genotype 3: the exception to all the...
TRANSCRIPT

Genotype 3: The exception to all the rules !
Douglas T. Dieterich, M.D
Director, Institute for Liver Medicine
Professor of MedicineDivision of Liver Diseases,
Icahn School of Medicine at Mount Sinai

Genotype Distribution of Hepatitis C
2
GT1a36%
GT1b24%
GT1 (Others)a
10%
GT216%
GT312%
GT41%
GT50.03%
GT61%
• HCV GT3 is the second most common genotype worldwide, estimated to affect 54.3 million people globally1
• In the US, 12% of chronic HCV patients are GT3, the third largest population2
aSubjects with genotype 1 and undetermined subtype. GT=genotype.1. Messina JP, et al. Hepatology. 2015;61:77-87. 2. Manos MM, et al. J Med Virol. 2012;84:1744-1750.
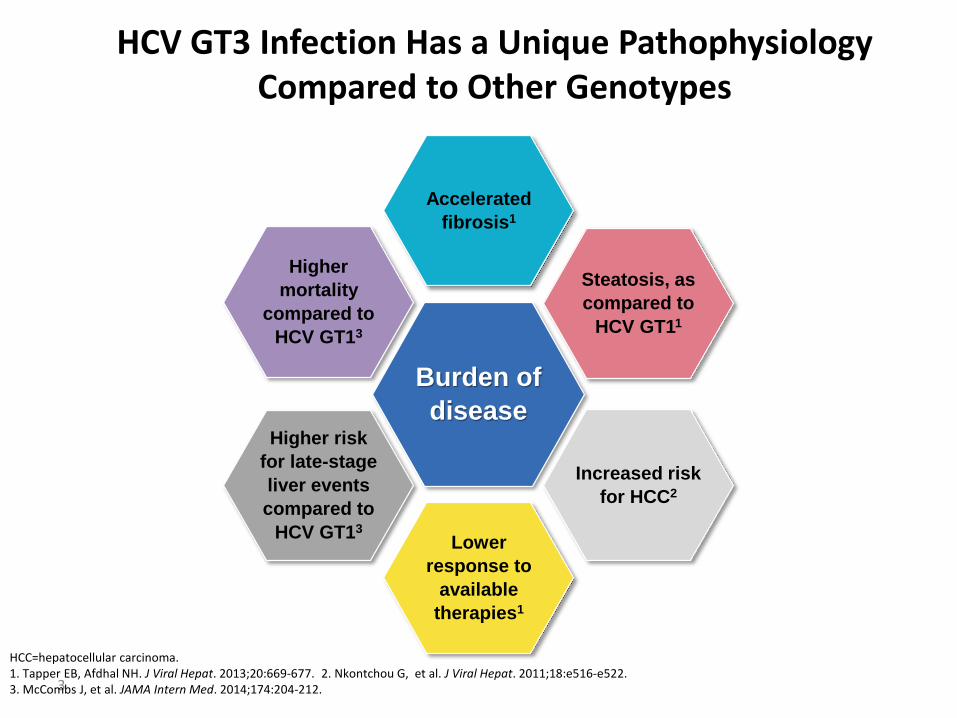
HCV GT3 Infection Has a Unique Pathophysiology Compared to Other Genotypes
3
Burden of
disease
Accelerated
fibrosis1
Steatosis, as
compared to
HCV GT11
Increased risk
for HCC2
Lower
response to
available
therapies1
Higher risk
for late-stage
liver events
compared to
HCV GT13
Higher
mortality
compared to
HCV GT13
HCC=hepatocellular carcinoma.1. Tapper EB, Afdhal NH. J Viral Hepat. 2013;20:669-677. 2. Nkontchou G, et al. J Viral Hepat. 2011;18:e516-e522. 3. McCombs J, et al. JAMA Intern Med. 2014;174:204-212.

HCV GT3 Infection Is Linked to Hepatic Steatosis
Metabolic Steatosis1-3
• Associated with high BMI, hyperlipidemia, and insulin resistance
• HCV acts as a cofactor in the development of the metabolic type of steatosis– HCV induces insulin resistance,
inducing the development of hepatic steatosis
Virally Induced Steatosis1,4
• Directly triggered by the cytopathic effect virus
• Virally induced steatosis is predominantly, and perhaps strictly, linked with HCV GT3 infection– In case of HCV GT3, a direct
relation between intrahepatic viral load and steatosis is observed, suggesting a direct viral effect
4
Across two studies, successful HCV treatment significantly improved or resolved hepatic steatosis in subjects infected with HCV GT3, but not in
those infected with GT11,5-7
BMI=body mass index.1. Roingeard P. J Viral Hepatitis, 2013;20:77-84. 2. Vanni E et al. Hepatol. 2009;50:697-706. 3. Milner KL et al. Gastroenterology 2010;138:932-941. 4. Rubbia-Brandt L, et al. J Hepatol. 2000;33:106-105. 5. Tapper EB, Afdhal NH. J Viral Hepatitis. 2013;20:669-677. 6. Kumar D, et al. Hepatol 2002;36:1266-1272. 7. Caśtera L, et al. Gut. 2000;53:420-424.

Pathogenesis of Hepatic Steatosis in Chronic HCV GT31-3
51. Roingeard P. J Viral Hepatitis. 2013;20:77-84. 2. Syed GH, et al. Trends Endocrinol Metab. 2010;21:33-40. 3. Asselah T, et al. Gut.2006;55:123-130.
• GT3 infection leads to alteration of lipid homeostasis in the liver cells, resulting in accumulation of lipid droplets and hepatic steatosis1,2
Increase Decrease

HCV GT3 Infection Associated With Higher Risk of Liver Disease Progression Compared to GT1
Nearly 1 of every 8 patients with chronic HCV in the US has GT31
Progression to Fibrosis Stage F3–F4*,†,2
• GT3 was associated with maximum likelihood of accelerated fibrosis progression compared to GT1 or GT42
*Predictors of fibrosis progression were assessed in 1189 patients from 2000 to 2008 in the Swiss Hepatitis C Cohort Study.†As modeled by Markov maximum likelihood estimation.‡Retrospective cohort study from fiscal years 2000 to 2009 of 110,484 US veterans with HCV in 128 Veterans Affairs facilities.
1. Manos MM, et al. J Med Virol. 2012;84(11):1744-1750.2. Bochud PY, et al. J Hepatol. 2009;51(4):655-666.3. Kanwal F, et al. Hepatology. 2014;60(1):98-105.
Cirrhosis at Time of Diagnosis by
Genotype‡,3
• Risk of cirrhosis was 31% greater for GT3 patients than for GT13
6

