for inclusion in the who essential medicines list ... · novartis page 3 ranibizumab (lucentis ®)...
TRANSCRIPT
Application for inclusion in the WHO Essential Medicines List Section 21, Ophthalmological Preparations
Ranibizumab (Lucentis®) ‐ Addition
Document type: Application for inclusion in WHO Essential Medicines List
Document status: Final
Release date: 28 November 2014
Property of Novartis

Novartis Page 2 Ranibizumab (Lucentis®)
Table of contents
Table of contents ................................................................................................................. 2
1 Summary statement of the proposal for inclusion, change or deletion ............................... 3
2 Name of the focal point in WHO submitting or supporting the application (where relevant) ............................................................................................................................... 4
3 Name of the organization(s) consulted and/or supporting the application .......................... 4
4 International Nonproprietary Name (INN, generic name) of the medicine ........................ 4
5 Formulation proposed for inclusion; including adult and paediatric (if appropriate) ......... 4
6 International availability – sources, of possible manufacturers and trade names ............... 4
7 Whether listing is requested as an individual medicine or as an example of a therapeutic group ................................................................................................................. 4
8 Information supporting the public health relevance (epidemiological information on disease burden, assessment of current use, target population) ............................................ 5
9 Treatment details (dosage regimen, duration; reference to existing WHO and other clinical guidelines; need for special diagnostics, treatment or monitoring facilities and skills .............................................................................................................................. 7
10 Summary of comparative effectiveness in a variety of clinical settings ............................. 9
Identification of clinical evidence and summary of available data ......................... 9
Summary of available estimates of comparative efectiveness .............................. 22
11 Summary of comparative evidence on safety: ................................................................... 24
Estimate of patient exposure to date ...................................................................... 24
Description of the adverse effects/reactions and estimates of their frequencies ... 24
Summary of comparative safety against comparators ........................................... 26
12 Summary of available data on comparative cost and cost-effectiveness within the pharmacological class or therapeutic group: ..................................................................... 32
Costs of the proposed medicine ............................................................................. 32
Resource use and comparative cost-effectiveness presented as range of cost per routine outcome ............................................................................................... 32
13 Summary of regulatory status of the medicine .................................................................. 33
14 Availability of pharmacopoeial standards (British Pharmacopoeia, International Pharmacopoeia, United States Pharmacopoeia) ................................................................ 34
15 Proposed (new/adapted) text for the WHO Model Formulary .......................................... 34
REFERENCES .................................................................................................................. 43

Novartis Page 3 Ranibizumab (Lucentis®)
1 Summary statement of the proposal for inclusion, change or deletion We propose to include ranibizumab (Lucentis®), a globally licensed anti-neovascularization agent, in the WHO Model Lists of Essential Medicines (EML) for1: the treatment of neovascular (wet) age-related macular degeneration (referred to as
nAMD or wet AMD) the treatment of visual impairment due to diabetic macular edema (DME) the treatment of visual impairment due to macular edema secondary to branch retinal
vein occlusion (BRVO) the treatment of visual impairment due to macular edema secondary to central retinal
vein occlusion (CRVO) the treatment of visual impairment due to choroidal neovascularization (CNV) secondary
to pathologic myopia (PM) (mCNV) Ranibizumab (marketed under the trade name Lucentis®) is the standard-of-care first-line therapy in these conditions and licensed in more than 100 countries for the treatment of nAMD, visual impairment due to DME and for visual impairment due to macular edema secondary to BRVO and CRVO. Also, ranibizumab is licensed in more than 80 countries for the treatment of patients with visual impairment due to myopic CNV. Genentech Inc. holds the development and commercialization rights for Lucentis in the US and is the license holder and manufacturer in the US. Novartis Pharma AG and its worldwide affiliates hold the development and commercialization rights for Lucentis outside the US. Ranibizumab is the first anti-VEGF agent that has demonstrated efficacy and a positive benefit-risk ratio in high quality, randomized clinical trials for each of the above indications. Ranibizumab has a well-established safety profile supported by more than 40 clinical studies and long term global real-world experience, including a dedicated Risk Management Plan and mandatory continuous safety monitoring for the approved ocular indications. Its safety profile has been well established in a clinical development program that enrolled more than 19,700 patients across indications and there are more than 3 million patient-treatment years of exposure globally since its launch in the United States in 20062. Ranibizumab is manufactured to the standards for intra-ocular (intravitreal) use3. Each therapeutic dose is filled in vials, or prefilled syringes, intended for single use and complies with US Pharmacopeia (USP 789) specific requirements for ophthalmic solutions, which are stricter than for parenteral (i.e. intravenous) products. Single use containers reduce the risks associated with compounding. Ranibizumab is an antibody fragment and devoid of the Fc portion present in anti-VEGF therapies used systemically. The lack of the Fc portion results in shorter serum half-life (2h) as Fc-receptor-mediated recycling into the bloodstream is abolished. As a result, the potential for systemic adverse events of ranibizumab is minimized4. Both bevacizumab (unlicensed for ocular use) and aflibercept (licensed for ocular use) have been developed for systemic application and correspondingly contain an Fc portion. Based on the proven efficacy in eye diseases which have the potential to cause severe loss of visual acuity, and may ultimately lead to blindness, and based on a well-characterized

Novartis Page 4 Ranibizumab (Lucentis®)
safety profile, we suggest the addition of the globally licensed ranibizumab solution for injection to the WHO's list of essential eye medicines.
2 Name of the focal point in WHO submitting or supporting the application (where relevant)
The application is being submitted by Novartis Pharma AG.
3 Name of the organization(s) consulted and/or supporting the application To be announced.
4 International Nonproprietary Name (INN, generic name) of the medicine Ranibizumab
5 Formulation proposed for inclusion; including adult and paediatric (if appropriate)
Ranibizumab 10 mg/ml solution for injection
6 International availability – sources, of possible manufacturers and trade names
Trade name: Lucentis® Ranibizumab is licensed and available in more than 100 countries for the treatment of nAMD, visual impairment due to DME and for visual impairment due to macular edema secondary to BRVO and CRVO. Also, more recently, ranibizumab is licensed in more than 80 countries for the treatment of patients with visual impairment due to myopic CNV, including the EU and Switzerland. Genentech Inc. holds the development and commercialization rights for in the US and is the license holder and manufacturer in the US. Novartis Pharma AG and its worldwide affiliates hold the development and commercialization rights for Lucentis outside the US and together are the license holder and manufacturer in these countries2.
7 Whether listing is requested as an individual medicine or as an example of a therapeutic group
Individual Medicine

Novartis Page 5 Ranibizumab (Lucentis®)
8 Information supporting the public health relevance (epidemiological information on disease burden, assessment of current use, target population)
Neovascular AMD Neovascular AMD (nAMD) is the leading cause of severe loss of visual acuity among the elderly population, affecting 30-50 million people worldwide1. Genetic, environmental and health factors play an important role in the pathogenesis of the disease. Among the clinical features, the cumulative deposition of acellular, polymorphous debris, known as drusen, between the retinal pigment epithelium and Bruch’s membrane at the central region of the macula is considered a main predictor of the establishment of a progressive and degenerative process, in which an advanced AMD, defined as the presence of choroidal neovascularization (CNV), can be the final result5. As a result of the increased life expectancy and growth of the elderly population, the cases of nAMD are expected to increase by at least 50% by the year 20206, 7. While nAMD may increase, the Beaver Dam Eye Study (BDES) and the Blue Mountain Eye Study (BMES) have shown that the incidence of visual impairment has reduced by almost 50% in 2008 compared to 2005 and earlier8. Reductions have also been observed when comparing similar age groups over time: the prevalence of visual impairment for persons aged 75 to 79 reduced from 6.2% those for those born between 1915 and 1919 to 3.0% for those born between 1930 and 1934. Similar reductions were seen in older age groups9. These reductions are mainly the reduction in cases of visual impairment in nAMD, which shows the effectiveness of current treatment options, with ranibizumab being the most important approved product, in reducing the cases of visual impairment and blindness. DME Diabetic macular edema (DME) describes the accumulation of fluid in the intraretinal layers of the macula as a result of leakage from the retinal microvasculature. DME can arise during the course of diabetic retinopathy – a chronic microvascular complication of Type 1 or Type 2 diabetes mellitus – and is a leading cause of visual impairment in the diabetic population10. The prevalence of visual impairment due to DME varies according to the type and duration of diabetes; as such, there is a wide range of prevalence estimates relating to these conditions. Overall, analysis of the literature suggests that in patients with diabetes, the prevalence rate of clinical significant DME is approximately 6-10%, with visual impairment due to DME affecting a small proportion (approximately 1-3%) of the diabetic population11. RVO Retinal vein occlusion (RVO) describes the narrowing or blockage of a retinal vein, the origins of which are multifactorial. In general, RVO presents with variable degrees of visual loss with any combination of fundal findings consisting of retinal vascular tortuosity, retinal hemorrhages, cotton wool spots, optic disc swelling and macular edema12. RVO is classified by the site of the venous occlusion as either branch RVO (BRVO), where a branch retinal vein is occluded, central RVO (CRVO), where the central retinal vein is occluded, or hemiretinal RVO, in which one or two of the trunks of the central retinal vein are occluded13.

Novartis Page 6 Ranibizumab (Lucentis®)
RVO is the second most frequent retinal disorder after diabetic retinopathy14. Based on a meta-analysis of 15 studies conducted in the US, Europe, Asia and Australia, the overall prevalence of RVO has been estimated to be approximately 0.52 cases per 100 individuals, although estimates from individual studies vary due to different sample sizes and study methodologies15. BRVO occurs more frequently than CRVO. The overall prevalence of BRVO has been estimated to be approximately 0.44 cases per 100 individuals, compared with 0.08 cases per 100 individuals for CRVO. Based on these estimates, approximately 16.4 million adults are affected worldwide, with 13.9 million having BRVO and 2.5 million having CRVO. The annual incidences of BRVO and CRVO are 0.12% and 0.03-0.04%, respectively16, 17, 18. PM Pathological myopia (PM) is a leading cause of vision loss, especially in a younger population (<50 years of age) and is ranked as one of the major causes of legal blindness in several countries19- 24. Pathologic myopia encompasses the condition of the abnormal elongation of the axial length of the eyeball (more than 26 mm) associated with high myopia refractive errors (usually greater than 6.0 diopters [D]) and clinic-anatomical characteristics mostly represented by changes of the posterior pole of the eye such as posterior staphyloma, atrophy of the retinal pigment epithelium (RPE), Bruch’s membrane cracks, subretinal hemorrhage, retinal detachment, and the one considered most vision threatening complication in patients with PM, CNV (Miller et al, 2001; Pruett, 1994). The stretching of the retina and thinning of the choroid is considered the key pathway leading to CNV formation, by way of increasing the probability of choroidal ischemia and subsequent atrophy of the adjacent RPE. These alterations are then closely associated with the break of Bruch’s membrane (“lacquer cracks”), the main predisposing feature for new vessels formation and growth into the subretinal space25, 26. The association of an axial length greater than 26.5 mm with a high myopic refractive error increases the probability of developing CNV from 5% to nearly 10% of the patients with associated myopic retinal changes, on average, over 10 years25, 27. Ultimately, the development of CNV leads to the visual impairment that these patients experience. The prevalence of CNV in patients with PM is high in patients under the age of 50 years; thus, due to the occurrence of this pathology at a young age, this condition has a profound impact on patients’ lives, also affecting the productivity of this working age group28, despite being a less prevalent disease than nAMD. Ranibizumab is the first licensed drug to date that has demonstrated efficacy in high quality, randomized clinical trials for each of the above indications and for which Health Authorities concluded on a positive benefit-risk ratio. The safety profile for all indications is well established. In clinical studies (including ANCHOR, MARINA, RESTORE, BRAVO, and CRUISE and RADIANCE), patients with nAMD, DME, BRVO, CRVO and myopic CNV treated with ranibizumab had a marked improvement in their independence (vision-related quality of life). Improvement was reported in near-vision activities (e.g. reading and cooking), distance activities (e.g. reading street signs and going up and down stairs at night) and vision-specific dependency (e.g. not having to stay at home most of the time)29- 35.

