government affairs update and training webinar for...
TRANSCRIPT

2/26/2015
1
Government Affairs Update andTraining Webinar for
Chapter Legislative Representatives
February 26, 2015
Lisa Tomlinson, Vice President of Government Affair s and Practice GuidanceNancy Hailpern, Director, Regulatory Affairs
Laura Evans, Legislative Affairs Representative

2/26/2015
2
Objectives
• Provide overview and training on the role of CLRs
• Provide updates on: – Federal Legislative Issues
– Federal Regulatory issues
– State Legislative Issues
APIC Overview

2/26/2015
3
Strategic Goals
Patient Safety: Demonstrate and support effective infection prevention and control as a key component of patient safety.
Implementation Science: Promote and facilitate the development and implementation of scientific research to prevent infection.
IP Competencies and Certification: Define, develop, strengthen, and sustain competencies of the IP across the career span and support board certification in infection prevention and control (CIC®) to obtain widespread adoption.
Advocacy: Influence and facilitate legislative, accreditation, and regulatory agenda for infection prevention with consumers, policy makers, health care leaders, and personnel across the care continuum.
Data Standardization: Promote and advocate for standardized, quality and comparable HAI data.
Strategic Goals 2020
Vision: Healthcare without infectionMission: Create a safer world through prevention of infection
APIC Advocacy Team

2/26/2015
4
APIC Government Affairs Team Staff Primary Role:
background in government affairs and advocacy
Public Policy Committee (PPC) Primary Role:
clinical background with volunteer public policy experience
Chapter Legislative Representatives (CLRs):
APIC
Staff
Chapters
(CLRS)
Public
Policy
Committee
clinical and chapter/local volunteer experience
APIC Policy
Influence
2015 Public Policy Committee
Committee ChairAnnemarie Flood RN, BSN, MPH, CIC
Committee Vice ChairD. Kirk Huslage RN, BSN, MSPH, CIC
MembersRebecca Fitzpatrick DNP, RN, CIC
Patrick Kleinkort RN, BSN, MHA, CICMary Alice Lavin RN, MJ, CIC
Rosie Lozano MPH, CICC. Nancy O’Connor MBSA, BSN, RN, CIC
Tarry Samsel BSN, RNC, CICMary Virgallito RN, MSN, CIC
Senior Advisor Susan Dolan RN, MS, CIC

2/26/2015
5
2015 Chapter Legislative Representatives
Rebecca StockwellMary-Lark DupontMary Alice LavinPatricia MarquezAngela GerkenStephanie KreilingCindy York Joanne HolmanDiane BennettCarol WardMaribeth ColuniGeorge AllenMary ShanksSharon BradleyChristine KettunenJoan BartholomewPongpetch HansrisukRosie LozanoKatie CaryEmily MillsAmy NicholsJan Ratterree
Janet SuttmillerSharon BerryErica DisharoonPatti Steger Amy JablonowskiPaula ListerKerry FlintNancy BarrettSusan SlavishSarah TiceSheila FletcherArlene BrumbachStephanie LambertKelley GarnerKitti FloodKarla WalshSuzanne Mamrose-HuntAbby KengerskyBarbara RomanPatrick KleinkortValerie HendersonShilla Patel
Beth GoodallM. Jeanne CummingsLarry KrebsbachMichelle KaiserPaul ThomasDr. Patti GrotaCasey LandholtKymberly LengyelCathy StampfliRhonda ReedAmanda ValykoTonya Anderson RomeroTarry SamselHelen GarciaMelissa AllenCarolyn CooperKatherine WardSusan CramerLinda Johnson Linda GoddardDonita Gorman
Ashlie MilfordBarbara BrenchleyVivian NutschCarol WilkieVirginia SwindleConnie BushJanet BaconTroy CutlerCharlotte WheelerTobin JohnsonDeeAnn VaageCaroline Taylor
CLR Roles and Responsibilities

