fine-needle aspiration cytology of benign and malignant adenomyoepithelioma: report of two cases
TRANSCRIPT
Fine-Needle Aspiration Cytologyof Benign and MalignantAdenomyoepithelioma:Report of Two CasesMasanori Kurashina, M.D.*
Cytological features of a malignant spindle-cell variant and abenign tubular variant of adenomyoepithelioma were examined toimprove diagnosis of this tumor. Fine-needle aspiration cytology,of both a malignant and a benign case, characterized cellular andcohesive cell clusters composed of epithelial and myoepithelialcells. The smears of the malignant case were rich in spindle-shaped myoepithelial cells, admixed with a few epithelial cells. Inabout a fourth of the clusters, atypical cells with enlarged hyper-chromatic nuclei and prominent nucleoli comprised more than20% of cells. The smears of the benign case were composed oftubular epithelial cells surrounding one to several layers of myo-epithelial cells with clear cytoplasm. Mild atypia was occasionallynoticed. A review of the literature showed that a cytologicaldiagnosis of malignancy is not warranted, if nuclear atypia is notgenerally severe. Focal severe atypia is not definitively indicativeof benignity or malignancy. Diagn. Cytopathol. 2002;26:29–34.© 2002 Wiley-Liss, Inc.
Key Words: adenomyoepithelioma; breast; cytology; needle aspi-ration; immunohistochemistry
Adenomyoepithelioma is defined as a tumor composed ofboth epithelial and myoepithelial cell components. Malignantadenomyoepithelioma is known to involve recurrences1–8 ormetastases,2,4,7,9,10 or even death.10,11 Moreover, some casesof adenomyoepithelioma develop malignant changes.1,4,6
Therefore, the exact cytological diagnosis of this disease isimportant. Because this tumor is relatively rare and thecytological features mimic those of other breast diseasessuch as tubular adenoma, intraductal papilloma, fibroade-noma, cystosarcoma phyllodes, fibrocystic disease, myoep-ithelioma, or carcinomas, the cytological and histologicaldiagnosis of this tumor tends to be misinterpreted the first
time.12–15 In the present study, two cases were studied andcompared to previously reported cases, in an effort to im-prove the accuracy of cytological diagnosis of this tumor.
Case ReportsCase 1A 73-yr-old woman, who had been mastectomized 9 yrbefore due to invasive ductal carcinoma (comedo type) ofher left breast, was discovered (upon examination by CT,MRI, and ultrasonography) to have minute tumors in theupper inner quadrant of her right breast. Fine-needle aspi-ration (FNA) cytology of the largest lump was performed,and local excision and lumpectomy of these small nodulesfollowed. Cytologic examination of the tumor led to suspi-cions of a spindle-cell mesenchymal tumor of unknowntype, suggesting borderline malignancy. A histological di-agnosis of intraductal papilloma was made from a surgicalspecimen; a final diagnosis of spindle-cell variant of malig-nant adenomyoepithelioma was made after precise histolog-ical and immunohistochemical examination. One year later,the patient was well without recurrence.
Case 2FNA cytology and examination of frozen sections wereperformed for a 73-yr-old woman who had noticed a tumorof her right breast in the lower outer quadrant region 2 mobefore. The tumor was diagnosed as ductal carcinoma.Though intraductal papilloma was the initial histologicaldiagnosis of the mastectomized specimen, precise histolog-ical and immunohistochemical examination revealed it to bea tubular variant of adenomyoepithelioma.
Cytologic FindingsThe aspirated smears were fixed in 95% ethanol and under-went Papanicolaou staining. In both cases, the cytologicpreparations were characterized by cellular and cohesivecell clusters.
