gender-specific differences associated with living donor liver transplantation: a review study
TRANSCRIPT
ORIGINAL ARTICLE
Gender-Specific Differences Associatedwith Living Donor Liver Transplantation:A Review StudyHanna C. Hermann, Burghard F. Klapp, Gerhard Danzer, and Christina PapachristouMedical Clinic for Internal Medicine and Psychosomatics, Charite–Universitatsmedizin Berlin,Berlin, Germany
Living donor liver transplantation (LDLT) has developed into an important therapeutic option for liver diseases. For living do-nor kidney transplantation (LDKT), gender-specific differences have been observed among both donors (two-thirds beingwomen and one-third being men) and recipients (two-thirds being men and one-third being women). The aim of this studywas to determine whether there is a gender disparity for LDLT. We contacted 89 national and international transplantationregistries, single transplant centers, and coordinators. In addition, a sample of 274 articles dealing with LDLT and its out-comes was reviewed and compared with the registry data. The data included the gender of the donors and recipients, thecountry of transplantation, and the donor-recipient relationship. The investigation showed that overall there were slightlymore men among the donors (53% male and 47% female). As for the recipients, 59% of the organs were distributed tomales, and 41% were distributed to females. Differences in the gender distribution were observed with respect to individualcountries. Worldwide, 80% of the donors were blood-related, 11% were not blood-related, and 9% were spouses. The dataacquired from the publications were similar to the registry data. Our research has shown that there are hardly any registrydata published, a lot of countries do not have national registries, or the access to these data is difficult. Even widely rangingpublished studies often do not give information on the gender distribution or the donor-recipient relationship. Further investi-gations are needed to understand the possible medical, psychosocial, or cultural reasons for gender distribution in LDLTand the differences in comparison with LDKT. Liver Transpl 16:375-386, 2010. VC 2009 AASLD.
Received June 30, 2009; accepted November 30, 2009.
INTRODUCTION
Liver transplantation is an important therapy forreducing the mortality in patients with terminal liverdiseases. Living donor liver transplantation (LDLT)represents a very effective alternative to deceased liverdonation and is a good possibility for expanding thedonor pool and therefore reducing the discrepancybetween needed and available organs.
The donors are mostly healthy family members orindividuals with close emotional ties to the recipients.These people are exposed to a high degree of psycho-logical pressure to make a decision because, on the
one hand, they can save a human life but, on theother hand, they will be exposed to health risks.Today, the outcome is very similar to that found fordeceased donors because of experience, consistentlyimproved matching of prospective donors, advances insurgical techniques, and the development of immuno-suppressive therapy; moreover, the outcome in chil-dren is even better than that in adults.1
Aspects of Gender
The aim of this study was to examine this topic withrespect to the aspect of the gender-specific
Additional Supporting Information may be found in the online version of this article.
Abbreviations: A, adult; CI, confidence interval; IRODaT, International Registry of Organ Donation and Transplantation; LDKT,living donor kidney transplantation; LDLT, living donor liver transplantation; MCS, multicenter study; NA, not available;P, pediatric; R, review; SCS, single-center study; UCLA, University of California Los Angeles.Address reprint requests to Hanna C. Hermann, (care of Christina Papachristou), Medical Clinic for Internal Medicine and Psychosomatics,Charite–Universitatsmedizin Berlin, Luisenstrasse 13a, 10117 Berlin, Germany. Telephone: þ49/30/450 553 278; FAX: þ49/30/450 553989;E-mail: [email protected]
DOI 10.1002/lt.22002Published online in Wiley InterScience (www.interscience.wiley.com).
LIVER TRANSPLANTATION 16:375-386, 2010
VC 2009 American Association for the Study of Liver Diseases.

distribution of the donors. The concept of gender inthe field of medicine includes not only sex, with bothits primary and secondary characteristics, but evenmuch more so the psychological, sociocultural, andspecific sexual characteristics that influence behavior.
If there is an irregular distribution, it is important tonotice it and take it into consideration because this alsoallows one to draw conclusions involving ethical, psy-chological, and behavioral aspects, which are importantfor the adequate care of both donors and recipients.
Living Donor Kidney Transplantation (LDKT)
LDKT has already been performed for over 50 years andis an established practice in treating terminal kidneydiseases. Gender-specific differences have been exam-ined in detail. Here, the majority of the donors arewomen (two-thirds), whereas women, in contrast, arerecipients of only one-third of the organs. This is thecase for all age groups and is similar in different ethnicgroups.2 According to the literature, an explanation forthis could be that men provide the main income for thefamily and that women feel more responsible for thehealth and welfare of the family and therefore considerthe act of donation to be their duty. Women are possiblymore susceptible to family pressure than men and cantherefore be persuaded more rapidly and more easily.From a medical viewpoint, it can be assumed thatwomen more frequently come into consideration asdonors because elderly women are less likely to sufferfrom cardiovascular illnesses and diabetes than elderlymen. One must say, however, that the chance of beingrejected as a donor because of existing illnesses is equalfor both men and women.3,4
Research Questions, Methods, and Aim of the
Study
One part of this study involved searching for and con-tacting registries that document transplant activity inthe different countries of the world. The other partconsisted of reviewing and summarizing the results ofprevious studies and publications dealing with LDLTto give an overview of the present literature concern-ing gender in LDLT. Subsequently, the gender-specificdifferences were examined and analyzed for both thedonors and the recipients. In the discussion, the datafrom the different national registries are comparedwith the findings in the reviewed publications. Theadvantages and disadvantages of using publicationdata, as well as the importance of looking at both theregistry data and the publication data, are discussed.Occurring problems are also presented and examinedin detail. Possible ideas concerning further interestinginvestigations that could offer more details regardingthis topic are provided. The results of this studyshould provide answers to the following questions:
1. What is the gender-specific distribution forLDLT?
2. Are there gender-specific differences with respectto geographical locations? Here, an attempt
should be made to find out what the differencesare between individual countries and/or conti-nents. Should there be differences, and whatcould be the proper explanation for them?
3. Who act as donors, for whom and how frequentlydo they act as donors (eg, women to men, womento women, men to men, and men to women), andwhat relationship do donors and recipients havewith one another?
4. Are the data presented in publications andreviews representative of the actual data pro-vided by the registries?
PATIENTS AND METHODS
Contacting and Searching for National
Registries
At first, the official Web site of the International Regis-try of Organ Donation and Transplantation (IRODaT)was examined. IRODaT is a registry that provides an-nual numbers on donation and transplantation activ-ity worldwide. National registries were sought to findout who is responsible for the data in each country. Ifthere was a Web site of a specific national registry, itwas searched for information concerning the numberof LDLT procedures performed until today, the num-ber of male and female donors as well as recipients,and the donor-recipient relationship. If there wasno information given, the registries were contacted bye-mail. The following questions were asked:
1. How many LDLT procedures have been per-formed up to now in the country?
2. How many recipients were male, and how manywere female?
3. How many donors were male, and how manywere female?
4. Is there any information about the relationshipbetween recipients and donors?
If there was no reply, the registries were contacted asecond time. In countries that do not have a nationalregistry, for which a Web site was not available inEnglish, or from which there was no reply to the sec-ond e-mail, transplant coordinators or single institu-tions were contacted.
Another way of obtaining data was the 2009 OrganDonation Congress (10th Congress of the Interna-tional Society for Organ Donation and Procurementand 16th Congress of the European Transplant Coor-dinators Organization), at which transplantation coor-dinators from different countries were contacted inorder to contact transplantation centers.
The data acquired from this research are docu-mented in Table 1.
Review Search Concerning Publications and
Reviews Dealing with LDLT
Furthermore, we conducted an article review ofpublications and reviews dealing with LDLT. In this
376 HERMANN ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

section, we describe how the search and selection ofarticles were carried out.
The PubMed database and the World Wide Web weresearched. Between February/March 2008 and October2009, the following MeSH headings and text words wereused: living donor liver transplantation, living donor liver
transplantation gender, living donor liver transplantationgender imbalance, living donor liver transplantation gen-der discrepancies, gender disparity, gender distribution,gender disproportion, living donation gender, living dona-tion gender discrepancies, living donation gender imbal-ance, living donation gender disparity, living donor liver
TABLE 1. Data from Registries and Transplantation Centers
Location*
Donors [n (%)]† Recipients [n (%)]‡Relationship Between the
Donors and Recipients [n %)]§
Male Female
Not
Recorded Male Female
Blood-
Related
Not Blood-
Related Spouse
Argentina — — — — — — —Austria 24 (52%) 22 (48%) 14 (30%) 32 (70%)Australia/
New Zealand23 (57%) 17 (43%) — — 35 4
Belgium 161 (49%) 166 (51%) 181 (55%) 146 (45%) 297 11 19Brazil — — — — — — —Bulgaria — — — — — — —Canada — — — — — — —China — — — — — — —Beijing, China 41 (59%) 28 (41%) 52 (75%) 14 (25%) 58 8Hong Kong,
China180 (40%) 258 (60%) 313 (71%) 125 (29%) 283 35 120
Croatia 2 (100%) 1 (50%) 1 (50%) 1 1Egypt — — — — — — —France 242 (56%) 188 (44%) 249 (58%) 181 (42%) 362 3 65Germany 429 (50%) 428 (50%) 496 (58%) 361 (42%) 713 27 117Hungary — — — — — — —India — — — — — — —Israel — — — — — — —Italy 134 (58%) 99 (42%) 1 148 (64%) 85 (36%) 206 8 20Iran — — — — — — —Japan — — — — — — —Tokyo, Japan 238 (54%) 202 (46%) 232 (53%) 208 (47%) 287 26 78Seoul, Korea
(2005-2007)1120 590 1270 440 1485 81 144
Lebanon 1 3 3 (75%) 1 (25%)Malaysia 37 (49%) 38 (51%) 41 (55%) 34 (45%) 63 12Mexico 26 (58%) 19 (42%) 20 (44%) 25 (56%) 43 1 1Netherlands 5 (36%) 9 (64%) 10 (71%) 4 (29%) 11 3Poland 50 (36%) 90 (64%) 64 (46%) 76 (54%)Portugal — — — — — — —Romania 23 (51%) 22 (49%) 13 (33%) 33 (67%) 37 2 7Saudi Arabia — — — — — — —Singapore — — — — — — —Spain — — 101 (54%) 87 (46%) 164 16 8Switzerland — — — — — — —Taiwan — — — — — — —Turkey — — — — — — —United Kingdom 87 (65%) 46 (35%) 4 81 56 132 1 2Ukraine — — — — — — —United States 1924 (49%) 1987 (51%) 2118 1792 2944 725 221Venezuela — — — — — — —Total sum 4745 (53%) 4211 (47%) 8 5407 (59%) 3701 (41%) 7121 (80%) 943 (11%) 823 (9%)
NOTE: A dash indicates that no data were provided for the category.*The country or city in which the transplants took place.†Data regarding the donors have been divided into the following categories: male, female, and not recorded.‡Data regarding the recipients have been divided into the following categories: male and female.§Data regarding the relationship between donors and recipients have been divided into the following categories: blood-related, not blood-related, and spouse.
GENDER-SPECIFIC DIFFERENCES IN LDLT 377
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

outcome, living donor liver transplantation Asia, livingdonor liver transplantation Korea, living donor livertransplantation Japan, living donor liver transplantationTaiwan, and donation þ gender.
After the MeSH headings and text words wereentered, a substantially different number of articleswere listed. Using the headings and abstracts of thearticles as a preliminary method for selection, weexcluded articles whose theme did not match the spe-cific exclusion and inclusion criteria.
Exclusion criteria for the preliminary selection ofpublications were as follows:
1. The article does not deal with LDLT donors/patients.
2. The article deals with very specific complications,such as biliary complications (because these com-plications do not occur in all donors/patients, thiswould represent a strong selection bias).
3. The article should be an observational study (longi-tudinal or cross-sectional) because such studiesare more likely to report data regarding the genderof donors and recipients and their type of relation-ship. Such studies also tend to be more represen-tative of the population involved. This is why thefollowing articles were excluded:a. Articles dealing with studies concerning
medications.b. Articles explaining the surgical techniques and
procedures of liver transplantation without pre-senting a recipient/donor sample.
c. Articles involving histological parameters andproteins and not the donors/recipients.
Inclusion criteria for the selection of publicationswere as follows:
1. The article includes information on the gender ofthe donors/recipients.
2. The article reports on the psychosocial outcomeof the donors/recipients, their quality of life, andthe donor-recipient relationship.
3. The article includes empirical reports from trans-plantation centers and countries.
4. The article presents the current state of affairsregarding LDLT.
To avoid counting patients twice, the selection waslimited to 1 article from each center if it was a single-center study. The article from each center that pre-sented the highest number of patients was preferred.If there were 2 publications from the same center, but1 article presented only the donors and the other pre-sented only the recipients, both were listed.
The next step was to collect all relevant informationfrom the abstracts. Each article was examined in theform of a PDF document and was searched for the termsmale, female, women, men, gender, sex, and relationship.Once again, the articles were examined with the afore-mentioned inclusion and exclusion criteria, and the inap-propriate articles were then subsequently sorted out. Forsome of the abstracts, no complete article was available,or it was available only in another language, so thesearticles were no longer considered in the sample.
From the remaining articles, information concerningthe study design, the number of donors and recipi-ents, their gender, their relationship to one another,their geographical allocation, and their age at the timeof listing was documented. Many of the articles tookonly a few of these aspects into consideration. Foreach study, the 95% confidence interval was calcu-lated for both the donors and recipients. It was usedto indicate the reliability of this survey.
In a second step, the data from articles concerningthe same country were summarized (see Table 2).
Comparison of Registry Data and Review Data
The information found in published articles was com-pared to the data acquired from the registries withrespect to the total number of donors and recipientsand the relationship between the donors and recipi-ents for selected countries.
RESULTS
Registry and Center Data
The inquiry was sent to 38 national registries, 4 inter-national registries, 32 single transplant centers, 9transplant coordinators, and 6 transplant surgeonscontacted at the 2009 Organ Donation Congress (10thCongress of the International Society for Organ Dona-tion and Procurement and 16th Congress of the Euro-pean Transplant Coordinators Organization) from 36different countries. Twenty national registries replied,and 15 provided data. All international registriesanswered, but only 1 international registry had dataavailable. Three transplant centers responded andprovided data. Eight e-mails could not be delivered.Two individuals replied, but neither was in charge ofdata. One of the persons contacted at the congressreplied and provided data for a country. Overall, thisstudy presents data from 19 countries.
In the supporting material, we present the con-tacted registries and transplant centers and theresponse rate.
Sample of the Registry Data
The registry data include official data from 17 countriesand 3 single transplant centers. The total sample consistsof 8933 LDLT cases for donors and 9108 LDLT cases forrecipients. Some registries record only the recipients.
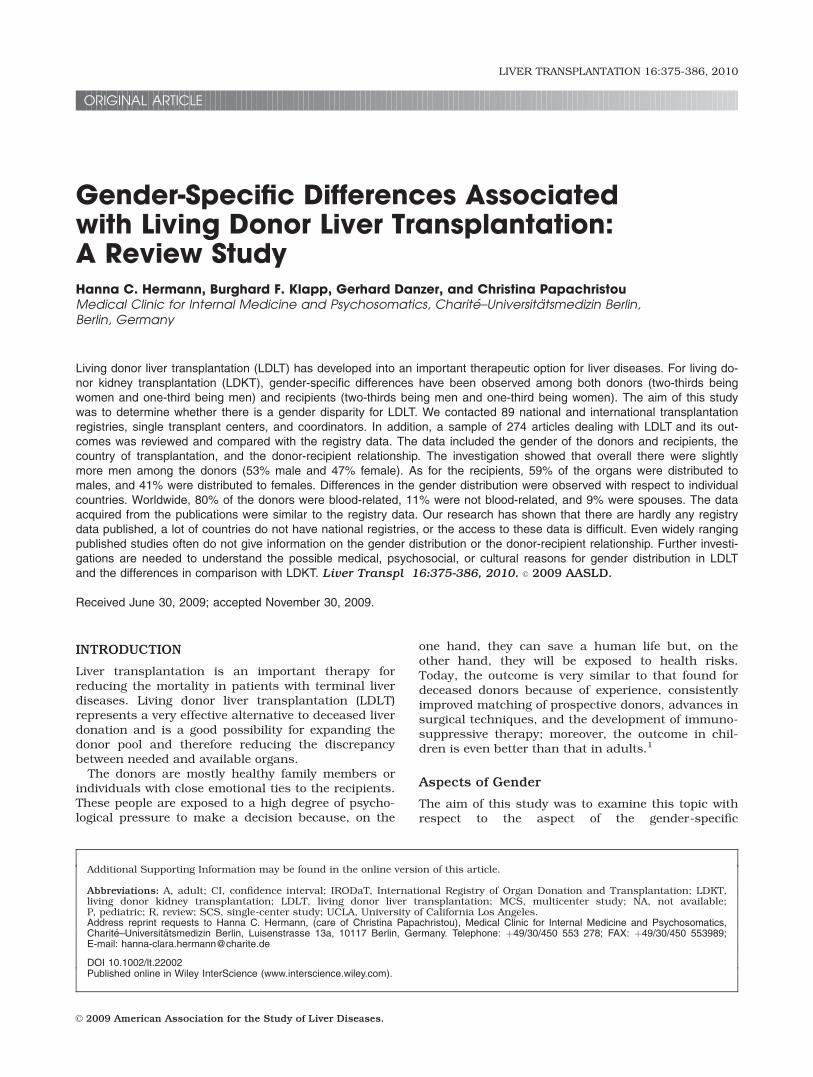
There was only a slight difference between the gen-ders among the donors: 4745 (53%) were male, and4211 (47%) were female (Fig. 1). Of the recipients,5407 (59%) were men, and 3701 were women (41%).
Relationship Between the Donors and Recipients
Most of the blood-related donors were parents (46%),who were followed by children (24%), siblings (18%),and other relatives (12%) such as uncles, aunts, cous-ins, and grandparents (Fig. 2).
Country and Continent Comparison with Respect
to the Donors
There were regional differences (Fig. 3). In 11 coun-tries or alternatively transplant centers, there were
378 HERMANN ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

TABLE
2.Data
from
theReviewedArticles
Source*
Loca
tion
Rec
ipients
(n)
95%
CIfor
Rec
ipients
†
Donors
(n)
95%
CIfor
Donors
†
Relationsh
ipBetwee
nth
e
Rec
ipients
andDonors
(n)
Stu
dy
Des
ign
Rec
ipient
Age
Male
Fem
ale
Male
Fem
ale
Biologically
Related
Not
Biologically
Related
Spouse
Jianget
al.5(2007)
Chen
gdu,China
23
30.698-0
.976
SCS
ALiu
etal.6(2009)
Chen
gdu,China
78
82
0.441-0
.597
91
14
55
SCS
NA
Liu
andFan7(2006)
HongKong,China
97
27
0.699-0
.851
50
74
0.316-0
.495
RA
Nget
al.8(2009)
HongKong,China
72
11
0.795-0
.940
SCS
AþP
Iwamoto
etal.9(2008)
Okoyama,Japan
76
61
0.472-0
.638
76
61
0.472-0
.638
SCS
AKawagishiet
al.10
(2009)
Sen
dai,Japan
29
0.046-0
.410
SCS
AþP
Ikeg
amiet
al.11(2008)
Fukuoka,Japan
15
27(24
adults)
0.221-0
.506
29
13
0.195-0
.480
39
12
SCS
AþP
Akamatsu
etal.12
(2007)
Tokyo,Japan
191
108
0.582-0
.693
179
120
0.613-0
.885
SCS
A
Moriokaet
al.13(2007)
Kyoto,Japan
167
168
0.444-0
.553
188
147
0.16-0
.478
SCS
AUed
aet
al.14(2006)
Japan
228
340
0.361-0
.443
255
313
0.408-0
.491
568
SCS
PYokoiet
al.15(2005)
Mie,Japan
13
14
0.529-0
.824
SCS
NA
Todoet
al.16(2004)
Hokkaido,Japan
246
70
0.729-0
.823
MCS
AEgawaet
al.17(2004)
Kyoto,Japan
201
339
0.331-0
.415
SCS
AþP
Yiet
al.18(2009)
Seo
ul,Korea
121
46
0.657-0
.792
120
47
0.650-0
.787
SCS
AHwanget
al.19(2005)
Seo
ul,Korea
(UlsanColleg
e)196
41
0.773-0
.873
MCS
A
Lee
etal.20(2004)
Seo
ul,Korea
(Sungkyunkwan
University)
97
44
0.606-0
.763
102
39
SCS
AþP
Chen
get
al.21(2009)
ChungGung,Taiw
an
110
35
0.689-0
.828
SCS
APolidoet
al.22(2007)
South
east
Asia
50
15
0.648;0.865
43
22
SCS
ALoet
al.23(2003)
Asia(K
orea,Japan,
andChina)
789
719
0.498-0
.549
685
823
0.507-0
.582
1197
15
137
MCS
AþP
Khalafet
al.24(2007)
Riyadh,SaudiAra
bia
(Hosp
italand
Res
earchCen
ter)
34
10
0.533;0.805
SCS
A
Abdullahet
al.25
(2005)
Riyadh,SaudiAra
bia
(NationalGuard
Hosp
ital)
17
30.621-0
.968
18
20.509-0
.689
19
1SCS
A
Yosryet
al.26(2009)
Giza,Egypt
69
50.875-0
.990
57
17
0.674-0
.866
SCS
AYosryet
al.27(2008)
Cairo,Egypt
35
30.835-1
.007
SCS
AEsm
atet
al.28(2005)
Cairo,Egypt
34
16
0.429-0
.48
SCS
AOzk
ard
esleret
al.29
(2008)
Izmir,Turk
ey69
44
0.521-0
.701
SCS
NA
Sev
mis
etal.30(2007)
Turk
ey27
19
0.683-0
.988
26
10
10
SCS
A
GENDER-SPECIFIC DIFFERENCES IN LDLT 379
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

TABLE
2.(Continued)
Source*
Loca
tion
Rec
ipients
(n)
95%
CIfor
Rec
ipients
†
Donors
(n)
95%
CIfor
Donors
†
Relationsh
ipBetwee
nth
e
Rec
ipients
andDonors
(n)
Stu
dy
Des
ign
Rec
ipient
Age
Male
Fem
ale
Male
Fem
ale
Biologically
Related
Not
Biologically
Related
Spouse
Honget
al.31(2009)
LosAngeles
,CA
42(14
adults)
58
(27
adults)
0.323-0
.517
SCS
AþP
Taioliet
al.32(2008)
Pittsburgh,PA
70
84
0.376-0
.533
72
82
0.389-0
.546
111
39
4SCS
ACampse
net
al.33
(2008)
Colora
do
46
0.096-0
.704
82
0.552-1
.048
SCS
A
Humaret
al.34(2008)
Minnes
ota
35
34
0.389-0
.625
29
40
0.304-0
.537
45
SCS
ALaiet
al.35(2009)
New
York
42
44
0.383-0
.594
SCS
AMek
eelet
al.36(2008)
Phoen
ix,AZ
32
10.133-1
.200
11
1SCS
AFisher
etal.37(2007)
United
States
45
13
0.647-0
.875
MCS
APompose
lliet
al.38
(2006)
Burlington,MA
55
30
0.536-0
.748
SCS
A
Verbes
eyet
al.39
(2005)
United
States
31
16
0.507-0
.791
29
18
0.351-0
.632
SCS
A
Shack
letonet
al.40
(2005)
UCLA
29
13
0.195-0
.480
16
20
6SCS
A
Olthofet
al.41(2005)
Philadelphia,PA
228
157
0.541-0
.642
205
180
0.464-0
.755
MCS
AThuluva
thet
al.42
(2004)
Baltim
ore,MD
384
330
0.500-0
.575
389
325
0.481-0
.583
MCS
A
DuBayet
al.43(2009)
Ontario,Canada
69
74
0.401-0
.564
108
22
13
SCS
AShahet
al.44(2007)
Toronto,Canada
95
58
0.539-0
.698
SCS
AAyala
etal.45(2009)
Madrid,Spain
13
80.411-0
.827
11
10
0.310-0
.737
SCS
ATsu
iet
al.46(2009)
Reg
ensb
urg,Germany
23
10
0.540-0
.854
22
11
0.506-0
.828
24
35
SCS
AErim
etal.47(2007)
Ess
en,Germany
53
47
0.428-0
.631
74
49
0.432-0
.73
102
13
8MSC
AWalter
etal.48(2005)
Berlin,Germany
15
31
0.472-0
.672
SCS
AKazemieret
al.49
(2009)
Rotterdam,th
eNetherlands
30
12
21
SCS
A
Gru
ttadauriaet
al.50
(2007)
Palerm
o,Italy
34
19
0.498-0
.769
26
27
0.032-0
.651
45
53
SCS
A
Ben
tabaket
al.51
(2005)
Algeria
44
0.157-0
.843
26
0.364-0
.793
SCS
A
Konstantinovet
al.52
(2004)
Russ
ia28
36
0.314-0
.567
SCS
AþP
Totalsu
m3991
3031
2895
2673
2539
205
245
*This
isalistingofth
eauth
ors
ofallth
ereview
edarticlesprovidingdata
on
gen
der,th
eco
untriesin
which
livingdonorlive
rtransp
lantation
wasperform
ed,and
the
relationsh
ipto
therecipients.
†The95%
CIwasca
lculatedforth
edistributionofmen
towomen
;it
wasuse
dto
indicate
thereliabilityofth
ises
timate.
380 HERMANN ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
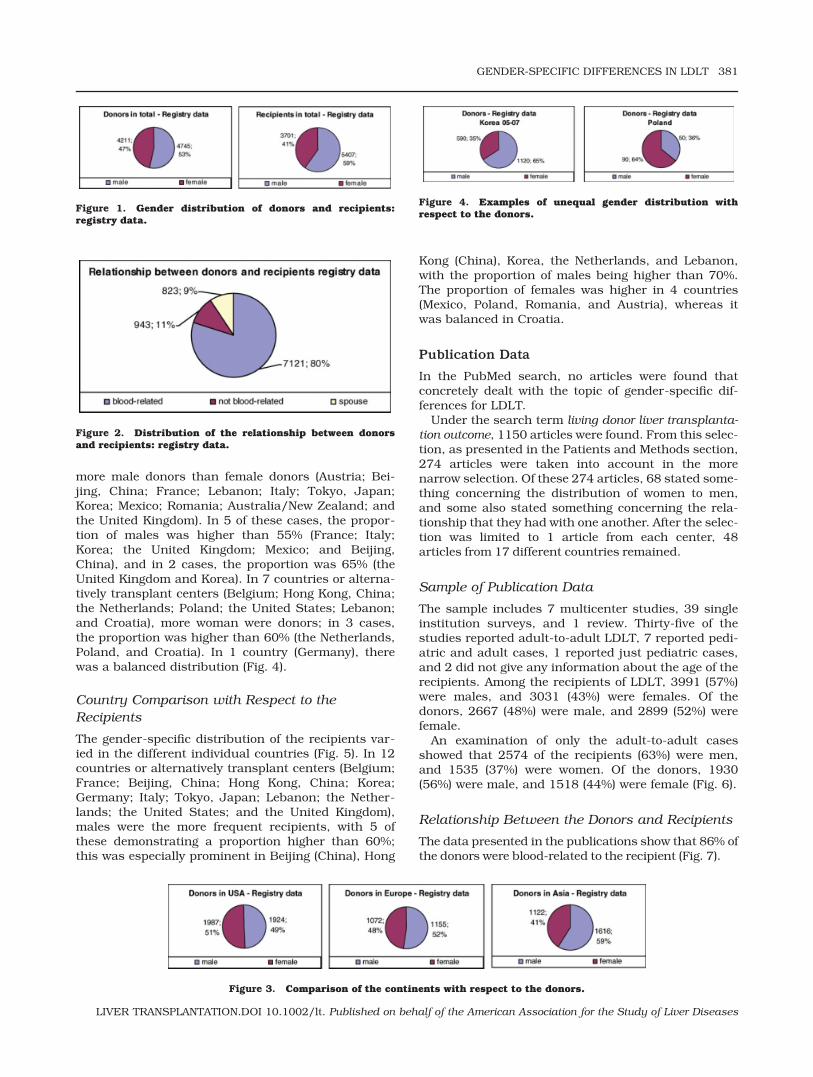
more male donors than female donors (Austria; Bei-jing, China; France; Lebanon; Italy; Tokyo, Japan;Korea; Mexico; Romania; Australia/New Zealand; andthe United Kingdom). In 5 of these cases, the propor-tion of males was higher than 55% (France; Italy;Korea; the United Kingdom; Mexico; and Beijing,China), and in 2 cases, the proportion was 65% (theUnited Kingdom and Korea). In 7 countries or alterna-tively transplant centers (Belgium; Hong Kong, China;the Netherlands; Poland; the United States; Lebanon;and Croatia), more woman were donors; in 3 cases,the proportion was higher than 60% (the Netherlands,Poland, and Croatia). In 1 country (Germany), therewas a balanced distribution (Fig. 4).
