“fit for the aged“ expert consensus validation f o r t a
TRANSCRIPT
1
The JAPAN-F O R T A List “Fit for The Aged“
Expert Consensus Validation 1
F O R T A
A B C D
Farhad Pazan*, Yana Gercke*, Christel Weiß**, Martin Wehling*
*Clinical Pharmacology Mannheim, Center for Geriatric Pharmacology, University of Heidelberg
** Department of Medical Statistics, Biomathematics and Information Processing, Medical Faculty of the University of Heidelberg in Mannheim
2
Disclaimer
Please keep in mind that the FORTA concept was conceived in Germany. While building on an international foundation of medical evidence and experience for
the medications listed, including already existing “negative lists” and classification systems, this version of the FORTA List primarily reflects prescribing
tendencies in Japan. The FORTA labels themselves, being evidence-based, may possibly be subject to change during the course of further consensus evaluation
procedures, depending on the state of evidence and clinical experience for a given substance1. Meanwhile, the FORTA principle has been validated in a randomized
clinical trial (VALFORTA) showing a large improvement of medication quality and amelioration of clinical parameters2.
With the goal of creating a user-friendly clinical tool, a summary of relevant comments is given directly in the FORTA List, drawing on the Delphi experts’
extensive clinical experience and existing evidence. This is however by no means comprehensive and does not necessarily refer to specific evidence or sources.
Therefore, the authors’ selection of suggestions, comments and warnings may be subjective1. ‘No comment’ reflects the absence of noteworthy or relevant words
of information or caution within the context of the expert evaluation. All information herein is believed to be true and accurate. However, the use of the content
does not acquit the reader of critical examination in individual cases. Neither the authors nor the University of Heidelberg or affiliated institutions, as the publishers
of this list, can accept legal responsibility for any errors or omissions made in the contents of this list1. We would also like to point out that the FORTA list has
been developed for physicians and is not suitable for direct use by patients or any other persons.
We welcome all comments and criticism which may contribute to the quality, safety and usability of the FORTA List.

3
The Japan-FORTA expert panel
The following 13 colleagues, representing Japan provided their expertise for purposes of evaluating the proposed FORTA List. They received no honoraria in
connection with this project. All panel members contributed actively to the development of the content of the FORTA List.
Expert Panel Members and their affiliations
Hiroshi Akazawa MD, PhD: Department of Cardiovascular Medicine, The University of Tokyo, Graduate School of Medicine, Tokyo, Japan.
Taro Kojima MD, PhD: Department of Geriatric Medicine, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan.
Ryota Kumaki, MS: Division of Social Pharmacy, Department of Healthcare & Regulatory Sciences, Showa University School of Pharmacy, Tokyo, Japan.
Masahiro Akishita MD, PhD: Department of Geriatric Medicine, Graduate School of Medicine, Institute of Gerontology, The University of Tokyo, Japan.
Yasushi Takeya MD: Department of Geriatric and General Medicine, Osaka University Graduate School of Medicine, Osaka, Japan.
Yoshiyuki Ohno PhD: Department of Pharmacy, The University of Tokyo Hospital, Faculty of Medicine, The University of Tokyo, Tokyo, Japan.
Takashi Yamanaka MD: Department of Home Care Medicine, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan.
Koichi Kozaki MD: Department of Geriatric Medicine, Kyorin University School of Medicine, Tokyo, Japan.
Yusuke Suzuki MD, PhD: Centre for Community Liaison and Patient Consultations, Nagoya University Hospital, Nagoya, Japan.
Katsuyoshi Mizukami MD, PhD: Graduate School of Comprehensive Human Sciences Faculty of Health and Sport Sciences, University of Tsukuba, Tokyo
campus, Tokyo, Japan
Fumihiro Mizokami, PhD: Department of Pharmacy, National Center for Geriatrics and Gerontology, Obu, Japan.
Yoshiyuki Ikeda MD, PhD: Department of Cardiovascular Medicine and Hypertension, Kagoshima University, Japan.
Atsuya Shimizu MD, PhD: Departments of Cardiology, National Center for Geriatrics and Gerontology, Obu, Japan.
4
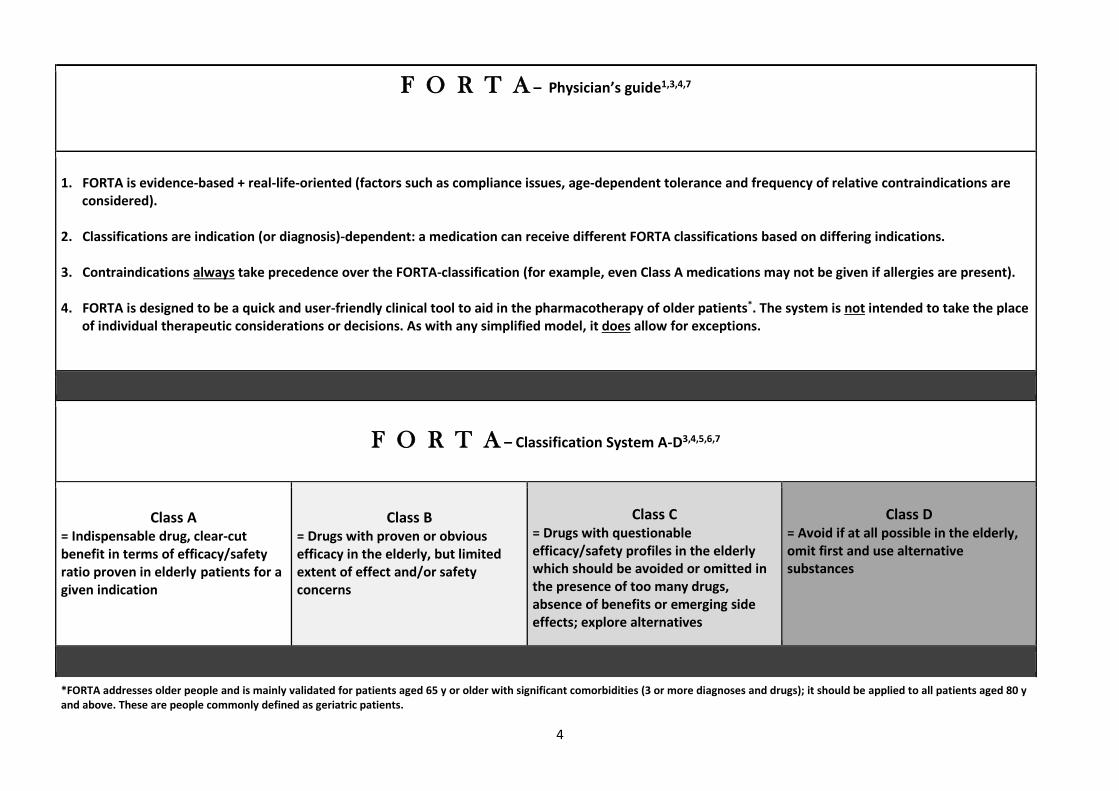
F O R T A – Physician’s guide1,3,4,7
1. FORTA is evidence-based + real-life-oriented (factors such as compliance issues, age-dependent tolerance and frequency of relative contraindications are considered).
2. Classifications are indication (or diagnosis)-dependent: a medication can receive different FORTA classifications based on differing indications. 3. Contraindications always take precedence over the FORTA-classification (for example, even Class A medications may not be given if allergies are present). 4. FORTA is designed to be a quick and user-friendly clinical tool to aid in the pharmacotherapy of older patients*. The system is not intended to take the place
of individual therapeutic considerations or decisions. As with any simplified model, it does allow for exceptions.
F O R T A – Classification System A-D3,4,5,6,7
Class A
= Indispensable drug, clear-cut benefit in terms of efficacy/safety ratio proven in elderly patients for a given indication
Class B
= Drugs with proven or obvious efficacy in the elderly, but limited extent of effect and/or safety concerns
Class C = Drugs with questionable efficacy/safety profiles in the elderly which should be avoided or omitted in the presence of too many drugs, absence of benefits or emerging side effects; explore alternatives
Class D = Avoid if at all possible in the elderly, omit first and use alternative substances
*FORTA addresses older people and is mainly validated for patients aged 65 y or older with significant comorbidities (3 or more diagnoses and drugs); it should be applied to all patients aged 80 y and above. These are people commonly defined as geriatric patients.
5
The F O R T A List1,5,6
Delphi Expert Consensus Validation
Classification of the most frequently used long-term medications† for the pharmacotherapy of older patients
by indication/diagnosis, ranked according to FORTA classification Newly proposed drugs are mentioned under the respective diagnosis and marked by *; they are listed in greater detail in the second part.
(† long-term defined as > 4 weeks. Please note that the distinction between acute/chronic may not always be clear-cut; exceptions are noted)
F O R T A A B C D

6
ARTERIAL HYPERTENSION
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/Group
Renin-Angiotensin system inhibitors
ACE inhibitors Angiotensin receptor
antagonists
A 10
1.000
1.0; 1
A 10
1.000
1.0; 1
Long-acting calcium antagonists, dihydropyridine type, for example amlodipine
A 10 1.000 1.0; 1
Betablockers B 10 1.000 2.0; 2
Diuretics
B 9
1.000 2.0; 2
Note: In small amounts; Japanese are highly sensitive to salt and diuretics are highly effective. Diuretic is the first-choice medicine for elderly people in Japan. Betablockers is a second-choice medicine because of contraindications and use attention many in elderly people, it is uncomfortable to make it the same classification as betablockers. However, it is a medicine to be warned by elderly people with diuretic drugs, and it is recommended to use them in small amounts
Aliskiren C 10 0.950 2.9; 3
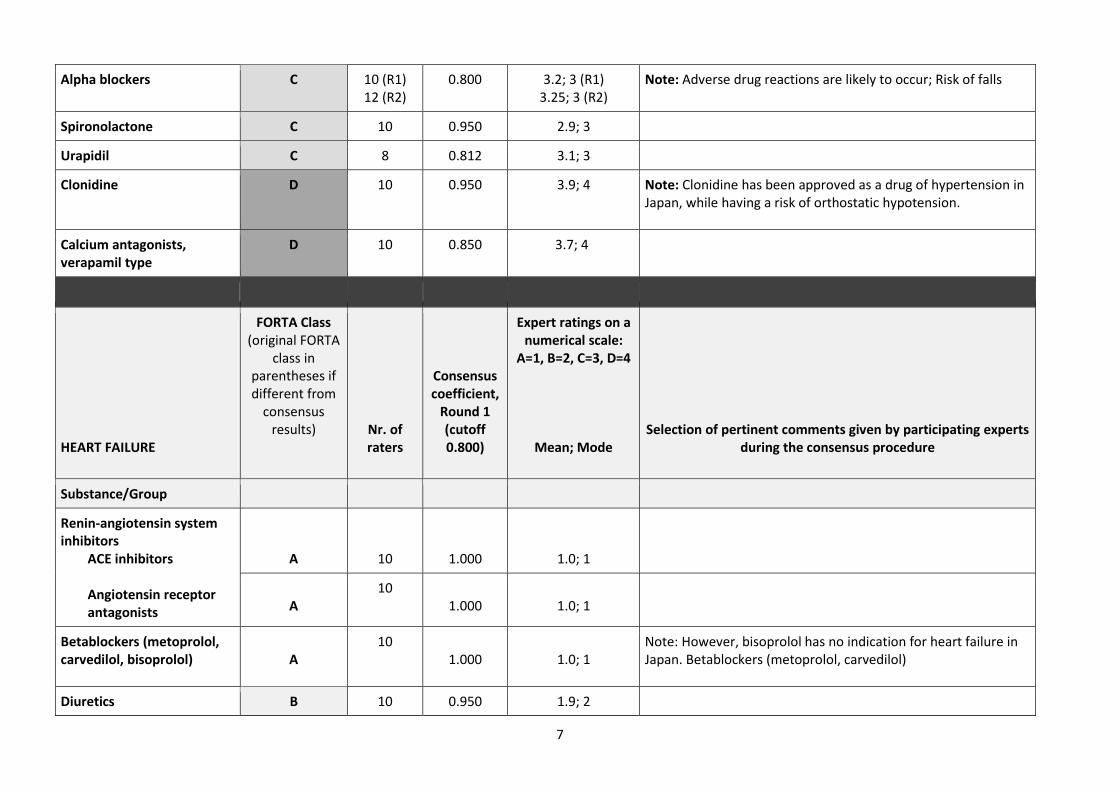
7
Alpha blockers C 10 (R1) 12 (R2)
0.800
3.2; 3 (R1) 3.25; 3 (R2)
Note: Adverse drug reactions are likely to occur; Risk of falls
Spironolactone C 10 0.950 2.9; 3
Urapidil C 8 0.812 3.1; 3
Clonidine D 10 0.950 3.9; 4 Note: Clonidine has been approved as a drug of hypertension in Japan, while having a risk of orthostatic hypotension.
Calcium antagonists, verapamil type
D 10 0.850 3.7; 4
HEART FAILURE
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/Group
Renin-angiotensin system inhibitors
ACE inhibitors
Angiotensin receptor antagonists
A
10
1.000
1.0; 1
A
10 1.000
1.0; 1
Betablockers (metoprolol, carvedilol, bisoprolol)
A
10 1.000
1.0; 1
Note: However, bisoprolol has no indication for heart failure in Japan. Betablockers (metoprolol, carvedilol)
Diuretics B 10 0.950 1.9; 2

