gotta go? urinary incontinence in the elderly
TRANSCRIPT

1
GottaGo?UrinaryIncontinence
intheElderly
Stephanie Sibicky,PharmD, BCGP, BCPS
NortheasternUniversityBouvéCollegeofHealthSciences|SchoolofPharmacy
ClinicalPharmacist– IntegratedTeachingUnitBrighamandWomen’sHospital
Objectives• Discuss theetiologyand pathophysiology of urinaryincontinence (UI).
• Evaluatepharmacologic and non-pharmacologic treatmentoptions for urinaryincontinence.
• Createpatient-specific recommendations forthetreatmentof urinaryincontinence based onavailableefficacy andsafetydata.
Epidemiology
0%
20%
40%
60%
80%
CommunityregularUI
CommunityanyUI
CommunityanyUI
Communityfrailoracutehospital
Nursinghome
%prevalence
♂♀
2.5Xmorecommon inwomen
Adapted from Essentials ofClinicalGeriatrics ,2013.

2
Consequences ofIncontinence
MedicalRiskofcystitis,urosepsis,
pressure sores,perineal rashes,
sleepdisturbances,
dehydration, falls
PsychosocialEmbarrassment,
isolation,depression,
predispositiontoinstitutionalization
EconomicCostofsupplies,medications,homehealthaide/care at
home,nursingfacility
TheAgingUrinaryTractPhysiologic Change ResultsIn…
↓bladder elasticity Lesscapacityforvolume
↑residualvolume Incompleteemptying
↑nocturnalsodiumandfluidexcretion Nighttimeawakeningtourinate
↑urethralresistance(men) Weakstream,difficultyurinating
↓urethral resistance(women, ↓estrogen) Urgency,goingtoomuch
Weakened pelvicfloormuscles Increasedpressureonthebladder
↑involuntarybladdercontractions Urgency,gottogoNOW!
Allcontribute,butnonealoneprecipitates incontinence
Anatomy&Pathophysiology
Ureters
DetrusorMuscle
ExternalSphincter
InternalSphincter
ParasympatheticNervousSystemSympathetic
NervousSystem(α-adrenergic)
BladderNeck
SomaticNervousSystem
Capacity ≈300ml

3
Pathophysiology:StoragePhase
Ureters
ExternalSphincter
InternalSphincter
ParasympatheticNervousSystemSympathetic
NervousSystem(α-adrenergic)
BladderNeck
SomaticNervousSystem
InhibitorySignal fromCortex
CONTRACTION(Closed) CONTRACTION
(Closed)
BladderFilling
DetrusorMuscle
RELAXATIONβ3
Pathophysiology:VoidingPhase
Ureters
DetrusorMuscle
ExternalSphincter
InternalSphincter
ParasympatheticNervousSystemSympathetic
NervousSystem(α-adrenergic)
BladderNeck
SomaticNervousSystem
InhibitorySignal fromCortexCONTRACTION
MICTURITION
RELAXATION(Open) RELAXATION
(Open)
AChM3
Pathophysiology:Summary
Picture credit: http:/ /sketchymedicine.com/2011/10/neural-control-of-micturitio n/

4
Evaluation&DiagnosisHISTORY
• Symptoms (onset, type,frequency, timing)
• Bladder record• Comorbidities,lifestyle,
medications, environment• Patient perception of
incontinence
PHYSICAL
• Mobilityissues• Gynecologicalandurological
evaluation• Tests
– Catheterizationorbladderultrasound (residualvolumes)
– Cystoscopyandflowstudies– Urinarystress test– UAandurinecultures– Bloodchemistries– Renal function– Postprandialglucose
GoalsofTherapy• Minimizesignsandsymptomsmostbothersometothepatient1. Non-pharmacologictechniques2. Medications3. Surgicalintervention
• Setrealistic expectations– Totaleliminationofsymptomsmaynotbefeasible– Communicatemostcommonsideeffects– Balancepatientgoals,expectations,andrisks
Classification:Acute/Transient• Recentonset• Associatedwithacutemedicalproblem– Heartfailure– Acuteconfusionoralteredmentalstatus– Surgicalprocedures