Country Comparison with Respect to the
Recipients
The gender-specific distribution of the recipients var-ied in the different individual countries (Fig. 5). In 12countries or alternatively transplant centers (Belgium;France; Beijing, China; Hong Kong, China; Korea;Germany; Italy; Tokyo, Japan; Lebanon; the Nether-lands; the United States; and the United Kingdom),males were the more frequent recipients, with 5 ofthese demonstrating a proportion higher than 60%;this was especially prominent in Beijing (China), Hong
Kong (China), Korea, the Netherlands, and Lebanon,with the proportion of males being higher than 70%.The proportion of females was higher in 4 countries(Mexico, Poland, Romania, and Austria), whereas itwas balanced in Croatia.
Publication Data
In the PubMed search, no articles were found thatconcretely dealt with the topic of gender-specific dif-ferences for LDLT.
Under the search term living donor liver transplanta-tion outcome, 1150 articles were found. From this selec-tion, as presented in the Patients and Methods section,274 articles were taken into account in the morenarrow selection. Of these 274 articles, 68 stated some-thing concerning the distribution of women to men,and some also stated something concerning the rela-tionship that they had with one another. After the selec-tion was limited to 1 article from each center, 48articles from 17 different countries remained.
Sample of Publication Data
The sample includes 7 multicenter studies, 39 singleinstitution surveys, and 1 review. Thirty-five of thestudies reported adult-to-adult LDLT, 7 reported pedi-atric and adult cases, 1 reported just pediatric cases,and 2 did not give any information about the age of therecipients. Among the recipients of LDLT, 3991 (57%)were males, and 3031 (43%) were females. Of thedonors, 2667 (48%) were male, and 2899 (52%) werefemale.
An examination of only the adult-to-adult casesshowed that 2574 of the recipients (63%) were men,and 1535 (37%) were women. Of the donors, 1930(56%) were male, and 1518 (44%) were female (Fig. 6).
Relationship Between the Donors and Recipients
The data presented in the publications show that 86% ofthe donors were blood-related to the recipient (Fig. 7).
Figure 1. Gender distribution of donors and recipients:registry data.
Figure 2. Distribution of the relationship between donorsand recipients: registry data.
Figure 3. Comparison of the continents with respect to the donors.
Figure 4. Examples of unequal gender distribution withrespect to the donors.
GENDER-SPECIFIC DIFFERENCES IN LDLT 381
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

Country Comparison: Publication Data
The data presented in the publications concerningindividual countries are summarized (Table 3).
Country Comparison with Respect to the Donors. Inthe sample, there were more male donors than femaledonors in 8 countries (Japan, Germany, Korea, SaudiArabia, Spain, Turkey, the United States, and Egypt).A proportion higher than 70% was observed in 3countries (Saudi Arabia, Korea, and Egypt). In 6countries (Algeria, Asia, Canada, China, Italy, andthe Netherlands), more women than men weredonors. In 2 countries, the proportion was higherthan 60% (Algeria and the Netherlands). In 4 coun-tries, no information was available concerning theserelationships.
Country Comparison with Respect to the Recipi-ents. The gender-specific distribution of the recipientswas different in the individual countries. In 15 coun-tries (Asia, Canada, Germany, Korea, Italy, Spain, Den-mark, Taiwan, Saudi Arabia, Singapore, Egypt, theNetherlands, China, Japan, and the United States),males were the more frequent recipients, with 7 ofthese demonstrating a proportion higher than 65%(China, Korea, Taiwan, Singapore, Saudi Arabia, Egypt,
and the Netherlands); this was especially prominent inKorea, China, Egypt, Saudi Arabia, and Singapore,with the proportion of males being higher than 75%.The proportion of females was higher in 1 country(Russia), whereas it was balanced in Algeria, and 1country did not provide information concerning theserelationships.
Comparison of the Registry Data and the
Publication Data
The results found in the publications are similar tothe registry data presented. These show that 9108LDLT cases have been carried out in the listed coun-tries until the present time. Among the 8925 donors,4728 (53%) were men, and 4197 (47%) were women.In the publications, 52% of the donors were male,and 48% were female. An examination of the recipi-ents shows that according to the registries, 59%were male, and 41% were female; in the publica-tions, 57% were male, and 43% were female. How-ever, when we considered the relationship, we foundthat there were larger differences between the regis-try data and the publication data. As for the registry
Figure 5. Comparison of the continents with respect to the recipients.
Figure 6. Gender distribution of donors and recipients:publication data
Figure 7. Distribution of the relationship between donorsand recipients: publication data.
TABLE 3. Summary and Comparison of the Literature
Data Concerning Individual Countries
Country
Recipient Donor
Male Female Male Female
China 192 41 132 150Japan 1126 1122 730 668Korea 414 131 120 47Taiwan 110 35South East Asia 50 15Asia (Korea,
Japan, andChina)
789 719 685 823
Saudi Arabia 17 3 52 12Egypt 104 8 91 33Turkey 96 63United States 936 775 763 661Canada 95 58 69 74Spain 13 8 11 10Germany 76 57 111 91Netherlands 3 0 1 2Italy 34 19 26 27Algeria 4 4 2 6Russia 28 36Final sum 3991 3031 2889 2667
382 HERMANN ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

data, there were fewer blood-related donors (80%)and more donors that were not blood-related (11%)or were spouses (9%) in comparison with the publi-cation data (Table 4).