8
Spironolactone B 10 1.000 2.0; 2
Digitalis preparations C 9 0.944 3.1; 3 Note: Digitalis use is limited to the cardiac insufficiency patient with atrial fibrillation
Eplerenone*
ACUTE CORONARY SYNDROME
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/Group
Renin-Angiotensin-System- Blocker: ACE-inhibitors
A 10 1.000 1.0; 1
Acetylsalicylic acid A 10 1.000 1.0; 1
Unfractionated heparin and low molecular weight heparin
A 10 1.000 1.0; 1
Frequency-lowering betablockers
A 10 1.000 1.0; 1
Atorvastatin A 10 1.000 1.0; 1

9
Nitroglycerin spray, single use, acute as on-demand medication
A
10 1.000
1.0; 1
Clopidogrel, prasugrel
B 10
9
0.950
0.944
1.9; 2
1.1; 1
Note: FORTA A for stent = limited duration (at least 1 year) based on guidelines
A for stent
Thrombolytics, especially rTPA (recombinant tissue-type plasminogen activator)
B
9 (R1)
12 (R2)
0.777
2.4; 2 (R1)
2.08; 2 (R2)
Nitrates, long-term
C 10 0.900 2.8; 3
CHRONIC THERAPY FOLLOWING MYOCARDIAL INFARCTION
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Renin angiotensin system blockers ACE Inhibitors
A 10
1.000
1.0; 1
Acetylsalicylic acid (100 mg/d)
A 10 1.000 1.0; 1

10
Frequency-lowering beta blockers up to 3 years Frequency-lowering beta blockers longer than 3 years
A 8 1.000 1.0; 1 Note: Japanese guidelines do not have a period of 3 years for the use of betablocker. Instead, the recommended grade is low for patients with low risk, such as maintaining cardiac function.
C 8 0.812 2.6; 3
Nitroglycerin spray, single use as on-demand medication
A 10 1.000 1.0; 1
Influenza vaccination (inactivated subunit vaccines)
A 10 1.000 1.0; 1
Clopidogrel (12 months after acute coronary syndrome)
A with aspirin intolerance
9 1.000 1.0; 1
Statins
A
9
8
1.000
1.000
1.0; 1
2.0; 2
B for very old (>85 years)
patients
Nitrates, long-term C 10 0.900 2.8; 3
Fibrates C 10 0.900 2.8; 3
Ezetimibe C 10 0.850 2.7; 3 Note: According to the results of the EWTOPIA75 trial
Amiodarone
C 10 0.950 3.1; 3 Note: High risk for fatal arrhythmia
D 10 0.950 3.9; 4
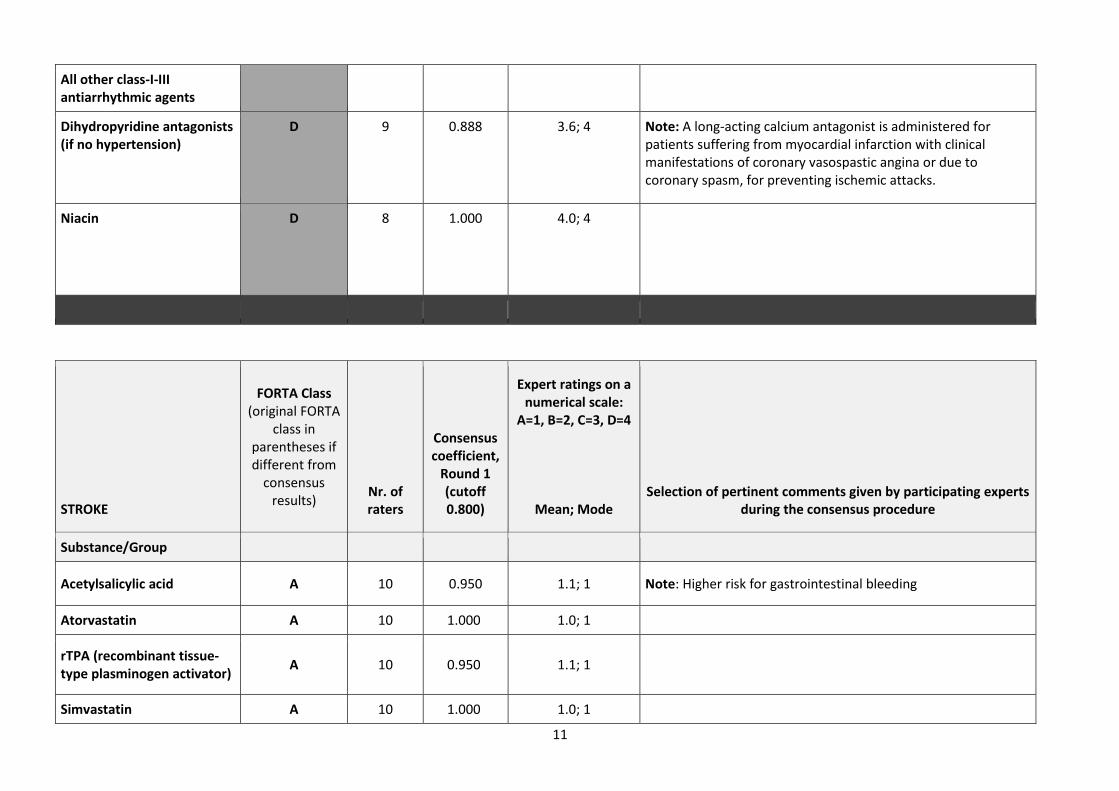
11
All other class-I-III antiarrhythmic agents
Dihydropyridine antagonists (if no hypertension)
D 9 0.888 3.6; 4 Note: A long-acting calcium antagonist is administered for patients suffering from myocardial infarction with clinical manifestations of coronary vasospastic angina or due to coronary spasm, for preventing ischemic attacks.
Niacin D 8 1.000 4.0; 4
STROKE
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/Group
Acetylsalicylic acid A 10 0.950 1.1; 1 Note: Higher risk for gastrointestinal bleeding
Atorvastatin A 10 1.000 1.0; 1
rTPA (recombinant tissue-type plasminogen activator)
A 10 0.950 1.1; 1
Simvastatin A 10 1.000 1.0; 1

12
Anticoagulants including new oral anticoagulants
A 10 0.950 1.1; 1 Note: Benefit depending on the type of stroke
Clopidogrel A 10 1.000 1.0; 1
Dipyridamole plus acetylsalicylic acid
(B) C
7 (R1) 11 (R2)
0.785
2.4; 2 (R1) 2.9; - (R2)
Note: For Japanese, according to JASAP study, this combination was not effective compared to aspirin alone; Higher risk for bleeding
ATRIAL FIBRILLATION
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Frequency-lowering betablockers
A 10 1.000 1.0; 1
New Oral Anticoagulants (NOACs) Except apixaban
B
10
8
0.900
0.937
1.8; 2
1.1; 1
Note: Several Japanese data have been reported, and all NOACs are treated equally.
Note: Less evidence for patients with higher CHADS2 score and frailty. Also, you need to take b.i.d. which might not be the first choice for older patients from the standpoint of drug adherence.
A

13
Digoxin Digitoxin
B
C
10
8
0.850
0.937
2.3; 2
3.1; 3
Note: There are many side effects, and elderly should avoid it. Note: Much higher risk than digoxin because we cannot monitor the plasma concentration
Oral anticoagulants (e.g. warfarin) Alternative: low molecular weight heparin
B
10
0.950
1.9; 2
C
7 1.000
3.0; 3
Diltiazem, verapamil
C
10
0.950
2.9; 3
Class III antiarrhythmic agent amiodarone All other class I/III antiarrhythmic agents
C
9
0.944
3.1; 3
D
10 1.000
4.0; 4
Acetylsalicylic acid (100 mg/d)
D
8 1.000 4.0; 4
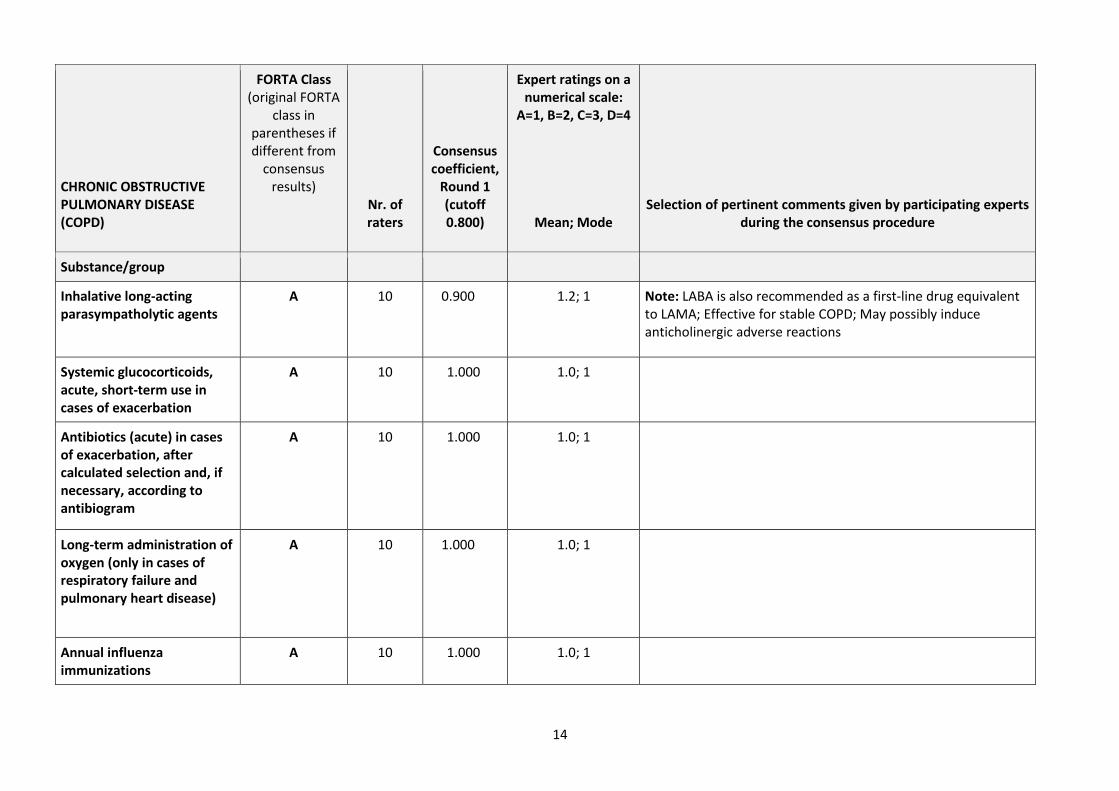
14
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Inhalative long-acting parasympatholytic agents
A 10 0.900 1.2; 1 Note: LABA is also recommended as a first-line drug equivalent to LAMA; Effective for stable COPD; May possibly induce anticholinergic adverse reactions
Systemic glucocorticoids, acute, short-term use in cases of exacerbation
A 10 1.000 1.0; 1
Antibiotics (acute) in cases of exacerbation, after calculated selection and, if necessary, according to antibiogram
A 10 1.000 1.0; 1
Long-term administration of oxygen (only in cases of respiratory failure and pulmonary heart disease)
A 10 1.000 1.0; 1
Annual influenza immunizations
A 10 1.000 1.0; 1
15
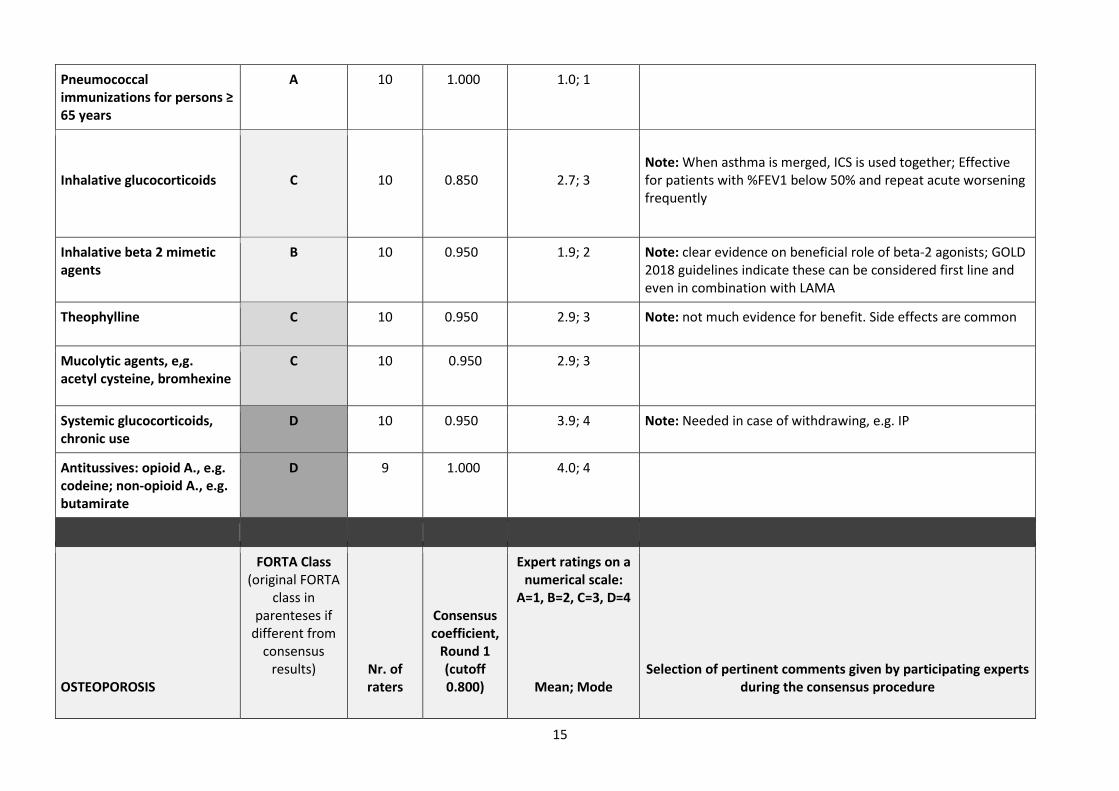
Pneumococcal immunizations for persons ≥ 65 years
A 10 1.000 1.0; 1
Inhalative glucocorticoids
C
10
0.850
2.7; 3
Note: When asthma is merged, ICS is used together; Effective for patients with %FEV1 below 50% and repeat acute worsening frequently
Inhalative beta 2 mimetic agents
B 10 0.950 1.9; 2 Note: clear evidence on beneficial role of beta-2 agonists; GOLD 2018 guidelines indicate these can be considered first line and even in combination with LAMA
Theophylline C 10 0.950 2.9; 3 Note: not much evidence for benefit. Side effects are common
Mucolytic agents, e,g. acetyl cysteine, bromhexine
C 10 0.950 2.9; 3
Systemic glucocorticoids, chronic use
D 10 0.950 3.9; 4 Note: Needed in case of withdrawing, e.g. IP
Antitussives: opioid A., e.g. codeine; non-opioid A., e.g. butamirate
D 9 1.000 4.0; 4
OSTEOPOROSIS
FORTA Class (original FORTA
class in parenteses if
different from consensus
results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure

16
Substance/Group
Parenteral bisphosphonates (e.g. ibandronate, IV every 3 months)
A 10 0.950 1.1; 1 Note: Risk of BRONJ (Bisphosphonate-related osteonecrosis of the jaw)
Denosumab A 10 0.950 1.1; 1 Note: Risk of ARONJ (Anti-resorptive agent-related osteonecrosis of the jaw)
Calcium and vitamin D supplements (as prophylaxis for persons ≥ 65 years)
A
10
0.900
1.2; 1
Note: evidence suggests that supplementation with Calcium and Vitamin D is not necessary, if oral food intake is adequate; no evidence for everyone; no proven benefit for prevention in patients who have adequate dietary calcium intake and normal vitamin D levels; FORTA C based on new 2018 US preventative task force recommendations; calcium increases BMD, but fracture prevention is minimal. Dietary intake preferred. No clear role when dietary intake is adequate and vitamin D level s are normal; inconsistent evidence to support benefit in fracture prevention
Bisphosphonates, orally administered
B 10 0.900 1.8; 2
Raloxifene (for women) B 10 0.900 2.0; 2
Teriparatide C 10 (R1) 10 (R2)
0.750 2.5; 3 (R1) 2.8; 3 (R2)
Alfacalcidol C 10 0.900 2.8; 3
Hormone replacement therapy (HRT): estrogen, except for perimenopausal)
D 10 0.950 3.9; 4
Basedoxifene (for women)*
Eldecalcitol*

17
Menatetrone*
TYPE II DIABETES MELLITUS
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Insulin and insulin analogs (if absolutely necessary)
B 10
0.900
1.8; 2
Note: can be used safely if monitor; avoid in frail, cognitively impaired; insulin is indispensable (when absolutely necessary)
Metformin B
10 0.900 2.0; 2 Note: High risk of lactic acidosis in older people with CKD;
Acarbose B 10 0.850 2.3; 2 Note: Frequently seen side effects (flatulence and diarrhea)
DPP4 (Dipeptidylpeptidase) Inhibitors
(B)
A
10 (R1) 11 (R2)
0.700
1.4; 1 (R1) 1.36; 1 (R2)
Note: It is most used in Japan; Reduces PG safely; Low possibility to cause hypoglycemia
GLP1 (Glucagon-Like Peptide-1) analogs
B 10 1.000 2.0; 2
3rd generation sulfonylureas (for example, glimepiride)
C
10 1.000
3.0; 3

18
Glinides (for example, nateglinide)
C 10 1.000 3.0; 3
PPAR-ɣ Ligands (Peroxisomal Proliferator-Activated Receptor gamma)
Pioglitazone
C
10
1.000
3.0; 3
1st generation sulfonylureas (for example, glyburide/glibenclamide)
D 10 0.950 3.9; 4
SGLT-2 inhibitors D 10 (R1) 11 (R2)
0.800 3.6; 4 (R1) 3.6; 4 (R2)
Note: Effective for the older diabetes patients, but necessary to watch for side effects
DEMENTIA
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Acetylcholinesterase inhibitors e.g. donepezil, galantamine, rivastigmine (in phases when clearly indicated)
B
10
0.900
1.8; 2
Note: Concerns for underuse
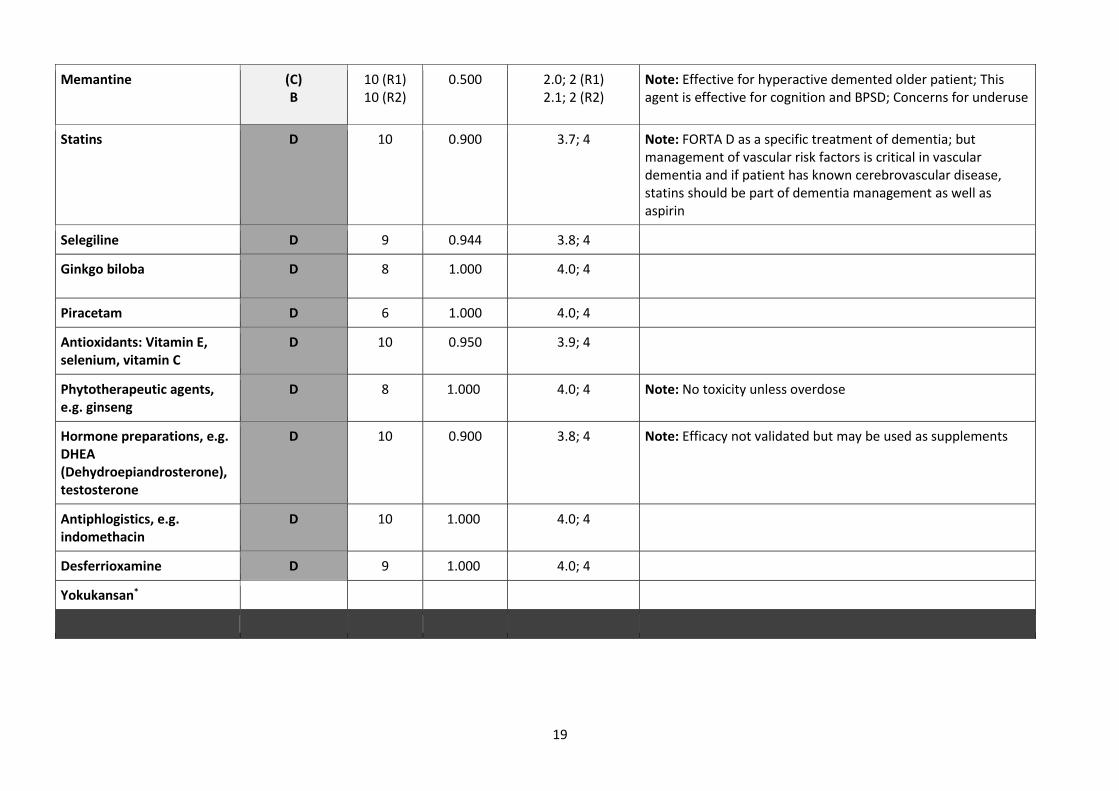
19
Memantine (C) B
10 (R1) 10 (R2)
0.500 2.0; 2 (R1) 2.1; 2 (R2)
Note: Effective for hyperactive demented older patient; This agent is effective for cognition and BPSD; Concerns for underuse
Statins D 10 0.900 3.7; 4 Note: FORTA D as a specific treatment of dementia; but management of vascular risk factors is critical in vascular dementia and if patient has known cerebrovascular disease, statins should be part of dementia management as well as aspirin
Selegiline D 9 0.944 3.8; 4
Ginkgo biloba D 8 1.000 4.0; 4
Piracetam D 6 1.000 4.0; 4
Antioxidants: Vitamin E, selenium, vitamin C
D 10 0.950 3.9; 4
Phytotherapeutic agents, e.g. ginseng
D 8 1.000 4.0; 4 Note: No toxicity unless overdose
Hormone preparations, e.g. DHEA (Dehydroepiandrosterone), testosterone
D 10 0.900 3.8; 4 Note: Efficacy not validated but may be used as supplements
Antiphlogistics, e.g. indomethacin
D 10 1.000 4.0; 4
Desferrioxamine D 9 1.000 4.0; 4
Yokukansan*
20
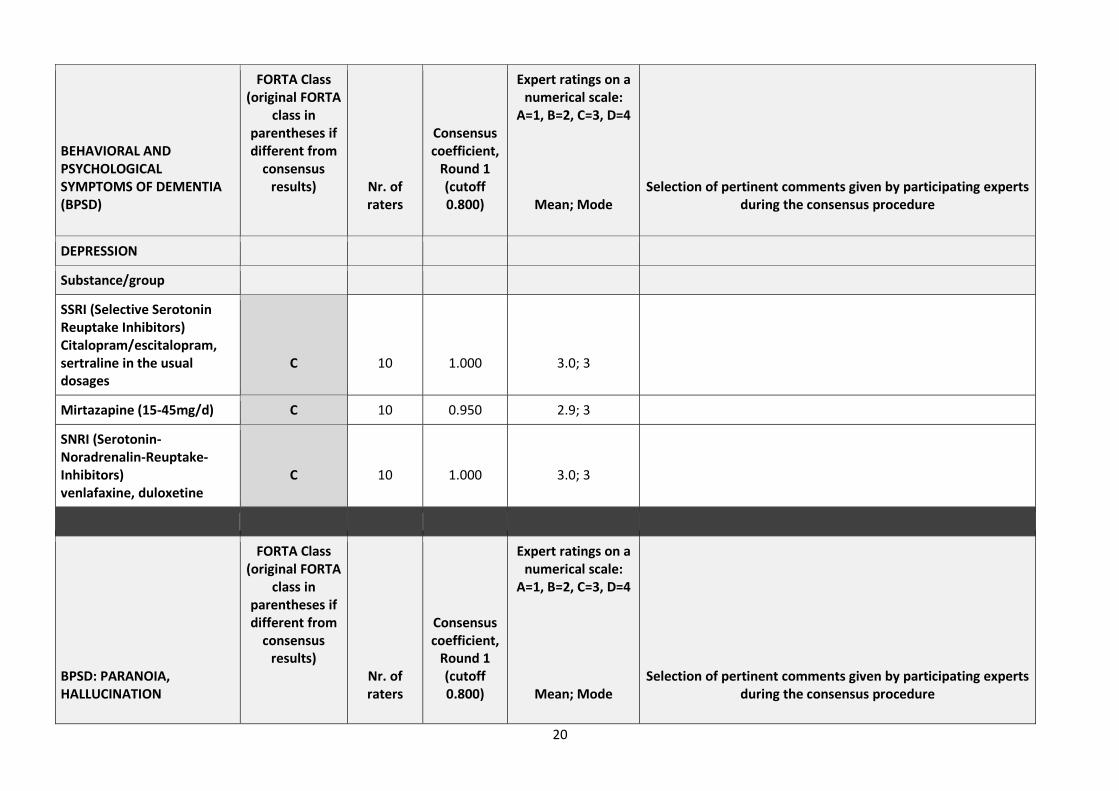
BEHAVIORAL AND PSYCHOLOGICAL SYMPTOMS OF DEMENTIA (BPSD)
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
DEPRESSION
Substance/group
SSRI (Selective Serotonin Reuptake Inhibitors) Citalopram/escitalopram, sertraline in the usual dosages
C
10
1.000
3.0; 3
Mirtazapine (15-45mg/d) C 10 0.950 2.9; 3
SNRI (Serotonin-Noradrenalin-Reuptake-Inhibitors) venlafaxine, duloxetine
C
10
1.000
3.0; 3
BPSD: PARANOIA, HALLUCINATION
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
21
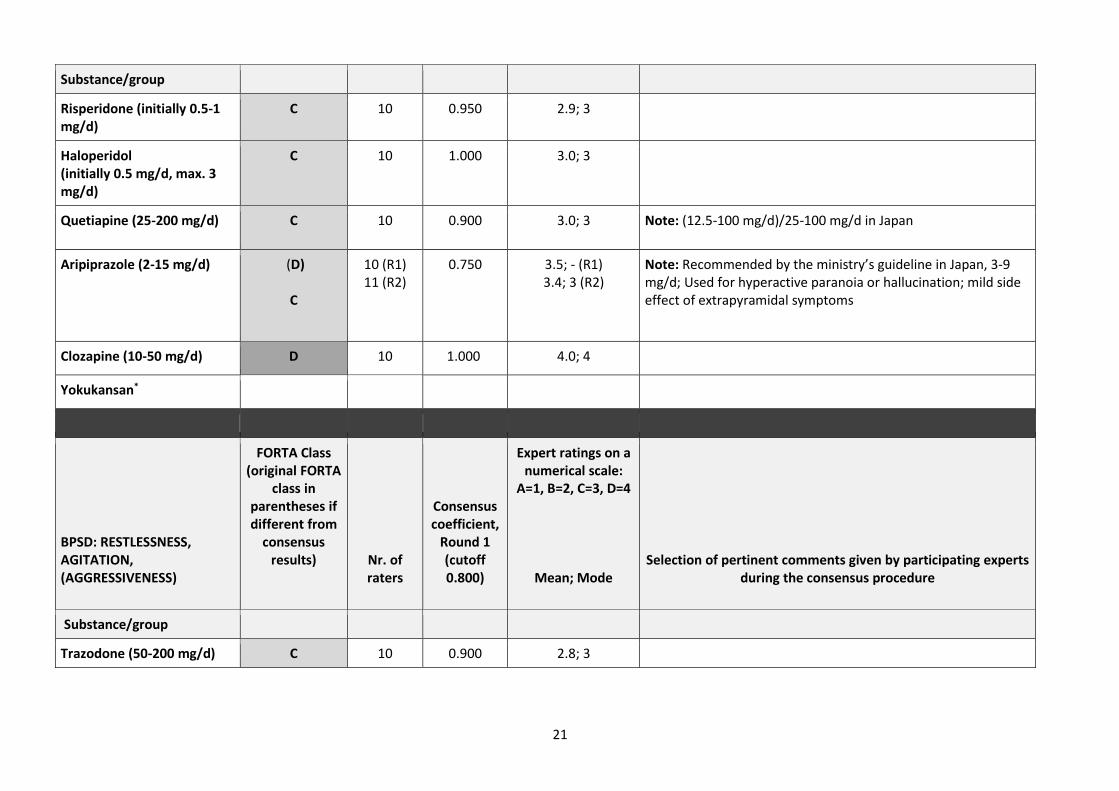
Substance/group
Risperidone (initially 0.5-1 mg/d)
C 10 0.950 2.9; 3
Haloperidol (initially 0.5 mg/d, max. 3 mg/d)
C 10 1.000 3.0; 3
Quetiapine (25-200 mg/d) C 10 0.900 3.0; 3 Note: (12.5-100 mg/d)/25-100 mg/d in Japan
Aripiprazole (2-15 mg/d) (D)
C
10 (R1) 11 (R2)
0.750 3.5; - (R1) 3.4; 3 (R2)
Note: Recommended by the ministry’s guideline in Japan, 3-9 mg/d; Used for hyperactive paranoia or hallucination; mild side effect of extrapyramidal symptoms
Clozapine (10-50 mg/d) D 10 1.000 4.0; 4
Yokukansan*
BPSD: RESTLESSNESS, AGITATION, (AGGRESSIVENESS)
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Trazodone (50-200 mg/d) C 10 0.900 2.8; 3

22
Risperidone (initiallly 0.5-1 mg/d, Maximum 3 mg/d)
C 10 0.950 2.9; 3
Quetiapine (25-200 mg/d) C
10 0.950 2.9; 3
Yokukansan*
Olanzapine (2.5-10 mg/d)*
BPSD: SLEEP DISORDERS
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Zopiclone
C 10 0.950 2.9; 3
Tetracyclic antidepressant Mirtazapine (15-30mg)
C 13 1.000 3.0; 3 Note: very commonly used as an adjunct agent for improved sleep (at 7.5-15 mg nightly) and as an appetite stimulant. Side effect profile minimal compared to benefits

23
Zolpidem
C
13
0.950
2.9; 3
Note: risks outweigh benefits in older adults; avoid if possible due to risk of psychomotor impairment, delirium, falls, fractures, MVAs. Adverse effects similar to benzodiazepines. Minimal efficacy; not recommended for use due to exacerbation of dementia/cognitive impairment; increased risk of falls/fractures; avoid; can worsen cognitive status; not aware of studies examining efficacy for this indication; risk for falls and delirium; although non-dependence forming, same risks as BZDs. Risks clearly outweigh benefits.
Ramelteon*
Suvorexant*
Trazodone*
Eszopiclone*
DEPRESSION Prophylaxis and therapy for patients with moderate to major depression
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
24
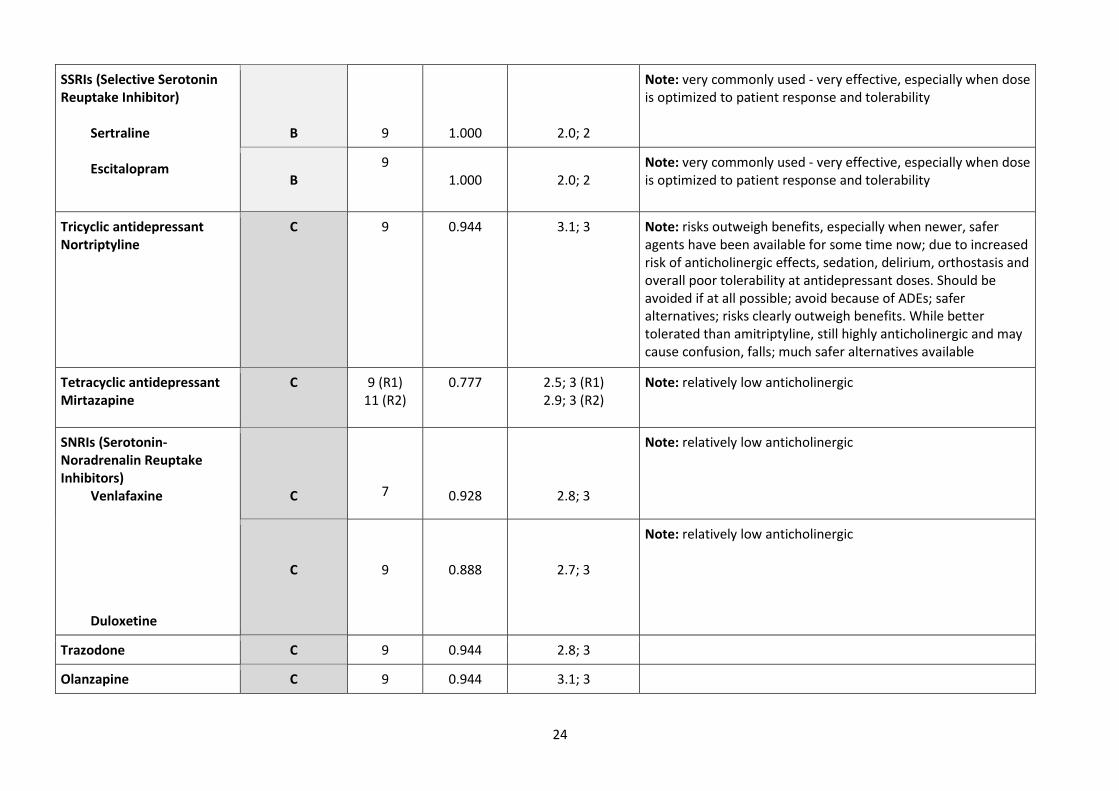
SSRIs (Selective Serotonin Reuptake Inhibitor) Sertraline Escitalopram
B
9
1.000
2.0; 2
Note: very commonly used - very effective, especially when dose is optimized to patient response and tolerability
B
9 1.000
2.0; 2
Note: very commonly used - very effective, especially when dose is optimized to patient response and tolerability
Tricyclic antidepressant Nortriptyline
C 9 0.944 3.1; 3 Note: risks outweigh benefits, especially when newer, safer agents have been available for some time now; due to increased risk of anticholinergic effects, sedation, delirium, orthostasis and overall poor tolerability at antidepressant doses. Should be avoided if at all possible; avoid because of ADEs; safer alternatives; risks clearly outweigh benefits. While better tolerated than amitriptyline, still highly anticholinergic and may cause confusion, falls; much safer alternatives available
Tetracyclic antidepressant Mirtazapine
C 9 (R1) 11 (R2)
0.777
2.5; 3 (R1) 2.9; 3 (R2)
Note: relatively low anticholinergic
SNRIs (Serotonin-Noradrenalin Reuptake Inhibitors) Venlafaxine Duloxetine
C
7
0.928
2.8; 3
Note: relatively low anticholinergic
C
9
0.888
2.7; 3
Note: relatively low anticholinergic
Trazodone C 9 0.944 2.8; 3
Olanzapine C 9 0.944 3.1; 3
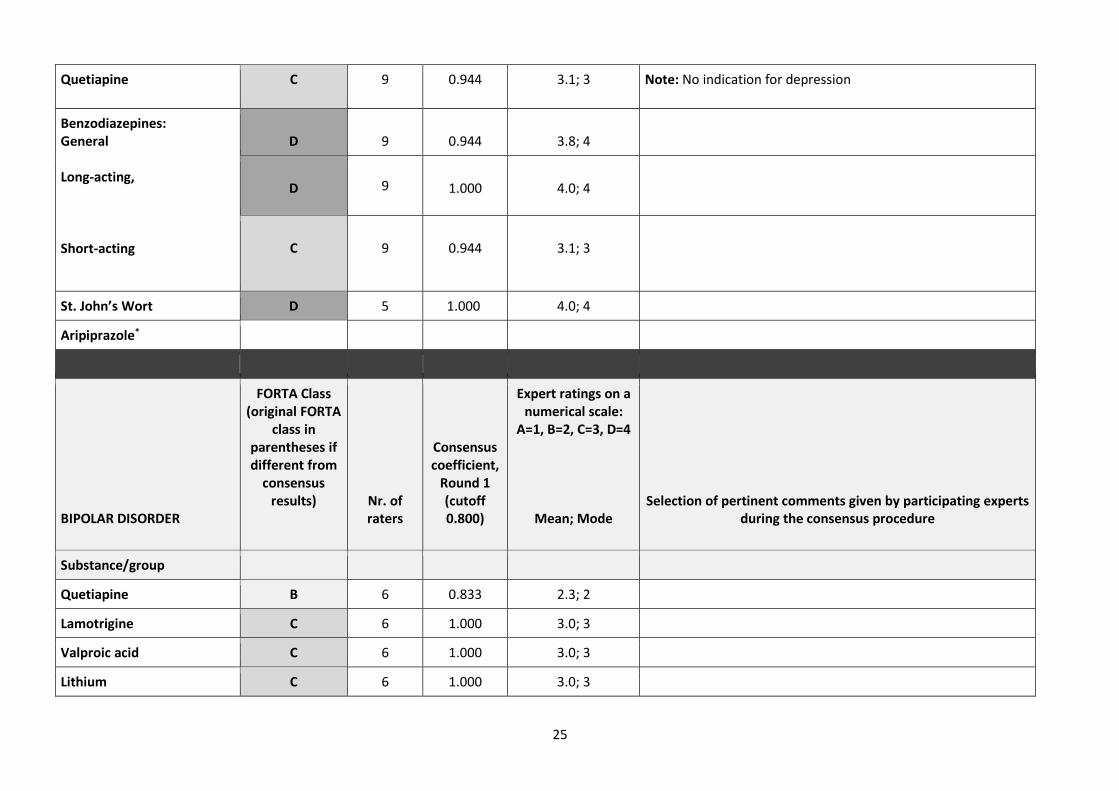
25
Quetiapine C 9 0.944 3.1; 3 Note: No indication for depression
Benzodiazepines: General Long-acting, Short-acting
D 9
0.944
3.8; 4
D 9
1.000
4.0; 4
C
9
0.944
3.1; 3
St. John’s Wort D 5 1.000 4.0; 4
Aripiprazole*
BIPOLAR DISORDER
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Quetiapine B 6 0.833 2.3; 2
Lamotrigine C 6 1.000 3.0; 3
Valproic acid C 6 1.000 3.0; 3
Lithium C 6 1.000 3.0; 3
26
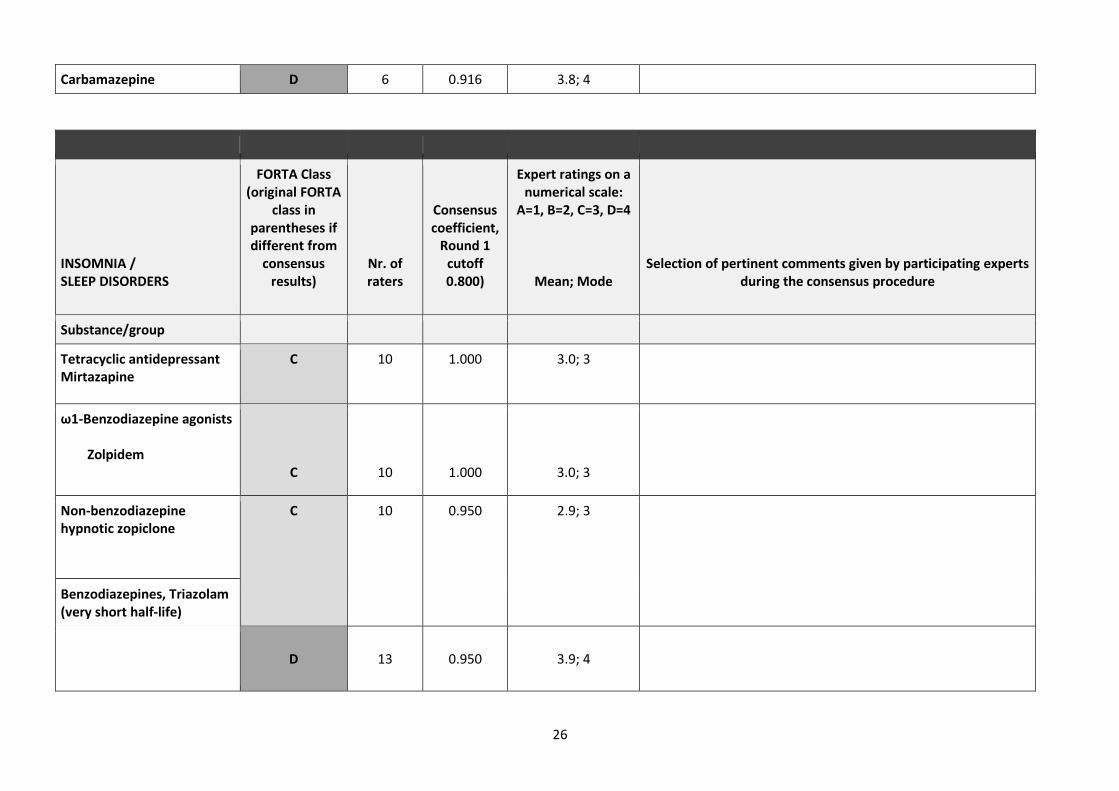
Carbamazepine D 6 0.916 3.8; 4
INSOMNIA / SLEEP DISORDERS
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Tetracyclic antidepressant Mirtazapine
C 10 1.000 3.0; 3
ω1-Benzodiazepine agonists Zolpidem
C
10
1.000
3.0; 3
Non-benzodiazepine hypnotic zopiclone
C 10 0.950 2.9; 3
Benzodiazepines, Triazolam (very short half-life)
D
13
0.950
3.9; 4

27
Antihistamine Diphenhydramine
D 13 1.000 4.0; 4
Ramelteon*
Survorexant*
CHRONIC PAIN
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Paracetamol (acetaminophen)
A 10 0.950 1.1; 1 Note: Risk of liver dysfunction should be considered
Opioids, e.g. Buprenorphine, oxycodone, hydromorphone Morphine
B
10 (R1) 11 (R2)
0.800
2.4; 2 (R1)
2.36; 2 (R2)
Note: Mostly used for cancer-related pain in Japan; Buprenorphine, Tramadol hydrochloride / Acetaminophen, codeine, morphin and phentanyl are approved for chronic pain
C
10
1.000
3.0; 3
Tramadol C 10 0.950 2.9; 3

28
SSRI (Selective Serotonin Reuptake Inhibitors) / SNRI (Serotonin- Norepinephrine-Reuptake Inhibitor), e.g. venlafaxine (only if absolutely necessary)
C 10 1.000
3.0; 3
Note: Venlafaxine is not approved for chronic pain
Tilidine/Naloxone
C 7 0.928 3.1; 3
Oxycodone/Naloxone C 8 1.000 3.0; 3
Antiepileptic agents (only for neuropathic pain) Pregabalin/gabapentin
Carbamazepine
C
10 1.000
3.0; 3
Note: has place in therapy for patients with neuropathic pain – diabetics, neurodegenerative diseases, etc. Renal dosing is needed, and careful assessment for possible potentiating effects with other agents that may be sedating or centrally depressing.
D
10
0.850
3.7; 4
Note: Indicated for trigeminal neuralgia; May be tried for trigeminal pain in the absence of alternatives
Tricyclic antidepressant amitriptyline
D 9 0.944 3.8; 4 Note: Indicated for peripheral neuropathic pain
NSAIDs (nonsteroidal anti-inflammatory drugs, for long-term use), e.g. naproxen
D
10 0.900
3.8; 4

