german hospitals in the post g-drg introduction era filedisturbing a ”corporatist market” german...
TRANSCRIPT

Disturbing a ”corporatist market”
German hospitals in the post
G-DRG introduction eraG-DRG introduction era
Dipl.-Ing. Alexander Geissler
Research Fellow
Department of Health Care Management
Berlin University of Technology
WHO Collaborating Centre for Health Systems,Research and Management
European Observatory on Health Systems and Policies
28 September 2010 1Aalto University Executive Education | Helsinki, Finland

Agenda
1) German healthcare (hospital) system overview
2) Ten years of DRGs in Germany
3) Strategic behaviour of hospitals in times of DRGs
4) Future trends and challenges
28 September 2010 Aalto University Executive Education | Helsinki, Finland 2

German healthcare system overview
Key characteristics:
a) Sharing of decision-making powers between the sixteen Länder
(states), the federal government and statutory civil society
organizations
i.e. important competencies are legally delegated to membership-based,
self-regulated organisations of payers and providers self-regulated organisations of payers and providers
b) Statutory health insurance (SHI)
SHI Cornerstone of health service provision is the Fifth book of the German
Social Law (SGB V)
i.e. it organizes and defines the self-regulated corporate structures and give
them the duty and power to develop benefits, prices and standards
28 September 2010 Aalto University Executive Education | Helsinki, Finland 3

German healthcare system overview
Key characteristics:
c) Sectoral boarders
SGB V separates the provision of outpatient and inpatient services.
Planning, resource allocation and financing are undertaken completely
separately in each sector.separately in each sector.
�Complicates the provision of health care delivery (e.g. communication)
�Increases the amount of specialists
�Increases the health care expenditure
28 September 2010 Aalto University Executive Education | Helsinki, Finland 4

German healthcare system overview
Financial flow of the SHI
- German GDP for health care in 2007: 10.4 % (~ € 253 bn)
- Main blocks: 57.5 % SHI, 9.3 % private insurance, 13.5 % out of pocket
Contribution rates (wage-related) Taxes
28 September 2010 Aalto University Executive Education | Helsinki, Finland 5
Health Fund (Pooling)
Morbi-RSA (Risk adjustment)
Health care provider
Third-party payer
(Sickness Funds)
Additional contributions
or
Bonuses

German healthcare system overview
Hospital facts for 2007
Hospitals
overallBeds
Beds per 100
000
inhabitants
Occupancy Cases
Cases per 100
000
inhabitants
ALOS*
Number
(Share in %)
Number
(Share in %)Number in % Number Number Days
2 087 506 954 616 77.2 17 178 573 20 883 8.3
(100) (100)
< 49 407 7 572 9 64.9 210 028 255 8.5
50 - 99 264 19 354 24 73.3 529 579 644 9.8
100 - 149 302 36 995 45 74.2 1 108 285 1 347 9.0
Size and type of
ownership
Hopital size in beds
28 September 2010 Aalto University Executive Education | Helsinki, Finland 6
150 - 199 208 35 903 44 74.8 1 179 137 1 433 8.3
200 - 299 326 79 578 97 76.1 2 612 288 3 176 8.5
300 - 399 203 69 613 85 77.4 2 361 352 2 871 8.3
400 - 499 131 58 258 71 77.6 1 953 598 2 375 8.4
500 - 599 96 52 545 64 77.1 1 870 325 2 274 7.9
600 - 799 64 43 654 53 78.8 1 564 800 1 902 8.0
> 800 86 103 482 126 80.7 3 789 184 4 606 8.0
677 250 345 304 78.9 8 697 755 10 573 8.3
(32.4) (49.4)
under private law 380 133 957 163 77.5 4 804 914 5 841 7.9
under publ i c law 297 116 388 141 80.5 3 892 841 4 732 8.8
- lega l ly dependent 161 54 319 66 79.5 1 755 576 2 134 9.0
- lega l ly independent 136 62 069 75 81.4 2 137 266 2 598 8.6
790 177 632 216 75.3 5 970 324 7 258 8.2
(37.9) (35.0)
620 78 977 96 76.2 2 510 494 3 052 8.7
(29.7) (15.6)
Public hospitals
Non-profit hospitals
Private hospitals

