fluids and 1 pediatrics - nursing lijan
TRANSCRIPT
FLUIDS ANDELECTROLYTES IN
PEDIATRICSInshirah qadri
1

Objectives▪ To recognize of the proper procedure of peripheral IV
access in pediatrics. identify▪ To review types of IV fluids used in children.▪ To identify basics fluid maintenance and requirement of
fluid ,electrolyte, & nutrition according to age.▪ To identify of the proper procedure of IV-formula
preparation and administration in pediatrics.▪ To identify basic concept of fluid balance in pediatrics.▪ To recognize Common complication of IV therapy.
2

Proper Procedure ofPeripheral IV Access in
Children• Important Concepts
• All procedures at a treatment room• The site selected for peripheral intravenous
perfusion depend on accessibility andconvenience.
• To Get Better IV access you can…• Number of IV access Attempts…
3

Developmental Considerations• INFANT
• Handle infant gently, speak softly• Avoid arm used for thumb sucking• Hold immediately after insertion• Don’t feed immediately prior to insertion• Avoid presence of extra personnel to
minimize stranger anxiety
4

Developmental Considerations• TODDLER/ PRESCHOOLER:
• Prepare child immediately prior toprocedure
• Give simple explanations in concreteterms
• Explain that you will help child hold still• Emphasize that the IV is not punishment
5
DevelopmentalConsiderations• SCHOOL-AGER
• Prepare child ahead of time, but on theday of insertion only
• Give the child choices as appropriate• Give positive reinforcement after
completion
6

DevelopmentalConsiderations
• ADOLESCENT
▪ Prepare teenager several hours to a daybefore procedure
▪ Approach discussions on a more adultlevel
▪ Discuss fears related to procedure▪ Include teenager in decisions
7

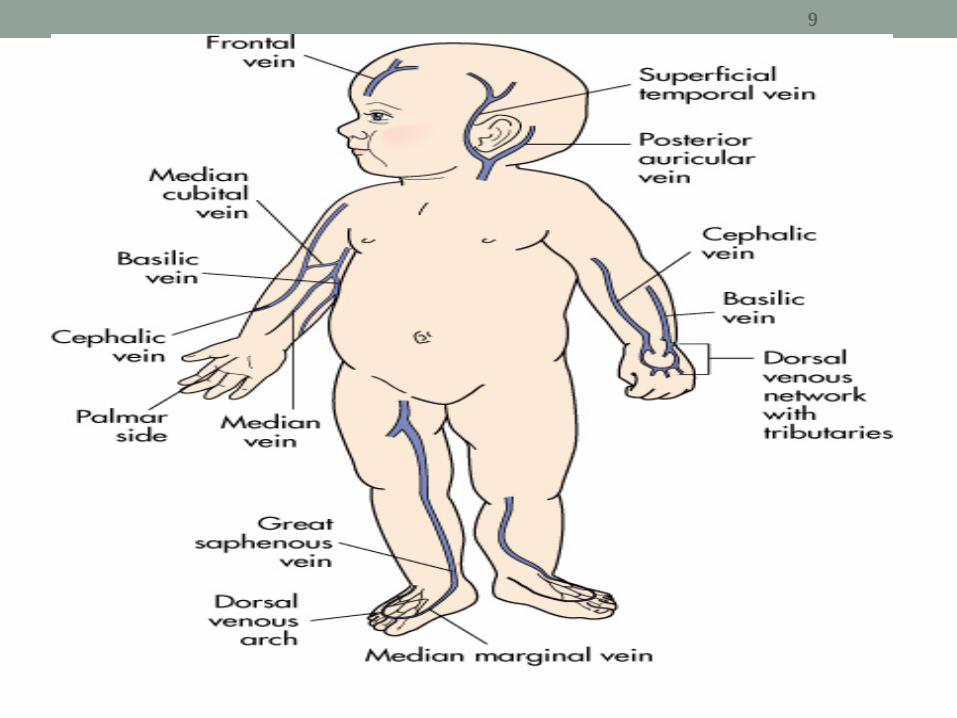
Pediatric Optimal Locations• Hands• Forearm• Feet• Scalp
8
9

Pediatric Catheter Gauges• Use the largest catheter you can successfully insert• Catheter Sizes:
Newborn: 24, 22 gaugeInfant < 1 year: 24, 22 gauge1 – 8 years: 22, 20, 18 gauge8 years and older: 20, 18, 16 gauge
10

