global training network programmeworld health organization
TRANSCRIPT

World Health Organization Global Training Network Programme
UNDERSTANDINGUNDERSTANDING
VACCINE REACTIONS (2) VACCINE REACTIONS (2)

World Health Organization Global Training Network Programme
PART 2PART 2
Vaccination of high-risk groups
Contraindications to vaccination
Adverse events associated with particular vaccines
Pathogenesis of serious adverse reactions

World Health Organization Global Training Network Programme
IMMUNIZATION OF SPECIAL POPULATIONSIMMUNIZATION OF SPECIAL POPULATIONS
5 dosesYYTetanus toxoid
N (need studies)YYellow fever
As for uninfectedYYHepB
6 and 9 monthsY (depends)YMeasles
0, 6, 10, 14 weeksY (IPV if available)YOPV
6, 10, 14 weeksYYDTP
BirthNYBCG
Optimal timing SymptomaticAsymptomaticVaccine
WHO/ UNICEF recommendations for vaccination of HIV-infected children and women of childbearing age

World Health Organization Global Training Network Programme
CONTRAINDICATIONSCONTRAINDICATIONS
True contraindications are rare
Current serious febrile illness delay vaccine administration
History of severe AEFI after previous dose
Evolving neurological disease avoid whole cell pertussis vaccine
(e.g. uncontrolled epilepsy)
Type 1 hypersensitivity to egg - avoid yellow fever & influenza but can use vaccines made in chick fibroblasts
Symptomatic HIV avoid BCG and yellow fever
WHO Immunization Policy 1996

World Health Organization Global Training Network Programme
CONTRAINDICATIONSCONTRAINDICATIONS
Anaphylactic reaction to neomicin, streptomycin or polymyxin B
IPV
Immunodeficiency, or immunodeficient household contact*
OPV
Encephalopathy within 7 days of administrationDTP
Anaphylactic reaction to vaccine or vaccine constituentSevere febrile illness
All vaccines
ContraindicationVaccine
* Risk benefit assessment when administered to HIV positive individuals
Adopted from Plotkin pg 66-67

World Health Organization Global Training Network Programme
CONTRAINDICATIONSCONTRAINDICATIONS
Anaphylactic reaction to common baker’s yeastHepatitis B
Anaphylactic reaction to egg, immunodeficiencyYellow fever
NoneHib
Anaphylaxis, pregnancy, immunodeficiency*MMR
ContraindicationVaccine
* Risk benefit assessment when administered to HIV-positive individuals
Adopted from Plotkin pg 66-67

World Health Organization Global Training Network Programme
ANAPHYLAXISANAPHYLAXIS
Type 1 hypersensitivity reaction
Circulatory failure
Bronchospasm +/- laryngospasm/laryngeal oedema
respiratory distress
May include pruritis, flushing, angioedema, seizures, vomiting, abdominal cramps & incontinence
Occurs in previously sensitized individuals

World Health Organization Global Training Network Programme
ANAPHYLAXISANAPHYLAXIS
Reported less from developing countriesLess sensitization?
Less reporting?
Anaphylaxis is rare (1/1 000 000 vaccinations)
Fainting is common
Untrained staff may misdiagnose fainting/dizzinessfor anaphylaxis or vice versa
Administration of adrenaline in a faint may bedangerous
PROMPT MANAGEMENT IS VITAL!

World Health Organization Global Training Network Programme
ADVERSE EVENTS ASSOCIATEDADVERSE EVENTS ASSOCIATED WITH SPECIFIC VACCINES WITH SPECIFIC VACCINES
WHO case definitions are used here
Lack of standardized case definitions in the literaturee.g. fever
The Brighton collaborationdeveloping case definitions for AEFI
promoting global implementation of these definitions
[email protected]://brightoncollaboration.org

World Health Organization Global Training Network Programme
SEIZURESSEIZURES
Particularly associated with measles and DTP vaccination (pertussis component)
febrile seizures Temp >38afebrile seizures Temp normal
Febrile seizures more common with pertussisAn association with non-febrile seizures has not been proven

World Health Organization Global Training Network Programme
ADVERSE REACTIONS TO BCG ADVERSE REACTIONS TO BCG
Disseminated BCGwidespread infection, 1-12 months after BCG
usually in immunocompromised individual
confirm by isolation of Mycobacterium bovisBCG strain
treat with antituberculous regimen including Rifampicin and Isoniazid
Osteitis/osteomyelitisinfection of the bone with M bovis BCG strain
management as above

World Health Organization Global Training Network Programme
ADVERSE REACTIONS TO BCG ADVERSE REACTIONS TO BCG
Suppurative lymphadenitisoccurs within 2-6 months of BCG vaccination
case definition
1 lymph node> 1.5 cm in size/draining sinus over a lymph node
usually occurs in the axilla, on the same side as innoculation
Managementheals spontaneously over monthsonly treat if sticking to skin or drainingsurgical drainage and local installation ofantituberculous drugsystemic Rx is ineffective

