good use of biotests in emergency dr. david tran fvhospital 28 april 2010
TRANSCRIPT

Good use of biotests Good use of biotests in emergencyin emergency
Dr. David TranDr. David Tran
FVHospitalFVHospital
28 April 201028 April 2010

Interest of a biotestInterest of a biotest
Can help the clinician to confirm or rule out a Can help the clinician to confirm or rule out a
diagnosis (troponine, lipase, AgNS1, d.dimeres)diagnosis (troponine, lipase, AgNS1, d.dimeres)
Can help the clinician to evaluate the general Can help the clinician to evaluate the general
condition of a patient (uree, creatinine, proteine)condition of a patient (uree, creatinine, proteine)
Can help the clinician to evaluate the seriousness Can help the clinician to evaluate the seriousness
of the illness (CRP, WBC, blood gaz)of the illness (CRP, WBC, blood gaz)

Drawback of a biotsetDrawback of a biotset
Blood test > disturbance for the patient (child) Blood test > disturbance for the patient (child)
Increase the cost of cares.Increase the cost of cares.
Sometime difficult to perform (ECBU, blood gaz)Sometime difficult to perform (ECBU, blood gaz)
Increase the waiting time (2h for blood test)Increase the waiting time (2h for blood test)
Sometime difficult to interpret (d.dimeres, BNP)Sometime difficult to interpret (d.dimeres, BNP)
The right questions before asking The right questions before asking for a biotestfor a biotest
Is-it really useful? Is-it really useful?
Do I need this test in emergency?Do I need this test in emergency?
Will the result modify the management of this Will the result modify the management of this
patient?patient?
Is it the right moment to ask for this test Is it the right moment to ask for this test (troponine, (troponine,
NS1 Ag)NS1 Ag)
What is the probability to have an abnormal result?What is the probability to have an abnormal result?
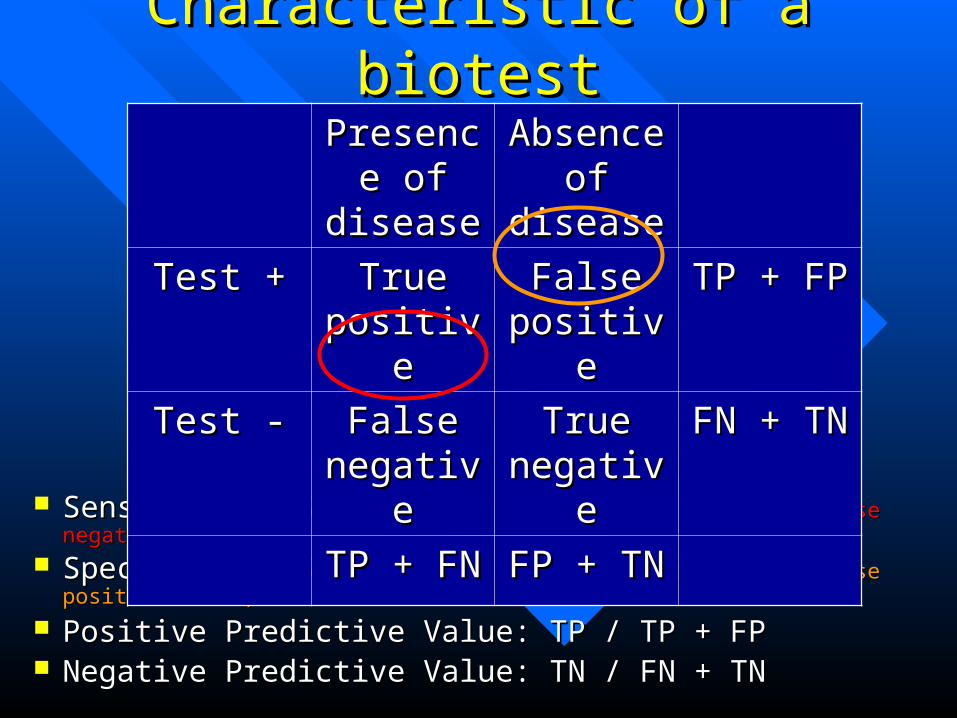
Characteristic of a biotestCharacteristic of a biotest
Sensitivity: Se = TP / TP + FN Sensitivity: Se = TP / TP + FN (Good Se = law false negative value)(Good Se = law false negative value)
Specificity: Sp = TN / FP + TN Specificity: Sp = TN / FP + TN (Good Sp = law false positive value)(Good Sp = law false positive value)
Positive Predictive Value: TP / TP + FPPositive Predictive Value: TP / TP + FP Negative Predictive Value: TN / FN + TN Negative Predictive Value: TN / FN + TN
Presence Presence of diseaseof disease
Absence Absence of diseaseof disease
Test +Test + True True positivepositive
False False positivepositive
TP + FPTP + FP
Test -Test - False False negativenegative
True True negativenegative
FN + TNFN + TN
TP + FNTP + FN FP + TNFP + TN