EMLA Cream• EMLA Cream is a topical anesthetic• Minimizes or prevents pain from needle puncture for an
IV, blood sample, or implanted port access.• Apply EMLA cream to the selected site 60 minutes before
the procedure.• Cover at least two sites in case the first attempt is not
successful.
11

12

Basic Concept :-Osmotic Pressure
13

Basic Concept :-Osmolality of the bloodIsotonicity of Blood ~ 275-315 mOsm/L
• Solutions having the same osmotic pressure asthat of blood are said to be isotonic with blood.
• Solutions with a higher osmotic pressure thanbody fluids are called hypertonic
• Solutions with a lower osmotic pressure arecalled hypotonic.
14

15

16

Types of IV fluids in children▪ 5% glucose in water (G/W or D/W)▪ G/W 10%, 20%.Give only via a central line as 1-2ml/kg bolus for hypoglycemia.
Monitor blood glucose▪ 25% or 50% glucose in water
Never as an infusionOnly used in NICU and at low vol. e.
g.: 1-2mls/hr via central line
▪ 0.9% NaCl(Normal Saline)
▪ 0.45% NaCl
17

18
Types of IV fluidsCont….▪ Glucose saline; G/S (G/W+ electrolytes)
different concentration of electrolytes, but all prepared in5% G/W
▪ G/S; 0.18% ,fifth (1/5 ) NaCL▪ G/S; 0.45%, half (1/2 ) NaCL
G/S 0.18% , G/S0.45%: Pediatric formulas most commonused in pediatric floors.
18

Types of IV fluids Cont….⚫ Ringer Lactate :
0-10 gram glucose/100ccNa 130 mEq/LNaHCO3 28 mEq/L as lactate
K 4 mEq/L273 mOsm/L
⚫ Water for injection
19

IVF - basic ConceptsCorrect :▪ Patient Name▪ Type▪ Dose▪ Route▪ Check IV site▪ Time▪ Documentation
IVF Calculation: according to the setFlow rate =total volume X dropping factor time in minutes
20
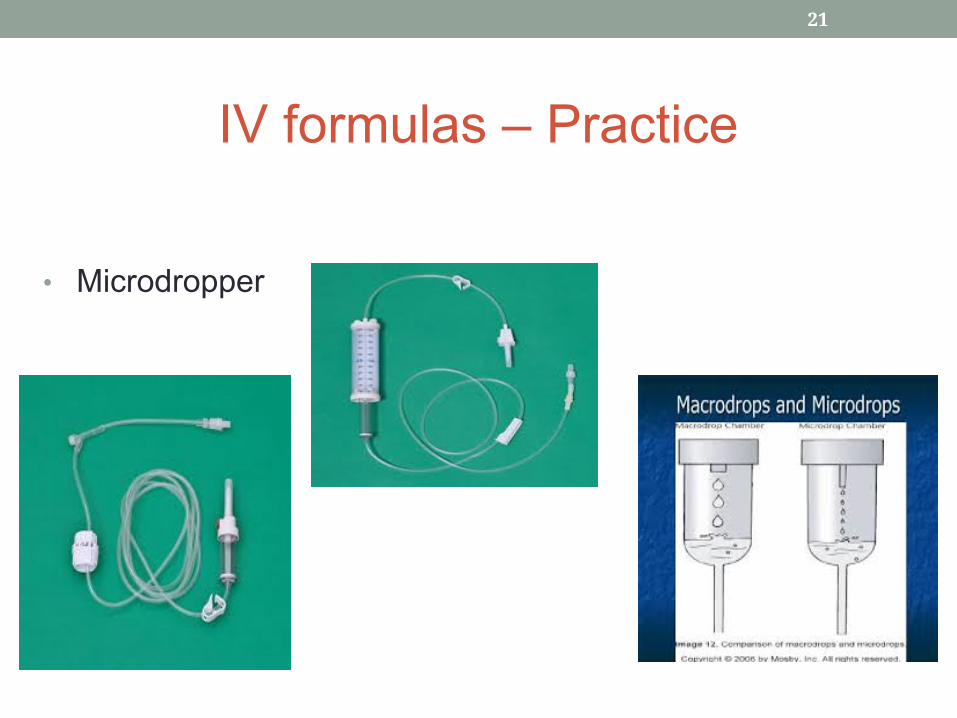
IV formulas – Practice
• Microdropper
21

