functional electrical stimulation for the upper limb in...
TRANSCRIPT

FES in tetraplegic SCI ver 3 16/08/2015
1
Functional electrical stimulation for the upper limb in tetraplegic spinal cord
injury: a systematic review
Siddeshwar Patil,1, 2 Wajid A Raza,2 Firas Jamil,2 Richard Caley,2 Rory J O'Connor1,
3
1. Academic Department of Rehabilitation Medicine, University of Leeds, D Floor,
Martin Wing, LGI, Leeds, UK
2. Yorkshire Regional Spinal Injuries Centre, Pinderfields General Hospital,
Wakefield, UK
3. National Demonstration Centre in Rehabilitation Medicine, Leeds Teaching
Hospitals NHS Trust, Leeds, UK
Address for correspondence: Dr S Patil, Academic Clinical Fellow in Rehabilitation
Medicine, Academic Department of Rehabilitation Medicine, University of Leeds, D
Floor, Martin Wing, LGI, Leeds, LS1 3EX, UK
Telephone: + 44 (0) 113 3922560
Facsimile: +44 (0) 113 392259
E-mail: [email protected]
Keywords: Spinal cord injury, rehabilitation, upper limb, functional electrical
stimulation
Word count: 2,295
FES in tetraplegic SCI ver 3 16/08/2015
2
Abstract
Introduction: Technological advances have helped to improve functional ability in
spinal cord injury survivors. The aim of this study is to systematically review the
evidence for functional electrical stimulation (FES) on functional tasks involving the
upper limb in people with spinal cord injuries.
Methods: We systematically searched from September 2009 to September 2014 in
relevant databases using a combination of keywords covering spinal cord injury and
FES. Studies were selected using predetermined criteria.
Results: The search yielded 144 studies. Only five studies met our inclusion criteria.
All five reported improvements immediately and at follow-up in functional ability as a
result of FES or FES combined with conventional therapy.
Discussion: There is some preliminary evidence that FES may reduce disability due
to upper limb-related activity limitations in tetraplegic spinal cord injury. Further work
needs to examine the role of FES in more detail, and in combination with other
treatments.
Abstract word count: 144/150

FES in tetraplegic SCI ver 3 16/08/2015
3
1.0 Introduction
Spinal cord injury (SCI) primarily affects young adults, with up to 1000 people
sustaining a SCI each year in the UK. Approximately 50,000 people live with SCI in
the UK, 80% of whom are male.[1, 2] The estimated annual cost of SCI is £1Bn in
direct healthcare costs and lost income. SCI causes permanent and life-altering
impairments in motor, sensory and psychosocial functioning. A SCI can be defined
as a lesion within the spinal cord resulting in disruption of neural communication.
Tetraplegia is when all four limbs are affected and is caused by a cervical level injury
to the spinal cord. The neurological outcome is determined by the extent of trauma to
the spinal cord at the time of injury and the consequent inflammatory cascade.
Individuals with high tetraplegia are unable to perform basic activities of daily living
(ADL) or express themselves through gestures or touch due to limitation of function
in one or both upper limbs. Restoration of hand function is a priority for these people
affected by SCI [1] and providing increased hand function for tetraplegic patients is
an important rehabilitation objective. For these individuals, wrist extension may be
preserved, but is of insufficient power to facilitate any activity. Wrist extension can
have an important impact on function, as it results in flexion of the fingers due to the
passive effect in the finger flexors which is known as the tenodesis grip. The
tenodesis grip is a grasp which can be strengthened by enhancing the force of wrist
extension. This may be achieved by surgical intervention or by functional electrical
stimulation (FES).[3]
Surgical intervention has its own risks of complications ranging from related to
anaesthesia to surgical procedure itself. In tetraplegic patients one has to be careful

