global oral cancer forum (group 2) understanding gaps in ... · understanding gaps in the oral...
TRANSCRIPT

1
Global Oral Cancer Forum (Group 2)
Understanding gaps in the oral cancer continuum
and developing strategies to improve outcomes
Saman Warnakulasuriya OBE, BDS, FDS, Dip Oral Med, PhD, DSc
Professor of Oral Medicine & Experimental Pathology, Kings College
London, UK; Director, WHO Collaborating Centre for Oral Cancer, UK
Pedro Diz Dios, MD, MDS, DDS, PhD
Professor, Special Needs Dentistry, Santiago de Compostela
University, Santiago de Compostela, Spain
Hector Lanfranchi, DDS, PhD Professor, Oral Medicine, School of DentistryUniversity of Buenos Aires, Argentina
Jed J. Jacobson, DDS, MS, MPH
Chief Science Officer and Senior Vice President, Delta Dental of Michigan, Ohio, Indiana and North Carolina, USA
Honghua
Professor and Chair, Department of Oral Medicine,School of Stomatology, University of Peking, China
Alexander Rapidis MD, DDS, PhD, FACS
Chairman Department of Oral and Maxillofacial/Head & Neck
Surgery, Greek Anticancer Institute, Saint Savvas Hospital, Athens,
Greece
20th February 2016

2
Introduction
Oral cancer is a global health problem and statistical data from various regions,
reported by Group 1 in the earlier session, confirms a rising incidence. Geographical
variations in oral cancer incidence seem to reflect disparities in socioeconomic
status of the global population (Johnson et al. 2011) and different lifestyles related
to the use of tobacco, areca nut and alcohol consumption (Warnakulasuriya, 2009).
Worldwide, oral cancer has one of the lowest overall 5-year survival rates, close to
50%; higher rates are reported from the US (63.2%; 2005-2011) (National Cancer
Institute, 2015). Poor prognosis for people diagnosed with oral cancer has remained
unaffected despite recent therapeutic advances (Chan et al., 2015). As discussed in
the present paper, poor prognosis is largely attributable to cancers of the oral cavity
and oropharynx being detected in advanced stages. Delays in diagnosis occur over
various stages of a patient’s cancer journey.
Delays encountered in diagnosis have been attributed to the advancement of the
stage of the disease at presentation to a specialist. In this session the authors aim to
discuss gaps in our knowledge related to delays in diagnosis of oral cancer; to
discuss barriers that remain for the early detection of this disease; and to bring to the
attention of the forum examples of programs developed for professionals that have
been established to overcome these delays. Organized Screening as a means of
early detection is presented by Group 3 and as Group 6 has the task to address
campaigns to improve public awareness: these will not be discussed here. From
these global experiences we hope to make recommendations for future research to
understand what we can do to recognize the disease earlier, and propose
development goals to avoid diagnostic delays.
Does the stage of the disease influence survival?
Carefully conducted follow-up studies have highlighted several prognostic factors for
oral cavity cancers. These include both patient and tumor factors, such as:
• Gender
3
• Socioeconomic and nutritional status
• Lifestyle-related risk factors
• Presence of comorbidities
• Location of the tumor
• Disease stage, including nodal status
• Expression of several key biomarkers.
In univariate studies most of these factors have shown significant associations. For
example, Tromp et al (2005) suggest that a trend among men for drinking more than
four alcoholic drinks per day has increased the risk of advanced stage disease
significantly (OR = 2.67, P = 0.026). However, when examined by multivariate
analysis with due adjustments, the significance of the majority of these prognostic
factors are attenuated, but the stage of the disease at diagnosis remains highly
significant and is confirmed as an independent risk factor that influences survival. In
a literature search of articles published since 2000 we found 16 studies– all with
multivariate analysis – confirming advanced stage of oral cancer is associated with
poor prognosis (Rodrigues et al, 2014; Rikardsen et al, 2014;Monteiro et al, 2014;
Ling et al, 2013; Dissanayaka et al, 2012; Pruegsanusak et al, 2012; Jan et al, 2011;
Liu et al, 2010; Kreppel et al, 2010; Mosleh-shirazi et al, 2008 ; Sargeran et al
2008 ;Lam et al, 2007 ; Aksu et al, 2006 ; Kademani et al, 2005; Sciubba 2001;
Pericot et al, 2000). Despite major efforts to identify new predictive parameters and
histological systems, the most recent Brazilian study by Rodrigues et al (2014) has
shown that clinical stage is still the most reliable prognostic factor for patients with
tongue cancer. These studies, which indicate positive associations of stage of
disease with survival, are listed in Tables 1 A & B. Examples of studies indicating a
direct association of the tumor stage with survival are illustrated in Figure 1. Oral
cancer is often staged by the TNM system. Data from a US study (Table 2) shows a
direct relationship between TNM stage of diagnosis and 5 - year survival (Sciubba,
2001). A recent study (Mücke et al, 2015) assessed how advanced a cancer is
using other parameters- such as by measuring tumor volume - has shown that a
large tumor volume was associated with a significantly poorer overall survival
(P<0.001).
In this article the authors argue that oral cancers have high death rates because the
disease is often at an advanced stage before it is diagnosed, and major interventions
4
that reduce delays in diagnosis could contribute to improvement in disease-specific
survival.
Reasons for presentation in advanced stages
Presentation at an advanced stage of the disease could occur either as a result of
the biologically aggressive nature of a malignancy or due to delays encountered in
the patients’ journey. Perhaps not much could be done by a clinician to interact
against the aggressive nature of a particular cancer. The vital question that is
important is: To what extent does delay in detection in primary care affect the stage
of presentation, and thereby the outcome for patients with the disease? Some argue
that it is still safe to leave this subject in a speculative limbo, without very much in the
way of evidence. A meta-analysis has reported on total diagnostic delay in oral and
oropharyngeal cancer based on 14 reported studies (Gomez et al., 2009).This
analysis estimated that patients with delayed diagnosis had a higher probability of
presenting with advanced stages of oral cancer compared with those without
delayed diagnosis. This was particularly the case for those with a delay longer than 1
month (Gomez et al., 2009). In a further review, the relationship between diagnostic
delay and stage at diagnosis varied in direction and magnitude, with no consistent
positive association in any of the head and neck cancer sites (Goy et al.,2009).
‘Unnoticed’, or minor, symptoms may be responsible for the discrepancy reported in
the literature between the stage of tumor and reported patient delay. Cleveland
(2012), reviewing Gomez et al’s (2009) meta-analysis, concluded that based on the
limited quality of the data, better evidence about the relationship between diagnostic
delay and disease progression or disease outcomes is needed.
For this review we examined later studies that reported total delay from 9 countries
since 2009. An updated data synthesis is listed in Table 3. Some improvement in
diagnostic delay in noted in few studies eg. from Argentina, Finland, Spain and Italy.
Delay in diagnosis during a patient’s cancer journey
Delays that occur from the time a patient experiences his/her first symptom to the
time of treatment can be conceptually divided into various stages, primarily based on
who is responsible for this delay. Patient delay is defined as the time elapsed
between symptom discovery and the first medical contact with a medical doctor or a
5
dentist concerning that symptom. Referral delay (also referred to as scheduling
delay) is defined as the period between the first medical contact in a primary care
setting with the general practitioner or dentist, and the next contact with the medical
specialist. Medical specialist delay is defined as the period from the first contact with
the medical specialist until definitive diagnosis. Based on the available resources in
the healthcare system, further delays could occur from the time of confirmed
diagnosis to the day the patient commences treatment (i.e. surgery). Total delay is
defined as the period between symptom discovery and initiation of therapy. Gomez
et al. (2010) and Guneri and Epstein (2014), in reviewing diagnostic delays, have
produced schematic diagrams to assist understanding of these various stages of
delay (Figures 2 A and B).
Patient delay
Goy et al.’s (2009) systematic review examined the evidence for an association
between patient-related delay in presenting to a primary care facility and stage at
diagnosis. The authors reviewed 10 eligible studies and findings indicated differing
relationships between patient delay and stage. Patients’ recall bias may have
affected these study results as inaccurate identification of the timing of symptom
onset was likely to influence most of these studies. The most significant finding was
reported by Brouha et al. (2005), who found that oral cancer patients who delayed
more than 1 month in seeking care following symptom onset were twice as likely to
have advanced-stage oral cavity cancer at diagnosis.
An integrative review on factors associated with patient delay and oral cancer was
conducted by Noonan (2014) and this review included 16 studies reported between
2001 and 2010. His findings are represented in Table 4.
Patient delay can largely be attributed to lack of public awareness of the signs and
symptoms of disease and oral symptoms being rarely attributed to cancer and
frequently interpreted as minor oral conditions (Scott et al., 2005). A qualitative
study conducted in Scotland among young people who were later diagnosed with
oral cancer outlines the reasons for postponing or barriers faced at a medical/dental
consultation (Grant et al, 2010). Population studies in the UK have recorded an
alarming lack of public awareness on oral cancer, that could be as low as 50%
6
(Warnakulasuriya et al., 1999). Mouth Cancer Awareness Campaigns and social
media interventions (discussed in Group 6) may need to be heightened at local and
national levels to improve the public awareness of mouth cancer. Kerr et al.(2004)
emphasise the need to develop and assess oral cancer education/awareness
programs, specifically customized to the various dental-medical professionals/
trainees and to populations at risk. The relevance and the magnitude of the observed
effects of any awareness campaign require further study.
Provider-related diagnostic delay
There are a limited number of studies conducted in primary care investigating the
interval to diagnosis (diagnostic delay). Diagnostic delay is traditionally measured by
the number of days elapsed since the patient reports the first sign and/or symptom
until a definitive diagnosis is reached. Many authors have used the mean or the
median of the time distribution to categorize the diagnostic delay (Pitiphat et al,
2002; Onizawa et al, 2003; McGurk et al, 2005). The “Median time” lapsed is more
frequently used because it is not affected by extreme values and the distributions
usually have very wide ranges. Other authors choose an arbitrary time point (more
than 30 days) to discriminate between delayed and non-delayed cases (Brouha et
al., 2005; Tromp et al., 2005).
A recent Australian study has reported that delays in patients seeking advice have
decreased compared to previous studies, while delays in professionals making a
diagnosis have not improved considerably. (Kaing et al., 2015)
A recent meta-analysis (Seonne et al., 2015) has concluded that diagnostic delay is
a moderate risk factor of mortality of head and neck cancer. Their investigation has
revealed serious methodological limitations in the studies on oral cancer diagnostic
delay. The authors recommended that the guidelines in the Aarhus Statement
(Weller et al., 2012) should be used by researchers reporting on early cancer
diagnosis to ensure standardized and uniform criteria, which would, in turn, permit
interventions aimed at diminishing time intervals to treatment and improve the
prognosis of the disease. The Aahrus statement, highlights that in the pathway of
oral cancer patients it is strongly recommended to describe “key events” and “time
intervals” instead of “diagnostic delay”.

7
Logistic issues relating to the ‘measurement of delay’ cannot be easily resolved
when transcribing data from patient records. Therefore, alternative ways of
measuring delay must be found. Using data from the English National Audit of
Cancer Diagnosis in Primary Care, Lyratzopoulos et al. (2013) found that the number
of pre-referral consultations has construct validity as a measure of the primary care
interval for a number of cancers. Among 18 common and rare cancers investigated
by this group, oral and oropharyngeal cancers was also included in their analyses. In
this audit, 21.9% of patients finally diagnosed with oral cancer had more than three
consultations in primary care prior to referral. A correlation between pre-referral
consultations and duration of primary care interval was intuitive, but evidence about
this association is sparse in the literature. Point-of-care diagnostic technologies (that
can be undertaken in primary care) can also have a part in reducing the number of
consultations before referral, and such tests (discussed by Group 4) merit further
development and evaluation.
Tumor aggressiveness may also play the role of a confounding factor in examining
the association between delay and survival. Rapid progression of a malignancy
could be affected by rapid proliferative activity of the tumor (e.g. biological
aggressiveness) as well as by any delay in the diagnosis (Seone et al., 2010). The
growth rate of a tumor varies enormously and there is little data in the recent
literature since the work of Evans et al. (1982). Scott et al. (2005) observed that
detecting a small cancer is only possible when the velocity of tumor growth is low
and a proportion of tumors may be silent until advanced in stage. In other cancer
sites, such as cervical, the results imply that in most cases stage at diagnosis is
affected more by the biology of the cancer than by diagnostic delay. They also noted
that a proportion of tumors may be silent until advanced in stage and evade a person
noticing the change.