2/26/2015
6
CLRs:
• Must be knowledgeable about APIC policy positions.
• Have an interest in and be willing to develop expertise in the legislative process and on federal and state legislative and regulatory issues.
• Serve as the primary contact between the chapter and APIC staff on public policy issues.
• Provide public policy reports at all chapter meetings.
• Mobilize chapter members to respond to issues, when requested by APIC staff, and provide necessary follow up to both chapter members and staff.
• Respond to APIC Action Alerts, notices, and other communication in a timely manner.
• Share major outcomes of chapter grassroots efforts with APIC.
Chapter Legislative Representative Roles and Responsibilities
Communication Tips

2/26/2015
7
APIC, founded in 1972, is an international organization of more than 15,000 members.
APIC is the leading provider of infection prevention resources through education, training, government advocacy, and implementation of research. APIC members represent healthcare facilities — including hospitals, outpatient surgery centers, long-term or specialty care facilities, and home care groups — as well as industry, and local and state health departments.
Many members serve on committees or boards of national organizations to influence improvements in patient safety in all healthcare settings.
What is APIC?
Policymakers may be familiar with infection prevention, but may not realize that there is a person whose job it is to prevent healthcare-associated infections (HAIs). Effectively communicating who infection preventionists (IPs) are will help policymakers understand the many hats that IPs wear on the job. IPs are professionals who dedicate their careers to preventing HAIs. These professionals play a significant role in: • Developing proven policies to ensure a safe environment for patients. • Ensuring compliance with standards and regulations designed to
protect patients and healthcare workers. • Tracking and monitoring activities to identify HAIs and other infectious
agents. • Acting as leaders in emergency preparedness to be ready for events
such as an influenza pandemic or acts of bioterrorism. • Leading and participating in healthcare quality improvement efforts. • Educating the public and healthcare personnel about infectious
diseases and how to limit their spread. • Reporting communicable diseases to the CDC.
Who are Infection Preventionists?

2/26/2015
8
Frequently Asked Questions?
http://consumers.site.apic.org/
Communicating with Policymakers
These images from APIC’s Infection Prevention and You campaign are a perfect example of the level of communication a policymaker may be able to process.

2/26/2015
9
Poll Question
Which of the following APIC resources are you familiar with? (Check all that apply)
Legislative Information and Toolkit

2/26/2015
10
State Key Contacts
Included in each CLR training manual is a list of key contacts within each state that a chapter covers. For example, the CLR manual for APIC Chapter 123 Intermountain Region will contain key contacts for Idaho, Montana, Oregon, Nevada, Washington and Utah.
Each list of key contacts includes the mailing address and phone number for the Governor, Lt. Governor (if applicable) and U.S. Senators. Instructions are provided for each CLR to locate their U.S. Representative, State Representative, and State Senator.
The toolkit includes:
· Tips for planning a legislative visit· Tips for deciding which legislators to meet with· Tips for preparing materials· Sample planning timeline· Sample meeting request letters· Sample talking points· Sample follow-up letters
The VIP Advocacy Toolkit
2/26/2015
11
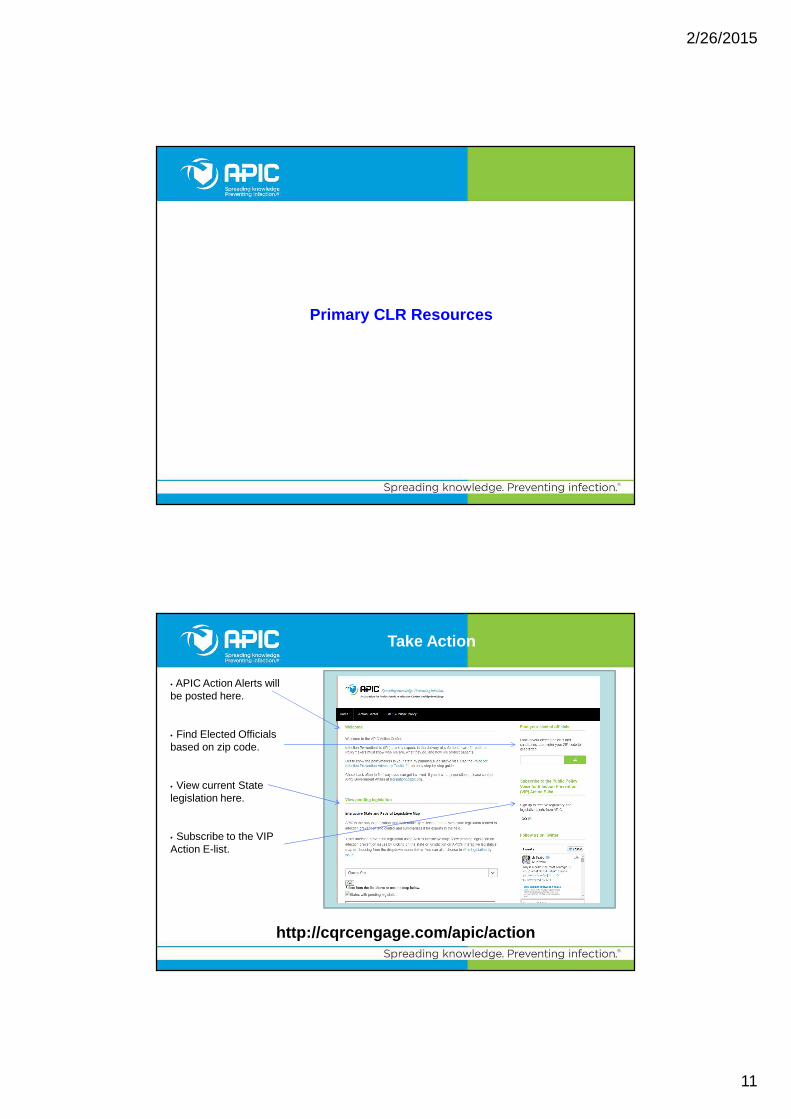
Primary CLR Resources
Take Action
• APIC Action Alerts will be posted here.
• Find Elected Officials based on zip code.
• View current State legislation here.
• Subscribe to the VIP Action E-list.
http://cqrcengage.com/apic/action

2/26/2015
12
Regulations
• This is a library of a wide range of Public Policy resources. For example:– Proposed
Federal regulations
– APIC comments on federal regulations
– Final Federal regulations
http://www.apic.org/Advocacy/Regulations
Interactive State Legislative Map
• This is where you can check for legislative updates for specific states and/or by issues we follow
• Options: – click on a
specific issue– choose a state
from the pull-down menu
– click on a specific state on the map
http://www.apic.org/Advocacy/Legislation
2/26/2015
13
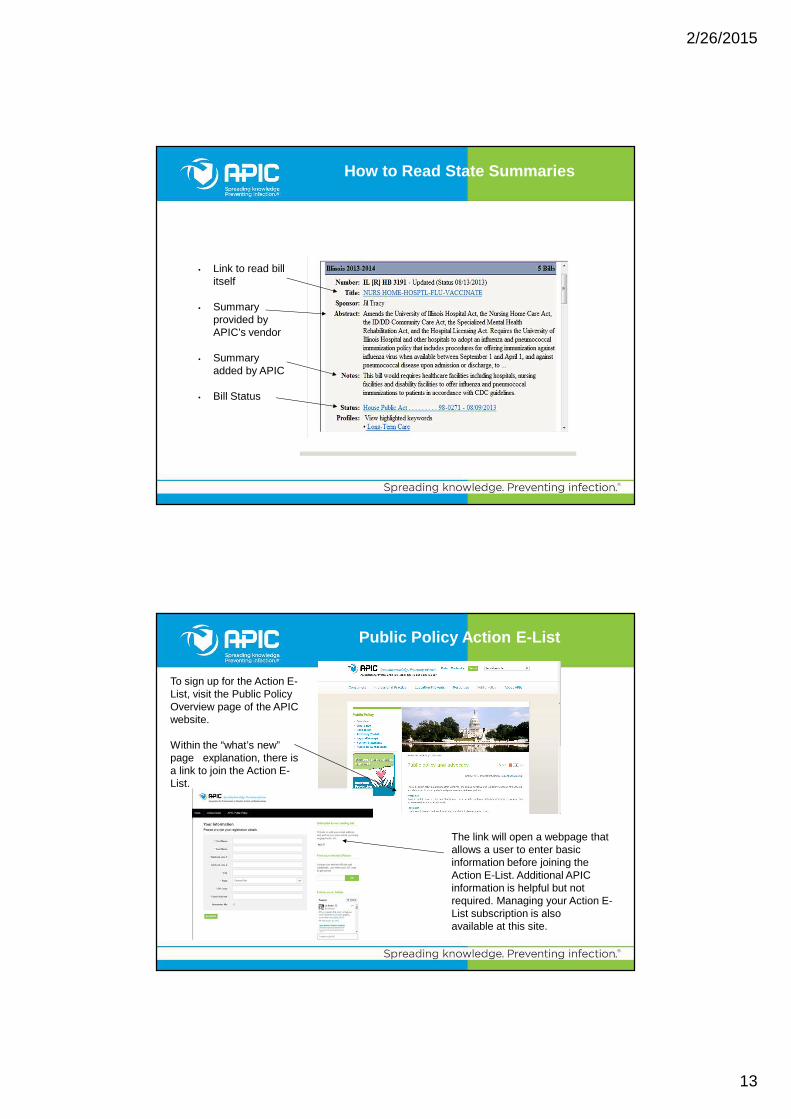
How to Read State Summaries
• Link to read bill itself
• Summary provided by APIC’s vendor
• Summary added by APIC
• Bill Status
Public Policy Action E-List
To sign up for the Action E-List, visit the Public Policy Overview page of the APIC website.
Within the “what’s new” page explanation, there is a link to join the Action E-List.
The link will open a webpage that allows a user to enter basic information before joining the Action E-List. Additional APIC information is helpful but not required. Managing your Action E-List subscription is also available at this site.

2/26/2015
14
• The library can be used to share documents and contains previous CLR presentations.
• This is where members can post questions, share experiences and discuss regulatory/legislative issues.
• Events can be posted here.
• Announcements will be posted here.
CLR Community on MyAPIC
Additional Public PolicyResources
2/26/2015
15
Additional Public Policy Resources
• “What’s New” Page
• Presentation-Ready Maps• CRE• HAI• MRSA• Long-term Care• Ambulatory Care
• Accessing APIC Regulatory Comments
• Public Policy Position Statements
Chapter Presentation Slides

2/26/2015
16
• latest addition to APIC Government Affairs resources for CLRs
• intended for CLR to present Public Policy Information to chapter (approximately 10-12 slides)
• federal issues• issues under Public Policy
Committee review
• available in the document section of the MyAPIC CLR community
• store in the CLR manual under “Chapter Presentation Slides”
VIP Chapter Presentation Slides
Federal Regulations

2/26/2015
17
Key Federal Legislative Actions on HAIs
Deficit Reduction Act Enacted‒ HAC Policy to impact 2008 payment– Uses funding as incentive for quality improvement
House Committee and GAO Issues Report on Need for H AI Coordination
American Recovery and Reinvestment Act (ARRA) – Grants to States for HAI Coordinators and activities
Omnibus Appropriations Act– States to develop HAI Plans (or lose block grant funds)
National Action Plan to Prevent HAIs – Response to Congressional Hearing and GAO report– Plan to better coordinate federal HAI activities
Affordable Care Act (Obamacare)– Required HAI reporting as part of healthcare quality improvement
programs
2008
2009
2010
2006
CMS Hospital Quality Improvement Programs
• Hospital-Acquired Conditions (HAC)/ Present on Admission (POA) indicators
• Hospital Inpatient Quality Reporting (IQR) Program
• Hospital Value-Based Purchasing (VBP) Program
• HAC Reduction Program (coming in FY 2015)

2/26/2015
18
• Non-reimbursement policy (impacted payment in beginning October 2008)
• Prohibits reimbursement of designated HACs that wer e not present on admission
• HAI-HACs include vascular catheter-associated infections; CAUTI; and SSIs following coronary arte ry bypass graft, certain orthopedic procedures, bariat ric surgery for obesity and cardiac implantable electr onic device
• HACs identified through claims data
Hospital-Acquired Conditions (HAC)Non-reimbursement policy
2011
• CAUTI – Acute Care ICUs (except NICUs) (Jan.) • CAUTI – LTCH, IRF, Cancer Hospitals (Oct)• SSI – Colon Surgeries and Abdominal Hyst.– Acute Care (Jan)• Dialysis Events – ESRD (Jan)• CLABSI – LTCH, Cancer Hospitals (Oct)
2012
• HCP Influenza Vaccination – ASCs/Hosp. Outpt. Depts. (Oct.) • SSI – Cancer Hospitals (Jan.)• HCP Influenza Vaccination – IRF (Oct.)
• CLABSI – Acute Care ICUs (Jan.)
• C. Diff – Acute Care (Jan.)• MRSA Bacteremia – Acute Care (Jan.) • HCP Influenza Vaccination – Acute Care (Jan.)• HCP Influenza Vaccination – LTCH (Jan.)
• CLABSI – Acute Care Med, Surg, Med/Surg Units (Jan.) • CAUTI – Acute Care Med, Surg, Med/Surg Units (Jan.)• MRSA Bacteremia – LTCH (Jan.), IRF (Jan.) • C. Diff – LTCH (Jan.), IRF (Jan.) • HCP Influenza Vaccination – Inpt. Psych. Fac. (Oct.)
Federal HAI Reporting to NHSN for CMS Quality Reporting Programs
• VAE – LTCH (Jan.)
Reporting Payment
2013
2014
2015
2016
2013
2014
2015
2016
2017
2018

2/26/2015
19
• 2010 - Established by the Affordable Care Act as incentive program to improve quality of healthcare.
• FY 2013 – first year of payment adjustments under the VBP program
• FY 2015 – first year NHSN-reported HAIs included in VBP program
Hospital Value-Based Purchasing (VBP) Program
• Total Performance Score – determined by hospital’s achievement and improvement compared to a 9-month baseline period.
– Penalty for poor performance– Hospitals that rank in the lowest-performing quarti le
of HACs receive a 1% penalty– Payment adjustment to account for HACs with
discharges beginning October 1, 2014 (FY 2015)– Total HAC score based on measures in 2 domains :
– Domain 1 includes certain AHRQ Patient Safety Indicators (determined by claims data)
– Domain 2 consists of HAI measures reported through NHSN
Hospital-Acquired Condition (HAC) Reduction Program

2/26/2015
20
• CLABSI (ICU)– NHSN reporting began 2011
– CMS payment for reporting began FY 2013
– Added to VBP beginning with FY 2015 payment
– Added to HAC Reduction Program beginning FY 2015
• CLABSI (medical, surgical, med/surg wards)– NHSN reporting begin 2015
– CMS payment for reporting begin FY 2017
Acute Care Payment Program Measures
• CAUTI (ICU)– NHSN reporting began 2012
– CMS payment for reporting began FY 2014
– Added to VBP beginning with FY 2016 payment
– Added to HAC Reduction Program beginning FY 2015
• CAUTI (medical, surgical, med/surg wards)– NHSN reporting began 2015
– CMS payment for reporting begin FY 2017
Acute Care Payment Program Measures

2/26/2015
21
• Surgical Site Infection following colon surgery/ ab dominal hysterectomy– NHSN reporting began 2012
– CMS payment for reporting began FY 2014
– Added to VBP FY 2016 payment
– Added to HAC Reduction Program FY 2016 payment
• MRSA Bacteremia LabID Event– NHSN reporting began 2013
– CMS payment for reporting began FY 2015
– Added to VBP FY 2017 payment
– Added to HAC Reduction Program FY 2017 payment
Acute Care Payment Program Measures
• C. difficile Infection LabID Event– NHSN reporting began 2013
– CMS payment for reporting began FY 2015
– Added to VBP FY 2017
– Added to HAC Reduction program FY 2017
• HCP Influenza Vaccination– NHSN reporting began 2013
– CMS payment for reporting began FY 2015
– Later revised to coincide with flu season – data collection October 1 –March 31; single report to NHSN by May 15 of year season ends
Acute Care Payment Program Measures

2/26/2015
22
• PPS-Exempt Cancer Hospital Quality Reporting Progra m (PCHQRP)– CLABSI (2012), CAUTI (2012), SSI -COLO, AB/HYST (2014)
• Long-Term Care Hospital Quality Reporting Program ( LTCQRP)– CLABSI (2012) , CAUTI (2012), HCP flu vaccination (2013), MRSA (2015), C.diff.
(2015), VAE (coming 2016)
• End-Stage Renal Disease (ESRD) Quality Incentive Pr ogram– BSI in outpatient hemodialysis, HCP flu vaccination (2015-16 flu season)
• Hospital Outpatient Quality Reporting Program• HCP flu vaccination (2014-15 flu season)
• Ambulatory Surgical Center Quality Reporting Progra m (ASCQRP)• HCP flu vaccination (2014-15 flu season)
• Inpatient Rehabilitation Facility (IRF) Quality Rep orting Program– CAUTI (2012), HCP flu vaccination (2014), MRSA (2015), C.diff (2015)
• Inpatient Psychiatric Facility (IPF) Quality Report ing Program– HCP flu vaccination (2015-16 flu season)
Quality Programs Outside of Acute Care
• CDC– Focus: Evidence-based guidelines for infection prevention and
control practice
• OSHA– Focus: Worker safety– Examples: Bloodborne Pathogens Standard, Respiratory Protection
Standard, considering possible Infectious Disease Standard
• FDA– Focus: Regulation of drugs; medical devices; human blood, tissue
and cell products
• EPA– Focus: Regulation of disinfectants and sterilants; medical waste
incinerators
• State and local health departments
Other Agencies Regulating Infection Prevention

2/26/2015
23
Federal Legislation
Centers for Disease Control and Prevention (CDC)• $32 million for NHSN and the Prevention Epicenters Program• $30 million for Advanced Molecular Detection (AMD) and response to infectious
diseases program• $500 million Core Infectious Diseases, which would include funding for:
− HAIs− Antimicrobial Resistance− Emerging Infections Program (EIP)
• $264 million Antibiotic Resistance Solutions initiative
Agency for Healthcare Research and Quality (AHRQ)• $10 million for HAI research grants• $4 million for HAI contracts including the Comprehensive Unit-Based Safety
Program (CUSP)
National Institutes of Health (NIH)• $4.6 billion for the National Institute of Allergy and Infectious Diseases’ (NIAID)
antibacterial and related diagnostics efforts
Funding for federal programs

2/26/2015
24
Antibiotic resistance
Federal antibiotic resistance initiatives include:
• Antibiotic Resistance Solutions Initiative− Would establish State AR
Prevention programs− Would create new AR isolate bank
and network of regional laboratories− Would provide real-time data on
antibiotic use and resistance trends using NHSN
• 21st Century Cures legislation− Would allow a limited population
approval pathway for antibacterial drugs
− Would provide for higher Medicare reimbursement of certain antibiotic drugs
State Legislation

2/26/2015
25
Pending state legislation
Immunization• WV HB 2556 and SB 286 – Would allow medical and personal exemptions from mandatory
immunizations for school children.• MN HF 393 and SF 380 – Would require education from a physician on the risks and benefits
of vaccination prior to receiving an exemption from school immunizations requirements.
Quarantine• NM SB 362 – Would establish protocols for the New Mexico Department of Health to place
individuals under quarantine.• TX SB 538 - Would allow the Governor to declare a state of infectious disease emergency
and establishes procedures for the Texas Department of State Health Services to place individuals under quarantine.
• MN HF 22 – Would establish financial protections for individuals under quarantine, including requiring the state/employer to cover any lost income.
Malpractice• NY AB 1124 – Would allow an individual who contracts an HAI to bring a cause of action for
injuries suffered as a result of the infection pursuant to the statute of limitations.
Looking ahead: NHSN State Competition
The NHSN competition is on!
APIC is supporting the President’s budget request of $32 million for NHSN and the Prevention EpiCenters.
APIC will soon be asking members to send a letter to Members of Congress supporting funding for NHSN and other federal infection prevention programs. The state with the highest percentage of letters sent will win a prize!
Alert your chapter today!

2/26/2015
26
Lisa Tomlinson, MA, Vice President of Government Af fairs and Practice [email protected]• Overall government affairs and practice guidance st rategy
Nancy Hailpern, Director of Regulatory [email protected]• Federal regulatory issues• HAI reporting at the federal level
Laura Evans, Legislative Affairs [email protected]• Federal and state legislation• Legislative maps
Questions?
When in doubt, e-mail: