fractures of the acetabulum surgical treatment and
TRANSCRIPT

Address: 1 Kraljice Natalije Street, Belgrade 11000, Serbia
+381 11 4092 776, Fax: +381 11 3348 653
E-mail: [email protected], Web address: www.srpskiarhiv.rs
Paper Accepted* ISSN Online 2406-0895
Review Article / Преглед литературе
Saša Milenković1,2,, Milan Mitković1,2, Milorad Mitković1, Predrag Stojiljković1,2
Fractures of the acetabulum – surgical treatment and complications
Преломи зглобне чашице кука – хируршко лечење и компликације
1University of Niš, Faculty of Medicine, Nis, Serbia; 2Niš Clinical Centre, Clinic for Orthopaedic Surgery and Traumatology, Niš, Serbia
Received: April 12, 2020
Accepted: November 13, 2020
Online First: November 18, 2020
DOI: https://doi.org/10.2298/SARH200412110M
*Accepted papers are articles in press that have gone through due peer review process and have been
accepted for publication by the Editorial Board of the Serbian Archives of Medicine. They have not
yet been copy-edited and/or formatted in the publication house style, and the text may be changed
before the final publication.
Although accepted papers do not yet have all the accompanying bibliographic details available, they
can already be cited using the year of online publication and the DOI, as follows: the author’s last
name and initial of the first name, article title, journal title, online first publication month and year,
and the DOI; e.g.: Petrović P, Jovanović J. The title of the article. Srp Arh Celok Lek. Online First,
February 2017.
When the final article is assigned to volumes/issues of the journal, the Article in Press version will be
removed and the final version will appear in the associated published volumes/issues of the journal.
The date the article was made available online first will be carried over.
Correspondence to:
Saša MILENKOVIĆ
University of Niš, Faculty of Medicine, Clinic for Orthopaedic Surgery and Traumatology, Niš Clinical Center,
18000 Niš, Serbia
E-mail: [email protected]

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
2
Fractures of the acetabulum – surgical treatment and complications
Преломи зглобне чашице кука – хируршко лечење и компликације
SUMMARY
Acetabular fractures represent severe injuries that
mostly occur in car accidents, or after falling from
greater heights, most often in the working male
population. Acetabular fractures are present in our
clinical practice and require a good education and
surgical training. Surgical experience is one of the
prerequisites for achieving good treatment results,
because these fractures are accompanied by numerous
complications. In order to acquire knowledge and
skills in this field of surgery, it is necessary to have a
national center for education at one of the Medical
Faculties in Serbia. All dislocated acetabular fractures
(≥ 2mm), require early surgery, anatomical reduction
and stable internal fixation of acetabular fracture.
Acetabular fracture-dislocation requires urgent
reduction of the dislocated femoral head. The
anatomic reduction of the fracture is related to the time
of definitive bone fixation of the fracture. After 14
days from the fracture, anatomic reduction is more
difficult to achieve. In addition to these factors that
positively affect the final results of treatment, there are
negative factors as well, that result in poor outcomes.
They are directly correlated to the initial trauma that
occurs at the time of injury. Fracture comminution,
large dislocation (> 20mm), injury of the femoral
head, posterior dislocation of the hip, impaction,
traumatic or iatrogenic sciatic nerve palsy, are factors
that negatively affect the results and are responsible
for complications, as opposed to positive factors.
Keywords: acetabulum; fractures; surgical treatment;
complications
САЖЕТАК
Преломи зглобне чашице кука представљају
изузетно тешке повреде које настају најчешће у
саобраћајним удесима или приликом пада са већих
висина, најчешће код радно активне мушке
популације. Преломи зглобне чашице кука су
присутни у нашој клиничкој пракси и захтевају
добру едукацију и обученост кадрова за лечење.
Хируршко искуство је један од предуслова за
постизање добрих резултата лечења јер ове
преломе прате бројне компликације. Ради стицања
знања и вештина из ове области хирургије
потребно је да постоји национални центар за
едукацију при неком од Медицинских факултета у
Србији. Сви дислоцирани преломи (≥ 2 мм)
зглобне чашице кука се лече хируршки, а за
постизање добрих резултата неопходна је рана
анатомска репозиција и стабилна унутрашња
фиксација. Код прелома зглобне чашице са
ишчашењем кука, неопходна је хитна репозиција
ишчашеног кука. Анатомска репозиција прелома је
повезана са временом дефинитивне коштане
фиксације прелома. После 14 дана од прелома
анатомска репозиција се теже постиже. Поред ових
фактора који позитивно утичу на крајње резултате
лечења, са друге стране постоје и негативни
фактори који утичу на постизање лоших резултата
лечења. Они су директно повезани са тежином
иницијалне повреде која настаје у тренутку
прелома. Коминуција прелома, велика дислокација
(> 20мм), повреда главе фемура, ишчашење кука,
утиснуће, трауматска или јатрогена повреда
седалног нерва, су фактори који негативно утичу
на резултате и одговорни су за компликације,
насупрот позитивних фактора.
Кључне речи: зглобна чашица кука; преломи;
хируршко лечење; компликације
INTRODUCTION
The poor outcomes of conservative treatment of acetabular fractures, back in the 1950s,
led Letournel and Judet to embark on a new era of surgical treatment. The principles of open
reduction and stable internal fixation that they founded are still valid today, despite the great
advances in orthopedics and traumatology [1]. Acetabular fractures are severe, occurring in
young, working, more frequently male population, in car accidents or in falls from heights