5
ReversibleCauses• Delirium or Dementia• Infections• Atrophic vaginitis,urethritis, atonic bladder• Psychologicalor Pharmaceuticals• Endocrine (diabetes, hypothyroidism) or Excessiveurine output/fluid intake
• Restrictedmobility or Retention• Stoolimpaction
Medication-InducedIncontinence
ACE(angiotens ion–convertingenzyme);NSAIDs(non-steroidalantiinflammatorydrugs)
Stress• α-blockers • Atypicalantipsychotics• ACE inhibitors
Urge• Antidepressants • Hormonereplacement• 5HT4-agonists• Directorindirectparasympathomimetics(cholinesteraseinhibitors)
Overflow• Anticholinergics • α-agonists• Antiparkinson drugs • Opioids• β-blockers • Calciumchannelblockers
Functional• H1-antagonists • Opioids• Antipsychotics • Alcohol• Benzodiazepines
IncreaseUrine
Production
• Diuretics • Thiazolidinedione• Lithium • Musclerelaxants• NSAIDs • Alcohol
TreatmentofAcute/TransientUI• Identifyandtreatunderlying cause• Treatsymptomsandpatientneeds• Remove,reduce,substitute offendingmedication• Attendtosurgicalcomplication, impaction, etc.• Improvemoodandmentalstatus• Antibiotics forinfection orvaginitis

6
CaseBW• BWisa72-year-oldfemalewhopresentstotheclinic complaining ofincreasedfrequency (every2hours), urgency,andmoderateleakage
• PMHincludes diabetes,uncontrolledhypertension, osteoporosis, andhypothyroidism
• Medicationsinclude metformin, HCTZ,amlodipine, calcium +vitaminD,andlevothyroxine
• Whenaskingherabout OTCuse,shementionsneedingtotakeMiralaxdaily
CaseBW,cont.Afterremovingthepotential acutecausesofUI,BWcontinues tohavesymptoms.Shementionsthatshehasleakagewhenshesneezesandoftenneedsto“racetotheladiesroom”throughout theday.
HowwouldyouclassifyBW’sincontinence?
a) Urgeb) Stressc) Overflowd) Mixed
Classification:Chronic/PersistentUrge Stress Overflow Functional
Cause Detrusormuscleoveractivity
Weakenedpelvicfloormuscles
Bladderdistension duetoobstruction(BPH,fecalimpaction)
Underlyingphysicalormental
impairmentimpactingability
totoilet
CommonSymptoms
Urgencywithorwithout
incontinence,frequency,nocturia orenuresis
Incontinencewithcoughing,
sneezing,laughing,exercise,
activitiesthatincreaseabdominalpressure,frequency
Incompletevoiding,
frequency,urgency,hesitancy,abdominalfullness,straining
Incontinence–looks likeurge
Mixed =usuallycombinationofurgeandstress incontinence

