getting back to work: self-efficacy as a predictor of employment outcome
TRANSCRIPT

S P R I N G 9 9 — V O L U M E 2 2 N U M B E R 4
Getting Back to W ork:
Self-Efficacy as a
P redictor of Employment
Outcome
M ic h a e l R e g e n o l d ,
M a r t in F. Sh e r m a n &
M ic k e y F en z e l
MICHAEL REGENOLD, MA, IS A THERAPIST AT HEGIRA,
WESTLAND COUNSELING CENTER, WESTLAND, MICHIGAN.
MARTIN F. SHERMAN, PHD, IS A PROFESSOR OF PSYCHOLOGY, IN THE
DEPARTMENT OF PSYCHOLOGY, LOYOLA COLLEGE, BALTIMORE, MARYLAND.
MICKEY FENZEL, PHD, IS AN ASSOCIATE PROFESSOR OF PSYCHOLOGY,
DEPARTMENT OF PSYCHOLOGY, LOYOLA COLLEGE.
PORTIONS OF THIS RESEARCH WERE PRESENTED AT THE AMERICAN
PSYCHOLOGICAL SOCIETY CONVENTION, WASHINGTON, DC, MAY, 1998. THE AUTHORS WOULD LIKE TO THANK ELLEN FABIAN FOR GUIDANCE
OFFERED ON THIS ARTICLE’S THEORETICAL DEVELOPMENT AND
COMMENTS ON DRAFTS OF THIS ARTICLE.
FOR FURTHER INFORMATION CONTACT MARTIN F. SHERMAN, DEPARTMENT OF PSYCHOLOGY, LOYOLA COLLEGE, 4501 N. CHARLES ST., BALTIMORE, MARYLAND 21210-2699 . ELECTRONIC MAIL MAY BE
SENT TO [email protected].
The primary purpose of this exploratory research was to examine whether self-efficacy would be predictive of future vocational outcomes for participants in a supported employment program. Participants were 86 persons associated with a private, non-profit agency located in Baltimore, Maryland, which provides supported employment services for persons with psychiatric disabilities. Stepwise logistic regression analyses supported the hypothesized relation between self-efficacy and whether the employment goal was attained Hypothesized relations between symptomatology and prior employment history and the outcome variable were also supported. The importance of this research is that it lends support to self-ef- ficacy as a promising predictor of vocational rehabilitation outcomes.
Periodic reviews of vocational rehabilitation research have identified several demographic and clinical factors that have and have not correlated with future vocational skills. For instance, Anthony and Jansen (1984) reported that poor predictors of future vocational success include psychiatric symptomatology, type of diagnosis, intelligence, aptitude, and personality. They also reported that a person’s ability to succeed in a community setting is a poor predictor of success in a work setting and suggested that a better predictor of future vocational success is the
ARTICLES
rating of a person’s work adjustment skills made in a workshop setting or sheltered job site. According to Anthony and Jansen (1984), the best demographic predictor is a person’s prior employment history. Anthony, Cohen, and Farkas (1990) reviewed studies that investigated demographic predictors of future vocational success and found that employment history was the demographic variable most predictive of future vocational success, accounting for between 27% and 53% of the variance in employment.
361

P S Y C H I A T R I C R E H A B I L I T A T I O N J O U R N A L Getting Back to Work: Self-Efficacy as a Predictor of Employment Outcome
Anthony (1994) cautioned researchers to consider the specific sample when identifying the predictors of future vocational success. Using regression analysis, Anthony reported that only symptomatology, criminal justice involvement, and marital status were predictive of future vocational functioning. Married individuals with less severe psychiatric symptoms and no criminal justice involvement were more likely to be employed during the 1-year follow-up period. Although the findings of Anthony and Jansen (1984) and Anthony (1994) might appear inconsistent with respect to symptomatology, this inconsistency may be explainable when one considers the nature of the samples that the researchers used. Participants in many previous studies reviewed by Anthony and Jansen (1984) resided in hospital settings. Anthony (1994) utilized a participant sample that consisted of individuals who resided in the community and participated in a community-based vocational program. Anthony (personal communication, March 10,1998) claims that the significant relation between symptomatology and vocational success although weak is stronger for negative symptoms (e.g., poverty of speech) than for positive symptoms (e.g., increased speech). In addition, Anthony (personal communication, March 10,1998) claims that the availability of knowledge, skills, and support for the person who is symptomatic makes a significant positive difference in vocational success. Overall, Anthony (1994) suggested that variables that were found to be predictive of future vocational success in earlier studies may lose their predictiveness with participants who, unlike some of those in previous samples, are goal-oriented and participate in a documented vocational rehabilitation intervention.Furthermore, as a sample becomes more specific, new relations between predictor variables and vocational out
come may emerge—relations that should be investigated.
Self-efficacy among persons with psychiatric disabilities has been described as a promising predictor of vocational outcomes (Anthony, 1994; Arns & Linney,1993), yet has rarely been studied empirically. Bandura (1986) has defined self-efficacy as “people’s judgments of their capacities to organize and execute courses of action required to attain designated types of performances” (p.391). Further, Bandura (1977) postulated that individuals’ expectations of their self-efficacy determine whether they will initiate coping behavior, how much effort will be exerted, and how long coping behavior will be sustained despite obstacles and adverse experiences. According to Bandura (1977), efficacy expectations affect individuals’ choices of settings and behaviors. Individuals with low efficacy expectations are likely to avoid situations and environments that exceed their perceptions of their own coping skills. Additionally, efficacy expectations can affect the extent and persistence of effort in executing activities. Individuals with greater self-efficacy tend to persist longer in the face of obstacles and, by demonstrating mastery in a situation, their efficacy expectations tend to increase further.
People with lower self-efficacy expectations tend to be more likely to cease their efforts prematurely, thereby reinforcing their beliefs that they do not possess the skills needed to perform successfully in the given situation. It should be noted, however, that efficacy expectations alone do not produce the desired performance. There must also be adequate incentives for people to perform desired behaviors. Given adequate incentives, efficacy expectations are a major determinant of a person’s behavior, the extent of effort that will be put forth, and the extent to which ef
ARTICLES
fort will be sustained when difficulties arise (Bandura, 1977).
Among barriers facing persons with psychiatric disabilities seeking vocational rehabilitation, Rutman (1994) lists cognitive, perceptual, affective, and interpersonal deficits intrinsic to or resulting from the mental disability. Cole and McGeary (1991) suggest a number of deficits typically encountered in persons with severe and persistent psychiatric disabilities. Two of these deficits which are particularly problematic in forming “judgments” of capabilities regarding organizing and executing courses of action, are
a) foundation deficits, including anxiety; hopelessness; guilt; perceptual problems; and cognitive problems of attention, memory and insight; and
b) skills deficits, such as lack of impulse control, poor self-concept, distorted perception of reality, and poor problem solving strategies.
Hence, the usefulness of self-efficacy expectations among individuals with psychiatric disabilities may be questionable.
While much research in career development literature has supported the idea that self-efficacy is related to vocational outcome (e.g., Lent, Hackett, & Brown,1996), there is a paucity of research in the psychiatric rehabilitation literature that has investigated this relation. The purpose of this research, therefore, was to examine the personal factor of self-ef- ficacy as a predictor of future vocational outcome among persons with psychiatric disabilities who were participating in a supported employment program. The primary hypothesis tested was that there would be a relation between degree of self-efficacy and whether the employment goal was attained, such that participants with a greater degree of self-efficacy would be more likely to
362

S P R I N G 9 9 — V O L UM E 2 2 N U M B E R 4
attain their employment goals. In addition, it was hypothesized that prior employment history and psychiatric symptomatology would predict future vocational outcome, such that participants with a prior employment history and those with a lesser degree of psychopathology would be more likely to attain their employment goals.
M e t h o d
ParticipantsParticipants were involved with the Schapiro Training and Employment Program (STEP), a private, non-profit agency located in Baltimore, Maryland, which provides supported employment services for persons with psychiatric disabilities. Participants qualified for the study if they were unemployed at the time of referral to the supported employment program and sought a paid, part-time or full-time job, or if they were employed at the time of referral, but sought a different paid, part-time or full-time job. Of a total of 112 potential individuals whom we approached in the study, 86 participants who qualified and elected to participate in the study were included in the analysis. The gender of participants was fairly evenly split, between women (51%) and men (49%). African-Americans comprised 45% and 2% were comprised of other ethnicities, 51% of the participants were Euro-American. In reference to age,35% of the participants were 25 to 34 years old, 31.5% were 35 to 44 years old, 17.5% were 45 to 54 years old, and 15% were 18 to 24 years old. Of the participants, 9% received a college degree, 33% attended some college, 37% received a high school diploma or GED, and 12% attended some high school in = 10). With respect to psychiatric disability, 28% of the participants were diagnosed with schizophrenia, 19% were diagnosed with depression, 21% were
diagnosed with bipolar disorder, 15% were diagnosed with schizoaffective disorder, and 15% had other diagnoses.
In addition to jobs, job site training, ongoing monitoring, and follow-up, participants of STEP took part in a 5-day,2-hour intake group phase in order to prepare them for the initial phase of a job search. This group activity assisted the people in acquiring the necessary skills of communication and budgeting. It also helped reduce the fears associated with future employment, and assisted them in clarifying their vocational goals. Following this intake group phase and preceding the people’s job search, a second group training experience, the job club phase, was provided. The job club provided people with a supportive atmosphere in which basic job seeking skills (e.g., interviewing, constructing resumes, understanding hiring procedures) were taught. The job club met 5 days for 2 hours each day.
MaterialsDemographic information on each person was collected from STEP files. Additionally, the researcher provided permission forms, the Brief Symptom Inventory, and the Career Search Efficacy Scale, to the participants.
Demographic sheet. The demographic sheet included the person’s age at the time of referral, gender, ethnicity, level of educational attainment, number of life-time institutionalizations, date of last institutionalization, longest time continually employed, date last employed, source of current income, and primary psychiatric diagnosis (determined by psychiatrist or psychologist).
Brief Symptom Inventory. The Brief Symptom Inventory (Derogatis & Spencer, 1982) is a 53- item, self-report symptom scale that was designed to measure levels of psychopathology. The Brief Symptom Inventory (BSI) is an ab
breviated version of the revised Symptom Checklist-90 (SCL-90-R). The items are rated on a 5-point scale (0 to4), reflecting degrees of distress, ranging from not at all to extremely. The inventory can be used with individuals who have a minimum of a sixth-grade reading level and takes approximately 10 to 12 minutes to complete. The BSI includes 9 dimensions: Somatization, Obsessive-Compulsive, Interpersonal Sensitivity, Depression, Anxiety,Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism. In addition, a general indicator of psychopathology is provided by the General Severity Index (GSI). In this study, GSI scores standardized for male and female psychiatric outpatients were used. The GSI is a weighted frequency score based on the sum of the ratings the participant has assigned to each symptom. Higher GSI scores are indicative of greater psychopathology
Convergent validity of the BSI with the Minnesota Multiphasic Personality Inventory (MMPI) scales has been demonstrated by Boulet and Boss (1991) and by Derogatis and Melisaratos (1983) with various inpatient and outpatient samples. Similarly, Derogatis (1993) has established predictive validity of the BSI in a number of studies. The GSI of the BSI has been demonstrated over a 2-week interval to have acceptable temporal stability—.90 (Derogatis & Melisaratos, 1983). Cronbach’s coefficient for the current study was .96.
Career Search Efficacy Scale. The 35- item Career Search Efficacy Scale (Solberg, Good, Nord, et al., 1994) was designed to assess the degree of confidence a person has for performing various career search tasks. The Career Search Efficacy Scale (CSES) consists of four subscales: Job Search Efficacy, Interviewing Efficacy, Networking Efficacy, and Personal Exploration
ARTICLES
363

P S Y C H I A T R I C R E H A B I L I T A T I O N J O U R N A L Getting Back to Work: Self-Efficacy as a Predictor of Employment Outcome
Efficacy. Each item begins with the question stem, “How confident are you in your ability to:” and is rated on a10-point rating scale ranging from 0 (very little) to 9 (very much). Sample items include “Prepare for an interview,” “Develop an effective cover letter to be mailed to employers,” and “Identify an employer with job opportunities you want.” In this study, all items were summed and the mean value was used as an overall index of career search self-efficacy, which ranged from 0 to 9. High scores indicate a greater degree of confidence in performing career search tasks.