Association of Genotype With Incidence of HCC
• Retrospective cohort study from 2000 to 2009 of 110,484 US veterans with HCV in 128 VA facilities
• Risk of HCC was 80% greater with GT3 than GT1 (adjusted HR, 1.80; 95% CI, 1.61-2.03)
7aPatients with prevalent cirrhosis and HCC were excluded from calculations of cumulative incidence.Kanwal F, et al. Hepatology. 2014;60:98-105.
Cumulative Incidence of HCC by Genotypea
0
0.80
Pro
po
rtio
n F
ree
of
HC
C
1 2 3 4 5 6 7 8 9 10 11
0.82
0.84
0.86
0.88
0.90
0.92
0.94
0.96
0.98
1.00
Number at risk 110,322 97,721 85,335 73,340 60,751 46,489 32,463 19,144 8413 1013
GT1GT2GT3GT4
Years From First Positive HCV RNA

Patient Hx
• 56 year old successful graphic artist born in UK
• Routine life insurance physical after he marries and has child in NYC.
• HCV Genotype 3a
• HCV RNA 3.2million
• HBsAb+
• Hepatitis A IgG +
• Does not want to take IFN
Treatment
• Enrolled in VALENCE clinical trial of SOF/ RBV for 24 weeks
• Perfect patient
• Showed up for all study visits
• EOT viral load negative

Question 1
• What are his chances of relapse?
– 10%
– 15%
– 20%
– 35%
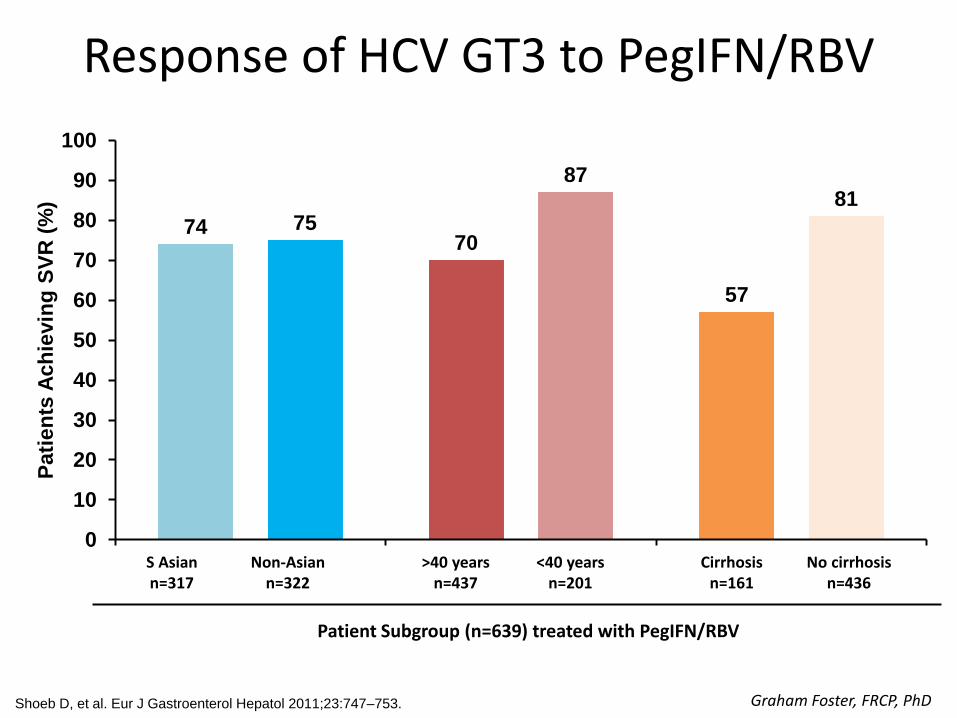
Response of HCV GT3 to PegIFN/RBV
7470
57
75
8781
0
10
20
30
40
50
60
70
80
90
100
Pati
en
ts A
ch
ievin
g S
VR
(%
)
Shoeb D, et al. Eur J Gastroenterol Hepatol 2011;23:747–753.
Patient Subgroup (n=639) treated with PegIFN/RBV
S Asiann=317
Non-Asiann=322
>40 yearsn=437
<40 yearsn=201
Cirrhosisn=161
No cirrhosis n=436
Graham Foster, FRCP, PhD

8882
77
9487
62
100
89
73
95 948689
94
69
0
20
40
60
80
100
Treatment-naïve Treatment-experiencednon-cirrhotic
Treatment-experiencedcirrhotic
SOF + RBV 24 weeks (BOSON) SOF + RBV 24 weeks (VALENCE)
LDV/SOF + RBV 12 weeks (ELECTRON-2) SOF + PEG-IFN + RBV 12 weeks (BOSON)
Zeuzem S, et al. N Engl J Med 2014;370:1993–2001; Gane E, et al. EASL 2014; Oral #6; Gane E, et al. N Engl J Med
2013;368:34–44; Lawitz E, et al. Lancet Infect Dis 2013;13:401–8; Gane E, et al. AASLD 2014; Poster #LB-11; Foster GR, et al.
EASL 2015; Oral #L05; Nelson DR, et al. Hepatology 2015;61:1127–35.
OMV/PTV/RTV + DSV [package insert]; LDV/SOF [package insert]; AASLD/IDSA/IAS-USA. Recommendations for testing, managing, and treating hepatitis C;
DCV [package insert]; RBV [package insert]; AASLD/IDSA. HCV guidelines; Roth D, et al. Lancet 2015 (C-SURFER Study).
Efficacy of DAAs in HCV GT 3:SOF-based Regimens
Graham Foster, FRCP, PhD

9397 100
91 8885
94 9287
60
0
20
40
60
80
100
Overall Nonchirrotic Cirrhotic Nonchirrotic Cirrhotic
SVR
12
(%
)
Genotype 2 (12 weeks)
Genotype 3 (24 weeks)
VALENCE: Sofosbuvir + RBV for 24 weeks
Zeuzem S, et al. NEJM 2014;370:1993
Treatment-Naive Treatment-Experienced
n=73 n=250 n=30 n=92 n=2 n=13 n=33 n=100 n=8 n=45

