future of academic general pediatrics—areas of opportunity
TRANSCRIPT

Future of Academic General Pediatrics—Areas of OpportunityJames M. Perrin, MD; Thomas G. Dewitt, MD
From the MGH Center for Child and Adolescent Health Policy, MassGeneral Hospital for Children, Harvard Medical School, Boston Mass(Dr Perrin) and the Division of General and Community Pediatrics, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine,Cincinnati, Ohio (Dr Dewitt)The authors have no conflicts of interest to disclose.Address correspondence to James M. Perrin, MD, 50 Staniford St #901, Boston, Massachusetts 02114 (e-mail: [email protected]).
Received for publication March 29, 2011; acceptedMarch 29, 2011.ACADEMIC PEDIATRICS 2011;11:181–188
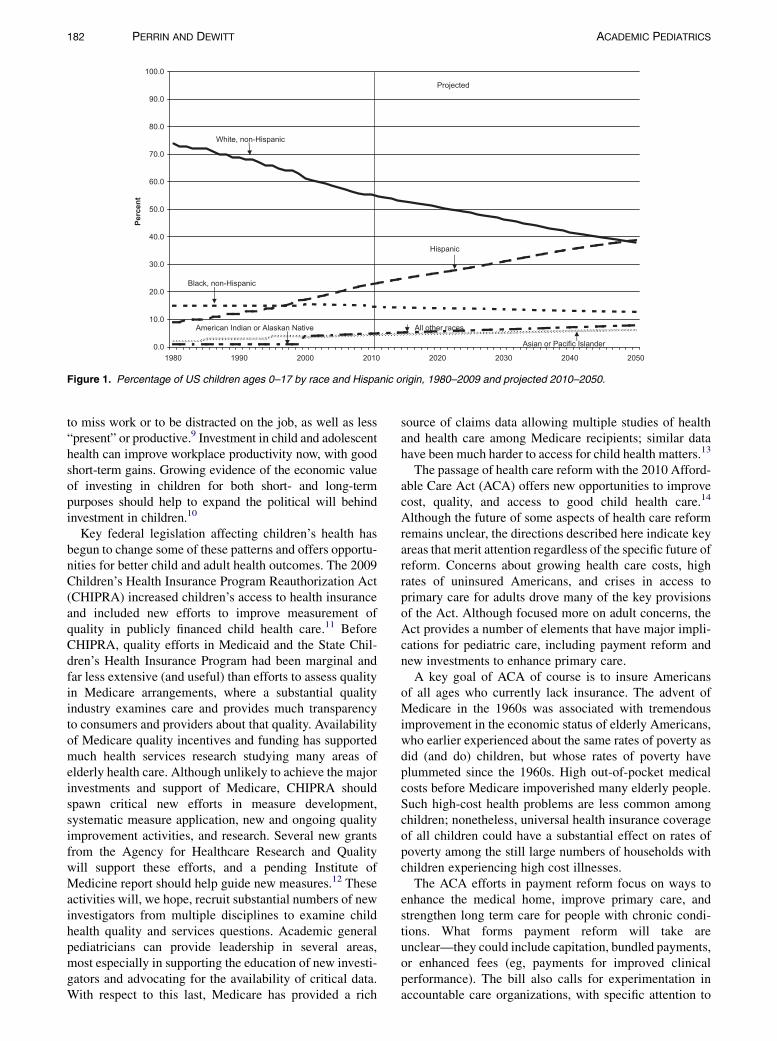
THE DYNAMIC CHANGE in the United States occurringin the diversity of pediatric populations and in healthcare will dramatically influence many dimensions ofcare, teaching, research, and advocacy in academic generalpediatrics. By 2025, the nonwhite and Hispanic pediatricpopulation will increase to 50% (Figure 1),1,2 leading thedemographic change that is projected to occur in thewhole United States population by 2050. This shift inpopulation demographics is occurring concurrently withsignificant changes in both health care funding and thesophistication and complexity of systems caring forchildren, accentuated by an explosion of informationtechnology. These latter trends have resulted in anincreasing number of children and youth with healthcoverage, complex chronic illness, and social media–informed parents. It is in this changing environment thatacademic pediatric generalists have an opportunity tostudy and actively engage in the change through appliedresearch and training with a great potential of positivelyinfluencing its course, and ultimately the health of children.
Starmer and colleagues recently identified 8 megatrendsin pediatrics that underscore the statements above.3 Thosethat most closely align include alterations in health caredelivery system(s), changing demographic and clinical char-acteristics of children and families, burgeoning health infor-mation technology, ongoing medical advances, and growthof consumer-driven health care. Globalism, a trend thatwill increasingly dominate child health, is also mentioned,but it is beyond the scope of this article. Alterations in healthcare delivery system(s), particularly financing and structure,have engendered systems thinking and approaches. Thechanging demographic and clinical characteristics of chil-dren and families have led to greater diversity and potentialfor discrimination and disparity. The burgeoning healthinformation technology, coupled with ongoing medicaladvances and growth of consumer-driven health care, has re-sulted in a more complex chronically ill population withbetter-informed parents and providers. Disasters, such asthose recently occurring in Haiti and Japan, were also listedas a megatrend in the context of environment, infection, andman-made. In the United States, the increasing prevalence,some might say national child health disasters—injury,asthma, obesity, and mental health conditions, especiallyattention-deficit/hyperactivity disorder and autism—clearlyhave environmental and man-made dimensions.