Maintenance Electrolyte Requirements
• Maintenance KRequirements:
1-2 mEq/100ml /day OR 1-2mEq/kg/day
• Maintenance CaRequirements:
IV: 60 to 100 mg/kg/day
22

Daily Nutritional RequirementProtein
(g/kg/d)Calories
(kcal/kg/d)Age
1.5601-3days2.712010 days
1.6-21253- 12mo.1901- 4Yr
0.9804 -7Yr0.9707 - 10Yr0.86013 - 18Yr0.850Adult
1 gm glucose = 3.4 calorie inIVF
23

Calculation of Maintenance FluidRequirements…the Holliday-Segar
Method
24
Calculation of Maintenance FluidRequirements…
A 9 –kg child would require ?14- kg child would require ??A 32-kg child would require???
25

26
Examples
• Weight
8Kg
15Kg
27Kg
• Maintenance fluid
100ml/Kg/day=800ml/day
1000ml+(50ml/kg*5)=1000+250=1250 ml/day 1500ml+(20ml/Kg*7)=1500+140=1640 ml/day
26

Class activity• A 7 –kg child would require ?
• 13- kg child would require ??
• A 34-kg child would require???
27

Phase I: Resuscitation usingIsotonic Fluids (NS/LR) at 20ml/kg.
Re-evaluation until urine outputand dehydration signs improved
Phase II: Calculate maintenance &deficit fluid
Determine if Isotonic, Hypotonic orHypertonic Dehydration
HypotonicNa <130
Isotonic130< Na <150
HypertonicNa >150Replace
fluids over48hrs**
Deficits28
Resuscitation phaseGoal: Restore circulation, re-perfuse brain, kidneys
▪ Mild-Moderate 20 mL/kg bolus given over 30 – 60 minutes.
▪ Severe May repeat bolus as needed (ideally up to60ml/kg)Fluids – something isotonic such as Normal saline (NS) orlactated ringers (LR)
29

Replacement PhaseStabilization Phase
(For Isotonic/Hypotonic Dehydration)• Goal: Replace deficit of fluids and electrolytes according
to Holliday Segar formula
ReplacementPhase1st 8 hrs
Stabilization PhaseNext 16 hrs
MIVF andMaint Na
1/3 2/3
Deficit Fluid &Deficit Na
1/2 1/2
Kathleen Asas, MD.MPH
30
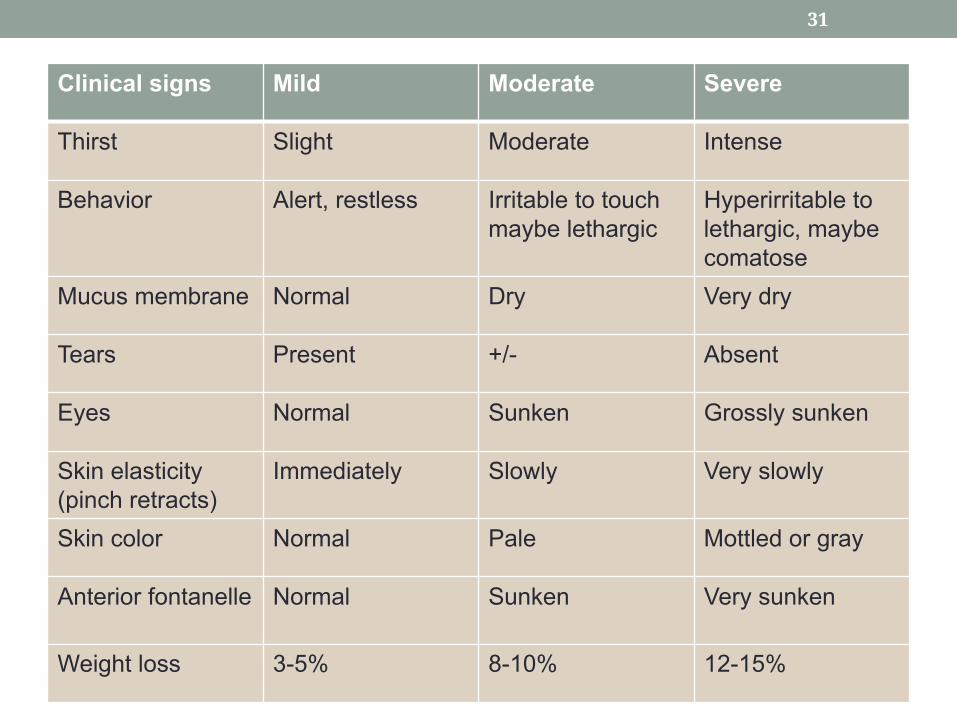
Clinical signs Mild Moderate Severe
Thirst Slight Moderate Intense
Behavior Alert, restless Irritable to touchmaybe lethargic
Hyperirritable tolethargic, maybecomatose
Mucus membrane Normal Dry Very dry
Tears Present +/- Absent
Eyes Normal Sunken Grossly sunken
Skin elasticity(pinch retracts)
Immediately Slowly Very slowly
Skin color Normal Pale Mottled or gray
Anterior fontanelle Normal Sunken Very sunken
Weight loss 3-5% 8-10% 12-15%
31