7
UrgeUrinaryIncontinence(UUI)• Involuntaryvoidingpreceded byabriefwarning• Causes:– Detrusormuscleinstability(involuntarycontraction)
– Twohypotheses• Neurogenic• Myogenic
• Overactivebladder(OAB)– Syndromeincludingurgency,frequency,andnocturia
–Withorwithout urgeincontinencePicture credit: http:/ /sketchymedicine.com/2012/02/stress -urge-overflow-and-mixed-incontinence/
UUITreatmentStrategy• Identifyandmitigateanyreversiblecauses
• Non-pharmacologic– Lifestyle(e.g.,diet,behavior)– Surgical
• Pharmacologic– Expectationof4-6weekresponse– Ifnoresponse,canswitchtoanotheragentinsameclass
• Diet(monitoring fluid,caffeine,bladder irritants)• Exerciseandweight loss• Smokingcessation• Schedulingregimens:– Timedvoiding– Bladdertrainingandscheduling
• Musclerehabilitation:– Pelvicfloormuscleexercises(e.g.,Kegelexercises)– Biofeedback,electricalstimulation– Acupuncture
• External urinecollection(menonly)• Surgery
Non-pharmacologic TreatmentofUUI
Subak LLetal.NEJM. 2009;360(5):481-90.Dallosso HM et al.BJU Int. 2003;92(1):69-77.
Dumoulin C etal.Cochrane Database SystRev. 2014; May 14;(5):CD005654.
8
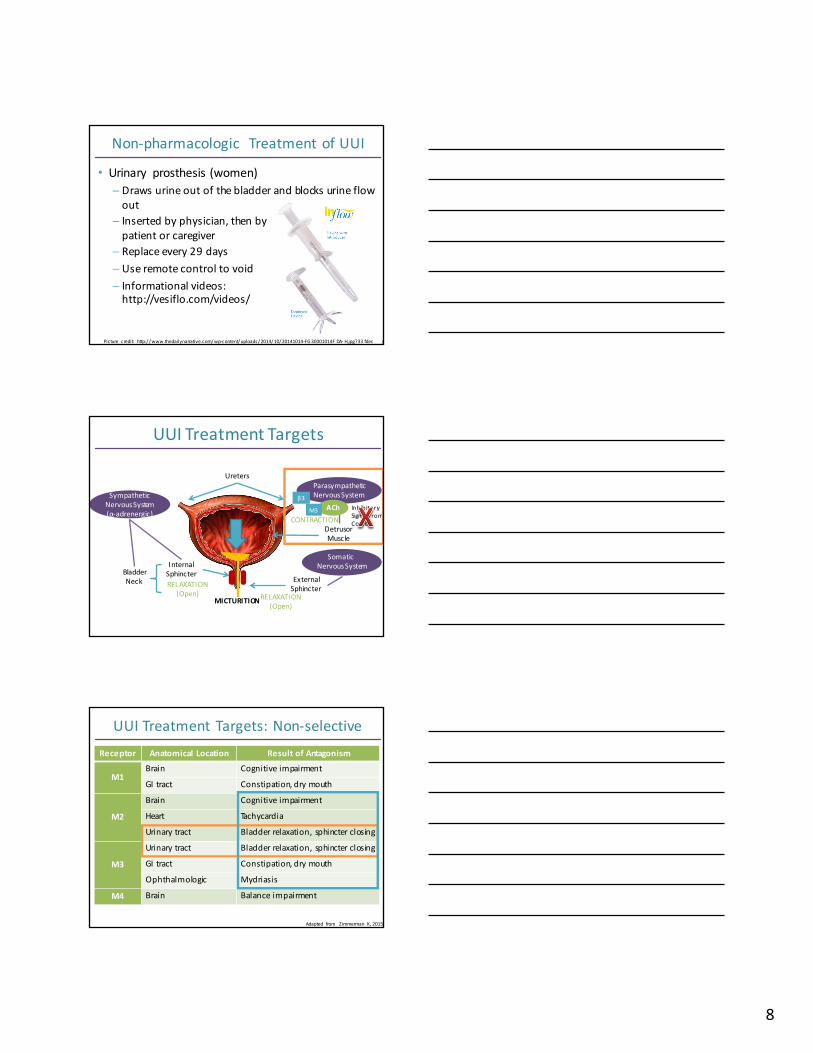
Non-pharmacologic TreatmentofUUI
• Urinary prosthesis(women)– Drawsurineoutofthebladderandblocksurineflowout
– Insertedbyphysician,thenbypatientorcaregiver
– Replaceevery29days– Useremotecontroltovoid– Informationalvideos:http://vesiflo.com/videos/
Picture credit: http:/ /www.thedailynarrative.com/wp-content/uploads/2014/10/20141014-FG30001014F DA- H.jpg?33 fdec /
UUITreatmentTargets
Ureters
DetrusorMuscle
ExternalSphincter
InternalSphincter
ParasympatheticNervousSystemSympathetic
NervousSystem(α-adrenergic)
BladderNeck
SomaticNervousSystem
InhibitorySignal fromCortexCONTRACTION
MICTURITION
RELAXATION(Open) RELAXATION
(Open)
AChM3
β3
UUITreatmentTargets:Non-selectiveReceptor Anatomical Location ResultofAntagonism
M1Brain Cognitiveimpairment
GItract Constipation,drymouth
M2
Brain Cognitiveimpairment
Heart Tachycardia
Urinary tract Bladderrelaxation, sphincterclosing
M3
Urinary tract Bladder relaxation,sphincter closing
GItract Constipation,drymouth
Ophthalmologic Mydriasis
M4 Brain Balance impairment
Adapted from Zimmerman K,2015.

