final radiology report - wales
TRANSCRIPT
Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 1 of 37
Diagnostics Redesign Group
Radiology Group Report
Contents Page
Ref
Subject
Page
Executive Summary 2 1 Introduction 4 2 Scope 4 3 Terms of Reference 4 4 National Context 5 5 Role of Diagnostic Imaging 7
5.1 Service Strategy 8 5.2 Benefits Realisation 9 5.3 Existing Services 10 5.4 Information Technology 11 5.5 Capacity Planning 12 6 Service review by modality 14
6.1 Interventional Radiology 14 6.2 MRI Scanning 15 6.3 CT Scanning 16 6.4 Fluoroscopy 17 6.5 Nuclear Medicine 18 6.6 General Radiography 18 6.7 Ultrasound scanning 19 6.8 PET CT 20 6.9 Mammography 21 7 Workforce Planning 22 8 Finance and Activity 27 9 Recommendations 30
Appendix 1 Terms of Reference 34 Appendix 2 Membership of the group 36 Appendix 3 Acronyms 37

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 2 of 37
Executive Summary Diagnostic imaging plays an increasingly important role in the provision of modern, effective healthcare for many patients. It can establish the presence or absence of disease, inform prognosis and monitor the effectiveness of treatments as well as guiding minimally invasive interventions. Traditionally in the NHS imaging tests, particularly the more sophisticated modalities such as CT and MRI, have been viewed as expensive. Access to imaging has therefore been tightly controlled by limiting referral rights and substantial waiting lists. As a result diagnostic imaging is often utilised relatively late in the patient’s journey through our healthcare system. There is an increasing view, supported by limited evidence, that improving access to sophisticated diagnostic imaging and utilising these tests earlier in the patient pathway can have significant overall benefits on the efficiency of a health economy. This is achieved by shortening patient pathways, reducing patient attendances, decreasing lengths of stay and limiting unnecessary and ineffective treatments. Although diagnostic-imaging costs will rise substantially there is the potential to offset this by efficiencies elsewhere in the healthcare system. Diagnostic imaging departments will be centred on each of the three acute (level 3) hospital sites in North Wales. This recommendation falls out of the decision in Designed for North Wales to continue to admit unselected trauma and unplanned admissions at each of these sites. These services would be supported by general radiography and / or ultrasonography provision at a number of community sites. The continuing development of the North Wales Regional Imaging Network will support standardisation of access and service provision across North Wales and the development of sub specialist services to support patient care. All three North Wales Trusts are forecasting substantial increases in demand for ultrasonography, CT and MRI. Extending working hours on current equipment will allow Trusts to meet this demand in the short term. This will not, however, be sufficient to meet future requirements or to enable a service reconfiguration placing diagnostic imaging at the front end of clinical services. For these modalities there will be a need to increase the amount of equipment available in North Wales as well as to ensure timely replacement of existing equipment. Both scenarios will require additional staffing. Given that the minimum training time for a Radiographer is 3 years and a Consultant Radiologist is 5 years, workforce planning to meet agreed increases in capacity needs to occur as a matter of some urgency. Some of the requirements for an increase in the diagnostic imaging workforce can be partially offset by a combination of skill mix and careful service planning – e.g. co-location of additional equipment to share existing reception facilities. A key enabler in this new service model will be improvements in current IT systems particularly the procurement of a suitable replacement Radiology Information System and the ability to transfer patient data to tertiary care providers based in England.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 3 of 37
A substantial increase in diagnostic imaging capacity will allow Trusts to meet future demand and reconfigure services to place imaging at the “front end” of patient services. This approach offers significant benefits but will require overall service redesign and considerable managerial input if efficiencies elsewhere in the system are to be recognised and captured.
Vision To ensure safe, timely access to a range of high quality, clinically effective and resource effective imaging services as determined by patient and service need.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 4 of 37
1.0 Introduction The Diagnostic Services (Imaging) Redesign Group has developed the vision for services
put forward in the consultation document ‘Designed for North Wales’ and its supporting work including the benchmarking against UK best practice undertaken by Teamwork. It builds upon the work of the Diagnostics Clinical Task and Finish Group. It has developed a more detailed picture of services to inform the Regional Strategic Outline Plan and the local health economy Strategic Outline Cases.