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
3
[2]. The incidence of acetabular fractures is about 3 fractures / 100 000 patients / year [3].
The city of Nis is the largest city of the Nisava district with a population of about 350 000,
over 2 000 000 inhabitants of Southern and Eastern Serbia gravitate towards it. It has a
tertiary institution and an incidence of acetabular fractures of about 3 fractures / 100 000
patients / year. Considering the gravitational and treatable population in the Clinical Center
Nis, the Clinic for Orthopedic and Traumatology has made a significant step forward with
regard to the modern approach and treatment of acetabular fractures. In younger patients,
these fractures are usually caused by a strong axial force acting through the femoral shaft or a
direct force acting through a greater trochanter. In the elderly, acetabular fractures can cause
low-energy trauma due to the presence of osteoporosis. Acetabular fractures, primarily
dislocated ( > 2mm), are treated surgically with open fracture reduction and stable internal
fixation with acetabulum reconstructive plates/screws. The complications that accompany
these fractures are numerous, traumatic sciatic nerve injury, iatrogenic sciatic nerve injury,
infection, revision osteosynthesis, deep vein thrombosis (DVT), heterotopic ossification (HO)
- Broker I- IV, femoral head osteonecrosis, secondary osteoarthritis of the hip (OA) [4].
Some of these complications require latter revision surgery, which is reflected in total hip
replacement [5]. Due to all of the above and the complexity of acetabular surgery, constant
education of the surgeon and surgical experience are required to achieve excellent and good
outcomes, as it has been shown that surgical experience is an important factor directly
correlated to achieving the excellent and good outcomes [6].
CLINICAL ANATOMY OF THE ACETABULUM
The clinical anatomy of the acetabulum divides the acetabulum into the anterior and
posterior columns, which are arranged in the inverted “Y” shape. The anterior column is the
anterior part of the iliac bone that extends to the pubic bone. It contains the anterior part and
the edge of the iliac wing, the pelvic edge, the anterior wall of the acetabulum, and the upper
branch of the pubic bone. The posterior column consists of parts of the iliac and ischiadic
bones, large and small ischiadic notches, posterior wall of the acetabulum, most of the
quadrilateral surface, and ischiadic tuberositas. The upper part of the acetabulum, through
which load forces are transmitted is called the roof of the acetabulum. The vertical line that

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
4
runs through the center of the femoral head and the line that goes through the fracture of the
acetabulum make an angle called the “acetabular roof angle” [4].
MECHANISM OF INJURY
Acetabular fractures are caused by the action of an axial force through the femoral
shaft. The type of fracture of the acetabulum, its anterior or posterior structure, depends on
the position of the femoral head at the time of impact into the acetabulum. Another way of
creating an acetabular fracture is through the action of a direct force over a greater trochanter
when the quadrilateral surface of the acetabulum (central luxation) is most commonly
fractured [4].
CLASSIFICATION OF ACETABULAR FRACTURES
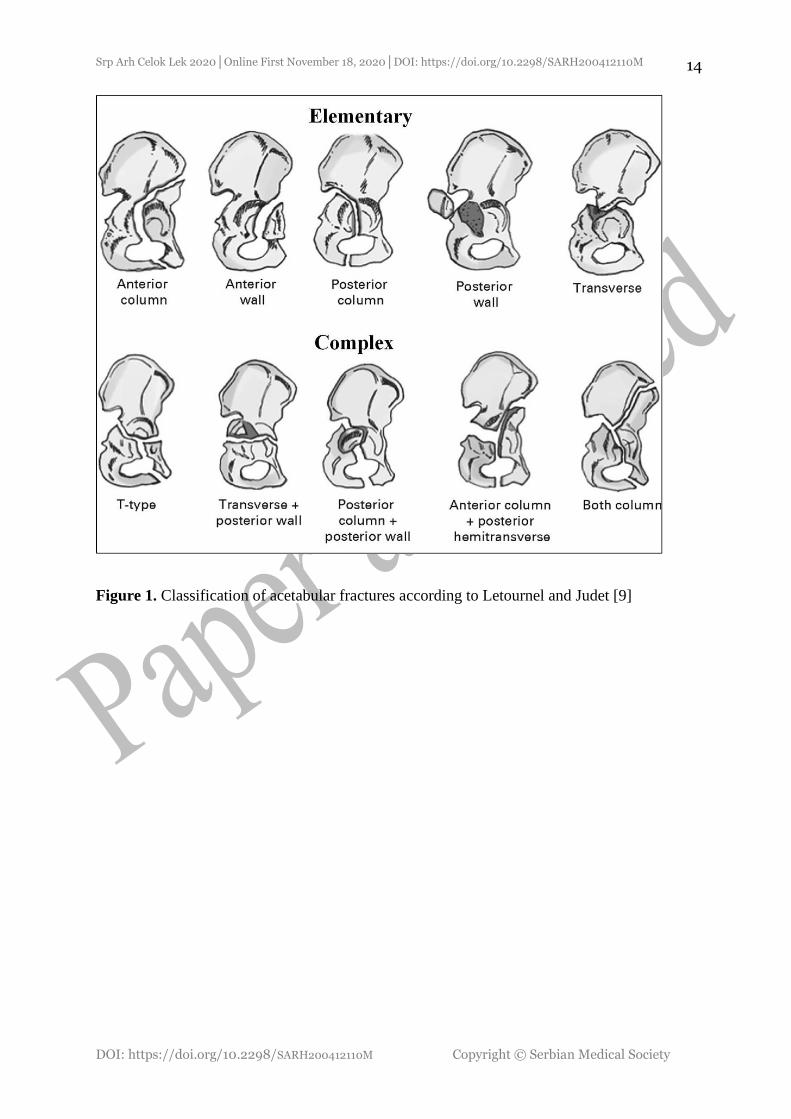
The pioneers of acetabular surgery, Letournel and Judet represented a classification that
stood the test of time, and is still valid and applicable worldwide. According to this
classification, acetabular fractures are divided into elementary and complex [7, 8, 9] (Figure
1).
RADIOLOGIC EVALUATION
Our teachers, our teachers' teachers used clinical examination and radiographic
diagnostics, which included radiography in the AP position and two oblique Judet views
(iliac oblique and obturator oblique). These three projections were sufficient for the
experienced surgeon to evaluate the stability of the fracture and determine the surgical
approach during surgical treatment. Modern diagnostics in the form of CT and 3D- CT allows
the surgeon to see a clear three- dimensional image of the acetabulum that will determine
type of surgical approach, allows him to see the size of the bone fragments, the degree of
dislocation, comminution, impaction, the presence of loose bodies in the acetabulum [10, 11].

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
5
TREATMENT OF ACETABULAR FRACTURE
Undislocated (≤2mm), stable acetabular fractures can be treated conservatively. The
question is, whether skeletal traction is required in this treatment? The authors believe that
skeletal traction is not necessary in undislocated acetabular fractures, the patient can walk
without weight- bearing for 6-8 weeks. Partial to full weight- bearing is allowed after this
period, with rehabilitation. In patients with dislocated fractures who cannot undergo surgical
treatment, closed reduction via skeletal traction with bed rest for the initial 6 to 8 weeks may
be used. Dislocated (≥ 2mm), and unstable acetabular fractures are treated surgically- by open
reduction and stable internal fixation, or by percutaneous minimally invasive surgery which
require experience and intraoperative fluoroscopy. In order to achieve satisfactory functional
and radiographic results, it is necessary to achieve acetabular congruence and anatomic
reduction, stable internal fixation. Early activation and rehabilitation is required, without
weight-bearing from 6 to 8 weeks after surgery, when partial weight- bearing begins to
increase and progressively increases over the next few weeks, until full weight- bearing is
achieved [6, 12, 13, 14]. The most common surgical approaches used for surgical open
reduction and internal fixation are anterior Ilio-Inguinal, anterior Ilio-Femoral, posterior
Kocher-Langenbeck, combined- anterior and posterior, modified Stoppa, anterior pararectal
surgical approach (Figure 2-5). Understanding of these surgical approaches requires training,
continuous education and raises the question of the existence of a national educational center,
because, regardless of the number of orthopedic surgeons, there are very few who are familiar
with this pathology.
PRIMARY TOTAL HIP REPLACEMENT AFTER ACETABULAR
FRACTURE
There is much controversy regarding primary total hip replacement in fresh acetabular
fractures. The issue of "fixed or replaced" is always the question, especially in older patients.
In any case, primary total hip replacement is used in the treatment of fresh acetabular
fractures, and numerous complications that accompany this surgery are described. Indications

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
6
are set on a case-by-case basis and recommended for individually selected cases [15, 16, 17]
(Figure 6).
COMPLICATIONS AFTER ACETABULAR SURGERY
Based on clinical practice and contemporary literature, the most common complications
accompanying the surgical treatment of acetabular fractures are: traumatic and iatrogenic
sciatic nerve palsy, thromboembolic complications (DVT) and pulmonary thromboembolism
(PE), infection, loss of osteosynthesis after surgical fixation of the fracture, heterotopic
ossification (HO), femoral head osteonecrosis, secondary osteoarthritis of the hip (OA) [4, 6,
18, 19].
TRAUMATIC AND IATROGENIC SCIATIC NERVE PALSY
Contemporary literature describes traumatic and iatrogenic sciatic nerve palsy or its
peroneal division [20, 21]. The injuries of the peroneal division of the sciatic nerve are most
common. These injuries are more common in the posterior hip dislocation associated with
acetabular fracture, caused by the pressure of the dislocated femoral head or the pressure of
the bone fragment from the posterior wall of the acetabulum at the time of injury. According
to Bogdan et al., out of 137 patients with acetabular fractures, 57% had traumatic nerve injury
[22]. Immediate reduction of dislocated hip and early fixation of the acetabulum reduce
pressure on the nerve and allow better functional recovery of the nerve. In addition to the
traumatic lesion, iatrogenic injuries to the sciatic nerve have also been described. Iatrogenic
injury can be caused by rough surgical work, manipulations during surgery, careless handling
of elevators and retractors, the presence of a postoperative hematoma. In order to prevent
iatrogenic injury to the sciatic nerve, knee flexion during surgery is necessary to relieve the
nerve, clear identification and protection of the nerve during surgery, special attention should
be paid to the presence of possible anatomic variations of the sciatic nerve (Figure 7),
postoperative drainage is required. Haidukewych et al., reported incidence of 7.9% of
iatrogenic sciatic nerve injuries after acetabular surgery [23].