DISCUSSION
In this review, the comparison of the gender-specificdistributions of LDLT showed that slightly more menthan women were donors and that more males thanfemales were recipients. Overall, the comparison ofdifferent countries and continents showed relativelysimilar results, but still there were regional differ-ences to be observed. In the United States andEurope, the gender distribution was more balanced.However, especially in Asia, many more recipients(70%) and donors (59%) were male than female.Also, there were larger differences in the propor-tional distribution found in countries in which a lownumber of transplants had taken place. Further-more, a predominant proportion of the individualswere blood-related.
Evaluation of the Gender-Specific Differences
Between the Donors
The research shows that LDLT does not, as initiallyassumed, show the same gender distribution asLDKT, for which twice as many women have donatedthan men, as already presented in the introduction.The reason for this difference and even the fact thatthere is a discrepancy between LDLT and LDKT areunfortunately not discussed in any of the articlesfound. Possible explanations for the more balancedrelationship could be that LDLT represents a largerand also much more risky action, and the man, in hisrole as the stronger and more protective individual,feels responsible for performing this action. Further-more, it could also be possible that many women areunable to donate their livers to adults because of thesmall liver volume, so the male members of the familyhave to donate their livers more frequently than in thecase of LDKT. The motivations for this, however,would have to be clarified through the use of an in-
depth patient interview. This could be an interestingtopic for further investigations.
However, the balanced gender distribution cannotbe seen in all of the countries. For instance, in HongKong, China (60%), and Poland (65%), womendonated predominantly, whereas men were seen to bethe primary donors in Korea and the United Kingdom(65%). Explanations for this would have to be relatedto cultural and social differences because these areaspects by which they differ from the other countries.At any rate, this could be investigated and exploredmore precisely in further studies.
Evaluation of the Gender-Specific Differences
Between the Recipients
For the recipients, there was a difference to beobserved. In 59% of the cases, males were the recipi-ents. When the various individual countries were con-sidered, however, the differences varied. In the Asiaticcountries, for example, a large percentage of the recip-ients were males (70%). In contrast, the gender distri-bution was quite balanced in Europe and the UnitedStates. However, no reason for this has been cited inthe articles. It is likely that men generally suffer moreoften from liver illnesses and must undergo livertransplantation more frequently. Also in favor of thisargument is the fact that men, especially in Asia, suf-fer from liver carcinomas 3 to 4 times more often thanwomen; the most frequent reasons for this are hepati-tis C and B infections and alcoholic cirrhosis of theliver. In China, the prevalence of demonstrating a hep-atitis B antigen is 10% to 20%; this finding could alsobe responsible for the unequal distribution betweenmen and women.53 In addition, the data from theOrgan Procurement and Transplantation Networkdata bank also speak in favor of this illness beingmore frequent in men. According to this, almost two-thirds of the patients who are waiting for liver trans-plantation in the United States are male.54 Anotherreason for this distribution might be related to thetraditional role allocation. The man is the head of thefamily and is responsible for earning the primaryincome, and so his health highly correlates with thewelfare and living standard of the entire family.
Evaluation of the Relationship of the Donors
and Recipients
Most donors are blood-related to the recipients. Thiswas already assumed because these are the individu-als who have close emotional ties to the recipientsand the matching of the genetic material is often suc-cessful. The second most frequent donors are donorsnot related by blood, such as friends, and familymembers not related by blood. Another very importantgroup of donors is spouses, who have a strong inter-est in the health of their partners simply because oftheir strong emotional and social relationships. Hereregional differences can also be observed. The second
TABLE 4. Comparison of the Registry Data and
Publication Data
Registry
Data [n (%)]
Publication
Data
[n (%)]
Donors Male 3571 (50%) 2836 (52%)Female 3569 (50%) 2654 (48%)
Recipients Male 3995 (56%) 4008 (57%)Female 3140 (44%) 3050 (43%)
Relationship Blood-related
5735 (78%) 2255 (86%)
Not blood-related
824 (12%) 138 (5%)
Spouse 659 (10%) 235 (9%)
GENDER-SPECIFIC DIFFERENCES IN LDLT 383
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

largest group was spouses in Europe and Asia anddonors not related by blood in the United States.
Evaluation of the Comparison of the Registry
Data and Publication Data
The review shows that data presented in the publica-tions and reviews can to a certain extent be represen-tative of the actual data from the registries.
It is important to know if publications that do give acertain view of LDLT performed worldwide reflect thereal situation. It is not possible for everyone to haveaccess to all the registry data. Most of the informationis primarily taken from publications because there isimmediate access and they help to enrich one’sknowledge. They also help with interpreting data, andoften explanations are given. In addition, publicationsare the only way of acquiring this sort of data forcountries that do not have a national registry or withwhich there is a lack of communication.
However, one cannot be sure that there is not a spe-cific selection of patients or that other patients areexcluded. Publication data do not give a transparentand clear look at this issue because there is alwaysbias, such as the selection of patients who volun-teered or case series that might have been small andnot representative of a given country’s distribution ofLDLT. This research shows that it is very difficult toacquire information on this topic in publications.Gender aspects and the relationship between donorsand recipients were generally not taken into consider-ation, and most of the publications did not even dis-tinguish between male and female patients.
Reflection on the Experience of Contacting
Registries and Transplant Centers
There are international registries that provide connec-tions to national transplant registries or transplantcoordinators, such as IRODaT and the EuropeanTransplantation Coordinators Organization. Theseregistries give an overview of the national registriesthat might be contacted and provide data on trans-plantation worldwide.
The response rate of contacted national registrieswas 45%, the rate for international registries was100%, and the response rate for single centers wasonly 10%. The low response rate could lead to a selec-tion bias. Asiatic countries, such as China, Taiwan,Singapore, Saudi Arabia, and Iran, especially did notreply. A further difficulty in the data selection was thata few registries charged for the information, and thusthe information was not obtained. Communication withthe European countries, the United States, and Aus-tralia was very positive. Most of these countries are rep-resented in the sample.
Overall, it can be said that contacting nationalregistries and institutions is a good way of obtainingactual data, but it is very difficult to acquire datafrom some registries, and even international registriessuch as IRODaT have difficulties with presenting data
on performed LDLT procedures for specific countriesfor each year.
Limitations and Weaknesses of This
Investigation
A difficulty of this investigation was that the only pub-licly accessible data bank to be found was in theUnited States. Other data banks and registries had tobe contacted, and there was a 55% nonreply rate.Thus, the data in this review represent most coun-tries, but not all. In particular, the Asiatic countriesare not well represented.
As for the data from the literature review, it can besaid that many authors have reported on the numberof LDLT procedures performed but have not includedinformation concerning the gender. For this reason,many articles could not be included in the evaluation,and thus bias is possible. A further problem could bethat the 7 multicenter studies might have used thesame data, so the patients and donors could havebeen occasionally counted and listed twice. However,this could not be detected in these reports and, conse-quently, could not be corrected.
In conclusion, it can be said that information con-cerning gender is frequently lacking in publicationsand even in reports from national registries. It is im-portant to pay more attention to details and toimprove documentation.