Department of Medical Technology, Nagoya University School ofHealth Sciences, Nagoya, Japan
*Correspondence to: Masanori Kurashina, M.D., Department of MedicalTechnology, Nagoya University School of Health Sciences, 1-1-20, Daiko-Minami, Higashi-ku, Nagoya 461-8673, Japan.E-mail: [email protected]
Received 16 March 2001; Accepted 19 September 2001
© 2002 WILEY-LISS, INC. Diagnostic Cytopathology, Vol 26, No 1 29DOI 10.1002/dc.10037

Case 1The specimen was rich in spindle-shaped cells (Fig. 1), butthere were a few cylinder-like epithelial cells arranged in alayer (Fig. 2). The spindle cells often consisted of bundlesadmixed with large or small spaces. The walls of thesespaces mostly consisted of spindle-shaped cells, but a few ofthese walls contained a small number of columnar epithelialcells. Slender elongated nuclei were prevalent in some clus-ters (Fig. 1). In about one fourth of the clusters, over 20%of the cells were atypical, with enlarged hyperchromaticnuclei and prominent nucleoli up to 2.5 �m in diameter. Thelargest tumor cell was 17.5 �m in diameter. Intranuclearcytoplasmic inclusions were occasionally present in plump,spindle-shaped myoepithelial cells (Fig. 3). Mitoses wereobserved in about 1.5% of atypical cells, which all hadnuclei with a minimum diameter greater than 10 �m. Asmall number of naked oval cells were found in thebackground.
Case 2
The clusters were composed of epithelial cells occasionallyforming tubules and one to several layers of round tospindle cells, with clear cytoplasm that possessed cytolog-ical features of myoepithelial cells (Fig. 4). These myoep-ithelial cells often surrounded the tubular or solid-tubularepithelial cells. The chromatin of the tumor cells was dis-perse, and the largest nuclei were 8.8 �m in diameter. Smallnucleoli were observed in about 30% of tumor cells. Mito-ses were observed in a small number of cells. An intranu-clear inclusion was found in a myoepithelial cell. Severalnaked, oval nuclei with dispersed chromatin were scatteredin the background. The cytological features were interpretedas ductal carcinoma, because tubular epithelial cells werestacked three-dimensionally and were not associated withthe naked myoepithelial cells adjacent to them, and becausethe clear cells were mistaken for epithelial cells at that time.
Fig. 1. Aspiration cytology, showing a cellular and cohesive cell cluster ofspindle-shaped tumor cells. The cluster of spindle cells often consisted ofbundles, admixed with large or small spaces (Papanicolaou stain, �200).
Fig. 2. A few cylinder-like epithelial cells arranged in a layer (Papanico-laou stain, �560).
Fig. 3. Atypical cells and intranuclear cytoplasmic inclusion in malignantadenomyoepithelioma (Papanicolaou stain, �1,000).
Fig. 4. Aspiration cytology of tubular adenomyoepithelioma, showing acohesive cluster composed of gland-forming epithelial cells and one toseveral layers of myoepithelial cells with clear cytoplasm (Papanicolaoustain, �200).
KURASHINA
30 Diagnostic Cytopathology, Vol 26, No 1

Pathologic FindingsCase 1Macroscopically, the main tumor, with a long axis of 0.7cm, was well-demarcated in some regions, but had irregularinvasive margins in other regions. There were seven smallsatellite nodules within 2.2 cm from the main tumor, with along axis ranging from 0.1–0.4 cm.
Microscopically, the larger three tumors were demarcatedentirely by thick hyaline fibrous tissue, but focal invasionwas observed in some regions of these tumors (Fig. 5). Twoother smaller tumors that were mainly composed of lessatypical spindle cells were not demarcated in the fattytissue. One tumor contained a cystically dilated lumenwithin the tumor nest. The main tumor and two other tumorswere predominantly composed of spindle cells admixedwith glandular lumina. The ratio of epithelial to myoepithe-lial components was different for each area and nodule:some regions were rich in the epithelial component, whileothers were almost completely composed of spindle-shapedcells. Both the epithelial and the myoepithelial cells occa-sionally showed a moderate degree of pleomorphism andatypia. The atypical cells showed enlarged, irregularlyshaped nuclei and one or two prominent nucleoli (Fig. 6). Inone large tumor, hyperchromatic large nuclei with a shortaxis greater than 10 �m were frequently present. Intranu-clear cytoplasmic inclusions were present in a small numberof spindle-shaped myoepithelial cells. Nuclear palisadingwas seen in some regions rich in spindle cells. The epithelialcells were cuboidal or flattened, with focal apocrine meta-plasia. Most of the tubular lumina contained a periodicacid-Schiff (PAS)-positive mucous substance, and some ofthe lumina contained psammoma bodies. Some epithelialcells exhibited diastase resistance and PAS positivity. Ne-crosis was not observed. Mitoses were observed in 2 per 10high-power fields. Near the main tumor, ductal hyperplasiawas present.