Research in primary care related to professional diagnostic delay
Professional delay in diagnosis of oral cancer has several definitions in the literature:
the time elapsed since the first consultation to a healthcare professional until the first
consultation to the treating professional (Allison et al., 1998), or until the appointment
for treatment (Kowalski et al., 1994). It has also been defined as the time since first
8
consultation to the receipt of the referral letter at the specialized services (Scully et
al., 1986; Schnelter,1992; Hollows et al., 2000). However, the commonly accepted
definition considers the time elapsed since the first consultation by a health
professional until a definitive diagnosis is reached (Hollows et al., 2000; Wildt et al.,
1995; Dimitroulis et al., 1992) or treatment is instituted. A number of definitions used
by research groups and the grouping of the different time periods make comparisons
difficult. This accounts for the reduced number of reviews addressing this issue. Data
relating to how professional diagnostic delay leads to poor outcomes is meagre.
A study in Cordoba, Argentina, examined professional delayed encountered before
arriving in 2 hospital centres (Morelatto et al. 2007). In a multivariate analysis the
authors found that professional delay was the most related variable to the stage at
the time of diagnosis (P>0.03). Detailed questioning revealed that eighty percent of
the patients received some prescription medication by a health professional for
cases later diagnosed to have oral cancer. 30% had received ploypharmacy, 26%
mouthwashes and 20% received antibiotics or anti-inflammatory agents.
In study based on self completed questionnaires among patients diagnosed with oral
cancer, Crossman et al. (2015) assessed the outcomes of the initial consultations
with their GP. Their inquiry revealed that after consultation with a GP (n=109), 53%
were referred to a specialist, 22% were referred for tests, 12% were told that their
symptom was not serious, and 12% were treated for another condition (Crossman et
al., 2015).
The following causes could be identified as causing professional diagnostic delay in
primary care:
• Not practicing a full clinical examination (Warnakulasuriya & Johnson, 1999)
• Clinical signs of cancer being mistaken as signs of inflammatory disease
(Onizawa et al., 2003)
• Low index of suspicion (Holland, 1982)
• Lack of familiarity and experience with the disease (Guggenheimer et al,
1989).
9
• Cancer symptoms, such as growths or ulcers, are not uncommon in the oral
cavity and are equally indicative of benign disorders (Llewellyn et al, 2004)
• Comorbidity has also been suggested (Allison et al, 1998), as in these
situations the clinicians tend to prioritize the stabilization of the existing
disease before paying attention to new symptoms.
Two key studies from Finland and Canada provide strong evidence that delay in primary care could significantly affect the outcome.
In a study from Finland (Alho et al 2006), the action taken in the general practices at
the initial visit of 221 patients later found to have cancer was analysed. Fifty-six
percent (n=123) received referrals, 24% (53) follow-up appointments and 20% (45)
neither (‘overlooked’). At 3 years, the risk of death was significantly higher among
patients whose head and neck symptoms were overlooked (adjusted hazard ratio
[HR] 1.89, 95% confidence interval [CI] 1.03–3.45). The excess risk associated with
being overlooked, however, was confined to subjects with tongue or glottic tumors
(HR 4.25, 95% CI 1.59–11.4).
The authors concluded that despite the rarity of patients with head and
neck carcinoma in primary care, patients with symptoms of these diseases and
especially with symptoms of tongue and glottic carcinomas should be initially
referred for further care or follow-up. Their data confirmed that those overlooked by
their primary care physician were at increased risk of death at 3 years compared with
patients who were initially referred or followed up. These significant findings led to
the authors’ conclusion that referral to a specialist or close follow-up should be
considered for patients presenting to their primary care physician with symptoms of
tongue and glottis cancer.
Groome et al (2011) reported a population-based study in Ontario, Canada, that
examined factors associated with early versus late-stage oral cavity cancer
diagnoses in a primary care setting. Their cohort study included all patients
diagnosed with invasive squamous cell carcinomas of the anterior tongue and floor
of mouth from 1991 to 2000. The principal data were collected through a province-
wide chart review. They reported that both physician-related and system-related
10
delay were much less common than patient-related delay, but physician-related delay
was associated with advanced stage disease (P = 0.04). Overall, physician-related
delay was documented in 14.3% and system-related delay in 1.6%of patients.
Although only 35% of all patients had a regular dentist in this study, it is of interest to
note that having a regular dentist and being followed up for a pre-cancerous lesion
led to a better chance of an early diagnosis in the floor of the mouth.
Delays in secondary care
The increasing volume of patients arriving in secondary care facilities for the
management of head and neck cancers can lead to longer waiting times for surgery
following confirmation of the diagnosis. Delays take place within the context of a
healthcare system that has waiting lists for operations and reduced manpower
resources. This could theoretically lead to progression of the disease and undue
psychological stress to the patients. A Dutch study (van Harten et al., 2014)
investigated the effect of longer waiting times (after reaching a diagnosis) on disease
outcome. Median waiting time for surgery following a confirmed diagnosis for
patients with oral cavity cancers was 38 days (25-75% IQR 27-50.5), and 41 days for
oropharyngeal cancers (25-75% IQR 30-54). The study did not reveal any adverse
effects of longer waiting times, but the data was compounded by advanced cases
being treated earlier to avoid further complication or inoperability had they waited
any longer for treatment. The authors mentioned that this finding can be used
cautiously to comfort patients who are anxious about delays they experience while
awaiting surgery. However, a later study by the same authors on a larger cohort of
Dutch patients (n=13,140) with a median waiting time of 37days for surgery or other
therapies, showed that longer waiting time, was significantly related to a higher
hazard of dying (p<0.0001) (van Harten et al., 2015).
Investigations on barriers that delay or affect early detection
The role of the primary care practitioner as the first point of contact for patients with
oral cancer has been increasingly highlighted (Fanaras and Warnakulasuriya, 2016).
It is generally assumed that patients with symptoms directly or indirectly related to
the oral cavity are likely to first visit their dentist for advice. However, many recent
studies (Eadie et al., 2009; Crossman et al., 2015; Kaing et al., 2015 ) have pointed

11
out that patients with oral cavity cancers are being referred by family physicians
more often than dentists. Vulnerable and high-risk groups, such as those from low
socioeconomic backgrounds, smokers, those who consume alcohol heavily, or the
elderly often have limited access to dental care. The awareness of general medical
practitioners - especially in such cases - is crucial as these patient cohorts are more
likely to visit their doctor first with symptomatic disease. New off-clinical counsellors
(herbalists and pharmacy assistants) have also been identified as potential creators
of patient diagnostic delay in oral cancer, raising the need for increasing oral cancer
awareness amongst community pharmacists (Varela-Centelles et al., 2012)
A number of research methods have been used to record the response of both dentists and doctors in a primary care setting to examine barriers faced by them to either screen asymptomatic individuals or to examine their approach into complaints of likely malignant lesions.
A lack of understanding of the clinical presentation of disease and confidence on the
part of health professionals has been suggested as a barrier for suspecting cancer
and dealing promptly with an appropriate referral or arranging a follow-up visit. This
particularly applies to general practitioners, for whom the availability of relevant
clinical updates is limited. A large number of medical practitioners state that they
have never received adequate training in the examination of the oral cavity and
detection of oral cancer and as a result there is lack of confidence and knowledge of
the risk factors and specific symptoms (Nicotera et al. 2004). The limited knowledge
and exposure to disease of the oral cavity is a common theme in most European
studies. Interestingly, the performed examinations for oral cancer and enquiry for risk
factors, such as smoking and alcohol use, become more frequent with the increase
in years of practising medicine.
Another barrier to performing routine screening has been shown to be the anxiety
caused to the patients by a false–positive diagnosis or the need for further
investigations (Noonan, 2014). However, annual oral cavity examinations could be
life-saving (Kerr, 2000).
12
It is of interest to examine data from few studies reported in primary care. Wade et al
(2010)i used a questionnaire based on the Theory of Planned Behaviour (Ajzen,
1985) to determine the general practitioners’ intention to perform screening for oral
cancer. The results were interesting as 97% of the participants claimed never to
have had training on the examination and screening of malignancy of the oral cavity,
and 68% stated they had no similar training for ear, nose and throat either. Scores
for subjective norm and internal control beliefs showed that although they believed
that screening for oral cancer was important and would have colleagues’ approval,
but that low confidence would prevent them from performing an examination.
External factors determining this behavior according to the same study were patient
refusal, time limitation and lack of appropriate equipment.
Paudyal et al (2014), in a systematic review aimed at the acceptance of screening
for oral cancer by the patients outside the primary dental care setting, reported that
the majority of screening methods are entirely accepted by patients and that lack of
acceptance of screening in a general practice setting is not a barrier itself. In fact,
some studies showed that a large proportion (70%) of the patients would firstly
consult their medical practitioner and then the dentist (Eadie et al., 2009) ii. Where
there was limited knowledge regarding oral cancer and screening methods on the
patients’ part, which could cause anxiety and constitute a barrier to treatment, the
provision of relevant information about the disease had a positive impact and made
acceptance more likely (Paudyal et al. 2014).
A qualitative methodology was used by Brocklehurst et al (2010) in order to explore
the general dental practitioners’ views on the issue of the opportunistic screening for
oral cancer. Semi-structured interviews were used to determine the factors
influencing the decision to screen and the screening process. Analysis of the data
has shown a lack of diligence on the part of the participants, which was also
demonstrated in earlier studies (Greenwood et al. 2001). Reported low incidence of
malignant lesions by the dentists and lack of awareness of clinical guidelines have
been identified as contributing factors. On the other hand, a lack of confidence was
not recorded in this study. Years of practice and clinical experience constituted a
factor providing the confidence to examine the oral cavity for malignancy. Patient
13
anxiety and awareness of the disease was also identified as a factor influencing
screening and promoting referral for further assessment.
Macpherson et al (2003) conducted a survey among dentists and primary care doctors in Scotland, initially using a postal questionnaire and then semi-structured interviews for qualitative analysis. The majority of the medical practitioners (94%) indicated that they usually examine the mouth in response to complaint
of pain or when there is a history of previous conditions of the oral cavity (81%). For 58% of the dentists, an examination for oral cancer was always included in routine dental checkups and 38% were screening only occasionally. A
small proportion of primary care doctors (23%) felt ‘confident’ that an observed lesion
required urgent referral, while the equivalent percentage for dentists and community
dental officers was 48%. Although the majority of the doctors agreed that they had a
significant role to play in oral cancer early diagnosis, 70% stated that the lack of training was a barrier to routine screening, with 37% declaring that they have never had any organized teaching on the subject. Lack of time was also identified by 47% of doctors as a contributing factor to limited screening of the oral cavity.
In order to help doctors and dentists in improving their skills in systematic examination of the oral cavity and neck, and to remind them of the signs to look for, recent attempts have been made to launch web-based learning tools, e.g.
www.oralcancer.ldv.org
http://learning.bmj.com/learning/module-intro/mouth-cancer-recognising-referring-
early.html?moduleId=10015809&locale=en_GB.
http://www.exodontia.info/files/BDA_2011._Early_Detection_of_Oral_Cancer._A_Ma nagement_Strategy.pdf
Strengths and weakness of available web resources and e learning platforms on oral cancer are reviewed by Varela-Centelles et al. (2015).
Other factors affecting delay
Social and cultural factors
14
Disadvantaged groups are more likely to be diagnosed with advanced disease or
worsened cancer-related outcomes (Wade et al., 2004). In whatever way we
measure deprivation – by education, income or occupation- people in lower social
classes are at a higher risk of developing oral cancer (Conway et al., 2008).
Inevitably, they also present late in health care settings: a study among patients
under 45 years of age from South East England confirmed that patients of a lower
social class were more likely to delay presentation to a healthcare setting (Llewellyn
et al., 2004).Even controlling for Socio Economic Status [SES], minority and
medically-underserved groups tend to present with late stage disease and
consequently suffer higher morbidity and mortality rates than other groups (Freeman,
2004). The 5-year survival rates for oral cavity, pharynx and other head and neck
cancers are significantly lower for male African Americans than Caucasians. Shavers
et al. (2003) suggested that differential rates of early detection may contribute to
racial differences in survival and mortality from cancers of the oral cavity and
pharynx. Patients who took traditional herbal medication before seeking professional
consultation had a significant delay in diagnosis (Tromp et al., 2005)
Evidence from other fields of oncology suggests that patient delay behavior may be
influenced by holding negative attitudes toward seeking medical help, and holding
negative beliefs about the consequences of the cancer. In patients reporting lifestyle
stress in the period prior to diagnosis, the risk of delay could be higher (Llewellyn et
al., 2004). (Table 4)
In a national population-based survey of adults in the UK (Robb et al., 2009) most
widely endosed barriers to seeking the first consultation was:
• Difficulty in making an appointment
• Not wanting to waste doctor’s time
• Worry about what the doctor might find
In addition to providing education, during public awareness we should consider
empovering the public to seek medical advice as well as strengthen support at
primary care by improving access.
15
Assessment of Oral Cancer Risk
Measuring risk for oral cancer has not received much attention. Regrettably,
prediction of cancer risk is a minor component of oral health risk appraisals.
As most people have not even heard of oral cancer, perception of individual oral
cancer risk is also poor (Warnakulasuriya et al., 1998). The Harvard Cancer Risk
Index offers a simple estimation of personal risk of cancer for a number of major and
common cancers (Colditz et al., 2000). It offers the potential for tailored health
promotion messages to at-risk populations and also serves as a guide to general
practitioners and dentists to screen or monitor the oral cavity of high-risk subjects
whenever they present in a healthcare setting with other comorbidities.
A private insurance company (Denplan) in the UK has developed a risk assessment
system for oral diseases (DEPPA) including an oral cancer risk assessment for
patients registered in their Private Health System. Recently the program recorded
60,000 assessments by 700 dentists registered to use DEPPA. The key informers
used are:
• Smoking and smokeless tobacco use
• Alcohol intake above safe limits (synergistically with smoking)
• Age and gender
• History of previous oral cancer
Based on above assessments, a score of 1-5 is assigned to patients at registration
and follow up. In January 2016, for example, 2587 patients were assessed using
DEPPA (average age was 56 years) and 10% were recorded to have several or
many risk indicators (Score of 4 or 5) [Personal information Drs Mike Busby and
Henry Clover ].
However, among young persons [arbitrarily set at under 45 years of
age], approximately 25% of those who develop oral cancer may not have had any
risk factors (Llewellyn et al., 2001), calling into question whether a high risk
16
assessment may significantly disadvantage this age group. Although oral cancer
among under 45-year-olds is still relatively rare, a review has shown that oral cancer
cannot be discounted in patients of any age who report no history of tobacco or
alcohol use (Llewellyn et al., 2001).
Access to care
There is lack of adequate healthcare coverage available to many persons living in
less developed countries to seek medical opinion when faced with minor /initial
mouth cancer symptoms. There are, of course, countries in the developing world,
such Cuba, Chile and Sri Lanka,which should be considered as exemptions which
provide universal access to free care. Elsewhere, even when it’s available it is
often inequitable and unaffordable. Socioeconomic inequalities and poor access
to care are not exclusive to low income countries. Long-term trends (based on US
SEER data) in oral and pharyngeal cancer (OPC) incidence, mortality and survival
show significant differences among U.S. blacks and whites. Five-year relative
survival rates for patients diagnosed during the period 1995-2001 were higher for
whites than for blacks and lowest for black males (Morse and Kerr, 2006). The US
healthcare system has been very fragmented and uncoordinated, resulting in
delays of diagnosis and treatment. With the passage of the Affordable Care Act
(ACA) there are provisions within the Accountable Care Organization’s (ACO)
framework that may help address some of these delays. ACOs will benefit as they
implement changes in their health systems to reduce costs and improve quality of
care. There is an opportunity for the Global Oral Cancer Forum [GOCF] to present
a value proposition to the ACOs that early detection and diagnosis, of oral and
oropharyngeal cancer can do both; improve morbidity associated with these
malignancies and reduce costs.
A number of organizations, such as the International Association of Dental
research (IADR) through Global Oral Health Inequalities: the Research Agenda
(GOHIRA have created awareness of the role of socioeconomic inequality in
access to care both within and between countries and have proposed new
research and mobilization of resources to be equably allocated to public health
17
programs ( Williams, 2014).
Some reported interventions to improve early detection
NICE (UK) Guidelines
Considering that survival rates in oral cancer patients had not improved for decades
the UK Department of Health (DoH),through the National Institute for Health and
Clinical Excellence (NICE) developed guidelines for the detection and referral of
head and neck cancers. These were set out in 2004 and recently revised. The
objective was to reduce any diagnostic delays that could occur in primary care.
These guidelines allowed all patients who met the DoH’s criteria for urgent (2-week)
referral to be referred directly to the designated oral and maxillofacial unit at a local
hospital or an oral medicine unit in a teaching dental hospital in the UK. The 2005
NICE guidelines for urgent referral in England and SIGN guidelines for Scotland
(http://sign.ac.uk/pdf/sign90.pdf) are collectively given below:
• Ulceration of oral mucosa persisting for more than 3 weeks
• Oral swellings persisting for more than 3 weeks
• All red or red and white patches of the oral mucosa
• Dysphagia persisting for more than 3 weeks
• Unexplained tooth mobility not associated with periodontaldisease
• Unresolved neck masses for more than 3 weeks.
Use of the 2-week waiting referral scheme in the UK was expected to provide rapid
access to secondary care facilities to confirm the diagnosis of suspected cancer.
NICE considered any referral criterion on the basis of a very low likelihood of cancer
and this 2005 guidance led to high proportion of false-positive referrals under the 2-
week wait system. An audit of 100 urgently referred cases to a secondary care
facility suggested that only 6% were subsequently confirmed with a cancer following
specialist investigations (Singh & Warnakulasuriya, 2006).
The revised NICE guideline (2016) includes only the first three symptoms of the
previous list, and the system suggests that red or white patches consistent with

18
leukoplakia or erythroplakia should be referred by GPs, but such patients are first
reviewed by a dentist prior to referral. This is so that dentists can exclude benign
disease such as geographic tongue and candida infection, which form a significant
proportion of false-positive referrals. Whether the revised guidelines will improve the
sensitivity of case detection remains to be seen.
Even persistent oral ulcers and erosions fail to arouse suspicion as this is a final
common manifestation, sometimes clinically indistinguishable, of a diverse spectrum
of conditions ranging from traumatic lesions, infectious diseases, systemic and local
immune-mediated conditions though a neoplastic ulcer need to considered on the
top of the list of the differential diagnosis drawn by a clinician. Compilato et al. (2009)
have, therefore, drawn up a guideline distinguishing simple, complex and destroying
(S-C-D system) ulcerations, as each requires different diagnostic evaluations and
referral priorities.
The UK was the first European country to establish national guidelines to facilitate
prompt referral of a suspected malignancy from primary to secondary care. The
availability of a government-funded National Health Service provides the cornerstone
for such a scheme and for an integrated care pathway. Countries with similar health
systems could attempt to reproduce the NICE referral guidelines to measure their
effectiveness. Based on the UK system, the Spanish Dental Council has introduced
a similar scheme to their dentists.
Spanish Oral Cancer Campaign
At a cost of €30,000 euros per year, the Spanish Dental Council has involved 2000- 3000 dentists per year (10% of Spain’s dental practitioners) in a national campaign
to promote early detection and prevention of oral cancer over the past 5 years. A
clinical guide on referral of malignancy suspected lesions (http://www.canceroral.es/)
was prepared, dentists attended a 4-hour course on early oral cancer diagnosis, and
received a free copy of a book on oral cancer. When evaluated among 440
participating dentists, the intervention appears to have improved the dentists’
knowledge, confirming the importance of this campaign (Seoane-Lestón et al.,
2010). Free oral screening was delivered over a 2-week period at volunteer private
19
dental clinics by 1700 dentists. An urgent pathway (similar to the UK) for the referral
of patients with suspicious lesions to maxillofacial surgery services was established,
but this has had an unbalanced impact in different regions. Furthermore, the Spanish
Dental Council found it difficult to persuade the public authority to actively participate
in this campaign.
Early Intervention in Oral Cancer in Portugal: The PIPCO program
In January 2014, a new initiative called Early Intervention in Oral Cancer (Projeto de
Intervençao Precoce de Cancro Oral; PIPCO) was officially approved in Portugal,
developed under the framework of the National Program of Oral Health Promotion,
and has been driven by the Portuguese Ministry of Health and the General Dental
Council. The program underpins easier access to primary care, more investigation
for oral symptoms and faster referral that could reduce the proportion of people
diagnosed with oral cancer at a later date.
As most of dental care is provided by dentists in private clinics, the aim of the
program is to involve private dentists in the oral cancer diagnostic process. The main
novelty of the Portuguese program is the combination of public and private
resources, and a joint doctor-dentist referral pathway for high-risk cases. The
program also benefits from the government underpinning payment for procedures
performed by private dentists enrolled on the project.
At the inception of the Project, all interested dentists working in Portugal were invited
to attend a 7-hour theoretical course on differential diagnosis of oral cancer and to
undertake a 1-hour evaluation of their knowledge on this topic and further calibration
on biopsy techniques. A total of 240 dentists were then selected based on the test
results and on geographical criteria (to achieve an appropriate distribution of
professionals involved across the country), to act as oral cancer diagnosticians. This
represented one selected dentist of 35 potential candidates each to provide care for
approximately 43,750 potential patients. The design of the study allows patients
visiting the family physician in the first instance (public health system) to be referred
to his/her dentist. The dentist is required to perform a screen and a differential
diagnosis at this visit (will receive a payment of $16 for the dentist check) and if

20
something suspicious is detected, he/she will perform a biopsy ($53). Biopsy will be
reported at the hospital laboratory (public health system) and the dentist will inform
the patient of the biopsy results and provide a referral to the nearest hospital for
further assessment.
From March to December 2014 (10 months), a total of 2,412 patients were referred
to dentists involved in this program for differential diagnosis. Biopsy samples were
taken in 320; 14 cases were confirmed as positive for oral cancer (0.5% of all
patients referred to a dentist by his/her GP and 4% of biopsies performed).
The Portuguese program is at an early stage for further evaluation, but represents
efforts by the government to enter a public-private partnership in an attempt to
develop a care pathway that will reduce diagnostic delays and combat difficulties to
access for care for high risk patients who may otherwise not visit a dentist. The
Portuguese program, if it proven successful in the coming years, could be
implemented in other countries with a particular focus on populations with low health
awareness and/or literacy, and taking into account its cost-effective approach for
affordable interventions in private clinics.
United States
State of Maryland
From early 2000 the State of Maryland in the US took a concerted effort to launch a
state-wide Comprehensive Oral Cancer Control Plan (Maybury, 2011). Over a 12
year period oral cancer examinations increased from a disturbingly low 20 percent to
40 percent of the population. The Maryland model not only included dentists but
other health professionals as well, including dental hygienists, physicians,
physician’s assistants and nurse practitioners. An early goal was to develop skills to
deliver diagnostic services in primary care and to address racial disparities in oral
cancer incidence. The Maryland model has demonstrated that a multi-sectorial
approach to provide education to the public and improving the skills of health
professionals can create substantial changes in the outcomes of oral cancer in a
state-wide population (Alfano, 2012). The steps taken by Marylanders may serve as
a model for other US states.
21
Detroit, Michigan
A social marketing campaign was launched in 2005-2007 to address excess
risk of oral cancer in Detroit tri-county area, Michigan. According to the 1998-2002
Surveillance Epidemiology and End Results data, rate of oral and pharyngeal cancer
(“oral cancer”) incidence among black males living in the Detroit tri-county
area (Macomb, Oakland, and Wayne) was one of the highest in the United States
(US) (25.7 per 100,000 persons) (Kolker, 2007). The Detroit Oral Cancer
Prevention Project, launched a multifaceted social marketing campaigns and
community outreach programs that primarily targeted black males living in the Detroit
tri-county area. During the campaign, 42 billboards, 1,327 radio adverticements
screened during 2 popular radio programs and 2 newspaper adverticements, were
used to increase awareness of high risk of oral cancer and promote free screening at
a clinic run by the project. In a community outreach intervention, 3 health educators
led 242 education sessions across 89 organizations. 1,020 adults were screened
and 78 were referred for further examinations (Ismail, 2012; Jedele, 2012). Dentists
and physicians in the area reported increased interest in oral cancer screening by
their patients. The authors’ data suggested that the campaign was more likely to be
associated with a decreasing trend of oral cancer incidence in the intervention
counties but caution should be taken in evaluating multiple factors that contribute to
the reduced oral cancer incidence rates and mortality because factors other than the
intervention may affect incidence and mortality rates such as reduced use of tobacco
products and advances in treating oral cancer. This study however, highlights a
potential impact of concerted efforts to improve the oral cancer awareness in the
high-risk communities.
South America
Retraining dentists in Argentina to reduce delays in diagnosis
Considering that the healthcare system for caring for oral cancer care in Argentina is
not coordinated systematically, in 1998 Oral Medicine academics introduced a data
gathering program that later led to a novel intervention.
Analysis of clinical data corresponding to 274 oral cancer (OSCC) patients
diagnosed and followed up for 5 years at the Oral Medicine Department of the
22
School of Dentistry of the University of Buenos Aires (FOUBA) (Brandizzi et al.,
2008), showed that 5-year survival rate was only 38%, and that the localizations with
worse prognosis were the floor of the mouth and tongue, with 19 and 27% 5-year
survival rate respectively. Morelatto et al (2007) in Córdoba province, Argentina,
further showed a 30-day professional delay in diagnosis in 68% of patients
diagnosed at stages I and II and 54% of patients diagnosed at stages III and IV.
Interestingly, professional delay was significantly longer in early stage cases. A
previous study involving an online survey conducted in alumni of the University of
Buenos Aires showed that only 30% of dentists routinely examine the oral mucosa.
In view of the above findings several strategies were implemented at different levels:
At the graduate teaching level, students were required to begin mandatory oral
examination of every patient by examining the tongue, especially the border of the
tongue. This strategy was adopted to try and change the habitual approach of
dentists. The second approach was to retrain the practicing dentists to undertake
routine screening and discuss their cases with regional specialists via tele-medicine.
More than 520 general dentists from different provinces throughout the country
received training including theory and practice work in seminar-based courses and
through an online hospital network. The training aimed to calibrate dentists to detect
potentially malignant disorders and oral cancer. Community specialists were
appointed to take appropriate photographs of suspicious oral lesions detected in
their region. These images were transmitted via e-mail in order for those in charge of
the region to establish presumptive diagnosis and mark the biopsy site/sites on the
photographic image. Difficult cases were analyzed and discussed by all the regional
heads.
After ten years of the program, the cases referred to the Oral Medicine
Department at the FOUBA were evaluated and compared to the data obtained
during the 10 years before implementing the project. In the second decade, 5-year
survival rate rose by 24%, increasing from 38% before the program to 62% after
implementation of the oral cancer prevention program described here. This
statistically significant change was more evident in tongue cancer survival rates,
which increased from 27% in the first period to 55% in the second.
In addition, the number of cases diagnosed at advanced stages of the disease (3
and 4) decreased from 66.3% to 50.7%.
23
Based on the results obtained with the project in Argentina, the International
Association for Dental Research (IADR) supported the implementation of an oral
cancer prevention program in Latin America, Through their Regional Development
Program. The program is currently underway in Venezuela, Panama, Colombia,
Peru, Uruguay, Chile, Paraguay and Argentina
Consequences of delayed diagnosis
The authors have thus far focused on the issues of poor prognosis and increased
morbidity resulting in poor quality of life for oral cancer survivors that could be
directly attributable to delays in diagnosis in either primary or secondary care. As a
result of delays, the increased cost burden of treating advanced cancers also
requires due consideration (Jacobson et al., 2012)
Despite the rising incidence of oral cancer and particularly oropharyngeal
cancers(OC/OP) and the potential for disability and disfigurement that may result
from treatment, published research on the direct and indirect cost burden of oral
cancer is limited. It may be hypothesized that early detection of cancers may
diminish the cost of care for individuals and employers, thus providing additional
impetus for more effective preventive efforts.
In the United States, an analysis of commercially-insured individuals revealed that
the average medical costs of OC/OP cancers in the first year after diagnosis was
$79,151, which is significantly higher than the cost to treat other cancers ($31,559-
$65,123) (Lawless, 2009; Short et al., 2011). Furthermore, individuals who received
surgery, radiation and chemotherapy (ie cases detected in advanced stages)
averaged $153,892 during the first year after diagnosis. These medical costs are
approximately twice any other reported cancer costs. These results are not
surprising given the multiple modalities of treatment driven by the significant number
of late or later stage diagnoses. Further, the average number of missed days of work
for those individuals who survived and were not disabled was 48.3 days compared to
other cancers at 44 days of missed work. Lastly, 52% of OC/OP cancer patients who
survived were permanently disabled and unable to return to work (Taylor, et al
2004). Therefore, delays in detection and diagnosis have a significant burden on
individuals as well as society.
24
Improving early diagnosis in primary care
The current standard for oral cancer detection in primary care in most countries is by
visual examination supplemented by palpation. Clinical skill building among primary
care practitioners should therefore be considered as a part of life-long learning.
As shown in a US study that pre and post tested knowledge on oral cancer ,
continuing education courses have a positive influence on participants' oral cancer
attitudes, knowledge, and behavior. Life long learning potentially could make a
difference, particularly on the earlier detection of asymptomatic lesions (Silverman et
al., 2010).
In most situations diagnostic and adjunctive diagnostic tests are essential
elements of healthcare delivery to confirm clinical findings of a suspicious
mucosal abnormality. These tests are designed to inform and guide decisions that
influence the course of illness and costs. Since the early 2000, a number of
adjunctive diagnostic and screening tests for oral squamous cell carcinoma have
been introduced These diagnostic tests are presented and discussed in detail by
Group 4 at the Forum.
Clinical and economic value for diagnostic tests can be established through the
following evaluation criteria:
� Feasibility (technical) of the dental office to produce consistent results
� Diagnostic accuracy as defined by sensitivity (false positive), specificity
(false negative) and positive and negative predictive values
� Impact on diagnostic and therapeutic thinking and behavior of the
dentist
� Impact on patient outcomes (improved outcomes)
� Impact on society (cost-effectiveness).
In the US, with the FDA approval of many commercial products, the field of
diagnostic testing is shifting the location of where this testing is conducted. With
today’s technology, there is a move away from central laboratory facilities to
point-of-care locations, such as outpatient treatment facilities and even
25
home-based tests. Home pregnancy tests and glucose monitoring are but two
examples of this shift. The extension to the dental office is within our grasp.
The OncAlert product, discussed in Group 4, represents a point of care
technology for oral cancer. These technologies have enhanced costs in the
short term, but could pay off in the future because of their potential to detect
cancers early.
In countries that lack a national health service, the commercial sector is central
to research, development and testing of diagnostic aids, and their input and
vision in partnership with governmental and academic organizations will be
essential for formulating solutions to early detection of cancer.
Conclusions
Every year half a million people are diagnosed with oral and oropharyngeal cancer
worldwide. On average 50% of them die with or of the disease within the first 5 years
of diagnosis. Diagnostic delay in the detection of oral and oropharyngeal cancers is
common. The data presented by our group has significant implications for future oral
cancer policy and planning cancer services. Clearly, late detections pose a major
public health challenge in most countries in the world. Some methodological issues
when researching referral delays in primary care need to be considered. We urge the
Forum to reflect on the overarching question on how to improve death rates from oral
cancer.
Although it is not known whether patient delay is a result of a lack of knowledge
with regard to oral cancer signs and symptoms, public education is still paramount
in raising people's awareness of oral cancer from an early age. To achieve this
goal, targeted education campaigns through media to alert the public about the
warning signs of oral cancer are needed. To reduce scheduling delays, medical and
dental school training about this disease must be improved. Opportunistic oral
cavity examinations with follow-up of suspicious lesions must be promoted to
reduce the burden of disease.

26
In addition, stronger evidence on the impact of delay on disease control could be
achieved through better measurement of delay duration. More detailed studies
relating delay to disease outcomes are needed. Views of patients and caregivers
are of critical importance for understanding any gaps in primary healthcare delivery.
Such evidence would underscore the need for programs to educate high-risk
persons and primary care providers about the importance of prompt referral in the
presence of symptoms, and may also provide a stronger argument than is currently
available for opportunistic screening of high-risk persons for oral cancer whenever
possible.
The study of patients’ visits to primary care facilities prior to a cancer diagnosis can
identify determinants and populations at risk of a delayed diagnosis. Development of
early detection guidelines will help to configure optimal diagnostic assessment
programs. Evidence-based guidelines with standards of care that suit local settings
are fundamental for improving the quality of care delivered when a person presents
to a GP or a dentist with a suspicious sign or symptom that needs an urgent referral.
Acknowledgements: We thank Dr Luis Monteiro (Oporto- Portugal) for conducting a
literature search on the stage of oral cancer and prognosis.
References
Johnson NW, Warnakulasuriya S, Gupta PC, Dimba E, Chindia M, Otoh EC, Sankaranarayanan R, Califano J, Kowalski L. Global oral health inequalities in incidence and outcomes for oral cancer: causes and solutions. Adv Dent Res. 2011 May;23(2):237-46.
Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009 Apr-May;45(4-5):309-16.
National Cancer Institute 2015. National Cancer Institute - Surveillance, Epidemiology, and End Results Program. SEER Stat fact sheets: oral cavity and pharynx cancer. seer.cancer.gov/statfacts/html/oralcav.html (accessed 23 December 2015).
Chan KK, Glenny AM, Weldon JC, Furness S, Worthington HV, Wakeford H Interventions for the treatment of oral and oropharyngeal cancers: targeted
27
therapy and immunotherapy. Cochrane Database Syst Rev. 2015 Dec 1;12:CD010341. doi: 10.1002/14651858.CD010341.pub2
Tromp DM, Brouha XD, Hordijk GJ, Winnubst JA, de Leeuw JR. Patient factors associated with delay in primary care among patients with head and neck carcinoma: a case-series analysis. Fam Pract. 2005 Oct;22(5):554-9.
Rodrigues PC, Miguel MCC, Bagordakis E, Fonseca FP et al. Clinicopathological prognostic factors of oral tongue squamous cell carcinoma: a retrospective study of 202 cases. International Journal Oral Maxillofacial Surgery 2014;43:475-801
Rikardsen OG, Bjerkli I-H, Uhlin-Hansen L, Hadler-Olsen E et al. Clinicopathological characteristics or oral squamous cell carcinoma in Northern Norway: a retrospective study. BMC Oral Health 2014;14:103
Monteiro L-S, Jose-Barbas do Amaral, Vizcaino J-R, Lopes C-A, Torres F-O. A clinical-pathological and survival study of oral squamous cell carcinomas from a population of the north of Portugal. Med Oral Path Oral Cir Bucal 2014;Mar 1:19(2) e120-6
Ling W,Mijiti A, Moming A. Survival Pattern and Prognostic Factors of Patients with Squamous Cell Carinoma of the Tongue: A Retrospective Analysis of 210 Cases. J Oral Maxillofac Surg 2013;71:775-785
Dissanayaka WL, Kumarasiri PVR, Liyanage RLP, Dias KD et al. Clinical and histopathologic parameters in survival or oral squamous cell carcinoma. Oral and Maxillofacial Pathology April 2012;113 No 4 April:518-525
Prugsanusak K, Peeravut S, Leelsmanit V et al. Survival and Prognostic Factors of Different Sites of Head and Neck Cancer: An Analysis from Thailand. Asian Pacific Journal of Cancer Prevention 2012; Vol 13:885-980
Jan J-C, Hsu W-H, Liu S-A, Wong Y-K et al. Prognostic Factors in Patients with Buccal Squamous Cell Carcinoma: 10 year Experience. J Oral Maxillofac Surg 2011; 69:396-404
Liu S-Y, Lu C-L,Chiou C-T, Yen C-Y et al. Surgical outcomes and prognostic factors of oral cancer associated with betel quid chewing and tobacco smoking in Taiwan. Oral Oncology 2010;46:276-282
Keppel M, Eich H T, Kubler A, Zoller JE, Scheer M. Prognostic Value of the Sixth Edition of the UIVV’s TNM Classification and Stage Grouping for Oral Cancer. Journal of Surgical Oncology 2010;102:443-449
Mosleh-Shirazi MS, Mohammadianpanah M, Mosleh-Shirazi MA. Squamous cell carcinoma of the oral tongue: a 25-year, single institution experience. The Journal of Laryngology& Otology 2009;123:114-120
28
Sargeran K, Murtomaa H, Safavi SMR, Vehkalahti MM, Teronen O. Survival after diagnosis of cancer of the oral cavity. British Journal of Oral and Maxillofacial Surgery 2008; 46:187-191
Lam L, Logan RM, Luke C, Rees Guy L. Retrospective study of survival and treatment pattern in a cohort of patients with oral and oropharyngeal tongue cancers from 1987 to 2004. Oral Oncology 2007;47:150-158
Aksu G, Karadeniz A, Saynak M, Fayda M et al. Treatment results and prognostic factors in oral tongue cancer: analysis of 80 patients. International Journal of Oral & Maxillofacial Surgery 2006;35:506-513
Kademani D, Bell RB, Bagheri S, Holmgren E, Dierks E, Potter B, Homer L. Prognostic factors in intraoral squamous cell carcinoma: the influence of histologic grade J Oral Maxillofac Surg. 2005 Nov;63(11):1599-605.
Pericot J, Escriba JM, Valdes Â, Biosca MJ, Monner,A, Castellsague X, Galiana R, Piulachs, P, Escutia E, Mari A. Survival evaluation of treatment modality in squamous cell carcinoma of the oral cavity and oropharynx. J Cranio-Maxillofacial Surgery 2000, 28, 49-55
Sciubba JJ. Oral cancer. The importance of early diagnosis and treatment. Am J Clin Dermatol 2001 2(4):239–51
Mücke T, Mitchell DA, Ritschl LM, Tannapfel A, Wolff KD, Kesting MR, Loeffelbein DJ, Kanatas A. Influence of tumor volume on survival in patients with oral squamous cell carcinoma. J Cancer Res Clin Oncol. 2015 Jun;141(6):1007-11.
Gómez I, Seoane J, Varela-Centelles P, Diz P, Takkouche B. Is diagnostic delay related to advanced-stage oral cancer? A meta-analysis. Eur J Oral Sci 2009; 117: 541–546
Goy J, Hall SF, Feldman-Stewart D, Groome PA, Diagnostic Delay and Disease Stage in Head and Neck Cancer: A Systematic Review. Laryngoscope 2009; 119:889–898
Cleveland JL, Thornton-Evans G. Total Diagnostic Delay in Oral Cancer may be Related to Advanced Disease Stage at Diagnosis. Journal Of Evidence-Based Dental Practice 2012 Jun;12(2):84-6.
Esmaelbeigi F, Hadji M, Harirchi I, Omranipour R, vand Rajabpour M, Zendehdel K. Factors affecting professional delay in diagnosis and treatment of oral cancer in Iran.Arch Iran Med 2014; 17: 253-7.
Gao W1, Guo CB. Factors related to delay in diagnosis of oral squamous cell carcinoma. J Oral Maxillofac Surg 2009; 67: 1015-20.
29
Joshi P, Nair S, Chaturvedi P, Nair D, Agarwal JP, D'Cruz AK. Delay in seeking specialized care for oral cancers: experience from a tertiary cancer center. Indian J Cancer 2014; 51: 95-7.
Morelatto RA, Herrera MC, Fernández EN, Corball AG, López de Blanc SA. Diagnostic delay of oral squamous cell carcinoma in two diagnosis centers in Córdoba Argentina. J Oral Pathol Med 2007; 36: 405-8.
Panzarella V, Pizzo G, Calvino F, Compilato D, Colella G, Campisi G. Diagnostic delay in oral squamous cell carcinoma: the role of cognitive and psychological variables.Int J Oral Sci 2014; 6: 39-45.
Peacock ZS, Pogrel MA, Schmidt BL. Exploring the reasons for delay in treatment of oral cancer. J Am Dent Assoc 2008; 139: 1346-52.
Sandoval M, Font R, Mañós M, Dicenta M, Quintana MJ, Bosch FX, et al. The role of vegetable and fruit consumption and other habits on survival following the diagnosis of oral cancer: a prospective study in Spain. Int J Oral Maxillofac Surg 2009; 38: 31-9.
Seoane J, Pita-Fernández S, Gómez I, Vazquez I, López-Cedrún JL, De Agustin D, et al. Proliferative activity and diagnostic delay in oral cancer. Head Neck 2010; 32: 1377-84.
Seoane-Romero JM, Vázquez-Mahía I, Seoane J, Varela-Centelles P, Tomás I, López-Cedrún JL. Factors related to late stage diagnosis of oral squamous cell carcinoma. Med Oral Patol Oral Cir Bucal 2012;1 7: e35-40.
Teppo H, Alho OP. Relative importance of diagnostic delays in different head and neck cancers. Clin Otolaryngol 2008; 33: 325-30.
Tong XJ, Shan ZF, Tang ZG, Guo XC. The impact of clinical prognostic factors on the survival of patients with oral squamous cell carcinoma.J Oral Maxillofac Surg 2014; 72: 2497. e1-10.
Gómez, I Warnakulasuriya S Varela-Centelles PI López-Jornet, P Suárez-Cunqueiro, M Diz-Dios, P Seoane, J . Is early diagnosis of oral cancer a feasible objective? Who is to blame for diagnostic delay?. Oral Diseases 2010; 16, 333–342
Güneri P, Epstein JB. Late stage diagnosis of oral cancer: components and possible solutions.Oral Oncol. 2014 Dec;50(12):1131-6.
Brouha XDR, Tromp DM, Hordijk GJ, Winnubst JAM, Leeuw RJ Oral and pharyngeal cancer: analysis of patient delay at different tumor stages . Head and Neck 2005; 27: 939-945.
Noonan B. Understanding the reasons why patients delay seeking treatment for oral cancer symptoms from a primary health care professional: an integrative literature review. Eur J Oncol Nurs. 2014 Feb;18(1):118-24
30
Scott SE, Grunfeld EA, Main J, McGurk M. Patient delay in oral cancer: a qualitative study of patients' experiences. Psychooncology. 2006 Jun;15(6):474-85.
Grant E, Silver K, Bauld L, Day R, Warnakulasuriya S. The experiences of young oral cancer patients in Scotland: symptom recognition and delays in seeking professional help. Br Dent J. 2010 May 22;208(10):465-71.
Warnakulasuriya S, Harris CK, Scarrott DM, Watt R, Gelbier S, Peters TJ, Johnson NW. An alarming lack of public awareness towards oral cancer. Br Dent J. 1999 Sep 25;187(6):319-22.
Kerr AR, Changrani JG, Gany FM, Cruz GD. An academic dental center grapples with oral cancer disparities: current collaboration and future opportunities. J Dent Educ. 2004 May;68(5):531-41.
Pitiphat W, Diehl SR, Laskaris G, Cartsos V, Douglass CW, Zavras AI. Factors associated with delay in the diagnosis of oral cancer. J Dent Res 2002; 81:192-197.
Onizawa K, Nishihara K, Yamagata K, Yusa H. Yanagawa T, Yoshide H . Factors associated with diagnostic delay of oral squamous cell carcinoma. Oral Oncol 2003; 39:781-788.
McGurk M, Chan C, Jones J, O’Regan E, Sherriff M. Delay in diagnosis and its effect on outcome in head and neck cancer. Br J Oral Maxillofac Surg 2005; 43: 281-284.
Brouha XDR, Tromp DM, Hordijk GJ, Winnubst JAM, Leeuw JRJ Role of alcohol and smoking in diagnostic delay in head and neck cancer patients. Acta Otolaryngeal 2005; 125: 552-556.
Kaing L, Manchella S, Love C, Nastri A, Wiesenfeld D. Referral Patterns for Oral Squamous Cell Carcinoma in Australia: 20 years progress. Aust Dent J. 2015 Mar 26. doi: 10.1111/adj.12314.
Seoane J, Alvarez-Novoa P, Gomez I, Takkouche B, Diz P, Warnakulasiruya S, Seoane-Romero JM, Varela-Centelles P. Early oral cancer diagnosis: The Aarhus statement perspective. A systematic review and meta-analysis. Head Neck. 2015 Mar 17. doi: 10.1002/hed.24050. [Epub ahead of print]
Weller D, Vedsted P, Rubin G, Walter FM, Emery J, Scott S, Campbell C, Andersen RS, Hamilton W, Olesen F, Rose P, Nafees S, van Rijswijk E, Hiom S, Muth C, Beyer M, Neal RD. The Aarhus statement: improving design and reporting of studies on early cancer diagnosis. Br J Cancer 2012; 106(7): 1262–1267.
Lyratzopoulos G, Abel GA, McPhail S, Neal RD, Rubin GP. Measures of promptness of cancer diagnosis in primary care: secondary analysis of national audit data on patients with 18 common and rarer cancers. Br J Cancer. 2013 Feb 19;108(3):686-90.
31
Seoane J, Pita-Fernández S, Gómez I, Vazquez I, López-Cedrún JL, De Agustin D, Varela-Centelles P. Proliferative activity and diagnostic delay in oral cancer. Head Neck. 2010 Oct;32(10):1377-84..
Evans SJ, Langdon JD, Rapidis AD, Johnson NW. Prognostic significance of STNMP and velocity of tumor growth in oral cancer. Cancer. 1982 Feb 15;49(4):773-6.
Scott SE, Grunfeld EA, McGurk M The idiosyncratic relationship between diagnostic delay and stage of oral squamous cell carcinoma. Oral Oncol. 2005 Apr;41(4):396-403.
Allison P, Franco E, Feine J (1998). Predictors of professional diagnostic delays for upper aerodigestive tract carcinoma. Oral Oncol 34: 127-132.
Kowalski LP, Franco EL, Torloni H, Fava AS, Sobrinho JA, Ramos G, Oliveira BV, Curado MP . Lateness of diagnosis of oral and oropharyngeal carcinoma: factors related to the tumour, the patient and health professionals. Oral Oncol 1994; 30B: 167-173
Scully C, Malmos D, Levers BGH, Porter SR, Prime SS. Sources and patterns of referrals of oral cancer: role of general practitioners. Br Med J 1986; 293: 599-601.
Schnelter JFC . Oral cancer diagnosis and delays in referral. Br J Oral Maxillofac Surg 1992; 30: 210-213.
Hollows P, McAndrew PG, Perini MG (2000). Delays in the referral and treatment of oral squamous cell carcinoma. Br Dent J 188: 262-265
Wildt J, Bundgaard T, Bentzen SM (1995). Delay in the diagnosis of oral squamous cell carcinoma. Clin Otolaryngol 20: 21-25.
Dimitroulis G, Reade P, Wiesenfeld D . Referral patterns of patients with oral squamous cell carcinoma, Australia. Oral Oncol 1992; 28: 23-27.
Morelatto RA, Herrera MC, Fernández EN, Corball AG, López de Blanc SA. Diagnostic delay of oral squamous cell carcinoma in two diagnosis centers in Córdoba Argentina. J Oral Pathol Med. 2007 Aug;36(7):405-8.
Crossman T, Warburton F, Richards MA, Smith H, Ramirez A, Forbes LJ. Role of general practice in the diagnosis of oral cancer. Br J Oral Maxillofac Surg. 2015 Dec 9. pii: S0266-4356(15)00670-1. doi: 10.1016/j.bjoms.2015.11.003.
Warnakulasuriya KAAS, Johnson NW (1999). Dentists and oral cancer prevention in the UK: opinions, attitudes and practices to screening for oral mucosal lesions and to counselling patients on tobacco and alcohol use: baseline data from 1991. Oral Dis 1999; 5: 10-14.
32
Onizawa K, Nishihara K, Yamagata K, Yusa H, Yanagawa T, Yoshide H (2003). Factors associated with diagnostic delay of oral squamous cell carcinoma. Oral Oncol 39: 781-788.
Guggenheimer J, Verbin RS, Johnson JT, Horkowitz CA, Myers EN . Factors delaying the diagnosis of oral and oropharingeal carcinomas. Cancer 1989 64: 932-935.
Alho OP, Teppo H, Mäntyselkä P, Kantola S. Head and neck cancer in primary care: presenting symptoms and the effect of delayed diagnosis of cancer cases. CMAJ. 2006 Mar 14;174(6):779-84.
Groome PA, Rohland SL, Hall SF, Irish J, Mackillop WJ, O'Sullivan B. A population-based study of factors associated with early versus late stage oral cavity cancer diagnoses. Oral Oncol. 2011 Jul;47(7):642-7
van Harten MC, de Ridder M, Hamming-Vrieze O, Smeele LE, Balm AJ, van den Brekel MW. The association of treatment delay and prognosis in head and neck squamous cell carcinoma (HNSCC) patients in a Dutch comprehensive cancer center. Oral Oncol. 2014 Apr;50(4):282-90.
van Harten MC, Hoebers FJ, Kross KW, van Werkhoven ED, van den Brekel MW, van Dijk BA. Determinants of treatment waiting times for head and neck cancer in the Netherlands and their relation to survival. Oral Oncol. 2015 Mar;51(3):272-8
Fanaras N, Warnakulasuriya S. Oral cancer diagnosis in primary care. Primary Dental Care 2016 (in press).
Varela-Centelles P, Pedrosa R, Lopez-Niño J, Sánchez M, Gonzalez-Mosquera A, Mendez A, Seoane J. Oral cancer awareness at chemist's and herbalist's shops: new targets for educational interventions to prevent diagnostic delay. Oral Oncol. 2012 Dec;48(12):1272-5.
Llewellyn CD, Johnson NW, Warnakulasuriya S . Factor associated with delay in presentation among younger patients and oral cancer. Oral Surg, Oral Med,Oral pathol, Oral Radiol Endod 2004; 97: 707-713.
Eadie D, MacKintosh AM, MacAskill S, Brown A. Development and evaluation of an early detection intervention for mouth cancer using a mass media approach. Br. J Cancer 2009;101:S73–9.
Nicotera G, Di Stasio SM, Angelillo IF. Knowledge and behaviors of primary care physicians on oral cancer in Italy. Oral Oncol. 2004 May;40(5):490-5.