The CSES subscales and full scale have been demonstrated to have acceptable internal consistency—Cronbach’s alpha for subscales ranged from .87 to .95 and .97 for full scale (Solberg, Good, Nord, et al., 1994). For the current study, Cronbach’s coefficient was .98. Acceptable construct validity has been demonstrated based on a principal components analysis, which yielded four subscales of the CSES with scales from the Career Decision-Making Self- Efficacy Scale (Solberg, Good, Nord, et al., 1994).
ProcedureInformation for the demographic sheet was collected by the researcher from referral summaries, vocational evaluation summaries, psychiatric discharge summaries, people’s resumes, and job coaches’ records. Permission forms, the BSI, and CSES were given, respectively, by the researcher and completed by the participants in an isolated room at a time following the information session and before the intake group phase. The information session is the initial meeting during which prospective persons are informed about supported employment services. The BSI and CSES were also administered after people completed the job club phase. People were asked to complete permission forms in
order to participate in this study. Directions were read and participants had an opportunity to ask questions regarding completing the scales.
The evaluation period lasted 13 months from March, 1996, through March,1997. The mean time from entry into the study until the end of the evaluation period was 7 months. Participants were determined to have attained their employment goal if they either (a) were unemployed at the time of referral to the supported employment program and did secure paid part-time or fulltime employment by the end of the evaluation period; or (b) were employed at the time of referral to the supported employment program and had the goal to attain a different paid part- time or full-time employment and did by the end of the evaluation period.
Variables and AnalysesThe predictor variables were symptomatology, prior employment history, and degree of career search self-efficacy The criterion or outcome variable was whether or not participants attained their employment goals of paid, part- time, or full-time employment by the end of the 13-month evaluation period. For analysis purposes, attainment of employment goal was coded as 1 and lack of attainment of employment goal was coded as a 2.
The standardized GSI scores used to measure symptomatology originated from the administration of the BSI following the information session and before the intake group phase. Prior employment history was assessed using measures of the number of years that an individual was continuously employed and the number of years since the individual was last employed. Continuous employment was defined as the greatest number of years that an individual was employed in one or more jobs, provided that the interim period of unemployment between jobs
was not equal to or greater than 6 months. Self-efficacy was measured using the mean score of all items on the CSES. Where missing BSI or CSES test item values were found for an individual, the individual’s mean value for all completed corresponding BSI or CSES test items was substituted.
