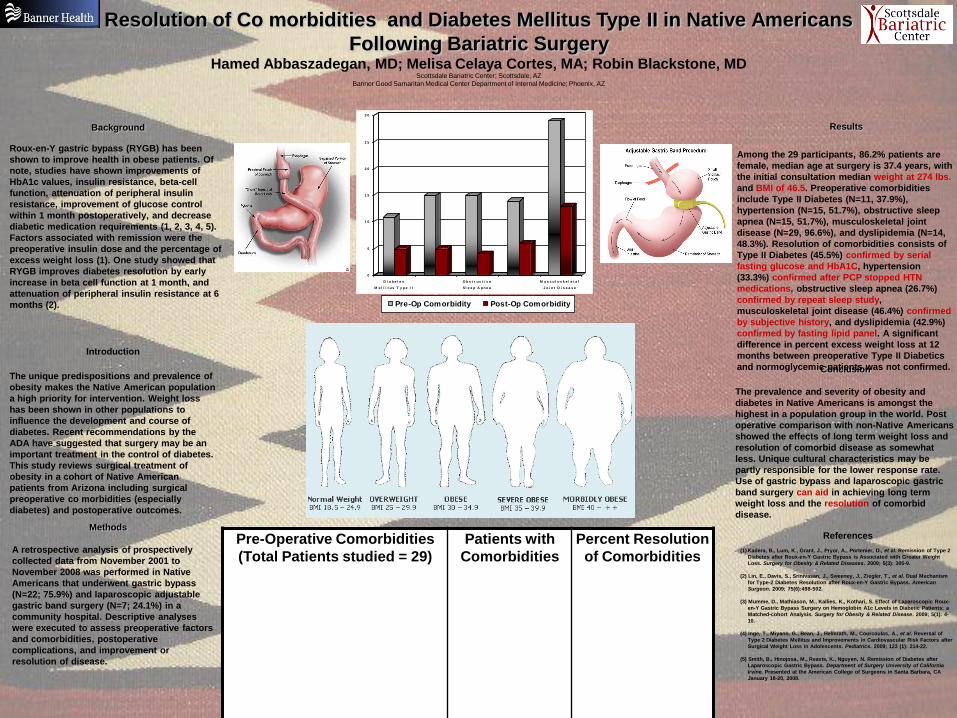
Roux-en-Y gastric bypass (RYGB) has been
shown to improve health in obese patients. Of
note, studies have shown improvements of
HbA1c values, insulin resistance, beta-cell
function, attenuation of peripheral insulin
resistance, improvement of glucose control
within 1 month postoperatively, and decrease
diabetic medication requirements (1, 2, 3, 4, 5).
Factors associated with remission were the
preoperative insulin dose and the percentage of
excess weight loss (1). One study showed that
RYGB improves diabetes resolution by early
increase in beta cell function at 1 month, and
attenuation of peripheral insulin resistance at 6
months (2).
Introduction
The unique predispositions and prevalence of
obesity makes the Native American population
a high priority for intervention. Weight loss
has been shown in other populations to
influence the development and course of
diabetes. Recent recommendations by the
ADA have suggested that surgery may be an
important treatment in the control of diabetes.
This study reviews surgical treatment of
obesity in a cohort of Native American
patients from Arizona including surgical
preoperative co morbidities (especially
diabetes) and postoperative outcomes.
Pre-Operative Comorbidities
(Total Patients studied = 29)
Patients with
Comorbidities
Percent Resolution
of Comorbidities
0
5
1 0
1 5
2 0
2 5
3 0
D i a b e t e s
M e l l i t u s T y p e I I
O b s t r u c t i v e
S l e e p A p n e a
M u s c u l o s k e l e t a l
J o i n t D i s e a s e
Pre-Op Comorbidity Post-Op Comorbidity
Resolution of Co morbidities and Diabetes Mellitus Type II in Native Americans
Following Bariatric SurgeryHamed Abbaszadegan, MD; Melisa Celaya Cortes, MA; Robin Blackstone, MD
Scottsdale Bariatric Center; Scottsdale, AZ
Banner Good Samaritan Medical Center Department of Internal Medicine; Phoenix, AZ
References
(1) Kadera, B., Lum, K., Grant, J., Pryor, A., Portenier, D., et al. Remission of Type 2
Diabetes after Roux-en-Y Gastric Bypass is Associated with Greater Weight
Loss. Surgery for Obesity & Related Diseases. 2009; 5(3): 305-9.