33
Kerr AR. Lifesaving oral cancer screening. N Y State Dent J. 2000 Aug-Sep;66(7):26-30
Wade J, Smith H, Hankins M, Llewellyn C. Conducting oral examinations for cancer in general practice: what are the barriers? Fam Pract. 2010 Feb;27(1):77-84
Ajzen I. From intentions to action: a theory of planned behaviour. In Kuhl J, Beckman J (eds). Action Contrilo: From Cognitions to Behaviors, New York: Springer, 1985: 11–39
Paudyal P, Flohr FD, Llewellyn CD. A systematic review of patient acceptance of screening for oral cancer outside of dental care settings. Oral Oncol. 2014 Oct;50(10):956-62
Brocklehurst PR, Baker SR, Speight PM. A qualitative study examining the experience of primary care dentists in the detection and management of potentially malignant lesions. 1. Factors influencing detection and the decision to refer. Br Dent J. 2010 Jan 23;208(2):E3; discussion 72-3
Greenwood M, Lowry R J. Primary care clinicians’ knowledge of oral cancer: a study of dentists and doctors in the North East of England. Br Dent J 2001; 191: 510–512.
Macpherson LMD, McCann MF, Gibson J, Binnie VI, Stephen KW. The role of primary healthcare professionals in oral cancer prevention and detection. Br Dent J 2003; 195: 277–81
Varela-Centelles P, Insua A, Seoane-Romero JM, Warnakulasuriya S, Rapidis A, Diz P, Seoane J. Available web-based teaching resources for health care professionals on screening for oral cancer. Med Oral Patol Oral Cir Bucal. 2015 Mar 1;20(2):e144-9.
Wade et al., cáncer disparities by race, ethnicity and socioeconomic status. CA J Cancer Clin 2004; 54: 78-98.
Conway DI, Petticrew M, Marlborough H, Berthiller J, Hashibe M, Macpherson LM. Socioeconomic inequalities and oral cancer risk: a systematic review and meta-analysis of case-control studies. Int J Cancer. 2008 Jun 15;122(12):2811-9.
Freeman HP. Poverty, culture and social injustice: determinants of cáncer disparities.CA J Cancer Clin 2004; 54: 72-77.
Shavers VL, Harlan LC, Winn D, Davis WW. Racial/ethnic patterns of care for cancers of the oral cavity, pharynx, larynx, sinuses and salivary glands. Cancer and Metastasis Reviews 2003; 23; 25-38
G.A. Colditz, K.A. Atwood, K. Emmons, R.R. Monson, W.C. Willett, D. Trichopoulos & D.J. Hunter, for the Risk Index Working Group, Harvard Center for Cancer

34
Prevention. Harvard Report on Cancer Prevention ;Volume 4: Harvard Cancer Risk Index. Cancer Causes and Control 2000; 11: 477-488
Llewellyn CD, N.W Johnson NW, Warnakulasuriya S. Risk factors for squamous cell carcinoma of the oral cavity in young people—a comprehensive literature review. Oral Oncol, 2001, 37; 401–418
Robb K, stubbings S. Ramirez A, Austoker J, Walker J, Hiom S,, Warde J. Public awareness of cáncer in Britain: a population-based survey of adults. Br J Cancer 2009; 101; S18-23.
Morse DE, Kerr AR. Disparities in oral and pharyngeal cancer incidence, mortality and survival among black and white Americans. J Am Dent Assoc. 2006 Feb;137(2):203-12.
Williams DM. The research agenda on oral health inequalities: the IADR-GOHIRA initiative. Med Princ Pract. 2014;23 Suppl 1:52-9.
NICE Guidelines on Cancer Services. Improving Outcomes in Head and Neck Cancers. the manual. London: NICE, 2004.
Singh P , Warnakulasuriya S. The two-week wait cancer initiative on oral cancer; the predictive value of urgent referrals to an oral medicine unit. Br Dent J. 2006 Dec 9;201(11):717-20; discussion 714.
Compilato D, Cirillo N, Termine N, Kerr AR, Paderni C, Ciavarella D, Campisi G. Long-standing oral ulcers: proposal for a new 'S-C-D classification system'. J Oral Pathol Med. 2009 Mar;38(3):241-53.
Seoane-Lestón J), Velo-Noya J, Warnakulasuriya S, Varela-Centelles P, Gonzalez-Mosquera A, Villa-Vigil MA, Rodríguez-Lozano F, Diz-Dios P. Knowledge of oral cancer and preventive attitudes of Spanish dentists. Primary effects of a pilot educational intervention. Med Oral Patol Oral Cir Bucal. 2010 May 1;15(3):e422-6.
Maybury C, Horowitz AM, Goodman HS.Outcomes of oral cancer early detection and prevention statewide model in Maryland. J Public Health Dent. 2012 Winter;72 Suppl 1:S34-8.
Alfano MC. Commentry on “Outcomes of oral cancer early detection and prevention statewide model in Maryland”. J Public Health Dent. 2012; 72; S40.
Kolker JL, Ismail AI, Sohn W, Ramaswami N. Trends in the incidence, mortality, and survival rates of oral and pharyngeal cancer in a high-risk area in Michigan, USA. Community Dent Oral Epidemiol 2007;35:489-499.
Ismail AI, Jedele JM, Lim S, Tellez M. A marketing campaign to promote screening for oral cancer. J AM Dent Assoc 2012;143(9):e57-66.
35
Jedele JM, Ismail AI. Evaluation of a multifaceted social marketing campaign to increase awareness of and screening for oral cancer in African Americans. Community Dent Oral Epidemiol 2010;38:371-382.
Brandizzi D, Gandolfo M, Velasco ML, Cabrini RL and Lanfranchi H, Clinical features and evolution of oral cancer: A study of 274 cases in Buenos Aires, Argentina. Med Oral Patol Oral Cir Bucal 2008, E 544-8
Jacobson, JJ, et al.: The cost burden of oral, oral pharyngeal, and salivary gland cancers in three groups: commercial insurance, Medicare, and Medicaid,Head &
Neck Oncology 2012, 4:15
Lawless GD: The Working Patient with Cancer: Implications for Payers and Employers. American Health and Drug Benefits. 2009, 2(4):168-73.
Short P, Moran J, Rajeshwari P: Medical expenditures of adult cancer survivors aged <65 years in the United States.Cancer. 2011,117(12); 2791-2800.
Taylor JC, Terrell JE, Ronis DL, Fowler KE, Bishop C, Lambert MT, Myers LL, Duffy SA, Bradford CR, Chepeha DB, Hogikyan ND, Prince ME, Teknos TN, Wolf GT: Disability in patients with head and neck cancer. Arch Otolaryngol Head Neck Surg. 2004, 130(6):764-9.
Silverman S Jr, Kerr AR, Epstein JB. Oral and pharyngeal cancer control and
early detection. J Cancer Educ. 2010 Sep;25(3):279-81
___________________________________________________________________
Fig 1. Kaplan Meier curves illustrating survival in relation to stage of disease in 7
studies published from 2005-2015 from various countries.
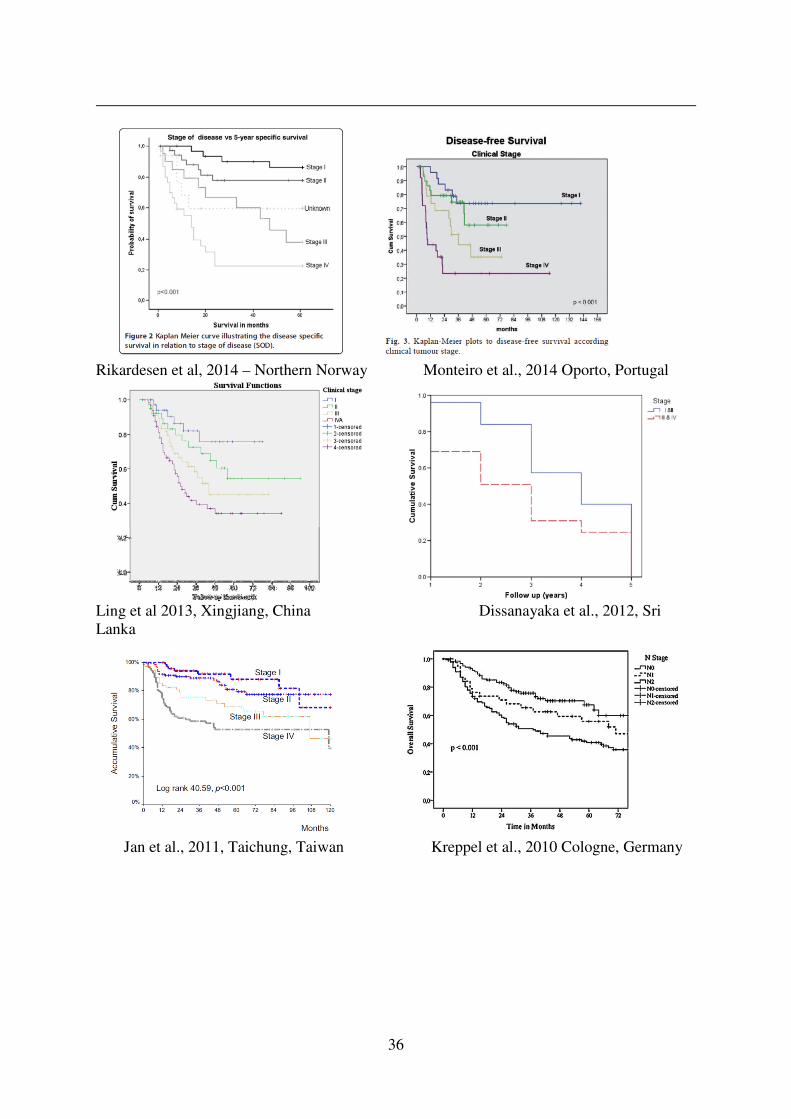
36
Rikardesen et al, 2014 – Northern Norway Monteiro et al., 2014 Oporto, Portugal
Ling et al 2013, Xingjiang, China Dissanayaka et al., 2012, Sri
Lanka
Jan et al., 2011, Taichung, Taiwan Kreppel et al., 2010 Cologne, Germany

37
Sargeran et al 2008, Finland Lam et al., 2007, Adelaide, Australia
Kademani et al 2005. Mayo Clinic, USA
Figs 2 A and B . Types /Stages of diagnostic delay in oral cancer (Gomez et al., 2008; Guneri & Epstein, 2014)
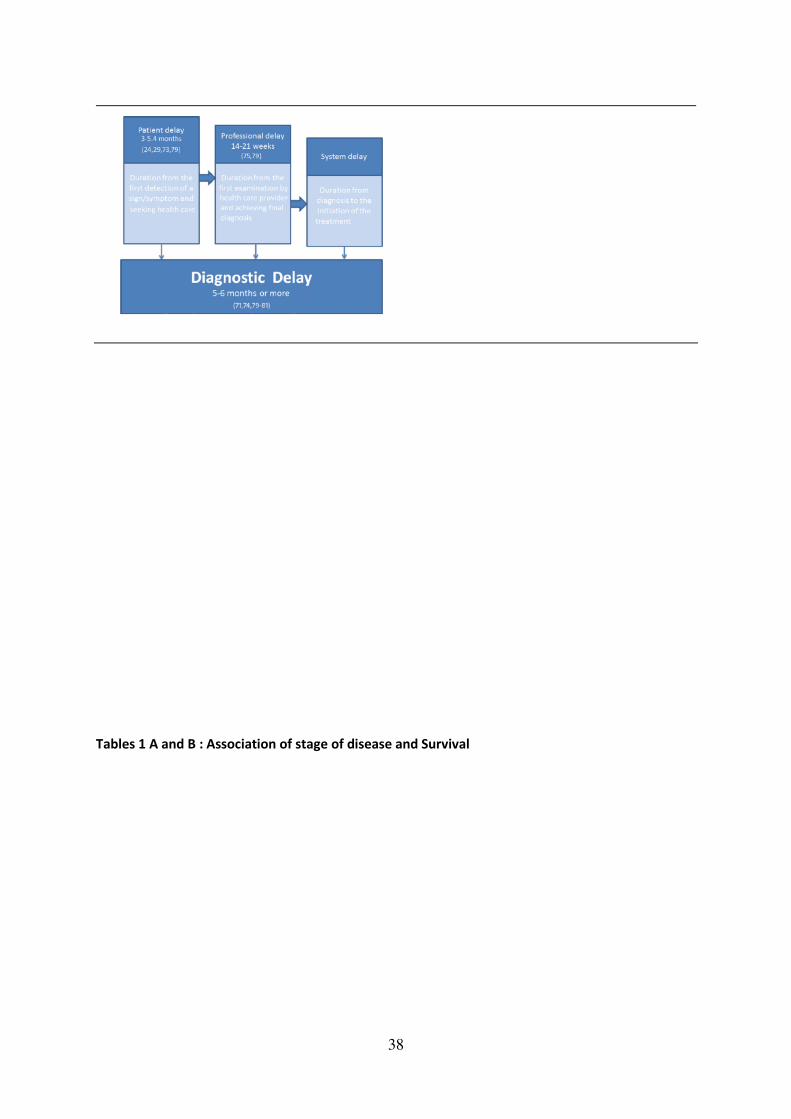
38
Tables 1 A and B : Association of stage of disease and Survival

39
Table 2 – Five- year survival rates in Oral Squamous Cell Carcinomas