ACADEMIC PEDIATRICSCopyright ª 2011 by Academic Pediatric Association 181
To understand the opportunity that these megatrends andtheir consequences present, it is important to appreciate thepublic policy context in which the above changes arehappening. With that understanding, one can then examinethe dimensions of advances in pediatric care with regard tonew systems of care incorporating evidence-based medi-cine, expanded concepts of medical home, and improvingchild health in the context of community. Training thepediatricians practicing in this new environment, a majoractivity in academic general pediatrics, will require theapplication and assessment of newer, more efficient andeffective approaches to that training, greatly affected byinformation technology. As with any change, researchshould not only assess the impact of that change, but alsoinform it using methodologies suited to the unique chal-lenges of studying child health, especially with regard totrajectories over time. Finally, throughout all the change,the need for effective advocacy for the vulnerable popula-tions that academic pediatric generalists serve is para-mount. This article provides a perspective on potentialareas of opportunity in academic general pediatrics in thedomains of care, education, research, and advocacy partic-ularly as it relates to pediatric care in the United States.
PUBLIC POLICY
Children and adolescents typically receive only a rela-tively small proportion of public financing, especially forhealth. As an example, only about 9%–10% of health careexpenditures are for children and youth under 18 yearsold.4,5 Although recent years have not brought muchchange in investment levels, increasing evidence hassupported the value of early investment,6 including 2 keynational reports, Neurons to Neighborhoods7 and Children’sHealth—The Nation’s Wealth.8 The case for long-terminvestment paying off seems increasingly well supported.Nonetheless, most funders (public and private) have limitedinterest in (or vision for) long-term outcomes. It is importantto recognize—and share with America’s employers—thenotion that children’s health (and ill health) has substantialimpact on the workforce performance and participation oftheir parents. Parents who worry about the after-schoolsituation for their child with attention-deficit/hyperactivitydisorder, their adolescent at risk of substance use, or thechild whose asthma is not well controlled are more likely
Volume 11, Number 3May–June 2011
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
1980 1990 2000 2010 2020 2030 2040 2050
Percen
t
Projected
White, non-Hispanic
Hispanic
Black, non-Hispanic
Asian or Pacific Islander
American Indian or Alaskan Native All other races
Figure 1. Percentage of US children ages 0–17 by race and Hispanic origin, 1980–2009 and projected 2010–2050.
182 PERRIN AND DEWITT ACADEMIC PEDIATRICS
to miss work or to be distracted on the job, as well as less“present” or productive.9 Investment in child and adolescenthealth can improve workplace productivity now, with goodshort-term gains. Growing evidence of the economic valueof investing in children for both short- and long-termpurposes should help to expand the political will behindinvestment in children.10
Key federal legislation affecting children’s health hasbegun to change some of these patterns and offers opportu-nities for better child and adult health outcomes. The 2009Children’s Health Insurance Program Reauthorization Act(CHIPRA) increased children’s access to health insuranceand included new efforts to improve measurement ofquality in publicly financed child health care.11 BeforeCHIPRA, quality efforts in Medicaid and the State Chil-dren’s Health Insurance Program had been marginal andfar less extensive (and useful) than efforts to assess qualityin Medicare arrangements, where a substantial qualityindustry examines care and provides much transparencyto consumers and providers about that quality. Availabilityof Medicare quality incentives and funding has supportedmuch health services research studying many areas ofelderly health care. Although unlikely to achieve the majorinvestments and support of Medicare, CHIPRA shouldspawn critical new efforts in measure development,systematic measure application, new and ongoing qualityimprovement activities, and research. Several new grantsfrom the Agency for Healthcare Research and Qualitywill support these efforts, and a pending Institute ofMedicine report should help guide new measures.12 Theseactivities will, we hope, recruit substantial numbers of newinvestigators from multiple disciplines to examine childhealth quality and services questions. Academic generalpediatricians can provide leadership in several areas,most especially in supporting the education of new investi-gators and advocating for the availability of critical data.With respect to this last, Medicare has provided a rich
source of claims data allowing multiple studies of healthand health care among Medicare recipients; similar datahave been much harder to access for child health matters.13
The passage of health care reform with the 2010 Afford-able Care Act (ACA) offers new opportunities to improvecost, quality, and access to good child health care.14