9
UUITreatment:Anticholinergics• Reducecholinergic transmissiontobladder,inhibit involuntarydetrusor contraction, increasebladder capacity,decreasefrequencyofurination
• Sideeffects:drymouth, visualdisturbances,constipation, dryskin
• Precautions – arrhythmias, cardiovasculardisease,GImotilityissues,dementia, andelderly
• Contraindications – GIobstruction, closedandnarrowangleglaucoma
UUITreatment:Efficacy• Anticholinergics haveamodestbenefit overplacebo– Reductionin0.6episodes/day– 50%ofpatientsstillunhappyorfrustratedwithsymptomsaftertreatment
• 60-70%ofwomendiscontinue within 6months• Similarefficacybetweenagentsalthough limitedhead-to-head trialsbetweenagents
• Extended-release agentshavelowerratesofadverseeffectsthanimmediatereleaseagents
ShamilyanTet al.AnnIntern Med.2012;156(12):861.AHRQ 2012. Availableathttp:/ /effectivehealthcare.ahrq.gov/ehc/products/169/1021/CER36_Urinary-
Incontinence_execsumm.pdf
Non-selectiveAnticholinergicsMedication Formulations AdverseEffects AdditionalCommentsOxybutynin IRtablets(Ditropan®) MOST Referencestandard
GradualdoseescalationERtablets(DitropanXL®) BettertoleratedthanIRPatch(Oxytrol®) OTCforwomenonly
Bypasses1stpassGel(Gelnique®) Bypasses1stpass
Tolterodine IRtablets(Detrol®) CYP2D6 >CYP3A4metabolismRenaldoseadjustments
ERcapsules (Detrol®LA) BettertoleratedthanIRFesoterodine ERtablets(Toviaz®) Adjustmentsforrenal
impairmentand3A4inhibitorsTrospium IRtablets (Sanctura®) Dose adjustmentforCrCl<30
ml/minERtablets (SancturaXR®)
LEASTBettertoleratedthanIRAvoidin renalimpairment

10
UUITreatmentTargets:SelectiveReceptor Anatomical Location ResultofAntagonism
M1Brain Cognitiveimpairment
GItract Constipation,drymouth
M2
Brain Cognitiveimpairment
Heart Tachycardia
Urinary tract Bladderrelaxation, sphincterclosing
M3
Urinary tract Bladder relaxation,sphincter closing
GItract Constipation,drymouth
Ophthalmologic Mydriasis
M4 Brain Balance impairment
SelectiveAnticholinergicsSolifenacin
• IRtablets (Vesicare®)• M3selectivity > M2• Efficacy
– Non-inferior tooxybutynin IR– Superior to tolterodine IR
• Side effects:– Less thanoxybutynin and
tolterodine– More thandarifenacin
• Maximum 5mg/day– Renal impairment (CrCl<30)– Moderate andseverehepatic
impairment
Darifenacin• ERtablets (Enablex®)• Truly selective forM3• Efficacy
– Non-inferior tooxybutynin IR– Moreeffective than
tolterodine IRat12weeks• Lessside effects than
oxybutynin• Norenal doseadjustment• Hepatic impairment
– Moderate –max7.5mg/day– Notevaluated in severe
Mirabegron: β-agonist• ERtablet(Myrbetriq®)• Reducesbladder contractions viarelaxation ofdetrusor musclethrough β3-agonism
• Efficacyin4-8weeks,reduction in0.5episodes/dayat50mgdose
• Maximum25mg/dayifCrCl<30ml/min• Sideeffects:hypertension, nasopharyngitis, UTI,constipation, tachycardia,headache

