gi grand rounds johanna chan gastroenterology fellow baylor college of medicine 6/27/13
TRANSCRIPT

GI Grand Rounds
Johanna ChanGastroenterology FellowBaylor College of Medicine6/27/13

No conflicts of interestNo financial disclosures

HPI•RFC: abnormal liver function tests•39yo transvestite man with DM1, frequent
hospitalizations for DKA•Admitted to hospital 4/4/13 with DKA•ALT 765, AST 629, total bilirubin 0.5, alk
phos 229, albumin 3.4•No documented hypotension, no available
INR, no other specific GI symptoms•Referred to GI clinic for follow up of LFTs

Past Medical History
•DM1, diagnosed in his 20s▫poorly controlled (Hgb A1c 13.7%)▫frequent hospitalizations for DKA▫complicated by peripheral neuropathy▫chronic early satiety and nausea (?
gastroparesis)•HTN•HLD•Hypothyroid
Medications
• Insulin•Gabapentin•Enalapril•Esomeprazole 20 mg PO daily•Simvastatin 40 mg PO QHS (stopped after
4/2013)•Levothyroxine 100 mcg PO daily•Tylenol 500 mg PO BID (stopped after
4/2013)•No herbs or supplements
HPI continued
•Presents to GI clinic approximately 6 weeks post-hospitalization
•Malaise, poor appetite, nausea, vomiting of clear yellow emesis, early satiety
•Clearly now markedly jaundiced, scleral icterus
•No abdominal pain, change in stools•60 lb unintentional weight loss over the
past 10 years

Other history•Family history
▫Mother DM2▫Brother DM1, HTN, HLD▫No rheumatologic or other autoimmune disease▫No family history of liver disease
•Social history▫Complete EtOH abstinence▫No history of IVDA or tobacco▫No blood transfusions or tattoos▫Unprotected sex (MSM)▫“Black market” hormone injections, Mexico,
1990s
Exam•T 98.2, BP 113/72, HR 85, RR 12, O2 sat 99%
RA•5’8”, 189 lbs•Gen: markedly jaundiced, AAOx4, NAD,
groomed casually in women’s clothing•HEENT: marked scleral icterus•Neck: supple, no LAD•CV: RRR no m/r/g•Chest: no spider angiomata, no gynecomastia•Lungs: CTAB no wheezes/rales/rhonchi•Abd: S/NT/ND, NABS, no fluid wave•Ext: no edema
Available labs
HIV negative
HAV IgM negative
HBsAg positive (negative in 2008)HBcAb IgM positive (negative in 2008)HBV DNA PCR 108,000,000HBV DNA log 10 8.04
HCV IgG negative
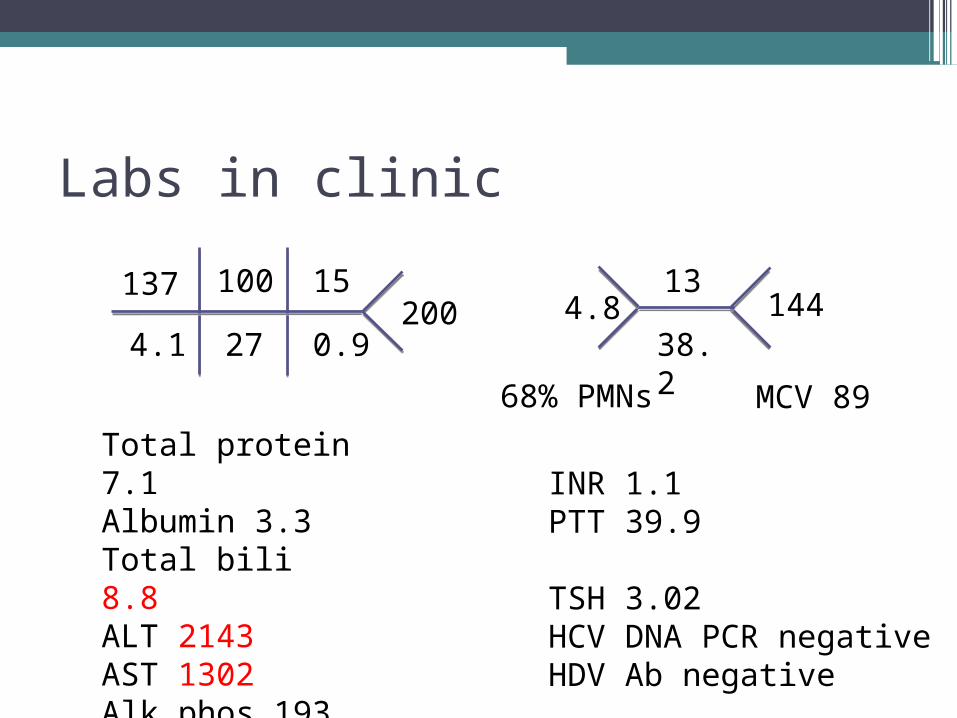
Labs in clinic
MCV 8968% PMNs
Total protein 7.1Albumin 3.3 Total bili 8.8 ALT 2143 AST 1302 Alk phos 193
INR 1.1 PTT 39.9
TSH 3.02HCV DNA PCR negativeHDV Ab negative
137
4.1 27
100 15
0.9200 4.8
38.2
13144
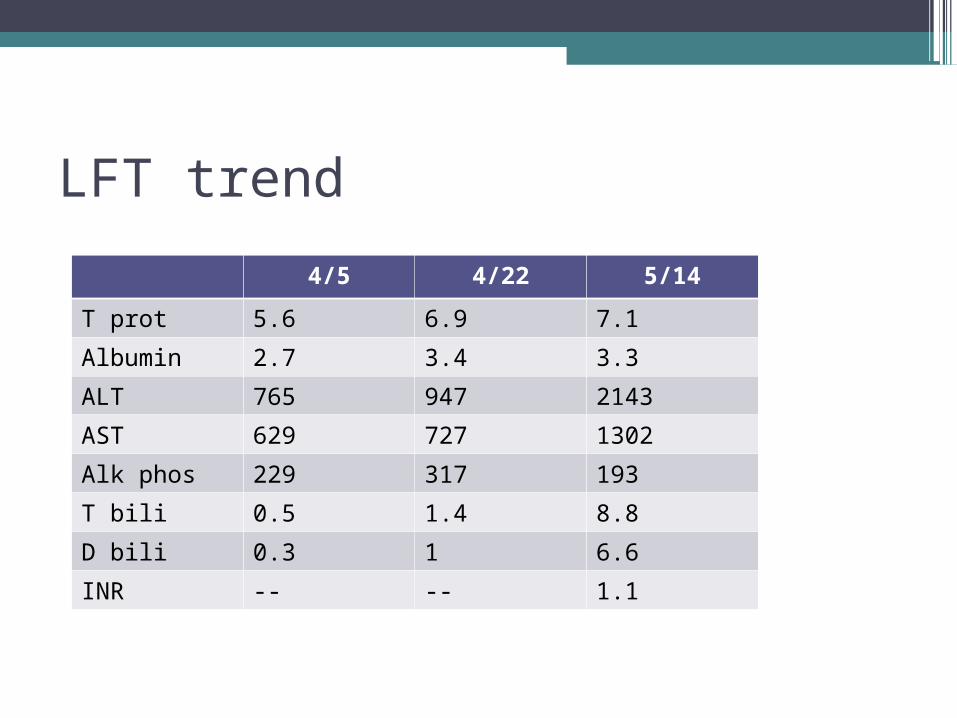
LFT trend
4/5 4/22 5/14
T prot 5.6 6.9 7.1
Albumin 2.7 3.4 3.3
ALT 765 947 2143
AST 629 727 1302
Alk phos 229 317 193
T bili 0.5 1.4 8.8
D bili 0.3 1 6.6
INR -- -- 1.1
Imaging
•RUQ U/S: mild hepatomegaly (17cm at right mid-clavicular line) with normal echogenicity, smooth contour; small sludge, CBD 0.3cm
Management?
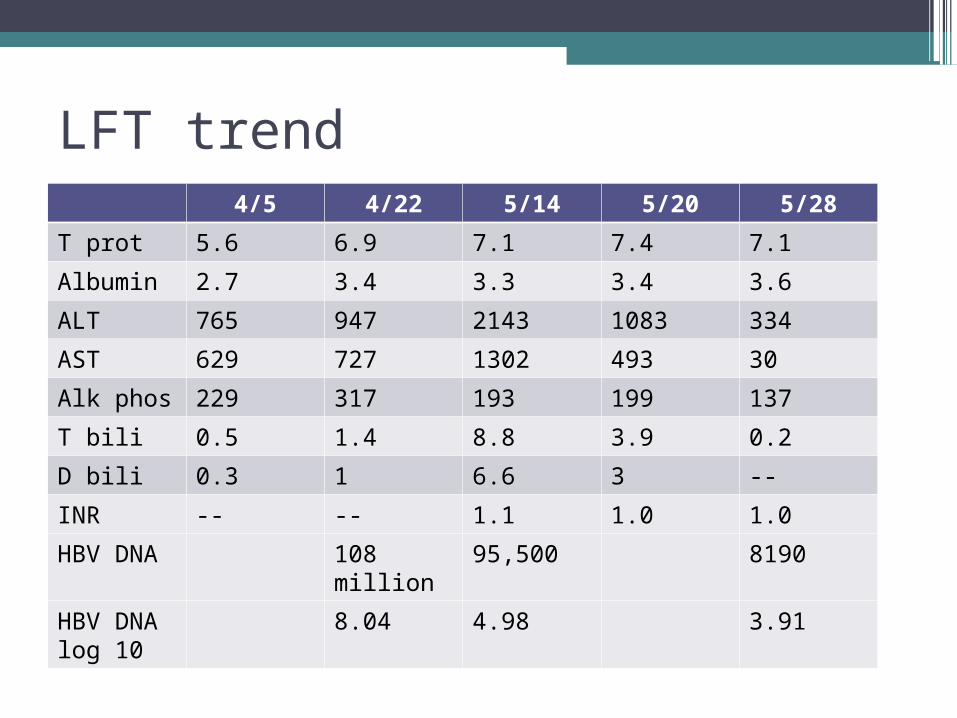
LFT trend4/5 4/22 5/14 5/20 5/28
T prot 5.6 6.9 7.1 7.4 7.1
Albumin 2.7 3.4 3.3 3.4 3.6
ALT 765 947 2143 1083 334
AST 629 727 1302 493 30
Alk phos 229 317 193 199 137
T bili 0.5 1.4 8.8 3.9 0.2
D bili 0.3 1 6.6 3 --
INR -- -- 1.1 1.0 1.0
HBV DNA
108 million
95,500 8190
HBV DNA log 10
8.04 4.98 3.91
Clinical questions
•Who is getting acute HBV in the U.S.?•What is severe acute HBV?•How and when should we treat severe
acute HBV?
Acute HBV demographics
•Acute HBV incidence has declined 82% since 1990
•8.5 cases per 100,000 in 1990•1.5 cases per 100,000 in 2007 (the lowest
rate ever recorded)•Declines in all age groups, but especially
in children <15 yrs, attributable to vaccination (national vaccination strategy implemented in 1991)
Daniels et al. MMWR Surveill Summ. 2009 May 22;58(3):1-27.
Acute HBV demographics
•In 2007, 4,519 acute symptomatic cases reported (43,000 additional new infections, asymptomatic)
•Risk factors for infection: 38% multiple sex partners, 11% MSM, 6% sexual contact with a person known to have hepatitis B. IVDU reported for 15% of persons.
•2007 reports: 76% had jaundice, 40% were hospitalized, and 2% died.Daniels et al. MMWR Surveill
Summ. 2009 May 22;58(3):1-27.
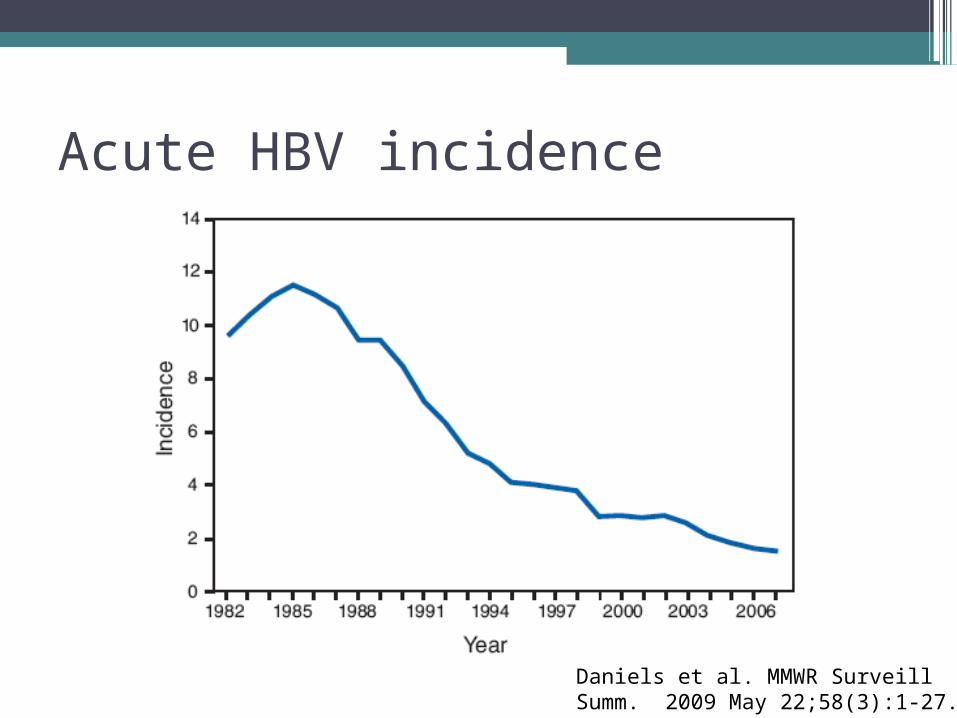
Acute HBV incidence
Daniels et al. MMWR Surveill Summ. 2009 May 22;58(3):1-27.
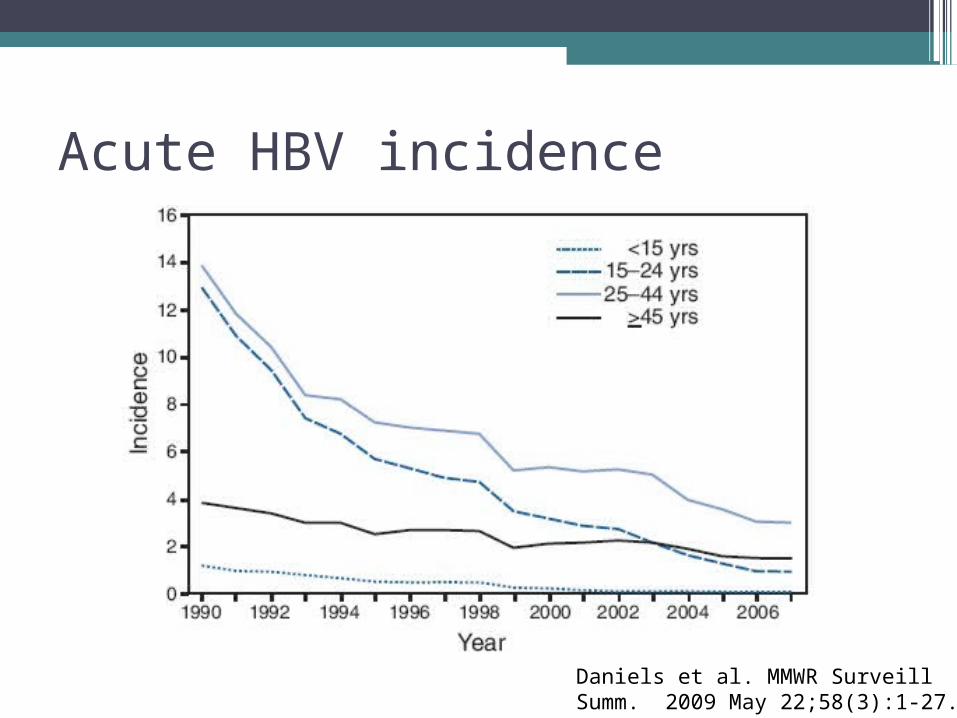
Acute HBV incidence
Daniels et al. MMWR Surveill Summ. 2009 May 22;58(3):1-27.

Acute HBV incidence
Daniels et al. MMWR Surveill Summ. 2009 May 22;58(3):1-27.

Management of severe acute HBV
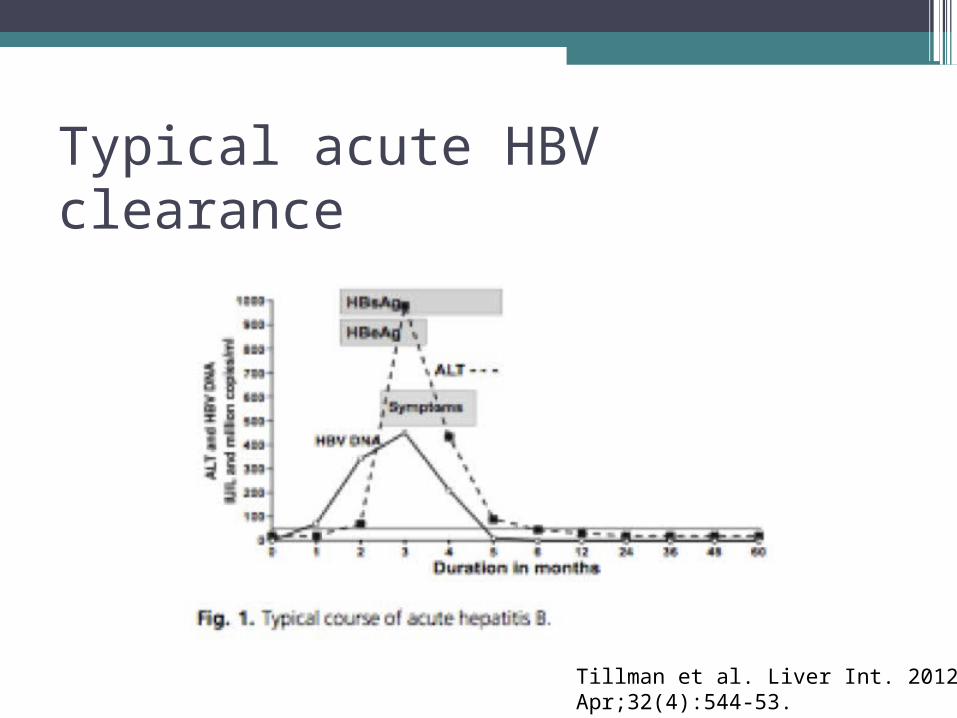
Typical acute HBV clearance
Tillman et al. Liver Int. 2012 Apr;32(4):544-53.