German healthcare system overview
Range of activities and services in hospital sector
Pre-hospital care
(GPs, Specialists)
Hospital Treatment Post-hospital care
(GPs, Specialists,
Rehabilitation)
28 September 2010 Aalto University Executive Education | Helsinki, Finland 7
Rehabilitation)
Referral by GP
or specialist
Inpatient care
Day-surgery
Highly specialized care on in-and outpatient basis (e.g. Cystic fibrosis)
Discharge to GP,
specialist or
rehabilitation

German healthcare system overview
Hospital capacity planning and financing
- Capacities are planned by the state governments on the basis of so-called
“hospital requirement plans”
- Financing follows the principle of duality since Hospital Financing Act
(KHG) in 1972
Taxes Infrastructure investments
28 September 2010 Aalto University Executive Education | Helsinki, Finland 8
Patients
States
Tax payers
Sickness funds
Hospitals
Taxes Infrastructure investments
Contributions Operating costs
Hospital services

German healthcare system overview
Operating costs
- Sickness funds negotiating activity based DRG budgets every year with every
“planned” Hospital
Casemix
X
Base rate
Supplementary
feesHospital budget+ =Surcharges+
- Budget over-run adjustment (hospital pays back):
65 % (standard DRGs), 25 % (drugs, medical, polytrauma and burns DRGs),
Negotiation for hardly predictable DRGs
- Budget under-run adjustment (hospital receives compensation) :
20% (standard DRGs)
28 September 2010 Aalto University Executive Education | Helsinki, Finland 9
Base ratefees + =+

German healthcare system overview
Infrastructure investments
- Long-term infrastructural assets require a case-by case grant application by
each individual hospital
- Flat-rate grants for short-term assets (3–15 years economic life) can be
granted
- In practice, infrastructural hospital investments are mainly determined by
the budgetary situation of the states and by political considerations
28 September 2010 Aalto University Executive Education | Helsinki, Finland 10

Agenda
1) German healthcare (hospital) system overview
2) Ten years of DRGs in Germany
3) Strategic behaviour of hospitals in times of DRGs
4) Future trends and challenges
28 September 2010 Aalto University Executive Education | Helsinki, Finland 11

Ten years of DRGs in Germany
Aims of DRG introduction
- Achieving a more appropriate and fair allocation of resources by utilising
DRGs instead of per diem charges
- Facilitating a precise and transparent measurement of the case mix and the
level of services delivered by hospitalslevel of services delivered by hospitals
- Increasing efficiency and quality of service delivery due to the improved
documentation of internal processes and increased managerial capacity
- Cost containment based on LOS and bed capacity reduction
28 September 2010 Aalto University Executive Education | Helsinki, Finland 12

Ten years of DRGs in Germany
1)
Ph
ase
of
pre
pa
rati
on Historical Budget
(2003)
2) Budget-neutral
phase
3) Phase of convergence
to state-wide base rates
Nationwide base rate
Fixed or maximum prices
Selective or uniform negotiations
4) Discussion on Policy
15 %20%
20%
20%
25%
2000-2002 2003 - 2004 2005 - 2009 2010 - 2014
Hospital specific base rate
1)
Ph
ase
of
pre
pa
rati
on
Transformation
DRG-Budget
(2004)
Quality Assurance (adjustments)
Budgeting (amount of services)
Dual Financing or Monistic
15 %
20%
20%
20%
25%
25%
Statewide
base rate
Hospital specific base rate
28 September 2010 Aalto University Executive Education | Helsinki, Finland 13

Ten years of DRGs in Germany
1) Phase of preparation
Health Ministry
(federal, state)
Self-Administration (DKG, GKV, PKV)
AdministrationHealth Policy
Goals
and
monitoring
Forming
a legal
frameworkOther Institutions (HTA, quality)
28 September 2010 Aalto University Executive Education | Helsinki, Finland 14
Consultation Development
DIMDI (German Institute of Medical
Information and Documentation)
InEK (German DRG Institute)
Technical
managementContribution
of expertise
Other Institutions (HTA, quality)
Variety of Institutions(Professional medical associations,
industry groups)
G-DRG
System

Ten years of DRGs in Germany
1) Phase of preparation: Options for system modelling
Patient
classification
system
Data collection
Price setting
Reimbursement
rate
• Diagnoses • Clinical data • Average prices • Outliers
28 September 2010 Aalto University Executive Education | Helsinki, Finland 15
• Diagnoses
• Procedures
• Severity
• Clinical data
• Cost data
• Sample size
• Average prices
• Cost weights
• Outliers
• High cost cases

Ten years of DRGs in Germany
1) Phase of preparation: Patient classification system
Case data
(demographic and clinical characteristics )
Implausibility of major diagnosis,
medical procedures, demographic
characteristics etc.
Transplantation,
ventilation etc.
Error DRGPre-MDC
Pre-MDC process
MDC assign-ment based on
major diagnosis
Basis DRGs(G-DRG Version 2010 : n=594, including 6 Error DRGs)
… … … MDC 23MDC 3MDC 2MDC 1
+ at least one surgical procedure
+ no (essential) procedure for the respective MDC
Medical
Partition
Major diagnosis
Co-morbidity, medical procedures, age, clinical severity, complication,
cause of hospital discharge
split
DRGs (n= 906)
unsplit
DRGs (n=294)
Surgical
Partition
Other
Partition
Significant differences in resource comsumption
+ no surgical procedure, but one other procedure being essential for the respective MDC
n=300n=294
28 September 2010 Aalto University Executive Education | Helsinki, Finland 16

Ten years of DRGs in Germany
1) Phase of preparation: Data collection
Checked and
anonymised data
InEKDevelopment of case fee
catalogue annually
checking data content
Data CentreCollecting datasets
DIMDIDevelopment and update
of classification base (ICD -
10 GM and OPS codes)
28 September 2010 Aalto University Executive Education | Helsinki, Finland 17
Case data for
reimbursement
(§ 301 SGB V) Until July 1
Case-related performance and
hospital-specific structural data
from every hospital (§21 KHEntgG)
until March 31
Additionally case-related
cost data from a sample of
hospitals until March 31
Hospitals
Sickness
fundsChecking data
via their medical
review board
Paying hospital
Collecting datasets
Checking case and
cost data technically
Anonymising data
Federal
Statistical
OfficePublication of data

Ten years of DRGs in Germany
1) Phase of preparation: Price setting mechanism
- Calculation of cost weights: Based on average costs of cases data sample:
Year 2003 2005 2007 2009 2010
Hospitals participating in cost
data collection125 148 263 251 253
- excluded for data quality 9 0 38 33 28
- actual 116 148 225 218 225
- Cost weight of each DRG = Average costs of DRG inliers/Reference value
- Cost weight = 1 = average costs of all patients in Germany
- actual 116 148 225 218 225
- included university hospitals 0 10 10 10 10
- number of cases available for
calculation633,577 2,909,784 4,239,365 4,377,021 4,539,763
- number of cases used for
calculation after data checks494,325 2,283,874 2,863,115 3,075,378 3,257,497
28 September 2010 Aalto University Executive Education | Helsinki, Finland 18

Ten years of DRGs in Germany
1) Phase of preparation: Reimbursement rate and outliers
Revenues
Short-stay
outliers
Long-stay
outliers
Inliers
28 September 2010 Aalto University Executive Education | Helsinki, Finland 19
LOSDeductions
(per day)
Surcharges
(per day)
Lower LOS
threshold
Upper LOS
threshold

Ten years of DRGs in Germany
1)
Ph
ase
of
pre
pa
rati
on Historical Budget
(2003)
2) Budget-neutral
phase
3) Phase of convergence
to state-wide base rates
Nationwide base rate
Fixed or maximum prices
Selective or uniform negotiations
4) Discussion on Policy
15 %20%
20%
20%
25%
2000-2002 2003 - 2004 2005 - 2009 2010 - 2014
Hospital specific base rate
1)
Ph
ase
of
pre
pa
rati
on
Transformation
DRG-Budget
(2004)
Quality Assurance (adjustments)
Budgeting (amount of services)
Dual Financing or Monistic
15 %
20%
20%
20%
25%
25%
Statewide
base rate
Hospital specific base rate
28 September 2010 Aalto University Executive Education | Helsinki, Finland 20

Ten years of DRGs in Germany
2) Budget-neutral phase
Unit of reimbursement changed:
From:2002 � Reimbursement unit = per diem2002 � Reimbursement unit = per diem
To:2004 � Reimbursement unit = case (DRG)
28 September 2010 Aalto University Executive Education | Helsinki, Finland 21

Ten years of DRGs in Germany
Budget-neutral phase
Lead to a hospital specific base rate (historical Budget /Casemix)
Example: € 100 Mil. Budget / 33 000 CM = € 3030 Hospital specific base rate
28 September 2010 Aalto University Executive Education | Helsinki, Finland 22
Base rate
Relative cost weight
Patient characteristics
Gender, Age,
Diagnoses, Severity
Treatment options
Procedures,Technologies,
Intensity
Hospital-specificX =
G-DRG
reimbursement

