final reportcst trainer - qaclinicalskills.co.uk peripatetic clinical skills trainer evaluation:...
TRANSCRIPT

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
! 1
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT LEEDS BECKETT UNIVERSITY www.leedsbeckett.ac.uk
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
!
! 2

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Michelle Briggs BSc, MSc, PhD, RN Professor, Institute for Health and Wellbeing Faculty of Health and Social Sciences Leeds Beckett University, Portland Building Leeds, United Kingdom LS1 3HE 0113 8121924 [email protected] Frances Darby BA (Hons), MA, PhD, PGCE, RN Research Assistant Faculty of Health and Social Sciences Leeds Beckett University Leeds, United Kingdom LS1 3HE 07876347080 9 (mobile) [email protected] Fiona Harrison Co-Director Practice Learning and Employability Unit Faculty of Health and Social Sciences Leeds Beckett University Leeds, United Kingdom LS1 3HE Acknowledgements: Clinical advisory group members Kay Ford Regional Clinical Skills AdvisorHealth Education Yorkshire and the Humber/Faculty of Health and Social Sciences Leeds Beckett University Jackie Mason Peripatetic Skills Trainer Health Education Yorkshire and the Humber/Faculty of Health and Social Sciences Leeds Beckett University Joanne Barrott
Manager to the Strategic Clinical Skills Advisory Team Previously Health Education Yorkshire and the Humber/Faculty of Health & Social Sciences Leeds Beckett University Sue Sherwin Head of School of Health and Community Studies Faculty of Health & Social Sciences Leeds Beckett University
�
! 3

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Introduction The aim of this evaluation was to assess the impact of the provision of the Clinical Skills Trainer (CST) post. The evaluation is based on the principles of realist evaluation (see figure 1) and aimed to produce a description of the current evidence base and potential impact of CST post and then chart whether and how this post has an impact in practice in care homes. Evaluation questions: What are the enablers to the provision of Clinical Skills Trainer (CST) post What are the barriers to the provision of the CST post? What has been the impact of providing the CST post?
� Figure 1 : Evaluation process (based on the principles of realist evaluation)
1. Literat
2. Devel
3. Intervi
4. Devel
! 1

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
The stages of the proposed evaluation are outlined below and are underpinned by realist evaluation methodology) SECTION 1 Report from Stage 1 : Literature review The review aims to describe the relevant evidence on the provision of peripatetic clinical skills training. The output from this stage presents and discusses the theories of how CS trainers may work and outlines the enablers and the barriers. SECTION 2 Report from Stage 2: Develop initial theories of the model of CST post To develop a possible theories of how the training may have an impact in the identified nursing homes. The output of this stage will be the development of the outline of what constitutes success and failure of the CST in these settings and a plan for impact data collection. This involves discussion of the findings of the literature with core team members SECTION 3 Report from Stage 3:Data collection for outcomes identified; Interview study Recruiting nursing homes and relevant stakeholders to collect data that will help test, refine the developing theory. SECTION 4 Report from stage 4: Develop analysis report on impact of the service To elicit impacts (positive and negative) of the training beyond those anticipated and develop impact case studies. ! 2

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Section 1: Literature review and stakeholder input The aim of the literature review was to identify and explore the types of training posts in clinical nursing skills that could be accessed by staff working in care homes and to develop an understanding of the factors which enable or prevent its implementation. Comprising the positive and negative impact of clinical skills training on the institutions and individuals involved, it provided an evidence base for the development and progression of the current project. The search strategy for the review was undertaken during July 2013 utilising library resources at Leeds Metropolitan University, Leeds University and the Royal College of Nursing. The databases searched were: British Nursing Index; Cinahl Plus (Cumulative Index of Nursing and Allied Health Literature); PubMed; Academic Search Complete; Medline; ProQuest Deep Indexing: Nursing; ProQuest Nursing and Allied Health Source; ProQuest Health and Medicine; Scopus. The search terms were derived from various combinations of the words in the phrases ‘clinical nursing skills training’, ‘peripatetic clinical skills training’, ‘nursing homes’, ‘care homes’, ‘nursing skills’, ‘training the trainer’, ‘clinical skills training programmes/courses’, ‘clinical skills trainer’. The search range included papers and articles published in the English language with no date being specified. After reviewing the bibliographies, literature was included which focused on clinical nursing skills and the approach taken to staff training by nursing and care homes. All literature dealing with skills other than clinical nursing skills or with no reference to the training process and not published in the English language were excluded. A total of 24 papers were included in the review from which core themes were identified. The extent of interest in the training of nursing home staff was reflected in the international range of papers and articles included in the review. The majority had their origins in the UK (n = 16) whilst other countries represented were the US (n = 3), the Republic of Ireland (n = 1), Northern Ireland (n = 1), Denmark (n = 1), Norway (n = 1) and Australia (n = 1). The number of institutions involved in any one programme ranged from 1 (Lekan et al., 2010) to 122 (Heeley-Creed et al., 2007). At a strategic level, each programme was managed by different combinations of statutory and voluntary agencies from the worlds of health, local government, social care and education. The training was delivered by educationalists (n = 4), multidisciplinary teams (often headed by a designated professional) (n = 13) or by lone designated practitioners (n = 10). Some of the training programmes were specifically for registered nurses (n = 7), whilst others were designed for non-registered healthcare staff (n = 6). The majority of the programmes provided training for all grades of staff (n = 10). The trainers used a variety of venues for their training sessions including health centres, nursing homes and nurse training centres. Seven programmes used only classroom teaching whilst 13 preferred to teach trainees in the workplace. Five programmes used a combination of the two. Only three of the training programmes were based on
! 3
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
a theoretical model; Lekan et al., (2010) referred to the Connected Learning Model whilst Raunkiaer and Timm (2010) and Lansdell and Mahoney (2011a & b) looked at Competency Development. The content of each training programme was either based around general workplace development issues, up skilling staff or updating existing skills (n = 7) or alternatively was focussed on a specific theme (n = 15). These themes were continence management (Hall et al., 1988; Ehlman et al., 2012), end of life care (Avis, 1999; Heals, 2008; Waldron et al., 2008; Raunkier and Timm, 2010; Lansdell and Mahoney, 2011a & b), diabetes care (Heeley-Creed et al.,2007; Hausken and Graue, 2013), nursing care of older people (Anderson, 2004), managing heart failure (Lekan et al., 2010), reducing the prevalence of hip fractures (Davies et al., 2004), dementia care (Borbasi et al., 2010), pressure ulcer prevention (Law, 2003) and care in nursing homes (Hayes and Martin, 2004). Interestingly, only four of the papers described programmes which, like the current project, involved a combination of university engagement with clinical nursing skills training being carried out in the workplace (Morgan and Conrad, 2008; Lekan et al., 2010; Butler, 2012; Ehlman et al., 2012). The clinical nursing skills that trainees could acquire from the programmes are listed in Figure 2:
! 4

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Figure 2 Review of Clinical skills training provided
CLINICAL NURSING SKILLS WOUND MANAGEMENT
• Managing diabetic foot ulcers • Dressing wounds • Pressure ulcer prevention
CONTINENCE MANAGEMENT • Proficiency in bladder ultrasound scanning • Male/female and suprapubic catheterisation
MAINTAINING INDEPENDENCE THROUGH MOBILITY AND COMMUNICATION • Preventing falls • Using hip protectors • Ear irrigation
ADMINISTRATION OF PRESCRIBED MEDICINE/THERAPY • Administering of insulin • Administering subcutaneous fluid replacement therapy • Administering vaccinations • Administering oxygen • Administering intravenous fluids • Managing syringe drivers
MONITORING AND RECORDING CLINICAL OBSERVATIONS • Recording and monitoring blood pressure and temperature, pulse and
respiration readings • Blood glucose monitoring • Urine testing
MAINTAINING INTEGRITY OF VITAL BODY SYSTEMS • Venepuncture • Cannulation • Cardiopulmonary resuscitation • Replacing gastrostomy tubes • Tracheotomy care • Managing central venous pressure lines
! 5

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
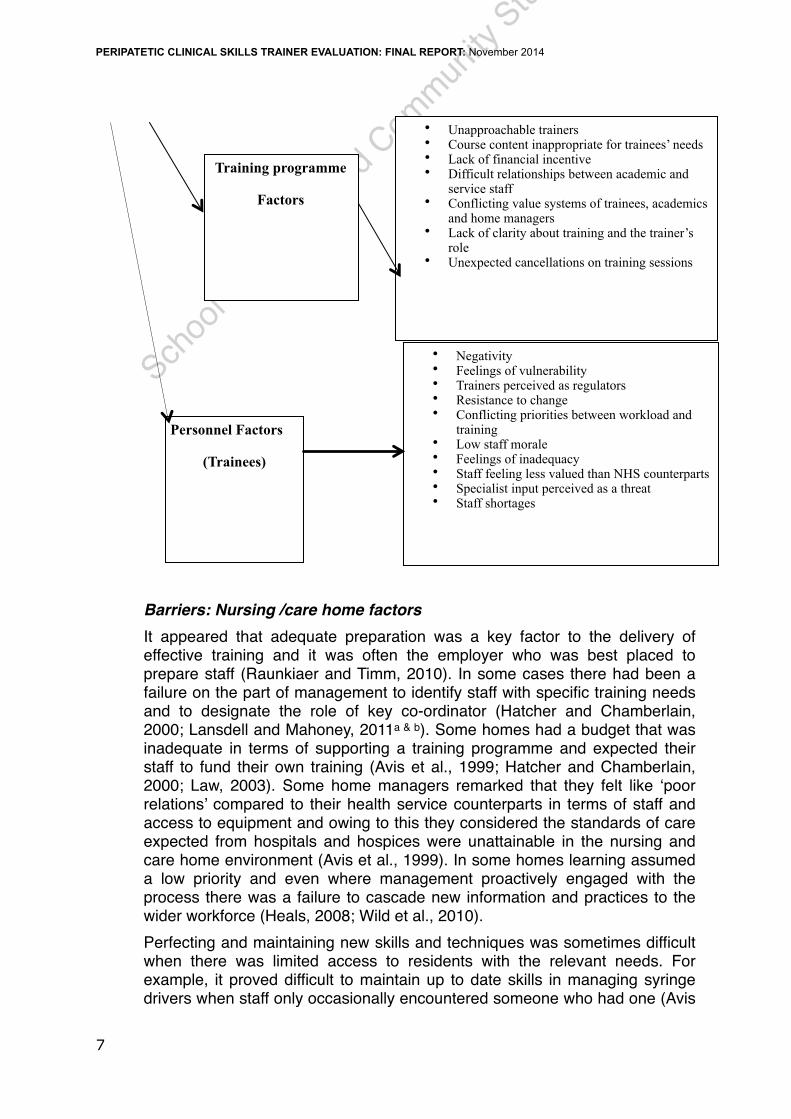
Review of Barriers to training The literature identified numerous issues that posed difficulties for the effective implementation of training programmes. They were grouped under three main themes; those that were a result of the nursing and care home management style and ethos, those that evolved from the course itself and those that were connected with the personal qualities of the trainees (Figure 3)
Figure 3 Barriers
! 6
BARRIERS
Nursing /Care home
Factors
• Changing workforce • Staff shortages • Upskilled staff taken away from basic duties • Learning has low priority • Inadequate staff preparation • New learning not shared with others • Lack of potential trainees • Lack of time • Training needs not identified • Poor administration • Inadequate training budget • Lack of key co-ordinator • Low management self esteem • Low management morale • Infrequent possibilities to practise new skills • Lack of trained nurse supervision
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Barriers: Nursing /care home factors It appeared that adequate preparation was a key factor to the delivery of effective training and it was often the employer who was best placed to prepare staff (Raunkiaer and Timm, 2010). In some cases there had been a failure on the part of management to identify staff with specific training needs and to designate the role of key co-ordinator (Hatcher and Chamberlain, 2000; Lansdell and Mahoney, 2011a & b). Some homes had a budget that was inadequate in terms of supporting a training programme and expected their staff to fund their own training (Avis et al., 1999; Hatcher and Chamberlain, 2000; Law, 2003). Some home managers remarked that they felt like ‘poor relations’ compared to their health service counterparts in terms of staff and access to equipment and owing to this they considered the standards of care expected from hospitals and hospices were unattainable in the nursing and care home environment (Avis et al., 1999). In some homes learning assumed a low priority and even where management proactively engaged with the process there was a failure to cascade new information and practices to the wider workforce (Heals, 2008; Wild et al., 2010). Perfecting and maintaining new skills and techniques was sometimes difficult when there was limited access to residents with the relevant needs. For example, it proved difficult to maintain up to date skills in managing syringe drivers when staff only occasionally encountered someone who had one (Avis
! 7
Training programme
Factors
Personnel Factors
(Trainees)
• Unapproachable trainers • Course content inappropriate for trainees’ needs • Lack of financial incentive • Difficult relationships between academic and
service staff • Conflicting value systems of trainees, academics
and home managers • Lack of clarity about training and the trainer’s
role • Unexpected cancellations on training sessions
• Negativity • Feelings of vulnerability • Trainers perceived as regulators • Resistance to change • Conflicting priorities between workload and
training • Low staff morale • Feelings of inadequacy • Staff feeling less valued than NHS counterparts • Specialist input perceived as a threat • Staff shortages

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
et al., 1999; Hatcher and Chamberlain, 2000). There were of course other practicalities that made delivering effective training difficult; the main issues here being time and staffing. Very often management stated that they just did not have the time to fulfil their obligations to the training. There were incidents of paperwork not being completed so preventing the implementation of new training programmes with other demands on time (inspections, audits) taking priority (Hatcher and Chamberlain, 2000; Waldron et al., 2008). Staff shortages meant that sometimes there were difficulties in dedicating a core group of staff to training as there was no one to cover for them on their shift – a problem that could be compounded by those trainees with new skills being taken away from providing basic care and leaving colleagues with an increased workload (Heals, 2008; Nelson et al, 2009; Lansdell and Mahoney, 2011a). Staff shortages also accounted for unexpected and sudden cancellations which resulted in a training sessions having to be abandoned (Hatcher and Chamberlain, 2000). Lack of adequate numbers of registered nursing staff resulted in junior colleagues being inadequately supervised and poor practice being easily passed on (Avis et al., 1999). Also, the nursing and care home workforce was constantly changing and so investment in new skills by institutions was sometimes seen as false economy when those skills were lost as individual staff members moved on to other workplaces (Avis et al., 1999; Law, 2003; Hays et al., 2012). Barriers Training programme factors Factors involving the programme itself produced obstacles to progress. An initial lack of clarity about the purpose of and reasons for the training along with a programme content that was considered inappropriate for the trainees’ needs resulted in a less than satisfactory experience for both trainee and trainer (Raunkiaer and Timm, 2010; Butler, 2012). Sometimes the lack of a financial incentive produced a negative effect on trainees’ motivation (Wild et al., 2010). Unapproachable trainers who were inflexible and unable to respond to trainees’ needs often made the situation worse by increasing any misgivings and doubts they had rather than allaying them (Davies et al., 2004). It should be acknowledged that the training programmes were being delivered in varied institutions by people from different workplace backgrounds and therefore there was the potential for occasional conflicts of interest where competing value systems came into play. This could lead to difficult relationships between trainees, academics and home managers (Butler, 2012). Barriers Personnel factors (trainees) Some trainees found that not only the conflict between value systems but also the conflicting priorities of work and training caused them to have difficulties. When they already considered themselves to be overworked they felt that they had little time to spare for training (Waldron et al., 2008). This combined with low staffing levels, low staff morale and a sense of being less valued than their health service counterparts produced obstacles to learning (Butler, 2012; Hays et al., 2012). Some staff were resistant to change and showed
! 8

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
reluctance to alter their practice, in some cases perceiving their trainers as regulators and specialist input as a threat (Anderson, 2004; Davies et al., 2004; Heals, 2008; Nelson et al, 2009; Hays et al., 2012).
Review of Enablers to training There were also factors that were perceived as facilitating the implementation and development of training. As in the previous section these fell into three main groupings; those connected with the nursing and care home management style and ethos, those that evolved from the course itself and those connected with the trainers (rather than the trainees) (Figure 4 overleaf)
Enablers: Nursing /care home factors
A key enabling factor was a home manager or owner who was keen and willing to support and progress the training agenda (Anderson, 2004). Effective, strong leadership and the ability to recognise what was working and what needed improving in terms of the workforce often resulted in openness to new ways of working and thinking (Wild et al., 2010; Lansdell and Mahoney, 2011a & b). Also if there was evidence of a learning culture within the home, trainers found that potential trainees were enthusiastic and committed to developing their skills (Davies et al., 2004; Wild et al., 2010; Lansdell and Mahoney, 2011a). It was often the case that these staff were well prepared to undertake training and were funded by their management (Wild et al., 2010). If the home had an integrated health and social care approach to its work then training appeared to be easier to implement and if staff were included at the planning stage it was found to produce well attended sessions (Heeley-Creed et al.,2007; Nelson et al, 2009; Wild et al., 2010). If this approach was extended to include the views and opinions of residents and relatives with the quality of their experiences being paramount it also had a positive influence (Davies et al., 2004; Wild et al., 2010). If homes had access to health service nursing staff as a teaching and learning support then staff development was obviously more easily achieved. These homes looked to health service nurses (often community nurses) to pass on their skills to their staff, sometimes through formal training sessions but often informally when a need was identified (Wild et al., 2010). Much depended on the personal interest of nursing and care staff and their willingness to acknowledge when they needed nurse led support (Heals, 2008; Wild et al., 2010). Senior staff who enthused about the benefits of training programmes and who ensured that there were adequate staffing levels to allow for training time were pivotal in the effective implementation of training programmes (Davies et al., 2004; Wild et al., 2010).
! 9

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Figure 4 Enablers to Training
Enablers: Training programme factors The practicalities of running training programmes had a major role to play in whether or not they were deemed to be successful. Groups had to be of a suitable size in order to give everyone the opportunity to contribute and to practise their skills. The skills training had to be relevant to each nursing and care home and was found to be more readily engaged with if it was built around real life case studies (Heeley-Creed et al.,2007; Raunkiaer and Timm, 2010; Hausken and Graue, 2013). Trainees also found training easy to engage with if it made provision for their personal needs. For example, people who were used to working in a practical environment were found to have difficulty in sitting attentively for long periods of time, their engagement and
! 10
FACILITATORS
Training programme
Factors
Personnel Factors
(Trainers)
Nursing /Care home
Factors
• Home owners and managers supportive of training
• Enthusiastic and committed staff • Recognising what works well and what needs
improving • Acknowledging the need for nurse led support • Strong leadership from management • Integrated health and social care approach • Adequate staffing levels • A developing learning culture • Teaching and learning support from NHS staff • Emphasis on the experiences of residents and
their relatives • Enthusiasm of relatives for new initiatives • Personal interest of staff in specialist subjects • Well prepared staff • Adequate training budget • Staff involvement at planning stage
• Financial incentives • Clinical skills award • Training tailored to each nursing/care home • Training built around the skill sets and
learning styles of trainees • Training groups of an optimum size • Course content based on real life studies • Provision made for trainees personal needs
and circumstances • Provision of refreshments
• Appropriate skills and approachability • Quick response to requests for help • Good access to resources • Efficient systems of recording and
disseminating information • Trainer who helps to cascade information to
all grades of staff • Promotion of collaborative learning to
strengthen communication among staff • Personal authority in order to communicate
effectively with managers and co-professionals
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
concentration being held more effectively by being presented with a limited number of short theoretical sessions and having frequent breaks (Raunkiaer and Timm, 2010). Training was also more successful when provision was made in the training schedule for trainees who worked late shifts and for those who had child care needs (Hausken and Graue, 2013). The offering of refreshments was viewed as a plus factor (Heeley-Creed et al.,2007). Trainees also liked having something to show for undertaking training. For some this was a clinical skills award whilst others were rewarded financially (Morgan and Conrad, 2008; Wild et al., 2010). Enablers: Personnel factors (trainees) The trainer was of paramount importance to the effective delivery of the training programme. If they had good access to resources and established efficient systems for recording and disseminating information the training was seen as being effective and sustainable (Davies et al., 2004). The personal qualities of the trainer were also important. A trainer who was appropriately skilled, whom the trainees were able to talk freely with, could relate to as a colleague and who could respond quickly to requests for help was particularly helpful to the outcomes of the programme (Davies et al., 2004). Conversely it was important that the trainer maintained a sense of personal authority in dealing with staff at strategic and management levels as this enabled more effective communication (Hays et al., 2012). Collaborative learning opportunities actually strengthened the communication networks between home staff and training providers which were vital in promoting the cascading of information about practice development to all grades of staff (Davies et al., 2004; Lekan et al., 2010).
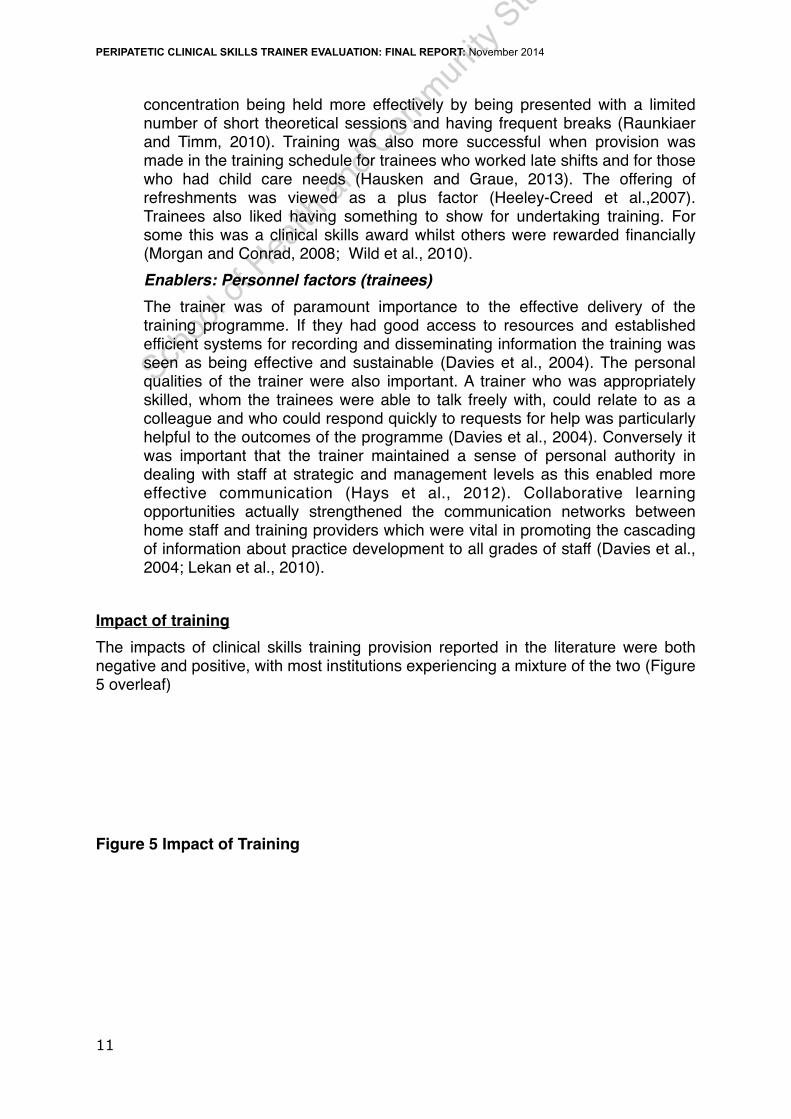
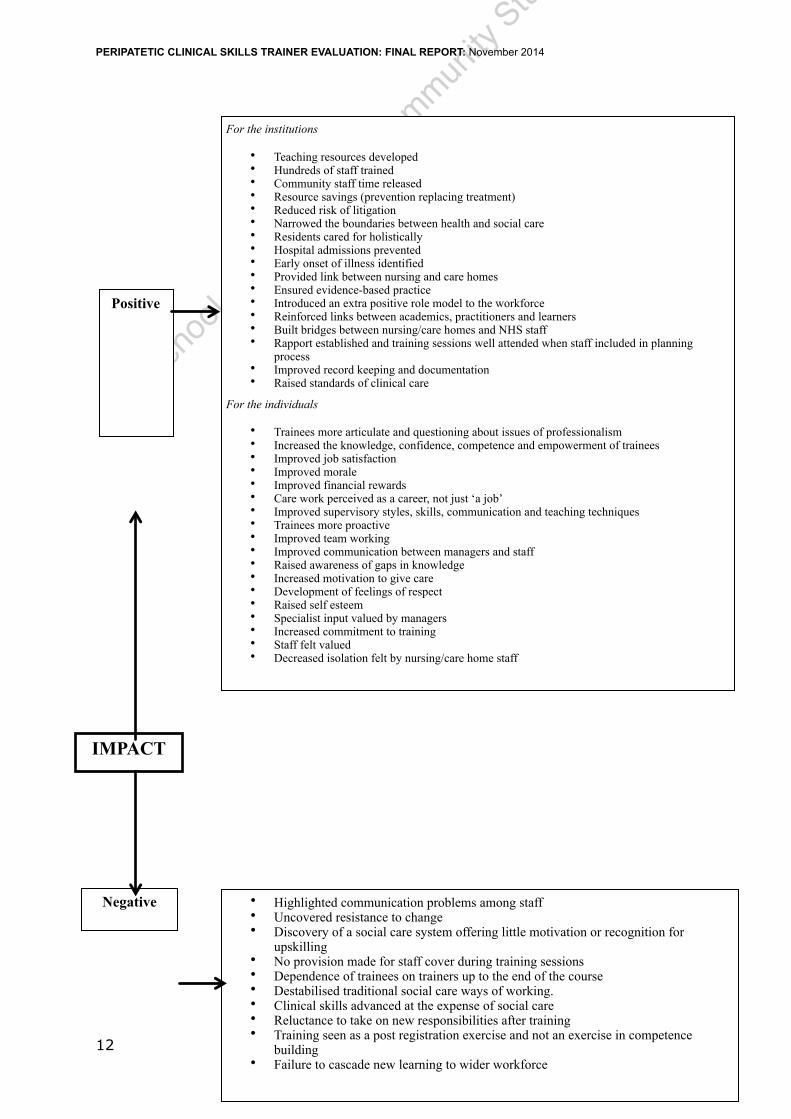
Impact of training The impacts of clinical skills training provision reported in the literature were both negative and positive, with most institutions experiencing a mixture of the two (Figure 5 overleaf) Figure 5 Impact of Training
! 11
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
! 12
IMPACT
Negative
Positive
For the institutions
• Teaching resources developed • Hundreds of staff trained • Community staff time released • Resource savings (prevention replacing treatment) • Reduced risk of litigation • Narrowed the boundaries between health and social care • Residents cared for holistically • Hospital admissions prevented • Early onset of illness identified • Provided link between nursing and care homes • Ensured evidence-based practice • Introduced an extra positive role model to the workforce • Reinforced links between academics, practitioners and learners • Built bridges between nursing/care homes and NHS staff • Rapport established and training sessions well attended when staff included in planning
process • Improved record keeping and documentation • Raised standards of clinical care
For the individuals
• Trainees more articulate and questioning about issues of professionalism • Increased the knowledge, confidence, competence and empowerment of trainees • Improved job satisfaction • Improved morale • Improved financial rewards • Care work perceived as a career, not just ‘a job’ • Improved supervisory styles, skills, communication and teaching techniques • Trainees more proactive • Improved team working • Improved communication between managers and staff • Raised awareness of gaps in knowledge • Increased motivation to give care • Development of feelings of respect • Raised self esteem • Specialist input valued by managers • Increased commitment to training • Staff felt valued • Decreased isolation felt by nursing/care home staff
• Highlighted communication problems among staff • Uncovered resistance to change • Discovery of a social care system offering little motivation or recognition for
upskilling • No provision made for staff cover during training sessions • Dependence of trainees on trainers up to the end of the course • Destabilised traditional social care ways of working. • Clinical skills advanced at the expense of social care • Reluctance to take on new responsibilities after training • Training seen as a post registration exercise and not an exercise in competence
building • Failure to cascade new learning to wider workforce
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
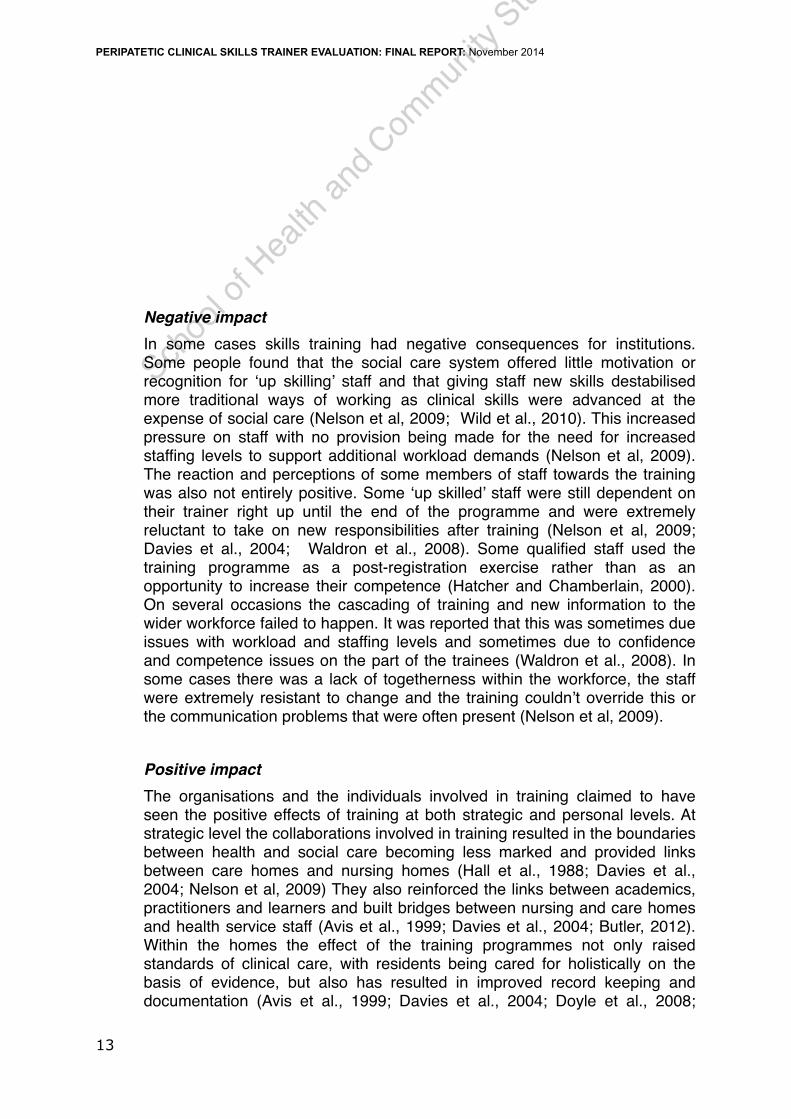
Negative impact In some cases skills training had negative consequences for institutions. Some people found that the social care system offered little motivation or recognition for ‘up skilling’ staff and that giving staff new skills destabilised more traditional ways of working as clinical skills were advanced at the expense of social care (Nelson et al, 2009; Wild et al., 2010). This increased pressure on staff with no provision being made for the need for increased staffing levels to support additional workload demands (Nelson et al, 2009). The reaction and perceptions of some members of staff towards the training was also not entirely positive. Some ‘up skilled’ staff were still dependent on their trainer right up until the end of the programme and were extremely reluctant to take on new responsibilities after training (Nelson et al, 2009; Davies et al., 2004; Waldron et al., 2008). Some qualified staff used the training programme as a post-registration exercise rather than as an opportunity to increase their competence (Hatcher and Chamberlain, 2000). On several occasions the cascading of training and new information to the wider workforce failed to happen. It was reported that this was sometimes due issues with workload and staffing levels and sometimes due to confidence and competence issues on the part of the trainees (Waldron et al., 2008). In some cases there was a lack of togetherness within the workforce, the staff were extremely resistant to change and the training couldn’t override this or the communication problems that were often present (Nelson et al, 2009). Positive impact The organisations and the individuals involved in training claimed to have seen the positive effects of training at both strategic and personal levels. At strategic level the collaborations involved in training resulted in the boundaries between health and social care becoming less marked and provided links between care homes and nursing homes (Hall et al., 1988; Davies et al., 2004; Nelson et al, 2009) They also reinforced the links between academics, practitioners and learners and built bridges between nursing and care homes and health service staff (Avis et al., 1999; Davies et al., 2004; Butler, 2012). Within the homes the effect of the training programmes not only raised standards of clinical care, with residents being cared for holistically on the basis of evidence, but also has resulted in improved record keeping and documentation (Avis et al., 1999; Davies et al., 2004; Doyle et al., 2008;
! 13
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
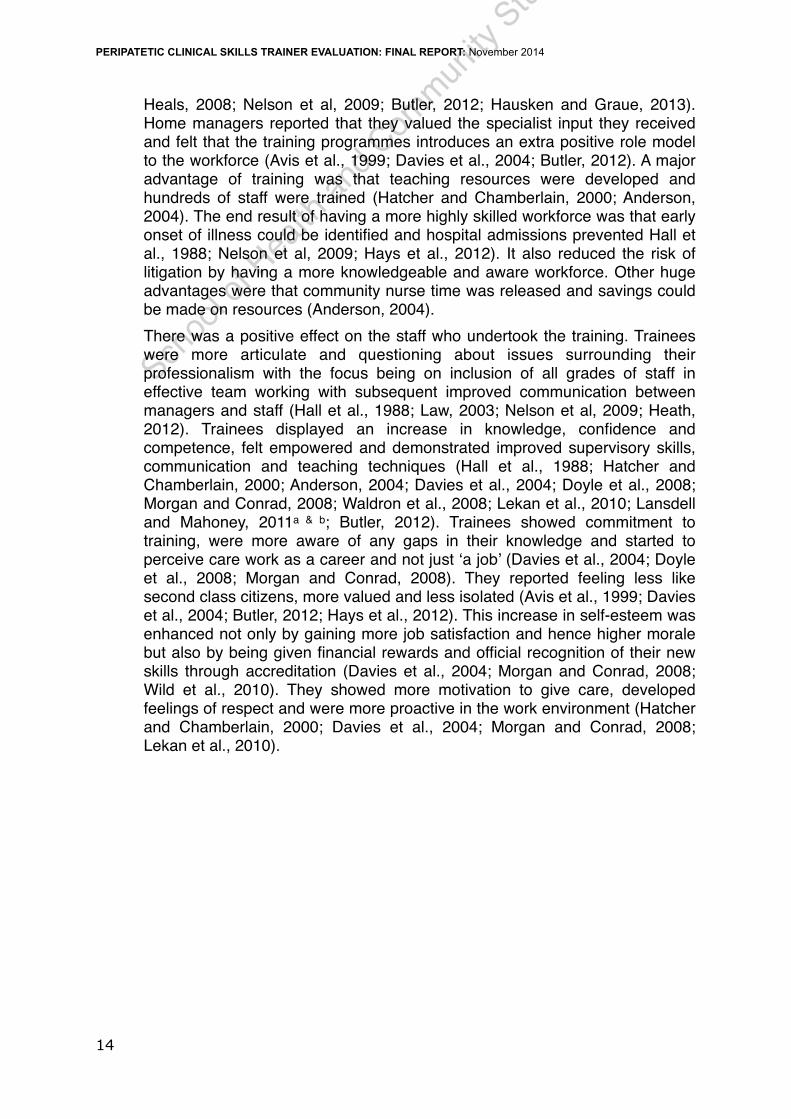
Heals, 2008; Nelson et al, 2009; Butler, 2012; Hausken and Graue, 2013). Home managers reported that they valued the specialist input they received and felt that the training programmes introduces an extra positive role model to the workforce (Avis et al., 1999; Davies et al., 2004; Butler, 2012). A major advantage of training was that teaching resources were developed and hundreds of staff were trained (Hatcher and Chamberlain, 2000; Anderson, 2004). The end result of having a more highly skilled workforce was that early onset of illness could be identified and hospital admissions prevented Hall et al., 1988; Nelson et al, 2009; Hays et al., 2012). It also reduced the risk of litigation by having a more knowledgeable and aware workforce. Other huge advantages were that community nurse time was released and savings could be made on resources (Anderson, 2004). There was a positive effect on the staff who undertook the training. Trainees were more articulate and questioning about issues surrounding their professionalism with the focus being on inclusion of all grades of staff in effective team working with subsequent improved communication between managers and staff (Hall et al., 1988; Law, 2003; Nelson et al, 2009; Heath, 2012). Trainees displayed an increase in knowledge, confidence and competence, felt empowered and demonstrated improved supervisory skills, communication and teaching techniques (Hall et al., 1988; Hatcher and Chamberlain, 2000; Anderson, 2004; Davies et al., 2004; Doyle et al., 2008; Morgan and Conrad, 2008; Waldron et al., 2008; Lekan et al., 2010; Lansdell and Mahoney, 2011a & b; Butler, 2012). Trainees showed commitment to training, were more aware of any gaps in their knowledge and started to perceive care work as a career and not just ‘a job’ (Davies et al., 2004; Doyle et al., 2008; Morgan and Conrad, 2008). They reported feeling less like second class citizens, more valued and less isolated (Avis et al., 1999; Davies et al., 2004; Butler, 2012; Hays et al., 2012). This increase in self-esteem was enhanced not only by gaining more job satisfaction and hence higher morale but also by being given financial rewards and official recognition of their new skills through accreditation (Davies et al., 2004; Morgan and Conrad, 2008; Wild et al., 2010). They showed more motivation to give care, developed feelings of respect and were more proactive in the work environment (Hatcher and Chamberlain, 2000; Davies et al., 2004; Morgan and Conrad, 2008; Lekan et al., 2010).
! 14
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
SECTION 2. Develop initial theories of the model of CST post & identify possible impact data Three models of delivery were developed by mapping the 24 studies in terms of the primary focus (see Table 1 overleaf).
1. Focussed on staff skills development (e.g. up skilling care assistants)
2. Focussed on a single Health condition (not resident need focussed) e.g. to improve diabetes care)
3. Safety of home/prevention of harm (e.g. initiative to prevent falls)
Two studies matched with the Leeds CST model in terms of involving a university and clinical skills training in the workplace, however 1 study was UK undergraduate nurse training placements not workforce development and the other study focussed on a single condition in USA. The Leeds CST model was not mirrored in the literature identified as it is a hybrid of staff clinical skills development + safety/prevention of harm + whole resident perspective using a connected learning model of partnership between university and clinical practice. Therefore all 24 studies informed the template for evaluation of the enablers, barriers and possible impacts. The data from figures 2-5 were fed into an interview study to explore the impact of the CST post (see Section 3).
! 15

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
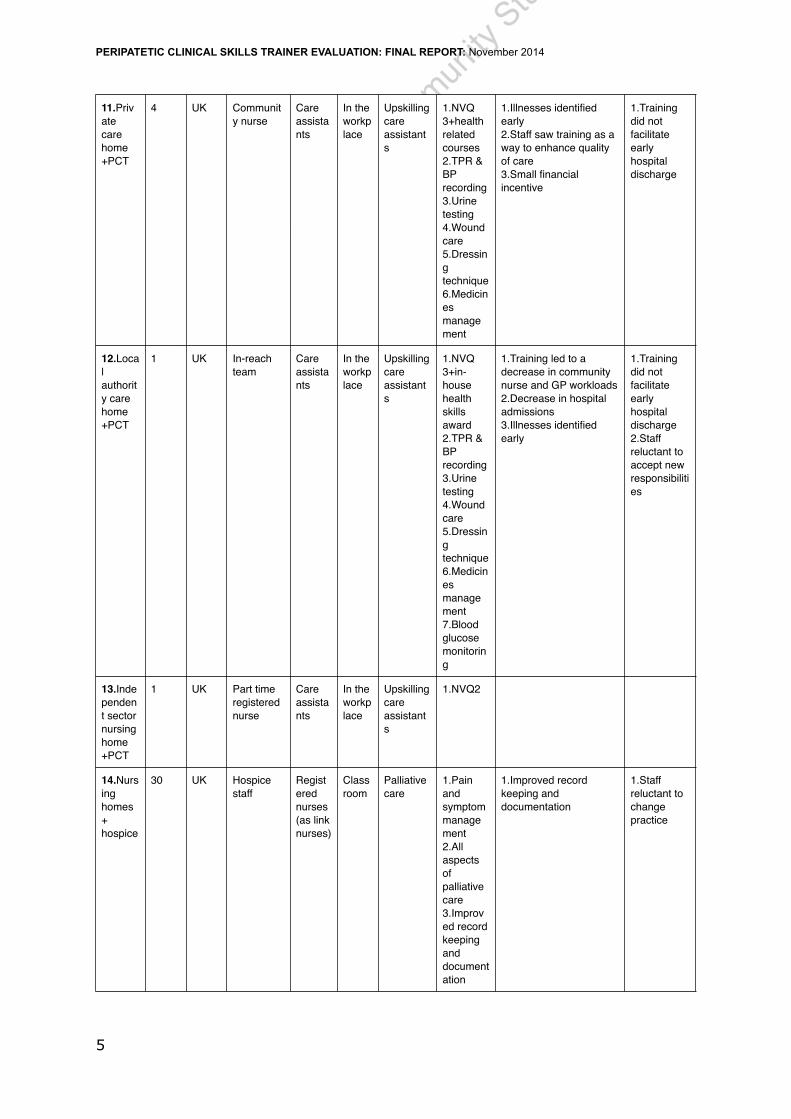
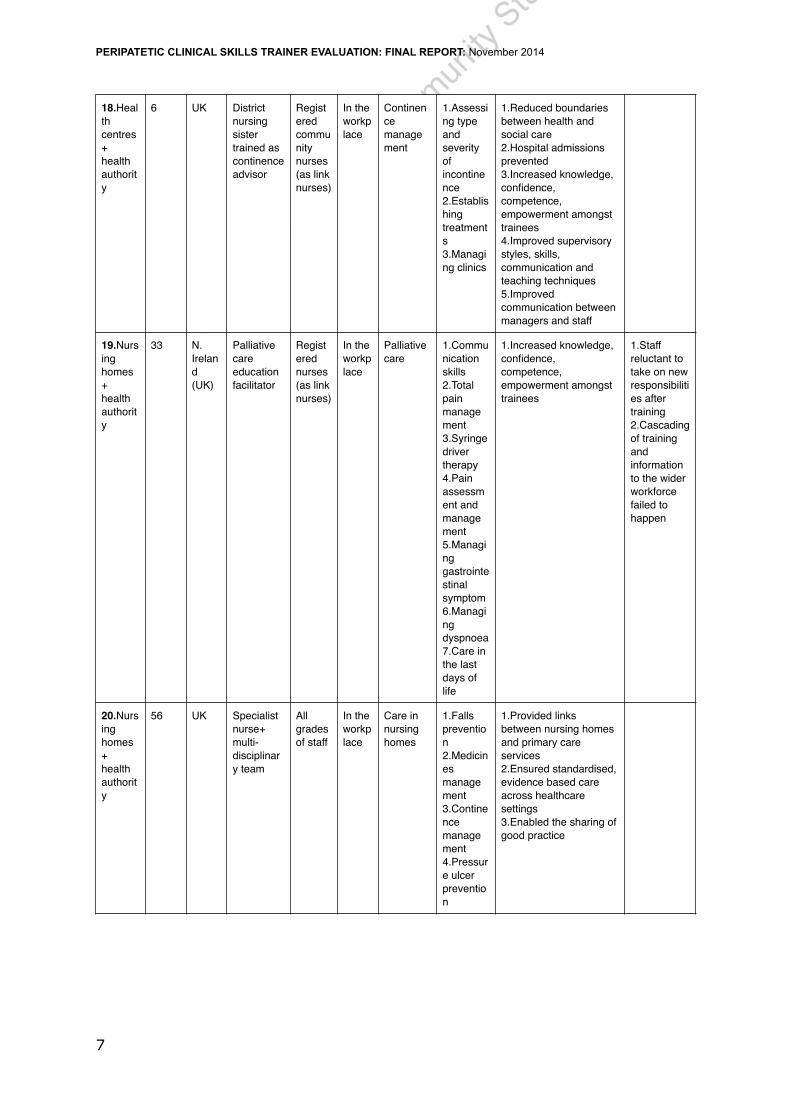
Table 1 A chart of 24 included studies in the review of evidence
Which organisations are involved?
How many sites are there?
In which country does the training happen?
Who delivers the training
Who is trained
Where is the setting?
What is the subject of the training?
What skills are developed?
Outcomes (O) Positive Impact
Outcomes (O) Negative Impact
1.DoH+university+nursing homes+adult care homes+home care+health agencies
8 US University teachers
Nursing assistants
Classroom and in the workplace
Workforce development
1.Management skills2.Communication skills
1.Increased knowledge, confidence, competence,empowerment amongst trainees2.Improved job satisfaction 3.Improved financial rewards4.Care work perceived as a career not a job 5.Improved supervisory styles, skills, communication and teaching techniques6.Trainees more proactive 7.Improved quality of care 8.Trainees relationships with residents improved 9.Improved clinical skills
2.Nursing home+university
1 US Advanced practice nurse
Registered nurses, nursing assistants, licensed practical nurses
Classroom, clinical unit and in the workplace
Managing heart failure Connected Learning Model
1.Heart failure clinical practice guidelines
1.Increased knowledge, confidence, competence,empowerment amongst trainees2.Improved supervisory styles, skills, communication and teaching techniques3.Trainees more motivated to give care 4.Staff more attentive to symptoms5.Improved record keeping and documentation 6. Improved quality in interactions between nurses and medical staff
3.Skilled nursing facilities+university
4 US Multi-disciplinary team
Registered nurses, licensed practical nurses, nursing assistants
Classroom and in the workplace
Managing urinary incontinence
1.Learning to use a bladder ultrasound scanner2.Continence management
1.Positive change in attitudes towards continence management
1.Decreased staff confidence when unsupported by skilled personnel
! 1

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
4.Nursing homes+university+ local authority
23 Denmark
University teachers
Assistant nurses, nursing aides, home helpers, social workers
Classroom
Palliative care Competency Development
1.Clinical knowledge about death 2.Communication skills3.Understanding law and ethics4.Managing routines and rituals5.Understanding attitudes towards life and death
1.Improved staff competencies in palliative care 2.Organisational initiatives improved palliative care 3.Shared knowledge of residents and relatives wishes4.Improved interdisciplinary co-operation 5.Trainees had increased professional expectations of themselves and each other6.Increased broadmindedness toward residents and colleagues
5.Nursing homes+home based services+university+local authority
5 zones with a base
Norway
Multi-disciplinary team (nurse led)
Registered nurses, nursing aides
Classroom
Diabetes care
1.Blood glucose monitoring 2.Insulin treatment3.Managing diabetic foot ulcers4.Diabetic nutrition 5.Diabetes and dementia care 6.Psychological care 7.Treatment protocols8.Annual reviews
1.Evidence based practice ensured 2.Increased knowledge, confidence, competence,empowerment amongst trainees
6.Hospitals for the elderly+Centre for Nurse Education (hospital based)
7 Irish Republic
Nurse educators
Registered nurses (2 per site to train as in-service trainers)
Classroom
Clinical skills
1.Venepuncture 2.Subcutaneous fluid replacement therapy3.Cannulation 4.CPR,5.Wound management6.Gastrostomy tube replacement
1.Raised standards of clinical care 2.Increased knowledge, confidence, competence,empowerment amongst trainees3.Improved supervisory styles, styles, skill, communication and teaching techniques4.Staff committed to training
! 2

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
7.Care homes+health authority
33 Australia
Nurse practitioner+multi-disciplinary team
All grades of staff
In the workplace
Dementia care
1.Managing difficult behaviours
8.Care homes+PCT
25 UK Specialist nurse
All grades of staff
In the workplace
Reducing the prevalence of hip fractures
1.Use of hip protectors
1.Link provided between care and nursing homes2.Evidence based practice ensured 3.Bridges built between nursing/care homes and NHS staff4.Increased knowledge, confidence, competence,empowerment amongst trainees5.Increased job satisfaction 6.Improved morale 7.Trainees more aware of gaps in knowledge 8.Trainees more motivated to give care 9.Trainees develop feelings of respect10.Staff feel less like second class citizens 11.Specialist input valued by home managers12.Staff felt valued
1.Staff reluctant to take on new responsibilities after training
! 3

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
9.Care homes+ local health & social care partnership
3 UK In-reach team (11 community nurses+1 physiotherapist)
Care assistants
In the workplace
Upskilling care assistants
1.NVQ 3+2.TPR & BP recording 3.Blood glucose monitoring 4.Urine testing 5.Skin care 6.Simple dressings
1.Reduced boundaries between health and social care 2.Residents treated holistically3.Hospital admissions prevented 4.Illnesses identified early5.Raised standards of clinical care 6.Trainees more articulate and questioning about issues surrounding their professionalism
1.Staff lacked togetherness and experienced communication problems2.Highlighted staff resistance to change 3.Social care system offered little recognition or motivation for upskilling 4.No provision for increased staffing needs to support additional workload demands5.Upskilled staff dependent on trainers until end of course 6.Destabilised traditional social care ways of working resulting in increased pressure
10.Voluntary sector care home+PCT
1 UK Community nurse+ Home’s own nurse trainer
Care assistants
In the workplace
Upskilling care assistants
1.NVQ 3+in-house health skills award 2.TPR & BP recording 3.Urine testing 4.Wound care 5.Dressing technique 6.Medicines management7.Catheter care
1.Decrease in hospital admissions2.Illnesses identified early3.Small pay increment
1.Training did not facilitate early hospital discharge 2.Staff reluctant to accept new responsibilities
! 4
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
11.Private care home+PCT
4 UK Community nurse
Care assistants
In the workplace
Upskilling care assistants
1.NVQ 3+health related courses2.TPR & BP recording 3.Urine testing 4.Wound care 5.Dressing technique 6.Medicines management
1.Illnesses identified early2.Staff saw training as a way to enhance quality of care 3.Small financial incentive
1.Training did not facilitate early hospital discharge
12.Local authority care home+PCT
1 UK In-reach team
Care assistants
In the workplace
Upskilling care assistants
1.NVQ 3+in-house health skills award 2.TPR & BP recording 3.Urine testing 4.Wound care 5.Dressing technique 6.Medicines management7.Blood glucose monitoring
1.Training led to a decrease in community nurse and GP workloads2.Decrease in hospital admissions3.Illnesses identified early
1.Training did not facilitate early hospital discharge 2.Staff reluctant to accept new responsibilities
13.Independent sector nursing home+PCT
1 UK Part time registered nurse
Care assistants
In the workplace
Upskilling care assistants
1.NVQ2
14.Nursing homes+hospice
30 UK Hospice staff
Registered nurses (as link nurses)
Classroom
Palliative care
1.Pain and symptom management2.All aspects of palliative care 3.Improved record keeping and documentation
1.Improved record keeping and documentation
1.Staff reluctant to change practice
! 5

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
15 Care homes+health and social services
51 UK Specialist support teams (including clinical nurse specialists)
Registered nurses
Classroom and in the workplace
Nursing care of older people
1.Vaccination2.Documentation, 3.Venepuncture 4.Adult protection 5.Oxygen therapy6.Syringe driver therapy7.Subcutaneous fluid administration 8.Diabetes care 9.Gastrostomy care 10.Falls and fractures strategy11.Pressure ulcer care 12.Clinical supervision
1.Teaching resources developed 2.Hundreds of staff trained 3.Community nurse time released 4.Prevention replacing treatment resulted in resource savings5.Reduced risk of litigation 6.Increased knowledge, confidence, competence,empowerment amongst trainees
16.Care homes+hospice
3 UK Hospice staff
All grades of staff
Classroom
End of life care Competency Development
1.Pain and symptom management2.All aspects of palliative care
1.Increased knowledge, confidence, competence,empowerment amongst trainees2.Reduction in hospital admissions
17.Care homes+university+hospital trusts
4 care homes/6 hospital trusts
UK University teacher
Student nurses
In the workplace
Nurse training
1.Developing students’ knowledge and clinical skills2.Assisting mentors to develop their roles
1.Evidence based practice ensured 2.Introduced an additional positive role model to the workforce 3.Strengthened links between academics, practitioners and learners4.Improved record keeping and documentation 5.Increased knowledge, confidence, competence,empowerment amongst trainees
! 6
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
18.Health centres+health authority
6 UK District nursing sister trained as continence advisor
Registered community nurses (as link nurses)
In the workplace
Continence management
1.Assessing type and severity of incontinence 2.Establishing treatments3.Managing clinics
1.Reduced boundaries between health and social care 2.Hospital admissions prevented 3.Increased knowledge, confidence, competence,empowerment amongst trainees4.Improved supervisory styles, skills, communication and teaching techniques5.Improved communication between managers and staff
19.Nursing homes+health authority
33 N. Ireland (UK)
Palliative care education facilitator
Registered nurses (as link nurses)
In the workplace
Palliative care
1.Communication skills2.Total pain management3.Syringe driver therapy4.Pain assessment and management5.Managing gastrointestinal symptom6.Managing dyspnoea 7.Care in the last days of life
1.Increased knowledge, confidence, competence,empowerment amongst trainees
1.Staff reluctant to take on new responsibilities after training 2.Cascading of training and information to the wider workforce failed to happen
20.Nursing homes+health authority
56 UK Specialist nurse+multi-disciplinary team
All grades of staff
In the workplace
Care in nursing homes
1.Falls prevention 2.Medicines management3.Continence management4.Pressure ulcer prevention
1.Provided links between nursing homes and primary care services2.Ensured standardised, evidence based care across healthcare settings3.Enabled the sharing of good practice
! 7

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
21.Nursing homes+health authority
43 UK Nurse advisor + peer support group of 6 district nurses
All grades of staff
Classroom
Palliative care
1.Accessing specialists2.Improving communication 3.Bereavement counselling 4.Crisis management5.Principles of palliative care 6.Pain and symptom control 7.Syringe driver therapy8.Aromatherapy
1.Residents treated holistically2.Bridges built between nursing/care homes and NHS staff3.Staff felt less like second class citizens4.Specialist input valued by home managers5.Nursing/care home staff felt less isolated 6.Improved standards of care 7. Improved staff confidence 8.Improved knowledge and skills9.Crisis prevention 10.Improved communication between services11.Improved support for staff, patients and relatives
! 8

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
22.Nursing.homes+health authority+social services
75 UK Community nurses seconded as trainers+specialist nurses
Registered nurses
In the workplace
Clinical skills
1.Male/female/suprapubic catheterisation 2.Assessment and record keeping 3.Enteral feeding and care of gastrostomy tubes4.Ear irrigation 5.Subcutaneous and intravenous fluid administration 6.Tracheotomy care 7.Care of central venous pressure lines8.Venepuncture 9.Parkinson’s disease management (training by specialist nurse [sn])10.Tissue viability (training by sn)11.Continence management (training by sn)12.Care of the terminally ill inc. syringe driver management (training by sn)
1.Hundreds of staff trained 2.Increased knowledge, confidence, competence,empowerment amongst trainees3.Trainees more motivated to give care
1.Qualified staff regarded training as a post-registration exercise not an opportunity to increase competence
! 9

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
23.Nursing homes+NHS trusts health consortium homes
Several
UK Specialist nurse
Qualified nurses (as link nurses)
Classroom
Pressure ulcer prevention
1.Wound care 2.Dressing technique
1.Trainees more articulate and questioning about issues surrounding their professionalism2.Improved quality of care 3.Increased knowledge, confidence, competence,empowerment amongst trainees4.Trainees more motivated to give care 5. Practice standardised across healthcare settings
24.Nursing & care homes private funding
122 UK Nurse educator+dietician
All grades of staff (to establish a link nurse in each home)
Classroom and in the workplace
Diabetes care
1.Cooks’ workshops2.Blood glucose monitoring 3.A specific session for care home managers4.Develop protocols of care
1.Staff involvement in planning resulted in well attended sessions2.Improved quality of care
! 10

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
! 11

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Section 3. An interview study to explore the impact of the CST post The CST post offered free at point of access training to nursing homes and community services staff across two pilot areas of Scarborough Whitby and Ryedale and Harrogate. This part of the evaluation was an interview study to explore views and gather narratives about the impact of the service provided by the CST post. Ethical approval was granted by Leeds Beckett University Local Research Ethics Committee.
Sampling and sample We used a purposive sampling strategy which refers to inviting individuals who are likely to generate appropriate and meaningful data. Potential participants’ were identified by the clinical advisory group. This group indicated their willingness to be contacted and consider contributing to the project. Members of the clinical advisory group contacted via email all those in their sampling frame with details of the project (see appendix participant information leaflet; if willing, the contact details (name and telephone number) were sent to the research assistant (FD) who arranged a time and date for an interview based on participants’ preference. We hoped to be able to interview 20% of this sampling frame therefore the target recruitment was n=15.
Data collection Participants were sent an information sheet and consent form, and offered an opportunity to discuss any questions or concerns before agreeing to participate. Semi structured interviews were carried out either at participants’ place of work or at the university. A topic guide based on the findings from stage 2 was used to prompt discussion. Each interview was recorded and data from both audio recorders was transferred to a password protected university server. All interviews were transcribed and for the purpose of transcribing, the audio files were uploaded on a secure online server. All personal identifiable data including any names, date of births, addresses and places of work were removed from the transcripts to ensure confidentiality. Data Analysis The interviews were analysed using QSR NVivo software. A framework approached was employed to order and manage the data through the process of the analysis. This is a matrix based analytic method which was developed by Ritchie et al., 2003. Framework embodies aspects of content and thematic analysis and involves summarising and classifying data within a thematic framework. The findings from stage 1 & 2 were used to develop the thematic framework and coding frame to index and chart the data. The analysis charts (see appendix) were then used to map the data and explore associations in order to arrive at explanatory accounts of impact and search for impact case studies. As an approach to research design, it is attractive to many health researchers and clinicians because of its ability to generate policy and practice orientated evidence (Green and Thorogood, 2009). FD reviewed the content of each of the transcripts, categorised the range of responses and this was independently reviewed by MB. The initial findings were then presented to key stakeholders for further refinement and development.
! 12
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Results A total of 749 staff were trained in 1 year which is an estimated 97% uptake from care homes in the designated project area. Individuals presenting 10 care homes were recruited for face to face interviews. These care homes represented 245/749 staff trained (33%). Nine of the care homes had nursing beds and 1 care home had residential beds only. The occupancy ranged from 23 to 85 residents. Two of the homes were owned by voluntary/non-profit making organisations, six of the homes were owned by private companies and two of the homes were owned by individuals. Sixteen interviews were carried out with the following groups.
• Care home managers • Care home deputy managers • Training leads • Proprietor • Registered nurses • Care assistant • Senior team leader (carer) • Trainees • Team leader – Integrated Community Care Team • Team leader – NHS Trust Clinical Development Team • Community Matron – Nursing home support • Clinical Specialist Nurse for Care Homes
! 13

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Clinical Nursing skills training needs highlighted in literature review
Training delivered Impact case study
MAINTAINING INTEGRITY OF VITAL BODY SYSTEMS Venepuncture Cannulation Cardiopulmonary resuscitation Replacing gastrostomy tubes Tracheotomy care Managing central venous pressure lines
Venepuncture; RN 89 RMN 23 HCA 8 Fine bore nasogastric tubes RN 16 Tracheostomy care RN 3 HCA 4 Total 144
Yes Case study 3, 4, 7, 10
CONTINENCE MANAGEMENT Proficiency in bladder ultrasound scanning Male/female and suprapubic catheterisation
Catheterisation male-female it suprapubic 145 registered nurses 1 HCA Fundamentals of catheter care what RN. 145 HCA Total 274
Yes Case study 5,6, 9
WOUND MANAGEMENT Managing diabetic foot ulcers Dressing wounds Pressure ulcer prevention
Pressure ulcer prevention RN 27 179 HCA Total 206
Yes Case study 1&2
ADMINISTRATION OF PRESCRIBED MEDICINE/THERAPY Administering of insulin Administering subcutaneous fluid replacement therapy Administering vaccinations Administering oxygen Administering intravenous fluids Managing syringe drivers
Imms and vacs training Yes Case study 8
MONITORING AND RECORDING CLINICAL OBSERVATIONS Recording and monitoring blood pressure and temperature, pulse and respiration readings Blood glucose monitoring Urine testing
Basic observation RN 1 HCA 124 Total 125
Yes Case study 11
! 14

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Table 2 Clinical training delivered mapped to impact case studies
Table 3-10 map the evidence gathered from the qualitative interviews on to the barriers, enablers and positive & negative impacts (see appendix for data charts).
Table 3 shows care home potential enabling factors identified from the literature mapped to evidence obtained from the interviews. We were able to identify evidence to map to all the enabling factors from the literature review. Most of the homes gave learning a high priority. For example, some care homes paid their staff to attend training on their days off. Other homes covered for staff to attend training whilst they were on duty. Some homes allowed their staff a certain number of paid training hours and paid for extra staff to cover for them whilst they trained. Some homes enabled their staff to access lots of training – in-house, distance, e-learning whereas some homes found it cheaper to use a ‘Train the Trainer’ model and just send one member on a course who can then come back and train others.
A small minority of the homes had a generous training budget and could easily fund training that is additional to mandatory courses. The majority of homes had designated staff training rooms and some homes booked training well in advance and plan their off duties around it. There were examples of a strong emphasis on staff development e.g. One manager used 3 monthly appraisals to ask staff about their training needs, another spoke of investing heavily in training, looking on it in terms of career progression and another manager was keen to promote training in order to protect staff’s professional registration, adhere to their code of conduct and meet with CQC regulations. Many commented on the development of a learning
MAINTAINING INDEPENDENCE THROUGH MOBILITY AND COMMUNICATION Preventing falls Using hip protectors Ear irrigation
No training requested/delivered No
! 15
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
culture as a result of undertaking training and some homes clearly had an ethos of caring as a career rather than a job which was supported by the training provision. Another aspect to consider was that some homes provided training experience to student and overseas nurses. Finally whilst there was evidence of an aspiration to include residents and families in training decisions it was recognised there was more to do this area with Residents families being largely unaware of staff training.
Table 4 shows care home potential barriers identified from the literature mapped to evidence obtained from the interviews. We were not able to map evidence from the interview for the following barriers identified in the literature review.
• Up skilled staff taken away from basic duties
• Inadequate staff preparation
• Learning not shared with others
• Lack of potential trainees
• Low management self esteem
• Low management morale
There were, however, reports of staff shortages and lack of time was an issue in some cases. For some managers their requests for training had to be authorised by their head offices and they were often refused finance which was evidence from some homes that training had a low priority in these homes. Some homes paid their staff to undertake mandatory training but it was suggested that they may be unable to pay for other training that staff might want to do. Most homes struggled to make a small training budget meet their needs whilst others had no designated financial support for training. Some homes paid their staff to undertake mandatory training but were unable to pay for other training that staff might want to do. Table 5 shows potential CST trainer enabling factors identified from the literature mapped to evidence obtained from the interviews about the training provision (i.e. the CST model of training delivery) The trainer was seen to be very flexible in her approach. She arranged times and venues to suit the homes; liaised with the prospective trainees and training leads as
! 16
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
well as the home managers in order to set venue, date and time. The trainer was willing to consult with the care homes, their managers and trainees about the shape and form of the training sessions. This was seen as important as when training was delivered at the care home many more staff members could attend. The trainer was able to adapt and tailor the course to the needs of individuals and homes. One of the strengths of the training was that it could be requested at point of need. If a home found they have a sudden urgent need for training they could ring the trainer who, if necessary, would devise and design some training. Respondents in the interview study reported that trainees learn not only how to perform a task but the reasons why it’s necessary and the consequences of performing it and that the trainer encouraged questions and trainees were happy to come forward with their queries. Their questions were all addressed with consideration and respect. The trainer always made time at the end of the training sessions to talk informally with the trainees about any issues they might have and this was seen as a strength and lead to good relationships for future training. Table 6 shows potential CST trainer barriers identified from the literature mapped to evidence obtained from the interviews about the training provision. There were no reports from those interviewed relating to the following barriers.
• Unapproachable trainers • Lack of financial incentives • Difficult relationships between academic and service staff • Conflicting value systems of trainees, academics and home managers • Course content inappropriate for trainees’ needs
There was some evidence for “Lack of clarity about training and the trainer’s role “ It was felt the communication and publicity sometimes hadn’t been effective with more information about what covered be provided rather than responding to care homes request or identified need. Unexpected cancellations on training sessions were sometimes a happen from care home perspective but the CST responded positively to this situation. Managers have experienced difficulties accessing training in clinical skills. There were reports from
! 17
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
some residential homes that they can get funding for NVQs, distance learning and mandatory training but have particular problems accessing training in specific subjects like pressure area care (even when it is the focus of safeguarding issues). Some homes have their own trainers who deliver mostly mandatory training.
Table 7 shows potential care home staff (trainee) enabling factors identified from the literature mapped to evidence obtained from the interviews about the training provision. There was a sense that trainees saw the trainer as being a help and support rather than a threat or regulator. It appeared evident that the trainer had accessed training herself in order to be able to provide training for care home staff and the trainer’s district nurse experience was considered essential to be able to seek out further training and the locate the training in a care home context. The trainer was available via phone or email and made follow up visits to homes after the sessions had been delivered. The trainer signposted staff to other sources of training, help and support and often arranged this to support care homes. The mix of theory and practice is good and the workbook was seen as a particular useful resource. The use of mannequins provided valuable practical experience. All grades of staff trained often in mixed groups and the interactive teaching style was appreciated Table 8 shows potential care home staff (trainee) barriers identified from the literature mapped to evidence obtained from the interviews about the training provision. There were no reports of the following potential barriers
• Specialist input perceived as a threat
• Feelings of vulnerability • Conflicting priorities between workload and training • Low staff morale • Trainers perceived as regulators
There were some reports of negativity and resistant to change. Some staff were reluctant to attend training sessions and were resistant to changes in their practice. There was evidence that some staff felt less valued that NHS colleagues and this could impact on their willingness to engage, although the fact that the training was
! 18
Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
tailored to their needs offset this somewhat. Staff shortages were evident and had a negative impact, at times, for example, when trainees sometimes had to leave training sessions to answer residents’ calls. Table 9 a&b provides an outline of the 35 potential positive impacts that were identified in the literature review and how they map onto the qualitative data. It was clear that hundreds of people were trained (749 in total) and resources were developed in seven clinical areas. Although this evaluation did not assess the content of individual training packages as the focus of this evaluation was to explore the impact of providing the training to the users of the service. There was reported evidence for all 35 potential impacts, although it was clear that some impacts were more frequent and others more complex. For example, there was a clear impact on community nursing and GP resources with regular reports and examples of visits and community resources being reduced. In terms of preventing hospital admissions, the picture was less clear as care home staff reported that ambulances and hospital admissions were usually triggered by GP involvement rather than the care home directly calling an ambulance and indeed one quote suggests that sometimes the systems do not allow care homes to prevent an ambulance being called.
“We have one lady who has got cancer and a month ago the staff were quite worried about her, but it was
a Saturday and they just wanted some advice, some information. But obviously when you phone up you
get put through to NHS Direct and you go through the whole list of questions and at the end of it
obviously it flags it up, you send an ambulance and no matter how many times a member of staff said ‘we
don’t need an ambulance, we just need to speak to somebody for some advice’ ‘no, we have to send an
ambulance’ ‘but we don’t need one! We just want advice’ So the ambulance service turned up and the
ambulance crew just looked at us and said ‘what do you want us to do?’ we’re like ‘we’re really sorry, we
tried everything for them NOT to send an ambulance’ and they were like ‘it’s not your fault, it’s a new
system that’s in place’ [111] And all they do is go down their checklist and if you don’t give the right
answers he says ‘obviously, you tell the truth about your patient and it flags it up send an ambulance.’
But even when the paramedic got on the phone he was like ‘they don’t need us – all they wanted was a
GP to come and see her for some advice.’ And even he had to battle to get us a GP. He was like ‘It’s
ridiculous. A new system was just a waste of time. It’s a waste of time, it’s a waste of money.’ “ [Care
home manager] (see Table 9 (a) Table 10 shows the qualitative evidence mapped onto the potential negative impacts of providing a clinical training post for care homes. The literature identified 9 potential negative impacts and these are listed below;
1. Reluctance to take on new responsibilities after training
! 19

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
2. Failure to cascade new learning to wider workforce
3. Training seen as a post registration exercise and not an exercise in competence
building
4. No provision made for staff cover during training sessions
5. Highlighted communication problems among staff
6. Dependence of trainees on trainers up to the end of the course
7. Destabilised traditional social care ways of working.
8. Clinical skills advanced at the expense of social care
9. Uncovered resistance to change
From this list only one negative impact was reported within the qualitative interviews and that was “Uncovered resistance to change”.
Therefore on balance more positive impacts were realised than negative impacts and the implementation of CST model generated evidence of using enablers to promote training than experiencing the potential barriers to training.
Section 4 Development of Impact case studies
In addition to mapping enablers, barriers and positive and negative impacts, the evaluation sought to develop impact case studies which emerged from the data. This report concludes with the eleven case studies that were evident and these are presented in narrative form below (names and identifiers have been changed). Please refer to Table 2 (page 11) to see how these impact case studies relate to the training provided.
Case Study 1
Care of the older person’s skin and pressure ulcer prevention
The carers in care home X noticed that Ted and Elsie had developed red pressure areas that had progressed into ulcers. As they were often not around when Ted and Elsie were having their wounds dressed they had no idea how deep the wounds were or how to grade them. They frequently turned them onto alternate sides but
! 20

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
didn’t know why they were doing it; it was just something they ‘had to do’. The wounds were proving slow to heal.
The manager was keen to put something in place to improve the situation so contacted the clinical skills trainer to run some training sessions for her staff. Forty staff attended the sessions and immediately started putting their new learning into practice.
They talked to each other about the reasons behind position changes and began using the 30 degree tilt. If they noticed a resident had a red mark on their skin they reported it immediately and documented it in the care plan in much more detail then they had before the training.
They started to use the new positioning with Ted and Elsie, supporting them with pillows both in and out of bed, using the 30 degree tilt. They now knew that there was no need to keep hoisting them back into bed, as long as they were positioned in their chairs in the correct way. Thankfully, the pressure ulcers have now healed. What were once Grade 2 pressure area ulcers are now very slight pink areas and the red areas that Ted had on his spine have gone?
The carers feel happy that they know the reasons for performing care tasks and are providing good quality care. Not only are they preventing distress and discomfort but they are also saving resources in terms of wound dressings and district nurse and community matron time.
Case Study 2
Care of the older person’s skin and pressure ulcer prevention
Tom became a resident in care home X in October. By November he had developed a large pressure ulcer on each of his heels. He was mobile and didn’t spend a lot of time in bed. He would only go to bed if he felt particularly sleepy. As the care home staff didn’t do a full body map when new residents came to them they had no idea if he’d acquired the ulcers in the home or if he already had them when he arrived. The district nursing team were called to assess Tom’s condition and his case went to safeguarding.
The care home manager realised that although her staff now knew that all the residents had to have a full body map, some of them didn’t know what they were
! 21

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
looking for and needed some training in pressure area care as a matter of urgency. The district nursing team said they could provide training but didn’t have the time and would not normally do it and the local hospital offered training and then withdrew the offer when they realised the care home was residential and not nursing - a reason that other providers cited when refusing to provide training. Social services expressed surprise at this as they believed that training was readily available. Eventually the tissue viability nurse at the local hospital told the manager about the clinical skills trainer pilot project and she got in contact.
Ten healthcare assistants underwent training. Some were already trained to NVQ Levels 2 and 3 but pressure area care had not been part of that particular training programme. The staff were keen to be included in the training sessions as they wanted to demonstrate that with the right support they could provide effective care. The only difficulty was getting everyone to the training sessions, but the trainer was willing to arrange sessions to meet the care home’s needs, even holding evening sessions if necessary.
Since the training the home has introduced the use of skin bundles which has raised awareness of residents’ mobility. They have acquired pressure cushions and mattresses and have started to use pressure area safety calendars. The staff now realise how important it is to re-position residents, even when they’re resting on air mattresses, and to check that their sheets aren’t wrinkled. They are able to recognise triggers for pressure ulcers, for instance if someone isn’t eating properly or is becoming less active. They can spot someone at risk and monitor and record their condition.
At the time of the safeguarding issue the staff were quite despondent but since the training they are feeling much more confident in their practice. Levels of morale and self-esteem have risen and some of the staff have felt empowered to carry on with more training, progressing with both NVQs and distance learning.
Tom is still visited by the district nurses although now much less than weekly as his pressure ulcers have healed. There are currently no pressure ulcers in the home.
Case Study 3
Fine bore naso-gastric tube feeding and care
! 22

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Bob had been in hospital for a year. Being in a vegetative state his primary need was for intensive basic nursing care and so he had been transferred to care home X. He was unable to be fed via a PEG as he was prone to becoming agitated and had pulled his PEG tube out on several occasions. His nutrition was now delivered through a fine bore nasogastric tube which often became dislodged, either during one his frequent coughing attacks or through him pulling on the tube. It was of paramount importance that the feeding tube should be in situ at all times as Bob was a diabetic. When the care home manager accepted Bob as a resident it was on the condition that someone from the Trust would come to the home and train the staff in caring for and maintaining the feeding tube. This happened when Bob first arrived at the home but over time some trained staff had moved on whilst others needed their skills refreshing and updating. The Trust trainer was unable to deliver the training due to time commitments so the care home manger turned to the community matron for support.
The community matron found that as Bob’s needs were so specialised there was no-one working in the community with the skills they needed. She contacted the local hospital and arranged training for the clinical skills trainer and herself. Together they organised a training package and sent some of the staff along to the hospital to be trained as well. They designated one of the staff members to be a ‘champion’ and to take the lead on issues surrounding Bob’s care. This champion, together with the clinical skills trainer is now responsible for keeping the staff’s skills up to date.
Prior to the training Bob had to have a bolster fastened to the tube to try to prevent it dislodging (which once resulted in Bob sustaining a torn septum) and, if it did, he had to go to hospital to have it re-inserted. Now Bob needs neither the bolster or to go to hospital. His daughter is particularly pleased that the care home staff now have the necessary skills. Bob is now spared the stress and discomfort of lying around in an A&E department and can have his care delivered in familiar surroundings by people he knows.
Case Study 4
Venepuncture
Care home X specialises in dementia care. It comprises two nursing units and two residential units. Although able to give advice to the carers working in the residential
! 23

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
units, the nurses in the nursing units are unable to give any practical help. When nursing tasks and duties are required the carers have to call on the district nursing team. This poses particular difficulties for the residents living with dementia as to be approached by a stranger who wants to perform some often invasive and personal procedures can be frightening and threatening. Residents often can’t comprehend what is happening to them and can often become agitated and aggressive so it’s far better if they see a familiar face. Having blood taken is one uncomfortable procedure that occurs frequently. When blood needs taking in the residential units the district nurses have to be called on – sometimes to make several visits in one week.
The care home manager realising the disadvantages of the process for staff, residents and the district nursing team contacted the CQC to see if they would allow carers to undertake venepuncture training. They were a little ambiguous in their reply as traditionally it has always been nurses who undertook this task. Undeterred, the CCG were contacted. They recognised the value of the proposal and confirmed that as long as the person taking blood had the appropriate competences and a grounding in theory they would be willing for it to happen – after all, the majority of hospital phlebotomists do not possess a nursing qualification.
Knowing she had the backing of the CCG the care home manager contacted the clinical skills trainer and arranged for two of her senior carers to be trained in venepuncture. The trainees were delighted and keen to learn their new skills. The training went well and when it came time to gain competence with the residents they found them more than willing to co-operate. If there had been any difficulty the trainer offered to return to the home at any time to observe the trainees’ practice and to sign off their competencies.
There is now no need to call out the district nurses when blood needs taking. It has become evident that it is more convenient having staff on site who can take blood, as very often the residents will initially decline the procedure and need several approaches before they agree to it. A district nurse would find it highly inconvenient, if not impossible, to keep returning to the home to persuade residents to co-operate. They are more comfortable having staff they know carry out the procedure and the carers feel confident in their practice and valued by their management and their colleagues. There are now about ten more carers keen to learn how to take blood
! 24