Biotest with good sensitivity Biotest with good sensitivity (Negative predictive value > rule out test)(Negative predictive value > rule out test)
NFS or CRP (Appendicitis)NFS or CRP (Appendicitis)
D. dimeres (Phlebitis)D. dimeres (Phlebitis)
BNP (cardiac failure)BNP (cardiac failure)
Transaminases (hepatitis)Transaminases (hepatitis)
Urine test (renal colic, urine infection)Urine test (renal colic, urine infection)

Biotest with good specificityBiotest with good specificity(Positive predictive value > diagnosis tests)(Positive predictive value > diagnosis tests)
Lipase (pancreatitis)Lipase (pancreatitis)
Troponine (myocardial infarction)Troponine (myocardial infarction)
Hemocultures (septicemie)Hemocultures (septicemie)
LCR (meningitis)LCR (meningitis)
Frottis sanguin (paludism)Frottis sanguin (paludism)

Example of BNP and cardiac failureExample of BNP and cardiac failureFigure 1: Characteristics of BNP testFigure 1: Characteristics of BNP test applied to a hypothetical 1,000 people applied to a hypothetical 1,000 people
attending an emergency room with dyspnoea and suspected CHFattending an emergency room with dyspnoea and suspected CHF
Few Few false negative valuefalse negative value (good sensitivity) (good sensitivity) A lot of A lot of false positive valuefalse positive value (poor specificity) (poor specificity) Interest of BNP to rule out the diagnosis of CHF if Interest of BNP to rule out the diagnosis of CHF if
the test is negative.the test is negative.
1. R Cardarelli, TG Lumicao. B-type natriuretic peptide: a review of its diagnostic, prognostic, and therapeutic monitoring value in heart failure for primary care physicians. Journal of the American Board of Family Practice 2003 16: 327-333.
2. JA de Lemos et al. B-type natriuretic peptide in cardiac disease. Lancet 2003 362: 316-322.

Limits of a biotest: exemple of NT-proBNPLimits of a biotest: exemple of NT-proBNP Non cardiac sources of variation of NT-proBNP Non cardiac sources of variation of NT-proBNP
((age age , female, female, renal function, renal function, obesity , obesity )) Other cardiac conditions increase the values of NT-Other cardiac conditions increase the values of NT-
proBNP (atrial fibrillation, aortic stenosis)proBNP (atrial fibrillation, aortic stenosis) Problem of Problem of gray zonegray zone (indecision zone) (indecision zone)

Influence of a biotest on the Influence of a biotest on the decision = post-test probabilitydecision = post-test probability
Usual biotests influence diagnosis or treatment Usual biotests influence diagnosis or treatment in only less than15% in only less than15%
Sandler G. Do emergency tests help in the management of acute medical admissions ? Br Med J (Clin Res Ed) 1984 Oct 13; 289(6450):973-7.
InterventionAutre diagnostic
Seuil d’abstention Seuil d’intervention
05% 50% 90%
100%
IndécisionAutres tests