CaseOmer admitted to pediatric floor as case of dehydration ,mother said baby had poor sucking and hypoactivity ,weight loss 2 kg , current weight 12kg .
▪ Identify the level of dehydration▪ Calculate the fluid deficit.▪ Calculate replacement phase(1st 8 hrs).▪ Calculate Stabilization Phase(Next 16 hrs).▪ Calculate micro-drop of fluid deficit for both phases.▪ Write additional signs of dehydration.
32
Fluid deficit …… Case answer
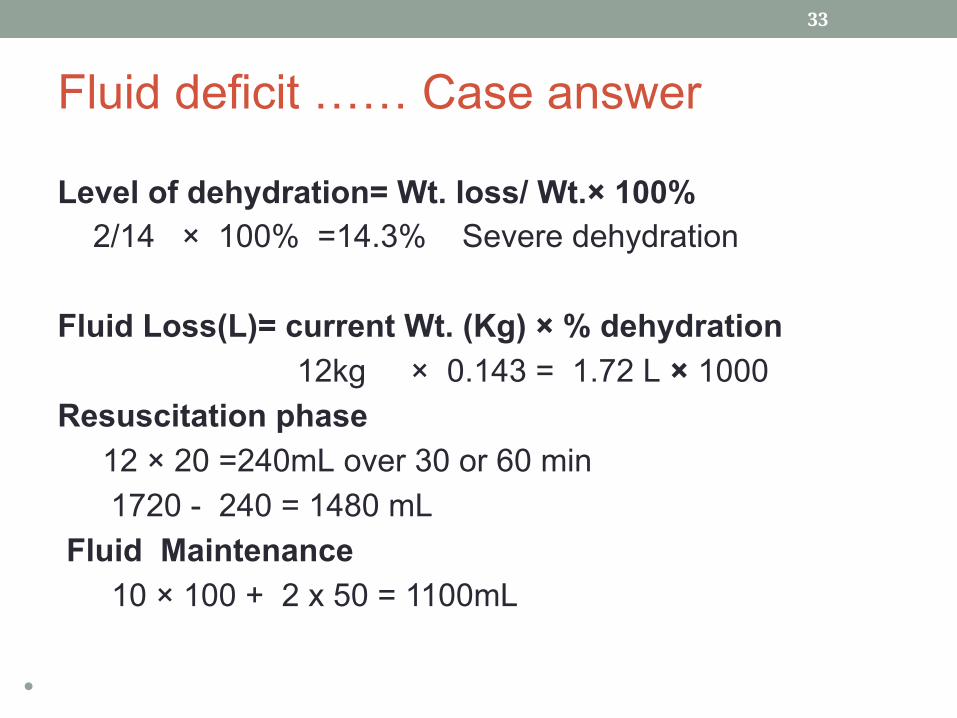
Level of dehydration= Wt. loss/ Wt.× 100% 2/14 × 100% =14.3% Severe dehydration
Fluid Loss(L)= current Wt. (Kg) × % dehydration 12kg × 0.143 = 1.72 L × 1000Resuscitation phase 12 × 20 =240mL over 30 or 60 min 1720 - 240 = 1480 mL Fluid Maintenance 10 × 100 + 2 x 50 = 1100mL
• Replacement Phase
33