Stepwise logistic regression analysis was used to examine whether the predictor variables of symptomatology, prior employment history, and degree of career search self-efficacy had a significant relation with employment attainment. Only 74 participants had information concerning continuous employment, and 73 participants had information regarding years since last employed. The cases for which this information was missing were not entered into the logistic regression equation.
R e su l t s
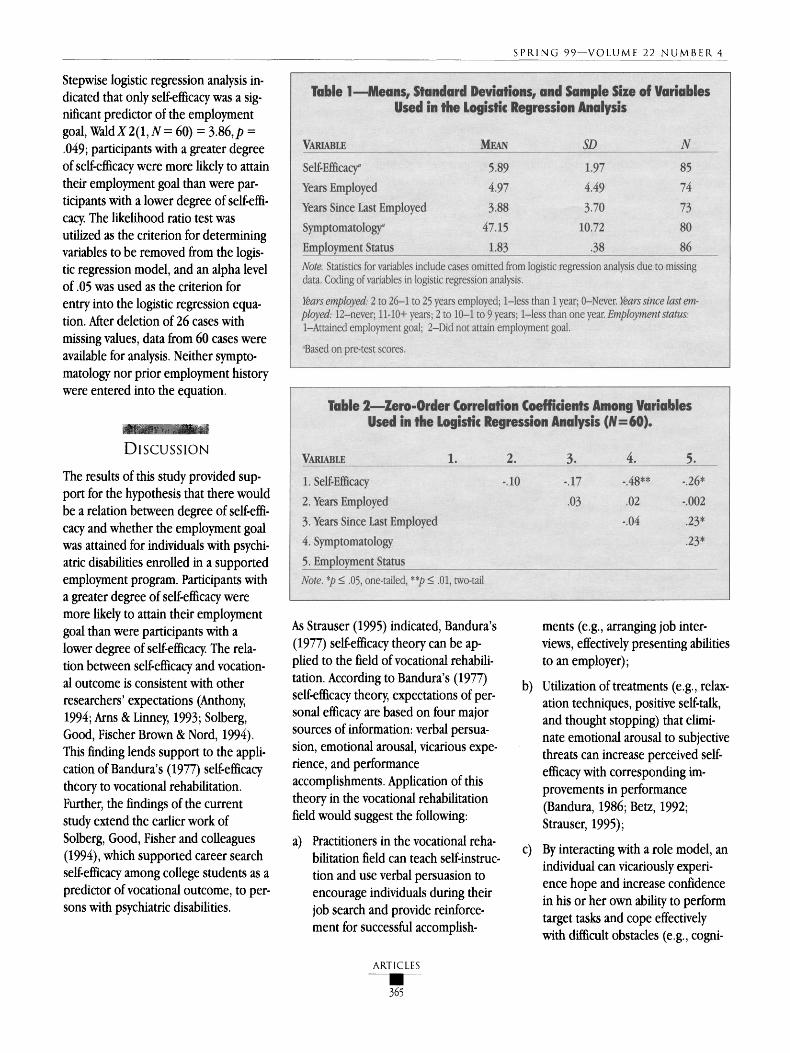
Table 1 shows the descriptive statistics for the variables used in the present study, and Table 2 presents the zero- order correlations between these variables. Results showed a significant negative correlation between self-efficacy and attainment of the employment goal, r (60) = - .26, p =.04; participants with higher self-efficacy scores were more likely to attain their employment goals than those with lower self-efficacy scores. Results also showed a positive correlation between years since last employed and whether or not the employment goal was attained, r (60) = .23, p =.04; participants with a longer length of time since last employed were less likely to attain their employment goal. In addition, there was a positive zero- order correlation between symptomatology and whether or not the employment goal was attained, r (60) = .23,p = .04, participants with a higher level of psychopathology were less likely to attain their employment goal.
ARTICLES
364
S P R I N G 9 9 — V O L UM E 2 2 N U M B E R 4
Stepwise logistic regression analysis indicated that only self-efficacy was a significant predictor of the employment goal, Wald X 2(1, N = 60) = 3-86,p = .049; participants with a greater degree of self-efficacy were more likely to attain their employment goal than were participants with a lower degree of self-effi- cacy. The likelihood ratio test was utilized as the criterion for determining variables to be removed from the logistic regression model, and an alpha level of .05 was used as the criterion for entry into the logistic regression equation. After deletion of 26 cases with missing values, data from 60 cases were available for analysis. Neither symptomatology nor prior employment history were entered into the equation.
D i s c u s s io n
The results of this study provided support for the hypothesis that there would be a relation between degree of self-efficacy and whether the employment goal was attained for individuals with psychiatric disabilities enrolled in a supported employment program. Participants with a greater degree of self-efficacy were more likely to attain their employment goal than were participants with a lower degree of self-efficacy. The relation between self-efficacy and vocational outcome is consistent with other researchers’ expectations (Anthony, 1994; Arns & Linney, 1993; Solberg, Good, Fischer Brown & Nord, 1994). This finding lends support to the application of Bandura’s (1977) self-efficacy theory to vocational rehabilitation. Further, the findings of the current study extend the earlier work of Solberg, Good, Fisher and colleagues(1994), which supported career search self-efficacy among college students as a predictor of vocational outcome, to persons with psychiatric disabilities.