Stage TMN classification 5-Year survival
rate (%)
I T1N0M0
(primary tumour less than 2cm)
85
II T2N0M0
(primary tumour between 2 and 4 cm)
66
Author N Location Survival Stage I & II Stage III & IV OR (HR) CI Adjusted variables
Rodrigues et al , 2014 202 TSCC DSS 80% 48.8% 2.12 (1.21-4.39) stage, smoking
Rikardsen et al , 2014 133 OSCC DSS I - 13%;
II - 20%
III - 50%
IV - 70%
NR primary site, stage, smoking and drinking
Monteiro et al , 2014 128 OSCC DFS I -78.9%
II - 74.6%
III - 51.3%
IV - 23.5%
I/III - 3.464 (1.158-10.360)
I/IV - 7.529 (2.707-20.937)
T status, N status, clinical stage, treatment option,
tumour grade, perineural permeation
Ling et al , 2013 210 TSCC DSS I - 75.7%
II - 54.4%
III - 45%
IV - 34.1%
I/IVa - 5.325 (1.765-1.256) tumor invasion depth, perineural invasion, resection
margin, treatment, stage
Dissanayaka et al , 2012 193 OSCC OS 73.3% 41.8% 0.382 stage, pattern of invasion, excision margins
Pruegsanusak et al , 2012 1186 HNC OS I - 45.7%
II - 37.5%
III - 20.1%
IV - 14.8%
I/III - 1.93 (1.24-3.00)
I/IV - 2.70 (1.80-4.06)
age, gender, treatment, stage, differentiation
Jan et al , 2011 394 BSCC OS I - 88.2%
II - 79.36%
III - 68.6%
IV - 52.1%
I/III - 2.88 (1.06-7.84)
I/IV - 3.38 (1.35-8.45)
surgical margins, cervical nodal metastasis, stage
Liu et al , 2010 698 OSCC CDSS I - 84%
II - 77%
III - 58%
IV - 37%
1.76 (1.3–2.5) alcohol drinking, level of nodal metastasis, stage,
differentiation, treatment failure
Kreppel et al , 2010 300 OC OS I - 82.9%
II - 70.1%
III - 57.4%
IVa - 45.9%
IVb - 34.3%
I/III - 5.127 (1.185–22.182)
I/IVa - 6.128 (1.500–25.031)
I/IVb - 8.116 (1.896–34.735)
age, UICC stage
Mosleh-Shirazi et al , 2008 102 TSCC OS I - 85.7%
II - 81.2%
III - 60.8%
IV - 49.2%
1.521 (0.986–2.346) stage, treatment
Sargeran et al, 2008 480 OC OS I - 51%
II - 44%
III - 13%
IV - 12%
I/III - 2.8 (1.8-4.4)
I/IV - 4.6 (3.1-6.8)
gender, age, treatment, stage, histology
Lam et al , 2007 212 TSCC DSS I/II - >50% III/IV - <40% I/IV - 2.81 (1.85-4.26) age, clinical stage
Aksu et al , 2006 80 TSCC OS I - 100%
II - 60%
III - 48%
IV - 17%
0.2 (0.07–0.54) stage, treatment type, loco-regional recurrence, tumour
size, T stage, N stage, systemic recurrence, tumour
Kademani et al , 2005 233 OSCC OS NR NR p = 0.014 NR
Pericot et al , 2000 88 OOSCC OS I - 81.8%
II - 69.5%
III - 78.%
IV - 47.9%
I/IV - 8.28 (1.46-47.00) stage, site, treatment, recurrence
TSCC, tongue squamous cell carcinoma; OSCC, oral squamous cell carcinoma; HNC, head and neck cancer; OC, oral cancer; OOSCC, oral and oropharynx squamous cell
carcinoma; DSS, disease-specific survival; DFS, disease-free survival; OS, overall survival; CDSS, cumulative disease-specific survival; NR, not referred.
Author N Location Survival Factors significant with survival Factors not found to be significant
Rodrigues et al , 2014 202 TSCC DSSstage; smoking age, gender, ethinicity, drinking habits, surgical margins
Rikardsen et al , 2014 133 OSCC DSSstage
age, tumour differenciation, primary site, smoking, p16
status
Monteiro et al , 2014 128 OSCC DFSclinical stage
age, gender, smoking, alcohol habits, margin status,
lymphatic invasion
Ling et al , 2013 210 TSCC DSS tumor invasion depth, perineural invasion,
treatment type, stagegender, age, residence, smoking habits, subsite
Dissanayaka et al , 2012 193 OSCC OSstage, pattern of invasion, excision margins age, gender, host response, presence of eosinophils
Pruegsanusak et al , 2012 1186 HNC OS stage, treatment, differentiation, age > 80
yearsgender
Jan et al , 2011 394 BSCC OS surgical margins, cervical nodal metastasis,
stageage; histological grade
Liu et al , 2010 698 OSCC CDSS alcohol drinking, level of nodal metastasis,
stage, differentiation, treatment failuregender, age, smoking habits, diagnostic delay
Kreppel et al , 2010 300 OC OS age, UICC stage gender, tumour site
Mosleh-Shirazi et al , 2008 102 TSCC OS stage, treatment gender, margin status, RT dose
Sargeran et al, 2008 480 OC OS stage, treatment gender, age, histology
Lam et al , 2007 212 TSCC DSS age, clinical stage gender, residence, multiple primaries
Aksu et al , 2006 80 TSCC OS stage, treatment type, loco-regional
recurrenceage, gender, alcohol consumption, smoking history
Kademani et al , 2005 233 OSCC OS stage, grade age, gender, race, tumor site, positive margins
Pericot et al , 2000 88 OOSCC OS stage, treatment, recurrence sex, age, neck surgery
TSCC, tongue squamous cell carcinoma; OSCC, oral squamous cell carcinoma; HNC, head and neck cancer; OC, oral cancer; OOSCC, oral and oropharynx squamous cell
carcinoma; DSS, disease-specific survival; DFS, disease-free survival; OS, overall survival; CDSS, cumulative disease-specific survival; NR, not referred.
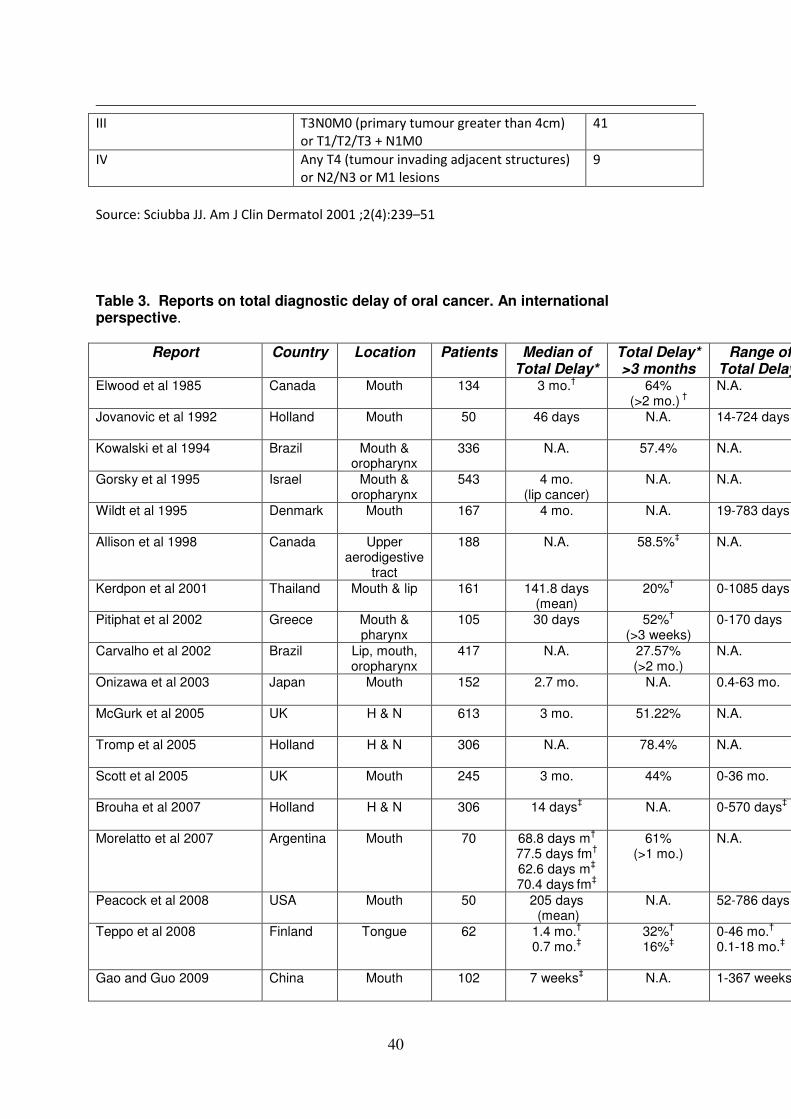
40
III T3N0M0 (primary tumour greater than 4cm)
or T1/T2/T3 + N1M0
41
IV Any T4 (tumour invading adjacent structures)
or N2/N3 or M1 lesions
9
Source: Sciubba JJ. Am J Clin Dermatol 2001 ;2(4):239–51
Table 3. Reports on total diagnostic delay of oral cancer. An international perspective.
Report Country Location Patients Median of Total Delay*
Total Delay* >3 months
Range of Total Delay*
Elwood et al 1985 Canada Mouth 134 3 mo.† 64% (>2 mo.) †
N.A.
Jovanovic et al 1992
Holland Mouth 50 46 days N.A. 14-724 days
Kowalski et al 1994 Brazil Mouth & oropharynx
336 N.A. 57.4% N.A.
Gorsky et al 1995 Israel Mouth & oropharynx
543 4 mo. (lip cancer)
N.A. N.A.
Wildt et al 1995
Denmark Mouth 167 4 mo. N.A. 19-783 days
Allison et al 1998 Canada Upper aerodigestive
tract
188 N.A. 58.5%‡ N.A.
Kerdpon et al 2001 Thailand Mouth & lip 161 141.8 days (mean)
20%† 0-1085 days
Pitiphat et al 2002 Greece Mouth & pharynx
105 30 days 52%† (>3 weeks)
0-170 days
Carvalho et al 2002 Brazil Lip, mouth, oropharynx
417 N.A. 27.57% (>2 mo.)
N.A.
Onizawa et al 2003
Japan Mouth 152 2.7 mo. N.A. 0.4-63 mo.
McGurk et al 2005
UK H & N 613 3 mo. 51.22% N.A.
Tromp et al 2005
Holland H & N 306 N.A. 78.4% N.A.
Scott et al 2005
UK Mouth 245 3 mo. 44% 0-36 mo.
Brouha et al 2007
Holland H & N 306 14 days‡ N.A. 0-570 days‡
Morelatto et al 2007
Argentina Mouth 70 68.8 days m† 77.5 days fm†
62.6 days m‡
70.4 days fm‡
61% (>1 mo.)
N.A.
Peacock et al 2008 USA Mouth 50 205 days (mean)
N.A. 52-786 days
Teppo et al 2008 Finland Tongue 62 1.4 mo.† 0.7 mo.‡
32%†
16%‡ 0-46 mo.† 0.1-18 mo.‡
Gao and Guo 2009 China Mouth 102 7 weeks‡ N.A. 1-367 weeks

41
Sandoval et al 2009
Spain Mouth 146 N.A. 37.7% N.A.
Seoane et al 2010 Spain Mouth 63 1.5 mo. 38.1% (>1.5 mo.)
0.5-12 mo.
Seoane Romero et al 2012 Spain Mouth 66 45 days 45.5% N.A.
Joshi et al 2014 India Mouth 201 7 mo. 50% 1-36 mo.
Panzarella et al 2014 Italy Mouth 156 N.A. 32% (>1 mo.)†
N.A.
Tong et al 2014 China Mouth 77 4.1 mo. (mean)
62.4% 1-18 mo.