Novartis Page 7 Ranibizumab (Lucentis®)
9 Treatment details (dosage regimen, duration; reference to existing WHO and other clinical guidelines; need for special diagnostics, treatment or monitoring facilities and skills
Below, the EU and US approved ranibizumab posology is provided per indication. There are differences in the respective recommendations and we are proposing to adopt the EU SmPC posology as it enables as needed, individualized treatment of patients and avoids undertreatment of patients resulting in potential sub-standard outcomes for patients or overtreatment of patients who do not need frequent injections, as well as being more cost-effective when compared to monthly dosing. Additionally, individualized treatment of patients is used in clinical standard practice in the majority of countries outside the US and therefore more accurately reflects the standard of care36. Posology Ranibizumab must be administered by a qualified ophthalmologist experienced in intravitreal injections.
EU SmPC (Sep 2014)1 US Prescribing Information (Oct 2014)1 The recommended dose for Lucentis is 0.5 mg given as a single intravitreal injection. This corresponds to an injection volume of 0.05 ml. The interval between two doses injected into the same eye should be at least four weeks. Treatment is initiated with one injection per month until maximum visual acuity is achieved and/or there are no signs of disease activity i.e. no change in visual acuity and in other signs and symptoms of the disease under continued treatment. In patients with wet AMD, DME and RVO, initially, three or more consecutive, monthly injections may be needed. Thereafter, monitoring and treatment intervals should be determined by the physician and should be based on disease activity, as assessed by visual acuity and/or anatomical parameters. If, in the physician’s opinion, visual and anatomic parameters indicate that the patient is not benefiting from continued treatment, Lucentis should be discontinued. Monitoring for disease activity may include clinical examination, functional testing or imaging techniques (e.g. optical coherence
2.2 Neovascular (Wet) Age-Related Macular Degeneration (AMD) LUCENTIS 0.5 mg (0.05 mL of 10 mg/mL LUCENTIS solution) is recommended to be administered by intravitreal injection once a month (approximately 28 days). Although not as effective, patients may be treated with 3 monthly doses followed by less frequent dosing with regular assessment. In the nine months after 3 initial monthly doses, less frequent dosing with 4-5 doses on average is expected to maintain visual acuity while monthly dosing may be expected to result in an additional average 1-2 letter gain. Patients should be assessed regularly. Although not as effective, patients may also be treated with one dose every 3 months after 4 monthly doses. Compared with continued monthly dosing, dosing every 3 months over the next 9 months will lead to an approximate 5-letter (1-line) loss of visual acuity benefit, on average. Patients should be assessed regularly. 2.3 Macular Edema Following Retinal Vein Occlusion (RVO) LUCENTIS 0.5 mg (0.05 mL of 10 mg/mL LUCENTIS solution) is recommended to be administered by intravitreal injection once a

Novartis Page 8 Ranibizumab (Lucentis®)
tomography or fluorescein angiography). If patients are being treated according to a treat-and-extend regimen, once maximum visual acuity is achieved and/or there are no signs of disease activity, the treatment intervals can be extended stepwise until signs of disease activity or visual impairment recur. The treatment interval should be extended by no more than two weeks at a time for wet AMD and may be extended by up to one month at a time for DME. For RVO, treatment intervals may also be gradually extended, however there are insufficient data to conclude on the length of these intervals. If disease activity recurs, the treatment interval should be shortened accordingly. In the treatment of visual impairment due to CNV secondary to PM, many patients may only need one or two injections during the first year, while some patients may need more frequent treatment (see section 5.1). Lucentis and laser photocoagulation in DME and in macular oedema secondary to BRVO There is some experience of Lucentis administered concomitantly with laser photocoagulation (see section 5.1). When given on the same day, Lucentis should be administered at least 30 minutes after laser photocoagulation. Lucentis can be administered in patients who have received previous laser photocoagulation. Lucentis and Visudyne photodynamic therapy in CNV secondary to PM There is no experience of concomitant administration of Lucentis and Visudyne.
month (approximately 28 days). In Studies RVO-1 and RVO-2, patients received monthly injections of LUCENTIS for 6 months. In spite of being guided by optical coherence tomography and visual acuity re-treatment criteria, patients who were then not treated at Month 6 experienced on average, a loss of visual acuity at Month 7, whereas patients who were treated at Month 6 did not. Patients should be treated monthly. 2.4 Diabetic Macular Edema (DME) LUCENTIS 0.3 mg (0.05 mL of 6 mg/mL LUCENTIS solution) is recommended to be administered by intravitreal injection once a month (approximately 28 days).
Method of administration (EU SmPC) Single-use container for intravitreal use only. Lucentis should be inspected visually for particulate matter and discoloration prior to administration. The injection procedure should be carried out under aseptic conditions, which includes the use of surgical hand disinfection, sterile gloves, a sterile drape and a sterile eyelid speculum

Novartis Page 9 Ranibizumab (Lucentis®)
(or equivalent) and the availability of sterile paracentesis (if required). The patient’s medical history for hypersensitivity reactions should be carefully evaluated prior to performing the intravitreal procedure. Adequate anaesthesia and a broad-spectrum topical microbicide to disinfect the periocular skin, eyelid and ocular surface should be administered prior to the injection, in accordance with local practice. The injection needle should be inserted 3.5-4.0 mm posterior to the limbus into the vitreous cavity, avoiding the horizontal meridian and aiming towards the centre of the globe. The injection volume of 0.05 ml is then delivered; a different scleral site should be used for subsequent injections. Method of administration according to the US Prescribing Information The intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape, and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad-spectrum microbicide should be given prior to the injection. Following the intravitreal injection, patients should be monitored for elevation in intraocular pressure and for endophthalmitis. Monitoring may consist of a check for perfusion of the optic nerve head immediately after the injection and tonometry within 30 minutes following the injection. Patients should be instructed to report any symptoms suggestive of endophthalmitis without delay. Each vial should only be used for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, filter, and injection needles should be changed before LUCENTIS is administered to the other eye. No special dosage modification is required for any of the populations that have been studied (e.g., gender, elderly).
10 Summary of comparative effectiveness in a variety of clinical settings
Identification of clinical evidence and summary of available data
Information as provided in the approved ranibizumab (Lucentis®) EU SmPC, dated Sep 20141: Treatment of wet AMD In wet AMD, the clinical safety and efficacy of Lucentis have been assessed in three randomised, double-masked, sham- or active-controlled studies of 24 months duration in patients with neovascular AMD. A total of 1,323 patients (879 active and 444 control) were enrolled in these studies. In study FVF2598g (MARINA), 716 patients with minimally classic or occult with no classic choroidal neovascularisation (CNV) received monthly intravitreal injections of Lucentis

Novartis Page 10 Ranibizumab (Lucentis®)
0.3 mg (n=238) or 0.5 mg (n=240) or sham (n=238) injections. In study FVF2587g (ANCHOR), 423 patients with predominantly classic CNV lesions received either: 1) monthly intravitreal injections of Lucentis 0.3 mg and sham PDT (n=140); 2) monthly intravitreal injections of Lucentis 0.5 mg and sham PDT (n=140); or 3) sham intravitreal injections and active verteporfin PDT (n=143). Sham or active verteporfin PDT was given with the initial Lucentis injection and every 3 months thereafter if fluorescein angiography showed persistence or recurrence of vascular leakage. Key outcome measures are summarised in Table 1 and Figure 1. Table 1 Outcomes at Month 12 and Month 24 in study FVF2598g (MARINA) and
FVF2587g (ANCHOR)
FVF2598g (MARINA) FVF2587g (ANCHOR)
Outcome measure Month Sham
(n=238)
Lucentis 0.5 mg
(n=240)
Verteporfin PDT (n=143)
Lucentis 0.5 mg (n=140)
Loss of <15 letters in visual acuity (%)a
(maintenance of vision, primary endpoint)
Month 12 62% 95% 64% 96%
Month 24 53% 90% 66% 90%
Gain of ≥15 letters in visual acuity (%)a
Month 12 5% 34% 6% 40%
Month 24 4% 33% 6% 41%
Mean change in visual acuity (letters) (SD)a
Month 12 -10.5 (16.6) +7.2 (14.4)
-9.5 (16.4) +11.3 (14.6)
Month 24 -14.9 (18.7) +6.6 (16.5)
-9.8 (17.6) +10.7 (16.5)
a p<0.01

Novartis Page 11 Ranibizumab (Lucentis®)
Figure 1 Mean change in visual acuity from baseline to Month 24 in study FVF2598g (MARINA) and study FVF2587g (ANCHOR)
Results from both trials indicated that continued ranibizumab treatment may also be of benefit in patients who lost ≥15 letters of best-corrected visual acuity (BCVA) in the first year of treatment. Study FVF3192g (PIER) was a randomised, double-masked, sham-controlled study designed to assess the safety and efficacy of Lucentis in 184 patients with all forms of neovascular AMD. Patients received Lucentis 0.3 mg (n=60) or 0.5 mg (n=61) intravitreal injections or sham (n=63) injections once a month for 3 consecutive doses, followed by a dose
0 2 4 6 8 10 12 14 16 18 20 22 24Month
-15
-10
-5
0 5
10
15
Mea
n ch
ange
in v
isua
l acu
ity ±
SE
(le
tters
)
-14.9
+6 6
Study FVF2598g (MARINA)
0 2 4 6 8 10 12 14 16 18 20 22 24Month
-15
-10
-5
0 5
10
15
Mea
n ch
ange
in v
isua
l acu
ity ±
SE
(le
tter
s)
-9.8
+10.7
Study FVF2587g (ANCHOR)
Sham (n=238) LUCENTIS 0.5 mg (n=240)
Verteporfin PDT (n=143) LUCENTIS 0.5 mg (n=140)
MARINA ANCHOR
+ 21.5
+20.5

Novartis Page 12 Ranibizumab (Lucentis®)
administered once every 3 months. From Month 14 of the study, sham-treated patients were allowed to cross over to receive ranibizumab and from Month 19, more frequent treatments were possible. Patients treated with Lucentis in PIER received a mean of 10 total treatments. The primary efficacy endpoint was mean change in visual acuity at 12 months compared with baseline. After an initial increase in visual acuity (following monthly dosing), on average, patients’ visual acuity declined with quarterly dosing, returning to baseline at Month 12 and this effect was maintained in most ranibizumab-treated patients (82%) at Month 24. Data from a limited number of subjects that crossed over to receive ranibizumab after more than a year of sham-treatment suggested that early initiation of treatment may be associated with a better preservation of visual acuity. In both the MARINA and ANCHOR studies, the improvement in visual acuity seen with Lucentis 0.5 mg at 12 months was accompanied by patient-reported benefits as measured by the National Eye Institute Visual Function Questionnaire (VFQ-25) scores. The differences between Lucentis 0.5 mg and the two control groups were assessed with p-values ranging from 0.009 to <0.0001. The efficacy of Lucentis in the treatment of wet AMD has been further confirmed in AMD studies finalised since the marketing approval. Data from two studies (MONT BLANC, BPD952A2308 and DENALI, BPD952A2309) did not demonstrate additional effect of the combined administration of verteporfin (Visudyne PDT) and Lucentis compared to Lucentis monotherapy. Treatment of visual impairment due to DME The efficacy and safety of Lucentis have been assessed in two randomised, double-masked, sham- or active controlled studies of 12 months duration in patients with visual impairment due to diabetic macular oedema. A total of 496 patients (336 active and 160 control) were enrolled in these studies, the majority had type II diabetes, 28 ranibizumab-treated patients had type I diabetes. In the phase II study D2201 (RESOLVE), 151 patients were treated with ranibizumab (6 mg/ml, n=51, 10 mg/ml, n=51) or sham (n=49) by monthly intravitreal injections until pre-defined treatment stopping criteria were met. The initial ranibizumab dose (0.3 mg or 0.5 mg) could be doubled at any time during the study after the first injection. Laser photocoagulation was allowed as rescue treatment from Month 3 in both treatment arms. The study had two parts: an exploratory part (the first 42 patients analysed at Month 6) and a confirmatory part (the remaining 109 patients analysed at Month 12). The mean average change in BCVA from Month 1 to Month 12 compared to baseline was +7.8 (±7.72) letters in the pooled ranibizumab-treated patients (n=102) from both parts of the study, compared to -0.1 (±9.77) letters for patients on sham treatment (p<0.0001 for the treatment difference). In the phase III study D2301 (RESTORE), 345 patients with visual impairment due to macular oedema were randomised to receive either intravitreal injection of ranibizumab 0.5 mg as monotherapy and sham laser photocoagulation (n=116), combined ranibizumab 0.5 mg and laser photocoagulation (n=118) or sham injection and laser photocoagulation (n=111). Treatment with ranibizumab was initiated with monthly intravitreal injections and continued until visual acuity was stable for at least three consecutive monthly assessments. The treatment was reinitiated when a reduction in BCVA due to DME progression was

Novartis Page 13 Ranibizumab (Lucentis®)
observed. Laser photocoagulation was administered at baseline on the same day, at least 30 minutes before injection of ranibizumab, and then as needed based on ETDRS criteria. 240 patients, who had previously completed the 12-month RESTORE study, were enrolled in the open-label, multicentre 24-month extension (RESTORE Extension) study. Patients were treated with ranibizumab 0.5 mg pro re nata (PRN) in the same eye that was selected as the study eye in the study D2301 (RESTORE). Treatment was re-initiated at monthly intervals upon a decrease in BCVA due to DME and continued until stable BCVA was reached. In addition, laser treatment was administered if deemed necessary by the investigator and based on ETDRS criteria. Key outcome measures are summarised in Table 2 (RESTORE and Extension) and Figure 2 (RESTORE).
Figure 2 Mean change in visual acuity from baseline over time in study D2301 (RESTORE)
BL=baseline; SE=standard error of mean
* Difference in least square means, p0.0001/0.0004 based on two-sided stratified Cochran-Mantel-Haenszel test The effect at 12 months was consistent in most subgroups. However, subjects with a fairly good baseline BCVA (>73 letters) together with macular oedema with central retinal
Mean V
A c
hang
e fr
om
BL
+/-
SE
(le
tters
)
-4
-2
0
2
4
6
8
10
12
Month
0 1 2 3 4 5 6 7 8 9 10 11 12
Treatment group Ranibizumab 0.5 mg (N = 115)Ranibizumab 0.5 mg + Laser (N = 118)
Laser (N = 110)
+ 6.8/+ 6.4
+ 6.2/+ 5.4*
+ 0.9

Novartis Page 14 Ranibizumab (Lucentis®)
thickness of <300 µm did not appear to benefit from treatment with ranibizumab compared to laser photocoagulation. Table 2 Outcomes at Month 12 in study D2301 (RESTORE) and at Month 36 in study
D2301-E1 (RESTORE Extension)
Outcome measures at Month 12 compared to baseline in study D2301 (RESTORE)
Ranibizumab
0.5 mg
n=115
Ranibizumab
0.5 mg + Laser n=118
Laser
n=110
Mean average change in BCVA from Month 1 to Month 12a (SD)
6.1 (6.4)a 5.9 (7.9)a 0.8 (8.6)
Mean change in BCVA at Month 12 (SD)
6.8 (8.3)a 6.4 (11.8)a 0.9 (11.4)
Gain of ≥10 letters or BCVA ≥84 letters at Month 12 (%)
37.4a 43.2a 15.5
Gain of ≥15 letters or BCVA ≥84 letters at Month 12 (%)
22.6 22.9 8.2
Outcome measure at Month 36 compared to D2301 (RESTORE) baseline in study D2301-E1 (RESTORE Extension)
Prior ranibizumab
0.5 mg
n=83
Prior ranibizumab
0.5 mg + laser
n=83
Prior laser
n=74*
Mean change in BCVA at Month 24 (SD) 7.9 (9.0) 6.7 (7.9) 5.4 (9.0)
Mean change in BCVA at Month 36 (SD) 8.0 (10.1) 6.7 (9.6) 6.0 (9.4)
Gain of ≥10 letters or BCVA ≥84 letters at Month 36 (%) 47.0 44.6 41.9
Gain of ≥15 letters or BCVA ≥84 letters at Month 36 (%) 27.7 30.1 21.6
ap<0.0001 for comparisons of ranibizumab arms vs. laser arm. n in D2301-E1 (RESTORE Extension) is the number of patients with a value at both D2301 (RESTORE) baseline (Month 0) and at the Month 36 visit.