(2) Lin, E., Davis, S., Srinivasan, J., Sweeney, J., Ziegler, T., et al. Dual Mechanism
for Type-2 Diabetes Resolution after Roux-en-Y Gastric Bypass. American
Surgeon. 2009; 75(6):498-502.
(3) Mumme, D., Mathiason, M., Kallies, K., Kothari, S. Effect of Laparoscopic Roux-
en-Y Gastric Bypass Surgery on Hemoglobin A1c Levels in Diabetic Patients: a
Matched-cohort Analysis. Surgery for Obesity & Related Disease. 2009; 5(1): 4-
10.
(4) Inge, T., Miyano, G., Bean, J., Helmrath, M., Courcoulas, A., et al. Reversal of
Type 2 Diabetes Mellitus and Improvements in Cardiovascular Risk Factors after
Surgical Weight Loss in Adolescents. Pediatrics. 2009; 123 (1): 214-22.
(5) Smith, B., Hinojosa, M., Reavis, K., Nguyen, N. Remission of Diabetes after
Laparoscopic Gastric Bypass. Department of Surgery University of California
Irvine. Presented at the American College of Surgeons in Santa Barbara, CA
January 18-20, 2008.
Conclusion
The prevalence and severity of obesity and
diabetes in Native Americans is amongst the
highest in a population group in the world. Post
operative comparison with non-Native Americans
showed the effects of long term weight loss and
resolution of comorbid disease as somewhat
less. Unique cultural characteristics may be
partly responsible for the lower response rate.
Use of gastric bypass and laparoscopic gastric
band surgery can aid in achieving long term
weight loss and the resolution of comorbid
disease.
Results
Among the 29 participants, 86.2% patients are
female, median age at surgery is 37.4 years, with
the initial consultation median weight at 274 lbs.
and BMI of 46.5. Preoperative comorbidities
include Type II Diabetes (N=11, 37.9%),
hypertension (N=15, 51.7%), obstructive sleep
apnea (N=15, 51.7%), musculoskeletal joint
disease (N=29, 96.6%), and dyslipidemia (N=14,
48.3%). Resolution of comorbidities consists of
Type II Diabetes (45.5%) confirmed by serial
fasting glucose and HbA1C, hypertension
(33.3%) confirmed after PCP stopped HTN
medications, obstructive sleep apnea (26.7%)
confirmed by repeat sleep study,
musculoskeletal joint disease (46.4%) confirmed
by subjective history, and dyslipidemia (42.9%)
confirmed by fasting lipid panel. A significant
difference in percent excess weight loss at 12
months between preoperative Type II Diabetics
and normoglycemic patients was not confirmed.
Methods
A retrospective analysis of prospectively
collected data from November 2001 to
November 2008 was performed in Native
Americans that underwent gastric bypass
(N=22; 75.9%) and laparoscopic adjustable
gastric band surgery (N=7; 24.1%) in a
community hospital. Descriptive analyses
were executed to assess preoperative factors
and comorbidities, postoperative
complications, and improvement or
resolution of disease.
Background

Example Posters

BACKGROUND
STUDY OBJECTIVE RESULTS
CONCLUSIONS
Complete data were available for nine quintuplet pregnancies. Every pregnancy required antepartum hospitalization. The average number of admissions to the hospital was 1.7 (SD+/-0.7). The mean length of antepartum stay was 46.9 days (SD+/-26.5). The overall mean gestational age at delivery was30.9 weeks or 30w6d (SD+/-10.2days). Only one pregnancy delivered prior to 24 weeks resulting in no viable infants. The gestational age at delivery for this pregnancy was 18 weeks. This pregnancy was delivered vaginally. The primary indication for delivery was chorioamnionitis. The mean gestational age of the remaining pregnancies was 32.5 weeks or 32w3d (SD+/-12.5days). The primary indication for delivery in the remaining ten deliveries were pre-elampsia (2/8, 25.0%), preterm labor (2/8, 25.0%), gestational age (2/8, 25.0%), severe pre-eclampsia (1/8, 12.5%), and premature preterm rupture of membranes (1/8, 12.5%). No pregnancy was allowed to progress further than 34 weeks gestation. All pregnancies were delivered by cesarean section. The mean estimated blood loss was 1288.9ml, SD+/-609.2. There were no intrauterine demises and 1 neonatal death excluding the 18 week delivery, resulting in a perinatal mortality rate of 25/1000.