Although the future of some aspects of health care reformremains unclear, the directions described here indicate keyareas that merit attention regardless of the specific future ofreform. Concerns about growing health care costs, highrates of uninsured Americans, and crises in access toprimary care for adults drove many of the key provisionsof the Act. Although focused more on adult concerns, theAct provides a number of elements that have major impli-cations for pediatric care, including payment reform andnew investments to enhance primary care.A key goal of ACA of course is to insure Americans
of all ages who currently lack insurance. The advent ofMedicare in the 1960s was associated with tremendousimprovement in the economic status of elderly Americans,who earlier experienced about the same rates of poverty asdid (and do) children, but whose rates of poverty haveplummeted since the 1960s. High out-of-pocket medicalcosts before Medicare impoverished many elderly people.Such high-cost health problems are less common amongchildren; nonetheless, universal health insurance coverageof all children could have a substantial effect on rates ofpoverty among the still large numbers of households withchildren experiencing high cost illnesses.The ACA efforts in payment reform focus on ways to
enhance the medical home, improve primary care, andstrengthen long term care for people with chronic condi-tions. What forms payment reform will take areunclear—they could include capitation, bundled payments,or enhanced fees (eg, payments for improved clinicalperformance). The bill also calls for experimentation inaccountable care organizations, with specific attention to

Table 1. Trends in Patient Care
� Systems-based and team care� Use of information technology and social media� Application of quality improvement in diverse populations andindividual care
� Inclusion of public health and nonmedical community resourcesin improving child health
� Interface between inpatient and outpatient care
ACADEMIC PEDIATRICS FUTURE OF ACADEMIC GENERAL PEDIATRICS 183
work on pediatric accountable care organizations. Recentcommentaries have noted that any payment methods creategood and bad incentives—no perfect system has beendesigned.15 How these different payment strategies impactpediatric health services merits careful assessment, hope-fully with experiments with very careful analyses of theirresults. The ACA also includes support for medical homepilots (using Medicaid and other financing), as well asincreased community supports (eg, the development ofcommunity programs to assist transformation of primarycare practices into medical homes); and expanded supportfor community health centers.
Medicaid, amain sourceof financing for child health care,will change with the implementation of the ACA, as expan-sions of Medicaid will now cover many currently uninsuredadults.16 The traditional Medicaid populations have beenpregnant women and children (and adolescents), peoplewith severe disability, and elderly populations. The expan-sion to working age adults will have a major effect on thedemographics of the Medicaid population (and potentiallyin its sources of political support), as well as in coveredbenefits. Proposed benefits for the newly insured adult pop-ulation are less generous than current childhood benefits—and especially do not include long-term care benefits.17
These more limited benefits could become the standard forMedicaid in general, resulting in less good coverage forchildren, especially those with chronic health conditions.
Much research has documented both the increasingnumbers of children and adolescents with chronic healthconditions and the impact of chronic conditions on childand family life.18 The ACA mentions chronic diseasemany times—mainly reflecting again adult disease andelderly populations. Yet, many of the incentives underconsideration could very much enhance the use of theFamily-Centered Medical Home for children, especiallythose with chronic conditions.19 Much evidence supportsthe notion of team practice and other practice enhancements(care coordination, patient registries, parents as partners incare) as key to providing high-quality continuing care forchildren with chronic conditions and their families.20,21
Whether the new incentives (payment reform, support forpractice transformation, community care coordinationresources) will be sufficient to transform primary careremains unclear, and there will remain problems ofunderinsurance among many children, including thosewith chronic conditions.
PATIENT CARE
In the area of patient care there are at least 5 domains thatprovide opportunity (Table 1). These include systems-based and team care, use of information technology andsocial media, application of quality improvement in diversepopulations and individual care, inclusion of public healthand nonmedical community resources in improving childhealth, and the interface between inpatient and outpatientcare. Each has great potential for improving child health,but also has inherent challenges that will require carefulstudy, assessment, and refinement.