Novartis Page 15 Ranibizumab (Lucentis®)
*of the 74 patients with prior laser treatment, 59 (79%) received ranibizumab in the extension study. The improvement in visual acuity seen with Lucentis 0.5 mg at 12 months was accompanied by patient-reported benefits with regards to most vision-related functions as measured by the National Eye Institute Visual Function Questionnaire (VFQ-25) scores. For other subscales of this questionnaire no treatment differences could be established. The difference between Lucentis 0.5 mg and the control group was assessed with p-values of 0.0137 (ranibizumab mono) and 0.0041 (ranibizumab+laser) for the VFQ-25 composite score. The mean number of injections administered in the 12-month RESTORE study was 7.0 in the ranibizumab 0.5 mg, 6.8 in the ranibizumab plus laser groups and 7.3 sham injections in the laser monotherapy group. On average, 6.4 ranibizumab injections were administered per patient in the 24-month extension period in patients who were treated with ranibizumab in study D2301 (RESTORE). Of the 74 patients from study D2301 (RESTORE) laser treatment arm, 59 (79%) received ranibizumab at some point during the extension phase. On average, these 59 patients received 8.1 ranibizumab injections in the 24-month extension. The proportions of patients who did not require any ranibizumab treatment during the extension phase were 19%, 25% and 20% in the prior ranibizumab, prior ranibizumab + laser and prior laser group, respectively. The long-term safety profile of ranibizumab observed in the 24-month extension study is consistent with the known Lucentis safety profile. In the phase IIIb study D2304 (RETAIN), 372 patients with visual impairment due to DME were randomised to receive intravitreal injections of either: ranibizumab 0.5 mg with concomitant laser photocoagulation on a treat-and-extend
(TE) regimen (n=121), ranibizumab 0.5 mg monotherapy on a TE regimen (n=128), ranibizumab 0.5 mg monotherapy on a PRN regimen (n=123). In all groups, treatment with ranibizumab was initiated with monthly intravitreal injections and continued until BCVA was stable for at least three consecutive monthly assessments. Laser photocoagulation was administered at baseline on the same day as the first ranibizumab injection and then as needed based on ETDRS criteria. On TE, ranibizumab was then administered, at scheduled treatment at intervals of 2-3 months. On PRN, BCVA was assessed monthly and ranibizumab was then administered during the same visit, if needed. In all groups, monthly treatment was re-initiated upon a decrease in BCVA due to DME progression and continued until stable BCVA was reached again. The study duration was 24 months. In the RETAIN study, after 3 initial monthly treatment visits, the number of scheduled treatment visits required by the TE regimen was 13 compared to the 20 monthly visits required by the PRN regimen. With both regimens, more than 70% of patients maintained their BCVA with a visit frequency of ≥2 months. Over 24 months the mean (median) number of injections was 12.4 (12.0) in TE ranibizumab + laser, 12.8 (12.0) in TE ranibizumab alone, and 10.7 (10.0) for the PRN ranibizumab treatment groups. The addition of laser was not associated with a reduced mean number of ranibizumab injections in the TE regimen.

Novartis Page 16 Ranibizumab (Lucentis®)
The key outcome measures are summarised in Table 3. Table 3 Outcomes in study D2304 (RETAIN)
Outcome measure compared to baseline
TE ranibizumab
0.5 mg + laser
n=117
TE ranibizumab
0.5 mg alone
n=125
PRN ranibizumab
0.5 mg
n=117
Mean average change in BCVA from Month 1 to Month 12 (SD)
5.9 (5.5) a 6.1 (5.7) a 6.2 (6.0)
Mean average change in BCVA from Month 1 to Month 24 (SD)
6.8 (6.0) 6.6 (7.1) 7.0 (6.4)
Mean change in BCVA at Month 24 (SD)
8.3 (8.1) 6.5 (10.9) 8.1 (8.5)
Gain of ≥10 letters or BCVA ≥84 letters at Month 24 (%)
43.6 40.8 45.3
Gain of ≥15 letters or BCVA ≥84 letters at Month 24(%)
25.6 28.0 30.8
ap<0.0001 for assessment of non-inferiority to PRN
In DME studies, the improvement in BCVA was accompanied by a reduction over time in mean CSFT in all the treatment groups. Treatment of visual impairment due to macular oedema secondary to RVO The clinical safety and efficacy of Lucentis in patients with visual impairment due to macular oedema secondary to RVO have been assessed in the randomised, double-masked, controlled studies BRAVO and CRUISE that recruited subjects with BRVO (n=397) and CRVO (n=392), respectively. In both studies, subjects received either 0.3 mg or 0.5 mg intravitreal ranibizumab or sham injections. After 6 months, patients in the sham-control arms were crossed over to 0.5 mg ranibizumab. In BRAVO, laser photocoagulation as rescue was allowed in all arms from Month 3.

Novartis Page 17 Ranibizumab (Lucentis®)
Key outcome measures from BRAVO and CRUISE are summarised in Tables 4 and 5 and Figures 3 and 4. Table 4 Outcomes at Month 6 and 12 (BRAVO)
Sham/Lucentis 0.5 mg
(n=132)
Lucentis 0.5 mg
(n=131)
Mean change in visual acuity at Month 6a (letters) (SD) (primary endpoint)
7.3 (13.0) 18.3 (13.2)
Mean change in BCVA at Month 12 (letters) (SD)
12.1 (14.4) 18.3 (14.6)
Gain of ≥15 letters in visual acuity at Month 6a (%)
28.8 61.1
Gain of ≥15 letters in visual acuity at Month 12 (%)
43.9 60.3
Proportion (%) receiving laser rescue over 12 months
61.4 34.4
ap<0.0001

Novartis Page 18 Ranibizumab (Lucentis®)
Figure 3 Mean change from baseline BCVA over time to Month 6 and Month 12 (BRAVO)
BL=baseline; SE=standard error of mean
Mea
n V
A
chan
ge fr
om
BL
+-
SE
(le
tters
)
0
2
4
6
8
10
12
14
16
18
20
Month
0 1 2 3 4 5 6 7 8 9 10 11 12
Treatment group Sham/Ranibizumab 0.5 mg (n=132)
Ranibizumab 0.5 mg (n=131)
sham-controlled arm
crossed-over to ranibizumab sham-controlled
+ 7.3
+ 18.3
+ 18.3
+ 12.1

Novartis Page 19 Ranibizumab (Lucentis®)
Table 5 Outcomes at Month 6 and 12 (CRUISE)
Sham/Lucentis 0.5 mg
(n=130)
Lucentis 0.5 mg
(n=130)
Mean change in visual acuity at Month 6a (letters) (SD) (primary endpoint)
0.8 (16.2) 14.9 (13.2)
Mean change in BCVA at Month 12 (letters) (SD)
7.3 (15.9) 13.9 (14.2)
Gain of ≥15 letters in visual acuity at Month 6a (%)
16.9 47.7
Gain of ≥15 letters in visual acuity at Month 12 (%)
33.1 50.8
ap<0.0001
Figure 4 Mean change from baseline BCVA over time to Month 6 and Month 12 (CRUISE)
BL=baseline; SE=standard error of mean
-2
0
2
4
6
8
10
12
14
16
18
20
Month
0 1 2 3 4 5 6 7 8 9 10 11 12
Treatment group Sham/Ranibizumab 0.5 mg (n=130) Ranibizumab 0.5 mg (n=130)
+ 14.9
+ 0.8
sham-controlled sham-controlled arm crossed-over to ranibizumab
+ 13.9
+ 7.3

Novartis Page 20 Ranibizumab (Lucentis®)
In both studies, the improvement of vision was accompanied by a continuous and significant reduction in the macular oedema as measured by central retinal thickness. In patients with BRVO (BRAVO and extension study HORIZON): After 2 years, subjects that were treated with sham in the first 6 months and subsequently crossed over to ranibizumab treatment had achieved comparable gains in VA (~15 letters) compared to subjects that were treated with ranibizumab from study start (~16 letters). However the number of patients completing 2 years was limited and in HORIZON only quarterly monitoring visits were scheduled. Therefore there is currently insufficient evidence to conclude on recommendations as to when ranibizumab treatment should be initiated in patients with BRVO. In patients with CRVO (CRUISE and extension study HORIZON): After 2 years, subjects that were treated with sham in the first 6 months and subsequently crossed over to ranibizumab treatment did not achieve comparable gains in VA (~6 letters) compared to subjects that were treated with ranibizumab from study start (~12 letters). The improvement in visual acuity observed with ranibizumab treatment at 6 and 12 months was accompanied by patient-reported benefits as measured by the National Eye Institute Visual Function Questionnaire (NEI VFQ-25) sub-scales related to near and distance activity. The difference between Lucentis 0.5 mg and the control group was assessed at Month 6 with p-values of 0.02 to 0.0002. Treatment of visual impairment due to CNV secondary to PM The clinical safety and efficacy of Lucentis in patients with visual impairment due to CNV in PM have been assessed based on the 12-month data of the randomised, double-masked, controlled pivotal study F2301 (RADIANCE). This study was designed to evaluate two different dosing regimens of 0.5 mg ranibizumab given as an intravitreal injection in comparison to verteporfin PDT (vPDT, Visudyne photodynamic therapy). The 277 patients were randomised to one of the following arms: Group I (ranibizumab 0.5 mg, dosing regimen driven by “stability” criteria defined as no
change in BCVA compared to two preceding monthly evaluations).
Group II (ranibizumab 0.5 mg, dosing regimen driven by “disease activity” criteria defined as vision impairment attributable to intra- or subretinal fluid or active leakage due to the CNV lesion as assessed by OCT and/or FA).
Group III (vPDT - patients were allowed to receive ranibizumab treatment as of Month 3).
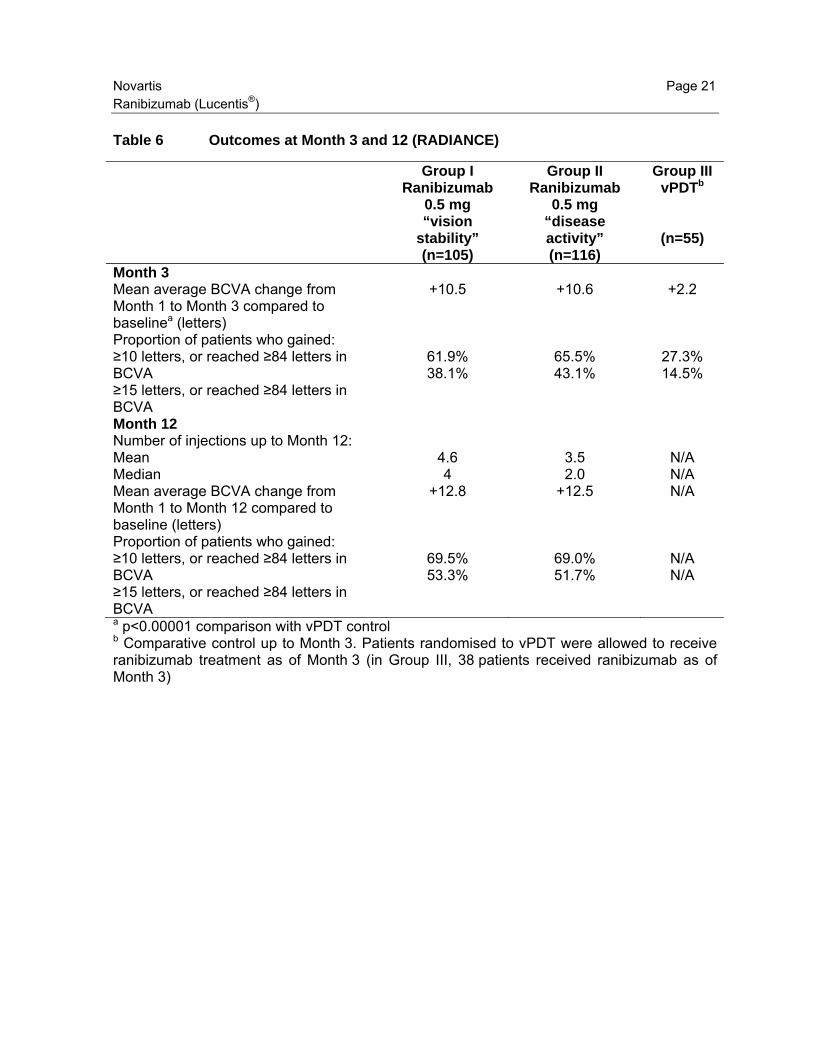
During the 12 months of the study, patients received on average 4.6 injections (range 1-11) in Group I and 3.5 injections (range 1-12) in Group II. In Group II, which is the recommended posology (see section 4.2), 50.9% of patients required 1 or 2 injections, 34.5% required 3 to 5 injections and 14.7% required 6 to 12 injections over the 12-month study period. 62.9% of Group II patients did not require injections in the second 6 months of the study. The key outcomes from RADIANCE are summarised in Table 6 and Figure 5.
Novartis Page 21 Ranibizumab (Lucentis®)
Table 6 Outcomes at Month 3 and 12 (RADIANCE)
Group I Ranibizumab
0.5 mg “vision
stability” (n=105)
Group II Ranibizumab
0.5 mg “disease activity” (n=116)
Group III vPDTb
(n=55)
Month 3 Mean average BCVA change from Month 1 to Month 3 compared to baselinea (letters)
+10.5 +10.6 +2.2
Proportion of patients who gained: ≥10 letters, or reached ≥84 letters in BCVA ≥15 letters, or reached ≥84 letters in BCVA
61.9% 38.1%
65.5% 43.1%
27.3% 14.5%
Month 12 Number of injections up to Month 12: Mean Median
4.6 4
3.5 2.0
N/A N/A
Mean average BCVA change from Month 1 to Month 12 compared to baseline (letters)
+12.8 +12.5 N/A
Proportion of patients who gained: ≥10 letters, or reached ≥84 letters in BCVA ≥15 letters, or reached ≥84 letters in BCVA
69.5% 53.3%
69.0% 51.7%
N/A N/A
a p<0.00001 comparison with vPDT control b Comparative control up to Month 3. Patients randomised to vPDT were allowed to receive ranibizumab treatment as of Month 3 (in Group III, 38 patients received ranibizumab as of Month 3)