Esmaelbeigi et al 2014 Iran Mouth 206
140 days N.A. 36-430 days
*Total delay: From the patient´s first becoming aware to commencement of definitive treatment; †
Patient delay: From the onset of symptoms to the first medical visit; ‡Professional delay: From the first medical visit to the diagnosis; N.A.: Not available; mo: Months; H&N: Head and neck; m: Males; fm: Females;
Table 4: Factors associated with patient delay and oral cancer ; From a systematic Review conducted by Noonan (2014)
Author &
publication
year
Focus Design Sample Findings: Factors associated with patient
delay and oral cancer
Kerdpon and
Sriplung,
2001
To investigate the
factors related to
patient and professional
delay in diagnosis of
oral cancer
Quantitative
Structured
questionnaire
n = 161 Prolonged patient delay associated with the
use of traditional herbal medicine.
No significant association between any
other variables investigated (sex, age,
marital status, religion, area of residence
etc)
Kumar et al.,
2001
To analyse the
psychosocial factors
related to delay in
presentation of oral
cancer patients
Quantitative
Questionnaire
n = 79 Ill-fated to have cancer (fate)
Cancer a curse
Non-availability of transport
trivial ulcers in mouth (symptom
interpretation)
Socioeconomic status was associated
(univariate analysis) with patient delay in
India Belief that prolonged treatment
renders the family stressful
Pitiphat et al.,
2002
To identify factors
associated with delay in
the diagnosis of oral
cancer
Explorative
Quantitative
Structured
Questionnaire
n = 105 Non smokers/Former Smokers have a
significantly higher risk of delay than
current smokers (no association with the
quantity consumed)
No association between delay and alcohol
use
No association between age, gender and
education with delay.
Strong association between sexually
transmitted disease and delay in diagnosis
Onizawa
et al., 2003
To analyze factors
contributing to delay in
the diagnosis of oral
cancer
Quantitative
Retrospective
case study
analyses
n = 152 There was no significant association
between delay and gender, age, past
history of malignant disease, number of
family members living in the same house,
daily medication, employment, tobacco use
or alcohol consumption
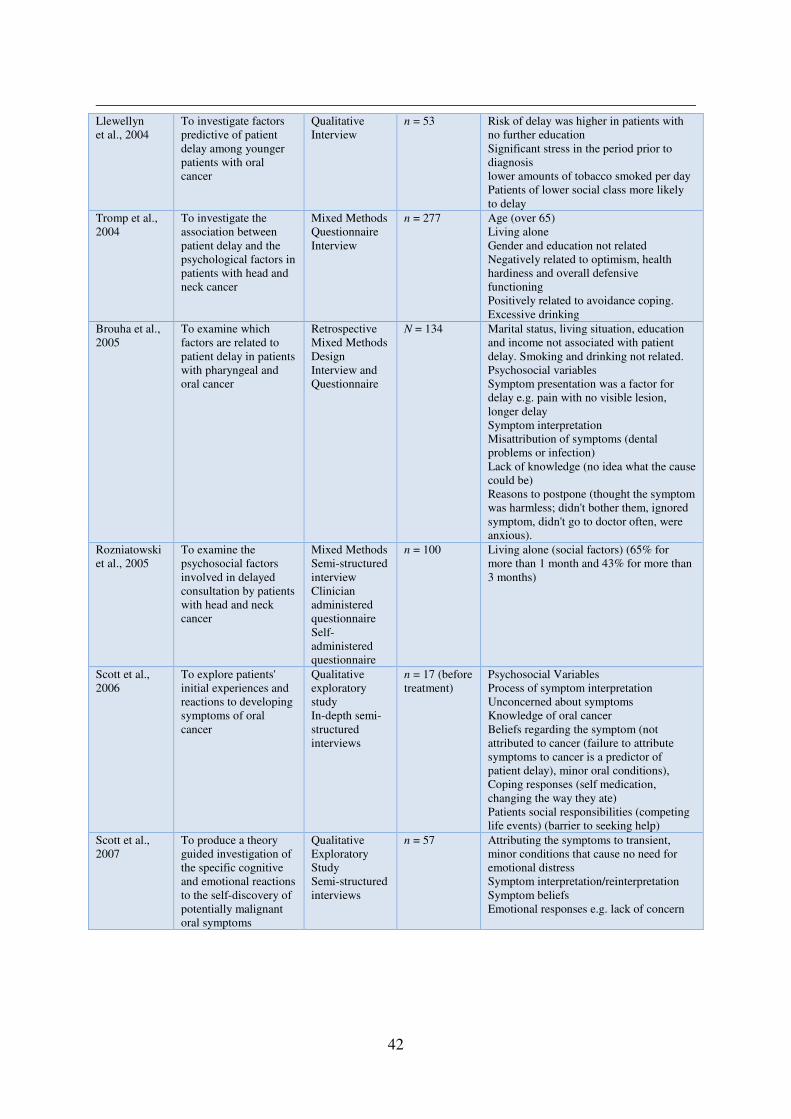
42
Llewellyn
et al., 2004
To investigate factors
predictive of patient
delay among younger
patients with oral
cancer
Qualitative
Interview
n = 53 Risk of delay was higher in patients with
no further education
Significant stress in the period prior to
diagnosis
lower amounts of tobacco smoked per day
Patients of lower social class more likely
to delay
Tromp et al.,
2004
To investigate the
association between
patient delay and the
psychological factors in
patients with head and
neck cancer
Mixed Methods
Questionnaire
Interview
n = 277 Age (over 65)
Living alone
Gender and education not related
Negatively related to optimism, health
hardiness and overall defensive
functioning
Positively related to avoidance coping.
Excessive drinking
Brouha et al.,
2005
To examine which
factors are related to
patient delay in patients
with pharyngeal and
oral cancer
Retrospective
Mixed Methods
Design
Interview and
Questionnaire
N = 134 Marital status, living situation, education
and income not associated with patient
delay. Smoking and drinking not related.
Psychosocial variables
Symptom presentation was a factor for
delay e.g. pain with no visible lesion,
longer delay
Symptom interpretation
Misattribution of symptoms (dental
problems or infection)
Lack of knowledge (no idea what the cause
could be)
Reasons to postpone (thought the symptom
was harmless; didn't bother them, ignored
symptom, didn't go to doctor often, were
anxious).
Rozniatowski
et al., 2005
To examine the
psychosocial factors
involved in delayed
consultation by patients
with head and neck
cancer
Mixed Methods
Semi-structured
interview
Clinician
administered
questionnaire
Self-
administered
questionnaire
n = 100 Living alone (social factors) (65% for
more than 1 month and 43% for more than
3 months)
Scott et al.,
2006
To explore patients'
initial experiences and
reactions to developing
symptoms of oral
cancer
Qualitative
exploratory
study
In-depth semi-
structured
interviews
n = 17 (before
treatment)
Psychosocial Variables
Process of symptom interpretation
Unconcerned about symptoms
Knowledge of oral cancer
Beliefs regarding the symptom (not
attributed to cancer (failure to attribute
symptoms to cancer is a predictor of
patient delay), minor oral conditions),
Coping responses (self medication,
changing the way they ate)
Patients social responsibilities (competing
life events) (barrier to seeking help)
Scott et al.,
2007
To produce a theory
guided investigation of
the specific cognitive
and emotional reactions
to the self-discovery of
potentially malignant
oral symptoms
Qualitative
Exploratory
Study
Semi-structured
interviews
n = 57 Attributing the symptoms to transient,
minor conditions that cause no need for
emotional distress
Symptom interpretation/reinterpretation
Symptom beliefs
Emotional responses e.g. lack of concern
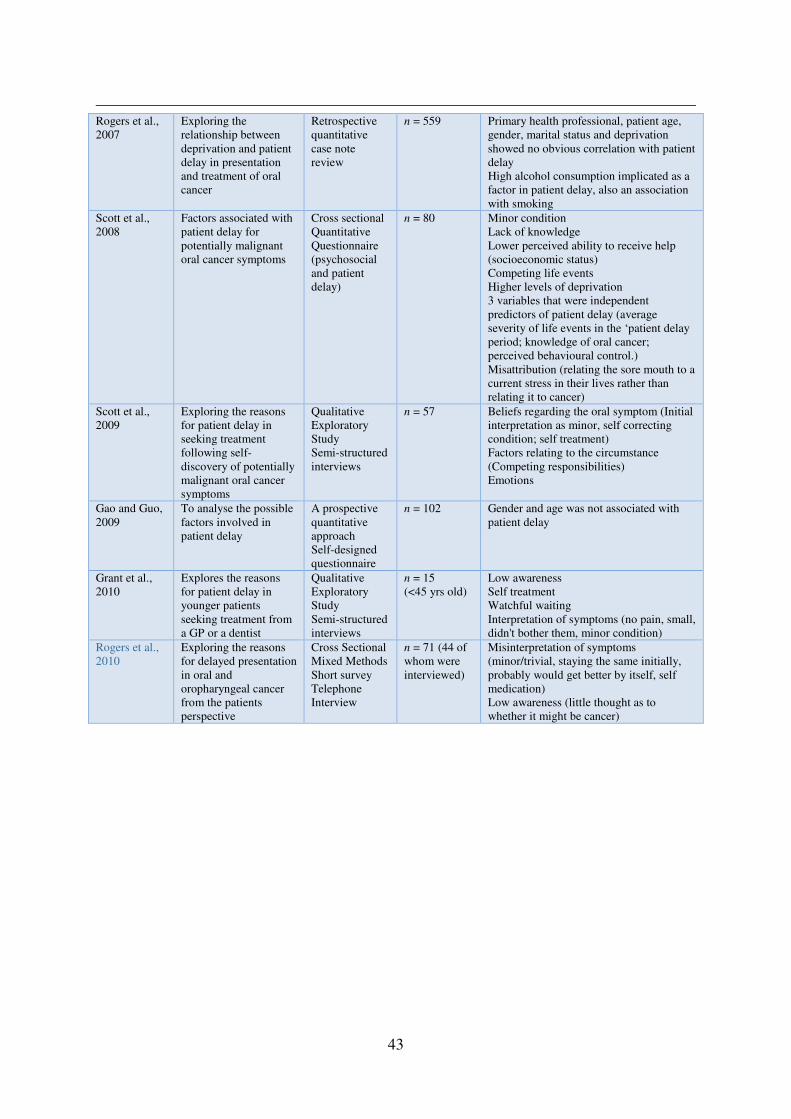
43
Rogers et al.,
2007
Exploring the
relationship between
deprivation and patient
delay in presentation
and treatment of oral
cancer
Retrospective
quantitative
case note
review
n = 559 Primary health professional, patient age,
gender, marital status and deprivation
showed no obvious correlation with patient
delay
High alcohol consumption implicated as a
factor in patient delay, also an association
with smoking
Scott et al.,
2008
Factors associated with
patient delay for
potentially malignant
oral cancer symptoms
Cross sectional
Quantitative
Questionnaire
(psychosocial
and patient
delay)
n = 80 Minor condition
Lack of knowledge
Lower perceived ability to receive help
(socioeconomic status)
Competing life events
Higher levels of deprivation
3 variables that were independent
predictors of patient delay (average
severity of life events in the ‘patient delay
period; knowledge of oral cancer;
perceived behavioural control.)
Misattribution (relating the sore mouth to a
current stress in their lives rather than
relating it to cancer)
Scott et al.,
2009
Exploring the reasons
for patient delay in
seeking treatment
following self-
discovery of potentially
malignant oral cancer
symptoms
Qualitative
Exploratory
Study
Semi-structured
interviews
n = 57 Beliefs regarding the oral symptom (Initial
interpretation as minor, self correcting
condition; self treatment)
Factors relating to the circumstance
(Competing responsibilities)
Emotions
Gao and Guo,
2009
To analyse the possible
factors involved in
patient delay
A prospective
quantitative
approach
Self-designed
questionnaire
n = 102 Gender and age was not associated with
patient delay
Grant et al.,
2010
Explores the reasons
for patient delay in
younger patients
seeking treatment from
a GP or a dentist
Qualitative
Exploratory
Study
Semi-structured
interviews
n = 15
(<45 yrs old)
Low awareness
Self treatment
Watchful waiting
Interpretation of symptoms (no pain, small,
didn't bother them, minor condition)
Rogers et al.,
2010
Exploring the reasons
for delayed presentation
in oral and
oropharyngeal cancer
from the patients
perspective
Cross Sectional
Mixed Methods
Short survey
Telephone
Interview
n = 71 (44 of
whom were
interviewed)
Misinterpretation of symptoms
(minor/trivial, staying the same initially,
probably would get better by itself, self
medication)
Low awareness (little thought as to
whether it might be cancer)

44