Example of d.dimeres for the diagnosis Example of d.dimeres for the diagnosis of deep vein thrombosis of deep vein thrombosis
= importance of probability pre-test= importance of probability pre-test
Prevalence 10% (Wells score) Prevalence 10% (Wells score)
> > law probabilitylaw probability
Prevalence 30% (Wells score) Prevalence 30% (Wells score)
> > intermediate probabilityintermediate probability
Prevalence 80% (Wells score) Prevalence 80% (Wells score)
> > high probablilityhigh probablility
Pre-test probability
Post-test probabilityLikelihood ratio
Need other test
Rule out DVT
Confirm DVT
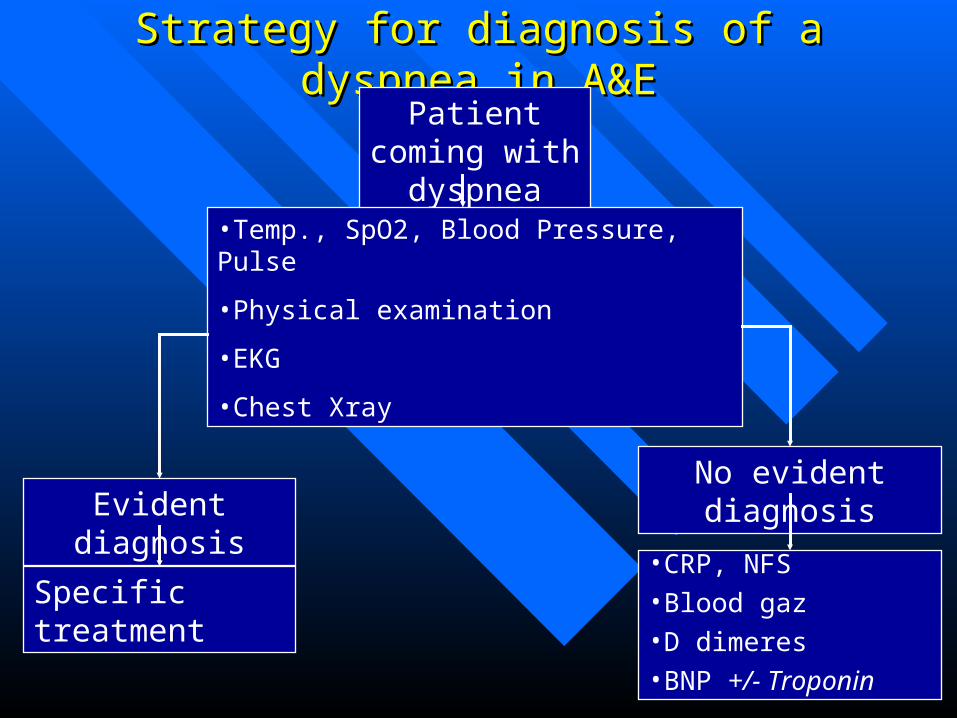
Strategy for diagnosis of a dyspnea in A&EStrategy for diagnosis of a dyspnea in A&EPatient coming with dyspnea
•Temp., SpO2, Blood Pressure, Pulse
•Physical examination
•EKG
•Chest Xray
Evident diagnosis
Specific treatment
No evident diagnosis
•CRP, NFS•Blood gaz•D dimeres•BNP +/- Troponin

Different steps of medical reasoningDifferent steps of medical reasoning
1.1. Evaluation pre-test Evaluation pre-test (clinic, prevalence, score etc)(clinic, prevalence, score etc)
2.2. Choose the right test Choose the right test (the one which will give us the (the one which will give us the
answer to our question)answer to our question)
3.3. Evaluation post-test (confrontation between Evaluation post-test (confrontation between
clinic and result of the test)clinic and result of the test)
4.4. Decision (intervention or not, other test?)Decision (intervention or not, other test?)

Avoid useless biotest Avoid useless biotest if no clinical orientation or if the if no clinical orientation or if the
diagnosis is evidentdiagnosis is evident Ionogramme, coagulation are often useless in most of Ionogramme, coagulation are often useless in most of
situations situations Thyroide hormone dosage without typical signs of Thyroide hormone dosage without typical signs of
thyrotoxicosis or hypothyroidethyrotoxicosis or hypothyroide Troponin is useless if no cardiologic orientation Troponin is useless if no cardiologic orientation
(chest pain and/or EKG anomalies)(chest pain and/or EKG anomalies) D dimeres are useless in case of high clinical D dimeres are useless in case of high clinical
probability of pulmonary embolism or deep vein probability of pulmonary embolism or deep vein thrombosis thrombosis (perform angio CT, or echo-doppler) (perform angio CT, or echo-doppler)

How to include a biotest in the medical reasoning ?How to include a biotest in the medical reasoning ?

Case Report 1: female 58 years old, “vertigo Case Report 1: female 58 years old, “vertigo sensation” for 3 days. Treatment for HTN with sensation” for 3 days. Treatment for HTN with
Amlor and Concor. Clinical exam finds TA Amlor and Concor. Clinical exam finds TA 19/10, pulse 60/min., T3719/10, pulse 60/min., T37
Clinical exam is normal (neuro, cardio, ORL). Clinical exam is normal (neuro, cardio, ORL).
EKG shows sinusal rhythm 60/min without EKG shows sinusal rhythm 60/min without
abnormalityabnormality
What kind of exam do you request?What kind of exam do you request?

Case report 2: A 3 years old boy consult for Case report 2: A 3 years old boy consult for fever sine 4 days, with cough and runny nosefever sine 4 days, with cough and runny nose
Alert, can eat & drink normally.T 36.8, RR 20/min, SaO2 Alert, can eat & drink normally.T 36.8, RR 20/min, SaO2
96% 96%
Auscultation normal, no rale, no murmur, abdomen supple, Auscultation normal, no rale, no murmur, abdomen supple,
no organomegaly, supple neck, no vomiting, no diarrhea.no organomegaly, supple neck, no vomiting, no diarrhea.
ENT: enlarge tonsils but no sign of infection (usual ENT: enlarge tonsils but no sign of infection (usual
according the mother)according the mother)
What test do you order: CBC, CRP, Ionogramme, Uree, What test do you order: CBC, CRP, Ionogramme, Uree,
Creat, ASAT, ALAT, Dengue NS1 or/and Dengue serology, Creat, ASAT, ALAT, Dengue NS1 or/and Dengue serology,
Urine test?Urine test?