Ten years of DRGs in Germany
1)
Ph
ase
of
pre
pa
rati
on Historical Budget
(2003)
2) Budget-neutral
phase
3) Phase of convergence
to state-wide base rates
Nationwide base rate
Fixed or maximum prices
Selective or uniform negotiations
4) Discussion on Policy
15 %20%
20%
20%
25%
2000-2002 2003 - 2004 2005 - 2009 2010 - 2014
Hospital specific base rate
1)
Ph
ase
of
pre
pa
rati
on
Transformation
DRG-Budget
(2004)
Quality Assurance (adjustments)
Budgeting (amount of services)
Dual Financing or Monistic
15 %
20%
20%
20%
25%
25%
Statewide
base rate
Hospital specific base rate
28 September 2010 Aalto University Executive Education | Helsinki, Finland 23
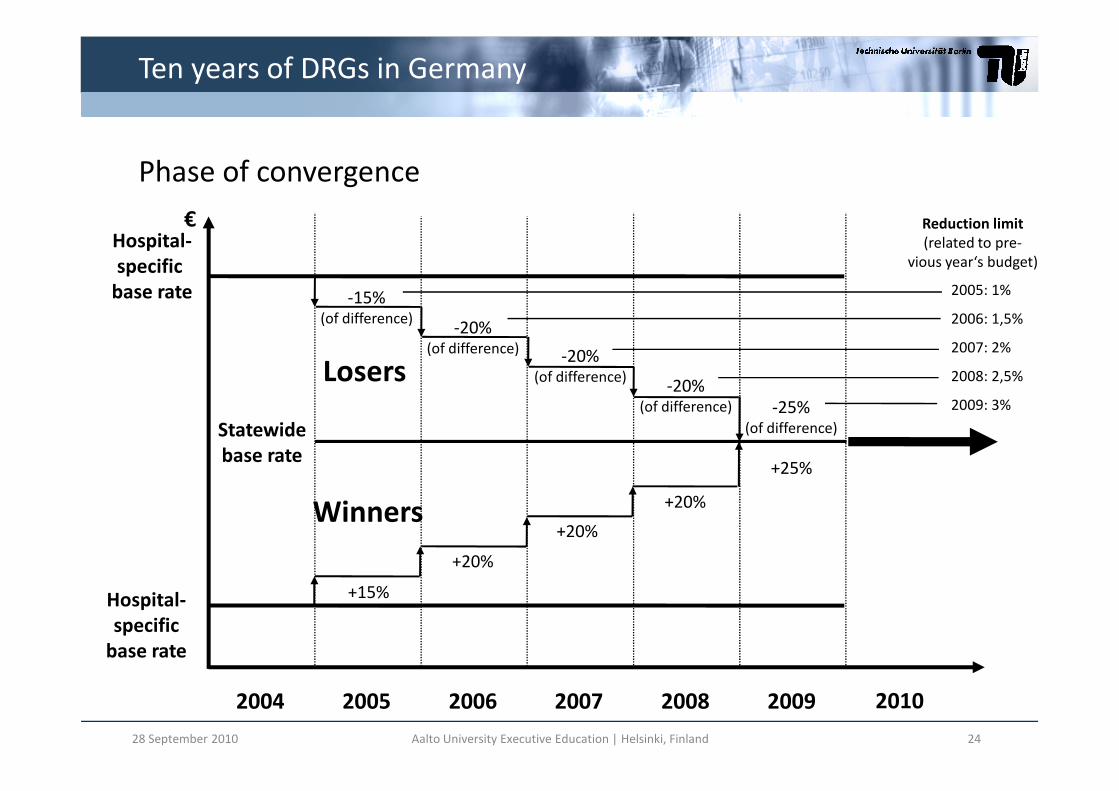
Ten years of DRGs in Germany
Phase of convergence
2005: 1%
2006: 1,5%
2007: 2%
2008: 2,5%
2009: 3%
€
Losers
-15%(of difference)
Hospital-
specific
base rate
-20%(of difference)
-20%(of difference)
-20%
-25%
Reduction limit
(related to pre-
vious year‘s budget)
28 September 2010 Aalto University Executive Education | Helsinki, Finland 24
2009: 3%
+15%
+20%
+20%
+20%
+25%
Statewide
base rate
Hospital-
specific
base rate
Winners
2004 2005 2006 2007 2008 2009 2010
(of difference) -25%(of difference)