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
7
THROMBOEMBOLIC COMPLICATIONS (DVT) AND PULMONARY
THROMBOEMBOLISM (PE)
Post- traumatic and postoperative thromboemolism is a significant problem in patients
with acetabular fractures. These complications accompany acetabular surgery despite
thromboprophylaxis, especially in elderly patients over 60 years of age, patients with
increased risk for DVT, complex fractures, and delayed osteosynthesis of acetabular fractures
after two weeks [24]. According to Wang, in a series of 110 patients with pelvic and
acetabular fractures, 29.09% had DVT, 3 patients had PE [25]. In addition, the incidence of
DVT in patients with acetabular fractures was significantly higher than that of patients with
pelvic fractures According to Althuwaykh et al., the incidence in a series of 404 patients with
acetabular fracture was 5%, while PE had 1.7% patients [26]. Despite the prophylaxis, the
prevalence of post- traumatic and postoperative thromboembolism is approximately 11%
[27].
INFECTIONS AND REVISION SURGERY
Early revision surgery is rarely used in cases of loss of fixation or surgical debridement
and irrigation in early infections after osteosynthesis of acetabular fractures. Infections,
superficial or deep, are rare due to good vascularization but are present and should be
considered. Postoperatively, antibiotic prophylaxis is required until postoperative drainage is
extracted. According to Ding et al., 7% of patients required revision surgery due to
debridement and irrigation after wound infection, according to Iqbal et al., 5.4%. required
revision [28, 29]. Similar data was reported by Suzuki et al. [30]. According to Negrin and
Seligson revision surgery due to secondary loss of reduction, seroma / hematoma, and wound
infection was in 6.0% [31]. According to Giannoudis et al., the incidence of infection after
surgical treatment of acetabular fractures was 4.4% [32].

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
8
HETEROTOPIC OSSIFICATION
Heterotopic ossification (HO) is also clearly described and it accompanies this type of
surgery [33]. In many centers, indomethacin or low- dose radiotherapy is administered as
prophylaxis to prevent the development of HO [34]. In Giannoudis' meta- analysis of 2394
displaced fractures, the HO incidence was 25.6% with Brooker grade III or IV at 5.7% [32].
FEMORAL HEAD OSTEONECROSIS
This complication can occur several months to several years after acetabular fracture.
As a result of the femoral head osteonecrosis, fragmentation and collapse of the femoral head
can occur, which will cause secondary osteoarthristis of the hip (OA). Although it is
sometimes difficult to differentiate diagnostically the osteoarthristis and osteonecrosis, it is
not uncommon to see both intraoperatively. Different authors describe the different incidence
of the femoral head osteonecrosis. According to Pavelka et al. , 11.7% of patients developed
of the femoral head osteonecrosis [35]. The fact is that the femoral head osteonecrosisis much
more common in acetabular fractures that are associated with posterior hip dislocation [36].
According to Giannoudis et al, the incidence of osteonecrosis was 5.6%. According to the
same authors, the incidence of osteonecrosis after acetabular fracture was 5%, and for
acetabular fractures associated with posterior hip dislocation it was 9.2% [32]. Posterior hip
dislocation is an orthopaedic emergency and therefore any dislocated hip should be reducted
emergency after hospitalization. A number of authors show the importance of urgent
reduction of the dislocated hip in the prevention of the femoral head osteonecrosis [37–40].
Late reduction after 24 hours from the injury increases the possibility of osteonecrosis.
According to one of our studies, the incidence of the femoral head osteonecrosis after
acetabular fracture- dislocations in which the hip was reducted within 24 h of injury was
5.55%, while in hip reducted in a time interval after 24 h of injury, osteonecrosis was 27.77%
[41].
Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
9
SECONDARY OSTEOARTHRITIS OF THE HIP (OA)
The occurrence of secondary osteoarthritis of the hip (OA) is associated with a non-
anatomical reduction of the acetabular fracture during definitive fixation. The literature
describes a significantly lower percentage of secondary osteoarthritis of the hip (OA) in
anatomically reducted acetabular fractures [42]. Secondary osteoarthritis of the hip (OA)
accompanies acetabular fractures and is usually associated with non- anatomical fracture
reduction. Meena et al. published that does not achieving anatomical reduction, associated
injuries, initial fracture dislocation (> 20mm), posterior hip dislocation, late definitive
fixation of acetabulum, age, can negatively affect the achievement of good outcome [43].
According to Matta, the number of anatomic reductions decreased as time to surgery
increased [44]. Pascarella et al., also describe the importance of anatomic reduction of
acetabular fractures in achieving excellent and good outcomes [40]. Pavelka et al., published
32.81% secondary osteoarthritis of the hip (OA), 24 months after acetabular fracture [35].
Cahueque et al., published 48% secondary osteoarthritis (OA), after 2 years from the
acetabular fracture [45]. There are other authors who believe that secondary osteoarthritis
(OA) occurs several years after the injury, despite anatomic reduction, which only confirms
the importance and severity of the acetabular fracture and the anatomical specificity of the
acetabulum and hip joint [46] (Figure 8). Some of the cases with secondary osteoarthritis of
the hip (OA), require further surgery- total hip replacement [5, 47].
TIME OF DEFINITIVE ACETABULAR FIXATION
Numerous authors agree that the time interval from injury to definitive acetabular
fixation should not be longer than 7 days, preferably 3 to 5 days. Dailey et al., achieved the
best anatomic reduction of acetabular fracture in the first 3 days after the fracture [42].
According to Brueton, the timing of surgery was found to be directly related to the quality of
the clinical result [48]. Similar results are presented by Matta et al. [44]. With the delay of
definitive acetabular surgery, the possibility of anatomic reduction is reduced. Definitive
osteosynthesis after two to three weeks of fracture impairs fracture reduction, increases
intraoperative bleeding, which adversely affects surgical work. In clinical practice, there are
also individual cases with acetabular fracture associated with posterior hip dislocation when