Novartis Page 22 Ranibizumab (Lucentis®)
Figure 5 Mean change from baseline BCVA over time to Month 12 (RADIANCE)
The improvement of vision was accompanied by a reduction in central retinal thickness. Patient-reported benefits were observed with ranibizumab treatment arms over vPDT (p-value <0.05) in terms of improvement in the composite score and several subscales (general vision, near activities, mental health and dependency) of the NEI VFQ-25.
Summary of available estimates of comparative efectiveness Head-to-head trials comparing aflibercept (Eylea) and ranibizumab in nAMD Aflibercept is a product owned by Bayer/Regeneron. Aflibercept is approved for ocular use in nAMD, and CRVO, in the US and EU, and in a number of additional countries. Aflibercept is also approved for DME in the US, EU and Japan, for BRVO in US and for mCNV in Japan. The VIEW 1 and 2 trials compared aflibercept and ranibizumab in nAMD. There is no comparative data available for the other indications.
-5
0
5
10
15
20
0 1 2 3 4 5 6 7 8 9 10 11 12
Mea
n V
A c
hang
e fr
om B
L +
- S
E (
lett
ers)
Month Ranibizumab 0.5 mg Group I by stabilisation (n=105)
Verteporfin PDT Group III (n=55)
Ranibizumab 0.5 mg Group II by disease activity (n=116)
Ranibizumab 0.5 mg/Verteporfin PDT Group III from Month 3 onwards (n=55)
Ranibizumab allowed
+1 4
+12.
+12.
+14 4
+13.8
+9.

Novartis Page 23 Ranibizumab (Lucentis®)
The safety and efficacy of aflibercept were assessed in two similarly-designed, randomized, multi-center, double-masked, active-controlled studies (VIEW 1 and VIEW 2) in patients with nAMD. A total of 2412 patients were treated and evaluable for efficacy (1817 with aflibercept) in the two studies. In each study, patients were randomly assigned in a 1:1:1:1 ratio to 1 of 4 dosing regimens: 1) ranibizumab 0.5 mg administered every 4 weeks; 2) Aflibercept 2 mg administered every 4 weeks; 3) Aflibercept 0.5 mg administered every 4 weeks; and 4) Aflibercept 2 mg administered every 8 weeks following 3 initial monthly doses. Patient ages ranged from 49 to 99 years with a mean of 76 years. In the second year of the studies, patients continued to receive the dosage strength to which they were initially randomized but on a modified dosing schedule guided by assessment of visual and anatomic outcomes with a protocol-defined maximum dosing interval of 12 weeks. In both studies, the primary efficacy endpoint was the proportion of patients in the Per Protocol Set who maintained vision, defined as losing fewer than 15 letters of visual acuity at week 52 compared to baseline. In the VIEW1 study, at week 52, 95.1% of patients in the aflibercept 2Q8 treatment group maintained vision compared to 94.4% patients in the ranibizumab 0.5Q4 group. Aflibercept treatment was shown to be non-inferior to the ranibizumab 0.5Q4 group. In the VIEW2 study, at week 52, 95.6% of patients in the aflibercept 2Q8 treatment group maintained vision compared to 94.4% patients in the ranibizumab 0.5Q4 group. Aflibercept treatment was shown to be non-inferior to the ranibizumab 0.5Q4 group. Head-to-head trials comparing intravitreal bevacizumab and ranibizumab in nAMD Bevacizumab (Avastin®) is developed and commercialized by Genentech and Roche, but is not approved to treat ocular conditions or compounding into smaller doses in any country. It was developed and is formulated for the intravenous treatment of certain cancers. However, although there is no formulation available that is suitable for intraocular injections and needs to be compounded into smaller doses, for some years now it is being used off-label to treat in particular nAMD. The CATT (Comparison of AMD Treatments) trial (1,107 patients) and the IVAN trial (610 patients) compared ranibizumab with intravitreal bevacizumab 37, 38, 39, 40. CATT Among patients following the same regimen for 2 years, mean gain in visual acuity was similar for both drugs (bevacizumab-ranibizumab difference, -1.4 letters; 95% confidence interval [CI], -3.7 to 0.8; P = 0.21). Mean gain was greater for monthly than for as-needed treatment (difference, -2.4 letters; 95% CI, -4.8 to -0.1; P = 0.046). The proportion of patients without fluid in OCT ranged from 13.9% in the bevacizumab-as-needed group to 45.5% in the ranibizumab monthly group (drug, P = 0.0003; regimen, P < 0.0001). At 2 years, patients in CATT receiving as needed ranibizumab fully maintained first-year vision gains with an average 5.7 injections in the second year. Patients treated with as needed intravitreal bevacizumab experienced a slight decline in vision despite receiving significantly more (+1.5) injections than patients treated with ranibizumab over the two year period.

Novartis Page 24 Ranibizumab (Lucentis®)
IVAN 525 participants reached the visit at 2 years: 134 ranibizumab in continuous regimen, 137 ranibizumab in discontinuous regimen, 127 bevacizumab in continuous regimen, and 127 bevacizumab in discontinuous regimen. For BCVA, bevacizumab was neither non-inferior nor inferior to ranibizumab (mean difference -1.37 letters, 95% CI -3.75 to 1.01; p=0.26).
11 Summary of comparative evidence on safety:
Estimate of patient exposure to date
Ranibizumab has a well-established safety profile supported by more than 40 clinical studies and long term global real-world experience, including a dedicated Risk Management Plan and mandatory continuous safety monitoring via a systematic pharmacovigilance program survey that addresses the approved use. Its safety profile has been well established in a clinical development program that enrolled more than 19,733 patients across indications and there are more than 3 million patient-treatment years of exposure globally since its launch in the United States in 20062.
Description of the adverse effects/reactions and estimates of their frequencies Information taken from the ranibizumab EU SmPC dated Sep 20141: The majority of adverse reactions reported following administration of ranibizumab are related to the intravitreal injection procedure. The most frequently reported ocular adverse reactions following injection of ranibizumab are: eye pain, ocular hyperaemia, increased intraocular pressure, vitritis, vitreous detachment, retinal haemorrhage, visual disturbance, vitreous floaters, conjunctival haemorrhage, eye irritation, foreign body sensation in eyes, increased lacrimation, blepharitis, dry eye and eye pruritus. The most frequently reported non-ocular adverse reactions are headache, nasopharyngitis and arthralgia. Less frequently reported, but more serious, adverse reactions include endophthalmitis, blindness, retinal detachment, retinal tear and iatrogenic traumatic cataract (see section 4.4). Patients should be informed of symptoms of these potential adverse reactions and instructed to inform their physician if they develop signs such as eye pain or increased discomfort, worsening eye redness, blurred or decreased vision, an increased number of small particles in their vision, or increased sensitivity to light. The adverse reactions experienced following administration of ranibizumab in clinical trials are summarised in the table below. Tabulated list of adverse reactions# The adverse reactions are listed by system organ class and frequency using the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated

Novartis Page 25 Ranibizumab (Lucentis®)
from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. Infections and infestations Very common Nasopharyngitis Common Urinary tract infection* Blood and lymphatic system disorders Common Anaemia Immune system disorders Common Hypersensitivity Psychiatric disorders Common Anxiety Nervous system disorders Very common Headache Eye disorders Very common Vitritis, vitreous detachment, retinal haemorrhage, visual
disturbance, eye pain, vitreous floaters, conjunctival haemorrhage, eye irritation, foreign body sensation in eyes, lacrimation increased, blepharitis, dry eye, ocular hyperaemia, eye pruritus.
Common Retinal degeneration, retinal disorder, retinal detachment, retinal tear, detachment of the retinal pigment epithelium, retinal pigment epithelium tear, visual acuity reduced, vitreous haemorrhage, vitreous disorder, uveitis, iritis, iridocyclitis, cataract, cataract subcapsular, posterior capsule opacification, punctuate keratitis, corneal abrasion, anterior chamber flare, vision blurred, injection site haemorrhage, eye haemorrhage, conjunctivitis, conjunctivitis allergic, eye discharge, photopsia, photophobia, ocular discomfort, eyelid oedema, eyelid pain, conjunctival hyperaemia.
Uncommon Blindness, endophthalmitis, hypopyon, hyphaema, keratopathy, iris adhesion, corneal deposits, corneal oedema, corneal striae, injection site pain, injection site irritation, abnormal sensation in eye, eyelid irritation.
Respiratory, thoracic and mediastinal disorders Common Cough Gastrointestinal disorders Common Nausea Skin and subcutaneous tissue disorders Common Allergic reactions (rash, urticaria, pruritus, erythema)

Novartis Page 26 Ranibizumab (Lucentis®)
Musculoskeletal and connective tissue disorders Very common Arthralgia Investigations Very common Intraocular pressure increased # Adverse reactions were defined as adverse events (in at least 0.5 percentage points of patients) which occurred at a higher rate (at least 2 percentage points) in patients receiving treatment with ranibizumab 0.5 mg than in those receiving control treatment (sham or verteporfin PDT). * observed only in DME population
Summary of comparative safety against comparators
Head-to-head trials comparing aflibercept and ranibizumab (ranibizumab) Information taken from the European Public Assessment report relating to the VIEW 1 and 2 trials in neovascular AMD patients (Sep 2012)41. The VIEW 1 and 2 trials “were two phase III, controlled (ranibizumab 4-weekly) studies of efficacy, safety and tolerability in which, in Year 1, 0.5 mg or 2 mg aflibercept was dosed 4-weekly or 8-weekly for 2 mg, and in Year 2, 4 to 12-weekly.” (In Section 2.6.1, page 68 of EPAR) “The safety assessment conducted by the applicant in the 2 pivotal studies is appropriate. When safety results are pooled from these studies, the rate of ocular and non-ocular TEAEs seems similar between VEGF Trap-Eye and comparator groups.” “For vascular disorders, hypertension appeared with similar rates between the ranibizumab and aflibercept groups (7.9% vs 6.5%). The overall rate of arterial thromboembolic events was higher in aflibercept groups (3.2%) compared to 1.8% in ranibizumab group.” “Taking into account the fact that almost 20% of drug substance goes through the systemic circulation, systemic effects of VEGF Trap-eye on the circulation cannot be excluded, and appropriate monitoring is foreseen in the RMP. The number of cerebrovascular events was higher in the VEGF Trap-Eye groups (35) compared with ranibizumab (2 cases) in the elderly, especially in the sub-group ≥ 85 years (20 vs 1 case), during the first year of treatment. Two-year data showed also the increased number of cerebrovascular events in the VEGF Trap-Eye groups vs ranibizumab: 53 vs 12 (27 vs 3 in the subgroup ≥ 85 years). One death due to CVA in the 0.5Q4 group and one death due to ischemic stroke in the 2Q8 group were considered as treatment related. Among severe non-ocular TEAEs, TIA (transient ischemic attack) was observed in 10 patients treated with VEGF Trap-eye, while no cases occurred in comparator group. The majority of these subjects had pre-existing risk factors for cardiovascular disease. No subject had a positive antidrug antibody status. Since subjects were randomised to treatment, it is reasonable to assume that there would be an equal prevalence of risk factors in those assigned to ranibizumab.

