finance team national hispanic medical association leadership fellowship 2003 jose castro md elsa...
TRANSCRIPT

Finance TeamNational Hispanic Medical Association
Leadership Fellowship 2003
Jose Castro MD
Elsa Escalera MD
Inginia Genao MD
Advisor: Charles Brecher PhD
The New Medicare Law:Implications for vulnerable
population

Outline Overview Medicare prescription drug
improvement and modernization act of 2003 Impact on the dual eligibles (Medicaid and
Medicare) Recommendations Summary

Overview of the Medicare prescription drug improvement and modernization act of 2003.
41.7 million beneficiaries of Medicare to new coverage of prescription drugs
$ 410 billion (calculated by CBO) 2004-2013 Voluntary benefit effective January 1, 2006 Annual premium in 2006 about $420—can vary by plan Annual $250 deductible indexed to drug spending Coverage gap (“donut hole”)—no coverage for spending between
$2,250 and $5,100 Subsidies for low-income beneficiaries

Standard Drug Benefit
2006 2013
Annual Deductible: $250 $445
Coinsurance to Initial Limit: 25% 25%
Initial Limit: $2,250 $4,000
Out-of-Pocket Threshold: $3,600 $6,400
Coverage Gap: $2,850 $5,066
Coinsurance Above OOP: (greater of)
$2/$5or 5%
$3/$8or 5%


Dual Eligibles
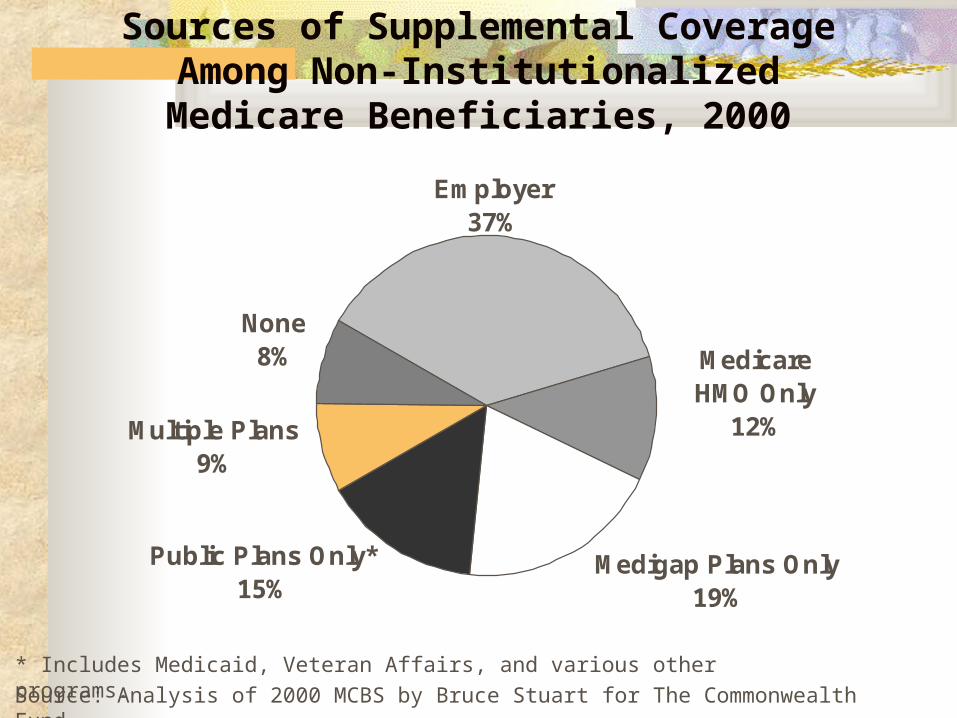
Sources of Supplemental CoverageAmong Non-InstitutionalizedMedicare Beneficiaries, 2000
None8%
Multiple Plans9%
Public Plans Only*15%
Medigap Plans Only 19%
Medicare HMO Only
12%
Employer37%
Source: Analysis of 2000 MCBS by Bruce Stuart for The Commonwealth Fund.
* Includes Medicaid, Veteran Affairs, and various other programs.

Dual eligibles: Who Are They? Medicaid fill gaps in Medicare > 7 million low-
income seniors: enrolled in both Medicaid/Medicare. Must have income well bellow the poverty line and
minimal assets to qualify for Medicaid, Dual eligibles are much poorer than other Medicare
beneficiaries. They also tend to have far more extensive health care
needs than other Medicare beneficiaries:

Dual Eligibles: How poor, how sick? 70% of dual eligibles have annual incomes < $ 10 K
compared to 13 % of all other Medicare beneficiaries. More than twice as likely to be in fair or poor health as other
Medicare beneficiaries (52% versus 24%). ~ 25% of dual eligibles are in long-term care facilities
compared to 2% of other Medicare beneficiaries. Dual eligibles are more than twice as likely to have
Alzheimer’s (6% versus 3%), more likely to have diabetes (24% versus 17%) and to have suffered a stroke (14% versus 11%) than other Medicare beneficiaries.
New Medicare Law for Dual eligibles
No deductible and no premium for enrolling in an average or low cost plan.
Special assistance with cost-sharing obligations (no doughnut hole for dual eligibles). Will not pay for 100% once they exceed limit of $2,250.
O income up to 100% of poverty: no more than $1/generic and $ 3/brand name drug in 2006. Majority will fall into this category.
O dual eligibles with income >100% of poverty. $2/generic and $5/brand name drug in 2006.

Impacts on Dual Eligibles: Should the Fight Continue?
Complex choices Navigating the system Variations from state to state Drug coverage restrictions under part D
plan Array of drugs covered Cost-sharing

III Recommendations Focus in Hispanics: will have additional
challenges. Measuring outcomes.

In 2002, almost 2 million Hispanics > 65 ys. Data gathering should be focused on this
group to estimate the impact the new Medicare law.
Data should be the best advocacy tool. One way to obtain reliable data is research.
Outcomes research Outcome research: measures outcomes. Set of analytic methods that produce
information about the benefits, risks, and costs of health care services.

Measuring outcomes There are many potential measurements that can be incorporated
in the study, but should be oriented to the particular characteristics of the study population, for example:
Measure Example Mortality cardiovascular associated mortality Physiology blood pressure Clinical events stroke Functional status SF-36, a 36 item health survey Experience with care Consumer Assessment of Health Plan

Summary Good benefits for many beneficiaries. May be a challenge for the most
vulnerable, in particular Hispanics. Outcome research focus in this population
and plan in advance.

Senate Majority Leader Bill Frist said, “This bill is an extraordinary day for seniors and indeed all Americans…The legislation we just passed is epochal…It modernizes Medicare to provide 21st century care for our seniors.”

Senate Minority Leader Tom Daschle predicts that seniors would mobilize as they did 38 years ago for the original Medicare Bill once they learn how the bill works. “They [lobbyists] will do well. Our seniors will not, and that is why the fight will go on.”