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
10
definitive acetabular fixation is performed within 24 hours after the injury, due to the need for
open reduction of the hip that couldn't have been reducted by the closed method (Figure 9).
SURGICAL EXPERIENCE
Surgical experience, reflected primarily in the manual ability and familiarity of the
surgeon with a certain surgical problem, is an important prerequisite for success. In
acetabular surgery, surgical experience is of great importance. Surgical experience is one of
the preconditions for successful treatment of acetabular fractures. In order to acquire
knowledge and necessary skills in this field of traumatology, it is necessary to have a national
education center at one of the Medical Faculties in Serbia. The literature clearly indicates the
importance of surgical experience in the treatment of acetabular fractures [7]. Even though
we have a sufficient number of orthopaedic surgeons in Serbia, we unfortunately have a small
number of surgeons who have experience in this field of traumatology. So far, this experience
has been gained abroad in large trauma centers under the guidance of experts. Although rare,
acetabular fractures are present in our traumatology practice. It matters whether the patient
will return to pre- operative activity after the acetabular fracture, or whether the acetabular
fracture will leave lasting consequences and disability.
CONCLUSION
Proper diagnosis of acetabular fractures, good knowledge of the acetabular anatomy,
experience of the surgeon, early definitive acetabular osteosynthesis, anatomic reduction and
early rehabilitation are only prerequisites for achieving excellent and good outcomes.
Whether we will have excellent or good outcomes depends on the initial trauma that caused
the damage. Damage is often inevitable, and whether it will be less or greater, it may also
depend on ourselves who deal with this segment of traumatology. We have achieved a lot in
acetabular surgery, but still not enough to say that we are in step with the developed world.
Including more of surgeons in our institutions, who will deal with acetabular surgery,
education and training, the existence of a national education center that will have the
Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
11
opportunity to educate on cadavers are necessary if we want to advance this demanding area
of traumatology – pelvic and acetabular surgery.
ACKNOWLEDGEMENT
This research was supported by the University of Niš, Faculty of Medicine, internal
project No. 64, titled “Total hip arthroplasty after earlier acetabular fractures.”
Conflict of interest: None declared.