Novartis Page 27 Ranibizumab (Lucentis®)
Arterial thromboembolic events are listed as an important potential risk in the RMP and covered in sections 4.4 and 4.8 of the SmPC. The higher proportion of TIAs and cerebrovascular events reported within the pooled data is of concern and will be carefully considered within further assessments of ATEs during routine pharmacovigilance procedures and PSURs.” (In Section 2.6.1, page 69 of EPAR) “Overall, the safety profile of aflibercept appears to be similar to the already marketed comparator drug, ranibizumab. No dose related effect was observed.” Comparison of unlicensed intravitreal bevacizumab and ranibizumab Ranibizumab, an anti-vascular endothelial growth factor (anti-VEGF) agent first licensed in 2006, has substantially improved the treatment of a number of sight-threatening retinal diseases as compared to other licensed treatments available at the time. Licensed indications include neovascular age-related macular degeneration (nAMD), diabetic macular edema, retinal vein occlusion and pathologic myopia1. Bevacizumab, also an anti-VEGF, is licensed for intravenous administration for the treatment of colorectal cancer and certain cases of breast, renal and lung cancer42. The use of bevacizumab in ophthalmic conditions is unlicensed. Molecular structure Ranibizumab and bevacizumab belong to the same class of VEGF-A inhibitors, however they are two distinct molecules, with markedly different pharmacokinetic and pharmacodynamic profiles43. Bevacizumab is a full-chain, Fc portion-containing monoclonal antibody (mAb), whilst ranibizumab is an antibody fragment from a different mAb, with a molecular weight over three-times lighter than that of bevacizumab1, 42. As a consequence, bevacizumab has significantly higher systemic exposure, resulting in systemic VEGF inhibition that could lead to changed safety profile regarding systemic adverse events43.

Novartis Page 28 Ranibizumab (Lucentis®)
Compared with bevacizumab: ‐ The lack of an Fc portion confers ranibizumab with limited active transportation from
the eye44 and greater retinal layer penetration than a normal antibody. ‐ Importantly, the molecular structure of ranibizumab results in a far shorter systemic
half-life (2 hours vs 20 days) and a far lower systemic exposure (over 70-times lower after 3 monthly injections)43.
o Whilst longevity in the plasma may be advantageous for an anticancer agent such as bevacizumab, increased anti-VEGF systemic exposure and subsequent VEGF suppression is not desirable in ophthalmic patients requiring localized intravitreal therapies.
‐ Ranibizumab quickly clears from the systemic circulation and has little effect on circulating free VEGF levels in the plasma. In contrast, bevacizumab accumulates systemically and therefore reduces systemic levels of VEGF43.
o Clinical experience with systemic VEGF inhibition in oncology has established that systemic VEGF inhibition is associated with several ‘class’ adverse effects, including hypertension, proteinuria, arterial thromboembolic events, cardiomyopathy, hemorrhage, wound healing complications, gastrointestinal perforation45.
Results from head-to-head clinical trials, meta-analyses and real-world evidence suggest potential differences in safety between ranibizumab and bevacizumab when used in nAMD. Lower levels of serious systemic adverse events for ranibizumab were observed as compared to bevacizumab (see below). Head-to-head trials (NB: in a head-to-head trial, two groups of patients with the same disease are compared. One group receives one treatment, and the second group receives the other): Whilst not being designed and powered to detect important safety differences for less frequent but serious adverse events, there is an emerging body of evidence from head-to-head trials such as CATT, IVAN and GEFAL indicating a potential difference in the safety profiles of ranibizumab and bevacizumab:
‐ CATT: The largest head-to-head study funded by the US National Eye Institute showed the rate of systemic serious adverse events (SAEs) with bevacizumab was 30% higher with bevacizumab than with ranibizumab (2 years: 24.4% vs 18.0%; p=0.009). There were also significantly more gastrointestinal (GI) disorders in the bevacizumab group46, 47.
‐ IVAN: The UK IVAN study showed a higher level of SAEs in the bevacizumab group than in those receiving ranibizumab, although this difference was not statistically significant (1 year: 12.5% vs 9.6%; 2 years: 27% vs 25.8%; not significant [ns])48, 49.
‐ GEFAL: This smaller 1-year French trial has also shown a consistent increase in the risk of SAEs with bevacizumab when compared to ranibizumab treatment (12.2% vs 10%; ns)50.

Novartis Page 29 Ranibizumab (Lucentis®)
‐ LUCAS: Fewer non-fatal myocardial infarctions (MIs) and cardiac events were seen in the bevacizumab group at 1 year. However, ranibizumab patients more often had a history of MI (11.9% vs 5.6%; p=0.021), which could explain the observed difference at 12 months. The rate of other adverse events was similar between the two drugs51.
Meta-analyses (NB: Meta-analyses use statistical techniques to overcome differences in trial designs and permit the combination and analysis of many different individual studies devoted to a specific topic): Multiple meta-analyses of head-to-head studies have been performed to increase the ability to detect differences between bevacizumab and ranibizumab, showing a 24-34% increased risk of experiencing systemic SAEs with bevacizumab than ranibizumab50, 48, 49, 52, 53. The most recent meta-analysis contained five RCTs and 2,686 randomized patients and confirmed that compared with ranibizumab, bevacizumab was associated with a statistically significant 34% increase in the number of patients with at least one systemic SAE53. Another recent report from the Cochrane Collaboration showed higher rates of GI disorders with bevacizumab compared with ranibizumab, but concluded overall that the systemic safety of bevacizumab in nAMD was similar to that of ranibizumab based on the analysis of arterial thrombotic events (ATEs)54. This conclusion is inconsistent with previously published meta-analyses, and closer scrutiny shows a sensitivity to the imbalanced baseline characteristics of the LUCAS study with respect to prior MI (26 [11.9%] in the ranibizumab group vs 12 [5.6%] in the bevacizumab group; p=0.021)51. The exclusion of 1year LUCAS data from the systematic review results in findings similar to those seen in other meta-analyses with bevacizumab being associated with a higher risk of systemic SAEs than ranibizumab. Real-world evidence (NB: These studies examine how existing medicines and treatments are working in the healthcare system. The large patient numbers can detect differences in low-rate adverse events): Potential differentiation between the safety profiles of ranibizumab and bevacizumab have also been shown in analyses of large US real-world medical insurance claims databases made by Curtis et al and Gower et al, where potential higher risks of death, hemorrhagic stroke and ocular inflammation with bevacizumab have been observed55, 56. Analyses of such databases should be interpreted with caution however, and no firm conclusions about the differences in the respective safety profiles of the two compounds should be derived from these data in isolation. Bevacizumab manufacturing and compounding raises important safety concerns Ranibizumab and bevacizumab are manufactured differently. Ranibizumab is manufactured to the more stringent intravitreal ophthalmic requirements than those required for intravenous medications57, 58. The compounding process for bevacizumab to enable intraocular use in clinical practice may also increase the risk of contamination and subsequent ocular infection59, 60. The compounding process where multiple intravitreal injections are aliquoted from a single vial of intravenous bevacizumab falls outside of the licensed mode of administration and generally takes place in hospitals or compounding pharmacies. Vial splitting and compounding of bevacizumab for intravitreal use in clinical practice carries an enhanced risk

Novartis Page 30 Ranibizumab (Lucentis®)
of sterility breach and bacterial contamination, and there have been several reports of infective endophthalmitis cases, some of which have resulted in product recalls of bevacizumab batches61, 62. Further, under real life conditions, and depending on the type of medical devices used during the compounding process (e.g. syringes or other containers) the quality of the finished product is uncontrolled and varies. There is also no control regarding stability of the various preparations, there is an increased risk of loss of efficacy, which increases with storage time, and of increased levels of particulate matter. Ranibizumab is formulated and manufactured in single use, preservative free vials or pre-filled syringes to stringent United States Pharmacopeial (USP) Convention standards for intravitreal use in terms of particulate matter levels and protein load, both of which minimize the potential for inflammatory adverse reactions58. Bevacizumab is manufactured to standards appropriate for its licensed intravenous oncology use, with a higher particulate matter limit than for intravitreal preparations57, 58. Compounded bevacizumab samples have been shown to contain increased levels of particulate matter, which has been associated with elevated intraocular pressure (IOP) and sterile endophthalmitis. The National Institute of Clinical Effectiveness (NICE) concluded in a single technology appraisal (Oct 2010)63: “There are safety concerns given that bevacizumab is not designed, manufactured or approved for intraocular use; bevacizumab formulation for systemic use does not meet the higher regulatory standards for intraocular use (USP 789). There have been large case series published of clusters of severe intraocular inflammation in Canada, and the manufacturer of bevacizumab issued Dear Health Professional letters across the world – including the UK - regarding a rise in the number of cases of sterile intraocular inflammation among patients treated with bevacizumab in nAMD.” There have been various reports suggesting that compounded product may not be prepared and provided to acceptable sterility standards for intravitreal use, including the following:
- In August 2011, clusters of infective endophthalmitis cases traced back to contamination during vial splitting led to an alert being issued by the FDA64, 65.
- In March 2012 a precautionary recall of compounded bevacizumab was issued by a leading compounding pharmacy in the UK after several reports of suspected sterile endophthalmitis were reported following intravitreal injection66.
- In March 2013, the FDA recalled a batch of compounded bevacizumab linked with cases of intraocular infections67.
There are only limited data regarding the stability of compounded bevacizumab and evidence indicates that its stability is impaired68. Active immunoglobulin levels in compounded bevacizumab samples have been shown to vary significantly among compounding pharmacies, leading to the possibility of variable efficacy depending on the amount of antibody present. Compounded bevacizumab samples have been shown to contain increased levels of particulate matter, which may lead to elevated intraocular pressure and inflammation68. Furthermore, the particulate matter content of compounded bevacizumab has been shown to increase over time in the weeks following compounding69.

Novartis Page 31 Ranibizumab (Lucentis®)
Finally, an analysis of Medicare claims data found that patients given bevacizumab were significantly more likely to require treatment for ocular inflammation (a sign of endophthalmitis) than those receiving ranibizumab70. The bevacizumab SmPC (August 2014)71 in Europe contains the following warning relating unlicensed use in the eye: “Intravitreal use Avastin is not formulated for intravitreal use. Eye disorders Individual cases and clusters of serious ocular adverse reactions have been reported following unapproved intravitreal use of Avastin compounded from vials approved for intravenous administration in cancer patients. These reactions included infectious endophthalmitis, intraocular inflammation such as sterile endophthalmitis, uveitis and vitritis, retinal detachment, retinal pigment epithelial tear, intraocular pressure increased, intraocular haemorrhage such as vitreous haemorrhage or retinal haemorrhage and conjunctival haemorrhage. Some of these reactions have resulted in various degrees of visual loss, including permanent blindness. Systemic effects following intravitreal use A reduction of circulating VEGF concentration has been demonstrated following intravitreal anti-VEGF therapy. Systemic adverse reactions including non-ocular haemorrhages and arterial thromboembolic reactions have been reported following intravitreal injection of VEGF inhibitors.” The US Bevacizumab PI (Nov 2014) contains the following information: “Eye disorders (from unapproved intravitreal use for treatment of various ocular disorders): Permanent loss of vision; Endophthalmitis (infectious and sterile); Intraocular inflammation; Retinal detachment; Increased intraocular pressure; Hemorrhage including conjunctival, vitreous hemorrhage or retinal hemorrhage; Vitreous floaters; Ocular hyperemia; Ocular pain or discomfort […] Systemic Events (from unapproved intravitreal use for treatment of various ocular disorders): Arterial thromboembolic events, Hypertension, Gastrointestinal perforation, Hemorrhage” Pharmacovigilance standards for ranibizumab There are differences in the pharmacovigilance processes for licensed and unlicensed products. Ranibizumab’s ocular efficacy and safety profile has been studied through an extensive clinical development program and substantiated by real-world experience comprising over 19-million injections and 3-million patient treatment years of exposure2. Safety monitoring related to the treatment of its licensed indications is continuous, via a systematic pharmacovigilance system and a formal approved global risk management plan. Novartis has also undertaken the largest observational study in retinal medicine, LUMINOUS, which, once

Novartis Page 32 Ranibizumab (Lucentis®)
fully recruited, will include 30,000 ranibizumab patients with up to 5 years’ longitudinal follow-up, thus providing additional safety information in a more diverse population than included within the pivotal trials. Currently, more than 29,000 patients are already enrolled in LUMINOUS.
12 Summary of available data on comparative cost and cost-effectiveness within the pharmacological class or therapeutic group:
Costs of the proposed medicine
Costs may vary in different settings because of negotiated procurement discounts. The UK NICE recommended ranibizumab when the manufacturer provided the product with the discount agreed in the patient access scheme (revised in 2012). http://publications.nice.org.uk/ranibizumab-and-pegaptanib-for-the-treatment-of-age-related-macular-degeneration-ta155
Resource use and comparative cost-effectiveness presented as range of cost per routine outcome
Most Health Technology Assessment authorities that evaluate the cost-effectiveness of drugs have deemed ranibizumab to be cost-effective. Below is a list of the most important agencies and decisions:
- In England & Wales, the National Institute for Clinical Effectiveness (NICE) considered ranibizumab to be cost effective in patients with wet AMD, CRVO, BRVO (if laser photocoagulation treatment was not beneficial or not suitable) , DME (in patients with CRT≥400 microns); and mCNV (when the manufacturer provides ranibizumab with the discount agreed in the patient access scheme)77-80
- The Scottish Medicines Consortium (SMC) has recommended ranibizumab as a cost-effective therapy for the treatment of all cases of wet AMD (in conjuction with NICE), BRVO, CRVO and mCNV; in DME, ranibizumab was recommended in adults with visual acuity below 75 letters score.77,81-84
- In Sweden, TLV has also deemed ranibizumab cost-effective for wet AMD - In Canada, CADTH has considered ranibizumab to be cost-effective in the treatment
of all patients with wet AMD and RVO; in DME ranibizumab was considered cost-effective for patients with clinically significant macuar edema with hbA1c ≤11%; the mCNV indication is currently under evaluation with CADTH85-87
- In addition, the PBAC has deemed ranibizumab to be cost-effective for the treatment of wet AMD, DME and RVO88-89.
The cost-effectiveness of ranibizumab has been demonstrated in multiple articles and research presentations in both nAMD90-100 and DME102, 103. One study has suggested that ranibizumab is not cost-effective in the treatment of nAMD patients, however this publication considered a short time horizon of 2 years and did not account for the benefits beyond those 2 years of treatment, as is customary in cost-effectiveness evaluations101.