Ten years of DRGs in Germany
Phase of convergence: Changing cost weights
- Increased precision due to more cost weights
- Treatment costs were better reflected over time
Year 2003 2005 2007 2009 2010
DRGs total 664 878 1082 1192 1200
25 May 2010 Hospital Financing in Germany: The G-DRG System 25
DRGs total 664 878 1082 1192 1200
Inpatient DRGs total 664 878 1077 1187 1195
Range of cost weights: min.-
max.(rounded)0.12 - 29.71 0.12 - 57.63 0.11 - 64.90 0.12 - 78.47 0.13 - 73.76
Day care DRGs total 0 0 5 5 5
Supplementary fees 0 71 105 127 143

Ten years of DRGs in Germany
1)
Ph
ase
of
pre
pa
rati
on Historical Budget
(2003)
2) Budget-neutral
phase
3) Phase of convergence
to state-wide base rates
Nationwide base rate
Fixed or maximum prices
Selective or uniform negotiations
4) Discussion on Policy
15 %20%
20%
20%
25%
2000-2002 2003 - 2004 2005 - 2009 2010 - 2014
Hospital specific base rate
1)
Ph
ase
of
pre
pa
rati
on
Transformation
DRG-Budget
(2004)
Quality Assurance (adjustments)
Budgeting (amount of services)
Dual Financing or Monistic
15 %
20%
20%
20%
25%
25%
Statewide
base rate
Hospital specific base rate
28 September 2010 Aalto University Executive Education | Helsinki, Finland 26

Ten years of DRGs in Germany
Main facts
- Central role of self-governing bodies
- Data driven system with annual updates
- Detailed analysis of hospital costs- Detailed analysis of hospital costs
- Ten-year process of introduction
28 September 2010 Aalto University Executive Education | Helsinki, Finland 27

Ten years of DRGs in Germany
Strengths and weaknesses of the G-DRG system
Strengths Weaknesses
Transparency and documentationNo quality adjustments for
reimbursement
Compliance of hospitals No reflection of different input prices
28 September 2010 Aalto University Executive Education | Helsinki, Finland 28
Compliance of hospitals No reflection of different input prices
Reimbursement toolUniform accounting system but no full
sample of hospitals
PrecisionIncreasing complexity with number of
DRGs

Agenda
1) German healthcare (hospital) system overview
2) Ten years of DRGs in Germany
3) Strategic behaviour of Hospitals in times of DRGs
4) Future trends and challenges
28 September 2010 Aalto University Executive Education | Helsinki, Finland 29

Strategic behaviour of hospitals in times of DRGs
Case payment vs. per diem charge: Changes of incentives
- Patients are no longer “revenue” but “cost” centers
- Every case has a contribution margin
Revenues/
Costs Long-stay
outliers
per diem
charge
28 September 2010 Aalto University Executive Education | Helsinki, Finland 30
LOSDeductions
(per day)
Surcharges
(per day)
Short-stay
outliers
outliers
Inliers
Lower LOS
threshold
Upper LOS
threshold

Strategic behaviour of hospitals in times of DRGs
Options to avoid deficits under activity based payments
Revenues
Costs/
Total costs
increase revenues
28 September 2010 Aalto University Executive Education | Helsinki, Finland 31
Length of stay
Total costs
DRG-type
payment
ALOS
reduce costs