The work of the group has informed the regional chronic disease management vision and
the community service frameworks. 2.0 Scope The Diagnostics Service Redesign Group agreed that the remit of diagnostics was so wide
that a useful review could not be achieved within the set timescale. The Group therefore focussed upon the two main areas of pathology services and clinical radiology. Departments of clinical radiology deliver a range of services including both diagnostic imaging and minimally invasive treatments by interventional radiology techniques. The latter services have strong and complex links to clinical specialities and have therefore not been considered in detail. This document therefore concentrates upon diagnostic imaging. ‘Diagnostic imaging’ describes the production of images of the human body that enable the diagnosis of disease and/or checks for the effectiveness of treatment. The use of diagnostic imaging for screening services e.g. breast cancer screening, is out with the scope of this document.
3.0 Terms of Reference The group needs to look at services for diagnostics in the round, but it will focus particularly on
1. Link closely with the work of the national Imaging Modernisation Project and Regional Imaging Networks. 2. The facilitation of long-term condition management in the community. 3. The facilitation of optimising the use of day surgery and minor outpatient
procedures. 4. Minimising the number of visits to a hospital site for diagnostic imaging. 5. Minimising duplication in imaging. 6. Exploiting the potential offered by IT developments 7. The groups work needs to link to the Access 2009 work (but not to duplicate it). 8. The need to shorten patient pathways. 9. The exploration of models of diagnostic delivery eg out of hours, planned and
unplanned work.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 5 of 37
4.0 National Context Two main documents set the scene within Wales for diagnostic imaging. Designed for Life
identifies the need to provide appropriate evidence based, quality assured clinical treatment and care. The national Diagnostic Services Strategy is an attempt to respond to the themes set out by D4L and to identify the role of diagnostics in the proposed service model. Both documents contain a number of common design principles and key objectives of relevance to diagnostic services including:
• Access to appropriate services when they are required.
• Diagnostic investigations that contribute to the effective delivery of patient
pathways.
• The use of technology and tele-health to reduce the need for hospital attendances.
• Comprehensive access to diagnostic test results that will contribute to effective demand management and appropriate use of services.
• Optimised services using the latest technology to provide effective test requesting,
results reporting, images, and information to clinicians and specialists.
• The development of specialist units staffed by well trained professionals and supported by high quality diagnostics
Vision 2015 will be delivered through a series of strategic frameworks, each covering three
years. Redesigning Care 2005-08, places emphasis on service redesign and reconfiguration via clinical networks and performance management as key enablers for improving health and social care in Wales. As part of this process the national Diagnostic Services Programme aims to implement the recommendations made in Designed for Life through the modernisation of diagnostic imaging and pathology services. An Imaging Modernisation Board, informed by the Imaging Modernisation Advisory Forum, oversees this process.
5.0 North Wales Context Designed for North Wales identified several key decisions that will shape diagnostic imaging services in the future:
• Services will increasingly be provided in a community setting • These services will be supported by a number of Level 1 and 2 facilities • Each of the three main existing district hospital sites (Level 3) will continue to
accept major trauma and other unselected unplanned admissions • Many tertiary services will continue to be provided by specialist centres largely
based in England

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 6 of 37
The document sets out that at Level 1 effective and rapid diagnosis will be available locally. High quality diagnostic facilities providing on-site support for treatment and diagnosis will be available at Level 2. Levels 3 and 4 will deal with complex cases that require a concentration of skills and equipment.