Novartis Page 33 Ranibizumab (Lucentis®)
Novartis also recognizes that economic and access to healthcare inequities exist and increasingly applies flexible pricing and access models. One example is Accentrix® in India. Accentrix is a more affordable licensed treatment that has been introduced as part of Novartis’ commitment to providing better access to high quality medicines to patients in low-income markets. The product offers all the benefits of ranibizumab, along with the additional benefit of a more affordable price.
The product is approved in India for five indications (nAMD, DME, BRVO, CRVO, and CNV seconday to pathologic myopia (mCNV)).
Offering Accentrix to patients in India through a patient access scheme in 2014 increased the number of ranibizumab IVTs for patients that could now access the licensed nAMD treatment by 7 fold. Novartis plans to work with health authorities to ensure ongoing access to ranibizumab in other countries where patients pay predominantly out of pocket. Work is currently underway in a diverse set of markets including countries from Asia (e.g. Malaysia, Thailand and Vietnam), Latin America (Brazil and Chile) and Africa (e.g. Nigeria and Kenya). Novartis is actively involved in other innovative access programs to enhance patient outcomes. For example in June 2014 the first critical illness insurance program to include nAMD was launched by Sunshine Life in China in collaboration with Novartis. In a selection of markets representing different geographies in Africa (Nigeria, Kenya, Ivory Coast and Mauritius) Novartis is working with key eye centers/hospitals and the complete distribution chain to find solutions to offer Lucentis at the lowest possible cost to patients. Novartis works with health authorities in offering a range of managed entry agreements, all with the intention of increasing the number of patients that can be treated with ranibizumab within budgets available. On average the net price paid for ranibizumab is 15 – 40% below the published list price.
13 Summary of regulatory status of the medicine Ranibizumab is registered in the following indications34:
• the treatment of neovascular (wet) age-related macular degeneration (wet AMD) • the treatment of visual impairment due to diabetic macular edema (DME) • the treatment of visual impairment due to macular edema secondary to retinal vein
occlusion (branch RVO or central RVO) • the treatment of visual impairment due to choroidal neovascularization (CNV)
secondary to pathologic myopia (PM) (mCNV) Ranibizumab was first registered by Genentech Inc in the USA on 30 Jun 2006 and by Novartis in the EU on 22 Jan 2007 for use in neovascular (wet) age-related macular degeneration (wet-AMD). Ranibizumab is currently registered in more than 100 countries worldwide for wet-AMD, for DME, BRVO, CRVO, and in more than 80 countries for mCNV.

Novartis Page 34 Ranibizumab (Lucentis®)
14 Availability of pharmacopoeial standards (British Pharmacopoeia, International Pharmacopoeia, United States Pharmacopoeia)
Lucentis is manufactured to the standards for intra-ocular (intravitreal) use3 . Each therapeutic dose is filled in containers (vials or prefilled syringes) intended for single use and complies with US Pharmacopeia (USP 789) specific requirements for ophthalmic solutions, which are stricter than for parenteral (i.e. intravenous) products. Single use containers are reducing the risks associated with compounding.
15 Proposed (new/adapted) text for the WHO Model Formulary Selected relevant information is taken from the Lucentis European Summary of Product Characteristics (SmPC Sep 2014)34. 1. NAME OF THE MEDICINAL PRODUCT Ranibizumab 10 mg/ml solution for injection 2. QUALITATIVE AND QUANTITATIVE COMPOSITION [Vial] One ml contains 10 mg ranibizumab*. Each vial contains 2.3 mg of ranibizumab in 0.23 ml solution. [Pre-filled syringe] One ml contains 10 mg ranibizumab*. One pre-filled syringe contains 0.165 ml, equivalent to 1.65 mg ranibizumab. The extractable volume of one pre-filled syringe is 0.1 ml. This provides a usable amount to deliver a single dose of 0.05 ml containing 0.5 mg ranibizumab. *Ranibizumab is a humanised monoclonal antibody fragment produced in Escherichia coli cells by recombinant DNA technology. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Solution for injection. Clear, colourless to pale yellow aqueous solution. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Ranibizumab is indicated in adults for: The treatment of neovascular (wet) age-related macular degeneration (AMD)

Novartis Page 35 Ranibizumab (Lucentis®)
The treatment of visual impairment due to diabetic macular oedema (DME) The treatment of visual impairment due to macular oedema secondary to branch retinal
vein occlusion (BRVO) The treatment of visual impairment due to macular oedema secondary to central retinal
vein occlusion (CRVO) The treatment of visual impairment due to choroidal neovascularisation (CNV) secondary
to pathologic myopia (PM) 4.2 Posology and method of administration Ranibizumab must be administered by a qualified ophthalmologist experienced in intravitreal injections. The recommended dose for ranibizumab is 0.5 mg given as a single intravitreal injection. This corresponds to an injection volume of 0.05 ml. The interval between two doses injected into the same eye should be at least four weeks. Treatment is initiated with one injection per month until maximum visual acuity is achieved and/or there are no signs of disease activity i.e. no change in visual acuity and in other signs and symptoms of the disease under continued treatment. In patients with wet AMD, DME, BRVO and CRVO, initially, three or more consecutive, monthly injections may be needed. Thereafter, monitoring and treatment intervals should be determined by the physician and should be based on disease activity, as assessed by visual acuity and/or anatomical parameters. If, in the physician’s opinion, visual and anatomic parameters indicate that the patient is not benefiting from continued treatment, ranibizumab should be discontinued. Monitoring for disease activity may include clinical examination, functional testing or imaging techniques (e.g. optical coherence tomography or fluorescein angiography). If patients are being treated according to a treat-and-extend regimen, once maximum visual acuity is achieved and/or there are no signs of disease activity, the treatment intervals can be extended stepwise until signs of disease activity or visual impairment recur. The treatment interval should be extended by no more than two weeks at a time for wet AMD and may be extended by up to one month at a time for DME. For BRVO and CRVO, treatment intervals may also be gradually extended, however there are insufficient data to conclude on the length of these intervals. If disease activity recurs, the treatment interval should be shortened accordingly. In the treatment of visual impairment due to CNV secondary to PM, many patients may only need one or two injections during the first year, while some patients may need more frequent treatment (see section 5.1). Ranibizumab and laser photocoagulation in DME and in macular oedema secondary to BRVO There is some experience of Lucentis administered concomitantly with laser

Novartis Page 36 Ranibizumab (Lucentis®)
photocoagulation (see section 5.1). When given on the same day, Lucentis should be administered at least 30 minutes after laser photocoagulation. Lucentis can be administered in patients who have received previous laser photocoagulation. Ranibizumab and verteporfin photodynamic therapy in CNV secondary to PM There is no experience of concomitant administration of ranibizumab and verterporfin. Special populations Hepatic impairment Ranibizumab has not been studied in patients with hepatic impairment. However, no special considerations are needed in this population. Renal impairment Dose adjustment is not needed in patients with renal impairment (see section 5.2). Elderly No dose adjustment is required in the elderly. There is limited experience in patients older than 75 years with DME. Paediatric population The safety and efficacy of Lucentis in children and adolescents below 18 years of age have not been established. No data are available. Method of administration Single-use container for intravitreal use only. Ranibizumab should be inspected visually for particulate matter and discoloration prior to administration. The injection procedure should be carried out under aseptic conditions, which includes the use of surgical hand disinfection, sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent) and the availability of sterile paracentesis (if required). The patient’s medical history for hypersensitivity reactions should be carefully evaluated prior to performing the intravitreal procedure (see section 4.4). Adequate anaesthesia and a broad-spectrum topical microbicide to disinfect the periocular skin, eyelid and ocular surface should be administered prior to the injection, in accordance with local practice. The injection needle should be inserted 3.5-4.0 mm posterior to the limbus into the vitreous cavity, avoiding the horizontal meridian and aiming towards the centre of the globe. The injection volume of 0.05 ml is then delivered; a different scleral site should be used for subsequent injections. 4.3 Contraindications Hypersensitivity to the active substance or to any of the excipients listed in section 6.1. Patients with active or suspected ocular or periocular infections. Patients with active severe intraocular inflammation.

Novartis Page 37 Ranibizumab (Lucentis®)
4.4 Special warnings and precautions for use Intravitreal injection-related reactions Intravitreous injections, including those with ranibizumab, have been associated with endophthalmitis, intraocular inflammation, rhegmatogenous retinal detachment, retinal tear and iatrogenic traumatic cataract (see section 4.8). Proper aseptic injection techniques must always be used when administering ranibizumab. In addition, patients should be monitored during the week following the injection to permit early treatment if an infection occurs. Patients should be instructed to report any symptoms suggestive of endophthalmitis or any of the above mentioned events without delay. Intraocular pressure increases Transient increases in intraocular pressure (IOP) have been seen within 60 minutes of injection of Lucentis. Sustained IOP increases have also been identified (see section 4.8). Both intraocular pressure and the perfusion of the optic nerve head must be monitored and managed appropriately. Bilateral treatment Limited data on bilateral use of ranibizumab (including same-day administration) do not suggest an increased risk of systemic adverse events compared with unilateral treatment. Immunogenicity There is a potential for immunogenicity with ranibizumab. Since there is a potential for an increased systemic exposure in subjects with DME, an increased risk for developing hypersensitivity in this patient population cannot be excluded. Patients should also be instructed to report if an intraocular inflammation increases in severity, which may be a clinical sign attributable to intraocular antibody formation. Concomitant use of other anti-VEGF (vascular endothelial growth factor) Ranibizumab should not be administered concurrently with other anti-VEGF medicinal products (systemic or ocular). Withholding Lucentis The dose should be withheld and treatment should not be resumed earlier than the next scheduled treatment in the event of: a decrease in best-corrected visual acuity (BCVA) of ≥30 letters compared with the last
assessment of visual acuity; an intraocular pressure of ≥30 mmHg; a retinal break; a subretinal haemorrhage involving the centre of the fovea, or, if the size of the
haemorrhage is ≥50%, of the total lesion area; performed or planned intraocular surgery within the previous or next 28 days. Retinal pigment epithelial tear Risk factors associated with the development of a retinal pigment epithelial tear after anti-VEGF therapy for wet AMD, include a large and/or high pigment epithelial retinal detachment. When initiating ranibizumab therapy, caution should be used in patients with these risk factors for retinal pigment epithelial tears.

Novartis Page 38 Ranibizumab (Lucentis®)
Rhegmatogenous retinal detachment or macular holes Treatment should be discontinued in subjects with rhegmatogenous retinal detachment or stage 3 or 4 macular holes. Populations with limited data There is only limited experience in the treatment of subjects with DME due to type I diabetes. Ranibizumab has not been studied in patients who have previously received intravitreal injections, in patients with active systemic infections, proliferative diabetic retinopathy, or in patients with concurrent eye conditions such as retinal detachment or macular hole. There is also no experience of treatment with ranibizumab in diabetic patients with an HbA1c over 12% and uncontrolled hypertension. This lack of information should be considered by the physician when treating such patients. In patients with PM, there are limited data on the effect of ranibizumab in patients who have previously undergone unsuccessful verteporfin photodynamic therapy (vPDT) treatment. Also, while a consistent effect was observed in subjects with subfoveal and juxtafoveal lesions, there are insufficient data to conclude on the effect of ranibizumab in PM subjects with extrafoveal lesions. Systemic effects following intravitreal use Systemic adverse events including non-ocular haemorrhages and arterial thromboembolic events have been reported following intravitreal injection of VEGF inhibitors. There are limited data on safety in the treatment of DME, macular oedema due to RVO and CNV secondary to PM patients with prior history of stroke or transient ischaemic attacks. Caution should be exercised when treating such patients (see section 4.8). Prior episodes of RVO, ischaemic branch RVO and central RVO There is limited experience with treatment of patients with prior episodes of RVO and of patients with ischaemic branch RVO (BRVO) and central RVO (CRVO). In patients with RVO presenting with clinical signs of irreversible ischaemic visual function loss, treatment is not recommended. 4.5 Interaction with other medicinal products and other forms of interaction No formal interaction studies have been performed. For the adjunctive use of verteporfin photodynamic therapy (PDT) and ranibizumab in wet AMD and PM, see section 5.1. For the adjunctive use of laser photocoagulation and ranibizumab in DME and BRVO, see sections 4.2 and 5.1. In clinical studies for the treatment of visual impairment due to DME, the outcome with regard to visual acuity or central retinal subfield thickness (CSFT) in patients treated with ranibizumab was not affected by concomitant treatment with thiazolidinediones.

Novartis Page 39 Ranibizumab (Lucentis®)
4.6 Fertility, pregnancy and lactation Women of childbearing potential/contraception in females Women of childbearing potential should use effective contraception during treatment. Pregnancy For ranibizumab no clinical data on exposed pregnancies are available. Studies in cynomolgus monkeys do not indicate direct or indirect harmful effects with respect to pregnancy or embryonal/foetal development (see section 5.3). The systemic exposure to ranibizumab is low after ocular administration, but due to its mechanism of action, ranibizumab must be regarded as potentially teratogenic and embryo-/foetotoxic. Therefore, ranibizumab should not be used during pregnancy unless the expected benefit outweighs the potential risk to the foetus. For women who wish to become pregnant and have been treated with ranibizumab, it is recommended to wait at least 3 months after the last dose of ranibizumab before conceiving a child. Breast-feeding It is unknown whether ranibizumab is excreted in human milk. Breast-feeding is not recommended during the use of Lucentis. Fertility There are no data available on fertility. 4.7 Effects on ability to drive and use machines The ranibizumab treatment procedure may induce temporary visual disturbances, which may affect the ability to drive or use machines (see section 4.8). Patients who experience these signs must not drive or use machines until these temporary visual disturbances subside. 4.8 Undesirable effects Summary of the safety profile The majority of adverse reactions reported following administration of ranibizumab are related to the intravitreal injection procedure. The most frequently reported ocular adverse reactions following injection of ranibizumab are: eye pain, ocular hyperaemia, increased intraocular pressure, vitritis, vitreous detachment, retinal haemorrhage, visual disturbance, vitreous floaters, conjunctival haemorrhage, eye irritation, foreign body sensation in eyes, increased lacrimation, blepharitis, dry eye and eye pruritus. The most frequently reported non-ocular adverse reactions are headache, nasopharyngitis and arthralgia. Less frequently reported, but more serious, adverse reactions include endophthalmitis, blindness, retinal detachment, retinal tear and iatrogenic traumatic cataract (see section 4.4). Patients should be informed of symptoms of these potential adverse reactions and instructed to inform their physician if they develop signs such as eye pain or increased discomfort,

Novartis Page 40 Ranibizumab (Lucentis®)
worsening eye redness, blurred or decreased vision, an increased number of small particles in their vision, or increased sensitivity to light. The adverse reactions experienced following administration of Lucentis in clinical trials are summarised in the table below. Tabulated list of adverse reactions# The adverse reactions are listed by system organ class and frequency using the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. Infections and infestations Very common Nasopharyngitis Common Urinary tract infection* Blood and lymphatic system disorders Common Anaemia Immune system disorders Common Hypersensitivity Psychiatric disorders Common Anxiety Nervous system disorders Very common Headache Eye disorders Very common Vitritis, vitreous detachment, retinal haemorrhage, visual
disturbance, eye pain, vitreous floaters, conjunctival haemorrhage, eye irritation, foreign body sensation in eyes, lacrimation increased, blepharitis, dry eye, ocular hyperaemia, eye pruritus.
Common Retinal degeneration, retinal disorder, retinal detachment, retinal tear, detachment of the retinal pigment epithelium, retinal pigment epithelium tear, visual acuity reduced, vitreous haemorrhage, vitreous disorder, uveitis, iritis, iridocyclitis, cataract, cataract subcapsular, posterior capsule opacification, punctuate keratitis, corneal abrasion, anterior chamber flare, vision blurred, injection site haemorrhage, eye haemorrhage, conjunctivitis, conjunctivitis allergic, eye discharge, photopsia, photophobia, ocular discomfort, eyelid oedema, eyelid pain, conjunctival hyperaemia.
Uncommon Blindness, endophthalmitis, hypopyon, hyphaema, keratopathy, iris adhesion, corneal deposits, corneal oedema, corneal striae, injection site pain, injection site irritation, abnormal sensation in eye, eyelid irritation.
Novartis Page 41 Ranibizumab (Lucentis®)
Respiratory, thoracic and mediastinal disorders Common Cough Gastrointestinal disorders Common Nausea Skin and subcutaneous tissue disorders Common Allergic reactions (rash, urticaria, pruritus, erythema) Musculoskeletal and connective tissue disorders Very common Arthralgia Investigations Very common Intraocular pressure increased # Adverse reactions were defined as adverse events (in at least 0.5 percentage points of patients) which occurred at a higher rate (at least 2 percentage points) in patients receiving treatment with ranibizumab 0.5 mg than in those receiving control treatment (sham or verteporfin PDT). * observed only in DME population Product-class-related adverse reactions In the wet AMD phase III studies, the overall frequency of non-ocular haemorrhages, an adverse event potentially related to systemic VEGF (vascular endothelial growth factor) inhibition, was slightly increased in ranibizumab-treated patients. However, there was no consistent pattern among the different haemorrhages. There is a theoretical risk of arterial thromboembolic events, including stroke and myocardial infarction, following intravitreal use of VEGF inhibitors. A low incidence rate of arterial thromboembolic events was observed in the ranibizumab clinical trials in patients with AMD, DME, BRVO, CRVO and PM and there were no major differences between the groups treated with ranibizumab compared to control. Reporting of suspected adverse reactions Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions. 4.9 Overdose
Cases of accidental overdose have been reported from the clinical studies in wet AMD and post-marketing data. Adverse reactions associated with these reported cases were intraocular pressure increased, transient blindness, reduced visual acuity, corneal oedema, corneal pain, and eye pain. If an overdose occurs, intraocular pressure should be monitored and treated, if deemed necessary by the attending physician.

Novartis Page 42 Ranibizumab (Lucentis®)
6. PHARMACEUTICAL PARTICULARS (Lucentis, Novartis) 6.1 List of excipients α,α-trehalose dihydrate Histidine hydrochloride, monohydrate Histidine Polysorbate 20 Water for injections 6.2 Incompatibilities In the absence of compatibility studies, this medicinal product must not be mixed with other medicinal products. 6.3 Shelf life 3 years 6.4 Special precautions for storage Store in a refrigerator (2C - 8C). Do not freeze. Keep the vial in the outer carton in order to protect from light. Prior to use, the unopened vial may be kept at room temperature (25°C) for up to 24 hours.

Novartis Page 43 Ranibizumab (Lucentis®)
REFERENCES 1. Lucentis US PI,
http://www.accessdata.fda.gov/drugsatfda_docs/label/2014/125156s105lbl.pdf, accessed on 27th Nov 2014, Lucentis EU SmPC, http://ec.europa.eu/health/documents/community-register/html/h374.htm, accessed on 17th Nov 2014.
2. Data on file. Novartis Pharma AG, Basel, Switzerland. 3. http://www.nice.org.uk/nicemedia/live/13125/53416/53416.pdf. Accessed on 28
September 2013 4. EMA. Lucentis Scientific Discussion. 2007. Available at:
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Scientific_Discussion/human/000715/WC500043550.pdf. Accessed on 28 November 2014.
5. Rosenfeld PJ, Martidis A, Tennant MTS. Age-related macular degeneration. In: Ophthalmology. 3rd edn. Yanoff M, Duker JS (editors). Philadelphia: Mosby/Elsevier, 2009: pp. 658-673
6. Friedman DS, et al. Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol. 2004 Apr;122(4):564-72.
7. Vingerling JR, et al. The prevalence of age-related maculopathy in the Rotterdam Study. Ophthalmology (1995) 102:205-210
8. Klein R, et al. Incidence of Visual Impairment Over a 20-Year Period: The Beaver Dam Eye Study. Ophthalmology (2013)
9. Hong T, et al. Long-term Changes in Visual Acuity in an Older Population over a 15-Year Period: The Blue Mountains Eye Study. Ophthalmology (2013) :1-9
10. Wilkinson CP. Classification of Diabetic Retinopathy: A Proposed International Clinical Disease Severity Grading Scale for Diabetic Retinopathy and Diabetic Macular Edema. Medscape (www.medscape.com), 2003: pp.1-9
11. Ling R, et al. Longitudinal study of a cohort of people with diabetes screened by the Exeter Diabetic Retinopathy Screening Programme. Eye (2002) 16, 140–145
12. Karia N. Retinal vein occlusion: pathophysiology and treatment options. Clinical Ophthalmology 2010:4 pp 809-816
13. Hayreh SS, et al. Incidence of various types of retinal vein occlusion and their recurrence and demographic characteristics. American Journal of Ophtalmology (1994) 117:429-441
14. Shahid H, et al. The management of retinal vein occlusion: is interventional ophthalmology the way forward? Br J Ophthalmol 2006;90:627–63
15. Rogers S, et al. The Prevalence of Retinal Vein Occlusion: Pooled Data from Population Studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010;117:313–319
16. Klein R, et al. The epidemiology of retinal vein occlusion: the Beaver Dam Eye Study. Trans Am Ophthalmol Soc. 2000;98:133-41; discussion 141-3
17. Klein R, et al. The 15-year cumulative incidence of retinal vein occlusion: the Beaver Dam Eye Study. Arch Ophthalmol. 2008 Apr;126(4):513-8. doi: 10.1001/archopht.126.4.513.

Novartis Page 44 Ranibizumab (Lucentis®)
18. Cugati S, et al. Ten-Year Incidence of Retinal Vein Occlusion in an Older Population: The Blue Mountains Eye Study. Arch Ophthalmol. 2006;124:726-732
19. Yoshida T, et al. Myopic choroidal neovascularization: A 10-year follow-up. Ophthalmology 2003;110:1297–1305.
20. Macdonald AE. Causes of blindness in Canada. An analysis of 24,605 cases registered with Canadian National Institute for Blind. Can Med Assoc J 1965;92:264-79
21. Avisar R, et al. Estimation of prevalence and incidence rates and causes of blindness in Israel, 1998-2003. Isr Med Assoc J 2006;8:880-1
22. Ghafour IM, et al. Common causes of blindness and visual handicap in the west of Scotland. Br J Ophthalmol 1983;67:209-13
23. Krumpaszky HG, et al. Blindness incidence in Germany. A population-based study from Wurttemberg-Hohenzollern. Ophthalmologica 1999;213:176-82
24. Wu L, et al. Causes and 3-year-incidence of blindness in Jing-An District, Shanghai, China 2001-2009. BMC Ophthalmol 2011;11:10
25. Ohno-Matsui K, et al. Patchy atrophy and lacquer cracks predispose to the development of choroidal neovascularisation in pathological myopia. Br J Ophthalmol 2003;87:570–573
26. Grossniklaus HE, et al. Pathologic findings in pathologic myopia. Retina. 1992;12(2):127-33.
27. Curtin BJ, et al. Axial length measurements and fundus changes of the myopic eye. Am J Ophthalmol. 1971 Jan;71(1 Pt 1):42-53.
28. Miller DG, et al. Vision loss in younger patients: a review of choroidal neovascularization. Optom Vis Sci. 2006 May;83(5):316-25.
29. Chang TS, et al. Improved vision-related function after ranibizumab treatment of neovascular age-related macular degeneration. Archives of Ophthalmology. 2007;125:1460-1469.
30. Mitchell P, et al. The RESTORE study Ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011;118:615-625.
31. Campochiaro P, et al. Ranibizumab for macular edema follwing branch retinal vein occlusion: Six-month primary end point results of a phase III study. Ophthalmology. 2010;117:1102-1112.
32. Brown D, et al. Ranibizumab for macular edema following central retinal vein occlusion: Six-month primary end point results of a phase III study. Ophthalmology. 2010;117:1124-1133.
33. Brown DM, et al. Results from year 1 of the ANCHOR Study, New England Journal of Medicine. 2006;355:1432-1444.
34. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000715/WC500043546.pdf. Accessed on 24th Nov 2014
35. Wolf, S., Balciuniene, V.J., Laganovska, G. et al. RADIANCE: a randomized controlled study of ranibizumab in patients with choroidal neovascularization secondary to pathologic myopia. Ophthalmology. 2014; 121: 682–692.

Novartis Page 45 Ranibizumab (Lucentis®)
36. Schmidt-Erfurth U, Chong V, Loewenstein A, et al. Guidelines for the management of neovascular age-related macular degeneration by the European Society of Retina Specialists (EURETINA). The British Journal of Ophthalmology. Sep 2014;98(9):1144-1167.
37. The CATT Research Group. Ranibizumab and Bevacizumab for Treatment of Neovascular Age-Related Macular Degeneration, Ophthalmology, April 30, 2012.
38. The CATT Research Group. Ranibizumab and Bevacizumab for Neovascular Age-Related Macular Degeneration. N Engl J Med, April 28, 2011 (10.1056/NEJMoa1102673)
39. The CATT Research Group. Ranibizumab and Bevacizumab for Neovascular Age-Related Macular Degeneration. N Engl J Med, April 28, 2011 (10.1056/NEJMoa1102673)
40. The IVAN Study Investigators, Ranibizumab versus Bevacizumab to Treat Neovascular Age-related Macular Degeneration. One-Year Findings from the IVAN Randomized Trial, Ophthalmology 2012;119:1399-1411.
41. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002392/WC500135744.pdf. Accessed on 28
September 2013. 42. Roche. Avastin Summary of Product Characteristics;
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000582/WC500029271.pdf. Accessed 23 November, 2014.
43. Avery RL, Castellarin AA, Steinle NC, et al. Systemic pharmacokinetics following intravitreal injections of ranibizumab, bevacizumab or aflibercept in patients with neovascular AMD. The British Journal of Ophthalmology. Jul 7 2014 doi: 10.1136/bjophthalmol-2014-305252 (Epub ahead of print).
44. Papadopoulos N, Martin J, Ruan Q, et al. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis. Jun 2012;15(2):171-185.
45. Chen HX, Cleck JN. Adverse effects of anticancer agents that target the VEGF pathway. Nature Reviews. Clinical Oncology. Aug 2009;6(8):465-477.
46. Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results. Ophthalmology. Jul 2012;119(7):1388-1398.
47. Martin DF, Maguire MG, Ying GS, Grunwald JE, Fine SL, Jaffe GJ. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. The New England Journal of Medicine. May 19 2011;364(20):1897-1908.
48. Chakravarthy U, Harding SP, Rogers CA, et al. Alternative treatments to inhibit VEGF in age-related choroidal neovascularisation: 2-year findings of the IVAN randomised controlled trial. Lancet. Oct 12 2013;382(9900):1258-1267.
49. Chakravarthy U, Harding SP, Rogers CA, et al. Ranibizumab versus bevacizumab to treat neovascular age-related macular degeneration: one-year findings from the IVAN randomized trial. Ophthalmology. Jul 2012;119(7):1399-1411.
50. Kodjikian L, Souied EH, Mimoun G, et al. Ranibizumab versus Bevacizumab for Neovascular Age-related Macular Degeneration: Results from the GEFAL Noninferiority Randomized Trial. Ophthalmology. Nov 2013;120(11):2300-2309.

Novartis Page 46 Ranibizumab (Lucentis®)
51. Berg K, Pedersen TR, Sandvik L, Bragadottir R. Comparison of Ranibizumab and Bevacizumab for Neovascular Age-Related Macular Degeneration According to LUCAS Treat-and-Extend Protocol. Ophthalmology. Sep 13 2014.
52. Schmucker C, Ehlken C, Agostini HT, et al. A safety review and meta-analyses of bevacizumab and ranibizumab: off-label versus goldstandard. PloS One. 2012;7(8):e42701.
53. Kodjikian L, Decullier E, Souied EH, et al. Bevacizumab and ranibizumab for neovascular age-related macular degeneration: an updated meta-analysis of randomised clinical trials. Graefe's Archive for Clinical and Experimental Ophthalmology = Albrecht von Graefes Archiv fur Klinische und Experimentelle Ophthalmologie. Oct 2014;252(10):1529-1537.
54. Moja L, Lucenteforte E, Kwag KH, et al. Systemic safety of bevacizumab versus ranibizumab for neovascular age-related macular degeneration. The Cochrane Database of Systematic Reviews. 2014;9:CD011230.
55. Curtis LH, Hammill BG, Schulman KA, Cousins SW. Risks of mortality, myocardial infarction, bleeding, and stroke associated with therapies for age-related macular degeneration. Archives of Ophthalmology. Oct 2010;128(10):1273-1279.
56. Gower EW, Cassard S, Chu, L., et al. Adverse event rates following intravitreal injection of Avastin or Lucentis for treating age-related macular degeneration. Presentation #6644 at Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting, May 3rd 2011.
57. USP 28/NF 23. Chapter <788> Particulate Matter in Injections. 58. USP 28/NF 23. Chapter <789> Particulate Matter in Ophthalmic Solutions. 59. Kahook MY, Liu L, Ruzycki P, et al. High-molecular-weight aggregates in repackaged
bevacizumab. Retina. Jun 2010;30(6):887-892. 60. Wickremasinghe SS, Michalova K, Gilhotra J, et al. Acute intraocular inflammation after
intravitreous injections of bevacizumab for treatment of neovascular age-related macular degeneration. Ophthalmology. Nov 2008;115(11):1911-1915.
61. Food and Drug Administration. Recalls, Market Withdrawals and Safety Alerts - Clinical Specialities Issues Voluntary Nationwide Recall of Avastin Unit Dose Syringes due to Potential Serious Eye Infection. 2013; http://www.fda.gov/Safety/Recalls/ucm344377.htm. Accessed 13 October, 2014.
62. Medicines and Healthcare Products Regulatory Agency. Company-led drug recall: Bevacizumab Intravitreal Injection 1.25mg/0.05ml - Moorfields Pharmaceuticals - CLDA(12)A/04.
63. http://www.nice.org.uk/nicemedia/live/13125/53416/53416.pdf. Accessed on 28 September 2013.
64. Pollack A. Avastin injections are reported to cause blindness. New York Times, 30th August 2011. Available at http://www.nytimes.com/2011/08/31/health/31drug.html
65. FDA. FDA alerts Health Care Professionals of infection risk from repackaged Avastin intravitreal injections (30 August 2011) available at http://www.fda.gov/Drugs/DrugSafety/ucm270296.htm

Novartis Page 47 Ranibizumab (Lucentis®)
66. Medicines and Healthcare products Regulatory Agency. Company-led drug recall: Bevacizumab Intravitreal Injection 1.25mg/0.05ml - Moorfields Pharmaceuticals - CLDA(12)A/04.
67. FDA. Recalls, Market Withdrawals, & Safety Alerts - Clinical Specialties Issues Voluntary Nationwide Recall of Avastin Unit Dose Syringes due to Potential Serious Eye Infection; March 18 2013 available at http://www.fda.gov/Safety/Recalls/ucm344377.htm
68. Kahook MY, Liu L, Ruzycki P et al. High-molecular-weight aggregates in repackaged bevacizumab. Retina 2010;30:887-92.
69. Palmer JM, Amoaku WM, Kamali F. Quality of bevacizumab compounded for intravitreal administration. Eye (Lond) 2013.
70. Gower EW, Cassard S, Chu L, Varma R, Klein R. Adverse event rates following intravitreal injection of avastin or lucentis for treating age-related macular degeneration. Abstract presented at ARVO meeting, May 2011, Fort Lauderdale, Florida. Invest Ophthalmol Vis Sci 2011;129.
71. http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000582/WC500029271.pdf. Accessed on 28 September 2013.
72. http://cteu.bris.ac.uk/trials/ivan/PIGPSafetyLetter.pdf. Accessed on 28 September 2013. 73. Hazell L, Shakir SA. Under-reporting of adverse drug reactions: a systematic review.
Drug Safety: an International Journal of Medical Toxicology and Drug Experience. 2006;29(5):385-396.
74. http://www.federanziani.it/2014/10/federanziani-allaifa-e-ai-nas-sospendere-immediatamente-l%e2%80%99uso-di-avastin-in-oftalmologia/. Accessed on 25 November 2014.
75. http://www.agenziafarmaco.gov.it/sites/default/files/comunicatistampa/COMUNICATO%20AIFA%20N%20391%20-%20AIFA%20-%20Valuteremo%20con%20attenzione%20i%20dati%20FederAnziani-FIMMG%20su%20potenziali%20reazioni%20avverse%20bevacizumab.pdf Accessed on 25 November 2014.
76. http://www.bbc.com/news/health-30138097. Accessed on 25 November 2014. 77. NICE technology appraisals [TA155], http://www.nice.org.uk/guidance/TA155. Revised
May 2012. Accessed on 25 November 2014. 78. NICE technology appraisals [TA274], http://www.nice.org.uk/guidance/TA274. Published
April 2013. Accessed on 25 November 2014. 79. NICE technology appraisals [TA283], http://www.nice.org.uk/guidance/TA283. Published
May 2013. Accessed on 25 November 2014. 80. NICE technology appraisals [TA298], http://www.nice.org.uk/guidance/TA298. Published
November 2013. Accessed on 25 November 2014. 81. SMC Advice on DME,
https://www.scottishmedicines.org.uk/SMC_Advice/Advice/711_11_ranibizumab_lucentis/ranibizumab_Lucentis_Resubmission. Published 10 December 2012. Accessed on 25 November 2014.
Novartis Page 48 Ranibizumab (Lucentis®)
82. SMC Advice on CRVO, https://www.scottishmedicines.org.uk/SMC_Advice/Advice/732_11_ranibizumab_Lucentis/ranibizumab_Lucentis. Published 7 November 2011. Accessed on 25 November 2014.
83. SMC Advice on BRVO, https://www.scottishmedicines.org.uk/SMC_Advice/Advice/732_11_ranibizumab_Lucentis/ranibizumab_Lucentis_Resubmission. Published 13 May 2013. Accessed on 25 November 2014.
84. SMC Advice on mCNV, https://www.scottishmedicines.org.uk/SMC_Advice/Advice/907_13_ranibizumab_Lucentis/ranibizumab_Lucentis. Published 11 November 2013. Accessed on 25 November 2014.
85. Lozano-Ortega G et al. The cost-effectiveness of ranibizumab compared to PDT-V and BSC for the treatment of age-related Macular Degeneration in Canada, abstract presented at ISPOR 2008; available from http://www.valueinhealthjournal.com/article/S1098-3015(10)70900-1/pdf, consulted in November, 24th 2014
86. Haig J et al. Economic Evaluation of Ranibizumab for the treatment of Diabetic Macular in Canada, abstract presented at ISPOR 2011; available from http://www.valueinhealthjournal.com/article/S1098-3015(11)00679-6/pdf, consulted in November, 24th 2014
87. Haig J et al. Economic Evaluation of Ranibizumab for the treatment of Macular Edema Secondary to Branch and Central Retinal Vein occlusion in Canada, abstract presented at ISPOR 2012; available from: http://www.valueinhealthjournal.com/article/S1098-3015(12)03778-3/pdf, consulted in November, 24th 2014
88. PBAC Advice on wAMD, http://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/pbac-outcomes/2009-03/a_positive_recommendations. Accessed on 28th November 2014.
89. PBAC Advice on DME and RVO, http://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/pbac-outcomes/2014-07. Accessed on 28th November 2014.
90. Hernandez-Pastor LJ, Ortega A, Garcia-Layana A, Giraldez J. Cost-effectiveness of ranibizumab compared with pegaptanib in neovascular age-related macular degeneration. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie 2010;248:467-76.
91. Hernandez-Pastor LJ, Ortega A, Garcia-Layana A, Giraldez J. Cost-effectiveness of ranibizumab compared with photodynamic treatment of neovascular age-related macular degeneration. Clinical therapeutics 2008;30:2436-51.
92. Brown A, Hodge W, al. e. Management of neovascular age-related macular degeneration: systematic drug class review and economic evaluation. Ottowa: Canadian Agency for Drugs and Technologies in Health 2008.
93. Common Drug Review. Ranibizumab (Lucentis-Novartis Pharmaceuticals Canada Inc.), Indication – Age-related macular degeneration (AMD): Overview of CDR clinical and pharmacoeconomic reports August 2008. Ottowa: Canadian Agency for Drugs and Technologies in Health 2008.

Novartis Page 49 Ranibizumab (Lucentis®)
94. Colquitt JL, Jones J, Tan SC et al. Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation. Health technology assessment 2008;12:iii-iv, ix-201.
95. Moeremans K, Gerlier L, Mitchell P, Gallagher M, Vincze G. Cost-utility analysis of a PRN (as needed) treatment schedule with ranibizumab (Lucentis®) in nAMD based on clinical evidence: A401. Value in health 2010;13:A401.
96. Fletcher EC, Lade RJ, Adewoyin T, Chong NV. Computerized model of cost-utility analysis for treatment of age-related macular degeneration. Ophthalmology 2008;115:2192-8.
97. Arreola-Ornelas H. Cost-effectiveness of ranibizumab in patients with neovascular wet age-related macular degeneration (NAMD) at the Mexican social security system (IMSS): A251. Value in Health 2012;15:A251.
98. Athanasakis K, Fragoulakis V, Tsiantou V et al. Cost-effectiveness analysis of ranibizumab versus verteporfin photodynamic therapy, pegaptanib sodium, and best supportive care for the treatment of age-related macular degeneration in Greece. Clinical therapeutics 2012;34:446-56.
99. Maniadakis N AK, Fragoulakis V, Tsiantou V, Kyriopoulos J. Economic evaluation of ranibizumab in the treatment of age-related macular degeneration in Greece: A399. Value in health 2010;13:A399.
100. Moeremans K, Gerlier L, Drieskens S et al. Cost-utility analysis of ranibizumab in wet-amd based on real-life data collected in the helios study after ranibizumab; Value in health 2011;14:A55.
101. Gower EW, Cassard SD, Bass EB, Schein OD, Bressler NM. A cost-effectiveness analysis of three treatments for age-related macular degeneration. Retina 2010;30:212-21.
102. Dewan V, Lambert D, Edler J, Kymes S, Apte RS. Cost-effectiveness analysis of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology 2012;119:1679-84.
103. Mitchell P, Annemans L, Gallagher M et al. Cost-effectiveness of ranibizumab in treatment of diabetic macular oedema (DME) causing visual impairment: evidence from the RESTORE trial. British journal of ophthalmology 2012;96:688-93.