Case answer• Replacement Phase(1st 8 hrs)1/3(Fluid Maintenance) + ½ (Remain fluid deficit)1/3 × 1100 mL + ½ × 1480 mL= 366mL + 740 = 1106 mL /8hrs
1106 mL / 8 hr = 138 mL/hr →138/60x60=138microdrop/min
• Stabilization Phase(Next 16 hrs) 2/3(Fluid Maintenance) + ½ (Remain fluid deficit) 2/3 × 1100 mL + ½ x1480 mL = 733 + 740 mL = 1473mL /16 hrs
• 1473mL / 16 hr = 92mL/hr → 92/60x60=92microdrop/min
34

Case answer• Intense thirst , Hyperirritable to lethargic, maybe
comatose, mottled or gray of skin color & poor elasticity, very dry mucus membrane, grossly sunken eyes & absent
tears, Very sunken anterior fontanel if less 2years old,
35

36

37

Common complication of PediatricIV therapy
• Mechanical factors shorten IV infusion dwellingtime
Insertion siteLength of catheterSize of vesselVessel fragilityActivity level of the patientForceful administration of boluses of fluidInfusion or irritants through small vessels.
38

I. Infiltration :- accumulation of fluid inthe tissue surrounding an IV needle site.
39

Cause :- penetration of the vein wall by the needle.
Signs & symptoms:-1� Flow rate may or may not be slow OR no flow of
solution .2� Infusion site is cool & hard to touch.3� Patient complain of pain, tenderness, burning or
irritation at infusion site.4� Fluid leaking around infusion site.
40

Common complication of IVtherapy cont….Corrective actions:-1� Stop IV infusion immediately & remove needle.2� Elevate extremity.3� IF noticed within 30 minutes of onset apply ice to the
swelling.4� IF noted later than 30 minutes of onset, apply warm
compresses to encourage absorption.5� Notify supervisor about infiltration.6� Restart IV in another location.7� Document observations & actions.
41
Common complication of IVtherapy cont….
II. Phlebitis:- (inflammation of the wall of thevein)
Causes:-1� Injury to the vein during puncture.2� From later needle movement.3� Irritation to vein as a result of long –term therapy.
42
Signs and symptoms:-1� Swelling around the infusion site.2� Patient complains of pain and tenderness.3� Redness and warmth along the vein.
Correctives actions:-1� Stop IV infusion immediately.2� Report observations to supervisors.3� Document observations and actions.
43
III. Air embolism :-The obstruction of blood vessels usually occurring
in the lungs or the heart by air carried via theblood stream.
❖ Causes:-1� Failure to remove air from tubing.2� Allowing the solution to run dry.3� Disconnected IV tubing.
44

Signs & symptoms:-1� Weak, rapid pulse.2� Cyanosis.3� Chest pain.
Corrective actions:-1� Notify supervisor & physician immediately.2� Immediately place patient on Lt side with feet elevated
to allow the pulmonary artery to absorb small airbubbles.
3� Administer O2 as needed.
45

Common complication of IVtherapy cont….IV. Circulatory over load:- An increased blood volume resulting from
excessive IV fluid being infused too rapidlyinto the vein.
Causes:-1. Fluid delivered too fast.2. Reduced kidney function.3. Congestive heart failure or cardiac
insufficiency.
46

Signs & symptoms1. High blood pressure.2. Distended neck veins.3. Rapid breathing, shortness of breath, tachycardia.4. Fluid intake is much greater than urinary out put
(positive balance).
47

Corrective actions:-1. Decrease flow rate.2. Place the patient in semi-sitting position to
facilitate breathing.3. Notify supervisor immediately.4. Record observations & actions taken.
48
Common complication of IVtherapy cont….
V . InfectionCauses:-1. Use of contaminated equipment.2. Poor aseptic technique.3. Contaminated site or IV equipment not
changed regularly.
49

Signs & symptoms:-1. Redness, swelling & soreness around IV site.2. Sudden rise in temperature & pulse.3. Drainage from IV site.
Corrective actions:- 1.Notify supervisor immediately.
2. Discontinue IV & take culture of wound toidentify pathogens present.
3. Use strict aseptic technique when cleaning &dressing the wound.
50

51

END LECTUREThank you
52