Within this population of quintuplet pregnancies, the mean gestational age at delivery for pregnancies delivering beyond 24 weeks gestation was 32.5 weeks. The primary indications for delivery were preeclampsia, preterm labor, and elective delivery at 34 weeks gestation. Antepartum hospitalization, PTL, anemia, and pre-eclampsia were frequent complications in this population. In comparison, placenta previa, PPROM, HELLP, twin-to-twin transfusion syndrome, and hyperemesis gravidarum were infrequently observed.
METHODS
To report the maternal morbidity as well as obstetrical complications in the quintuplet pregnancies cared for at our institution over a twelve year period.
All patients cared for by Phoenix Perinatal Associates an Affiliate of Obstetrix Medical Group, with a sextuplet or quintuplet pregnancy were reviewed. The charts reviewed included both Phoenix Perinatal Associates (PPA) outpatient office records and hospital charts. Only those patients cared for by PPA were reviewed. A patient list was compiled and only those charts were requested from the BGSMC medical records department. Statistical analysis was not be done prior to the review as this is a retrospective chart review of pregnancy outcomes. Also, there were not enough patients to find a statistically significant difference. Descriptive data was presented as means with standard deviations and percentages of patients with outcome variables.
Good Samaritan is one of the nation’s leading centers for multiple births and high-risk obstetrics. Our obstetricians deliver more high order multiples – triplets, quadruplets and quintuplets -- than any other facility in the world. Over one hundred high order multiple pregnancies have been cared for at Banner Good Samaritan Medical Center by Obstetrix Medical Group. Elliott and Rodin first published outcomes of our first 10 sets of quadruplets in 1992. Since then, we have cared for and delivered 80 more mothers with quadruplets. We now have also cared for nine mothers with quintuplets and two with sextuplets.
Variable Frequency (%)
Antepartum Hospitalization 100.0
Hyperemesis Gravidarum 11.1
Hyperemesis Gravidarum requiring TPN 11.1
Anemia 77.8
Anemia requiring antepartum transfusion 55.6
Previa 0.0
Pre-eclampsia 75.0
Twin-to-twin Transfusion Syndrome 11.1
HELLP Syndrome 12.5
PPROM 11.1
Introduction
It is estimated that 6-10% of school-aged children suffer from Attention Deficit Hyperactivity
Disorder (ADHD). Treatments for ADHD include the use of stimulants, (methylphenidate, etc.)
and psychotherapy(1). A significant number of patients treated with psychostimulants exhibit an
inadequate response or cannot tolerate their use (2). The potential for abuse with the use of
stimulants is a concern and is a factor in the quest for non-stimulants to treat the condition.
Atomoxetine (StratteraTM), known chemically as benzenepropanamine N-methyl-alpha-(2-
methoxyphenoxy), hydrochloride, was approved for the treatment of ADHD in November 2002.
Marketed as a non-stimulant alternative in the treatment of ADHD, atomoxetine is a specific
norepinephrine reuptake inhibitor. Atomoxetine has little affinity for other noradrenergic receptors
or for other neurotransmitter transporters or receptors (3).
In therapeutic doses, atomoxetine is rapidly absorbed from the gastrointestinal tract, with peak
plasma level occurring in 1-2hours after ingestion. Atomoxetine is metabolized by aromatic ring
hydroxylation, benzylic oxidation, N-Demethylation and by hepatic microsomal enzyme P4502D6.
As a result of P4502D6 metabolism, pharmacokinetics is influenced by polymorphic
expression (3).
To our knowledge, there are no other reports of Atomoxetine overdose in the literature. The
purpose of this study was to describe the effects of isolated Atomoxetine overdose.
Methods
We conducted a retrospective chart review of all human exposure calls (~150, 000 charts) for
atomoxetine ingestions reported toour Poison Control Center (PCC) during the years immediately
following the release of the drug. Of the ~150,000, 17 accounted for isolated atomoxetine
ingestions.
Inclusion criteria were defined as any oral atomoxetine ingestion in human beings, irrespective of
age, referred to our PCC. Chart review was conducted using Crystal Reports™ in Visual
Dotlab™. The only exclusion criterion was the inability to meet the inclusion criteria.
Following a brief training of systematic chart review, reviewer’s blinded purpose of this study
completed a standardized data collection sheet. A third reviewer, acting as a tie-breaker was used
in cases of conflict between the two reviewers. Age, outcomes and signs and symptoms were
recorded. Patients were followed for up to 24 hours or until cessation of signs and symptoms. The
study received expedited review from the institutional board review for all patient identifiers were
removed and here were no interventions.