Algahtani: Results• Genotype 3 treatment with SOF/RBV
was less effective in “real world”– TE cirrhosis -- only 44% SVR– Markers of advanced liver disease
(MELD, albumin, plt count) predictive of EVR
Alqahtani S, et al. 50th EASL; Vienna, Austria; April 22-26, 2015. Abst. P0840.
0
20
40
60
80
100
16/18G3
SOF/P/R
87/133G3
SOF/R
19/22G4
SOF/P/R
3/7G4
SOF/R
12/12G4
SOF/SMV
4/4G4
SOF/SMV/R
89 86
65
43
100 10022/50
CirrExper
17/23Cirr
Naïve
18/23Non-cirr
Exper
30/37Non-cirr
Naïve
44
7874
81
26/50Cirr
Exper
4/23Cirr
Naïve
4/23Non-cirr
Exper
6/37Non-cirr
Naïve
52
1717 16
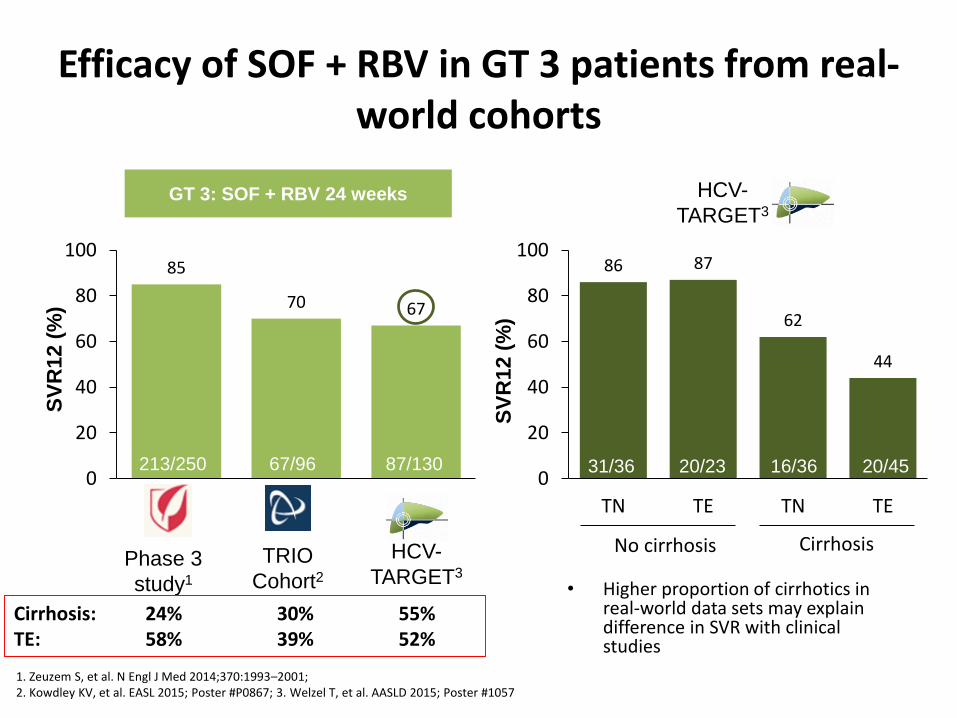
Efficacy of SOF + RBV in GT 3 patients from real-world cohorts
1. Zeuzem S, et al. N Engl J Med 2014;370:1993–2001; 2. Kowdley KV, et al. EASL 2015; Poster #P0867; 3. Welzel T, et al. AASLD 2015; Poster #1057
85
70 67
0
20
40
60
80
100
GT 3: SOF + RBV 24 weeks
Phase 3
study1
TRIO
Cohort2HCV-
TARGET3
213/250 67/96
SV
R12 (
%)
86 87
62
44
0
20
40
60
80
100
TN TE TN TES
VR
12 (
%)
No cirrhosis Cirrhosis
31/36 20/23 16/36 20/45
HCV-
TARGET3
Cirrhosis: 24% 30% 55%TE: 58% 39% 52%
87/130
PB
• Higher proportion of cirrhotics in real-world data sets may explain difference in SVR with clinical studies
RW37

8681
89 88 8981
0
20
40
60
80
100
Efficacy of other SOF-based regimens in GT 3 patients from real-world cohorts
9386
0
20
40
60
80
100
SOF + DCV for 12 weeks is not approved by the EMA for use in GT 3 patients with cirrhosis; SOF + DCV + RBV for 12 or 24 weeks and SOF + DCV for 24 weeks are not
approved by the EMA for use in GT 3 patients without cirrhosis.
1. Foster G et al. Gastroenterology 2015;149:1462–70; 2. Welzel T, et al. AASLD 2015; Poster #1057; 3. Nelson DR, et al. Hepatology 2015;61:1127–35; 4. Welzel T, et al; AASLD 2015; Oral #37; 5. Hèzode C, et al. AASLD 2015; Oral #206
Phase 3
study1
HCV-
TARGET2
SV
R12 (
%)
GT 3: SOF + PEG-IFN + RBV
12 weeks
GT 3: SOF + DCV for 12 weeks
GT 3: SOF + DCV ± RBV 24 weeks
SV
R12 (
%)
168/181
12/14
Phase 3
study3
European4 French5
Compassionate use programmes
135/152
42/49
29/33
47/58
147/166
43/53
PB
Cirrhosis: 44% 71% Cirrhosis: 21% 87% 79%
SOF + DCV 12 weeks 24 weeks + RBV 24 weeks
RW38
Treatment Course
• He relapses at SVR 4 with viral load of 4.6 million
• Very disappointed since he did everything that was asked of him

Question 2
• What do you tell him?
– Go back to the UK; Graham Foster will give you SOF Peg RBV! Suck it up!
– You cant cure them all!
– Better things are on the horizon remain hopeful!
• Its now August 2015 and he comes in asking about new treatments for HCV

Question 3
• Which combination would likely work and be available?
– SOF PEG RBV
– SOF LDV RBV
– SOF DCV

High Overall Virologic Response in HCV GT3 Patients in ALLY 31,2
• SVR12 rates comparable regardless of age, gender, baseline HCV RNA level, or IL28B allele status1,2
• Cirrhotic population: 19% in treatment-naïve group, 25% in treatment-experienced group2
− Among patients with cirrhosis, 34% (11/32) had baseline platelet counts ≤100 X 109 cells/L
• 16 patients relapsed after end of treatment and 1 patient was an on-treatment failure with detectable HCV RNA at final on-treatment visit; of these 17 patients, 12 were cirrhotic2
1. (daclatasvir) Prescribing Information. Bristol-Myers Squibb Company, Princeton, NJ. 2. Nelson DR, et al. Hepatology. 2015;61(4):1127-1135.
* HCV RNA < lower limit of quantification (25 IU/mL). †In the treatment-experienced cohort, 7 patients were sofosbuvir + ribavirin failures, of whom 5 achieved SVR12.
2 ‡Includes 11 patients with missing or inconclusive cirrhosis status.
96
63
0
20
40
60
80
1009086
89
0
20
40
60
80
100
SV
R1
2(%
)*
91/101 44/51 135/152
CirrhoticNoncirrhotic‡
115/120 20/32
Treatment-Naïve
Treatment-Experienced†
Overall
SV
R1
2(%
)*
21

ALLY-3 Study: Impact of Baseline NS5A Y93H Mutation on SVR12 Rates With Daclatasvir + Sofosbuvir
0
20
40
60
80
100
SV
R12 (
%)
98%
13%
No Cirrhosis
67%
CirrhosisAll Patients
92%
68%
25%
No Y93H With Y93H
Genotype 3
Nelson DR, et al. Hepatology. 2015;61:1127-1135.
Population sequencing.
(n=135) (n=13) (n=107) (n=9) (n=28) (n=4)