Case 2
Macroscopically, the tumor was well-demarcated and itslong axis was 1.8 cm long. Histologically, the tumor waslocated in a large duct surrounded by thick fibrous tissue. Itconsisted of many branching tubules, each of which wassurrounded by one to several layers of myoepithelial cellswith clear cytoplasm (Fig. 7). In some regions in whichthere was a great proliferation of these myoepithelial cells,clear cell nodules were formed without associated tubularepithelial cells. Most tubular epithelial cells were columnarwith dark cytoplasm, and they occasionally contained prom-inent nucleoli. In the luminal portion of a few of the tubules,there were solid cell nests accompanied by tiny glandularspaces. These cells were oval to slender in shape, withlighter-colored cytoplasm. Mitotic figures in myoepithelialcells were counted in 5 per 10 high-power fields. Intranu-clear inclusions were observed in a small number of epithe-
Fig. 5. Histologic section of malignant adenomyoepithelioma, showingfocal invasion (hematoxylin-eosin stain, �100).
Fig. 6. Atypical cells in malignant adenomyoepithelioma, showing en-larged, irregularly shaped nuclei and one or two prominent nucleoli (he-matoxylin-eosin stain, �400).
Fig. 7. Histologic sections of adenomyoepithelioma, showing tubular andsolid-tubular structures surrounding one to several layers of myoepithelialcells with clear cytoplasm (hematoxylin-eosin stain, �400).
ADENOMYOEPITHELIOMA
Diagnostic Cytopathology, Vol 26, No 1 31

lial and myoepithelial cells. Toluidin blue staining revealedvery faint traces of metachromatic mucous substance in onefocus.
Immunohistochemical ExaminationMultiple immunohistochemical examinations were per-formed on materials fixed in formalin and embedded inparaffin, using the labelled streptavidin-biotin-peroxidase(LSAB) method. A polyclonal antibody against keratin anda monoclonal antibody against desmin were purchased fromDAKO (Santa Barbara, CA). Monoclonal antibodies againstepithelial membrane antigen (EMA), smooth muscle actin(SMA), vimentin, S-100 protein, and Mib-1 were purchasedfrom Immunotech (Marseille, France). A monoclonal anti-body against cytokeratin 18 was purchased from ZymedLaboratories, Inc. (San Francisco, CA).
The tubular epithelial cells and a small number of myo-epithelial cells were positive for cytokeratin 18 (Fig. 8a,b).Epithelial cells and some myoepithelial cells were positivefor keratin. Tubular epithelial cells were frequently positivefor EMA, but only a few nontubular epithelial cells andmyoepithelial cells were positive. Most myoepithelial cells,and a small number of epithelial cells, were positive forSMA (Fig. 8c,d). Myoepithelial cells were positive forvimentin, and negative for desmin. In case 2, S-100 proteinwas occasionally positive on both epithelial and myoepithe-lial cells. However, in case 1, S-100 reactivity was mostlyconfined to these cells in the peripheral regions of thetumors. In case 1, 3.3% of atypical cells and 0.3% ofelongated spindle cells were Mib-1-positive; in case 2, 3.0%of tumor cells were Mib-1-positive.
DiscussionTo diagnose adenomyoepithelioma correctly, it is importantto understand various patterns exhibited by this tumor.Tavassoli6 histologically classified adenomyoepitheliomainto three categories of variants: spindle-cell, tubular, andlobulated. The epithelial cells are often formed into one ofthe following structures: tubular, apocrine metaplasia, solid,papillary, cystic, or trabecular. The myoepithelial cells oftenhave round to spindle-shaped nuclei,14,16 clear cytoplasm,17
or dispersed naked oval nuclei.14,15,18 Electron microscopicexamination has revealed that spindled myoepithelial cellsadhere to each other via desmosomes.11,16,17,19,20 This ex-plains why spindled myoepithelial cells in smears usuallyform cohesive cell clusters, though loosely cohesive clustershave also been observed.11,12 Though it is not knownwhether other types of myoepithelial cells in adenomyoepi-thelioma contain many desmosomes (equal to those in spin-dled myoepithelial cells), large clusters of cohesive myoep-ithelial cells like those seen in case 2 have been reported forthe tubular type.14 Similar findings have not been reported
for other cases of this variant.15,17,22,23 Thus, it appears that,in most cases, myoepithelial cells with clear cytoplasm arenot so cohesive as in case 2.