Cost accounting
- From a managerial perspective the core for all options is the knowledge
about hospitals` treatment costs
- Common cost accounting approach in
(voluntary) cost data sample participating
hospitals across Germany
Strategic behaviour of hospitals in times of DRGs
1:
Labour
costs
of
the o
ther
medic
al sta
ff
2:
Labour
costs
of
the n
urs
ing s
taff
3:
Labour
costs
of
the a
dm
inis
trative a
nd
4b:
Dru
g c
osts
(in
div
idual costs
/ actu
al
5:
costs
of
impla
nts
and g
raft
s
6a:
Mate
rial costs
(w
ithout
dru
gs,
6b:
Mate
rial costs
(in
div
idual costs
/
actu
al consum
ption,
without
dru
gs,
7:
Medic
al in
frastr
uctu
re c
osts
8:
Non-
medic
al in
frastr
uctu
re c
osts
Cost- Element Groups
- Average costs for each DRG freely available
(in German) on InEK website (www.gdrg.de)
28 September 2010 Aalto University Executive Education | Helsinki, Finland 32
1:
Labour
costs
of
the o
ther
medic
al sta
ff
2:
Labour
costs
of
the n
urs
ing s
taff
3:
Labour
costs
of
the a
dm
inis
trative a
nd
technic
al sta
ff
4a:
Dru
g c
osts
4b:
Dru
g c
osts
(in
div
idual costs
/ actu
al
consum
tion)
5:
costs
of
impla
nts
and g
raft
s
6a:
Mate
rial costs
(w
ithout
dru
gs,
impla
nts
and g
raft
s)
6b:
Mate
rial costs
(in
div
idual costs
/
actu
al consum
ption,
without
dru
gs,
impla
nts
/ gra
fts
7:
Medic
al in
frastr
uctu
re c
osts
8:
Non-
medic
al in
frastr
uctu
re c
osts
1: Normal ward 1.1 1.2 1.3 1.4a 1.4b - 1.6a 1.6b 1.7 1.8
2: Intensive care unit 2.1 2.2 2.3 2.4a 2.4b 2.5 2.6a 2.6b 2.7 2.8
3: Dialysis unit 3.1 2.3 3.3 3.4a 3.4b - 3.6a 3.6b 3.7 3.8
4: Operating room 4.1 - 4.3 4.4a 4.4b 4.5 4.6a 4.6b 4.7 4.8
5: Anaesthesia 5.1 - 5.3 5.4a 5.4b - 5.6a 5.6b 5.7 5.8
6: Maternity room 6.1 - 6.3 6.4a 6.4b - 6.6a 6.6b 6.7 6.8
7: Cardiac diagnostics/ therapy 7.1 - 7.3 7.4a 7.4b 7.5 7.6a 7.6b 7.7 7.8
8: Cardiac diagnostics/ therapy 8.1 - 8.3 8.4a 8.4b 8.5 8.6a 8.6b 8.7 8.8
9: Radiology 9.1 - 9.3 9.4a 9.4b 9.5 9.6a 9.6b 9.7 9.8
10: Laboratories 10.1 - 10.3 10.4a 10.4b 10.5 10.6a 10.6b 10.7 10.8
11: Other diagnostic and therapeutic areas 11.1 11.2 11.3 11.4a 11.4b 11.5 11.6a 11.6b 11.7 11.8
Labour Material Infrastructure
Co
st-
Cen
tre G
rou
ps
Ho
sp
it
al
un
its
wit
h
bed
s
Dia
gn
osti
c a
nd
treatm
en
t are
as

28 September 2010 Aalto University Executive Education | Helsinki, Finland 33
InEK cost data browser: Average costs for normal birth without co-
morbidities or complications in German cost calculating hospitals

DRGs as a management tool
- Product definition and cost accounting empower hospital managers to
improve treatment processes
- Higher quality of care can be achieved due to well organized care chains
Strategic behaviour of hospitals in times of DRGs
- DRGs enable hospitals to benchmark themselves within peer groups
28 September 2010 Aalto University Executive Education | Helsinki, Finland 34

Agenda
1) German healthcare (hospital) system overview
2) Ten years of DRGs in Germany
3) Strategic behaviour of hospitals in times of DRGs
4) Future trends and challenges
28 September 2010 Aalto University Executive Education | Helsinki, Finland 35

Future trends and challenges
DRG introduction was just the first step
Discussion on policy:
Nationwide base rate:
- State governments would lose area of authority
- Statewide rates have the advantage of state specific adjustments
Fixed or maximum prices (selective or uniform negotiations):
- In case of maximum prices sickness funds must be able to negotiate selective
prices for highly specialized, elective or integrated treatment models
- This could lead to a price challenge with neglecting the quality
3628 September 2010 Aalto University Executive Education | Helsinki, Finland

Future trends and challenges
DRG introduction was just the first step
Discussion on policy:
Quality assurance (price adjustments):
- Pay for performance elements are broadly agreed as soon as quality is measurable measurable
- Already possible but not done: not paying for non-performance , present on admission marker
Dual or monistic financing of investments:
- Investment lag due to public dept
- Assumption that monistic financing would make investments easier to schedule due to investment surcharges on top of every DRG
3728 September 2010 Aalto University Executive Education | Helsinki, Finland

Thank you very much for
your time and attention!
This and more presentationsare available on:
www.mig.tu-berlin.de
3828 September 2010 Aalto University Executive Education | Helsinki, Finland