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
12
REFERENCES
1. Letournel E, Judet R. Fracture of the acetabulum. 2nd edition. Berlin: Springer-Verlag; 1993.
2. Dakin GJ, Eberhardt AW, Alonso JE, Stannard JP, Mann KA. Acetabular fracture patterns: Associations with
motor vehicle crash information. J Trauma. 1999; 47(6): 1063- 1071. doi: 10.1097/00005373-199912000-00012
3. Laird A, Keating JF. Acetabular fractures: A 16-year prospective epidemiological study. J Bone Joint Surg Br.
2005; 87(7):969- 973. doi: 10.1302/0301-620X.87B7.16017
4. Milenković S. Pelvic and acetabular fractures. Monography. Medical faculty of Nis: Nis; 2018. ISBN 978-86-
6265-042-9
5. Milenkovic S, Mitkovic M, Mitkovic M, Stojiljkovic P. Total hip arthroplasty after acetabular fracture surgery.
Int Orthop. 2020. doi: 10.1007/s00264-020-04676-w
6. Ziran N, Soles GLS, Matta JM. Outcomes after surgical treatment of acetabular fractures: a review. Patient Saf
Surg. 2019;13:16. doi:10.1186/s13037-019-0196-2
7. Alton TB, Gee AO. Classifications in brief: Letournel classification for acetabular fractures. Clin Orthop Relat
Res. 2014; 472(1): 35- 38. doi:10.1007/s11999-013-3375-y
8. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open
reduction. Preliminary report. J Bone Joint Surg Am. 1964; 46- A: 1615- 1646. PMID: 14239854
9. Hutt JRB, Ortega-Briones A, Daurka JS, Bircher MD, Rickman MS.. The ongoing relevance of acetabular
fracture classification. Bone Joint J. 2015; 97 (8): 1139- 1143. doi: 10.1302/0301-620X.97B8.33653
10. Lawrence DA, Menn K, Baumgaertner M, Haims MA. Acetabular fractures: Anatomic and clinical
considerations. American Journal of Roentgenology. 2013; 201( 3): 425- 436. doi:10.2214/AJR.12.10470
11. Scheinfeld MH, Dym AA, Spektor M, Avery LL, Dym RJ, Amanatullah DF. Acetabular fractures: What
Radiologists should know and how 3D CT can aid classification. RadioGraphics 2015; 35:555- 577. doi:
10.1148/rg.352140098
12. Milenkovic S. Elementary acetabular fractures- Our experiences. 4th Congress of North Macedonian Association
of Orthopadics and Traumatologists (MADOT 2018); Abstract book: 42. Ohrid- North Macedonia. 2018.
13. Milenkovic S, Saveski J, Radenkovic M, Vidic G,Trajkovska N. Surgical treatment of displaced acetabular
fractures. Srp Arh Celok Lek. 2011; 139 (7-8): 496-500. doi: 10.2298/SARH1108496M
14. Milenković S, Mitković M, Radenković M, Mladenović D, Micić I. Surgical treatment of the posterior wall
acetabular fractures. Third Congress of Serbian Trauma Association (STA); Abstract book: 119. Zlatibor. 2012.
15. Mears DC, Velyvis JH. Acute total hip arthroplasty for selected displaced acetabular fractures: Two to twelve-
year results. J Bone Joint Surg Am. 2002; 84 (1):1-9. doi: 10.2106/00004623-200201000-00001
16. Iqbal F, Ullah A, Younus S, Aliuddin A, Zia OB, Khan N. Functional outcome of acute primary total hip
replacement after complex acetabular fractures. Eur J Orthop Surg Traumatol. 2018; 28 (8):1609- 1616. doi:
10.1007/s00590-018-2230-y.
17. Malhotra R, Gautam D. Acute total hip arthroplasty in acetabular fractures using modern porous metal cup. J
Orthop Surg (Hong Kong). 2019 ; 27 (2): 2309499019855438. doi: 10.1177/2309499019855438.
18. Milenkovic S. Acetabular fractures- our experience, results and complications. First Congrres of the Association
of Orthopaedics and Traumatologists of Montenegro (AMOT) with international participation; Abstract book:
103. Bečici- Montenegro. 2019. ISBN 978-9940-9972-0-5
19. Milenkovic S, Mitkovic M, Mitkovic M. Complications after posterior wall fractures of the acetabulum. VIth
Congress of Serbian Trauma Association (STA). Invited Lecturer; Abstract book: 56- 62.Vrnjačka Banja. 2020.
20. Lehmann W, Hoffmann M, Fensky F, Nüchtern J, Großterlinden L, Aghayev E, Lehmann H, Stuby F, Rueger
JM. What is the frequency of nerve injuries associated with acetabular fractures? Clin Orthop Relat Res. 2014;
472 (11): 3395- 3403. doi: 10.1007/s11999-014-3838-9
21. Issack PS, Helfet DL. Sciatic nerve injury associated with acetabular fractures. HSS J. 2009; (1): 12- 18. doi:
10.1007/s11420-008-9099-y
22. Bogdan Y, Tornetta P3rd, Jones C, Gilde A, Schemitsch E, Vicente M, Horwitz D, Sanders D, Firoozabadi R,
Leighton R, Robinson J, Marcantonio A, Hamilton B. Neurologic injury in operatively treated acetabular
Fractures. J Orthop Trauma. 2015; 29 (10): 475- 478. doi: 10.1097/BOT.0000000000000362
23. Haidukewych GJ, Scaduto J, Herscovici DJr, Sanders RW, Di Pasquale T. Iatrogenic nerve injury in acetabular
fracture surgery: A comparison of monitored and unmonitored procedures. J Orthop Trauma. 2002; 16 (5): 297-
301. doi: 10.1097/00005131-200205000-00002
24. El-Daly, I, Reidy, J, Culpan, P, Bates P. Thromboprophylaxis in patients with pelvic and acetabular fractures: a
short review and recommendations. Injury 2013; 44: 1710- 1720. doi: 10.1016/j.injury.2013.04.030
25. Wang P, Kandemir U, Zhang B, Wang B, Li J, Zhuang Y, Wang H, Zhang H, Liu P, Zhang K. Incidence and
risk factors of deep vein thrombosis in patients with pelvic and acetabular fractures. Clin Appl Thromb Hemost.
2019; 25: 1076029619845066. doi: 10.1177/1076029619845066

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
13
26. Althuwaykh SH, Alnasser AM, Khubrani AM, Alamari ZS, Aljuhani WS. Prevalence of venous
thromboembolism in patients with acetabular or hip fractures and their association with hemoglobin
concentration. J Musculoskelet Surg Res. 2020; 4(1): 21- 24. doi: 10.4103/jmsr.jmsr_86_19
27. Stannard JP, Singhania AK, Lopez- Ben RR, Anderson ER, Farris RC, Volgas DA, McGvin JrGR, Alonso JE.
Deep- vein thrombosis in high- energy skeletal trauma despite thromboprophylaxis. J Bone Joint Surg Br. 2005;
87 (7): 965- 968. doi: 10.1302/0301-620X.87B7.15989
28. Ding A , OʼToole VR, Castillo R, Reahl B, Montalvo R , Nascone WJ , Sciadini FM , Carlini RA , Manson TT.
Risk factors for early reoperation after operative treatment of acetabular fractures. J Orthop Trauma. 2018;
32(7): 251- 257. doi: 10.1097/BOT.0000000000001163
29. Iqbal F,Younus S, Asmatullah, Bin Zia O, Khan N. Surgical site infection following fixation of acetabular
fractures. Hip Pelvis. 2017; 29(3): 176- 181.
doi: 10.5371/hp.2017.29.3.176 176
30. Suzuki T, Morgan SJ, Smith WR, Stahel PF, Gillani SA, Hak DJ. Postoperative surgical site infection following
acetabular fracture fixation. Injury.2010; 41:396- 399. doi: 10.1016/j.injury.2009.11.005
31. Negrin L, Seligson D. Results of 167 consecutive cases of acetabular fractures using the Kocher- Langenbeck
approach: a case series. J Orthop Surg Res. 2017; 12(1): 66. doi: 10.1186/s13018-017-0563-6
32. Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the
acetabulum. A meta-analysis. J Bone Joint Surg Br. 2005; 87(1):2-9. PMID: 15686228
33. Firoozabadi R, Alton T, Sagi HC. Heterotopic ossification in acetabular fracture surgery. J Am Acad Orthop
Surg. 2017; 25 (2): 117- 124. doi: 10.5435/JAAOS-D-15-00366
34. Baschera, D, Rad H, Collopy D, Zellweger R. Incidence and clinical relevance of heterotopic ossification after
internal fixation of acetabular fractures: retrospective cohort and case control study. J Orthop Surg Res. 2015;
10: 60. doi: 10.1186/s13018-015-0202-z
35. Pavelka T, Salášek M, Bárta P, Fridrich F, Džupa V. Avascular necrosis of femoral head and coxarthrosis
progression after acetabular fractures. Acta Chir Orthop Traumatol Cech. 2019; 86 (6): 381- 389. PMID:
31941564
36. Milenkovic SS, Mitkovic MM, Mitkovic BM. Avascular necrosis of the femoral head after traumatic posterior
hip dislocation with and without acetabular fracture. Eur J Trauma Emerg Surg. On line september 2020. doi:
10.1007/s00068-020-01495-x
37. Hougaard K, Thomsen PB. Traumatic posterior dislocation of the hip- prognostic factors influencing the
incidence of avascular necrosis of the femoral head. Arch Orthop Trauma Surg. 1986; 106(1): 32-35. doi:
10.1007/BF00435649
38. Ahmed G, Shiraz S, Riaz M, Ibrahim T. Late versus early reduction in traumatic hip dislocations: A meta-
analysis. Eur J Orthop Surg Traumatol. 2017; 27 (8), 1109-1116. doi: 10.1007/s00590-017-1988-7
39. Kellam P, Ostrum RF. Systematic review and meta- analysis of avascular necrosis and posttraumatic arthritis
after traumatic hip dislocation. J Orthop Trauma. 2016; 30(1):10-16. doi: 10.1097/BOT.0000000000000419
40. Pascarella R, Cerbasi S, Politano R, Balato B, Fantasia R, Orabona G, Massimo Mariconda M. Surgical results
and factors influencing outcome in patients with posterior wall acetabular fracture. Injury. 2017; 48 (87): 1819-
1824. doi:10.1016/j.injury.2017.05.039
41. Milenković S, Mitković M, Saveski J, Micić I, Stojiljković P, Stanojković M, Mitković M, Stamenić S, Spalević
M. Avascular necrosis of the femoral head in the patients with posterior wall acetabular fractures associated
with dislocations of the hip. Acta Chir Iugosl. 2013; 60 (2): 65- 69. doi: 10.2298/aci1302065m.
42. Dailey SK, Phillips CT, Radley JM, Archdeacon MT. Achieving anatomic acetabular fracture reduction-When
is the best time to operate? J Orthop Trauma. 2016; 30 (8): 426- 431. doi: 10.1097/BOT.0000000000000576
43. Meena UK, Tripathy SK, Sen RK, Aggarwal S, Behera P. Predictors of postoperative outcome for acetabular
fractures. Orthop Traumatol Surg Res. 2013; 99(8): 929-935. doi: 10.1016/j.otsr.2013.09.004
44. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed
operatively within three weeks after the injury. J Bone Joint Surg Am. 1996; 78-A(11):1632- 1645. PMID:
8934477
45. Cahueque M, Martínez M, Cobar A, Bregni M. Early reduction of acetabular fractures decrease the risk of post-
traumatic hip osteoarthritis? Journal of Clinical Orthopaedics and Trauma. 2017; 8(4): 320- 326. doi:
10.1016/j.jcot.2017.01.001
46. Alonso JE, Volgas DA, Giordano V, Stannard JP. A review of the treatment of hip dislocations associated with
acetabular fractures. Clin Orthop Relat Res. 2000; 377: 32- 43. doi: 10.1097/00003086-200008000-00007
47. Milenković S, Mitković M, Mitković M, Sojiljković P. Total hip arthroplasty in treating post-traumatic arthrosis
of the hip after acetabular fracture. Balneoclimatologija. 2017; 41 (2): 202- 205. YU ISSN 0350/5952
48. Brueton RN. A Review of 40 Acetabular Fractures: The importance of early surgery. Injury.1993; 24 (3): 171-
174. doi: 10.1016/0020-1383(93)90285-e
Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
14
Figure 1. Classification of acetabular fractures according to Letournel and Judet [9]
Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
15
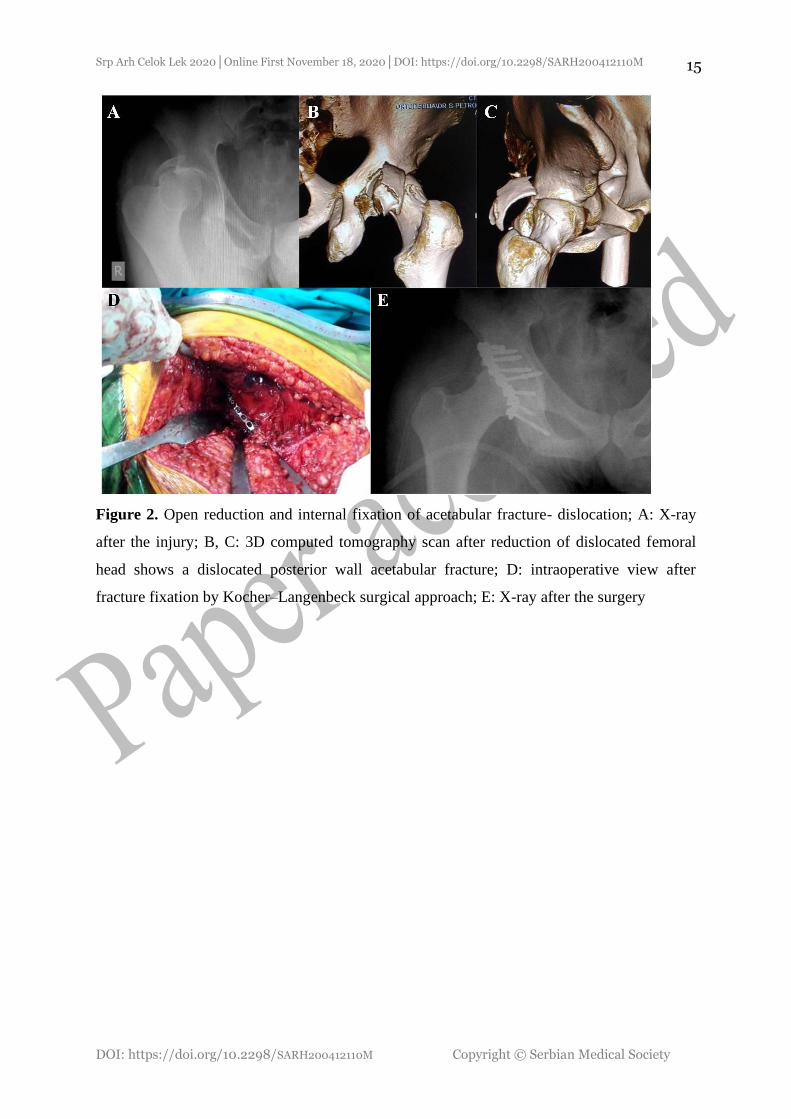
Figure 2. Open reduction and internal fixation of acetabular fracture- dislocation; A: X-ray
after the injury; B, C: 3D computed tomography scan after reduction of dislocated femoral
head shows a dislocated posterior wall acetabular fracture; D: intraoperative view after
fracture fixation by Kocher–Langenbeck surgical approach; E: X-ray after the surgery