Ongoing Real-World Study: SVR12 Rates WithRetreatment of Prior DAA Failures (Genotype 3)
• RAVs in sofosbuvir + RBV failures (n=14): 100% SVR12– No RAVs: 79%
– NS5A (A30K/S): 21%
• Retreatment regimens– Daclatasvir + sofosbuvir +
RBV for 12 (n=3) or 24 (n=10) weeks
– Ledipasvir/sofosbuvir + RBV for 24 weeks (n=1)
Vermehren J, et al. J Hepatol. 2016;64(suppl 2):S188. Abstract PS103.
0
20
40
60
80
100
SV
R1
2 (
%)
100% 100%
12 Weeks(n=3)
Interim SVR12 Rates (ITT)
100%
24 Weeks(n=10)
24 Weeks(n=1)
DAC + SOF + RBV LDV/SOF + RBV

ALLY-3+: Cirrhosis +RBV
HC
V R
NA
< L
LOQ
TD/T
ND
(%)
Overall 12 Weeks 16 Weeks
0
10
20
30
40
50
60
70
80
90
100 87 88 86
2630
1416
1214
Treatment-ExperiencedCirrhotic Patients
0
10
20
30
40
50
60
70
80
90
100
Naive Experienced
HC
V R
NA
< L
LOQ
TD/T
ND
(%)
Treatment HistoryAll Patients
1213
3337
92 89
SVR12 (ITT) by Prior Treatment
Leroy V, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. LB-3.

The case continues
• Insurance refuses to pay because he was only stage 2
• Do you send him out for cheeseburger and repeat fibroscan?
• Multiple class action lawsuits are initiated so there is hope in the future for treatment
• Do you tell him that new combinations are coming that work well for Geno 3 patients who failed a SOF based regimen?

ASTRAL-3: SVR12 By Treatment Arm
Mangia A, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. 249.
95
80
0
20
40
60
80
100
SOF/VEL SOF+RBV
SVR
12
(%
)
264/277 221/275
P=0.001

ASTRAL-3: SVR12 By Cirrhosis Status and Treatment History
Mangia A, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. 249.
97 91 97 9087
66
86
63
0
20
40
60
80
100
No Yes Naïve Experienced
SVR
12
(%
)
Cirrhosis Status Treatment History
SOF/VEL SOF+RBV
163187
7380
5583
200206
176204
6471
4571
4 relapses2 other
16 relapses8 other
4 relapses2 other
15 relapses13 other
22 relapses6 other
7 relapses 7 relapses 1 non-response23 relapses2 other
191197
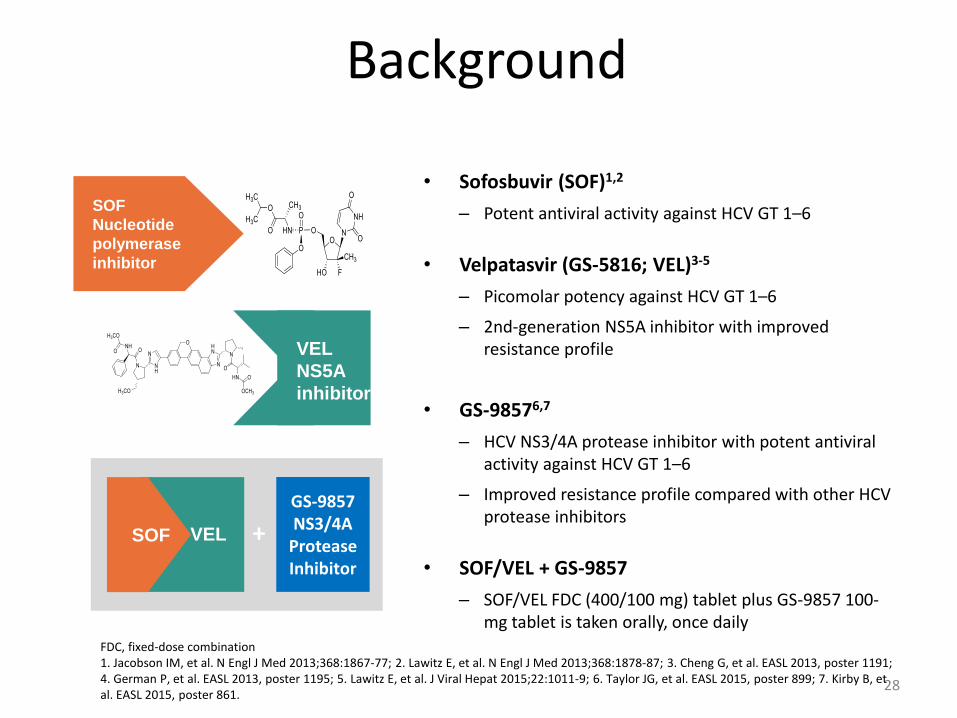
Background
• Sofosbuvir (SOF)1,2
– Potent antiviral activity against HCV GT 1–6
• Velpatasvir (GS-5816; VEL)3-5
– Picomolar potency against HCV GT 1–6
– 2nd-generation NS5A inhibitor with improved resistance profile
• GS-98576,7
– HCV NS3/4A protease inhibitor with potent antiviral activity against HCV GT 1–6
– Improved resistance profile compared with other HCV protease inhibitors
• SOF/VEL + GS-9857
– SOF/VEL FDC (400/100 mg) tablet plus GS-9857 100-mg tablet is taken orally, once daily
FDC, fixed-dose combination1. Jacobson IM, et al. N Engl J Med 2013;368:1867-77; 2. Lawitz E, et al. N Engl J Med 2013;368:1878-87; 3. Cheng G, et al. EASL 2013, poster 1191; 4. German P, et al. EASL 2013, poster 1195; 5. Lawitz E, et al. J Viral Hepat 2015;22:1011-9; 6. Taylor JG, et al. EASL 2015, poster 899; 7. Kirby B, et al. EASL 2015, poster 861.
28
SOF
Nucleotide
polymerase
inhibitor
VEL
NS5A
inhibitor
+
GS-9857NS3/4A
Protease Inhibitor
VELSOF

GT 1
GT 3
SOF/VEL + GS-9857
SOF/VEL + GS-9857
SOF/VEL + GS-9857
SOF/VEL + GS-9857
SOF/VEL + GS-9857
SOF/VEL + GS-9857
SOF/VEL + GS-9857
SOF/VEL + GS-9857
TN Cirrhosis (n=15)
TN No Cirrhosis(n=30)
TECirrhosis (n=17)
TN Cirrhosis (n=18)
TECirrhosis (n=19)
DAA-Experienced ± Cirrhosis (n=30)
PI-TE± Cirrhosis (n=28)
SOF/VEL + GS-9857: Study Design
SVR12
Gane E, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. 38.
Week 0 6 184 168 20

SOF/VEL + GS-9857: SVR12 Rates
100
8983
100
0
20
40
60
80
100
8 8 6 8
SVR
12
(%
)
SOF/VEL + GS-9857
17/17 25/28 15/18 19/19
8 WeeksTE
Cirrhosis
8 WeeksPI TE ±
Cirrhosis
6 WeeksTN
Cirrhosis
8 WeeksTE
Cirrhosis
3 relapses2 relapses1 withdrew consent
GT 1 GT 3
Gane E, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. 38.
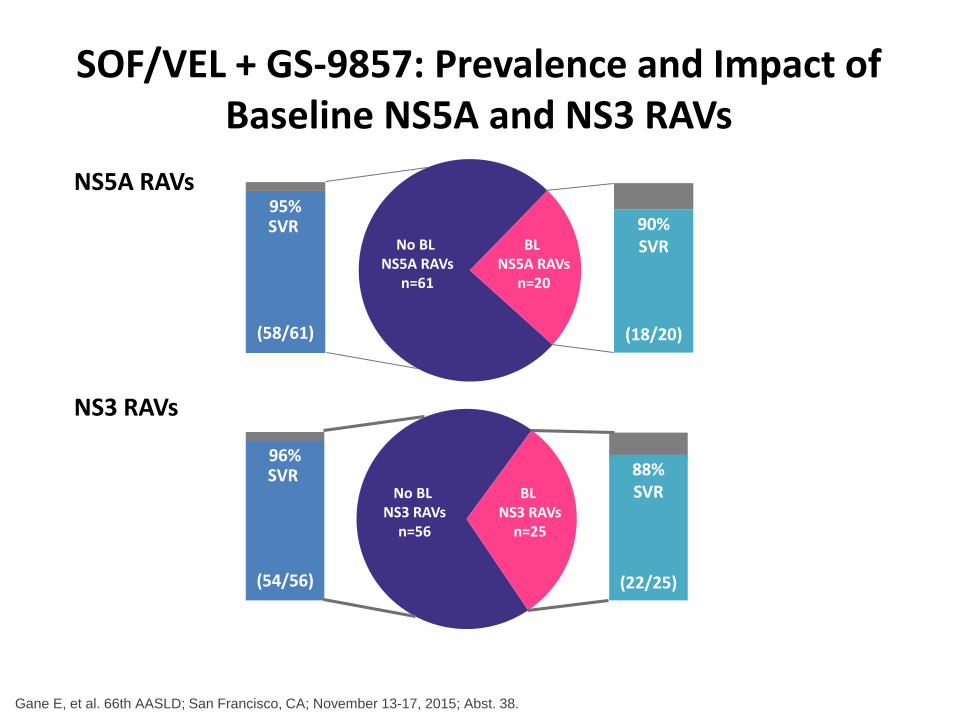
SOF/VEL + GS-9857: Prevalence and Impact of Baseline NS5A and NS3 RAVs
NS5A RAVs
NS3 RAVs
No BL NS3 RAVs
n=56
BL NS3 RAVs
n=25
(54/56)
96%SVR 88%
SVR
(22/25)
No BL NS5A RAVs
n=61
BL NS5A RAVs
n=20
90% SVR
(18/20)(58/61)
95%SVR
Gane E, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. 38.

EASL 2016, Barcelona
High Efficacy of Sofosbuvir/Velpatasvir Plus GS-9857 for 12 Weeks in Treatment-Experienced
Genotype 1–6 HCV-Infected Patients, Including Those Previously Treated With Direct-Acting
Antivirals
Eric Lawitz1, Kris Kowdley2, Michael Curry3, Nancy Reau4, Mindie Nguyen5, Paul Kwo6, Ira Jacobson7, Tram T. Tran8, Ronald Nahass9, Federico Hinestrosa10, Robert Herring Jr.11, Michael Bennet12, Jenny C. Yang13, Luisa M. Stamm13, Di An13, Hadas Dvory-Sobol13, Diana M. Brainard13, John G. McHutchison13, Eugene
Schiff14, Mitchell Davis15, Kyle Etzkorn16, Raymond T. Chung17, David Pound18, Maribel Rodriguez-Torres19, K. Rajender Reddy20, Ziad Younes21, Edward J.Gane22
1Texas Liver Institute, San Antonio, Texas, USA; 2Swedish Medical, Seattle, Washington, USA; 3Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA; 4Rush University Medical Center, Chicago, Illinois, USA; 5Stanford University, Palo Alto, California, USA; 6Indiana University School of Medicine, Indianapolis, USA; 7Mount Sinai Beth Israel, New York, USA; 8Cedars
Sinai Medical Center, Los Angeles, California; 9ID Care, Hillsborough, New Jersey, USA; 10Orlando Immunology Center, Florida, USA; 11Nashville Gastrointestinal Specialists Inc., Tennessee, USA; 12Medical Associates Research Group, Inc., San Diego,
California; 13Gilead Sciences, Inc., Foster City, California; 14University of Miami, Florida, USA; 15Digestive CARE-South Florida Center of Gastroenterology, Wellington, Florida, USA; 16Borland-Groover Clinic, Jacksonville, Florida, USA; 17Massachusetts General Hospital, Boston, Massachusetts; 18Indianapolis Gastroenterology Research Foundation, Indianapolis, Indiana, USA;
19Fundación De Investigación De Diego, San Juan, Puerto Rico; 20University of Pennsylvania , Philadelphia, USA; 21Gastro One, Germantown, Tennessee, USA; 22Auckland Clinical Studies, New Zealand

SOF/VEL + GS-9857 - Study Design
• Two Phase 2, multicenter, open-label studies (US, New Zealand)
– GS-US-367-1168: G1
– GS-US-367-1169: G2, 3, 4, 5, 6
• Broad inclusion criteria
– HCV treatment experienced, including DAA experienced
• G1: NS5A inhibitor or ≥2 DAA classes
• G2–6: Peg-IFN + RBV or any DAA
– 50% with compensated cirrhosis
0 12 24
SVR12SOF/VEL + GS-9857N=128
Week
Lawitz E, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. PS008.
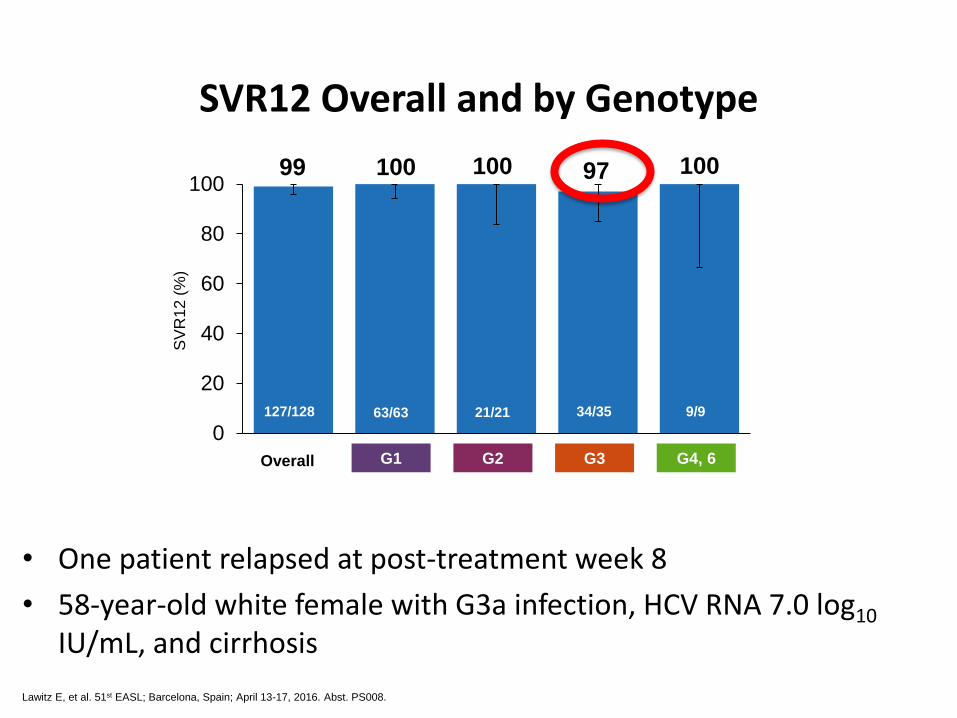
99 100 100 97 100
0
20
40
60
80
100
SVR12 Overall and by Genotype
• One patient relapsed at post-treatment week 8
• 58-year-old white female with G3a infection, HCV RNA 7.0 log10
IU/mL, and cirrhosis
SV
R12
(%
)
Overall G3G2 G4, 6G1
63/63127/128 9/934/3521/21
Lawitz E, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. PS008.

