from chest pain to multiple myeloma: radiology in...
TRANSCRIPT

From Chest Pain to Multiple Myeloma:
Radiology in Practice Mekeme
Utuk, Harvard Medical School Year III
Gillian Lieberman, MD
January 2012Mekeme
Utuk, 2013Gillian Lieberman, MD

2
Our Patient –
RB
•
RB is a 58yoM with no significant PMH presented to PCP with 2 weeks of vague upper chest pain with some SOB.
Mekeme
Utuk, 2013Gillian Lieberman, MD

3
Chest Pain Differential Diagnosis •Cardiovascular:
–
*Myocardial ischemia (angina/MI)– *Pericarditis– Aortic stenosis–
*Pulmonary Embolism– *Aortic dissection– Myocarditis–
Mitral Valve Prolapse–
Pulmonary Hypertension–
Right ventricular hypertrophy
•Pulmonary:– Pneumonia– Pleurtitis– Bronchitis–
(*Tension) Pneumothorax– Tumor
•Musculoskeletal:–
Cervial
or thoracic disc disease or arthritis– Shoulder arthritis– Costochondritis– Subacromial
bursitis
•Gastrointestinal:– *Esophageal rupture– GERD– Esophageal spasm– Peptic Ulcer Dz– Biliary
Disease– Pancreatitis
•Other:– Anxiety/panic attack– Herpes zoster– Breast disorders– Chest wall tumor–
Thoracic outlet syndrome– Mediastinitis
* = “Don’t miss” diagnosis!!
Mekeme
Utuk, 2013Gillian Lieberman, MD
4
Back to RB
•
PCP initially attributed pain to costochondritis.•
Pain was refractory to NSAIDs.
•
An outpt
stress test was performed, which was normal.
•
Pain persisted for several more days and spread to mid-back.
•
Pt went to his local ED, where a CTA was performed to rule out a pulmonary embolism.
Mekeme
Utuk, 2013Gillian Lieberman, MD

5
Computed Tomography Angiography (CTA)
•
Fast, simple, noninvasive technique that provides images with excellent spatial resolution and good soft tissue contrast.
•
Using a single contrast medial bolus injection, CTA allows for complete visualization of the entire aorta and its branches.
•
The imaging modality of choice in the evaluation of patients with suspected pulmonary embolus.
Mekeme
Utuk, 2013Gillian Lieberman, MD

6
Review: Great Vessels on CTA
http://www.e-radiography.net/technique/ chest/Chest_t4_labelled_mediastinum_ct.jpg
Mekeme
Utuk, 2013Gillian Lieberman, MD
Axial CT+, Arterial Phase

7
Companion Patient #1: PE on CTA
•
Unenhanced CT scan demonstrates subtle regions of hyperattenuation.
http://radiographics.rsna.org/content/31/5/1425.full.pdf+html
•
Confirmatory CT pulmonary angiogram demonstrates acute pulmonary embolism within the right main
and left interlobar
pulmonary arteries.
Mekeme
Utuk, 2013Gillian Lieberman, MD
Axial CT- Axial CT+
8
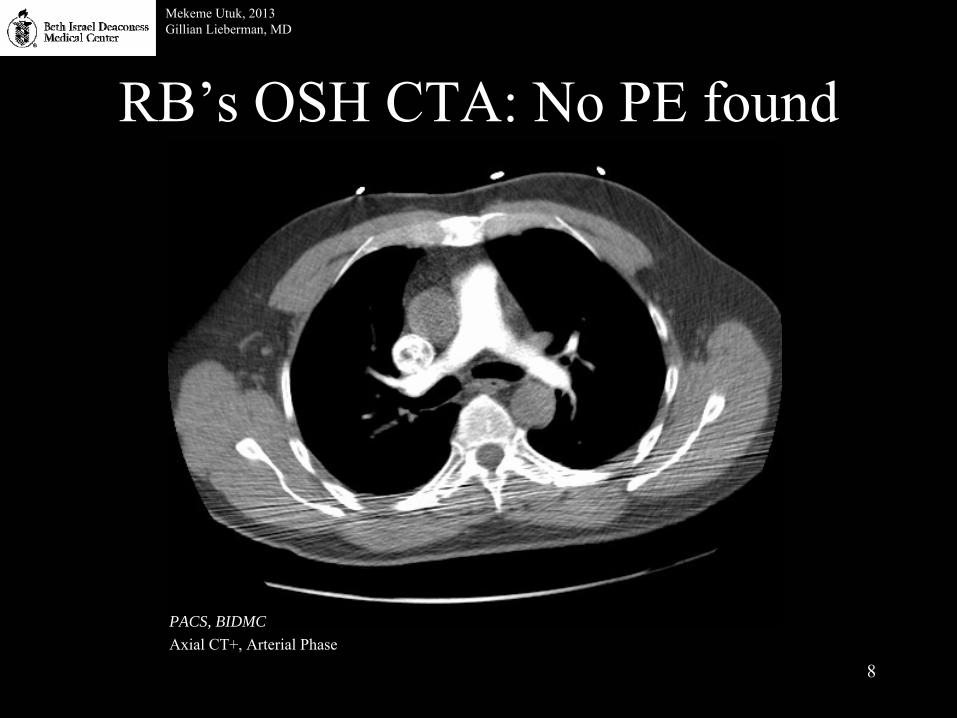
RB’s
OSH CTA: No PE found
PACS, BIDMCAxial CT+, Arterial Phase
Mekeme
Utuk, 2013Gillian Lieberman, MD

9
•
To recap, tests RB has had:–
Stress test: normal
–
CTA: no pulmonary embolus
•
However, other views on CTA did find something significant.
Mekeme
Utuk, 2013Gillian Lieberman, MD
10
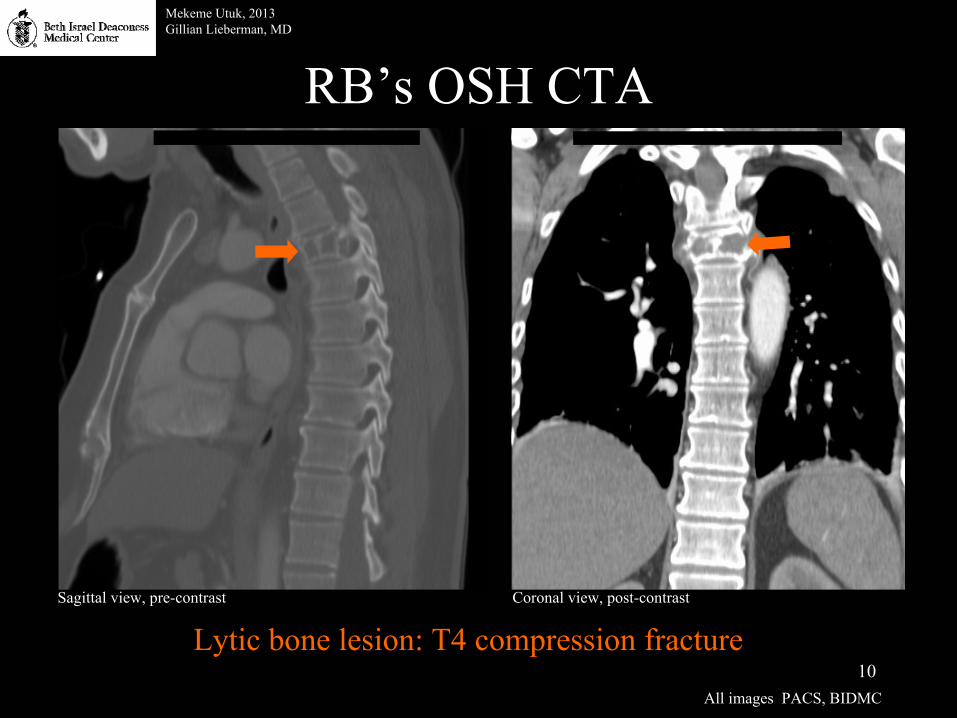
RB’s
OSH CTA
Coronal view, post-contrastSagittal
view, pre-contrast
Mekeme
Utuk, 2013Gillian Lieberman, MD
All images PACS, BIDMC
Lytic
bone lesion: T4 compression fracture

11
Our Patient: Hospital Course
•
With the lytic
bone lesion seen on CTA, RB was diagnosed with a T4 compression fracture, and transferred to BIDMC for further workup.
Mekeme
Utuk, 2013Gillian Lieberman, MD

12
Narrowing the CP Differential•Cardiovascular:
–
*Myocardial ischemia (angina/MI)– *Pericarditis– Aortic stenosis–
*Pulmonary Embolism– *Aortic dissection– Myocarditis–
Mitral Valve Prolapse–
Pulmonary Hypertension–
Right ventricular hypertrophy
•Pulmonary:– Pneumonia– Pleurtitis– Bronchitis–
(*Tension) Pneumothorax– Tumor
•Musculoskeletal:–
Cervial
or thoracic disc disease or arthritis– Shoulder arthritis– Costochondritis– Subacromial
bursitis
•Gastrointestinal:– *Esophageal rupture– GERD– Esophageal spasm– Peptic Ulcer Dz– Biliary
Disease– Pancreatitis
•Other:– Anxiety/panic attack– Herpes zoster– Breast disorders– Chest wall tumor–
Thoracic outlet syndrome– Mediastinitis
* = “Don’t miss” diagnosis!!
Mekeme
Utuk, 2013Gillian Lieberman, MD

13
Lytic
Bone Lesion DDx FOG MACHINES:
FOG
MACHINES
= Fibrous Dysplasia= Osteoblastoma= Giant Cell Tumor
= Metastasis/Myeloma= Aneurysmal
Bone Cyst
= Chondroblastoma= Hyperparathyroidism (brown tumors) / Hemangioma= Infection= Non-ossifying Fibroma= Eosinophilic
Granuloma
/ Enchondroma
= Solitary Bone Cyst
Mekeme
Utuk, 2013Gillian Lieberman, MD

14
Mekeme
Utuk, 2013Gillian Lieberman, MD
Let’s take a step back and review how to approach bone lesions in general.

15
A Simple Approach to Bone Lesions
•
Age•
Location
•
Margins•
Periosteal
Reaction
•
Matrix•
Number
•
Soft Tissue
Mekeme
Utuk, 2013Gillian Lieberman, MD

16
Bone Lesions by Age•
Our Patient:
58yo
Mekeme
Utuk, 2013Gillian Lieberman, MD
http://www.radiologyassistant.nl/en/494e15cbf0d8d

17
Bone Lesions by Location
http://www.radiologyassistant.nl/en/494e15cbf0d8d
Mekeme
Utuk, 2013Gillian Lieberman, MD
•
Our Patient: T4 lesion

18
Bone Lesions by Margins and Periosteal
Reaction
•
Margin: helps indicate whether a lesion is benign or malignant–
Geographic: well-defined margin from normal bone; usually benign
–
Moth-Eaten–
Permeative: most aggressive; poorly demarcated; usually malignant
Burgener, et al. Bone and Joint Disorders. 2nd
Ed.
Mekeme
Utuk, 2013Gillian Lieberman, MD
Non-ossifying fibroma,distal femur
Non-hodgkin’s
lymphoma,distal femur
Ewing sarcoma,proximal femur
•
Periosteal
Reaction: non-
specific reaction that occurs whenever bone is irritated (e.g. by tumor, trauma, infection)
http://www.radiologyassistant.nl/en/494e15cbf0d8d

19
Bone Lesions by Matrix
•
Matrix: –
Opacity:•
Lytic
(black)
•
Sclerotic (white)•
Mixed
–
Calcification pattern: gives clues regarding the lesion’s tissue of origin•
Osteoid
matrix: “cloud-like”
•
Chondroid
matrix: “arcs and rings”
Mekeme
Utuk, 2013Gillian Lieberman, MD
All images http://www.radiologyassistant.nl/en/494e15cbf0d8d
Osteosarcoma
Chondrosarcoma

20
Bone Lesions by Number and Soft Tissue
•
Number–
Most bone tumors are solitary
–
Multiple osteolytic
lesions-
FEEMHI:•
Fibrous dysplasia•
Enchondromas•
Eosinophilic
Granuloma•
Metastases and myeloma•
Hyperparathyroidism•
Infection
•
Soft tissue involvement generally indicates aggressive lesions (i.e. malignant)
Mekeme
Utuk, 2013Gillian Lieberman, MD

21
Our Patient: Narrow the DDx
•
58yoM•
T4 compression fracture
Mekeme
Utuk, 2013Gillian Lieberman, MD
FOG
MACHINES
= Fibrous Dysplasia= Osteoblastoma= Giant Cell Tumor
= Metastasis/Myeloma= Aneurysmal
Bone Cyst= Chondroblastoma= Hyperparathyroidism (brown tumors) / Hemangioma= Infection= Non-ossifying Fibroma= Eosinophilic
Granuloma
/ Enchondroma= Solitary Bone Cyst

22
•
After being transferred to BIDMC, RB had more imaging done.
Mekeme
Utuk, 2013Gillian Lieberman, MD
Let’s review some spinal anatomy, and then continue
with RB’s findings.

23
Review: Spinal Anatomy
http://www.trialsightmedia.com/exhibit_store/images/thoracicspine.jpg
Axial T1 MRI, pre-contrastPACS, BIDMC
Mekeme
Utuk, 2013Gillian Lieberman, MD
Sagittal T1 MRIhttp://www.greatriverspineclinic.com/causes-of-back-pain/lower-back-pain/lumbar-spinal-stenosis/

24
Our Patient: Spinal MRIMekeme
Utuk, 2013Gillian Lieberman, MD
•
Pathologic fracture at T4 level
with compression of the vertebral body and retropulsion
and enhancing epidural and paraspinal
soft tissue.• Spinal canal is narrowed by ~50%• No other areas of bony abnormalities
All images PACS, BIDMC
Sagittal, T1-weighted, post-contrast
Close-up of lesionSagittal
T1-weighted, post-contrast
Sagittal, T1-weighted, pre-contrast

25
Our Patient: Additional workup
•
RB also had a CT chest, abdomen, and pelvis to look for a primary tumor.
•
No primary tumor was found.•
Up to date on all age-related cancer screenings (colon, prostate)
•
Thus, diagnosis is likely myeloma, not metastasis
Mekeme
Utuk, 2013Gillian Lieberman, MD

26
Multiple Myeloma: Facts•
Neoplastic
proliferation of a single line of plasma cells that make a monoclonal immunoglobulin.
•
Increased incidence >50yo, African Americans•
Unclear etiology –
It is known that neoplastic
plasma cells release osteoclast
activating factor, which causes the stereotypical osteolytic
lesions•
Clinical features: –
Bone pain, fractures, and vertebral collapse secondary to osteolytic
lesions–
Pathologic fractures–
Hypercalcemia–
Anemia (2/2 bone marrow infiltration)–
Renal failure (2/2 hypercalcemia
and immunoglobulin precipitation in renal tubules, which causes Bence-Jones protein casts)
–
Recurrent infections (2/2 decreased humoral
immunity)•
70% of MM patients will die of infection (usually lung or urinary tract)
Mekeme
Utuk, 2013Gillian Lieberman, MD

27
Multiple Myeloma: More Facts
•
Treatment–
Indications: hypercalcemia, bone pain, spinal cord compression
–
General treatment plan:•
Systemic CTX•
Radiation therapy (if no response to CTX, or disabling pain)•
Autologous
peripheral blood stem cell transplant > BMT•
Prognosis is poor:–
Median survival 2-4y with treatment; a few months w/o treatment.
–
10% 5y survival rate
Mekeme
Utuk, 2013Gillian Lieberman, MD

28
Diagnosing Multiple Myeloma •
Diagnostic Criteria:–
Bone marrow with ≥ 10% abnormal plasma cells, plus either:
•
Monoclonal (M-) protein in the serum•
M-protein in the urine•
Lytic
bone lesions (usually skull or axial skeleton)•
Radiographic Studies:–
Skeletal Survey (plan radiographs)
–
CT, MRI, and PET scans are more sensitive than radiographs. However, their use is reserved for patients with:
•
Bone pain w/ a normal skeletal survey•
Compression fractures•
Neurologic deficits possibly 2/2 cord compression
Mekeme
Utuk, 2013Gillian Lieberman, MD

29
Mekeme
Utuk, 2013Gillian Lieberman, MD
Let’s review these different imaging modalities while
continuing with RB’s workup.

30
MM Imaging: Skeletal Survey•
Initial modality for staging and monitoring disease progression •
Skeletal survey can show “punched-out” lytic
lesions, diffuse osteopenia, or fractures
Mekeme
Utuk, 2013Gillian Lieberman, MD
Companion Pt #2:67yoF with MM
All images PACS, BIDMC
No significantfindings on SS
(besides T4 lesion)Axial Skull Right humerus
RB’s
Skull

31
MM imaging: CT•
Faster and more sensitive than bone survey–
Can visualize lytic
lesions <5mm•
Excellent for evaluating bone stability and fractures
Mekeme
Utuk, 2013Gillian Lieberman, MD
Companion Pt #3:66yoF with MM
Skull, Axial CT-Chest/Abd/Pelvis Coronal CT+
All images PACS, BIDMC
RB’s
CT:No significant
findings(besides T4 lesion)

32
MM Imaging: MRI•
More sensitive than bone scan.
•
No ionizing radiation (unlike CT)
•
Can detect bone marrow lesions in MM pts with no findings on skeletal survey
•
Many MR sequences are used–
T1: HYPOintense
lesion
w/in hyerintense
BM–
STIR/T2: HYERintense
lesion w/in hypointense
BM–
Gadolimium: see post-contrast enhancement of MM lesions in BM
Mekeme
Utuk, 2013Gillian Lieberman, MD
Thoracic spine, Sagittal
T1Thoracic spine,
STIR
RB’s
MRI:No significant
findings(besides T4 lesion)
Sagittal
T1, PACS BIDMC
Hanrahan
et al. Current Concepts in the Evaluation of Multiple Myeloma with MR Imaging and FDG PET/CT. RadioGraphics. 2010.

33
MM imaging: FDG PET•
FDG (Flourodeoxyglucose): a glucose analogue
•
PET (Position Emission Tomography): nuclear imaging modality that creates 3D images of functional
processes in
the body–
Detects gamma rays emitted by a positron-emitting radionuclide tracer
–
Tracer is ligated
to biologically active molecule (e.g. FDG)•
FDG PET: The concentration of tracer imaged represent metabolic activity in the tissue via glucose uptake–
Helpful in monitoring treatment progression
Mekeme
Utuk, 2013Gillian Lieberman, MD

34
MM Imaging: FDG PET cont’dMekeme
Utuk, 2013Gillian Lieberman, MD
•
Note uptake in spine and chest area
Sagittal Sagittal
•
3mo after BMT•
Note decreased FDG uptake, which indicates a positive response to treatment.
•
RB did not undergo
FDG PET
Hanrahan
et al. Current Concepts in the Evaluation of Multiple Myeloma with MR Imaging and FDG PET/CT. RadioGraphics. 2010.
Companion Pt #4

35
Our Patient: Recap•
OSH: –
CTA
•
Day 1 of admission:–
MRI on C/T/L Spine
–
Skeletal Survey–
CT of Chest, Abdomen, Pelvis
•
Only significant finding: –
T4 lytic
lesion and compression fracture
Mekeme
Utuk, 2013Gillian Lieberman, MD

36
Our Patient: Significant Labs•
Hgb
15.5, Hct
44.8 no anemia
•
Ca 9.5 no hypercalcemia•
BUN 12, Crt
1 no renal failure
•
Negative SPEP and UPEP no M-protein•
No Bence-Jones protein excretion
Mekeme
Utuk, 2013Gillian Lieberman, MD
Is this really Multiple Myeloma??

37
Potential Diagnosis: Solitary Plasmacytoma
of Bone
•
Like MM, SPB is a neoplastic
proliferation of plasma cells.
•
Histologically
identical to MM•
Diagnostic criteria:–
Solitary bone lesion with clonal
plasma cells seen on bx
–
Normal BM with no clonal
plasma cells–
Normal skeletal survey and MRI of spine, except for solitary lesion
–
No anemia, hypercalcemia, or renal insufficiency
Mekeme
Utuk, 2013Gillian Lieberman, MD

38
Our Patient: Rest of Hospital Course•
Day 6 Surgery:–
T4 vertebrectomy
–
T3-T5 fusion
•
Day 8 Surgery: –
T1-T8 fusion
–
Transpedicular decompression
–
Multiple thoracic laminotomies
–
Iliac Crest BM Bx
Mekeme
Utuk, 2013Gillian Lieberman, MD
Cross-table lateralPACS, BIDMC
Thoracic spine radiograph in the OR, s/p
T1-T8 fusion

39
Our Patient: Updates•
T4 lesion pathology did show clonal
plasma cells
•
Unfortunately, BM bx
showed clonal
plasma cell dyscrasia
–
This ruled out SPB and confirmed MM
•
Received several cycles of radiation treatment
•
~5mo after initial presentation, underwent autologous
peripheral stem cell transplant•
Currently awaiting f/u
BM bx
to evaluate transplant response
Mekeme
Utuk, 2013Gillian Lieberman, MD
2.5w post-op, thoracic spine with instrumentationPACS, BIDMC

40
Take-Home Points•
Chest pain ≠ Cardaic
or Pulmonary diagnosis
Keep a broad DDx•
When evaluating bone lesions, age and location are very important–
MM: >50yo, Skull/axial skeleton
•
MM: Anemia, Hypercalcemia, Renal Failure –
But not every patient will have read the text books
•
When considering multiple myeloma, also consider solitary plasmacytoma
of bone
•
Imaging and biopsies are imperative to proper management–
CC CTA MRI Skeletal Survey CT Bx Diagnosis Txall within 8 days!
Mekeme
Utuk, 2013Gillian Lieberman, MD

41
References•
Agabegi
SS, E Agabegi. Step-Up to Medicine. 2nd
Edition. Baltimore, MD: Lippincott Williams & Wilkins; 2008: 338-339.
•
Burgener
FA, M Kormano, T Pudas. Bone and Joint Disorders. 2nd
Edition. New York, NY: Theime; 2006: 75-76.
•
Hanrahan
CJ, CR Christensen, JR Crim. Current Concepts in the Evaluation
of Multiple Myeloma with MR Imaging and FDG PET/CT. RadioGraphics. 2010. 30 (1): 127-U153.
•
Jan van der
Woude
H, R Smithuis. Bone Tumors –
Differential Diagnosis. The Radiology Assistant. http://www.radiologyassistant.nl/en/494e15cbf0d8d. Accessed 01/19/12.
•
Meyer, Christopher A., Achala
S. Vagal, Danielle Seaman. Put Your Back into It: Pathologic Conditions of the Spine at Chest CT. RadioGraphics.
2011; 31:1425-1441. •
Miller, WT. Thoracic Spine Trauma. Seminars in Roentegenology: Fractures of the Vertebral Column and Pelvis. 1992; 27(4):261.
•
Oldnall, Nick. Radiographgy
of the Chest. Xray2000 Nick’s Website. http://www.e-
radiography.net/technique/ chest/Chest_t4_ labelled_mediastinum_ ct.jpg. Acccessed
01/21/11.•
Rajkumar
SV. Clinical features, laboratory manifestations, and diagnosis
of multiple myeloma. UpToDate. http://www.uptodate.com/contents/clinical-features-laboratory-manifestations-and-
diagnosis-of-multiple-myeloma?source=search_result&search= multiple+myeloma&selectedTitle=1%7E150. Accessed 01/21/11.
•
Rajkumar
SV. Diagnosis and management of solitary plasmacytoma
of bone.UpTpDate. http://www.uptodate.com/contents/diagnosis-and-management-of-solitary-plasmacytoma-of-
bone?source=related_link. Accessed 01/21/11.
•
Zeiger, Roni
F.Chest
Pain. McGraw-Hill's Diagnosaurus
2.0. http://www.accessmedicine.com.ezp-prod1.hul.harvard.edu/diag.aspx. Accessed 01/18/11.
Mekeme
Utuk, 2013Gillian Lieberman, MD

42
Acknowledgements
•
David Glazier, MD•
Mai-Lan
Ho, MD
•
Gillian Lieberman, MD•
Claire Odom
•
Dr. James Brush, MD•
David Feinbloom, MD
•
Anthony Breu, MD
Mekeme
Utuk, 2013Gillian Lieberman, MD