Though histologically biphasic cellular components areeasily found, cytological specimens may be obtained fromareas in which one cell component is predominant, as incase 1. When the majority of cells in a cytological specimenare cohesive myoepithelial cells, careful examination for thepresence of epithelial cells is necessary in order to differ-entiate it from myoepithelioma. On the other hand, when aspecimen is predominantly composed of epithelial cells,carcinoma or adenoma is usually diagnosed.23 Since dis-persed naked oval nuclei have been observed in fibroade-noma and phyllodes tumors, they are not specific for ad-enomyoepithelioma. In phyllodes tumors, stromal cellsshow a spindled shape with mild to severe atypia, but theyare usually discohesive. Although stromal cells in highlycellular fragments of malignant phyllodes tumors show atendency toward cohesiveness,24,25 their spindle-shapedcells are seem to be less cohesive than those ofadenomyoepithelioma.
In adenoma, adenosis, and intraductal papilloma, glandu-lar epithelial cells are predominant, whereas in adenomyo-epithelioma, myoepithelial cells are numerous in many ar-eas and are rich in cytoplasm. Cytologically, in the threeformer tumor types, myoepithelial cells are present in adispersed pattern, because myoepithelial cells in these tu-mors are usually present as a single layer, and do not cohereas tightly to each other as in adenomyoepithelioma.
In benign cases, intranuclear cytoplasmic inclusions havebeen observed in the large nuclei of myoepithelial cells inbenign cases.14,18 In the present cases, such inclusions werenot confined to atypical myoepithelial cells, and they werefound in both malignant and benign cases. In terms of breastcytology, these inclusions are not specific indicators ofadenomyoepithelioma.14,18
Metachromatic myxoid substance has often been ob-served in cytologic studies in which specimens were stainedwith Diff-Quik or May-Grunwald-Giemsa.12,15,16,21,22 Re-cently, an adenomyoepithelioma producing a large amountof myxoid matrix was reported.26 However, in some reportsof adenomyoepithelioma, there is no mention of this sub-stance.14,17,18 In the present cases, Toluidin blue stainingrevealed only faint traces of it in one focus of case 2, andthere was no evidence of it in case 1. Thus, adenomyoepi-thelioma is not always associated with myxoid substance,although the presence of it increases the likelihood ofadenomyoepithelioma.
Cytological reports on adenomyoepithelioma have beenconfined almost completely to benign cases,12,14–18,21,22 ex-cept for one malignant case in which the description sug-gested mild cytological atypia.9 In other words, cytologicalcriteria for differentiating between benign and malignantadenomyoepitheliomas have not been established. The data
KURASHINA
32 Diagnostic Cytopathology, Vol 26, No 1
from histological reports of malignant adenomyoepithe-lioma indicate that cellular atypia was varied. Some showedmarked atypia including enlarged nuclei, irregular nuclearcontours, coarse chromatin and distinct nucleoli, and/or amoderate degree of cellular pleomorphism,9,27 but in somecases, atypia was mild or focally marked.2,4,11,23,28,29 More-over, focally marked cellular atypia has been reported incases of adenomyoepithelioma.12,15,18,30 Therefore, a cyto-logical specimen exhibiting mild cellular atypia or focallymarked atypia cannot be conclusively diagnosed as benignor malignant based on atypia. In previous reports, mitoticactivity was high in many malignant cases and low in mostbenign cases, but exceeded 10 mitoses per 10 high-powerfields in 3 benign cases6 and was under 5 mitoses per 10high-power fields in 6 malignant cases.2,8 Thus, it is evidentthat there is some overlap in cytological atypia betweenbenign and malignant adenomyoepithelioma. Cytologicalspecimens in which many of the clusters predominantlyconsist of atypical cells with enlarged, hyperchromatic, ovalto plump spindling, irregularly shaped nuclei, and enlargednucleoli may be malignant.
Though most reported cases of adenomyoepithelioma,including malignant cases, have involved a single nodule,the present case 1 and a few previously reported malignantcases involved multiple nodules.11,28 Some of the nodules incase 1 showed focal invasion. Because multiple noduleshave been reported in a few cases of benign adenomyoepi-thelioma,6 their cellular atypia and infiltrating tendencyconstitute important data for differentiation between malig-nancy and benignity.