100 98 99 100 100 97 100
0
20
40
60
80
100
No Yes No Yes 0* 1 ≥2
No. of DAA ClassesPrior NS5A
ExperienceCirrhosis
SVR12 by Subgroup
*GT 2-6 patients who failed prior Peg-IFN+RBV regimens. 35
SV
R1
2 (
%)
67/67 92/93 27/2735/35 35/36 65/6560/61

Resistance Analysis
*Deep sequencing with 1% assay cutoff. 36
99%
SVR12
100%SVR12
51/51
99%SVR12
76/77
40% No Baseline
RAVs
(51/128)
60% Baseline RAVs
(77/128)
20%NS5A RAVs
only
15% NS3 RAVs
only
23%Multiple
class
RAVS2%
NS5B RAVs only

EASL 2016, Barcelona
Sofosbuvir/Velpatasvir in Combination With Ribavirin for 24 Weeks Is Effective
Retreatment for Patients Who Failed Prior NS5A-Containing DAA Regimens:
Results of the Retreatment Study
Edward J. Gane1, Mitchell L. Shiffman2, Kyle Etzkorn3, Giuseppe Morelli4, Catherine Stedman5, Mitchell N. Davis6, Federico Hinestrosa7,
Hadas Dvory-Sobol8, K.C. Huang8, Anu Osinusi8, John McNally8, Diana M. Brainard8, John G. McHutchison8, Alex Thompson9, Mark Sulkowski10
1Auckland Clinical Studies, Auckland, New Zealand; 2Liver Institute of Virginia, Richmond, Virginia, USA; 3Borland Groover Clinic, Jacksonville, Florida, USA; 4University of Florida, Gainesville, Florida, USA; 5Christchurch Clinical Studies
Trust, Christchurch, New Zealand; 6South Florida Center of Gastroenterology, Wellington, Florida, USA; 7Orlando Immunology Center, Orlando, Florida, USA; 8Gilead Sciences, Inc., Foster City, California, USA; 9St Vincent’s Hospital,
Melbourne, Australia; 10Johns Hopkins University School of Medicine, Baltimore, Maryland, USA

9197 91
76
0
20
40
60
80
100
3334
1317
1314
Total GT 1 GT 2 GT 3
Results: SVR12 by Genotype
38
SVR
12
(%
)
1 relapse*
1 nonresponse2 relapses1 WC1 relapse+
5965
+ Relapse after discontinuing treatment at week 3 *Relapse after discontinuing treatment at Week 8, Error bars represent 95% confidence intervals; WC, withdrew consent.

SVR12 by NS5A RAVs
• 11/13 GT 3 patients with RAVs had Y93H; 9 (82%) achieved SVR12
• 5 patients had 2 NS5A RAVs; all 5 achieved SVR12
• 3 patients had NS3 RAVs; all 3 achieved SVR12
1% deep sequencing cut-off. *1 patient could not be sequenced; 1 patients who withdrew consent was excluded.
39
GT 2 (n=13*)GT 1 (n=34) GT 3 (n=16)
100% SVR
100% SVR
100% SVR
38%No RAVs
5/13
62%RAVs8/13
82%No RAVs
28/34
18%RAVs6/34
19%No RAVs3/16
81%RAVs13/16
100% SVR
77% SVR
10/133/38/85/56/6
96% SVR
27/28

ABT-493 identified by AbbVie and Enanta.1. Ng TI, et al. Abstract 636. CROI, 2014. 2. Ng TI, et al. Abstract 639. CROI, 2014.
Next Generation Direct-acting Antivirals
ABT-530PangenotypicNS5A inhibitor
ABT-493Pangenotypic NS3/4A
protease inhibitor
In vitro:1,2
• High barrier to resistance
• Potent against common NS3 variants (eg., positions 80, 155, 168) and NS5A variants (eg., positions 28, 30, 31 and 93)
• Additive/synergistic antiviral activity
Clinical PK & metabolism:
• Once-daily oral dosing
• Minimal metabolism and primary biliary excretion
• Negligible renal excretion (<1%)

Stable HCV GT3a Replicon EC50
NS3/4A Protease Inhibitor
nM NS5A Inhibitor pM
ABT-493 1.6 ABT-530 2
Grazoprevir1 35 Elbasvir7 140
GS-98572 6.1 Velpatasvir8 20
Simeprevir3,4 472 Ledipasvir9 168,000
Paritaprevir 19 Ombitasvir 19
Asunaprevir5 1162 Daclatasvir10 530
Odalasvir 48
MK-840811 2
ABT-493 and ABT-530 Have Potent Activities Against All HCV Genotypes, Including GT3
1. Lahser F, et al. AASLD, 2014. 2. Taylor J, et al. EASL, 2015. 3. Olysio prescribing information. 4. Chase R, et al. IAPAC, 2013.5. McPhee F, et al. AAC, 2012. 6. Yang H, et al. AAC, 2014. 7. Liu R, et al. AAC doi:10.1128/AAC.01390-15 8. Cheng G, et al. EASL, 2013.9. Cheng G, et al. EASL, 2012 10. Wang C, et al. AAC, 2014.11. http://files.shareholder.com/downloads/ACHN/0x0x602481/8b28c708-13b6-420d-9325-401c57b89001/ACHN_R_D_Day_Final.pdf12. Asante-Appiah E, AASLD, 2014.