Case report 3: A man 69 years old consult for Case report 3: A man 69 years old consult for inflammation at left leg appeared 1 day after a flight. inflammation at left leg appeared 1 day after a flight.
Past history HTN, Hypercholesterolemia, Thyroide pb.Past history HTN, Hypercholesterolemia, Thyroide pb.
Pulse 85/min, TA 17/9, RR 18/min, SaO2 96%Pulse 85/min, TA 17/9, RR 18/min, SaO2 96%
Swollen left ankle with inflammation along the lower part Swollen left ankle with inflammation along the lower part
of the left calf. No pain at the calf. Cardio-pulmonary exam of the left calf. No pain at the calf. Cardio-pulmonary exam
is normal.is normal.
Doppler shows a superficial thrombosis of the internal Doppler shows a superficial thrombosis of the internal
saphene vein, no deep vein thrombosis.saphene vein, no deep vein thrombosis.
What biotest(s) would you ask in the list below: What biotest(s) would you ask in the list below: Ionogramme, Glycemia, Uree-Creat, ASAT-ALAT-GGT, CRP, NFS, Ionogramme, Glycemia, Uree-Creat, ASAT-ALAT-GGT, CRP, NFS,
TP, TCA, D dimere, CPK, Groupe Rh x 2, Urine test, T4L-TSH?TP, TCA, D dimere, CPK, Groupe Rh x 2, Urine test, T4L-TSH?

Case report 4: a man 69 years old, treated with Case report 4: a man 69 years old, treated with Digoxin and Furosemide for cardiac insufficiency, Digoxin and Furosemide for cardiac insufficiency, coming for “fatigue and dyspnea” since a few days coming for “fatigue and dyspnea” since a few days
Clinical exam finds TA 11/7, pulse 40/min., mild Clinical exam finds TA 11/7, pulse 40/min., mild crackles in the lungs and swollen legs.crackles in the lungs and swollen legs.
EKG:EKG:
What are you diagnosis hypothesis and what kind of exams are you going to ask?

Case report 5: A man 48 years old, coming for Case report 5: A man 48 years old, coming for permanent chest pain for 2 hours. permanent chest pain for 2 hours.
Risks factors smoke and overweightRisks factors smoke and overweight Vital sign: Vital sign: TA 11/7, pulse 95/min, SaO2 95%, T37.8.TA 11/7, pulse 95/min, SaO2 95%, T37.8.
Clinical exam is normal (cardio/pulmonary)Clinical exam is normal (cardio/pulmonary) What are your diagnosis hypothesis?What are your diagnosis hypothesis? EKG:EKG:
What kind of exams are you going to ask to confirm you hypothesis?

Case report 6: a female 58 years old hospitalized 5 Case report 6: a female 58 years old hospitalized 5 days ago for ankle fracture come to A&E for days ago for ankle fracture come to A&E for dyspnea and chest pain since the day beforedyspnea and chest pain since the day before
Vital signs: pulse 95/min, TA 19/10, RR 20/min, SaO2 Vital signs: pulse 95/min, TA 19/10, RR 20/min, SaO2 94%, T37.794%, T37.7
Pain at left chest and shortness of breath, auscultation is Pain at left chest and shortness of breath, auscultation is normalnormal
EKG:EKG:
What kind of exam are you going to ask to confirm your diagnosis?

Interest of “bilan pre-op” for patient Interest of “bilan pre-op” for patient without severe history (ASA 1 or 2)*without severe history (ASA 1 or 2)* CBC useful only if there is a risk of hemorrhage during CBC useful only if there is a risk of hemorrhage during
surgery (hip fracture, colectomy, gastrectomy, etc)surgery (hip fracture, colectomy, gastrectomy, etc) TP, TCA, platelets are useful only if surgery at risk of TP, TCA, platelets are useful only if surgery at risk of
hemorrhagehemorrhage Ionogramme, Uree, Creat are useless if the is no clinical Ionogramme, Uree, Creat are useless if the is no clinical
orientation and no medication.orientation and no medication. Groupe ABO, Rh and RAI are not recommended if law Groupe ABO, Rh and RAI are not recommended if law
risk of hemorrhage during surgery.risk of hemorrhage during surgery.
* Examens pre-operatoires systematiques (ANAES 1998)