Immunohistochemically, high-molecular-weight cytoker-atin (34BE12)31 and S-100 protein32 are not specific formyoepithelial cells. In a report in which normal specimens,papilloma, and mastopathy were examined, epithelial cellsstained positively for low-molecular-weight cytokeratins,but myoepithelial cells did not.33 In the two present cases, asmall fraction of myoepithelial cells were positive for cytoker-atin 18, which is a low-molecular-weight cytokeratin. Pos-itivity of myoepithelial cells for cytokeratin 18 was reportedin a relatively small number of malignant cases.2,4,12,23 Alsoin the present cases, a small fraction of myoepithelial cellswere positive for EMA. Thus, a slight overlap of immuno-histochemical features between epithelial and myoepithelialcells occurred in a small fraction of cells in the presentadenomyoepithelioma cases. Such a finding was not previ-
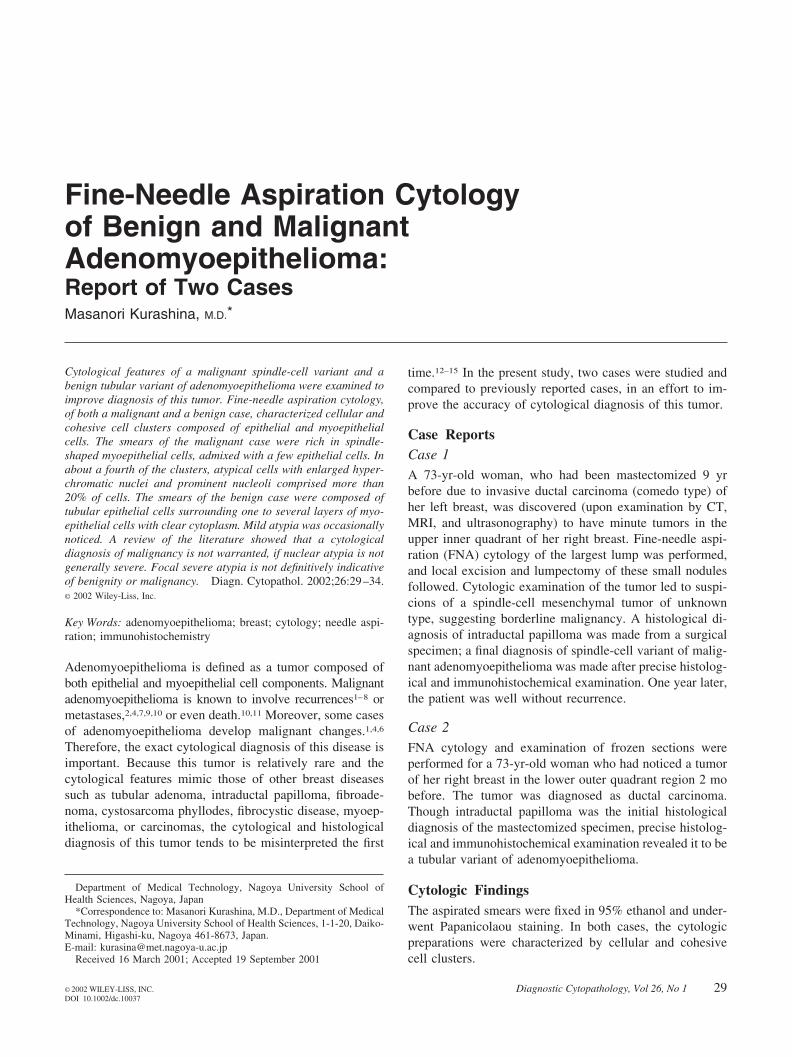
Fig. 8. Immunohistochemical findings. a: Cytokeratin 18 positivity in case1 in about one half of the epithelial cells and a few myoepithelial cells(immunoperoxidase, �200). b: Cytokeratin 18 positivity in case 2 in theepithelial cells and a small number of myoepithelial cells with clearcytoplasm (arrow; immunoperoxidase, �400). c: SMA positivity in case 1in most spindle cells and a few epithelial cells (arrow; immunoperoxidase,�200). d: SMA positivity in case 2 in myoepithelial cells and a smallnumber of epithelial-like cells in a solid-tubular epithelial lesion (arrow;immunoperoxidase, �400).