NS5A Inhibitor Fold Change in EC50 for GT3 NS5A Variants
M28T A30K Y93H
ABT-530 0.4 1.1 2.5
Ledipasvir1 NA >1000 >1000
Velpatasvir2 NA 10 – 100 >100
Daclatasvir3 46 56 - 62 2738 – 2752
Elbasvir4 NA 50 486
Ombitasvir5 423 NA 6728
MK-8408 NA NA NANA, not available
ABT-530 Retains Antiviral Activity Against Common GT3 Single-Position NS5A Variants
1. Hernandez D, et al. J Clin Virol, 2013. 2. Doehle BP, et al. EASL, 2015. 3. Wang C, et al. AAC, 2013:57:611-3.4. Gane E, et al. EASL, 2015. 5. Krishnan P, et al. AAC, 2015.
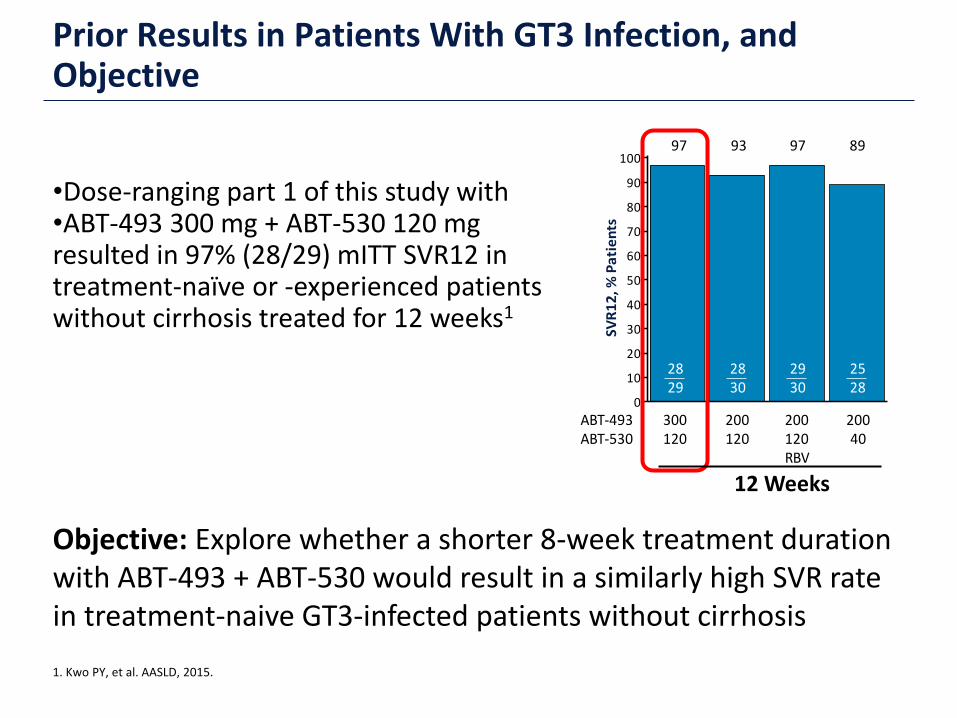
•Dose-ranging part 1 of this study with •ABT-493 300 mg + ABT-530 120 mg resulted in 97% (28/29) mITT SVR12 in treatment-naïve or -experienced patients without cirrhosis treated for 12 weeks1
Prior Results in Patients With GT3 Infection, and Objective
1. Kwo PY, et al. AASLD, 2015.
Objective: Explore whether a shorter 8-week treatment duration with ABT-493 + ABT-530 would result in a similarly high SVR rate in treatment-naive GT3-infected patients without cirrhosis
SVR
12
, % P
ati
en
ts
0
10
20
30
40
50
60
70
80
90
1008993
2829
2830
300120
200120RBV
97
20040
2528
2930
200120
ABT-493ABT-530
97
12 Weeks

•No virologic failures
•1 patient withdrew consent after treatment week 6 due to intolerance of blood draws and had an undetectable HCV RNA at the time of discontinuation
mITT SVR12 rate excludes non-virologic failures
SVR12 AnalysisSV
R12
, % P
atie
nts
0
10
20
30
40
50
60
70
80
90
10097
2829
SVR12
100
mITTSVR12
2828

ABT-493 and ABT-530 +/- RBV in G3 with Cirrhosis
• Higher rates of liver steatosis and an increased risk for hepatocellular carcinoma and fibrosis progression than other HCV genotypes
• Approximately 30% of HCV infections worldwide
• Now the most difficult-to-cure genotype, particularly in patients with cirrhosis
Current EASL recommendations for G3-infected patients with cirrhosis
SVR12
SOF + RBV for 24 weeks 79%
SOF + Peg-IFN/RBV for 12 weeks 88%
SOF + DCV + RBV for 24 weeks 85%
Kwo P, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. LB01.

Kwo P, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. LB01.
ABT-493 and ABT-530 +/- RBV in G3 with CirrhosisSVR12 by ITT Analysis
100 100
0
20
40
60
80
100
.ABT-493+ ABT-530
ABT-493+ ABT-530 + RBV
SVR
12
, % P
atie
nts
24 /24
24 / 24

C-CREST 1 and 2: Grazoprevir/MK-8408/MK-3682
• 240 patients (G1a, n = 46; G1b, n = 47; G2, n = 61; G3, n = 86)
• Treatment naïve, non-cirrhotic
Gane E, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-139.
FW = follow-up week; TW = treatment week
Study Design
G1 (n=23)G2 (n=16)G3 (n=21)
Mk-3682 (300 mg) +GZR + MK-8408
Mk-3682 (300 mg) +GZR + MK-8408
D1 TW4 TW8 FW4 FW8 FW12 FW24
Mk-3682 (450 mg) +GZR + EBR
Mk-3682 (300 mg) +GZR + EBR
SVR121st Endpoint
SVR242nd Endpoint
G1 (n=23)G2 (n=15)G3 (n=22)
G1 (n=24)G2 (n=14)G3 (n=21)
G1 (n=23)G2 (n=16)G3 (n=22)

100
69
86
100
60
86
100
71
95
8794
91
0
20
40
60
80
100
G1 G2 G3
SVR
24
(%
)
C-CREST 1 and 2: Secondary endpoint
Gane E, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-139.
LTFU = lost to follow up† One G1b patient receiving MK-3682 (450 mg)/GZR/MK-8408 and 1 G3 patient receiving MK-3682 (300 mg) GZR/EBR were lost to follow-up between FW12 and FW24; both had achieved SVR12.
MK-3682 (300 mg)/GZR/EBRMK-3682 (450 mg)/GZR/EBRMK-3682 (300 mg)/GZR/MK-8408MK-3682 (300 mg)/GZR/MK-8408