FES in tetraplegic SCI ver 3 16/08/2015
4
about possible tracheal stenosis that could lead to difficult intubation and the need to
perform a tracheotomy after extubation due to a postoperative tracheal edema.
Surgical procedure related complications range from pin migration, reflex
sympathetic dystrophy to ineffective and/or insufficient results. Elongation of and or
stretching of tendon are one of the many reasons for insufficient results as reported
both by Rothwell et al and Friden et al.[4, 5] Apart from complications, the resultant
spasticity which is very common following SCI is a contraindication to surgical
intervention. Cleveland FES center is researching the use of FES to block unwanted
spasticity.[6]
Advances in rehabilitation engineering, including wheelchair and FES technology,
have helped to further increase mobility in people with SCI [7] and use of this
technology can help overcome the limitations of surgical intervention in achieving the
desired improvement in hand function.
The concept of electrotherapy has evolved from the times of its application using
electric eels in ancient Greece, Egypt and Rome for pain management, to storage of
electricity by Leyden and Alessandro Volta to stimulation of peroneal nerve for foot-
drop using a prototype electric device to stimulate and restore function when the
term FES was coined in 1961.[7]
The first implantable FES was rolled out as Freehand in 1986 in Cleveland, OH,
USA.[8] This however required several surgical procedures for each individual for
optimal use of the device.[9] A majority of the literature on Freehand reported
positive outcomes, however were mostly case series. Despite positive outcomes, the
first generation Freehand system is no longer available.

FES in tetraplegic SCI ver 3 16/08/2015
5
Although since 1986, there has been ongoing research and developments in the field
of FES/Neuro-prosthesis, Spinal Cord Injury Rehabilitation Evidence (SCIRE) project
documents availability of only level 4 evidence from one pre-post study that used,
Implanted Stimulator-Telemeter (IST-12).[10] In view of no level 1 evidence being
available until 2008 for the use of FES as a standalone therapy, we decided to
review literature between 2009 and 2014.
There is evidence suggesting that intensive task-specific training can enhance hand
function in people with tetraplegia.[11] This can most likely be achieved by FES until
surgical procedures can be easily accessible.
The aim of this review is to systematically review the evidence for FES on motor
control and functional ability of the upper limb in spinal cord injured people.

FES in tetraplegic SCI ver 3 16/08/2015
6
2.0 Methods
2.1 Literature search
This review is based on a systematic literature search of studies published from
September 2009 to September 2014 in the databases of PubMed, EMBASE,
PsycInfo, and Food, Science & Technology abstracts.
The following keywords were used in this search: tetraplegia, neuromuscular
electrical stimulation, functional electrical stimulation, upper extremity, hand,
functional ability, motor control.
In addition to searching databases, the references of relevant publications were also
checked.
2.2 Study selection
The initial selection of articles was based on title and abstract. Two reviewers (SP
and WAR) independently selected, summarized and scored the studies. Consensus
reached by discussion in case of disagreements. The study inclusion criteria were:
1) Involving patients with complete or incomplete cervical SCI
2) Investigating FES, possibly comparing it with other conventional therapies
3) Limited to adults and human studies
4) Be reported in a full-length publication in a peer-reviewed journal
We excluded those studies focusing on FES for spinal levels other than cervical SCI,
studies examining restoration of functions other than motor control and functional
abilities, children, or duplicates and part presentations of one larger study.

FES in tetraplegic SCI ver 3 16/08/2015
7
2.3 Methodological quality judgment
We applied the levels of evidence to better understand the methodological quality of
the included studies. We used the Jovell and Navarro-Rubio classification (Table 1)
of study design.[12] The classification system of Jovell and Navarro-Rubio
mentioned by the authors graded evidence from meta-analyses of RCTs or from
large RCTs as 'good'; small RCTs and non-randomised controlled trials as 'good to
fair'; non-randomised controlled retrospective studies, cohort studies and case-
control studies as 'fair'; and noncontrolled and other studies as 'poor'.
2.4 Data extraction
We examined the reports of the studies and gathered the following data:
1. Patient characteristics
2. Type of FES used – surface or implanted
3. Outcome measures used
4. Conclusions based on results
These characteristics of the studies were used to compare the effect of FES in upper
limb function following cervical SCI.