29
Cox-2 inhibitors, e.g. celecoxib
(D)
C
10 (R1) 11 (R2)
0.600 3.2; 4 (R1) 3.2; 3 (R2)
Note: Cox-2 inhibitor is associated with a lower incidence of symptomatic ulcers and ulcer complications combined compared with conventional NSAIDs. JAMA 2000, (284), 1247; Relatively low risk of gastrointestinal hemorrhage compared to NSAIDs; Commonly used in Japan; May be used with caution
EPILEPSY
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Levetiracetam B 9 0.944 2.1; 2
Lamotrigine B 9 0.888 2.2; 2
Gabapentin B 9 0.944 2.1; 2
Topiramate B 8 0.937 2.1; 2
Lorazepam (emergency use) Lorazepam (long-term use)
B
8
0.937
2.1; 2
D
8 1.000
4.0; 4
Lacosamide C 5 1.000 3.0; 3
30
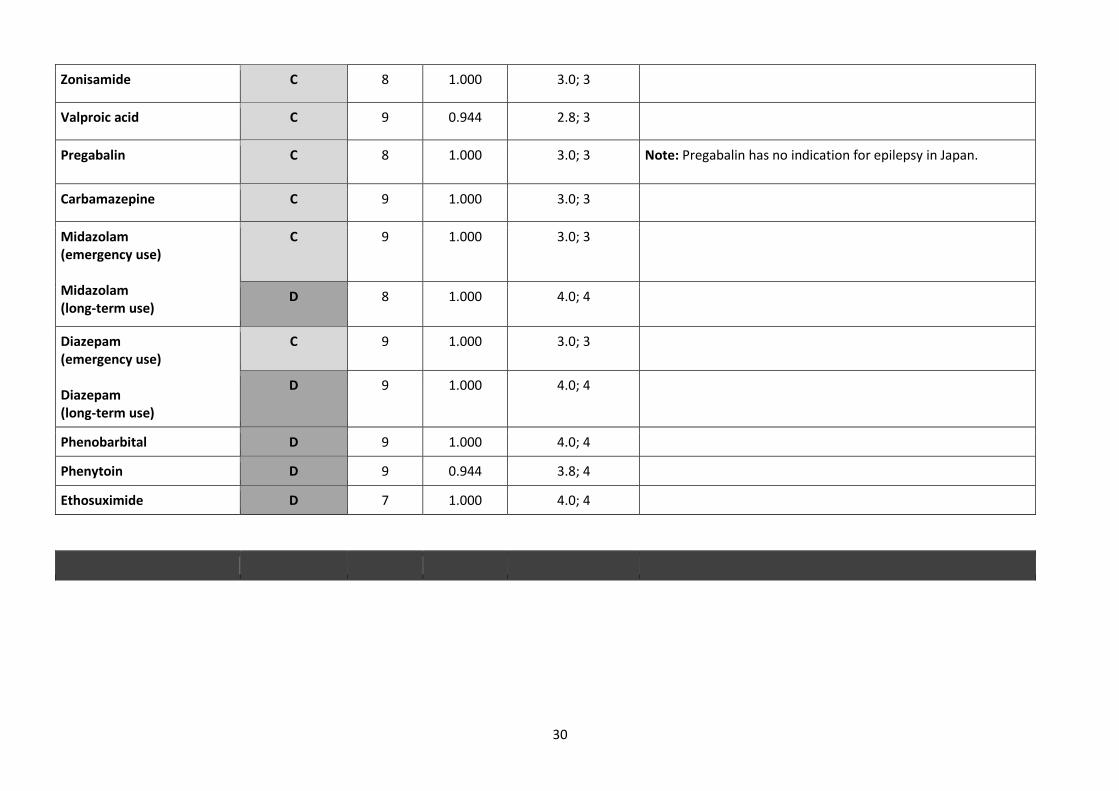
Zonisamide C 8 1.000 3.0; 3
Valproic acid C 9 0.944 2.8; 3
Pregabalin C 8 1.000 3.0; 3 Note: Pregabalin has no indication for epilepsy in Japan.
Carbamazepine C 9 1.000 3.0; 3
Midazolam (emergency use) Midazolam (long-term use)
C
9 1.000 3.0; 3
D 8 1.000 4.0; 4
Diazepam (emergency use) Diazepam (long-term use)
C 9 1.000 3.0; 3
D 9 1.000 4.0; 4
Phenobarbital D 9 1.000 4.0; 4
Phenytoin D 9 0.944 3.8; 4
Ethosuximide D 7 1.000 4.0; 4
31
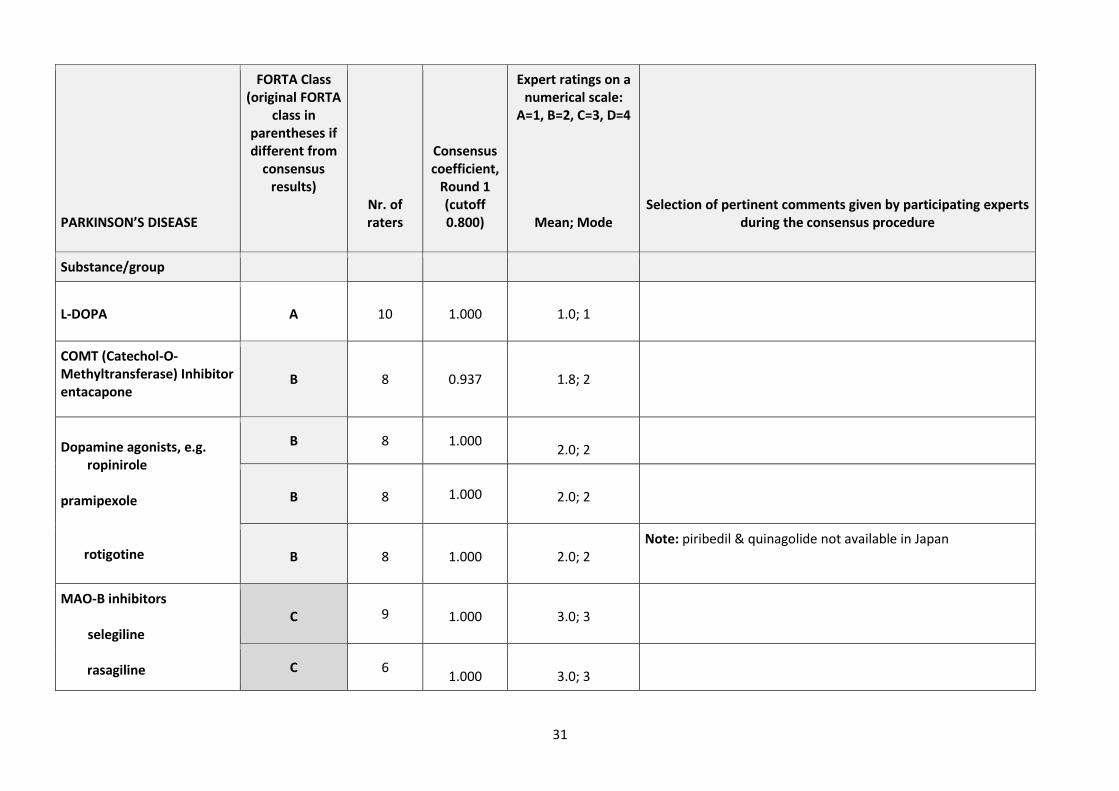
PARKINSON’S DISEASE
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
L-DOPA
A
10
1.000
1.0; 1
COMT (Catechol-O-Methyltransferase) Inhibitor entacapone
B 8 0.937 1.8; 2
Dopamine agonists, e.g. ropinirole pramipexole rotigotine
B 8 1.000
2.0; 2
B
8 1.000
2.0; 2
B
8
1.000
2.0; 2
Note: piribedil & quinagolide not available in Japan
MAO-B inhibitors
selegiline rasagiline
C 9
1.000
3.0; 3
C 6
1.000
3.0; 3
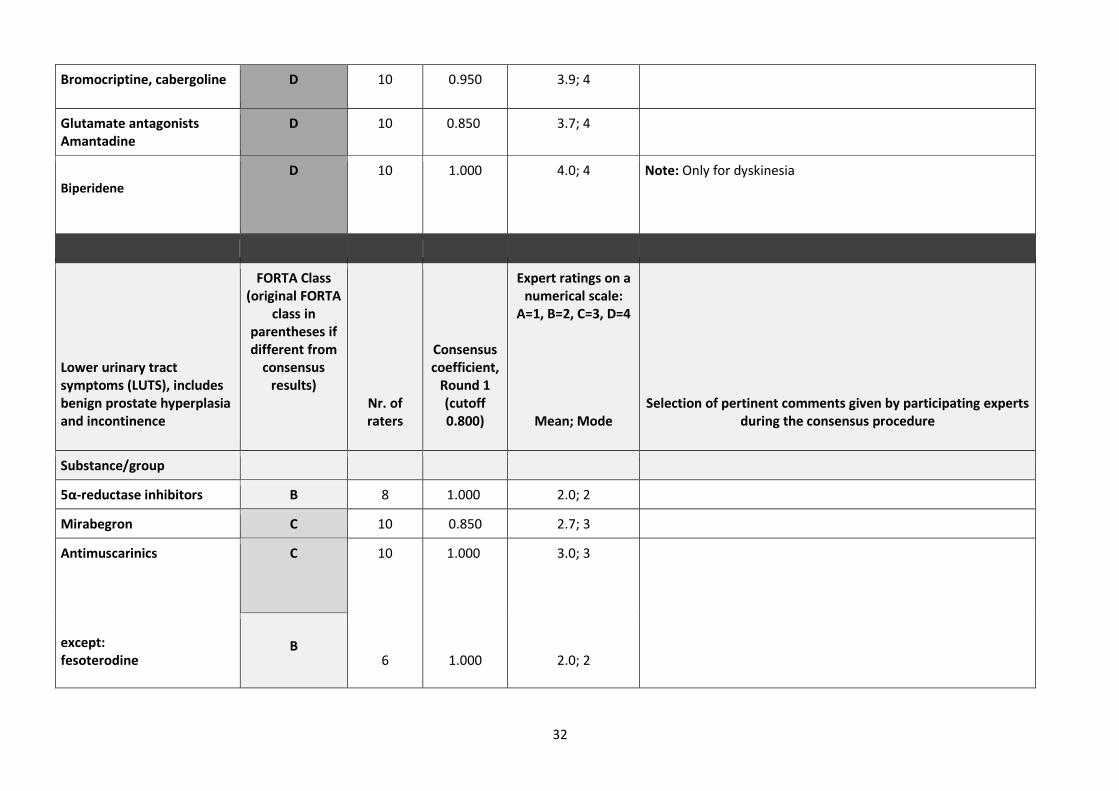
32
Bromocriptine, cabergoline D 10 0.950 3.9; 4
Glutamate antagonists Amantadine
D 10 0.850 3.7; 4
Biperidene
D 10 1.000 4.0; 4 Note: Only for dyskinesia
Lower urinary tract symptoms (LUTS), includes benign prostate hyperplasia and incontinence
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
5α-reductase inhibitors B 8 1.000 2.0; 2
Mirabegron C 10 0.850 2.7; 3
Antimuscarinics except: fesoterodine
C 10
6
1.000
1.000
3.0; 3
2.0; 2
B
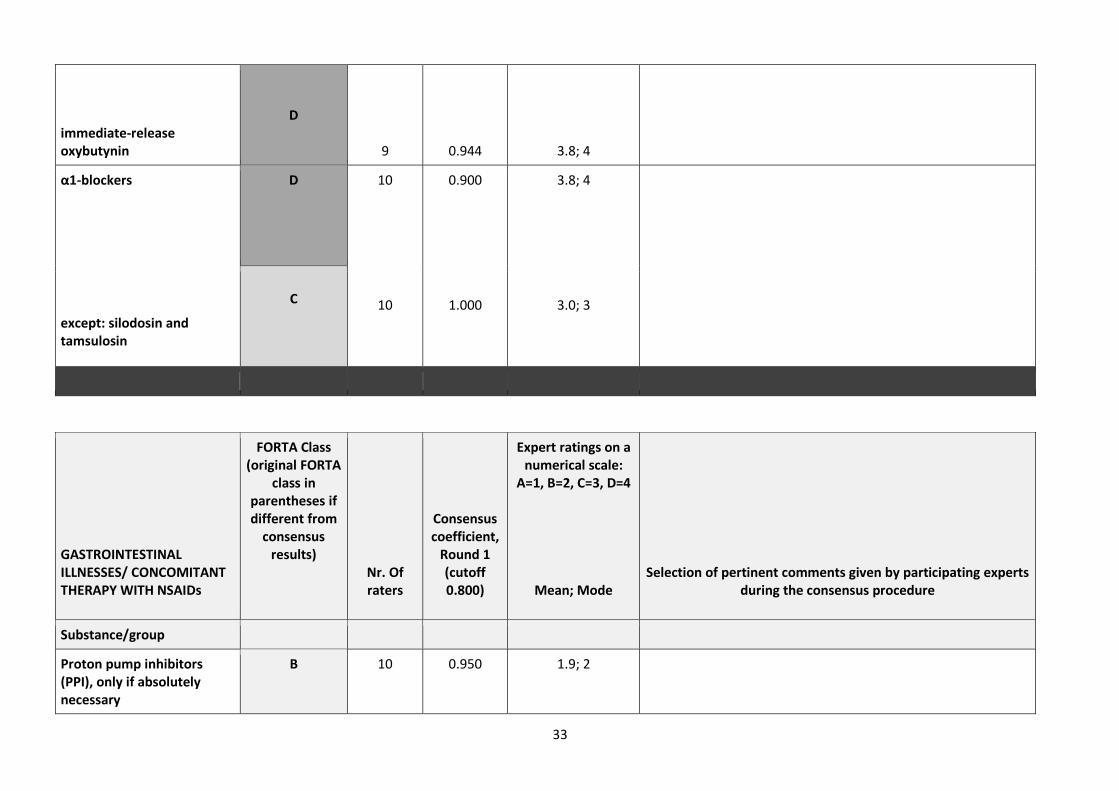
33
immediate-release oxybutynin
D
9
0.944
3.8; 4
α1-blockers except: silodosin and tamsulosin
D 10
10
0.900
1.000
3.8; 4
3.0; 3
C
GASTROINTESTINAL ILLNESSES/ CONCOMITANT THERAPY WITH NSAIDs
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. Of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
Proton pump inhibitors (PPI), only if absolutely necessary
B 10 0.950 1.9; 2
34
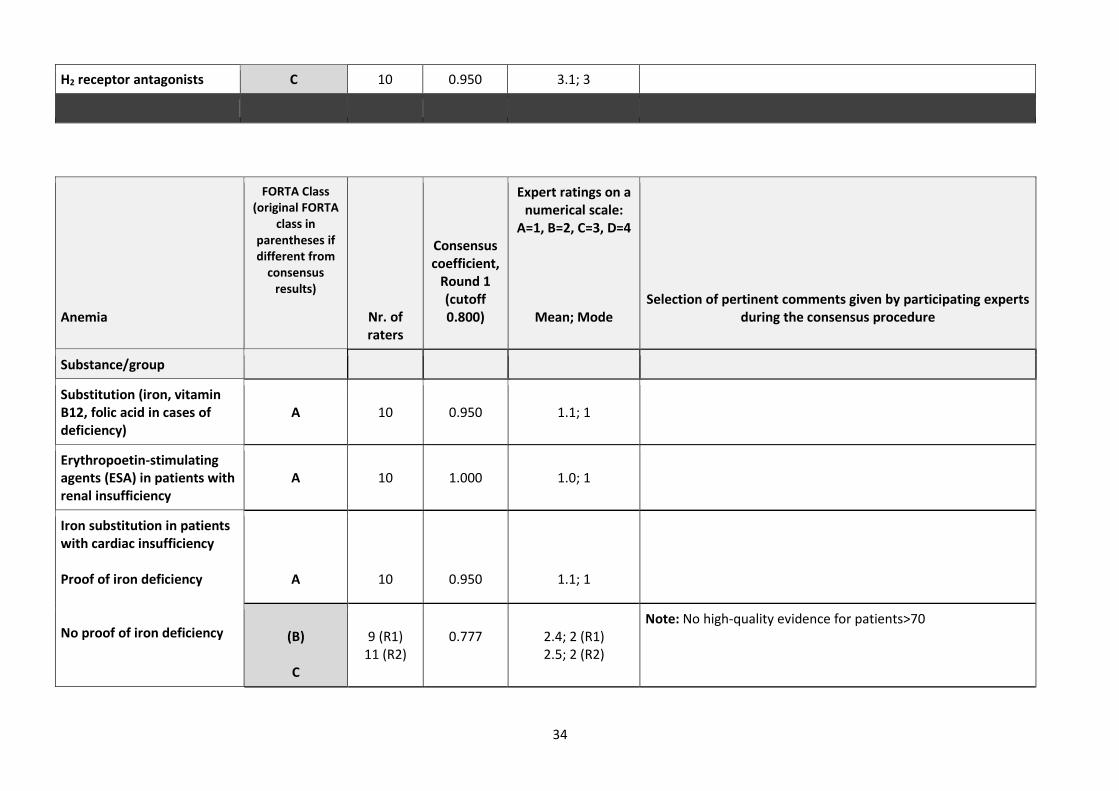
H2 receptor antagonists C 10 0.950 3.1; 3
Anemia
FORTA Class (original FORTA
class in parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Substitution (iron, vitamin B12, folic acid in cases of deficiency)
A
10
0.950
1.1; 1
Erythropoetin-stimulating agents (ESA) in patients with renal insufficiency
A
10
1.000
1.0; 1
Iron substitution in patients with cardiac insufficiency Proof of iron deficiency No proof of iron deficiency
A
10
0.950
1.1; 1
(B)
C
9 (R1)
11 (R2)
0.777
2.4; 2 (R1) 2.5; 2 (R2)
Note: No high-quality evidence for patients>70
35
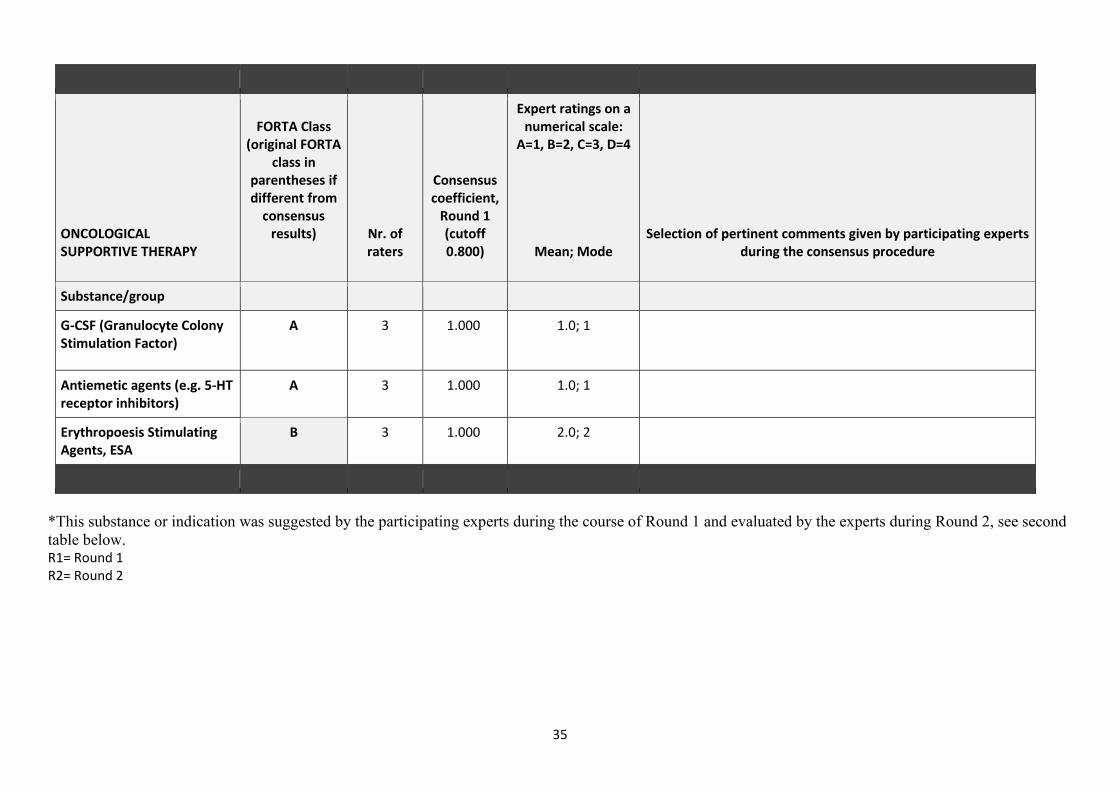
ONCOLOGICAL SUPPORTIVE THERAPY
FORTA Class
(original FORTA class in
parentheses if different from
consensus results)
Nr. of raters
Consensus coefficient,
Round 1 (cutoff 0.800)
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts
during the consensus procedure
Substance/group
G-CSF (Granulocyte Colony Stimulation Factor)
A 3 1.000 1.0; 1
Antiemetic agents (e.g. 5-HT receptor inhibitors)
A 3 1.000 1.0; 1
Erythropoesis Stimulating Agents, ESA
B 3 1.000 2.0; 2
*This substance or indication was suggested by the participating experts during the course of Round 1 and evaluated by the experts during Round 2, see second
table below. R1= Round 1 R2= Round 2
36
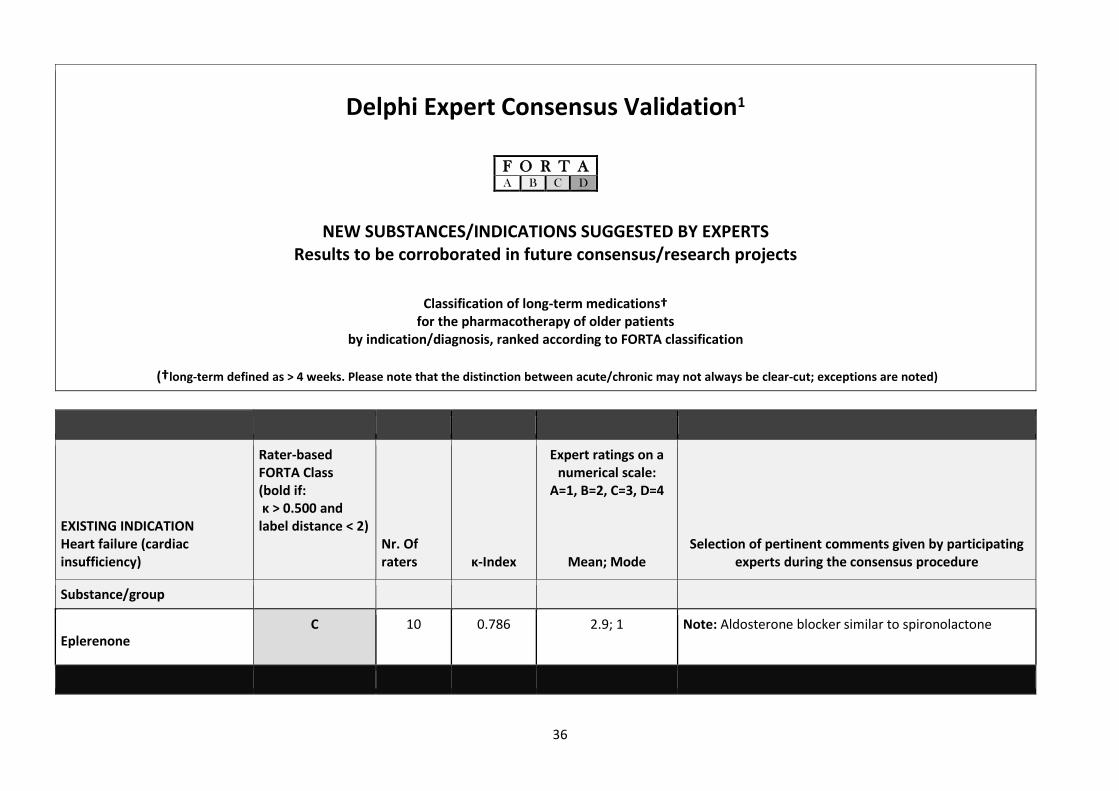
Delphi Expert Consensus Validation1
NEW SUBSTANCES/INDICATIONS SUGGESTED BY EXPERTS Results to be corroborated in future consensus/research projects
Classification of long-term medications†
for the pharmacotherapy of older patients by indication/diagnosis, ranked according to FORTA classification
(†long-term defined as > 4 weeks. Please note that the distinction between acute/chronic may not always be clear-cut; exceptions are noted)
F O R T A A B C D
EXISTING INDICATION Heart failure (cardiac insufficiency)
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. Of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Eplerenone
C 10 0.786 2.9; 1 Note: Aldosterone blocker similar to spironolactone

37
EXISTING INDICATION OSTEOPOROSIS
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. Of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Basedoxifene (for women) B 9 0.466 2.3; 1 Note: recommended for osteoporosis treatment as adjunct to drug therapy; efficacy data unclear, but good safety profile (with vitamin D)
Eldecalcitol B 10 0.324 2.2.; 2 Note: Stronger effect on bone mineral density and preventing vertebral fracture compared to alfacalcidol
Menatetrone
C 9 0.762 3.1; 3 Note: not effective
EXISTING INDICATION DEMENTIA
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. Of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Yokukansan C 8 0.257 2.5; 3

38
EXISTING INDICATION INSOMNIA / SLEEP DISORDERS:
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. Of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Ramelteon B 10 0.534 2.1; 2 Note: Melatonin receptor agonist. Mild effect
Survorexant B 10 0.398 2.2; 3 Note: Lower risk of side effects compared to benzos or non-benzos.
EXISTING INDICATION BPSD: RESTLESSNESS, AGITATION, (AGGRESSIVENESS)
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Yokukansan
B
11
0.301
2.3; 3
Note: The first-line drug for BPSD in Japan (Chinese herbal medicine). Mild effect; Effective with relatively safe for hyperactive BPSD with demented older patients
Olanzapine (2.5-10 mg/d) C 11 0.806 2.9; 3 Note: Recommended by the ministry’s guideline in Japan.
39
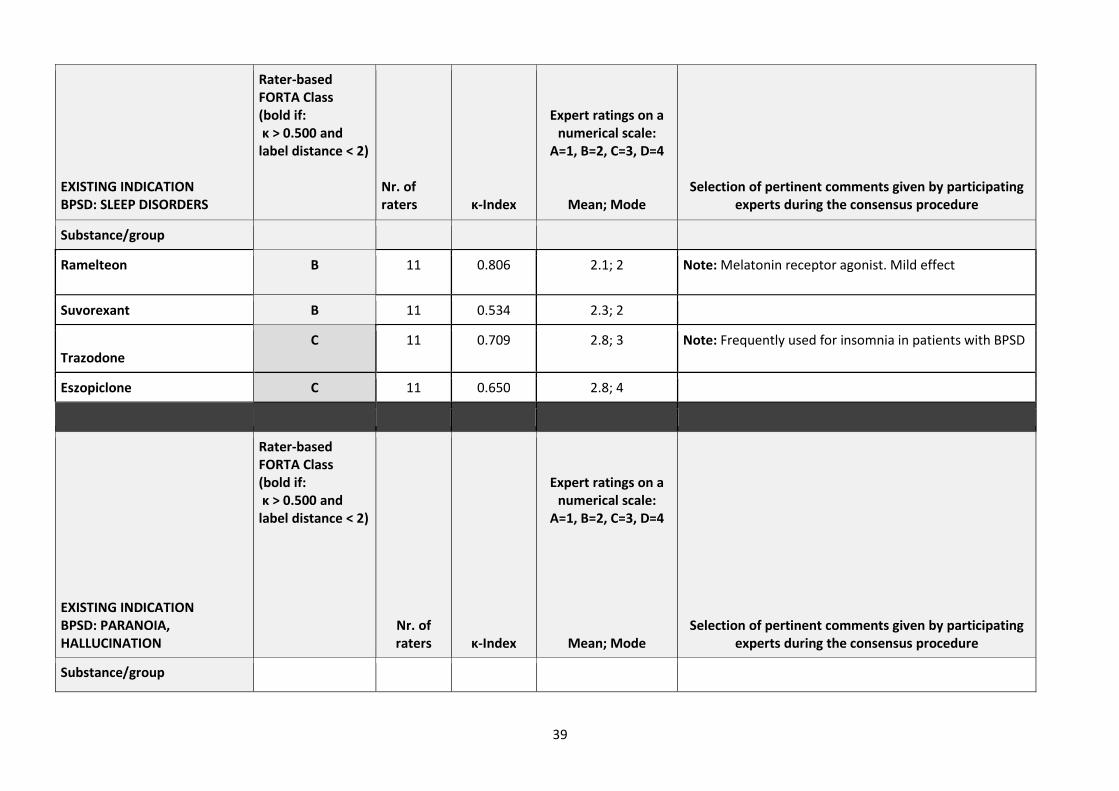
EXISTING INDICATION BPSD: SLEEP DISORDERS
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Ramelteon B 11 0.806 2.1; 2 Note: Melatonin receptor agonist. Mild effect
Suvorexant B 11 0.534 2.3; 2
Trazodone
C 11 0.709 2.8; 3 Note: Frequently used for insomnia in patients with BPSD
Eszopiclone C 11 0.650 2.8; 4
EXISTING INDICATION BPSD: PARANOIA, HALLUCINATION
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
40
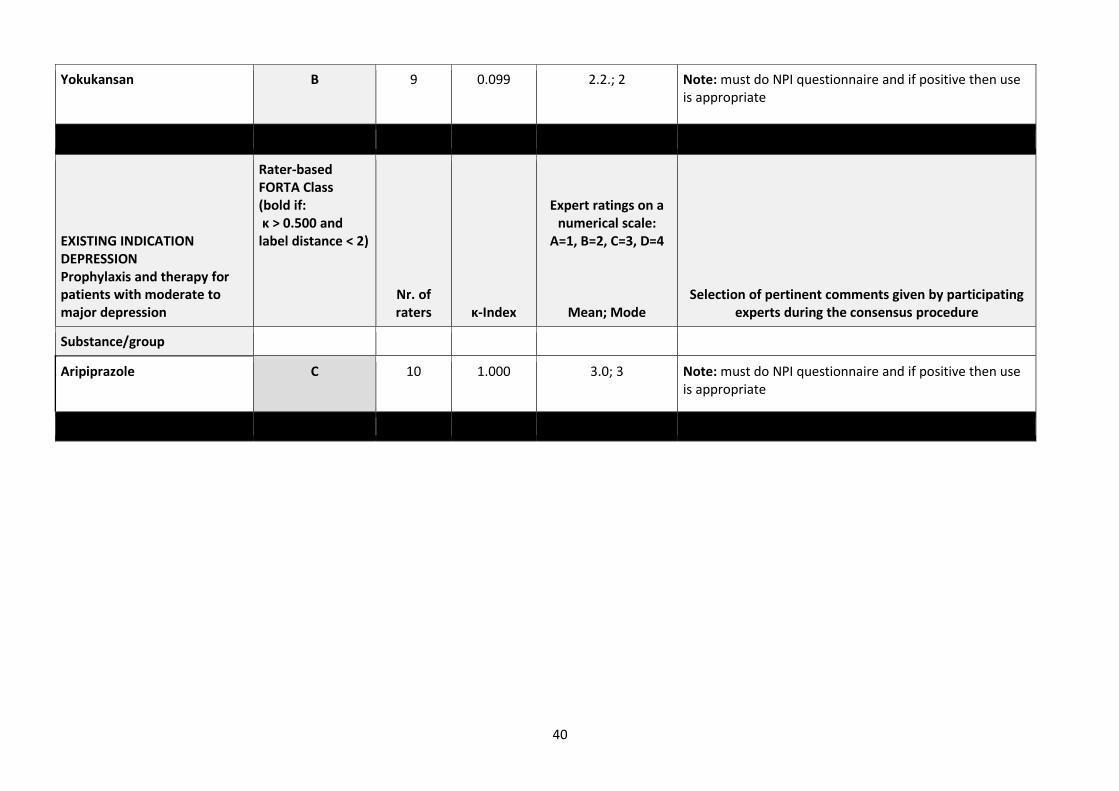
Yokukansan B 9 0.099 2.2.; 2 Note: must do NPI questionnaire and if positive then use is appropriate
EXISTING INDICATION DEPRESSION Prophylaxis and therapy for patients with moderate to major depression
Rater-based FORTA Class (bold if: κ > 0.500 and label distance < 2)
Nr. of raters
κ-Index
Expert ratings on a numerical scale:
A=1, B=2, C=3, D=4
Mean; Mode
Selection of pertinent comments given by participating experts during the consensus procedure
Substance/group
Aripiprazole C 10 1.000 3.0; 3 Note: must do NPI questionnaire and if positive then use is appropriate
41
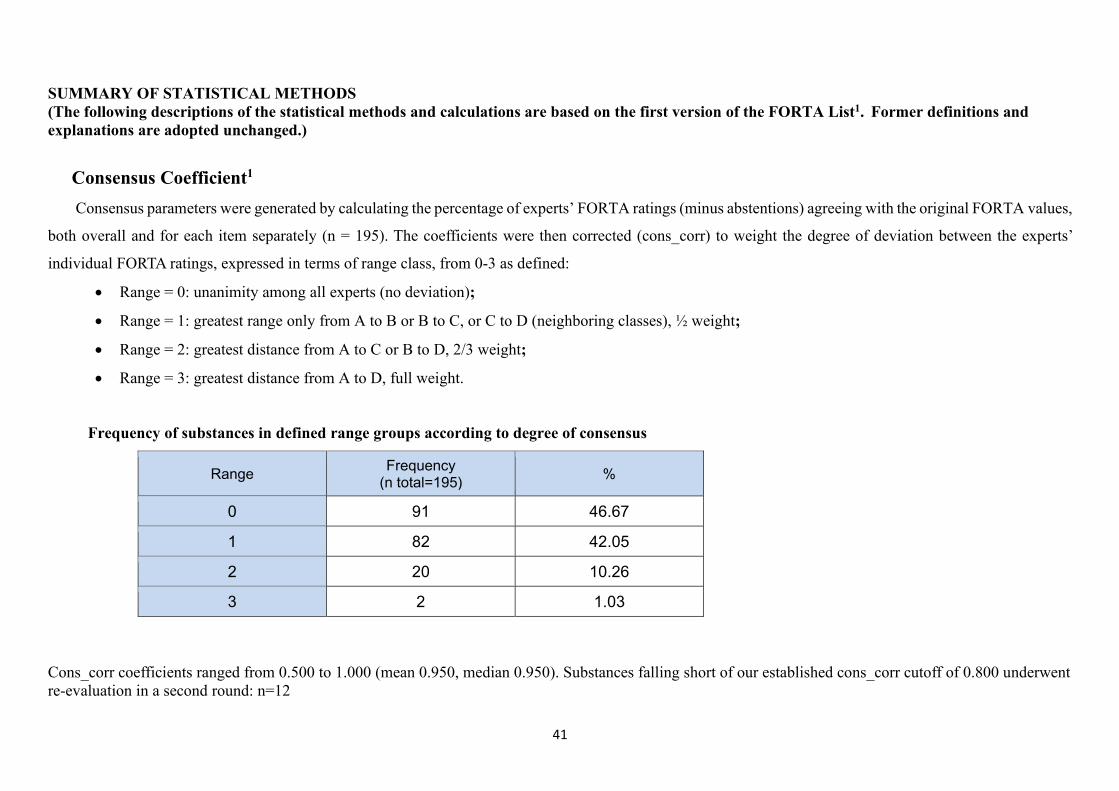
SUMMARY OF STATISTICAL METHODS
(The following descriptions of the statistical methods and calculations are based on the first version of the FORTA List1. Former definitions and
explanations are adopted unchanged.)
Consensus Coefficient1
Consensus parameters were generated by calculating the percentage of experts’ FORTA ratings (minus abstentions) agreeing with the original FORTA values,
both overall and for each item separately (n = 195). The coefficients were then corrected (cons_corr) to weight the degree of deviation between the experts’
individual FORTA ratings, expressed in terms of range class, from 0-3 as defined:
• Range = 0: unanimity among all experts (no deviation);
• Range = 1: greatest range only from A to B or B to C, or C to D (neighboring classes), ½ weight;
• Range = 2: greatest distance from A to C or B to D, 2/3 weight;
• Range = 3: greatest distance from A to D, full weight.
Frequency of substances in defined range groups according to degree of consensus
Range Frequency
(n total=195) %
0 91 46.67
1 82 42.05
2 20 10.26
3 2 1.03
Cons_corr coefficients ranged from 0.500 to 1.000 (mean 0.950, median 0.950). Substances falling short of our established cons_corr cutoff of 0.800 underwent
re-evaluation in a second round: n=12
42
Confirmation/determination of FORTA labels1
In order to compare the rater-based FORTA labels with the original author-based labels, the labels A, B, C and D were transformed as follows1:
A→ 1
B → 2
C → 3
D → 4
These numerical “grades” were used for the calculation of arithmetic mean. The mode (=grade appearing most frequently for rated item) is also shown. For the
12 re-evaluated items, grading was performed twice. The rater-based FORTA labels are derived from the arithmetic mean from Round 1, or if re-evaluated,
from Round 2. The range for each grade was set at:
If 1 ≤ m < 1.5 → FORTA Class A
If 1.5 ≤ m < 2.5 → FORTA Class B
If 2.5 ≤ m < 3.5 → FORTA Class C
If m ≥ 3.5 → FORTA Class D
m= arithmetic mean based on the grades 1-4
The results of The Delphi Consensus Validation Procedure confirmed the original FORTA labels for 96.9% of all substances (n=195); for 6 of the 195 substances
(3.1%), the FORTA labels changed over the course of two rounds. All consensus-based FORTA ratings are listed in bold print: A B C D, and the original author-
based FORTA ratings are supplied in parentheses: (A) (B) (C) (D).
43
Asterisks in the first table mark substances or indications suggested by the panel members during the course of Round 1 and
assessed by the experts during Round 2.
Selection process for new substances and indications1
• A total of 15 substances were accepted for potential addition to the revised FORTA List. Selection criteria: 1) acceptance of all substances
suggested by ≥ 1 experts during Round 1, and all suggested indication areas; 2) acceptance of all substances/indication areas affirmed by >50%
of experts during Round 2 that the substance/indication should be included in the FORTA List; 3) acceptance of all substances assigned a
FORTA label by ≥ 4 raters (excluding abstentions) during Round 2. The 15 substances included:
o 15 new substances belonging to pre-existing FORTA indications
• A kappa index was generated for each of those added substances to analyze the distribution of the raters’ FORTA labels given. The kappa
index is defined as the (proportion of “matching” labels – 0.25) / 0.75. This gives due consideration to the fact that a figure of 25% can
theoretically be attained by chance alone with this particular constellation (the choice of 4 distinct labels, as with multiple choice).
Mean and mode were calculated according to the numerical scale used for the original FORTA substances
A → 1
B → 2
C → 3
D → 4
If 1 ≤ m < 1.5 → FORTA Class A
If 1.5 ≤ m < 2.5 → FORTA Class B
If 2.5 ≤ m < 3.5 → FORTA Class C
If m ≥ 3.5 → FORTA Class D
44
m= arithmetic mean based on the grades 1-4
• Only 9 of the 15 new substances had a kappa index higher than 0.500. Suggesting a high level of inter-rater agreement for 60.0% these
substances.
45
REFERENCES
1. Kuhn-Thiel AM. et al. Consensus validation of the FORTA (Fit fOR The Aged) List: a clinical tool for increasing the appropriateness of pharmacotherapy
in the elderly. Drugs Aging. 2014; 31:131-140.
2. Wehling M. et al. VALFORTA: a randomized trial to validate the FORTA (Fit fOR The Aged) classification. Age Ageing, 2016;45:262-7.
3. Wehling M. Drug therapy in the elderly: too much or too little, what to do? A new assessment system: fit for the aged FORTA. Dtsch Med Wochenschr
2008; 133: 2289-91.
4. Wehling M. Multimorbidity and polypharmacy: how to reduce the harmful drug load and yet add needed drugs in the elderly? Proposal of a new drug
classification: fit for the aged. J Am Geriatr Soc 2009; 57: 560-561.
5. Wehling M, Burkhardt H. Arzneitherapie für Ältere. Springer-Verlag, Heidelberg, 4. Auflage 2016.
6. Wehling M, Ed., Drug Therapy for the Elderly. Springer-Verlag, Wien 2013
7. Wehling M. How to Use the FORTA ("Fit fOR The Aged") List to Improve Pharmacotherapy in the Elderly. Drug Res. 2016;66:57-62.