Further publications on gender aspects or dispar-ities regarding LDLT would be helpful in order tounderstand the different gender distributions of LDLTand LDKT and to look for possible answers that couldexplain the specific country differences. In addition, itwould be useful to delve more deeply into the psycho-logical and sociocultural aspects of the subjectbecause this is important for the adequate care ofboth the donors and recipients, for improvements inoutcome, and for further possible developments ofthis therapy.
Finally, the development of a worldwide, interlinkeddata bank that also includes information on the gen-der and relationship of donors and recipients wouldfacilitate access to information regarding donationrates and individual characteristics of donors andrecipients in individual countries.
ACKNOWLEDGMENTSThe authors thank the Austrian Health Institute, theAustralia and New Zealand Organ Donation Registry,Eurotransplant, the People’s Liberation Army GeneralHospital of China, the French Agency of Biomedicine,Queen Mary Hospital of Hong Kong, the NationalTransplant Center of Italy, the University of TokyoGraduate School of Medicine, the National Organiza-tion for Organ and Tissue Donation and Transplanta-tion of Lebanon, the National Transplant ResourceCenter of Malaysia, the National Transplant Center ofMexico, the Dutch Transplant Foundation, Poltrans-plant, the National Transplant Agency of Romania,
384 HERMANN ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

NHS Blood and Transplant (UK), the United Networkfor Organ Sharing, and the Seoul National UniversityCollege of Medicine for providing data from theirregistries.
REFERENCES
1. Tamura S, Sugawara Y, Makuuchi M. Impact of recipientage on the long-term outcome of living donor liver trans-plantation for post-Kasai biliary atresia. Am J Trans-plant 2007;7:728.
2. Achille M, Soos J, Fortin M-C, Paquet M, Hebert M-J.Differences in psychosocial profiles between men andwomen living kidney donors. Clin Transplant 2007;21:314-320.
3. Biller-Adorno N. Gender imbalance in living organ dona-tion. Med Health Care Philos 2002;5:199-204.
4. Thiel GT, Nolte C, Tsinalis D. Gender imbalance in livingkidney donation in Switzerland. Transplant Proc 2005;37:592-594.
5. Jiang XZ, Yan LN, Li B, Wen TF, Zeng Y, Wang WT, et al.Safety of donor in adult-to-adult living donor liver trans-plantation using right lobe graft. Transplant Proc 2007;39:150-152.
6. Liu B, Yan LN, Li J, Li B, Zeng Y, Wang WT, et al. Usingthe Clavien grading system to classify the complicationsof right hepatectomy in living donors. Transplant Proc2009;41:1703-1706.
7. Liu CL, Fan ST. Adult-to-adult live-donor liver transplan-tation: the current status. J Hepatobiliary Pancreat Surg2006;13:110-116.
8. Ng KK, Lo CM, Chan SC, Chok KS, Cheung TT, Fan ST.Liver transplantation for hepatocellular carcinoma: theHong Kong experience. J Hepatobiliary Pancreat Surg;doi:10.1007/s00534-009-0165-8.
9. Iwamoto T, Yagi T, Umeda Y, Sato D, Matsukawa H, Mat-suda H, et al. The impact of donor age on the outcome ofadult living donor liver transplantation. Transplantation2008;85:1240-1245.
10. Kawagishi N, Takeda I, Miyagi S, Satoh K, Akamatsu Y,Sekiguchi S, Satomi S. Long-term outcome of ABO-in-compatible living-donor liver transplantation: a single-center experience. J Hepatobiliary Pancreat Surg 2009;16:468-472.
11. Ikegami T, Taketomi A, Soejima Y, Yoshizumi T, SanefujiK, Kayashima H, et al. Living donor liver transplantationfor acute liver failure: a 10-year experience in a singlecenter. J Am Coll Surg 2008;206:412-418.
12. Akamatsu N, Sugawara Y, Tamura S, Kaneko J, MatsuiY, Togashi J, Makuuchi M. Impact of live donor age(�50) on liver transplantation. Transplant Proc 2007;39:3189-3193.
13. Morioka D, Egawa H, Kasahara M, Ito T, Haga H, TakadaY, et al. Outcomes of adult-to-adult living donor livertransplantation. A single institution’s experience with335 consecutive cases. Ann Surg 2007;245:315-325.
14. Ueda M, Oike F, Ogura Y, Uryuhara K, Fujimoto Y, Kasa-hara M, et al. Long-term outcomes of 600 living donorliver transplants for pediatric patients at a single center.Liver Transpl 2006;12:1326-1336.
15. Yokoi H, Isaji S, Yamagiwa K, Tabata M, Sakurai H, UsuiM, et al. Donor outcome and liver regeneration afterright-lobe graft donation. Transpl Int 2005;18:915-922.
16. Todo S, Furukawa H, for the Japanese Study Group onOrgan Transplantation. Living donor liver transplanta-tion for adult patients with hepatocellular carcinoma: ex-perience in Japan. Ann Surg 2004;240:451-453.
17. Egawa H, Oike F, Buhler L, Shapiro AM, Minamiguchi S,Haga H, et al. Impact of recipient age on outcome of
ABO-incompatible living-donor liver transplantation.Transplantation 2004;77:403-411.
18. Yi NJ, Suh KS, Lee HW, Shin WY, Kim J, Kim W, et al.Improved outcome of adult recipients with a high Modelfor End-Stage Liver Disease score and a small-for-sizegraft. Liver Transpl 2009;15:496-503.
19. Hwang S, Lee SG, Joh JW, Suh KS, Kim DG. Liver trans-plantation for adult patients with hepatocellular carci-noma in Korea: comparison between cadaveric donorand living donor liver transplantations. Liver Transpl2005;11:1265-1272.
20. Lee DS, Gil WH, Lee HH, Lee KW, Lee SK, Kim SJ, et al.Factors affecting graft survival after living donor livertransplantation. Transplant Proc 2004;36:2255-2256.
21. Cheng YF, Huang TL, Chen TY, Tsang LL, OuHY, YuCY, et al.Liver graft regeneration in right lobe adult living donor livertransplantation. AmJTransplant 2009;9:1382-1388.
22. Polido WT Jr, Lee KH, Tay KH, Wong SY, Singh R, LeongSO, Tan KC. Adult living donor liver transplantation inSingapore: the Asian Centre for Liver Diseases andTransplantation experience. Ann Acad Med Singapore2007;36:623-630.
23. Lo CM. Complications and long-term outcome of livingliver donors: a survey of 1,508 cases in five Asian cen-ters. Transplantation 2003;75:12-15.
24. Khalaf H, Al-Sofayan M, El-Sheikh Y, Al-Bahili H, Al-Sagheir M, Al-Sebayel M. Donor outcome after living liverdonation: a single-center experience. Transplant Proc2007;39:829-834.
25. Abdullah K, Abdeldayem H, Hali WO, Sakran A, YassenK, Abdulkareem A. Twenty cases of adult-to-adult living-related liver transplantation: single-center experience inSaudi Arabia. Transplant Proc 2005;37:3144-3146.