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
16
Figure 3. Open reduction and stable internal fixation of acetabular fracture- dislocation; A:
X-ray after the injury; B: 3D computed tomography view shows fracture of the posterior wall
of the acetabulum and posterior hip dislocation; C: sagittal CT view shows posterior
acetabular fracture-dislocation; D: intraoperative view after fracture fixation; E: postoperative
X-ray

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
17
Figure 4. T-fracture of the acetabulum associated with iliac bone fracture in a 20-year-old
patient; A: X-ray after the injury; B: 3D computed tomography view; C, D: intraoperative
views after fracture fixation through the anterior ilio-inguinal surgical approach; E:
intraoperative fluoroscopy; F: postoperative X-ray; G: X-ray six months after the injury; H:
functional outcome, after six months post-injury was excellent

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
18
Figure 5. T-fracture of the acetabulum in a 14-year-old patient; in such fractures, surgical
reduction and fracture fixation is usually performed with a combined anterior and posterior
Kocher-Langenbeck approach in one act or staging surgery at intervals of two to three days;
given the patient’s age and fracture reduction achieved, we used only anterior approach and
further treatment was continued with cutaneous traction for three weeks; A: X-ray after the
injury; B: 3D computed tomography view after the injury; C: X-ray after fracture fixation
through the anterior ilio-inguinal approach; D: X-ray after six months

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
19
Figure 6. Primary total hip replacement after fresh posterior wall acetabular fracture with
posterior hip dislocation in a 74-year-old patient; A: X-ray after the injury; B: 3D computed
tomography view; C: sagittal computed tomography view shows posterior hip dislocation
with a fracture of the posterior wall of the acetabulum; D: X-ray after primary total hip
replacement

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
20
Figure 7. Anatomical variation of the sciatic nerve shows a sciatic nerve high division in the
gluteal region, in a 48-year-old patient with a comminuted posterior wall acetabular fracture
associated with posterior hip dislocation and traumatic palsy of sciatic nerve; A: X-ray after
the injury; B: intraoperative view after acetabular fracture fixation. Arrows show sciatic
nerve high division

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
21
Figure 8. Hip ankylosis in a 73-year-old patient, caused by secondary osteoarthritis of the
hip; the acetabular surgery was done at another institution 39 years previously

Srp Arh Celok Lek 2020│Online First November 18, 2020│DOI: https://doi.org/10.2298/SARH200412110M
DOI: https://doi.org/10.2298/SARH200412110M Copyright © Serbian Medical Society
22
Figure 9. Intraoperative view during the open reduction of dislocated hip in a 55-year-old
patient with the posterior wall acetabular fracture associated with posterior hip dislocation