As noted above there is a movement toward systems-based, not individual-based, practices that incorporateteam carewith increasing use of nurses, other nonphysicianpersonnel, and even community resources. This is due notonly to financial incentives, but also to an appreciation thatwell designed systems of care can provide routine care,both preventive and acute, efficiently and effectively withhigh quality and consistency. A team and systems approachmay also facilitate implementation of the key elements ofthe medical home. These include increased interactionwith an array of community resources that enhance childhealth and attention paid to critical aspects of patientdiversity, eg, cultural and economic factors, that maylead to disparate care. The challenges in these systemsare the interaction and coordination among the elementsin the team and community, and, more importantly, theinteraction of the patient and family with the team. Thedoctor-patient/family dyad relationship is a critical factorin adherence and there is a need to explore approaches toenhancing that relationship in a systems and team setting.22
Additionally, effective mechanisms need to be developedfor detecting and addressing individual patient variationsthat require more than routine care if a systems/guidelineapproach is heavily relied upon.The explosion of information technology and social
media is another dimension of the challenges of communi-cation and interpersonal skills in the practice of generalpediatrics. The electronic health record provides readyaccess to patient information and practice guidance, butmay also interfere with the patient-physician interaction.Ultimately aspects of the electronic health record may beshared real-time with patients and families. This interac-tion may be complicated by parents being more informedthrough internet websites and increasingly using socialmedia to communicate with other parents, resulting attimes in inaccurate information. There are already manyexamples of the use of social media and electronic portalsthat effect interactions between patients, families andphysicians, and that use is expanding in the form ofmHealth.23 It is this complex interplay of electronic healthrecords, extensive internet access and social networking byparents and patients, and patient-physician interactionsthat will require thoughtful development and assessment.The role of active ongoing quality improvement (QI) as
an integral component of pediatric practice can be a keyfactor in reducing significant disparity of care. Standard-ized, evidence-based approaches to routine care havebeen shown repeatedly to lead to better outcomes in popu-lations of patients. Given the increasing diversity in thepediatric population, it is critical to assure that guidelines
184 PERRIN AND DEWITT ACADEMIC PEDIATRICS
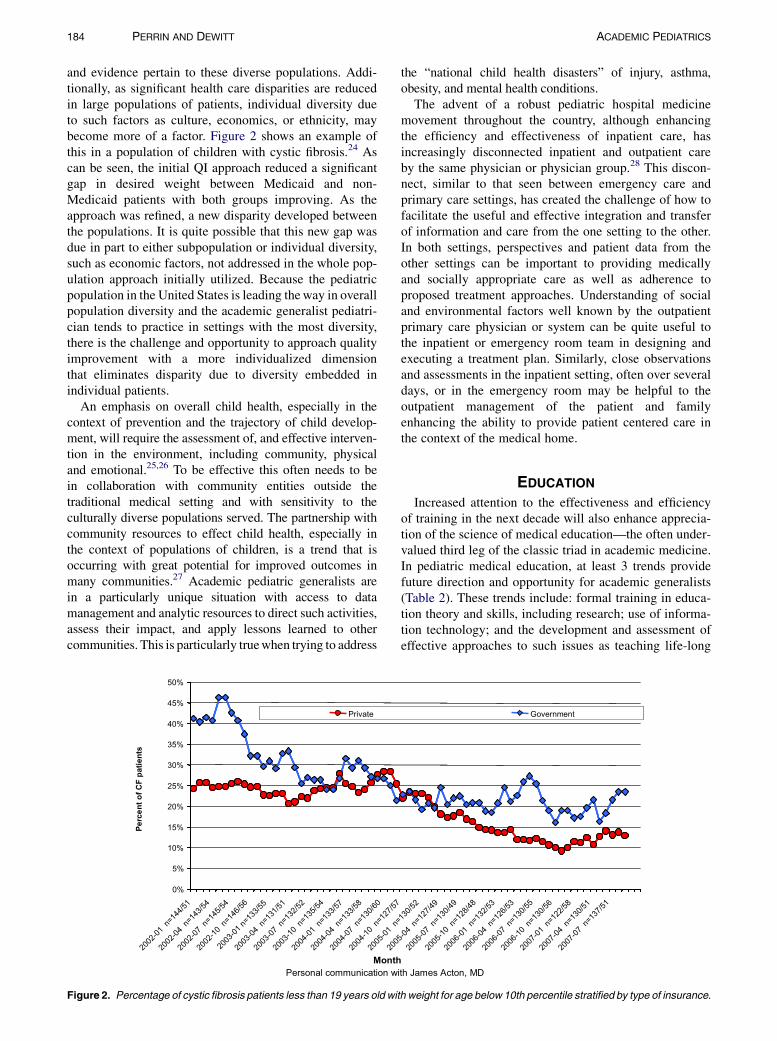
and evidence pertain to these diverse populations. Addi-tionally, as significant health care disparities are reducedin large populations of patients, individual diversity dueto such factors as culture, economics, or ethnicity, maybecome more of a factor. Figure 2 shows an example ofthis in a population of children with cystic fibrosis.24 Ascan be seen, the initial QI approach reduced a significantgap in desired weight between Medicaid and non-Medicaid patients with both groups improving. As theapproach was refined, a new disparity developed betweenthe populations. It is quite possible that this new gap wasdue in part to either subpopulation or individual diversity,such as economic factors, not addressed in the whole pop-ulation approach initially utilized. Because the pediatricpopulation in the United States is leading theway in overallpopulation diversity and the academic generalist pediatri-cian tends to practice in settings with the most diversity,there is the challenge and opportunity to approach qualityimprovement with a more individualized dimensionthat eliminates disparity due to diversity embedded inindividual patients.
An emphasis on overall child health, especially in thecontext of prevention and the trajectory of child develop-ment, will require the assessment of, and effective interven-tion in the environment, including community, physicaland emotional.25,26 To be effective this often needs to bein collaboration with community entities outside thetraditional medical setting and with sensitivity to theculturally diverse populations served. The partnership withcommunity resources to effect child health, especially inthe context of populations of children, is a trend that isoccurring with great potential for improved outcomes inmany communities.27 Academic pediatric generalists arein a particularly unique situation with access to datamanagement and analytic resources to direct such activities,assess their impact, and apply lessons learned to othercommunities. This is particularly truewhen trying to address
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
2002
-01 n
=144
/51
2002
-04 n
=143
/54
2002
-07 n
=145
/54
2002
-10 n
=146
/56
2003
-01 n=
133/5
5
2003
-04 n
=131
/51
2003
-07 n
=132
/52
2003
-10 n
=135
/54
2004
-01 n
=133
/57
2004
-04 n
=133
/58
2004
-07 n
=130
/60
2004
-10 n
=127
/57
2005
-01 n
200
Month
Pe
rc
en
t o
f C
F p
atie
nts
Private
Personal communication wi
Figure 2. Percentage of cystic fibrosis patients less than 19 years old wit
the “national child health disasters” of injury, asthma,obesity, and mental health conditions.The advent of a robust pediatric hospital medicine
movement throughout the country, although enhancingthe efficiency and effectiveness of inpatient care, hasincreasingly disconnected inpatient and outpatient careby the same physician or physician group.28 This discon-nect, similar to that seen between emergency care andprimary care settings, has created the challenge of how tofacilitate the useful and effective integration and transferof information and care from the one setting to the other.In both settings, perspectives and patient data from theother settings can be important to providing medicallyand socially appropriate care as well as adherence toproposed treatment approaches. Understanding of socialand environmental factors well known by the outpatientprimary care physician or system can be quite useful tothe inpatient or emergency room team in designing andexecuting a treatment plan. Similarly, close observationsand assessments in the inpatient setting, often over severaldays, or in the emergency room may be helpful to theoutpatient management of the patient and familyenhancing the ability to provide patient centered care inthe context of the medical home.
EDUCATION
Increased attention to the effectiveness and efficiencyof training in the next decade will also enhance apprecia-tion of the science of medical education—the often under-valued third leg of the classic triad in academic medicine.In pediatric medical education, at least 3 trends providefuture direction and opportunity for academic generalists(Table 2). These trends include: formal training in educa-tion theory and skills, including research; use of informa-tion technology; and the development and assessment ofeffective approaches to such issues as teaching life-long
=130
/52
5-04
n=12
7/49
2005
-07 n
=130
/49
2005
-10 n
=128
/48
2006
-01 n
=132
/53
2006
-04 n
=126
/53
2006
-07 n
=130
/55
2006
-10 n
=130
/56
2007
-01 n
=122
/58
2007
-04 n
=130
/51
2007
-07 n
=137
/51
Government
th James Acton, MD
h weight for age below 10th percentile stratified by type of insurance.

ACADEMIC PEDIATRICS FUTURE OF ACADEMIC GENERAL PEDIATRICS 185
learning habits, monitoring training and posttrainingknowledge and skills, and training directed toward medicalhome care. The importance of these themes is particularlyaccentuated by the many dimensions of health carereform.29
There is a greater appreciation of the need to approachmedical education as a rigorous discipline with applicationof evidence-based theory and assessment of outcomes,including medical outcomes.30 The Academic PediatricAssociation has been a pioneer in pediatric education inthis regard with regional and national workshops and longi-tudinal programs, such as the Faculty Scholars program.Increasingly leaders in pediatric medical education areexpected to have advanced training, including masters ordoctorate degrees in education, as part of their qualifica-tions. In many ways this shift is similar to the expectationof more formal training for clinical researchers thatevolved thirty years ago, usually in the form of fellowshipsthat have masters in clinical epidemiology or public healthas a foundation.31 To continue this trend in education, thedevelopment of more medical education fellowships,similar to the Macy Faculty Scholar Program at Harvardfor professional development of academic leaders, is crit-ical. These must focus on medical education innovationand research to determine more effective and efficientforms of training, a need accentuated by recent decreasesin duty hours for trainees and increases in clinical demandson faculty.
Just as in patient care, information technology iscreating changing paradigms in educational strategies,not only for physician training, but also patient and familyeducation. Early assessment of innovative use of onlinelearning and social media has demonstrated an effective-ness and efficiency that suggests traditional lectures arerelatively inefficient and less effective. Because onlinelearning is usually asynchronous it allows the learner tohave the educational experience at their convenience orthe delivery of information at the point of care. These allowthe education to occur at relatively high learner motivationsituations, considered a key element of effective education,and are best illustrated by the point-of-care concept.32
These concepts are equally true for patient and familyeducation with the added dimension of the challenge ofcommunication in an increasingly culturally diversepopulation. In both learner settings there is clear opportu-nity for a well trained medical education faculty to assessimpact, including patient outcomes. This is enhanced bythe ability to electronically track learner interaction withtraining through electronic learning management systems.Ultimately, the linkage of these electronic learningmanagement systems with electronic health records may
Table 2. Trends in Medical Education
� Formal training in education theory and skills, including research� Use of information technology� Development and assessment of effective approaches to:
� Teaching lifelong learning habits� Monitoring training and posttraining knowledge and skillstraining directed toward medical home care
facilitate assessment of those patient outcomes linkedto training.As leaders in pediatric medical education, academic
pediatric generalists also have the opportunity to developand assess emerging paradigms in the field. These includeenhancement of life-long learning behaviors, monitoringprogress throughout training and practice such as themaintenance of certification approach promulgated bythe American Board of Pediatrics, and effective waysof training future pediatricians in the application ofsystems-based care, quality improvement, and the tenetsof medical home related to child health. This opportunityis enhanced by a generalist perspective that allowsa synthesis and teaching of the many determinants of childhealth that can be intertwined in the teaching of theseparadigms. Of note, these learning processes begin inmedical school and continue throughout the career trajec-tory. Determining the effectiveness of current approachesto these processes and developing new ones, enhanced inpart by the information technology and a generalistperspective, clearly is in the realm of the well trainedmedical educators mentioned above.
RESEARCH
DATABASES AND ANALYSES
Research in child health, especially the types of researchcarried out in academic general pediatrics, has muchopportunity for change, consolidation, and expansion inthe next decade. New databases, linked with much moresophisticated data management systems, will allow newstrategies for (much more efficient) analysis. Newer infor-mation technology capacities have supported various trialand registry databases (eg, Redcap,33 I2B234) and havemuch promise for pediatric health services research.Abilities to link data systems will likely allow investigatorsto examine health data in the context of social andenvironmental data, include genomics and other biologicinformation, and permit more longitudinal analyses thando many current cross-sectional sets. The NationalChildren’s Study is a prototype for this work and shouldprovide much new material for study in the coming years.Changing methods and databases will couple with newanalytic strategies, such as multi-level modeling, to addressinteresting health services research questions.Another promising development arises from the growing
number of condition-specific research networks (eg, cysticfibrosis, congenital heart disease, autism, inflammatorybowel disease), and many of these offer exciting opportuni-ties for health services and quality improvement research.
RESEARCH PARADIGMS
Although the randomized, controlled trial (RCT) haslong had stature as the gold standard for research, newerresearch paradigms will likely introduce investigators tonew ways of developing evidence. Researchers knowof course the many limitations of the RCT—the length oftime required to mount and complete an RCT, the lack ofgeneralizability to populations different from those in the

186 PERRIN AND DEWITT ACADEMIC PEDIATRICS
trial, and lack of ability to change the intervention based onpreliminary findings. For children especially, commontherapies often lack evidence from RCTs—more so thanfor most adult medicine treatments. More importantly,many questions central to child health concerns do notlend themselves to RCTs. Quality improvement and pedi-atric education highlight areas very much needing newresearch paradigms. Much attention to quality of evidencehas come from the work of the Agency for HealthcareResearch and Quality–funded Evidence-Based PracticeCenters and the GRADE program35—working to systema-tize the development and review of evidence. This workinitially focused on evaluations of randomized, controlledtreatment trials, although it has extended over recent yearsto include screening and diagnosis as well as diagnosis andtreatment for rare diseases, where RCTS are unlikely toexist. Distinctions between quality improvement andrandomized trials include the differences in speed of datacollection and reporting of findings, the ability to makechanges as the quality improvement project proceeds,responsiveness to local conditions as some characteristicsof quality improvement. Numerous theories of qualityimprovement exist, lending themselves to careful planningand implementation of research studies. Work in imple-mentation research and comparative effectiveness partlyaddresses needs for better research strategies to demon-strate what works and how. Cluster randomized trials areone promising research design. Szilagyi has pointed outthe critical nature of improving research along the wholetranslational pathway, with academic general pediatricshaving particular relevance in the T3 to T4 translation.36
Research in pediatric education reflects a core activity ofAcademic Pediatric Association (APA) members and otheracademic generalists.37 Efforts by the APA and the Associ-ation of Pediatric Program Directors to enhance facultyknowledge of research designs and methods have ad-dressed ways to improve the internal and external validityof studies, develop the ability to generalize from a singleprogram to many, and develop robust and reproduciblefindings. Educational studies and others increasinglymake good use of qualitative methods, which can providein-depth understanding of health care phenomena andhelp to strengthen the development of quantitative researchmodels.
Expanding interest in studies of social determinants ofchild and adolescent health in part reflect the great changesin the diversity of the child population in North America.This work, increasingly multidisciplinary, has examinedthe physiological and developmental interactions of thechild with her social and physical environment and addeda series of additional areas, including roles of culture andimmigrant experience to this complex mix. This workhas also helped to substantiate the cumulative risk ofmultiple adverse effects over time—in some ways mirror-ing the work of Marmot and others in the UnitedKingdom38—and led to an evidence base indicating theimportance of life course theories in understanding theseinteractions and their long-term outcomes. Going wellbeyond simple notions of social class, these theories
provide much support for exciting new ways to addresschild and family health.As pediatric health services research expands with these
new methods, sources, and theories, some common themeswill likely persist—especially, the 4 Ds that have helpeddistinguish key elements of child and adolescent health:development and its effects on disease manifestationsand treatment, dependency of children on their parentsand other adults, different epidemiology (from that ofadults) with fewer chronic conditions, and different demo-graphics (described above).39 To this, Stille and colleaguesrecently added a fifth D, the patchwork of differentpayment systems for child health (lacking the consistentcoverage of Medicare).19 These themes, coupled withmuch greater understanding of diversity in North Americanhouseholds, provide much guidance still to good researchquestions. The next decade will see major changes in theorganization and financing of child health services, andthese changes can also provide much food for thoughtregarding critical research questions—which organiza-tional schemes work best, for whom, how? How canpayment reform enhance key characteristics of child healthcare and prevention?
ADVOCACY
The previous sections provide some guidance for thecontent of advocacy for children’s health. Academic gener-alists provide the bulk of care for high risk children andyouth in the United States and have special knowledge oftheir needs.We also have special expertise in a wide varietyof issues from educating pediatric professionals to abuse/neglect, development and behavior, environmental risks,chronic illness, prevention, and epidemiology. All of theseissues remain vital in the coming decades. Economicchange and new policies alone should attract much atten-tion to the value of advocacy, to include children in thechanging program and policy environments (Table 3).What characteristics of new payment methods can besthelp children? What changes in the social and physicalenvironment may affect child health? How does under-standing of diversity lead to better prevention and treat-ment? Answers to these questions will not come withoutsupport for investigators to address them and leaders touse their findings. Advocacy can rest very much on theclinical, cultural, and community insights of academicgeneralists, linked closely to the development of evidenceto support best advocacy.40
Critical to advocacy over this time is assurance that chil-dren and adolescents receive the benefits from changes inhealth care and insurance under CHIPRA and the ACA.Furthermore, increasing political support behind otherkey investments in children merits ongoing work.Academic generalists in their advocacy must partner withother professional organizations and even morebuild coalitions, especially with families and employers(who benefit when their employees’ children are well).Academic generalists can support the central theme ofprevention and bring their understanding of trajectories

Table 3. Public Policy Opportunities
� Children’s Health Insurance Program Reauthorization Act.� Quality measures development� Quality improvement state demonstrations
� Health Care Reform (Affordable Care Act)� Medical home enhancement� Care coordination and team work� Payment reform
� Accountable care organizations and other payment models� Children with special health care needs
ACADEMIC PEDIATRICS FUTURE OF ACADEMIC GENERAL PEDIATRICS 187
for children in diverse circumstances and ways to enhancethese trajectories over time and diminish cumulative risk.
SUMMARY
Children, youth, and families face a series of new trendsthat will affect their health and well-being. Dramaticgrowth in diversity among children and families has majorimplications for program development and research intoways to improve health while diminishing disparities.Accompanying changes in the sociodemographic makeupof US children, the nation is experiencing watershedchanges in health care delivery, information technology,and quality measurement, all of which provide majoropportunities for the academic general pediatric commu-nity in education, policy, practice, and programs. Majorpolicy developments reflected in the CHIPRA reauthoriza-tion and the ACA provide challenges to ensure the bestapplication of new strategies (eg, medical home, newpayment approaches) to benefit children’s health andlong-term outcomes. The future is now—and academicgeneralists should step to these new challenges.
REFERENCES
1. Shipman SA, Lurie JD, Goodman DC. The general pediatrician:
projecting future workforce supply and requirements. Pediatrics.
2004;113:435–442.
2. Federal Interagency Forum on Child and Family Statistics. POP3,
racial and ethnic composition: percentage of US children ages 0–17
by race and Hispanic origin, selected years 1980–2007 and projected
2008–2020. Available at: http://www.childstats.gov/americaschildren/
demo.asp. Accessed February 26, 2010.
3. Starmer AJ, Duby JC, Slaw KM, et al. Members of the 2020 Task
Force. Vision of pediatrics in the year 2020 and beyond: preparing
for plausible futures. Pediatrics. 2010;126:971–981.
4. Kithara D, Carper K. National Health Care Expenses in the US
Civilian Non-Institutionalized Population, 2007. Statistical Brief
272. December 2009. Agency for Healthcare Research and Quality,
Rockville, Md. Available at: http://www.meps.ahrq.gov/mepsweb/
data_files/publications/st272/stat272.pdf. Accessed February 2,
2011.
5. Machlin S. Trends in Health Care Expenditures for Children Under
Age 18:2006 Versus 1996. Statistical Brief 253. August 2009. Agency
for Healthcare Research and Quality, Rockville, Md. Available at:
http://www.meps.ahrq.gov/mepsweb/data_files/publications/st253/
stat253.pdf. Accessed February 2, 2011.
6. Guyer B,Ma S, Grason H, et al. Early childhood health promotion and
its life course health consequences. Acad Pediatr. 2009;9:142–149.
7. Institute of Medicine. In: Shonkoff JP, Phillips DA, eds. From
Neurons to Neighborhoods. Washington, DC: National Academies
Press; 2000.
8. National Research Council and Institute of Medicine. Children’s
Health—The Nation’sWealth: Assessing and Improving Child Health.
Washington, DC: National Academies Press; 2004.
9. Perrin JM, Fluet C, Anderson B, et al. Benefits for employees with
children with special needs: findings from the Collaborative
Employee Benefit Study. Health Aff. 2007;26:1096–1103.
10. Heckman J, Cunha F. Investing in our young people. In: Reynolds AJ,
Rolnick AJ, Englund MM, Temple JA, eds. Childhood Programs
and Practices in the First Decade of Life. New York: Cambridge
University Press; 2010.
11. Kaiser Family Foundation. Children’s Health Insurance Program
Reauthorization of 2009 (CHIPRA). 2009. Available at: http://
www.kff.org/medicaid/upload/7863.pdf. Accessed February 2, 2011.
12. Children’s Health Insurance Reauthorization Act. Available at: http://
www.ahrq.gov/chipra/. Accessed February 28, 2011.
13. Cooper WO, Kuhlthau K. Evaluating Medicaid managed care
programs for children. Ambul Pediatr. 2001;1:112–116.
14. HR 3590. The Patient Protection and Affordable Care Act of 2010.
Available at: http://frwebgate.access.gpo.gov/cgi-bin/getdoc.cgi?
dbname¼111_cong_bills&docid¼f:h3590enr.txt.pdf. Accessed
August 5, 2010.
15. Berenson RA, Rich EC. How to buy a medical home? Policy options
and practical questions. J Gen Intern Med. 2010;25:619–624.
16. Ku L. Ready, set, plan, implement: executing the expansion of
Medicaid. Health Aff (Millwood). 2010;29:1173–1177.
17. Perrin JM. Treating underinsurance. N Engl J Med. 2010;363:
881–883.
18. Perrin JM, Bloom SR, Gortmaker SL. The increase of childhood
chronic conditions in the United States. JAMA. 2007;297:2755–2759.
19. Stille C, Turchi RM, Antonelli R, et al. Academic Pediatric Asso-
ciation Task Force on the Family-Centered Medical Home. The
family-centered medical home: specific considerations for child
health research and policy. Acad Pediatr. 2010;10:211–217.
20. Homer CJ, Klatka K, Romm D, et al. A review of the evidence for the
medical home for children with special health care needs. Pediatrics.
2008;122:e922–e937.
21. Kuhlthau K, Bloom S, Van Cleave J, et al. Evidence for family-
centered care for children with special health care needs: a systematic
review. Acad Pediatr. 2011;11:136–143.
22. Haskard Zolnierek KB, DiMatteo MR. Physician communication and
patient adherence to treatment: a meta-analysis. Med Care. 2009;47:
826–834.
23. Estrin D, Sim I. Open mHealth architecture: an engine for health care
innovation. Science. 2010;330:759–760.
24. DeWitt TG. Diversity in pediatrics: the challenge and the opportunity.
Ambul Pediatr. 2008;8:73–76.
25. Schor EL. Rethinking well-child care. Pediatrics. 2004;114:210–216.
26. Halfon N, DuPlessis H, Inkelas M. Transforming the US child health
system. Health Aff. 2007;26:315–330.
27. Hertzman C, Bertrand J. Children in poverty and the use of early
development instrument mapping to improve their worlds. Paediatr
Child Health. 2007;12:687–692.
28. Landrigan CP, Conway PH, Edwards S, Srivastava R. Pediatric
hospitalists: a systematic review of the literature. Pediatrics. 2006;
117:1736–1744.
29. Caudill TS, Lofgren R, Jennings CD, Karpf M. Health care reform
and primary care: training physicians for tomorrow’s challenges
[commentary]. Acad Med. 2011;86:158–160.
30. Chen F, Bauchner H, Burstin H. A call for outcomes research in
medical education. Acad Med. 2004;79:955–960.
31. DeWitt TG, Cheng TL. The role of Title VII funding in academic
general pediatrics fellowships and leadership. Acad Med. 2008;83:
1103–1106.
32. Dee CR, Teolis M, Todd AD. Physicians’ use of the personal digital
assistant (PDA) in clinical decision making. J Med Libr Assoc.
2005;93:480–486.
33. Redcap. Available at: http://www.project-redcap.org/. Accessed
February 2, 2011.
34. I2B2. Available at: https://www.i2b2.org/. Accessed February 2, 2011.

188 PERRIN AND DEWITT ACADEMIC PEDIATRICS
35. Brozek JL, Akl EA, Alonso-Coello P, et al. Grading quality of
evidence and strength of recommendations in clinical practice
guidelines. An overview of the GRADE approach and grading quality
of evidence about interventions. Allergy. 2008;64:669–677.
36. Szilagyi P. Translational research and pediatrics. Acad Pediatr. 2009;
9:71–80.
37. Gusic ME. Celebrating education and building the community of
pediatric educators. Acad Pediatr. 2010;10:89–90.
38. Marmot M, Wilkinson RG, eds. Social Determinants of Health. 2nd
ed. Oxford: Oxford University Press; 2005.
39. Forrest CB, Simpson L, Clancy C. Child health services research.
Challenges and opportunities. JAMA. 1997;277:1787–1793.
40. Richmond JB, Kotelchuck M. Coordination and development of
strategies and policy for public health promotion in the United States
(revised). In: Holland WW, Detels R, Knox EG, eds. Textbook of
Public Health. 2nd ed. London: Oxford Press; 1991;1:441–454.