FES in tetraplegic SCI ver 3 16/08/2015
8
3.0 Results
3.1 Selection of studies
The literature search in PubMed yielded 132 studies. Searches in EMBASE yielded
an additional 12 studies; no further studies were found on searches in other
databases. Only five studies met the inclusion criteria and were included for analysis
(see flow diagram). An overview of the characteristics of the reviewed articles is
displayed in Table 2.
3.2 Methodological quality judgment
Two of the selected studies were small, randomized controlled trials with
measurements prior to commencing therapy and completion of therapy.[13, 14]
Applying the Jovell and Novarro-Rubio classification, a methodological score of III
was assigned. One study was classified as Cohort study with a methodological score
of VI. [15] The remaining two studies were single case study and two clinical case
studies with a methodological score of VIII. One of them was proof of concept study.
[16, 17]
3.3 Description of interventions
In two studies, FES was compared with conventional occupational therapy. One
study each described the use of myo-electrically controlled functional electrical
stimulation, implanted FES, and FES with a brain computer interface. The electrical
stimulation consisted of neuromuscular stimulation and partly innervated muscles.

FES in tetraplegic SCI ver 3 16/08/2015
9
3.4 Description of study participants
In the comparative studies, the sizes of both the groups were comparable. In three
studies, the neurological level at baseline ranged from C4 to C7; one study was at
single level C4 and one study was above C3. The time since injury was at least 6
months in one study and more than 3 weeks but less than 24 weeks in another
study. In two studies, the time since injury was equal to or more than 2 years; in
another study it was between 13 months and 11 years.
3.5 Outcome measures
The outcome measures employed in the selected studies covered a variety of the
domains that comprise the International Classification of Functioning, Disability and
Health (ICF).[18] The domain of body functions and structures was represented by
the Graded Redefined Assessment of Strength, Sensitivity and Prehension
(GRASSP) and the Toronto Rehabilitation Institute Hand Function Test (TRI-
HFT).[10] More specific functions were measured using the Grasp and Release Test
(GRT) and grasp strength.[19] The activities domain was recorded using the Action
Research Arm Test (ARAT), the Functional Independence Measure (FIM), the Spinal
Cord Independence Measure (SCIM) and noting performance in general activities of
daily living (ADL). [18] The participation domain was assessed using ad hoc visual
analogue scales (VAS) and the National Aeronautics and Space Administration task
load index questionnaire (NASA-TLX).[20] Clinically relevant change scores with
respect to the cohort were recorded where possible.

FES in tetraplegic SCI ver 3 16/08/2015
10
In total, there were 10 different outcome measures between the five included studies
assessing functional outcomes and motor control.
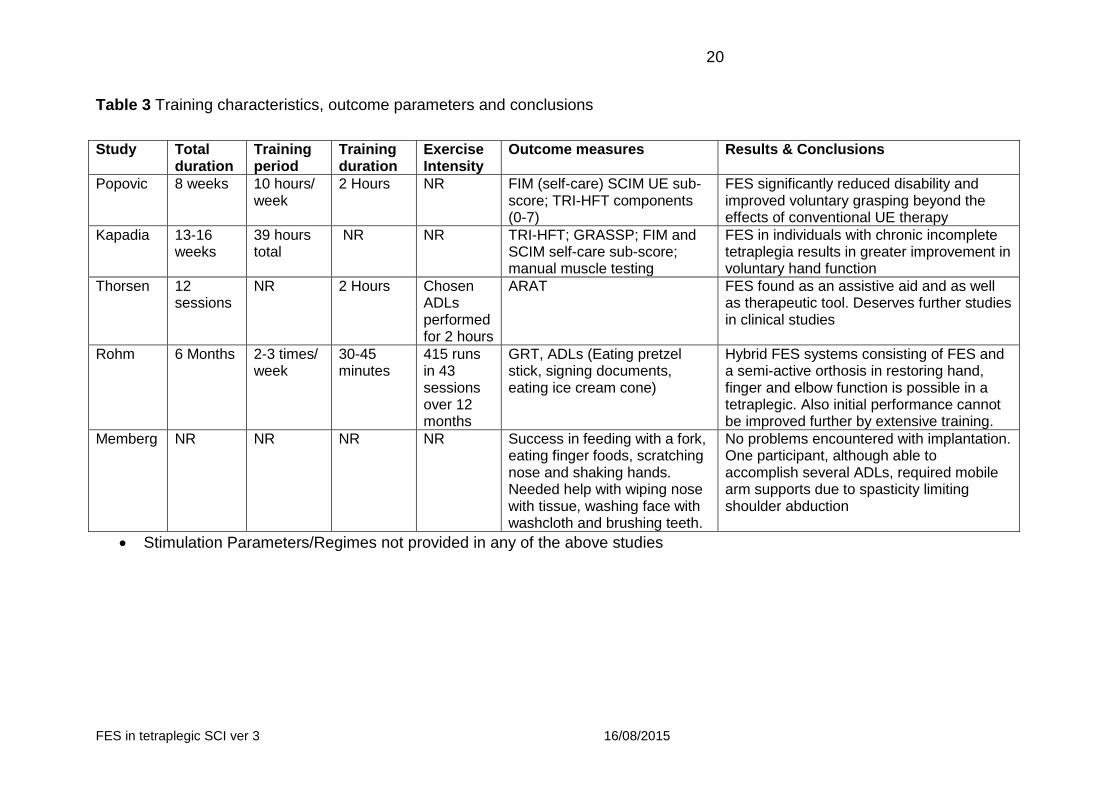
3.6 Study outcomes
All five studies reported improvement, both immediate and at follow-up, in motor
control and/or functional ability of upper extremity as a result of FES or FES with
conventional therapy (Table 3).[13-17]
Memberg reported successful implantation of the FES and established safety and
effectiveness.[17] This group however did report difficulty in optimal achievement
due to lack of ability to overcome increased shoulder adduction movement due to
spasticity and needed the support of mobile arm support. Rohm reported hybrid FES
systems have the ability to restore hand; finger and elbow function and that initial
performance achieved by the BCI FES did not improve any further with further
extensive training.[16]