As Strauser (1995) indicated, Bandura’s (1977) self-efficacy theory can be applied to the field of vocational rehabilitation. According to Bandura’s (1977) self-efficacy theory, expectations of personal efficacy are based on four major sources of information: verbal persuasion, emotional arousal, vicarious experience, and performance accomplishments. Application of this theory in the vocational rehabilitation field would suggest the following:
a) Practitioners in the vocational rehabilitation field can teach self-instruc- tion and use verbal persuasion to encourage individuals during their job search and provide reinforcement for successful accomplish
ARTICLES
ments (e.g., arranging job interviews, effectively presenting abilities to an employer);
b) Utilization of treatments (e.g., relaxation techniques, positive self-talk, and thought stopping) that eliminate emotional arousal to subjective threats can increase perceived self- efficacy with corresponding improvements in performance (Bandura, 1986; Betz, 1992; Strauser, 1995);
c) By interacting with a role model, an individual can vicariously experience hope and increase confidence in his or her own ability to perform target tasks and cope effectively with difficult obstacles (e.g., cogni
365

P S Y C H I A T R I C R E H A B I L I T A T I O N J O U R N A L Getting Back to Work: Self-Efficacy as a Predictor of Employment Outcome
tive, perceptual, and interpersonal deficits; stigma) to initiate and sustain actions in order to attain employment (Bandura, 1986; Rutman,1994). Through services that assist people with learning a set of skills (e.g., basic job seeking skills, reducing fears associated with future employment, clarifying vocational goals), individuals have the opportunity to interact with other people and to vicariously experience successful accomplishment of vocational tasks.
d) Finally, performance accomplishments can be used to increase efficacy by developing mastery of work and job seeking skills (e.g., interviewing, constructing resumes, understanding hiring practices; Strauser, 1995). As Hackett and Betz(1981) noted, successful performance of a task is the paramount source of strong career self-efficacy.
Zero-order correlation analysis supported the hypotheses that there would be a relation between the predictors of symptomatology and prior employment history (defined as years since last employed) and employment goal. The finding that prior employment history was related significantly to whether or not the employment goal was attained is consistent with the findings of Anthony, Cohen, and Farkas (1990). Additionally, the finding that symptomatology was significantly related to whether or not the employment goal was attained is consistent with the findings of Anthony (1994). The strong negative correlation between self-efficacy and symptomatology may be due to a direct or indirect causal connection between symptomatology and self-efficacy. Strauser (1995) specifies how self-efficacy can be increased or decreased as a function of four major sources of information. For instance, self-efficacy can be negatively affected by symptomatology
when a person engages in negative selftalk (verbal persuasion). Experiencing anxiety while performing a task may be interpreted as ineffective coping (emotional arousal). Also symptomatology may impair an individual’s performance (performance accomplishments), and may result in decreasing self-efficacy. However, the correlational nature of this relationship prevents us from making any strong causal statements. Interestingly, the relations between symptomatology and prior employment history and the outcome variable disappear when one accounts for the variation explained by self-efficacy. This suggests the possibility that self-efficacy may be mediating the relation between symptomatology and prior employment history and the outcome variable.Future research may be able to ascertain the likelihood of this.
The two primary limitations of the current exploratory study are a small sample and a one-dimensional measure of vocational outcome. The small sample size may account for the lack of significant relations between some of the predictor variables and the criterion variable in the regression equation. Second, the current study investigated the relations between the predictor variables and only one outcome variable, whether or not the employment goal was attained. Research that uses a unidimensional outcome measure may be too narrow in scope, and should also include outcome variables with respect to the individual’s satisfaction, employer satisfaction, and benefits to the community (DeStefano, 1990; Fabian, 1991). Because only one outcome variable was used, inter-study comparisons are limited.
Based on the findings of the current study, self-efficacy as a predictor of vocational outcome for persons with psychiatric disabilities merits further investigation. Further, because of the in
consistent results of studies of the factors that predict vocational outcomes, future researchers are encouraged to investigate variables used in earlier studies that predicted vocational successes to determine if these variables maintain their predictive utility. As Anthony(1994) suggested, different samples in vocational studies may account for inconsistent results. Mowbray, Bybee, Harris, and McCrohan (1995) offer another explanation for the inconsistency among studies’ results— differing definitions of variables studied in vocational rehabilitation research— and, therefore, recommend accurate specification of variables measured.
Additional recommendations for future studies include the use of multivariate analyses to understand better the complex relations among predictor variables and the unique variance accounted for in the vocational outcome by each predictor variable; an increase in the sample size; the use of a multidimensional vocational outcome measure; and the investigation of self- efficacy as a potential mediator variable.