Results
Symptoms were reported in 9 of 17 patients. Symptoms included gastrointestinal upset,
hyperactivity, drowsiness, throat irritation, dizziness, tremor, tachycardia and tremor. Ages
ranged from 9 months to 28 years (mean of 15.6 years). Doses of Atomoxetine were 10 –
1,2000mg.
Symptoms were delayed as long as three hours in three patients. All neurological symptoms were
preceded by tachycardia. Tachycardia was reported in 58%, emesis was reported in 34% and
17% had agitation and received benzodiazepines. All symptoms resolved within 30 hours.
Discussion
Little is known about the effects of isolated Atomoxetine overdose. Sawant and Daviss report a
case of a 15-year-old male with a 1,200 mg Atomoxetine ingestion. His hospital course was
complicated by two grand mal seizures and QTC prolongation.
Atomoxetine, as the sole agent was presumed, from a pill count. However, the patient had access
to Bupropion, Risperidone and Alprazolam as well.(4) To our knowledge there are no additional
reports of Atomoxetine reported in the literature.
In our study about isolated Atomoxetine ingestions developed symptoms. Symptoms may have
been delayed for up to three hours. All symptoms resolved in 30 hours. Some of the limitations of
our study include the retrospective nature, small sample size, lack of conformation of ingestion
and the patient’s self-reporting of ingestions.
We conclude that isolated Atomoxetine ingestions commonly result in toxicity and can be delayed
for up to 3 hours post ingestion.
References
1) Michelson D, Faries D, Wernicke J, Kelsey D, Kendrick K, Sallee FR, Spencer T
Atomoxetine in the treatment of children and adolescents with attention-
deficit/hyperactivity disorder: a randomized, placebo-controlled, dose-response study.
Pediatrics. 2001 Nov;108(5):E83.
2) Spencer T, Heiligenstein JH, Biederman J, Faries DE, Kratochvil CJ, Conners CK,
Potter WZ. Results from 2 proof-of-concept, placebo-controlled studies of
atomoxetine in children with attention-deficit/hyperactivity disorder.
J Clin Psychiatry. 2002 Dec;63(12):1140-7.
3) Chalon SA, Desager JP, Desante KA, Frye RF, Witcher J, Long AJ, Sauer JM, Golnez
JL, Smith BP, Thomasson HR, Horsmans Y. Effect of hepatic impairment on the
pharmacokinetics of atomoxetine and its metabolites. Clin Pharmacol Ther. 2003
Mar;73(3):178-91.
4) Sawant S, Daviss SR. Seizures and prolonged QTc with atomoxetine overdose
Am J Psychiatry. 2004 Apr;161(4):757. No abstract available
5) Wernicke JF, Kratochvil CJ. Safety profile of atomoxetine in the treatment of children
and adolescents with ADHD. J Clin Psychiatry. 2002;63 Suppl 12:50-5. Review.
6) Michelson D, Allen AJ, Busner J, Casat C, Dunn D, Kratochvil C, Newcorn J, Sallee
FR, Sangal RB, Saylor K, West S, Kelsey D, Wernicke J, Trapp NJ, Harder D.
Once-daily atomoxetine treatment for children and adolescents with attention deficit
hyperactivity disorder: a randomized, placebo-controlled st
Am J Psychiatry. 2002 Nov;159(11):1896-901.

BACKGROUNDABSTRACT
METHODS
RESULTS
CONCLUSIONS
Objective: To determine if a remote proctor can successfully educate and improve simulated operative hysteroscopic performance by intern residents and medical students.
Design: Randomized study evaluating the performance and complications associated with a simulated hysteroscopic myomectomy when performed by interns and medical students who received concurrent education and feedback via real time tele-video.
Setting: Urban teaching hospital: Banner Good Samaritan Medical Center, Phoenix, AZ 85006
Participants: Seven PGY-1 and eleven medical students undergoing third year clerkships or fourth year electives in the OB/GYN department at Banner Samaritan Hospital.
Conclusion: Remote training via tele-video on simulated virtual reality trainers can reduce medical errors and could be a valid means to educate and/or evaluate surgical and subspecialty surgical residents in the future.
Baseline data obtained included the number of hysteroscopic procedures observed and or performed. All participants were given a standardized tutorial over the simulated program, study objectives, and the components of a resectoscope. Participants underwent the hysteroscopic simulation of a myomectomy using the Immersion Hysteroscopic Simulator. Interns and medical students were randomized into two arms: The study participants received assistance from a remote proctor via real time interactive tele-video, and the control group participants performed the tests without assistance. Data collected included: Time required to identify specific areas of the uterus, total myoma volume resected and complications encountered; i.e. uterine perforations. A post-test evaluation of the project was given to seek feedback about their experience.
Current methods of evaluating residents’ surgical skills and techniques have revolved around subjective, usually retrospective faculty assessment. It has been shown that this type of evaluation lacks reliability, validity and can be influenced by interpersonal factors not associated with technical skill[1]. Reznick et al from the University of Toronto was first to describe an objective assessment of technical skills 1,2,3. Goff et al from the University of Washington has also successfully demonstrated that their Objective Structured Assessment of Technical Skills (OSATS) curriculum is “an innovative, reliable, and valid method of assessing surgical skills”4. It has been demonstrated and suggested that objective assessment of laparoscopic psychomotor skills is possible with virtual reality5. It was our goal to inquire if it is possible to remotely both proctor and evaluate endoscopic skills with a virtual reality hysteroscopic trainer via a remote telecommunications link with given specific objective tasks to complete.
Participants Able to Complete Module I Without
Perforation
0
0.2
0.4
0.6
0.8
1
1 2
Control Group VS Proctor Group
Series1
Fibroid Resection Without Perforation
0
0.2
0.4
0.6
0.8
1
1 2
Control Group VS Proctor Group
Series1
Perforations Encountered
0
0.1
0.2
0.3
0.4
0.5
1 2
Control Group VS Proctor Group
Series1
Module I (Specific Location and Identification of Intrauterine Foci) provides a number of striking differences between the control and study arms. The number of participants who were able to complete the module without perforation showed the control participants finished 8 out of 16 attempts vs. 15 out of 16 attempts for the study group (Fischman’s Exact Test p= .015). The study arm’s improvement between the first and second trial showed a 29.9% reduction in time (Paired T-Test p= .015). An analysis of the control’s improvement was impossible to perform given only 2 participants were able to complete the module.
Module II (Resection of a Submucosal Fibroid) showed the same trend as Module I in regards to improved efficacy and safety with a remote proctor. However, given the small sample size, the data was not statistically significant. The control group managed to complete a portion of a myomectomy without perforation 11 out of 16 attempts versus 15 out of 16 attempts for the study arm (Fischer’s Exact Test p= .172). A majority of the participants in the control group deployed the cauterizing loop, and with continuous cut current, literally used a saw like motion to resect out the fibroid. Statistically significant was the 106% improvement of resection between the first and second trials for the seven participants that were able to complete both tests in the study group (Paired T-Test p= .011). Compare this with the 18.3% improvement for the four participants in the control group (Paired T-Test p= .161).
Finally, there were a total of 32 opportunities to perforate the uterus in each arm of the study. In the control group, with no proctoring, there were 13 perforations for a 40.6% perforation rate. The study arm encountered 2 perforations for a 6.2% perforation rate.
This study provides information that it may be possible to instruct and to help develop proper endoscopic surgical technique from a remote location with a virtual reality based system. The advantage of a remote instructor lies in the possibility that a single instructor at one location may be able to educate a number of trainees in various locations, i.e. different resident programs. This novel idea will reduce instructor costs by reducing travel time and lodging expenses. This study also suggests that it is possible to evaluate a person’s performance on a simulated task. This has immense possibilities in medical education as a single proctor could more objectively evaluate a number of test takers across the nation from a single location, and this evaluation of performance would be free of interpersonal bias.
REFERENCES1. Reznick RK. Teaching and testing technical skills. Am J Surg 1993;165:358-61.
2. Reznick R, Regehr G, MacRae H, Martin J, McCulloch W. Testing technical skill via an innovative “bench station “ examination. Am J Surg 1997;173:226-30.
3. Winckel CP, Reznick RK, Cohen R, Taylor B. Reliability and construct validity of a structured technical skills assessment form. Am J Surg 1994;167:423-427.
4. Goff BA, Lentz GM, Lee D, Fenner D, Morris J, Mandel LS. Development of a bench station objective structured assessment of technical skills for obstetrics and gynecology residents. Obstet Gynecol 2001;98:412-6.
5. Haluck RS, Gallagher AG, Satava RM, Webster R, Bass TL, Miller CA. Reliability and validity of endotower, a virtual reality trainer for angled endoscopic navigation.Medicine Meets Virtual Reality 2002.