FES in tetraplegic SCI ver 3 16/08/2015
11
4.0 Discussion
Individuals with tetraplegia as a result of either traumatic or non-traumatic spinal cord
injury are dependent on their care providers with their activities of daily living.
Tetraplegic patients identify improvement in upper extremity function as one of their
greatest needs.[21] Traditionally, rehabilitation strategies to reduce reliance on
others and achieve greater hand function consisted of prescription of orthotic
devices, adaptive equipment and use of compensatory techniques. Advances in the
understanding of the impact of tetraplegia and its complications means that
technological rehabilitation interventions can assist the delivery of these traditional
methods. In addition to these interventions, surgical techniques have been
established to increase upper extremity function.[22]
Although FES techniques have improved and are emerging as promising
interventions, there are only a few controlled studies reporting on its effectiveness.
All the five studies in this review reported positive effects owing to FES on motor
control and functional abilities; four of the studies focused on chronic SCI.
As most of the studies focused on chronic SCI, it can be assumed that functional
ability and motor control still has the potential to improve with therapy. This is in
accordance with the findings of Popovic who reported improvement in FIM, SCIM
and TRI-HFT in both groups (FES+COT and COT only).[13] One of the explanations
for motor function improvement in the chronic stage is reorganization of the brain
and spinal cord.[23]

FES in tetraplegic SCI ver 3 16/08/2015
12
Additionally, one of the studies reported spasticity as a limiting factor in ability to
achieve ADLs.[22] We can speculate that if FES/hybrid FES as therapy is
commenced in the acute stage of SCI, we could overcome this secondary
complication being a limitation in the successful outcome. Although it is difficult to
differentiate between spontaneous recovery and the effects of FES, it is reasonable
to assume that principles of reorganization of the brain and spinal cord as mentioned
for chronic SCI also apply to acute SCI.
In this review, although there were studies rated as good to fair, there were biases.
These were small number of participants, high loss to follow-up at 6 months,[14] and
only two studies having a control group.[13] It was difficult to compare results across
studies due to the wide variety of outcome measures. To accurately assess the
impact of various interventions on upper extremity function it is important to match
outcome scales to the domains of the ICF to provide a standardized framework for
assessing outcome. Limitations of these studies were lack of depth in describing the
characteristics of FES therapy and the intensity of treatment was not clear in some
studies. As stated in the ICF domain of environment, contextual factors having a
bearing on the principles of training need to be considered. Intensity, task specificity
and goal-oriented practice are important principles of motor control and should be
described fully in reports.[14]
In addition to FES in isolation, hybrid FES comprising orthotic devices or
exoskeletons in addition to the FES system can be explored to make tasks easier for
people requiring arm support or with limitations due to spasticity.[24] These systems

FES in tetraplegic SCI ver 3 16/08/2015
13
may also increase the intensity of therapy facilitating arm movements that enable
patients to perform more repetitive movements.
FES is not a new concept in rehabilitation engineering and many studies have shown
positive effects on upper extremity motor control and functional abilities. However,
only a small number of controlled trials were found. These are weakened by bias in
terms of numbers recruited or limitations in the outcome measures. The current
evidence base is predominately for chronic SCI patients. The beneficial effects of
FES can only be made available in future studies by being more specific in
describing the characteristics of FES therapy and verifying the outcomes following
ICF domains.
CONCLUSION:
We can conclude that there are surgical and technological interventions available for
improved arm and hand function. Surgery and FES can be used in combination
where needed by moving voluntary muscles and activating paralysed muscles with
FES. In view of limitations and contraindications to surgical intervention, FES may
have an advantageous role but this is only a speculation in view of lack of studies
with larger sample and in accordance with ICF framework.
As research continues to advance and provide more options and evidence for
improved function in this population than ever before, contribution of well-designed
outcome studies to the evidence base will ultimately help address the complicated
problem of improving hand function in tetraplegic individuals. This can result in

FES in tetraplegic SCI ver 3 16/08/2015
14
reduction of dependency of this population on their caregivers and care cost
reduction.
FES in tetraplegic SCI ver 3 16/08/2015
15
5.0 References
1. Anderson, K.D., Targeting recovery: priorities of the spinal cord-injured
population. J Neurotrauma, 2004. 21(10): p. 1371-83.
2. O'Connor, R.J. and P.C. Murray, Review of spinal cord injuries in Ireland.
Spinal Cord, 2006. 44(7): p. 445-8.
3. Keith, M.W., et al., Tendon transfers and functional electrical stimulation for
restoration of hand function in spinal cord injury. J Hand Surg Am, 1996. 21(1): p.
89-99.
4. Rothwell A et al.,Donor tendon stetch following deltoid to triceps transfer. J
Bone Joint Surg Br 2002 vol 84-B no. SUPP III 267-268
5. Friden J and Lieber RL. Quantitative evaluation of the posterior deltoid to
triceps tendon transfer based on muscle architectural properties. J Hand Surg Am.
2001 Jan; 26(1): 147-55
6. Bryden et al., Surgical restoration of arm and hand function in people with
tetraplegia. Topics in Spinal Cord Injury Rehabilitation 2012 Winter; 18(1): 43-9
7. Liberson, W.T., et al., Functional electrotherapy: stimulation of the peroneal
nerve synchronized with the swing phase of the gait of hemiplegic patients. Arch
Phys Med Rehabil, 1961. 42: p. 101-5.
8 Cornwall R, Hausman MR. Implanted neuroprostheses for restoration of hand
function in tetraplegic patients. J Am Acad Orthop Surg. 2004;12:72–79
9 Keith MW et al., Tendon transfers and functional electrical stimulation for
restoration of hand function in spinal cord injury. J Hand Surg.1996;21A:89–99.

FES in tetraplegic SCI ver 3 16/08/2015
16
10 Kilgore et al., An implanted upper extremity neuroprosthesis using myoelectric
control. J Hand surg Am. 2008 Apr; 33(4): 539-550
11 Beekhuizen, K.S. and E.C. Field-Fote, Massed practice versus massed
practice with stimulation: effects on upper extremity function and cortical plasticity in
individuals with incomplete cervical spinal cord injury. Neurorehabil Neural Repair,
2005. 19(1): p. 33-45
12. Jovell, A.J. and M.D. Navarro-Rubio, [Evaluation of scientific evidence]. Med
Clin (Barc), 1995. 105(19): p. 740-3.
13. Popovic, M.R., et al., Functional electrical stimulation therapy of voluntary
grasping versus only conventional rehabilitation for patients with subacute
incomplete tetraplegia: a randomized clinical trial. Neurorehabil Neural Repair, 2011.
25(5): p. 433-42.
14. Kapadia, N., V. Zivanovic, and M.R. Popovic, Restoring voluntary grasping
function in individuals with incomplete chronic spinal cord injury: pilot study. Top
Spinal Cord Inj Rehabil, 2013. 19(4): p. 279-87.
15. Thorsen, R., et al., A noninvasive neuroprosthesis augments hand grasp force
in individuals with cervical spinal cord injury: the functional and therapeutic effects.
ScientificWorldJournal, 2013. 2013: p. 836959.
16 Rohm, M., et al., Hybrid brain-computer interfaces and hybrid
neuroprostheses for restoration of upper limb functions in individuals with high-level
spinal cord injury. Artif Intell Med, 2013. 59(2): p. 133-42.
17 Memberg, W.D., et al., Implanted neuroprosthesis for restoring arm and hand
function in people with high level tetraplegia. Arch Phys Med Rehabil, 2014. 95(6): p.
1201-1211.e1.

FES in tetraplegic SCI ver 3 16/08/2015
17
18. World Health Organisation, International Classification of Functioning,
Disability and Health. First ed, ed. W.H. Organisation. 2001, Geneva: WHO. 1-302.
19. http://www.rehabmeasures.org/rehabweb/allmeasures.aspx?PageView=Shared
20. http://humansystems.arc.nasa.gov/groups/tlx/paperpencil.html
21. Snoek, G.J., et al., Survey of the needs of patients with spinal cord injury:
impact and priority for improvement in hand function in tetraplegics. Spinal Cord,
2004. 42(9): p. 526-32.
22. Moberg, E., The present state of surgical rehabilitation of the upper limb in
tetraplegia. Paraplegia, 1987. 25(4): p. 351-6.
23. Adkins, D.L., et al., Motor training induces experience-specific patterns of
plasticity across motor cortex and spinal cord. J Appl Physiol (1985), 2006. 101(6): p.
1776-82.
24. Hesse, S., et al., Upper and lower extremity robotic devices for rehabilitation
and for studying motor control. Curr Opin Neurol, 2003. 16(6): p. 705-10.
Table 1 Classification of study designs by Jovell and Navarro-Rubio (1995)
Level Strength of evidence Type of study design
I Good
Meta-analysis of RCTs
II Large-sample RCTs
III Good to fair
Small-sample RCTs
IV Non-randomized controlled prospective trials
V Non-randomized controlled retrospective trials
VI Fair Cohort studies

FES in tetraplegic SCI ver 3 16/08/2015
18
Level Strength of evidence Type of study design
VII Case–control studies
VIII Poor
Non-controlled clinical series; descriptive studies
IX Anecdotes or case reports
Abbreviation: RCT- Randomised controlled trials.

FES in tetraplegic SCI ver 3 16/08/2015
19
Table 2 Study and participant characteristics
Study Design Intervention groups
Number of participants
Time since injury
Age Neurological level
Memberg et al
Case studies
Implanted FES
2 11 years
13 Months
48 years
27 years
C1 C3
Thorsen et al
Cohort Myoelectrically controlled FES
27 > 6 months
Mean age 40
years
C5 to C7
Popovic et al
RCT OT + FES (8 weeks) versus OT (8 weeks)
21 17 Weeks
3 Weeks – 21
Weeks
Mean age 45
years
C4 to C7
Rohm et al
Single case study
Brain computer interface + FES
1 24 Months
40 years
C4
Kapadia et al
RCT FES (13-16 weeks) versus OT (13-16 weeks)
8 ≥24 Months
- C4 to C7
Abbreviations: FES: functional electrical stimulation; OT: occupational therapy
FES in tetraplegic SCI ver 3 16/08/2015
20
Table 3 Training characteristics, outcome parameters and conclusions
Study Total duration
Training period
Training duration
Exercise Intensity
Outcome measures Results & Conclusions
Popovic 8 weeks 10 hours/ week
2 Hours NR FIM (self-care) SCIM UE sub-score; TRI-HFT components (0-7)
FES significantly reduced disability and improved voluntary grasping beyond the effects of conventional UE therapy
Kapadia 13-16 weeks
39 hours total
NR NR TRI-HFT; GRASSP; FIM and SCIM self-care sub-score; manual muscle testing
FES in individuals with chronic incomplete tetraplegia results in greater improvement in voluntary hand function
Thorsen 12 sessions
NR 2 Hours Chosen ADLs performed for 2 hours
ARAT
FES found as an assistive aid and as well as therapeutic tool. Deserves further studies in clinical studies
Rohm 6 Months 2-3 times/ week
30-45 minutes
415 runs in 43 sessions over 12 months
GRT, ADLs (Eating pretzel stick, signing documents, eating ice cream cone)
Hybrid FES systems consisting of FES and a semi-active orthosis in restoring hand, finger and elbow function is possible in a tetraplegic. Also initial performance cannot be improved further by extensive training.
Memberg NR NR NR NR Success in feeding with a fork, eating finger foods, scratching nose and shaking hands. Needed help with wiping nose with tissue, washing face with washcloth and brushing teeth.
No problems encountered with implantation. One participant, although able to accomplish several ADLs, required mobile arm supports due to spasticity limiting shoulder abduction
Stimulation Parameters/Regimes not provided in any of the above studies
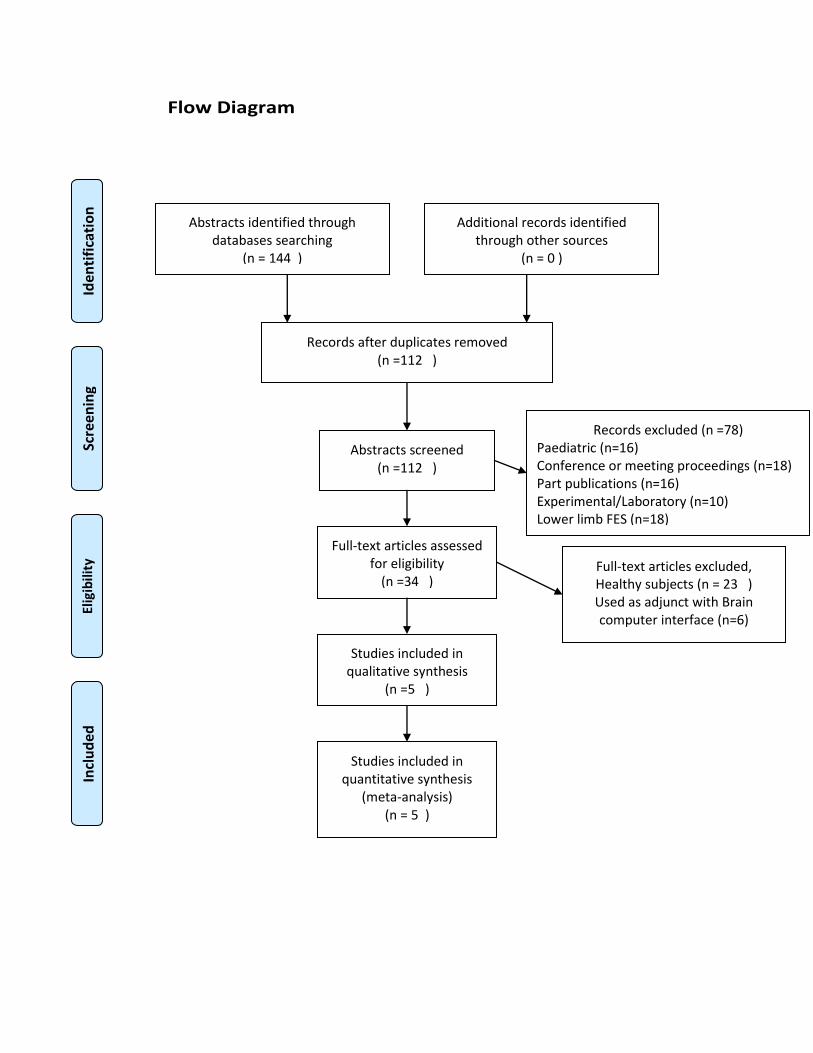
Flow Diagram
Abstracts identified through databases searching
(n = 144 )
Scre
enin
g In
clu
ded
El
igib
ility
Id
enti
fica
tio
n
Additional records identified through other sources
(n = 0 )
Records after duplicates removed (n =112 )
Abstracts screened (n =112 )
Records excluded (n =78) Paediatric (n=16) Conference or meeting proceedings (n=18) Part publications (n=16) Experimental/Laboratory (n=10) Lower limb FES (n=18)
PedPp
Full-text articles assessed for eligibility
(n =34 ) Full-text articles excluded, Healthy subjects (n = 23 ) Used as adjunct with Brain computer interface (n=6)
Studies included in
qualitative synthesis (n =5 )
Studies included in quantitative synthesis
(meta-analysis) (n = 5 )