C-CREST 1 and 2: Grazoprevir/MK-8408/MK-3682 No Impact of Baseline RAVs on SVR
Gane E, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-139.
0
10
20
30
40
50
60
70
80
90
100
SVR1297%
0
10
20
30
40
50
60
70
80
90
100
SVR12100%
GT1 NS5A RAVs GT1 NS3 RAVs GT1 NS5B RAVs
0
10
20
30
40
50
60
70
80
90
100
SVR1297%
0
10
20
30
40
50
60
70
80
90
100
SVR1298%
0
10
20
30
40
50
60
70
80
90
100
SVR1299%
0
10
20
30
40
50
60
70
80
90
100
SVR1295%
Prevalence Prevalence Prevalence
No RAVsn=70(76%)
No RAVsn=38(41%)
No RAVsn=73(79%)
RAVsn=22(24%)
RAVsn=54(59%)
RAVsn=19(21%)
6870
3738
7273
2222
5354
1819
0
10
20
30
40
50
60
70
80
90
100
SVR12100%
0
10
20
30
40
50
60
70
80
90
100
SVR1285%
GT3 NS5A RAVs GT3 NS3 RAVs GT3 NS5B RAVs
0
10
20
30
40
50
60
70
80
90
100
SVR12100%
0
10
20
30
40
50
60
70
80
90
100
SVR1292%
0
10
20
30
40
50
60
70
80
90
100
SVR1293%
0
10
20
30
40
50
60
70
80
90
100
SVR12100%
Prevalence Prevalence Prevalence
No RAVsn=22(52%)
No RAVsn=4(10%)
No RAVsn=41(98%)
RAVsn=20(48%)
RAVsn=38(90%)
RAVsn=1(2%)
2222
44
3841
1720
3538
11
NGS was performed with a 15% sensitivity threshold. GT3 NS5A RAVs: any change from wild type at 10 positions (24, 28, 30, 31, 32, 38, 58, 62, 92, 93).GT3 NS3 RAVs: any change from wild type at 14 positions (36, 54, 55, 56, 80, 107, 122, 132, 155, 156, 158, 168, 170, 175).GT3 NS5B RAVs: any change from wild type at 6 positions (159, 239, 282, 316, 320, 321).
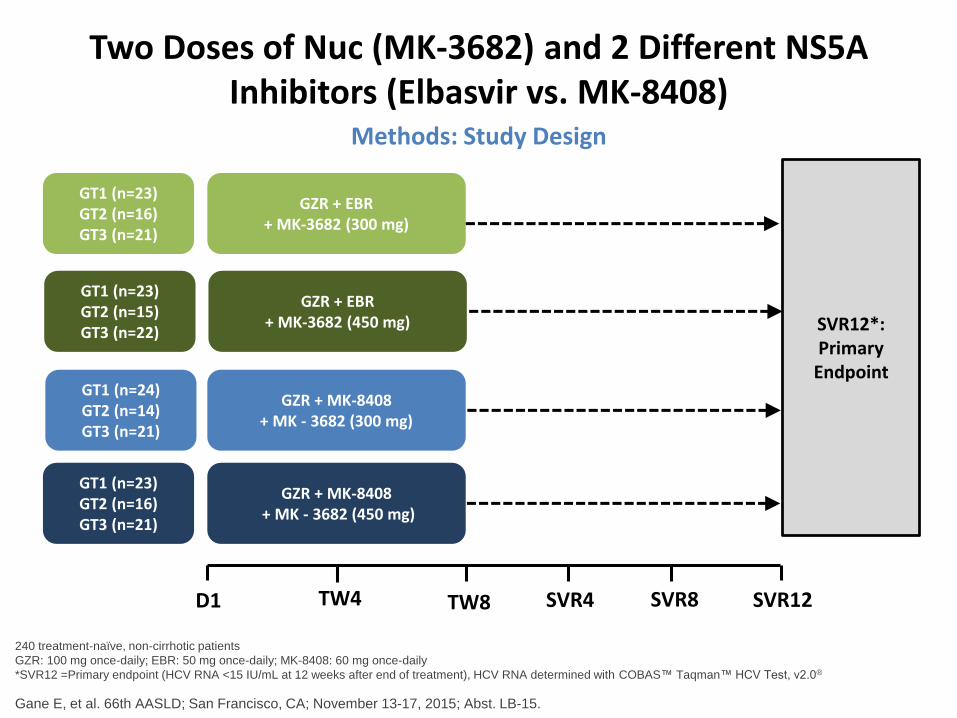
Two Doses of Nuc (MK-3682) and 2 Different NS5A Inhibitors (Elbasvir vs. MK-8408)
Gane E, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. LB-15.
240 treatment-naïve, non-cirrhotic patients
GZR: 100 mg once-daily; EBR: 50 mg once-daily; MK-8408: 60 mg once-daily
*SVR12 =Primary endpoint (HCV RNA <15 IU/mL at 12 weeks after end of treatment), HCV RNA determined with COBAS™ Taqman™ HCV Test, v2.0®
Methods: Study Design
GT1 (n=23)GT2 (n=16)GT3 (n=21)
GT1 (n=23)GT2 (n=15)GT3 (n=22)
GT1 (n=24)GT2 (n=14)GT3 (n=21)
GT1 (n=23)GT2 (n=16)GT3 (n=21)
GZR + EBR + MK-3682 (300 mg)
GZR + MK-8408+ MK - 3682 (300 mg)
GZR + EBR + MK-3682 (450 mg)
GZR + MK-8408+ MK - 3682 (450 mg)
SVR12*: Primary
Endpoint
D1 TW4 TW8 SVR4 SVR8 SVR12

8 Week Regimen of GZR/MK-8408/MK-3682 (450 mg)
Gane E, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. LB-15.
*Primary efficacy: SVR12 of full analysis set (FAS). All 240 enrolled patients completed 8 weeks of treatment and reached follow-up 12 weeks after end of treatment.
100
69
90
100
60
86
100
71
9591 94 91
0
20
40
60
80
100
GT1 GT2 GT3
% S
VR
12
GZR/EBR/MK-3682 300 mg GZR/EBR/MK-3682 450 mgGZR/MK-8408/MK-3682 300 mg GZR/MK-8408/MK-3682 450 mg
2323
2323
2424
2123
1116
915
1014
1516
1921
1922
2021
2022

8 Week Regimen of GZR/MK-8408/MK-3682 (450 mg) Compared to Prior 12-Week Regimens
Gane E, et al. 66th AASLD; San Francisco, CA; November 13-17, 2015; Abst. LB-15., *Zeum et al., Ann Int Med 163:1, 2015; †Brown et al., EASL,
2015, Abst P0771; ‡Gane et al., EASL, 2015, Abst P0776
95
80
45
100
71
9591 94 91
0
20
40
60
80
100
GT1 GT2 GT3
% S
VR
12
12 Weeks GZR/EBR = RBV
8 Weeks GZR/MK-8408/MK-3682 (300 mg)
8 Weeks GZR/MK-8408/MK-3682 (450 mg)
273*288
2424
2123
24†
301014
1516
9‡
20
2021
2022

Conclusion
• Geno 3 responsible for about a third of global HCV
• It causes steatosis and more rapid progression to ESLD and HCC
• It has been our most difficult genotype to treat
• Better drugs for it are on the horizon!