Recommendation: TABLE 1 Imaging Modality Level 1 Where appropriate:
General radiography Ultrasonography
Level 2 Depending on the configuration of clinical services:
General radiography Ultrasonography CT
Level 3 Full range of imaging modalities which must include:
General radiography Ultrasonography Multi-slice CT MRI Nuclear Medicine Interventional fluoroscopy Fluoroscopy
In addition may include: Cardiac Imaging Visiting mobile imaging units
Level 4 Full range of imaging modalities
That the provision of diagnostic imaging services at each Level should be based on Table 1.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 7 of 37
5.1 Role of Diagnostic Imaging Diagnostic imaging performs the following functions:
1. Enables appropriately trained clinicians to establish the presence or absence of disease 2. Allows appropriately trained clinicians to inform the clinical management plans of patients 3. Aids prognosis. 4. Monitors the effectiveness of treatment 5. Imaging guided interventions (see interventional radiology)
Negative tests also have a value. , particularly in allowing clinicians to reassure patients that
their symptoms are not due to serious disease. This can avoid repeated consultations by patients.
It needs to be recognised that as the patient has to be physically present for an imaging
examination, and as such examinations are either performed by clinical staff or under their direct supervision, there is considerable opportunity to ensure the choice of examination is appropriate to the clinical problem. As a result there is very little unnecessary duplication of tests in diagnostic imaging.
Imaging technology has changed enormously since the development of the first commercial
CT scanner in 1972. The pace of change shows no sign of slowing with multi-slice CT, high field MRI, MR spectroscopy and PET/CT all now commercially available. The rapid development of new technologies and the widening applications for existing imaging modalities is the single biggest driver for service change. However, all imaging modalities have limitations and the interpretation of imaging findings depends crucially on the clinical context. It is vital to appreciate that imaging tests have to follow the clinical assessment and cannot be a substitute for the clinical assessment. However, current systems of work limit access to diagnostic imaging tests partly on the basis that they are costly. This is particularly true for the more sophisticated tests that have the greatest potential to influence patient management. However, there is accumulating evidence, largely from other health economies, that early access to sophisticated imaging can shorten patient journeys and hence allows more effective use of resource.
Vision To ensure safe, timely access to a range of high quality, clinically effective and resource effective imaging services as determined by patient and service need.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 8 of 37
5.2 Service Strategy The service model for diagnostic imaging meets the expectations set out in Designed for
North Wales. It suggests re-engineering both diagnostic services and clinical services to place appropriate diagnostic tests earlier in the care pathway. To achieve this, significant investment in additional diagnostic imaging capacity is required. Increasing capacity without controlling access runs the risk of encouraging inappropriate testing which fails to benefit patients. This risk will be heightened as more sophisticated imaging becomes available to clinicians working in the community and to other healthcare professionals. Good quality care pathways guide clinicians in selecting the most appropriate imaging test at the most effective point in the patients’ care.
Recommendation: Evidence based care pathways detailing the role and optimal timing of diagnostic imaging tests should be developed for common conditions. Recommendation: The role of the Map of Medicine in relation to care pathways and diagnostic imaging should be formally assessed. In line with Designed for Life and recommendations from the Department of Health in
England and various professional bodies to allow each of the three main hospitals to care for unselected trauma and emergency patients will require 24 hour access to the following services on each site:
• General radiography • Ultrasonography • Multi-slice CT • Nuclear medicine • Fluoroscopy services
Access to interventional radiology and MRI should also be available on a 24-hour basis,
although not necessarily on site. Once the decision to require these facilities on each acute site is accepted it is then logical to
centre additional services on these sites as efficiencies naturally accrue from using existing reception and other support facilities and by building on the existing technical and medical staffing.
Recommendation:
Evidence-based care pathways clearly specifying relevant imaging tests and their timing should be developed and adopted for all common conditions.
The role of the Map of Medicine in achieving the above should be formally investigated.
Additional imaging capacity should be based around the three acute Level 3 sites as set out in Designed For North Wales.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 9 of 37
Community based facilities will continue to provide general radiography and
ultrasonography services. The existing North Wales radiology network will evolve. The availability of PACS across
North Wales will facilitate the sharing of expertise and the development of subspecialisation across the region improving the quality of patient services.
The resource for responding to this rise in demand will come from both within the current
resources but also from the reinvestment in radiology services of some of the resources saved through the reduction in outpatient appointment and in-patient episodes facilitated by the early and more effective use of imaging services.
5.3 Benefits realisation This document asks for a major investment in diagnostic imaging and Departments of
Clinical Radiology. The service strategy set out will produce the following benefits:
1. More timely and accurate diagnosis 2. A reduction in waiting times for diagnostic imaging 3. Shortening the patient journey by earlier and more appropriate imaging 4. Avoiding unnecessary treatment e.g. non-curative surgery for patients with cancer 5. Avoiding admission by earlier testing and more thorough assessment of a patient’s condition 6. Reducing length of stays in hospital through providing more timely tests and better understanding of patients’ conditions. 7. The potential to release resources from other areas that could be used to fund investment in increasing capacity in imaging services.
Example A patient is admitted to an acute medical ward. A CT scan is requested for confirmation of
the suspected diagnosis and assessment. The patient’s condition is stabilised and is not life threatening. In view of this the CT scan is arranged for 48 hours time on an inpatient basis. The patient could be discharged home with early review following the scan result. However, under current arrangements if the patient is discharged the scheduled inpatient scan appointment will be cancelled and the examination added to the outpatient waiting list. The clinical team responsible is therefore likely to keep the patient in a hospital bed to obtain an earlier scan. By guaranteeing that booked inpatient studies will be honoured even if the patient is discharged home in the interim the clinical team are encouraged to allow suitable patients home earlier thus reducing lengths of stay.
Example Provision of ultrasonography in one-stop urology clinics. This facilitates a comprehensive
assessment of patients in allowing determination of a treatment plan on a single visit. This

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 10 of 37
decreases the number of patient attendances required and could support a reduction in the new to follow up ratios in outpatients.
Example Many patients with upper gastrointestinal tract symptoms require assessment by both
ultrasonography and gastroscopy. Although under current arrangements General Practitioners have direct access in all Trusts to both ultrasonography and endoscopy services many patients are still referred to a Consultant Gastroenterologist. These patients are assessed in an outpatient clinic and then referred for both ultrasonography and endoscopy with a follow-up outpatient appointment. Due to delays in the system it is not infrequent for patients to return to their follow-up appointment without having undergone one or both of the diagnostic tests. With an agreed care pathway patients could be assessed to an agreed standard in primary care and then referred to one-stop service providing ultrasonography and endoscopy on the same day and then returned to either primary care or a consultant outpatient appointment depending upon the test results.
5.4 Existing Services Clinical Radiology services are provided by each of the three Trusts across North Wales.
Specialist services are provided by centres in England particularly at the Walton Centre for Neuro Sciences and at Alder Hey for paediatrics but the majority of services are provided locally from each of the acute hospital sites. These are supported by a number of community hospital units providing plain radiographs and some provide limited ultrasonography. An informal Clinical Network (The North Wales Radiology Advisory Group) has been in existence for a number of years and has been invaluable in increasing standardisation in terms of clinical and quality standards based, for instance, on Royal College guidance. This enhances consistent levels of service delivery, reduces potential risk and facilitates sharing patient care across Trust boundaries. In 2006 WHC 06 (002) led to the creation of three Regional Imaging Networks across Wales. These networks act as links to the all Wales Imaging Modernisation Project. The North Wales Network has recognised the importance of maintaining strong clinical input and has agreed that the North Wales Radiology Advisory Sub Committee be recognised as a formal clinical advisory group.
The facilities supporting services are inadequate in some cases, with consequent levels of
variability in functionality and capacity. Some areas of departments exceed 25 years of age and no department was designed to cope with modern imaging requirements or patient throughputs. Despite this the Acute Hospital Portfolio reports of 2003/4 and 2006/7 confirm that radiology services in North Wales are generally provided to a high standard and in an efficient manner as compared against other departments both in Wales and in England. Overall the imaging equipment available is of a good to high standard and reasonably modern, (source Welsh Health Estates All Wales Equipment Register – Appendix 1). To maintain this position continued investment in replacing and updating imaging equipment is required, (source Welsh Health Estates Equipment Register).
Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 11 of 37
Recommendation Older imaging equipment is often technically more difficult to operate, produces less useful
images, is significantly slower thus limiting patient throughput and frequently exposes patients to more risk in the form of higher radiation doses.
Recommendation There is evidence, presented in detail under the modality headings, that access to some
imaging investigations in North Wales is lower than that in other parts of Wales and less than the average within England.
5.5 Information Technology Each Trust has a dedicated Radiology Information System (RIS) and a Picture Archiving
and Communication System (PACS). All use RaDIS, which is the all-Wales RIS, (except for Swansea) developed by Health Solution Wales (HSW). This system is now 19 years old, is not standardised across Trust boundaries and is recognised as no longer fit for purpose. The lack of standardisation and the failure to define common coding definitions limits the ability to transfer both patients between different departments and images between different PACS. HSW have recently developed a newer version of RaDIS, (RaDIS 2), although this has limited additional functionality and does not address the need to adopt common standards and codes. The Imaging Modernisation Project has developed an approved business case for a national replacement RIS supported by Informing Health Care. This will not be available until 2009 at the earliest. Meanwhile at least one Trust requires urgent upgrades to the RIS hardware to avoid the risk of a critical system failure. HSW state that RaDIS will not operate on modern servers. Server replacements or upgrades therefore automatically require a change of software.
Recommendation A particular issue in North Wales is the need to ensure compatibility of any RIS development with the systems in place at our tertiary referral centres in England.
Each Trust should agree a formal rolling equipment replacement programme supported by advice from the Regional Imaging Network.
Trusts should consider the need to upgrade to the RaDIS 2 system offered by Health Solution Wales
Rolling equipment replacement programmes should be adequately resourced across the region.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 12 of 37
Recommendation The ability to transfer images and patient information across existing healthcare boundaries
in North Wales and to English Level 4 providers will be essential if this service model is to function effectively and to enable a stronger network approach. The North Wales Trusts appropriately specified their PACS to ensure the technical ability to transfer images. Therefore images can now be transferred between Trusts but the process is slow, often unreliable and requires considerable manual intervention. The lack of standardisation of the RaDIS systems in each Trust also limits the ability of clinicians to view images obtained in different Trusts.
Recommendation Recommendation
5.6 Capacity Planning The following factors were used in estimating future demand:
• Workload generated by Access 2009 • Population growth and the impact of an ageing population • Reductions due to substitution either between tests or arising from new technology. • New technology allowing new tests to be undertaken. • New indications for existing tests • New screening programmes. It was agreed that these would be additional to the
above assumptions and would need to be dealt with as and when they arise. The work undertaken by the Regional Imaging Network on forecasting demand was
utilised. Current referrals significantly exceed capacity in all three Trusts particularly in the area of Ultrasonography, CT and MRI.
North Wales Trusts and the North Wales Planning Forum should ensure that the specification and procurement of the replacement national RIS is fully compatible with systems in Trusts in England providing services to Welsh patients.
The replacement national RIS should use common codes and standards to facilitate transfer of patient information and images across North Wales.
The DAWN2 network should be upgraded to allow transfer of images across existing Trust boundaries in a more timely fashion.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 13 of 37
TABLE 2 Combined Data 2005/06
CT Ultrasound
MRI Nuclear Medicine
Plain Films
NEWT 6,546 16,854 3,958 1,326 68,363 C&D 4,183 9,186* 2,289 722 No data NWWT 7,920 29,729 4,284 1,148 110,014 TOTALS 18,649 55,769* 10,531 3,196
• Excludes Obstetric US C+D Trust NEWT data Average 2005/06 and 2006/07 C&D data Calculated capacity (CPT) 06/07 N.B. Apparent variations in activity between Trusts should be interpreted with caution as
much of this may reflect variations in data collection and the lack of standardisation between RaDIS systems.
Each trust modelled future capacity requirements using a variety of tools including the following
• The NLIAH capacity planning tool • Historical modality growth rates • The Merseyside North Cheshire SHA Review of Imaging Services • Work undertaken by the National Imaging Modernisation Lead for England • Expert professional advise on future developments in imaging • Individual Trust responses by modality
Further group analysis indicates that where there are discrepancies between Trusts this was
almost entirely attributable to a combination of the limitations of the NLIAH capacity planning tool and the degree to which future developments and service changes had been recognised and incorporated. Examples would include the growth in non-invasive cardiac imaging by both CT and MR; the development of virtual colonoscopy; and the requirement to routinely scan patients with suspected stroke with MRI as well as CT. Based on this information the likely changes in demand were forecast as set out below.
Recommendation:
Services should be planned around the following changes in activity detailed in table 3:

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 14 of 37
TABLE 3
MODALITY
DEMAND CHANGE
General Radiography
Increase by 96% to 2009/10 then increase with population growth
Fluoroscopy Static to 2019/10 then population growth. Obstetric and Gynaecology Ultrasonography
Increase with population growth
General Ultrasonography
Increase by 117% 2009/10 then population growth
CT Growth of 250% to 2009/10 thereafter population growth was agreed
MRI Growth of 290% to 2009/10 thereafter population growth was agreed
Radionuclide Imaging Growth in conventional nuclear medicine which will be static through to 2009/10 and then slow decline
PET/CT Growth would be drawn from the current business case which takes into account NICE guidance
NB. It should be understood that the above figures are based on the best available
evidence and expert advice. They are, however, predictions and should be viewed as such. The demand for imaging services will, to an extent, be determined by the rate of change in clinical service provision. Base line is 2004/5 data.
6.0 Service Review by Modality 6.1 Interventional Radiology As noted previously this subspecialty has strong links to other clinical services, particularly
surgery. Pre-procedural and post-procedural care is largely provided by these other clinical services. Service provision should therefore be considered as part of the decision making process on the nature and location of surgical specialities and subspecialties. Availability of interventional radiology services is currently only required urgently for the care of a relatively small number of emergency admissions. This may change as the indications for interventional radiology increase e.g. aortic stent grafting for abdominal aortic aneurysm. In addition, for some patients, such services are critical e.g. emergency nephrostomy for patients with obstructed kidneys; arterial embolisation for acute haemorrhage associated with trauma etc.
Recommendation: MRI Scanning Extended provision of interventional radiology should be considered using a networked approach.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 15 of 37
6.2 MRI Scanning MRI (Magnetic Resonance Imaging) is a relatively new modality that uses a strong
magnetic field and radio waves to produce high definition cross sectional images. The applications for MRI have grown almost exponentially supported by rapid technological innovation by the major equipment manufacturers.
Although there are a variety of access targets set both nationally and internationally the
basis on which these have been set is often unclear. For example the Department of Health have previously, (2001) identified an access target for MRI of 35 scans per thousand population. However, this appears to have been based solely on international comparisons and did not have any clinical basis for its recommendation. Benchmarking the level of MRI scanning in North Wales shows that it is considerably behind comparable areas in England whether based on the number of scanners or number of examinations per head of population.
Recommendation It is likely that over the planning timeframe being considered MRI will partially replace
some general radiographic and contrast studies as the standard imaging technique. In addition to LDP activity this will contribute to a substantial increase in demand together with the development of non-invasive cardiac assessment by MRI, MR angiography, increasing assessment of musculoskeletal conditions and cancers using MRI and increased monitoring of treatment particularly in oncology.
Although moving to extended working hours should assist Trusts in meeting the 2009
targets the increase in capacity will not be sufficient to meet these additional demands. Recommendation The most effective option to provide this additional capacity is currently unclear. Increase
in capacity in England using mobile services has encountered significant clinical governance issues and under utilisation of capacity purchased while waiting lists remain significant. Use of smaller, cheaper MRI scanners dedicated to scanning limbs only may allow the transfer of significant work from larger, more expensive equipment. Despite this should the predicted changes in clinical practice result in the demand increases forecast it is likely that additional full sized scanners will be required on major hospital sites.
MRI capacity in each Trust should be increased by moving to extended working hours
Each acute hospital site should consider, with advice from the Regional Imaging Network, how it will meet future demand additional to that provided by extended working hours.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 16 of 37
6.3 CT Scanning CT (Computed Tomography) scanning utilises x-rays and electronic detectors to produce
cross sectional images of the body. CT has been a key part of the imaging department since the 1990’s with the development of spiral and multi-slice technology. These developments now mean that a scan of the head that in the 1990’s used to take 15 minutes can now be completed in 10 seconds. Although the scan can be completed in a significantly shorter time and produces images of a much higher quality the time required to report on all of the images has increased significantly due to the increased quantity of data for analysis.
The CT equipment across North Wales is all multi-slice although each Trust has only one
scanner. All of the CT equipment across North Wales is NHS owned/leased and managed by the organisation in which it is based. CT equipment utilisation is based on the core working hours of 9am-5pm Monday to Friday with all departments providing on-call emergency services 24 hours per day supported by 24-hour availability of consultant radiologists to provide image interpretation. Most departments currently manage both outpatient elective and A/E (emergency) patients on the same machine or within the same lists, although this fits with the principles of maximising productivity it reduces the quality of the service patients receive. This reduction in quality is easily identified with patients waiting within imaging departments past their designated scan times (due to urgent patients being ‘squeezed’ in earlier in the list) or emergency patients having to wait longer than guidelines would recommend due to a slot being unavailable.
All departments have capacity shortfalls and have plans to extend working hours once
funding is available. All Trusts have indicated they will require increased CT capacity to assist in meeting the Access 2009 targets and have submitted LDP bids on this basis.
Recommendation
It is likely that over the planning timeframe being considered CT will partially replace some general radiographic and contrast studies as the standard imaging technique on acute sites. In addition to LDP activity this will contribute to a substantial increase in demand together with the development of non-invasive cardiac imaging by CT, CT angiography, virtual endoscopy and increased monitoring of treatment particularly in oncology.
Although moving to extended working hours should assist Trusts in meeting the 2009 targets the increase in capacity will not be sufficient to meet these additional demands. 24 hour CT availability is also essential to deal with major trauma and in dealing with other, unselected acute admissions. CT scanners require planned downtime for maintenance, upgrades etc. and are subject to unplanned downtime. All North Wales Trusts have experienced significant difficulties due to the lack of availability of on-site CT. In future it is difficult to see how a hospital without CT available could continue to accept trauma or unselected urgent care patients. Mobile services are available, but generally not at short
CT capacity in each Trust should be increased by moving to extended working hours

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 17 of 37
notice nor are they suitable for trauma or other potentially unstable patients. Both on this basis and to meet forecast demand two CT scanners should be available on each major acute (Level 3) site. This has been recognised in England and most acute Trusts now have access to two or more CT scanners.
Recommendation 6.4 Fluoroscopy Fluoroscopic examinations have been an important part of imaging departments for a
number of years. The range of examinations requiring fluoroscopy includes barium meals, enemas, ‘T’ tube cholangiograms, hysterosalpingograms etc.
Historically North Wales Trusts possessed a large number of fluoroscopy rooms. All Trusts
have disinvested in this area to varying degrees. Currently local Trusts have three/five fluoroscopy rooms. Some Trusts have already significantly reduced their fluoroscopy capacity. This is likely to further reduce over time. However, more sophisticated fluoroscopy equipment remains important in guiding interventional radiology procedures.
Recommendation Recommendation Recommendation N.B. The development of a national screening programme for colorectal cancer may
partially invalidate these recommendations depending upon the choice of screening methodology.
Each acute hospital site admitting major trauma and/or unselected emergency care patients should have available on-site two multislice CT scanners based on clinical risk and forecast demand.
Investment in fluoroscopy capacity should reduce in line with decreasing demand
Trusts should not replace fluoroscopy equipment without careful consideration and advice from the Regional Imaging Network
Each Trust should ensure fluoroscopy provision is adequate to support interventional radiology procedures

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 18 of 37
6.5 Nuclear Medicine Nuclear medicine uses radioactive isotopes to label compounds that target specific areas of
the body or pathologies. Nuclear medicine is a modality that assesses function as well as anatomy and is an important part of cancer and coronary heart disease assessment and monitoring. PET CT is a combined imaging technology and is dealt with separately.