The importance of this research is that it supported the hypothesis that degree of self-efficacy would be significantly related to whether or not an employment goal was attained. This research provided support for supported employment services, which are designed to increase career search self-efficacy and therefore are integral in assisting persons with psychiatric disabilities who may from the outset of the job search be facing difficult obstacles (e.g., cognitive, perceptual, and interpersonal deficits; discrimination) in initiating and sustaining actions to successfully attain employment (Bandura, 1977; Rutman, 1994).
ARTICLES
366

S P R I N G 9 9 — V O L UM E 2 2 N U M B E R 4
R e f e r e n c e s
Anthony, W A. (1994). Characteristics of people with psychiatric disabilities that are predictive of entry into the rehabilitation process and successful employment. Psychosocial Rehabilitation Journal, 17, 3-13.
Anthony, W A., Cohen, M. R., & Farkas, M.D. (Eds.) (1990). Psychiatric rehabilitation. Boston: Boston University, Center for Psychiatric Rehabilitation.
Anthony, W A., & Jansen, M. A. (1984). Predicting the vocational capacity of the chronically mentally ill: Research and policy implications. American Psychologist, 39, 537-544.
Ams, P G., & Linney, J. A. (1993). Work, self, and life satisfaction for persons with severe and persistent mental disorders. Psychosocial Rehabilitation Journal,17, 63-79.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavior change. Psychosocial Review, 84,191-215.
Bandura, A. (Ed.) (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall.
Betz, N. (1992). Counseling uses of career self-efficacy. The Career Development Quarterly, 41, 20-26.
Boulet, J., & Boss, M. W (1991). Reliability and validity of the Brief Symptom Inventory. Psychosocial Assessment, 3, 435-437.
Cole, C., & McGeary, S. (1991). Evaluating psychological and cognitive factors in the psychiatrically challenged worker. Work, 1(3), 19-31.
Derogatis, L. R. (1993). Brief Symptom Inventory: Administration, scoring, and procedures manual-II.Minneapolis, MN: National Computer Systems.
Derogatis, L. R., & Melisaratos, N. (1983). The Brief Symptom Inventory: An introductory report. Psychological Medicine, 13, 596-605.
Derogatis, L. R., & Spencer, M. S. (1982).The Brief Symptom Inventory (BSI): Administration, scoring, and procedures manual-I. Baltimore: Johns Hopkins University School of Medicine, Clinical Psychometrics Research Unit.
DeStefano, L. (1990). Designing and implementing program evaluation. In F. R. Rusch (Ed.), Supported employment: Models, methods, and issues (pp.229-246). Sycamore, NY: Sycamore Publishing Company.
Fabian, E. (1991). Using quality-of-life indicators in rehabilitation program evaluation. Rehabilitation Counseling Bulletin, 34, 344-356.
Hackett, G., & Betz, N. (1981). A self-efficacy approach to the career development of women. Journal of Vocational Behavior, 18, 326-339.
Lent, R. W, Hackett, G., & Brown, S. D.(1996). A social cognitive framework for studying career choice and transition to work .Journal of Vocational Education Research, 21(4), 3-31.
Mowbray, C. T., Bybee, D., Harris, S. N., & McCrohan, N. (1995). Predictors of work status and future work orientation in people with a psychiatric disability. Psychiatric Rehabilitation Journal, 19(2), 17-28.
Rutman, I. D. (1994). How psychiatric disability expresses itself as a barrier to employment. Psychosocial Rehabilitation Journal, 17(5), 15-35.
Solberg, S. V, Good, G. E., Fischer, A. R., Brown, S., & Nord, D. (1994). Career decision-making and career search activities: Relative effects of career search self-efficacy and human agency. Unpublished manuscript, Loyola University, Chicago.
Solberg, S. V, Good, G., Nord, D., Holm, C., Hohner, R., Zima, N., Heffeman, M., & Malen, A. (1994). Assessing career search expectations: Development and validation of the career search efficacy seale . Journal of Career Assessment, 2(2), 111-123.
Strauser, D. R. (1995). Applications of self- efficacy theory in rehabilitation counseling. Journal of Rehabilitation, 61,7-11.
ARTICLES
367