26. Yosry A, Abdel-Rahman M, Esmat G, El-Serafy M, OmarA, Doss W, et al. Recurrence of hepatitis C virus (geno-type 4) infection after living-donor liver transplantin Egyptian patients. Exp Clin Transplant 2009;7:157-163.
27. Yosry A, Esmat G, El-Serafy M, Omar A, Doss W, SaidM, et al. Outcome of living donor liver transplantation forEgyptian patients with hepatitis C (genotype 4)-relatedcirrhosis. Transplant Proc 2008;40:1481-1484.
28. Esmat G, Yosry A, El-Serafi M, Omar A, Doss W, HosnyA, et al. Donor outcomes in right lobe adult living donorliver transplantation: single-center experience in Egypt.Transplant Proc 2005;37:3147-3150.
29. Ozkardesler S, Ozzeybek D, Alaygut E, Unek T, Akan M,Astarcioglu H, et al. Anesthesia-related complications inliving liver donors: the experience from one center andthe reporting of one death. Am J Transplant 2008;8:2106-2110.
30. Sevmis S, Diken T, Boyvat F, Torgay A, Habera M. Righthepatic lobe donation: impact on donor quality of life.Transplant Proc 2007;39:826-828.
31. Hong JC, Yersiz H, Farmer DG, Duffy JP, Ghobrial RM,Nonthasoot B, et al. Longterm outcomes for whole andsegmental liver grafts in adult and pediatric liver trans-plant recipients: a 10-year comparative analysis of 2,988cases. J Am Coll Surg 2009;208:682-689.
32. Taioli E, Marsh W. Epidemiological study of survival af-ter liver transplant from a living donor. Transpl Int 2008;21:942-947.
33. Campsen J, Blei AT, Emond JC, Everhart JE, Freise CE,Lok AS, et al., for the Adult-to-Adult Living Donor LiverTransplantation Cohort Study Group. Outcomes of livingdonor liver transplantation for acute liver failure: theadult-to-adult living donor liver transplantation cohortstudy. Liver Transpl 2008;14:1273-1280.
34. Humar A, Beissel J, Crotteau S, Kandaswamy R, Lake J,Payne W. Whole liver versus split liver versus living
GENDER-SPECIFIC DIFFERENCES IN LDLT 385
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases

donor in the adult recipient: an analysis of outcomes bygraft type. Transplantation 2008;85:1420-1424.
35. Lai JC, Pichardo EM, Emond JC, Brown RS Jr. Resourceutilization of living donor versus deceased donor livertransplantation is similar at an experienced transplantcenter. Am J Transplant 2009;9:586-591.
36. Mekeel KL, Moss AA, Reddy KS, Douglas DD, VargasHE, Carey EJ, et al. Living donor liver transplantationin polycystic liver disease. Liver Transpl 2008;14:680-683.
37. Fisher RA, Kulik LM, Freise CE, Lok AS, Shearon TH,Brown RS Jr, et al. Hepatocellular carcinoma recurrenceand death following living and deceased donor livertransplantation. Am J Transplant 2007;7:1601-1608.
38. Pomposelli JJ, Verbesey J, Simpson MA, Lewis WD, Gor-don FD, Khettry U, et al. Improved survival after live do-nor adult liver transplantation (LDALT) using right lobegrafts: program experience and lessons learned. Am JTransplant 2006;6:589-598.
39. Verbesey JE, Simpson MA, Pomposelli JJ, Richman E,Bracken AM, Garrigan K, et al. Living donor adult livertransplantation: a longitudinal study of the donor’s qual-ity of life. Am J Transplant 2005;5:2770-2777.
40. Shackleton CR, Vierling JM, Nissen N, Martin P, PoordadF, Tran T, Colquhoun SD. Morbidity in live liver donors:standards-based adverse event reporting further refined.Arch Surg 2005;140:888-895.
41. Olthoff KM, Merion RM, Ghobrial RM. Outcomes of 385adult-to-adult living donor liver transplant recipients: areport from the A2ALL Consortium. Ann Surg 2005;242:314-323.
42. Thuluvath PJ, Yoo HY. Graft and patient survival afteradult live donor liver transplantation compared to amatched cohort who received a deceased donor trans-plantation. Liver Transpl 2004;10:1263-1268.
43. DuBay DA, Holtzman S, Adcock L, Abbey S, GreenwoodS, Macleod C, et al. Adult right-lobe living liver donors:quality of life, attitudes and predictors of donor out-comes. Am J Transplant 2009;9:1169-1178.
44. Shah SA, Levy GA, Greig PD, Smith R, McGilvray ID,Lilly LB, et al. Reduced mortality with right-lobe livingdonor compared to deceased-donor liver transplantation
when analyzed from the time of listing. Am J Transplant2007;7:998-1002.
45. Ayala R, Grande S, Albizua E, Crooke A, Meneu JC, Mor-eno A, et al. Long-term follow-up of donor chimerismand tolerance after human liver transplantation. LiverTranspl 2009;15:581-591.
46. Tsui TY, Scherer MN, Schnitzbauer AA, Schlitt HJ, ObedA. Adult living donor liver transplantation: body massindex and MELD score of recipients are independent riskfactors for hospital mortality. Langenbecks Arch Surg2009;394:235-241.
47. Erim Y, Beckmann M, Kroencke S, Valentin-Gamazo C,Malago M, Broering D, et al. Psychological strain inurgent indications for living donor liver transplantation.Liver Transpl 2007;13:886-895.
48. Walter M, Pascher A, Papachristou C, Danzer G, Lan-grehr M, Frommer J, et al. Psychological and somaticaspects of living liver donors: preoperative assessmentand postoperative course [in German]. Dtsch MedWochenschr 2005;130:1749-1755.
49. Kazemier G, Metselaar HJ, de Man RA, Tran TC, Groen-land TH, Tilanus HW. Liver transplantation with a livingdonor: the first 3 cases in Rotterdam [in Dutch]. NedTijdschr Geneeskd 2008;152:817-821.
50. Gruttadauria S, Marsh JW, Cintorino D, Biondo D, LucaA, Arcadipane A, et al. Adult to adult living-related livertransplant: report on an initial experience in Italy. DigLiver Dis 2007;39:342-350.
51. Bentabak K, Graba A, Boudjema K, Griene B, Debzi N,Bekkouche N, et al. Adult-to-adult living related livertransplantation: preliminary results of the HepaticTransplantation Group in Algiers. Transplant Proc 2005;37:2873-2874.
52. Konstantinov BA, Got’e SV, Tsyrul’nikova OM, Filin AV,Kim EF. Transplantation of the liver right lobe from arelated donor [in Russian]. Khirurgiia 2004;8:7-12.
53. El-Serag HB. Hepatocellular carcinoma: an epidemiologicview. J Clin Gastroenterol 2002;35:72-78.
54. Organ Procurement and Transplantation Network.http://www.optn.org/latestData/rptData.asp. AccessedMarch 2008.
386 HERMANN ET AL.
LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases