francisco caceres servicio de urologia - presurgy.com · zampa, luigi storti, francesco attisani,...
TRANSCRIPT
FRANCISCO CACERES
SERVICIO DE UROLOGIA
EMDA

EMDA
Administración de fármacos por
vía sistémica.
Produce efectos tóxicos no
deseados en otros órganos.
Altas concentraciones al lugar elegido

IONTOFORESIS
Técnica de aplicación transcutanea de sustancias ó fármacos, mediante la corriente eléctrica que utiliza sus iones (ioniza) y moléculas para conseguir una mayor penetración en tiempo y profundidad en los tejidos.
Estudios demuestran que la concentración del fármaco es 800 veces mayor que una aplicación tópica
EMDA

ELECTROSMOSIS
Transporte de solutos no ionizados (partículas de la dilución) que a través de la solución aparece con la iontoforesis.
EMDA : iontoforesis+electro-osmosis transporta los elementos ionizados y no ionizados del
fármaco
EMDA

EMDA

Maquina Physionizer 3.0
Sencilla programación guardando la ultima en memoria
Energía por 10 pilas (portátil)
Posibilidad de corriente pulsada ó continua
Reglaje de intensidad de 0 a 30 mA
Máximo voltaje de 55 Voltios
Sistema de seguridad ante sobrecarga, calentamiento ó fallo
Aviso de baterías bajas, error de conexiones
EMDA

CATETER URETROVESICAL
Catéter de silicona de 16 Fr. con alma de plata
Balón de anclaje en cuello con 4 ml de aire
Toma positiva al aparato
Puerto de perfusión del fármaco
Puerto de balón
Conexión +
Puerto del fármaco
Balón
Orificios
EMDA

INDICACIONES
Andrología
Oncología
Cistopatías complejas
Patología prostática
E. Peyronie
Tumores de vejiga
Vejiga espástica, hiperactiva Cistitis recurrentes Cistitis intersticial
Prostatitis recurrentes Prostatitis infecciosa
EMDA
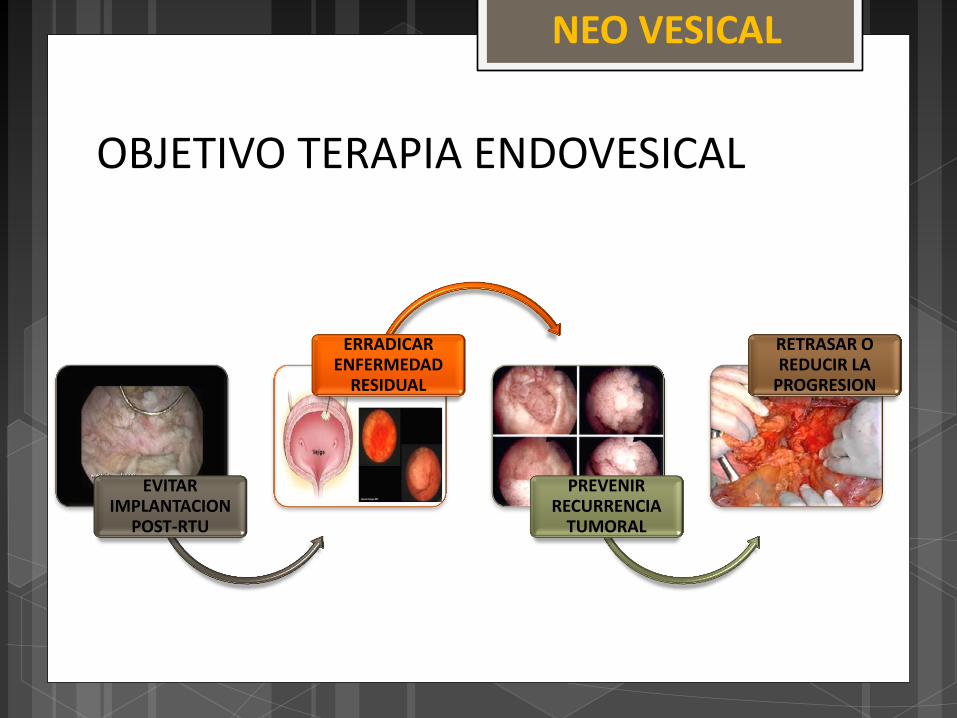
OBJETIVO TERAPIA ENDOVESICAL
EVITAR IMPLANTACION
POST-RTU
ERRADICAR ENFERMEDAD
RESIDUAL
PREVENIR
RECURRENCIA TUMORAL
RETRASAR O REDUCIR LA
PROGRESION
NEO VESICAL

NEO VESICAL
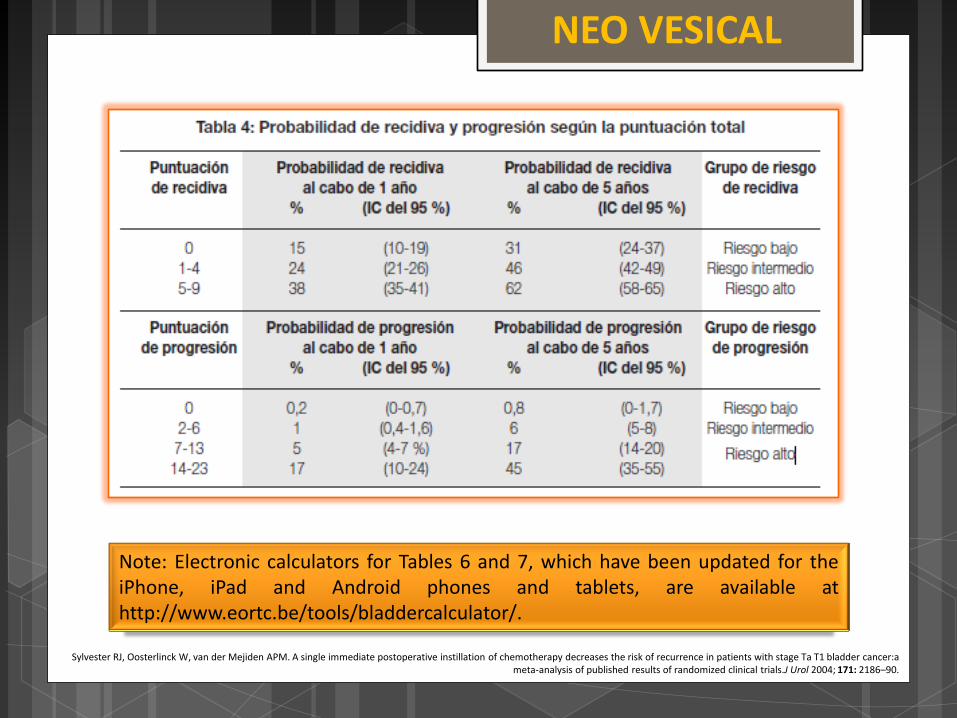
Sylvester RJ, Oosterlinck W, van der Mejiden APM. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage Ta T1 bladder cancer:a meta-analysis of published results of randomized clinical trials.J Urol 2004; 171: 2186–90.
NEO VESICAL
Sylvester RJ, Oosterlinck W, van der Mejiden APM. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage Ta T1 bladder cancer:a meta-analysis of published results of randomized clinical trials.J Urol 2004; 171: 2186–90.
Note: Electronic calculators for Tables 6 and 7, which have been updated for the iPhone, iPad and Android phones and tablets, are available at http://www.eortc.be/tools/bladdercalculator/.

NEO VESICAL

NEO VESICAL

INMUNOTERAPIA
TERAPIA ADYUVANTE
BCG
Reacción inmunológica
Apoptosis celular
Mecanismo antitumoral
Eficacia
Nivel IL-8
Di Stasi SM, Giannantoni A, Giurioli A, et al. Sequential BCG and electromotive mitomycin versus BCG alone for high-risk superficial bladder cancer: a randomised controlled trial. Lancet Oncol 2006;7:43–51.

QUIMIOTERAPIA
MMC
Destrucción células tumorales
circulantes
Evita implantes tumorales
Erradicación de focos tumorales
Producción superóxido
Unión al DNA
Bloquea síntesis
Di Stasi SM, Giannantoni A, Giurioli A, et al. Sequential BCG and electromotive mitomycin versus BCG alone for high-risk superficial bladder cancer: a randomised controlled trial. Lancet Oncol 2006;7:43–51.

In 2008 an estimated 386 300 cases were diagnosed
Newly diagnosed bladder cancer cases
75–85% present as non-muscle invasive disease
confined to the urothelium (stage Ta)
lamina propria (stage T1)
carcinoma in situ (stage Tis)
NEO VESICAL

RECIDIVA
Celulas tumorales
Durante la resección
Circulantes Nuevos
implantes
NEO VESICAL
• Recidivas 31-78 %
• Instilación inmediata después de RTU
Weldon TE, Soloway MS. Susceptibility of urothelium to neoplastic cellular implantation. Urology 1975; 5: 824–27

NEO VESICAL

• Patients received 40 mg mitomycin
• Dissolved in 50 mL sterile water
• within 6 h of TURBT.
• Retained in the bladder for 60 min with catheter clamping
• Continuous intravesical irrigation with saline for 8 h
Mitomycin immediately after TURBT
Sylvester RJ, Oosterlinck W, van der Mejiden APM. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage Ta T1 bladder cancer:a meta-analysis of published results of randomized clinical trials.J Urol 2004; 171: 2186–90.
NEO VESICAL

Sylvester RJ, Oosterlinck W, van der Mejiden APM. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage Ta T1 bladder cancer:a meta-analysis of published results of randomized clinical trials.J Urol 2004; 171: 2186–90.
Pre-TURBT intravesical EMDA
•Mitomycin 30 min before anaesthesia
•40 mg mitomycin
•Dissolved in 100 mL sterile water
•Retained in the bladder for 30 min
•While 20 mA pulsed electric current for 30 min was given externally.
EMDA
•Controlled electric
• Intravesical electrode
•Electrodes (on skin of the lower abdomen).
NEO VESICAL

TERAPIA VESICAL ADYUVANTE
low-risk
• No adjuvant intravesical therapy
Intermediate-risk
• 3 weeks after TURBT
• 40 mg PD mitomycin
• Once a week for 6 weeks
High-risk
• Initial intravesical treatment of 81 mg BCG
• Retained in the bladder for 120 min
• once a week for 6 weeks
Sylvester RJ, Oosterlinck W, van der Mejiden APM. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage Ta T1 bladder cancer:a meta-analysis of published results of randomized clinical trials.J Urol 2004; 171: 2186–90.
NEO VESICAL

INTERVALO LIBRE DE ENFERMEDAD
NEO VESICAL

“Supone un considerable avance aplicar EMDA antes de una resección transuretral, ya que la perforación de la vejiga con su consecuente extravasación del fármaco no es una preocupación. El incremento de concentración y profundidad de la mitomicina en las paredes de la vejiga, que potencialmente previenen el sembrado de células tumorales, parece ser la explicación más acertada de estos excelentes resultados.”
Oosterlinck, W. Nat Rev. Clin. Oncol, advanced online publication 13 September 2011; dol:10.1038/nrelinone.2011.140

EMDA presenta menor tasa de recurrencia p<0,005
Mejor absorción de mitomicina
• Destrucción
• Inhibir implantación de células
Grupo intermedio multifocalidad
Grupo de alto riesgo + BCG
No grupos de bajo riesgo
Costo efectivo
• Reducción absoluta 21 %
• Igual a tratar 4,8 pctes
RTU-V completa
CONCLUSIONES

ALTO RIESGO + BCG
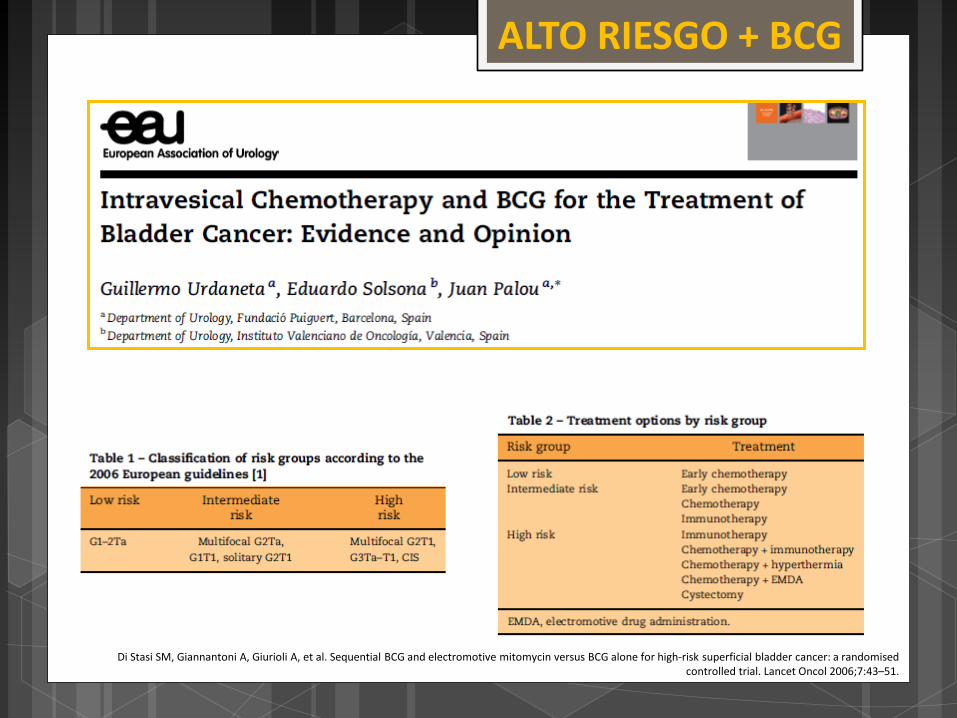
Di Stasi SM, Giannantoni A, Giurioli A, et al. Sequential BCG and electromotive mitomycin versus BCG alone for high-risk superficial bladder cancer: a randomised controlled trial. Lancet Oncol 2006;7:43–51.
ALTO RIESGO + BCG

Sequential BCG and electromotive
mitomycin versus BCG
alone for high-risk superficial bladder
cancer: a randomised
controlled trial
Savino M Di Stasi, Antonella Giannantoni, Arcangelo Giurioli, Marco Valenti, Germano
Zampa, Luigi Storti, Francesco Attisani, Andrea De Carolis,
Giovanni Capelli, Giuseppe Vespasiani, Robert L Stephen*
Lancet Oncol 2006; 7: 43–51
ALTO RIESGO + BCG

El estudio con 16 años de seguimiento compara los siguientes protocolos de tratamientos:
I. Solo BCG – 81 mg BCG una vez por semana durante 6 semanas seguido por una vez por mes durante 10 meses.
Total tratamientos:
16 tratamientos con BCG
ALTO RIESGO + BCG

II. BCG con EMDA MMC – 2 semanales de 81 mg BCG seguido por 3 semanales de 40 mg MMC con EMDA + 2 mensuales de 40 mg MMC seguido por 3 mensuales de 81 mg BCG.
Total tratamientos: 5 tratamientos de BCG y 5 tratamientos de EMDA MMC =
10 tratamientos total
ALTO RIESGO + BCG

BCG SOLO BCG/EMDA MMC % recidiva 62% 45% #meses hasta recurrencia 26 meses 79 meses % progresión 28% 12% % mortalidad por 23% 9% patología
ALTO RIESGO + BCG
Savino Mauro Di Stasi*, Cristian Verri, Emanuele Liberati, Rome, Italy, Francesco Masedu, L'Aquila, Italy, Luca Topazio, Rome, Italy, Marco Valenti, L'Aquila, Italy

In patients with stage pT1 urothelial bladder cancer
intravesical BCG combined with electromotive mitomycin provided better results than BCG alone in terms of higher response rates and longer remission
times.
Savino Mauro Di Stasi*, Cristian Verri, Emanuele Liberati, Rome, Italy, Francesco Masedu, L'Aquila, Italy, Luca Topazio, Rome, Italy, Marco Valenti, L'Aquila, Italy
ALTO RIESGO + BCG