11
OtherPharmacologicTreatment• Tricyclic Antidepressants (e.g.,imipramine)– Increasesbladdercapacityandoutletresistance,anticholinergicproperties
– Sideeffects:weakness,fatigue,posturalhypotension,hipfractures
• Botox® (onabotulinumtoxinA)–Muscleparalyticwheninjectedintodetrusormuscle– ApprovedJanuary2013– Injectedinto20sitesviaurethraevery12weeks– Decreases1.6-1.9episodes/day
CaseBW,cont.Besidesnon-pharmacologic options, which
treatmentforurgeUIwouldbemostappropriateforBW?
a) Mirabegronb) OxybutyninIRc) Darifenacind) TolterodineLA
StressUrinaryIncontinence(SUI)• Involuntaryleakageduetoincreasedintra-abdominalpressure thatovercomesurethralresistance
• Causes–Weakpelvicfloormuscles– Sphincterincompetence– Trauma/damage tourethra–Women>>>Men
Picture credit: http:/ /sketchymedicine.com/2012/02/stress -urge-overflow-and-mixed-incontinence/

12
StressUrinary Incontinence Triggers
Pictu recred i ts:h ttp ://www.heal th .com/heal th /gal lery/0 ,,20 35 82 79 _2 ,0 0.html ;h ttp ://assets.n ydai lynews.com/po lopo ly_fs/1 .16 68 83 .1 31 40 26 304 !/img/h ttp Image/image.jp g_gen /derivatives/land scape_6 3 5 /alg-lau gh in g-jp g.jp g
h ttp ://img.webmd .com/d tmcms/l ive/webmd/con sumer_assets/si te_images/articles/heal th _too ls/in con tin en ce_in _women_sl id eshow/getty_rm_ph o to_o f_woman_after_sneezin g.jp g
Non-Pharmacologic Treatment forSUI
Pelvicfloormuscletraining Pessaries
Bladder
Uterus
Picture credit: http:/ /1qghdw20tywd2qc5uw1w82ap-wpengine.netdna-ss l.com/wp-conten t/uploads/2016/09/vagina.jpg;http:/ /2nznub4x5d61ra4q12fyu67t.wpengine.netdna -cdn.com/ img/54645e rt.jpg
http:/ /www.seekwellness .com/mystore/products_pictures/stepfree%20weights .jpghttp:/ /mciverclinic.com/ images/uploads/pessary.jpg
PharmacologicTreatmentforSUI• Noagent isFDAapprovedforthetreatment ofSUIintheUnitedStates
• Duloxetine(Cymbalta®)– Serotoninandnorepinephrinereuptakeinhibitor
• Involvedincontrolofurethralsmoothmuscleincatsandrats• Facilitatespathwaybetween bladderandsympatheticnervoussystem• Increasessphinctertoneduringstoragephase
– Off-label inUSduetotosuicidalideation,indicatedinUK– Sideeffects(diminishwithtime):nausea,drymouth– Olderadultsunderrepresentedinstudies
GOALIncreasecontractionandtoneof
urethralsphincter
Cardozo Letal.Curr Med Res Opin.2010;26(2):253-61.

13
PharmacologicTreatmentforSUI• α-Adrenergicagonists– Pseudoephedrine,phenylephrine– Cautioninelderlyduetosideeffects– Contraindicatedinhypertensionorobstruction
• Topicalestrogen(creams,vaginaltablets,rings)– SUI+vaginitisorurethritisduetoestrogendeficiency
– NOsystemictherapy– Usedincombinationwithα-agonists
• ImipramineMalallahMA et al.IntUrogynecolJ. 2015;26(4):477-85.
CodyJD et al.Cochrane DatabaseSystRev.2012 Oct17;10:CD001405.
MixedUrinaryIncontinence
URGE
STRESS
Picture credit: http:/ /sketchymedicine.com/2012/02/stress -urge-overflow-and-mixed-incontinence/
TreatmentofMixedUI• Initialtherapydependsonpredominatesymptoms
• Canusecombination oftreatmentstrategiesforUUIandSUIintheabsenceofobstruction– Pelvicfloormuscletrainingandbladdertraining– Behavioralinterventions–Medications

14
OverflowUrinary Incontinence (OUI)
• Volumeofurineinbladder overcomes closingpressure
• Symptoms:– Diminishedstream– Strainingtovoid– Senseofincompleteemptying
• Causes:– Neurogenicbladder– Atonicbladder– Obstruction(BPH,strictures,neuropathy,impaction)
‒ Interruptedflow‒ Hesitancy
Picture credit: http:/ /sketchymedicine.com/2012/02/stress -urge-overflow-and-mixed-incontinence/
TreatmentofOUINon-pharmacologic
• Obstruction removal(surgery)
• Bladder training andvoidingschedule
• Catheterization– Self-catheterization 3-4x/day– Surgicallyplaced
Pharmacologic
• Bethanechol (Urecholine®)– Cholinomimetic– SEs:muscle cramping,
diarrhea– Cancause life threatening
ADE inasthmaorheartdisease
• αA1-receptor antagonists– Locatedinbladder neck,
urethra, andperiurethraltissues
– TreatmentofBPH inmen– Use inwomen forthis reason
FunctionalIncontinence• Personisunableorunwilling toreachthetoilet• Causes:–Musculoskeletaldisorders/weakness– Disabilities,visionloss– Cognitiveimpairment– Physicalrestraints– Psychologicalimpairments– Environment–Medications(e.g.,sedatives,neuroleptics)

15
TreatmentforFunctionalUI• Scheduledorprompted toileting• Removalofbarriers andobstacles• Physicaltherapy• Assistivedevices– Bedsidecommode– Urinals– Elevatedtoiletseats
CaseBW,cont.Afterremovingthepotential acutecausesofUI,BWcontinues tohavesymptoms.Shementionsthatshehasleakagewhenshesneezesandoftenneedsto“racetotheladiesroom”throughout theday.
HowwouldyouclassifyBW’sincontinence?
a) Urgeb) Stressc) Overflowd) Mixed
ChoosingPharmacologicTherapy
MosthavesimilarefficaciesNewisnot
alwaysbetter!!!
Considersymptoms,
comorbidities,drug
interactions,sideeffects,etc.
Formularyrestrictionandinsurancecoverage
16
TreatmentApproachinElderly• Determine ifthereisanotherunderlying cause• Anticholinergics areon2015BeersCriteria tobeavoidedinelderlywith dementiaorcognitiveimpairment
• Startlowandgoslow– Doseadjustforrenalandhepaticimpairment– Titrationbasedonsideeffectsandtolerability
• Trialofoneagentforupto2months• Consider switchtoanother agentifnoimprovementandtreatmentisstillnecessary
JAm Geriatr Soc63:2227–2246, 2015.
CounselingTips• Reduceintakeoffluidduring theday,especiallyintheevening(after6pm)
• Avoidcaffeinatedbeverages• Minimizetheuseofartificial sweeteners,acidicandspicyfoods
• Letyourpharmacist knowaboutnewmedicationsyouaretakingtoseeiftheycontribute toyoursymptoms
CaseBW,cont.Fourweeksafterstartingdarifenacin, BWreturns totheclinic becausethismedication isnot working.Shehasseencommercialsforanewmedicationcalled“Mybearstricks”andasksifthisisabetteroptions.Herblood pressuretodayis122/78.
Howwouldyouproceed?
a) Checkwithherinsurancefirsttoseeifitiscoveredb) Counselherthataneffectcantakeupto2monthsc) Recommendaswitchtosolifenacininstead

17
TakeHomePoints• UIisaprevalentcondition withthepotential tohaveasignificantimpactonolderadults
• TreatmentforUIshould include non-pharmacologic approachesbeforeinitiatingpharmacologic agents
• Efficacy,adverseevents,andpatientpreferenceneedtobeconsidered whendevelopingatreatmentplan
• Pharmacistscanmonitor forefficacyandhelpmitigateadverseeffectsforpatientswithUI
References• Subak LL,Wing R,West DS, et al. PRIDE Investigators. Weight loss totreat urinary
incontinence inoverweight and obese women. NEngl J Med. 2009Jan29;360(5) :481-90.doi: 10.1056/NEJMoa0806375.
• Dallosso HM,McGrother CW, Matthews RJ,et al. Leicestershire MRC Incontinence StudyGroup. The association of dietand otherlifestyle factorswithoveractive bladder and stressincontinence: a longitudinal studyinwomen. BJUInt. 2003Jul;92(1) :69-77.
• Dumoulin C,Hay-Smith EJ, Mac Habée-Séguin G. Pelvic f loormuscle training versus notreatment, orinactive controltreatments, forurinary incontinence inwomen. CochraneDatabase Syst Rev. 2014May 14;(5) :CD005654.doi:10.1002/14651858.CD005654.pub3.
• Qaseem A, Dallas P,Forciea MA, et al; Clinical Guidelines Committee of the AmericanCollege of Physicians. Nonsurgical management of urinary incontinence inwomen: a clinicalpractice guideline fromthe American College of Physicians. Ann InternMed 2014:161:429-440.
• CodyJD, JacobsML, Richardson K,et al. Oestrogen therapy forurinaryincontinence in post-menopausal women. Cochrane Database Syst Rev. 2012Oct17;10:CD001405.doi:10.1002/14651858.CD001405.pub3.
• Richter HE, BurgioKL, Brubaker L, et al. Pelvic Floor Disorders Network. Continence pessarycompared withbehavioral therapy orcombined therapy forstressincontinence: arandomized controlled trial. Obstet Gynecol. 2010Mar;115(3) :609-17.doi:10.1097/AOG.0b013e3181d055d4.
References• CardozoL, Lange R, VossS, et al. Short- and long-term eff icacy andsafety of duloxetine in
women withpredominant stress urinary incontinence. CurrMed Res Opin. 2010Feb;26(2) :253-61.doi:10.1185/03007990903438295.
• Malallah MA, Al-Shaiji TF. Pharmacological treatment of purestress urinary incontinence: anarrative review. IntUrogynecol J.2015Apr;26(4) :477-85.doi:10.1007/s00192-014-2512-9.Epub2015Jan29.
• ReynoldsWS, McPheeters M, Blume J, etal. Comparative Effectiveness of AnticholinergicTherapy forOveractive Bladder inWomen: A Systematic Review andMeta-Analysis. ObstetGynecol. 2015 Jun;125(6) :1423-32.doi:10.1097/AOG.0000000000000851.
• Shamliyan T, Wyman JF, Ramakrishnan R,et al. Benef its andharms of pharmacologictreatment forurinaryincontinence inwomen: a systematic review. AnnInternMed. 2012Jun;156(12):861-74.
• Effective Health Care Program. Nonsurgical Treatments forUrinary Incontinence inAdultWomen: Diagnosis and Comparative Effectiveness. Agency forHealthcare Research Quality2012.Available at:http://effectivehealthcare.ahrq. gov/ ehc/products/169/1021/CER36_Urinary-Incontinence_execsumm.pdf (Accessed onNovember 19, 2012).
• Solifenacin and darifenacin foroveractive bladder. Obstet Gynecol. 2005Aug;106(2) :401-2.• Campbell SE, Glazener CM, HunterKF, etal. Conservative management for
postprostatectomy urinary incontinence. Cochrane Database Syst Rev. 2012Jan18;1:CD001843.doi:10.1002/14651858.CD001843.pub4.Review.Update in: CochraneDatabase Syst Rev. 2015;1:CD001843.
18
QUESTIONS?
Thank [email protected]
GottaGo?UrinaryIncontinence
intheElderly
Stephanie Sibicky,PharmD, BCGP, BCPS
NortheasternUniversityBouvéCollegeofHealthSciences|SchoolofPharmacy
ClinicalPharmacist– IntegratedTeachingUnitBrighamandWomen’sHospital