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
and the care home manager exercising her professional judgement as to who would be the most suitable candidates for this role.
Case Study 5
Catheterisation
Care home X employs a lot of nurses and care staff from overseas. In some of their home countries there is less regulation than in the United Kingdom and nurses regularly carry out procedures less commonly done here.
Thelma was a resident in care home X. She started to complain of abdominal discomfort which over a short period of time grew worse. On examination her abdomen was becoming distended, but the care staff couldn’t understand why. They called the GP who came in to see Thelma and decided she had urinary retention. She needed catheterising as a matter of some urgency. The nurse on duty was unable to carry out the procedure as she wasn’t trained to UK standards and so the district nurse was called in. When the district nurse arrived she demanded to know why the care home staff hadn’t catheterised Thelma as it was a medical emergency. The issue went to safeguarding.
The nurses at care home X are now trained to UK standards by the clinical skills trainer. They are proficient in catheterisation, catheter care, basic observations, and venepuncture and pressure ulcer prevention.
Case Study 6
Fundamentals of catheter care Care of the older person’s skin and pressure ulcer prevention
Trudy is a care assistant at care home X. She has worked there for just over a year and it’s her first experience of working in a care home. With no previous experience everything was new to Trudy and she has welcomed the opportunity to undertake training. She attended training sessions on catheter care and pressure ulcer prevention given by the clinical skills trainer and hosted at the care home. She was able to attend because she was on duty and her training time was rostered so was covered by a colleague.
The courses were attended by a mixed group of both care assistants and registered nurses. Trudy felt a valued part of the group and didn’t feel silly asking the most
! 25

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
basic of questions. Much of the training was based on real life scenarios which she found useful as she was able to relate it to her work on the unit. Passionate about her work, the training has enhanced Trudy’s care giving. She now feels she understands why things happen and has amended her practice in line with the training guidelines. She is confident that what she does now is best practice. Trudy is keen to enrol on more training sessions when they are offered and has asked to be considered for venepuncture training.
Case Study 7
Venepuncture
Whilst on a doctor’s round at care home X the GP mentioned how useful it would be if the nurses at the home could take blood as when there were bloods to be taken the she would always be called in to do it. The care home manager mentioned this to the staff and a couple of nurses immediately expressed interest in venepuncture training.
The manager and clinical lead had once discussed the possibility of staff being up skilled in venepuncture but had had great difficulty in finding appropriate training. Having heard about the clinical skills trainer at the Care Home Forum they contacted the trainer to find out exactly what the training consisted of and to explore why it was needed and if there was enough blood taking opportunities for it to be viable. Establishing contact with the trainer was very easy, the trainer liaised with the potential trainees and the clinical lead and the sessions were timetabled.
The trainees thoroughly enjoyed the training sessions but one nurse felt a little apprehensive about putting the training into practice. The trainer was contacted and came back to the home to work closely with her until she gained in confidence. Even now, the trainer is only a phone call away.
The nurses now take all the bloods for routine checks, for Hbs, FBCs, LFTs, thyroid and kidney function – everything except INRs and for that they go to a local surgery.
If blood samples are needed urgently the GP will call the care home, fax through the details and a nurse will be able to take the blood within minutes if necessary. The GPs are impressed with the training and the impact it has had. They are saving time and resources and getting results faster.
! 26

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
The two colleagues who were trained have established a filing system and an information booklet. They record the blood samples they have taken and leave messages for each other if needed. They pass information on to the rest of the staff and everyone takes any blood forms and relevant information straight to them. They have formed a very effective team, working in tandem.
Case Study 8
Immunisations and Vaccinations
In autumn last year the community nurses were due to have an annual update on immunisations and vaccinations in preparation for delivering flu vaccines. 130 nurses needed training in a very short space of time and over a very wide geographical area.
The senior nurse met with the clinical skills trainer and together they devised some training sessions. There was consultation with the community nursing teams with regard to local knowledge and protocols and after only a couple of weeks eight sessions were successfully delivered within a week across several sites with each trainee being given an information handbook.
This has now formed the basis for the development of in-house training which will be used in future years.
Case Study 9
Care homes and community nurse time
The senior community nurse is asked to complete numerous tasks when visiting residents – often unrelated to her booked visit. There may well have been requests to take bloods or to attend to someone’s catheter. Now that more care home staff are trained in phlebotomy and catheterisation there are fewer requests for unscheduled tasks. The fact that the trainer actually trains in the homes means that she has reached more staff members and post training she is able to observe their practice, supporting them until they gain in confidence and skill. In terms of scheduled tasks, during the last six months the senior nurse has had no callouts to perform either male or suprapubic catheterisations. She feels this indicates just one positive impact of the clinical skills trainer project.
Case Study 10
! 27

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Venepuncture
Jayne, a senior nurse at care home X had been trained in venepuncture in the past but knew that she needed her skills updating as she hadn’t practised for a while. She rang the local hospital who told her that they were only training their own staff and couldn’t extend into the community. She searched the Internet for alternatives and decided to pay £250 for a course offered by a private company.
A few months later Jayne found about the clinical skills trainer project and arranged for staff at the care home to attend several courses. She elected to go on the venepuncture course which was hosted by another care home. She found that this course compared favourably with the course she had paid to attend. It was far more interactive and the trainer being a nurse made a big difference as she was able to relate to the trainees and their working environment.
Now that Jayne has updated her skills and feels competent and confident to practise she never has to call on anyone else to take the bloods of residents on the nursing unit – when she is on duty. However when she is off duty others have to deliver the service. This either falls to the community nurses, the community phlebotomy team or the GP surgery. Residents who are able to go to the GP surgery, but for some this can be quite traumatic. Jayne is not allowed to take bloods on the residential unit. There are other nurses at the home who are keen to join Jayne and undertake the training.
Case Study 11
Basic Observations
The senior nurses in care home X noticed that although their care assistants were taking and recording temperature, pulse, respiration rates and blood pressure levels competently, they had little understanding of what the readings actually meant. They relied on them to use their observation skills and to recognise problems as very often there was only one nurse on duty. When readings appeared to be abnormal they were always quick to report back to senior staff but were unable to recognise their significance. Always keen to take up the offer of training, the senior care assistants attended a basic observation course run by the clinical skills trainer. It fired their enthusiasm and empowered them in their practice.
! 28

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
The senior care assistants now have not only a competence but an understanding of what they’re doing. They are telling their junior colleagues what to watch out for. They know that when a resident looks unwell they take their basic observations and look for abnormalities and as a result their response has become quicker and more informed. For example, when a resident shows signs of having a urinary tract infection it no longer progresses to an advanced stage as the care assistants realise much sooner that something is wrong. When they record the basic observations they know what they mean, know that they are abnormal and know why that might be. They pass on the information immediately to the nurse in charge who calls in the district nurse or the GP. By managing conditions like this more effectively the risk of a potential hospital admission is averted.
References Anderson, W., 2004. Specialist support teams: influencing the nursing care of older
people. Nursing Older People 16 (1), 18-20. Avis, M., Greening Jackson, J., Cox, K., Miskella, C., 1999. Evaluation of a project
providing community palliative care support to nursing homes. Health and Social Care in the Community
7 (1), 32-38. Berry, L., 2013. Francis Report proposal of registered role rejected. Nursing Older
People 25 (4), 5. Borbasi, S., Emmanuel, E., Farrelly, B., Ashcroft, J., 2010. A Nurse Practitioner
initiated model of service delivery in caring for people with dementia. Contemporary Nurse 36 (1-2), 49-60.
Butler, K., 2012. Benefits of a peripatetic support mentor. Nursing Times 108 (34), 23-25.
Davies, S., Doherty, D., Glover, J., Johnson, T., 2004. Preventing hip fractures in care homes 2: role of the specialist nurse. British Journal of Nursing 13 (22), 1335-1341.
Doyle, S., Gallagher, J., Bell, M., Rochford, C., Roynane, S., 2008. Establishing a ‘train the trainer’ education model for skills development. Nursing Older People 20 (5), 34-37.
Ehlman, K., Wilson, A., Dugger, R., Eggleston, B., Coudret, N., Mathis, S., 2012. Nursing Home Staff Members’ Attitudes and Knowledge about Urinary Incontinence: The Impact Of Technology and Training. Urologic Nursing 32 (4), 205-213.
Green, N. Thorogood 2009 Qualitative Methods for Health Research Sage Publications Ltd., London
Hall, C., Castleden, C.M., Grove, G.J., 1988: Fifty six continence advisors, one peripatetic teacher. BMJ 297, 1181-1182.
Hatcher, S.L., Chamberlain, J.A., 2000. Clinical skills training in the nursing home. Nursing and Residential Care 2 (3), 125-129.
! 29

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
Hausken, M.F., Graue, M., 2013. Developing, implementing and evaluating diabetes care training for nurses and nursing aides in nursing homes and municipal home-based services. European Diabetes Nursing 10 (1), 19-24.
Hays, R., Clarkson, P., Tucker, S., Challis, D., 2012. Healthcare support services for care home residents. Nursing Older People 24 (10), 26-30.
Hayes, N., Martin, F., 2004. Supporting care homes: the older people’s specialist nurse. British Journal of Nursing 13 (21), 1250-1257.
Heals, D., 2008. Development and implementation of a palliative care link-nurse programme in care homes. International Journal of Palliative Nursing 14 (12), 604-609.
Heath, H., 2012. How to optimise the registered nurse contribution in care homes. Nursing Older People 24 (2), 23-28. Heeley-Creed, D., Brown, K., Hill, J., 2007. Carlisle and District diabetes training in
nursing and residential care homes. Practical Diabetes International 24 (1), 15-18.
Lansdell, J., Mahoney, M., 2011a. An end of life care training programme from hospice staff. Nursing and Residential Care 13 (9), 438-440.
Lansdell, J., Mahoney, M., 2011b. Developing competencies for end-of–life care in care homes. International Journal of Palliative Nursing 17 (3), 143-148.
Law, J., 2003. Pressure ulcer prevention: education for nursing home staff. British Journal of Nursing 12 (9), 566-569. Lekan, D., Hendrix, C.C., McConnell, E.S., White, H., 2010. The Connected
Learning Model for disseminating evidence-based care practices in clinical settings.
Nurse Education in Practice 10, 243-248. Morgan, J.C., Konrad, T.R., 2008. A mixed-method evaluation of a workforce
development intervention for nursing assistants in nursing homes: the case of WIN A STEP UP.
The Gerontologist 48 (Special Issue 1), 71-79. Nelson, S., Wild, D., Szczepura, A., 2009. The forgotten sector: workforce
development in residential care for older people. Nursing and Residential Care 11 (4), 200-203.
Raunkiaer, M., Timm, H., 2010. Development of palliative care in nursing homes: evaluation of a Danish project. International Journal of Palliative Nursing 16 (12), 613-620.
Ritchie, L. Spencer, W. O’Connor 2003 Carrying out qualitative analysis In J. Ritchie, J. Lewis (Eds.), Qualitative Research Practice, Sage Publications, London pp. 219–261
Waldron, M., Hasson, F., Kernohan, W.G., Whittaker, E., McClaughlin, D., 2008.Evaluating education in palliative care with link nurses in nursing homes.
British Journal of Nursing 17 (17), 1078-1083. Wild, D., Szczepura, A., Nelson, S., 2010. Residential care home workforce
development. University of the West of England. Joseph Rowntree Foundation.
! 30

Schoo
l of H
ealth
and C
ommun
ity Stud
ies Le
eds B
ecke
tt Univ
ersity
PERIPATETIC CLINICAL SKILLS TRAINER EVALUATION: FINAL REPORT: November 2014
! 31