ADENOMYOEPITHELIOMA
Diagnostic Cytopathology, Vol 26, No 1 33

ously reported for benign adenomyoepithelioma, but hasbeen reported for phyllodes tumors.34 EMA positivity ofspindle-cell components has also been reported for spindle-cell carcinoma. The high frequency of EMA-positive cellsin spindle-cell components of spindle-cell carcinoma andelectron microscopic findings have demonstrated that spin-dle-cell carcinoma derives from epithelial cells.35 The stain-ing patterns for desmin and vimentin in the present caseswere consistent with previous reports in the literature.19,30
In conclusion, the present cytological diagnosis of adeno-myoepithelioma was characterized by cohesive clusters com-posed of epithelial and myoepithelial cells. Because it is evi-dent that there is overlap in cytological atypia between benignand malignant adenomyoepithelioma, cytological differentia-tion between benignity and malignancy is warranted whenspecimens show mild atypia or focal marked atypia.
References1. Kiaer H, Nielsen B, Paulsen S, Sorensen IM, Dyreborg U, Blichert-
Toft M. Adenomyoepithelial adenosis and low-grade malignant ad-enomyoepithelioma of the breast. Virchows Arch [A] 1984;405:55–67.
2. Loose JH, Patchefsky AS, Hollander IJ, Lavin LS, Cooper HS, KatzSM. Adenomyoepithelioma of the breast. A spectrum of biologicbehavior. Am J Surg Pathol 1992;16:868–876.
3. Pauwels C, De Potter C. Adenomyoepithelioma of the breast withfeatures of malignancy. Histopathology 1994;24:94–96.
4. Rasbridge SA, Millis RR. Adenomyoepithelioma of the breast withmalignant features. Virchows Arch 1998;432:123–130.
5. Rosen PP. Adenomyoepithelioma of the breast. Hum Pathol 1987;18:1232–1237.
6. Tavassoli FA. Myoepithelial lesions of the breast. Myoepitheliosis,adenomyoepithelioma, and myoepithelial carcinoma. Am J SurgPathol 1991;15:554–568.
7. Trojani M, Guiu M, Trouette H, De Mascarel I, Cocquet M. Malignantadenomyoepithelioma of the breast. An immunohistochemical, cyto-photometric, and ultrastructural study of a case with lung metastases.Am J Clin Pathol 2000;98:598–602.
8. Young RH, Clement PB. Adenomyoepithelioma of the breast. A reportof three cases and review of the literature. Am J Clin Pathol 1988;89:308–314.
9. Bult P, Verwiel JM, Wobbes T, Kooy Smits MM, Biert J, Holland R.Malignant adenomyoepithelioma of the breast with metastasis in thethyroid gland 12 years after excision of the primary tumor. Case reportand review of the literature. Virchows Arch 2000;436:158–166.
10. Simpson RH, Cope N, Skalova A, Michal M. Malignant adenomyo-epithelioma of the breast with mixed osteogenic, spindle cell, andcarcinomatous differentiation. Am J Surg Pathol 1998;22:631–636.
11. Chen PC, Chen CK, Nicastri AD, Wait RB. Myoepithelial carcinomaof the breast with distant metastasis and accompanied by adenomyo-epitheliomas. Histopathology 1994;24:543–548.
12. Birdsong GG, Bishara HM, Costa MJ. Adenomyoepithelioma of thebreast: report of a case initially examined by fine-needle aspiration.Diagn Cytopathol 1993;9:547–550.
13. Choi JS, Bae JY, Jung WH. Adenomyoepithelioma of the breast—itsdiagnostic problems and histogenesis. Yonsei Med J 1996;37:284–289.
14. Laforga JB, Aranda FI, Sevilla F. Adenomyoepithelioma of the breast:report of two cases with prominent cystic changes and intranuclearinclusions. Diagn Cytopathol 1998;19:55–58.
15. Niemann TH, Benda JA, Cohen MB. Adenomyoepithelioma of thebreast: fine-needle aspiration biopsy and histologic findings. DiagnCytopathol 1995;12:245–250.
16. Vielh P, Thiery JP, Validire P, Annick de Maublanc M, Woto G.Adenomyoepithelioma of the breast: fine-needle sampling with histo-logic, immunohistologic, and electron microscopic analysis. DiagnCytopathol 1993;9:188–193.