World Health Organization Global Training Network Programme

World Health Organization Global Training Network Programme

World Health Organization Global Training Network Programme
ENCEPHALOPATHY AND ENCEPHALITISENCEPHALOPATHY AND ENCEPHALITIS
Possibly associated with measles & pertussis vaccine
Case definition of encephalopathy2 out of 3 of
seizuresalteration of consciousness lasting for one day or moredistinct change in behavior for one day or more
Temporal relationshipwithin 48 hrs with DTPwithin 7-12 days after measles or MMR

World Health Organization Global Training Network Programme
ENCEPHALITIS AND MEASLES VACCINATIONENCEPHALITIS AND MEASLES VACCINATION
An analysis of claims for encephalitis following measles vaccine in the USA found clustering of events 8-9 days after vaccination (Wetbel 1998, Duclos 1998)
This supports, but does not prove, thepossibility that measles vaccine was causative
Risk is less than 1 case per million

World Health Organization Global Training Network Programme
TIMING OF VACCINATIONSTIMING OF VACCINATIONS
>2 killed antigens
killed and live antigens
>2 live antigens
None can be given simultaneously/at any interval
None (except cholera andyellow fever)
4 weeks, if not administered simultaneously (except OPV can be given any time before, after/with MMR and oral typhoid
World Health Organization Global Training Network Programme
MANAGEMENT OF ANAPHYLAXISMANAGEMENT OF ANAPHYLAXIS
Restore respiratory and cardiovascular function
SQ adrenaline: counteract bronchoconstriction and
vasodilation
Crystalloids - restore intravascular volume & prevent
shock
Establish and maintain airway
Corticosteroids to prevent “late-phase” reaction
Aminophylline as adjunctive for bronchospasm
Antihistamines not effective as primary therapy

World Health Organization Global Training Network Programme
TOXIC SHOCK SYNDROMETOXIC SHOCK SYNDROME
A one-year-old child died within 12 hours of receiving measles vaccine. It was reported as a possible anaphylaxis because of its rapidonset. Investigation found that the vaccine used was likely to have been reconstitutedsome days prior to this particular use.
Cause: Non sterile injection: NOT ANAPHYLAXIS!!!

World Health Organization Global Training Network Programme
BCG ADVERSE REACTIONSBCG ADVERSE REACTIONS
CaseAn outbreak of lymphadenitis three months after BCG immunization was traced to a switch to a differentstrain of vaccine. The investigation also highlighted a number of programme errors (vaccines not properlyreconstituted, and injections not given intradermally).
Cause: Vaccine reaction compounded by programme errors
World Health Organization Global Training Network Programme
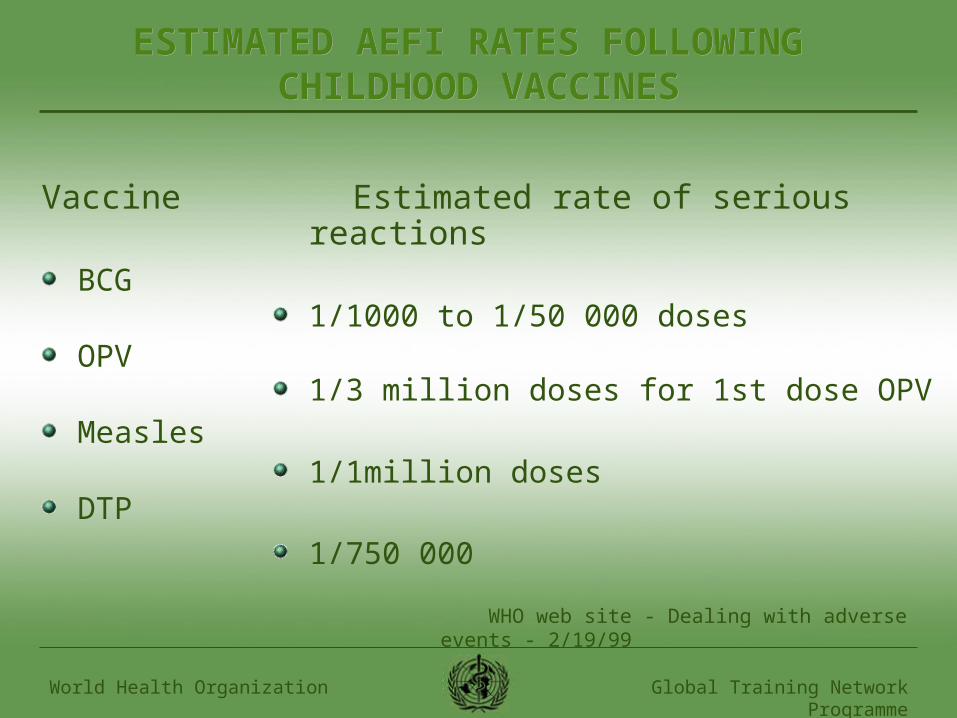
ESTIMATED AEFI RATES FOLLOWING ESTIMATED AEFI RATES FOLLOWING CHILDHOOD VACCINESCHILDHOOD VACCINES
Vaccine
BCG
OPV
Measles
DTP
Estimated rate of serious reactions
1/1000 to 1/50 000 doses
1/3 million doses for 1st dose OPV
1/1million doses
1/750 000
WHO web site - Dealing with adverse events - 2/19/99