Acute hepatitis B
•In approximately 1% of cases, acute HBV progresses to liver failure with need for transplantation

Treatment with lamivudine for severe acute HBV•Large series of 37 patients (multicenter)•Definition of severe acute hepatitis:
▫Bilirubin >=10 mg/dl▫INR > 1.6▫Presence of hepatic encephalopathy
•Transplant-free survival with lamivudine for severe/acute to fulminant hepatitis B was 78.3% (29 of 37 patients) compared with 21.6% of historic controls (p < 0.001). Tillman HL et al. J Viral Hepat
2006; 13:256-63.
Treatment with newer antivirals for acute HBV•Prospective study, 6 patients in Germany
with HBV-related acute liver failure•Entecavir 1 mg/day within 1-18 days of
admission, continued for at least 3 months
•Normalization of INR, ALT, and bilirubin within 3 months
•1 patient went on to develop chronic hepatitis B
Jochum C et al. Digestion 2009; 80:235-40.

Risk of increasing chronicity with treating acute HBV•57 patients hospitalized with acute HBV
acquired in adulthood in Japan•7 of 57 patients developed persistence
(HBsAg positive 6 months after index hospitalization)
•6 of the 7 received prednisolone or glycyrrhizin during acute illness, 1 did not
•Infection persisted in 86% of patients who received treatment vs. 2% of patients who did not (p = 0.01) Kobayashi M et al. J Med Virol
2002; 68:522-8.

Take home points
•Fortunately, frequency of severe acute to fulminant liver failure in acute HBV is low
•For acute severe to fulminant HBV-related liver failure, lamivudine has shown benefits in transplant-free survival
•Small case series promising for entecavir in the setting of acute severe to fulminant HBV-related liver failure
References• Daniels D, Grtydal S, Wasley A; Centers for Disease Control and
Prevention. Surveillance for acute viral hepatitis – United States, 2007. MMWR Surveill Summ. 2009 May 22;58(3):1-27.
• De Socio GV et al. Severe acute hepatitis B treated with entecavir. Mediterr J hematol Infect Dis. 2011;3(1):32011010.
• Jochum C et al. Hepatitis B-associated acute liver failure: immediate treatment with entecavir inhibits hepatitis B virus replication and potentially its sequelae. Digestion 2009; 80:235-40.
• Kobayashi M et al. Viral genotypes and resonse to interferon in patients with acute prolonged hepatitis B virus infection of adulthood in Japan. J Med Virol 2002; 68:522-8.
• Kumar M et al. A randomized controlled trial of lamivudine to treat acute hepatitis B. Hepatology. 2007 Jan; 45(1):97-101.
References continued• Tillman HL, Zachou K, Dalekos GN. Management of severe acute
to fulminant hepatitis B: to treat or not to treat or when to treat? Liver Int. 2012 Apr;32(4):544-53.
• Tillman HL et al. Safety and efficacy of lamivudine in patients with severe acute or fulminant hepatitis B, a multicenter experience. J Viral Hepat 2006; 13:256-63.
• Yu JW et al. The study of efficacy of lamivudine in patients with severe acute hepatitis B. Dig Dis Sci. 2010 Mar; 55(3):775-83.
• Yu JW et al. Lamivudine treatment is associated with improved survival in fulminant hepatitis B. Liver Int 2011; 31:499-506.

Questions?