17. Nilsson B, Wee A, Rauff A, Raju GC. Adenomyoepithelioma of thebreast. Report of a case with fine needle aspiration cytology andhistologic, immunohistochemical and ultrastructural correlation. ActaCytol 1994;38:431–434.
18. Valente PT, Stuckey JH. Fine-needle aspiration cytology of mammaryadenomyoepithelioma: report of a case with intranuclear cytoplasmicinclusions. Diagn Cytopathol 1994;10:165–168.
19. Weidner N, Levine JD. Spindle-cell adenomyoepithelioma of thebreast. A microscopic, ultrastructural, and immunocytochemical study.Cancer 1988;62:1561–1567.
20. Zarbo RJ, Oberman HA. Cellular adenomyoepithelioma of the breast.Am J Surg Pathol 2001;7:863–870.
21. Torlakovic E, Ames ED, Manivel JC, Stanley MW. Benign andmalignant neoplasms of myoepithelial cells: cytologic findings. DiagnCytopathol 1993;9:655–660.
22. Hock YL, Chan SY. Adenomyoepithelioma of the breast. A casereport correlating cytologic and histologic features. Acta Cytol 1994;38:953–956.
23. Nomura K, Fukunaga M, Uchida K, Aizawa S. Adenomyoepitheliomaof the breast with exaggerated proliferation of epithelial cells: report ofa case. Pathol Int 1996;46:1011–1014.
24. Shabb NS. Phyllodes tumor. Fine needle aspiration cytology of eightcases. Acta Cytol 1997;41:321–326.
25. Shimizu K, Masawa N, Yamada T, Okamoto K, Kanda K. Cytologicevaluation of phyllodes tumors as compared to fibroadenomas of thebreast. Acta Cytol 1994;38:891–897.
26. Sugano I, Nagao T, Tajima Y, Ishida Y, Nagao K, Oeda Y, TakahashiT. Malignant adenomyoepithelioma of the breast: a non-tubular andmatrix-producing variant. Pathol Int 2001;51:193–199.
27. Ahmed AA, Heller DS. Malignant adenomyoepithelioma of the breastwith malignant proliferation of epithelial and myoepithelial elements:a case report and review of the literature. Arch Pathol Lab Med2000;124:632–636.
28. Tamura S, Enjoji M, Toyoshima S, Terasaka R. Adenomyoepithe-lioma of the breast. A case report with an immunohistochemical study.Acta Pathol Jpn 1988;38:659–665.
29. Tsuda H, Mukai K, Fukutomi T, Hirohashi S. Malignant progressionof adenomyoepithelial adenosis of the breast. Pathol Int 1994;44:475–479.
30. Koyama M, Kurotaki H, Yagihashi N, Aizawa S, Sugai M, Kamata Y,Oyama T, Yagihashi S. Immunohistochemical assessment of prolifer-ative activity in mammary adenomyoepithelioma. Histopathology1997;31:134–139.
31. Joshi MG, Lee AK, Pedersen CA, Schnitt S, Camus MG, Hughes KS.The role of immunocytochemical markers in the differential diagnosisof proliferative and neoplastic lesions of the breast. Mod Pathol1996;9:57–62.
32. Bassler R, Katzer B. Histopathology of myoepithelial (basocellular)hyperplasias in adenosis and epitheliosis of the breast demonstrated bythe reactivity of cytokeratins and S100 protein. Virchows Arch [A]1992;421:435–442.
33. Jarasch ED, Nagle RB, Kaufmann M, Maurer C, Boker WJ. Differ-ential diagnosis of benign epithelial proliferations and carcinomas ofthe breast using antibodies to cytokeratins. Hum Pathol 1988;19:276–289.
34. Aranda FI, Laforga JB, Lopez JI. Phyllodes tumor of the breast. Animmunohistochemical study of 28 cases with special attention to therole of myofibroblasts. Pathol Res Pract 1994;190:474–481.
35. Nakayama Y, Iwasaki H, Iwanaga S, Nakamura H, Shiroshita T,Kikuchi M, Jozaki H, Hashimoto M, Ikeda S. Spindle cell carcinomaof the breast: a case report and an immunohistochemical study includ-ing p53 and Ki-67 expression. Pathol Int 1997;47:404–411.
KURASHINA
34 Diagnostic Cytopathology, Vol 26, No 1