fluid balance and venous access in children
DESCRIPTION
pediatric surgeryTRANSCRIPT

Fluid balance and vascular Fluid balance and vascular accessaccess
in Children in Children
ByBy
Khaled AshourKhaled Ashour
Paediatric Surgery Paediatric Surgery DepartmentDepartment

What should we know?What should we know?
Distribution of body fluids Distribution of body fluids in infants & children.in infants & children.
Why are children more Why are children more vulnerable for fluid vulnerable for fluid imbalance.imbalance.
Fluid requirements for all Fluid requirements for all age groups.age groups.
Assessment of state of Assessment of state of hydration.hydration.
Vascular access.Vascular access.

•Fluid balance is fundamental to life.
•Monitoring and maintaining fluid balance in sick children requires an understanding of normal requirements and losses and of the effect of different clinical problems on fluid balance.

Why children are more prone Why children are more prone for fluid imbalance and for fluid imbalance and
dehydration?dehydration? Large body surface areaLarge body surface area High extracellular fluid High extracellular fluid
ratio.ratio. Difficult calculation of the Difficult calculation of the
accurate requirement.accurate requirement. Prematurity of kidneys.Prematurity of kidneys. Frequent feeding problemsFrequent feeding problems Difficult venous access.Difficult venous access. Relatively small total body Relatively small total body
fluids.fluids.

Normal body waterin children (Metheny and Snively 1983)
Age group Approx water content in body
Premature infant 90%Newborn infant 70-80%12-24 months 64%Adult 60%


Intracellular fluid Interstitial fluid
Intravascular fluid

Fluid distribution according to age(Hiu Lam 1998, Metheny and Snively 1983)
Intracellular Intracellular fluidfluid
Extracellular Extracellular fluidfluid
NewbornNewborn 47%47% 53%53%
12 months12 months 53%53% 47%47%
24 months24 months 60%60% 40%40%
Adult maleAdult male 67%67% 33%33%
Infants versus older children regarding extracellular fluid
Infants have a greater proportion of extracellular fluid than older children and adults.
Because extracellular fluid is more easily lost from the body than intracellular fluid, infants are more at risk of developing dehydration than older children and adults (infants also have a larger surface area to body mass ratio).
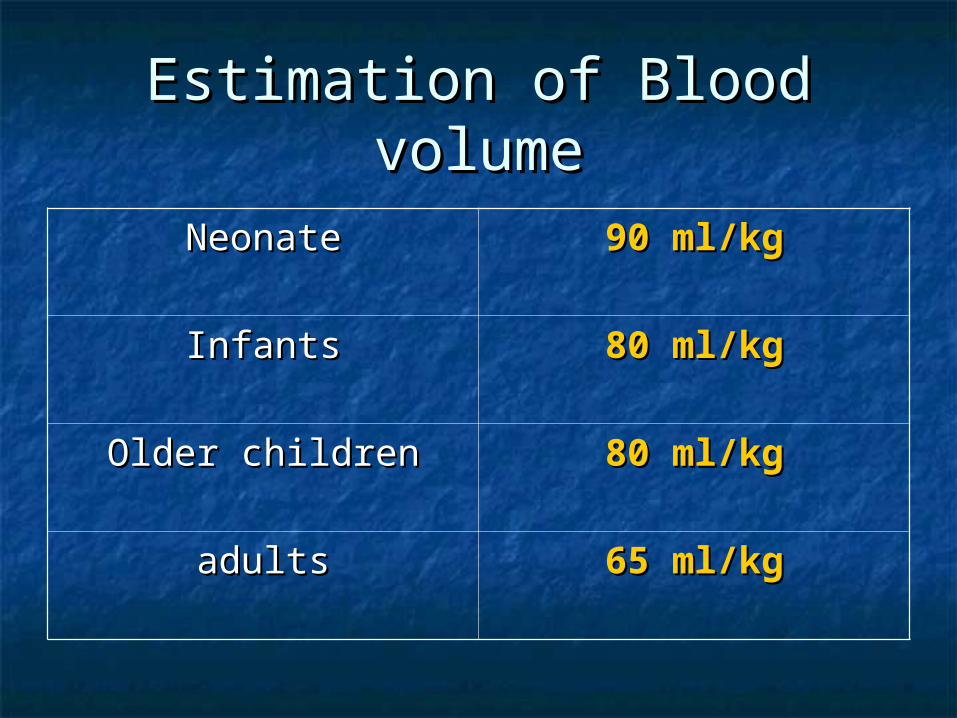
Estimation of Blood volumeEstimation of Blood volume
NeonateNeonate 90 ml/kg90 ml/kg
InfantsInfants 80 ml/kg80 ml/kg
Older childrenOlder children 80 ml/kg80 ml/kg
adultsadults 65 ml/kg65 ml/kg

Importance of balanced & Importance of balanced & adequate body fluidadequate body fluid
Balanced adequate body fluid is very Balanced adequate body fluid is very important in maintaining adequate important in maintaining adequate and effective circulation.and effective circulation.
Adequate circulation in turns will Adequate circulation in turns will maintain normal tissue perfusion, maintain normal tissue perfusion, and hence, all body cells will get and hence, all body cells will get adequate nutrition, and get rid of adequate nutrition, and get rid of waste products.waste products.

Factors affecting tissue Factors affecting tissue perfusionperfusion
Dynamic movement of body fluid Dynamic movement of body fluid between the vascular spaces and between the vascular spaces and the tissues. the tissues.
1.1. Osmotic pressure.Osmotic pressure.
2.2. Oncotic pressure.Oncotic pressure.
3.3. Hydrostatic pressure. Hydrostatic pressure.

Tissue perfusion regulationTissue perfusion regulation

Fluid intake & lossFluid intake & loss
ININ Oral fluids.Oral fluids. Food.Food. Retention enemaRetention enema Parentral:Parentral:
IVIV
IOIO
PeritonealPeritoneal
OUTOUT Urine.Urine. Stool.Stool. Perspiration.Perspiration. Bleeding.Bleeding. Surgical drains.Surgical drains. Stoma.Stoma. Burns.Burns.

How can we maintain the fluid How can we maintain the fluid balance in sick babies and balance in sick babies and
children?children?
Fluid requirement for Fluid requirement for neonates, infants & Children neonates, infants & Children
How much?? How much?? Amount of fluidAmount of fluid How?? How?? Route of administrationRoute of administration What?? What?? Type of fluidType of fluid

How much to give?How much to give?Amount of fluidAmount of fluid
Parameters of requirements:Parameters of requirements:
1) Resuscitation:1) Resuscitation:
Replacement of previous loss Replacement of previous loss
2) Maintenance fluid:2) Maintenance fluid:
Daily requirements.Daily requirements.
3) Ongoing loss:3) Ongoing loss:
NG suction, stoma out put, etc..NG suction, stoma out put, etc..

1) Resuscitation 1) Resuscitation
Given in case of initiating treatment Given in case of initiating treatment for a dehydrated child, or with acute for a dehydrated child, or with acute fluid loss.fluid loss.
Rate of 10-20 ml/kg N saline.Rate of 10-20 ml/kg N saline. Child is to be reviewed / 15 min.Child is to be reviewed / 15 min. Can be repeated.Can be repeated.

2) Maintenance2) MaintenanceA – Neonates <44 weeksA – Neonates <44 weeks
require more than require more than infants and infants and childrenchildren
DayDay ml/kg/dayml/kg/day
00 4040
11 6060
22 8080
33 100100
44 120120
55 150150
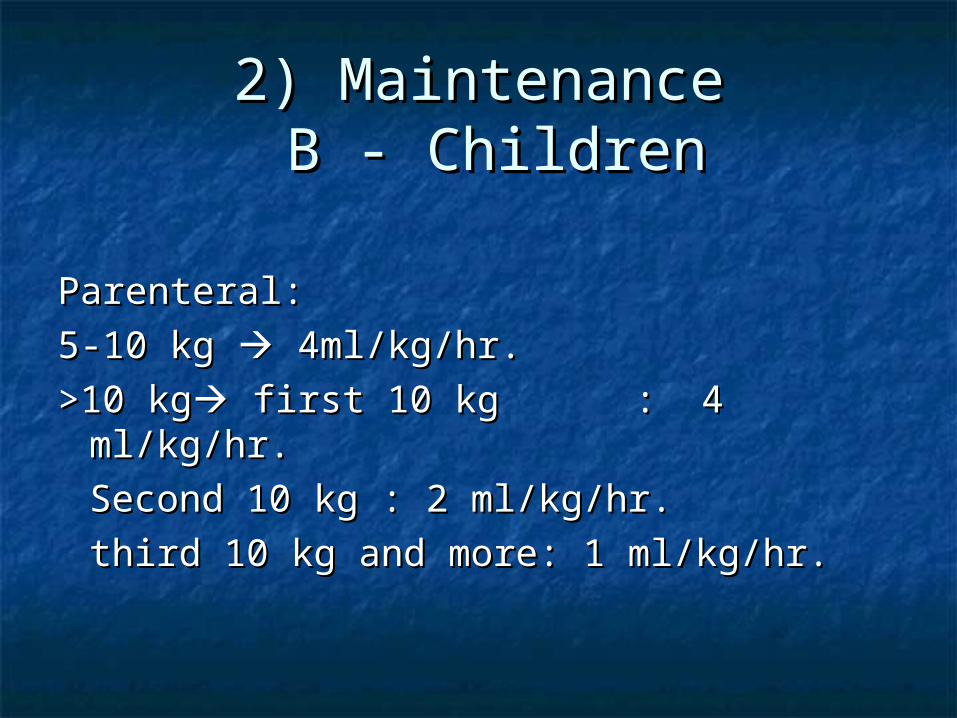
2) Maintenance2) Maintenance B - Children B - Children
Parenteral: Parenteral:
5-10 kg 5-10 kg 4ml/kg/hr. 4ml/kg/hr.
>10 kg>10 kg first 10 kg : 4 ml/kg/hr. first 10 kg : 4 ml/kg/hr.
Second 10 kg : 2 ml/kg/hr.Second 10 kg : 2 ml/kg/hr.
third 10 kg and more: 1 third 10 kg and more: 1 ml/kg/hr.ml/kg/hr.

3) Ongoing loss3) Ongoing loss
The amount depends upon the The amount depends upon the calculated loss (NG, Drain, Stoma, etc..)calculated loss (NG, Drain, Stoma, etc..)
Type of fluid: 0.9% N saline + KcL.Type of fluid: 0.9% N saline + KcL.
NB: For stoma loss, we may replace only NB: For stoma loss, we may replace only the amount of stoma output that the amount of stoma output that exceeds 15 ml/kg/day.exceeds 15 ml/kg/day.
UOP: Excess of 5 ml/kg/hrUOP: Excess of 5 ml/kg/hr

What (Type of fluid)What (Type of fluid)1. Crystalloids1. Crystalloids
Neonates: Neonates:
- Maintenance: 10% Dextrose- Maintenance: 10% Dextrose
0.18 N Saline0.18 N Saline
- Replacement: 0.9% N Saline- Replacement: 0.9% N Saline Infants and children:Infants and children:
- Maintenance: 5% Dextrose- Maintenance: 5% Dextrose
0.45% N saline0.45% N saline
- Replacement: 0.9% N Saline- Replacement: 0.9% N Saline

What (Type of fluid)What (Type of fluid)2. Colloids2. Colloids
Bloods, and blood productsBloods, and blood products FactorsFactors PNPN Gelfusion (Synthetic colloids)Gelfusion (Synthetic colloids)
How to assess the adequacy of How to assess the adequacy of the fluid you are giving?the fluid you are giving?
Assessment of Assessment of dehydration dehydration
and and overhydration.overhydration.
Assessment of the state of Assessment of the state of hydration.hydration.
General status of the General status of the child.child.
Activity.Activity. UOP.UOP. Skin & Mucus Skin & Mucus
membrane.membrane. Capillary refilling time Capillary refilling time
(CRT).(CRT). Pulse, blood pressure.Pulse, blood pressure. Respiration.Respiration. Temperature.Temperature. Body weight.Body weight.
Venous access in Venous access in PaediatricsPaediatrics

PICC

1. Peripheral lines1. Peripheral lines

Types of cathetersTypes of catheters

LocationLocation


Rules for peripheral lines Rules for peripheral lines
Start from distal Start from distal veins first, then veins first, then proximalproximal
Upper limb then Upper limb then lower limblower limb
Preserve ACF for Preserve ACF for PICC linesPICC lines
Scalp and neck Scalp and neck veins last resort.veins last resort.

Peripheral linesPeripheral linesDurability??Durability??
Variable, can Variable, can stay up to one stay up to one week.week.
Infection, Infection, superficial superficial phlebitis, non-phlebitis, non-durability.durability.

2. Central lines2. Central lines
Types of central linesTypes of central lines
TunneledTunneled Hickman lineHickman line PortacathPortacath
Non-tunneledNon-tunneled CVP linesCVP lines Vascath linesVascath lines PICC linesPICC lines Femoral linesFemoral lines

Hickman lineHickman line

Hickman linesHickman lines

Hickman lineHickman line
Tunneled central lineTunneled central line Inserted in the SVC / R AtriumInserted in the SVC / R Atrium Can be used for IVC in difficult cases.Can be used for IVC in difficult cases. Durable (up to years)Durable (up to years) Main complications: Sepsis, Main complications: Sepsis,
blockage, and migration.blockage, and migration. Needs GA for removal.Needs GA for removal.

Port a cathPort a cath

Port a cathPort a cath
Port a cathPort a cath
SVC / R atriumSVC / R atrium More durableMore durable More expensiveMore expensive No external tubes.No external tubes. Bigger scarBigger scar Needs GA for removal.Needs GA for removal.

Peripherally inserted central Peripherally inserted central cathetercatheter
PICCPICC

PICC linesPICC lines
PICC linesPICC lines
Can be as durable as Hickman lineCan be as durable as Hickman line May not need GA.May not need GA. Removal doesn’t need GARemoval doesn’t need GA Should be treated as a central line Should be treated as a central line
(Aseptic techniques).(Aseptic techniques).
Non- tunneledNon- tunneledVascath (CVP catheter)!!Vascath (CVP catheter)!!

Vas CathVas Cath

Femoral lineFemoral line

Intraosseous injectionIntraosseous injection

IO routeIO route
Only in critical emergency, with Only in critical emergency, with absolutely no apparent venous absolutely no apparent venous access, and urgent need for access, and urgent need for transfusion.transfusion.
Needs expertise, proper needlesNeeds expertise, proper needles Very painful, not durable.Very painful, not durable. Limited to <7 years old childrenLimited to <7 years old children