Nuclear medicine usually falls under the remit of the diagnostic imaging department yet the
regulatory framework is far tighter requiring additional qualifications for the reporting clinician, (ARSAC licences). Few current radiology trainees receive the training needed to become an ARSAC licence holder. A shortage of licence holders in the future is likely to mean that a North Wales network is required to maintain the service on all three sites. In the detection of coronary heart disease it is likely that it will be replaced by MR scans. A network across North Wales would help support and maintain services and usage. This solution is supported by the British Nuclear Medicine Society.
Overall, in volume terms, the demand for nuclear medicine has been falling with newer
techniques using other modalities (e.g. CT pulmonary angiography replacing nuclear medicine ventilation/perfusion scans for suspected pulmonary embolus). This trend looks set to continue. What is not apparent from the raw activity data is a shift towards the more complex end of the nuclear medicine scanning spectrum. This increase in complexity of scans means that although there is a loss in the overall volume of demand this is being offset and equipment is still being utilised at much the same level.
One specific exception to the generally reducing demand trend is with the provision of some
specialist heart scanning. This is supported by a NICE technology appraisal (exemption issued in Wales) as it allows better patient selection for cardiac angiography. It is likely that in the medium to longer term CT or MR scanning will become the preferred tests.
Recommendation Recommendation 6.6 General Radiography General radiography is the oldest of all x-ray imaging modalities with the majority of all
patients attending hospital having at least one radiograph during their management. General radiography activity is roughly stable but with very high throughput still remains a major
At present each Trust will need to maintain nuclear medicine facilities at roughly current levels
The Regional Imaging Network should co-ordinate a network approach to ensure nuclear medicine services across North Wales meet clinical governance requirements and that departments in each Trust are appropriately supported by ARSAC licence holders.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 19 of 37
consumer of resource. Radiography will remain the first request of choice for skeletal and chest imaging both in the acute and community setting.
There are a large number of community based general radiography facilities across North
Wales some with only limited access. Their distribution is largely historical and does not correlate well with population distribution or travel times. These do provide a valuable resource avoiding long travel times for many patients requiring only simple imaging and moving activity away from the main acute hospital sites. PACS allows provision of the same standards of service available at the main sites.
Direct digital radiography equipment allows higher patient throughputs under appropriate
condition but at a significantly higher cost than conventional radiography. This additional cost may be worthwhile in some settings particularly if combined with skill-mix initiatives.
Recommendation Recommendation 6.7 Ultrasound Scanning Ultrasound scanning is a technique that uses sound waves to produce images. This
technique is particularly good for demonstrating the anatomy of soft tissues especially in the abdomen. More modern machines are also capable of reliably demonstrating a range of musculoskeletal conditions. For this reason it is anticipated that orthopaedics, rheumatology and primary care will see a substantial growth in the use of ultrasound. Ultrasonography is quick, relatively cheap, highly accurate in skilled hands, increasingly portable and acceptable to most patients. Ultrasound also offers good opportunities for near patient testing i.e. use of community facilities, but the cost-effectiveness of this will be dependent on demand.
Recommendation
General radiography facilities should be provided in community settings based on population need and access. Such facilities should have direct links to Trust PACS.
Busy sites should carefully consider the cost benefit ratio of investing in DR when replacing conventional general radiography equipment
Ultrasonography facilities should be provided in community settings based on population need and access. Such facilities should have direct links to Trust PACS.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 20 of 37
Ultrasound can be loosely grouped into two main categories. The first is obstetric ultrasound where ultrasound is used to monitor the development of the foetus during pregnancy and identify abnormalities. This type of ultrasound scans is performed primarily by ultrasonographers (radiographers who have undergone additional training either at post-graduate diploma or MSc level) and are currently working in extended roles (i.e. reporting as well as acquiring images). The second category of ultrasound scanning, and the focus for this section of the document, is non-obstetric ultrasound (or general ultrasound) where ultrasound is provided as a diagnostic investigation. This service is provided by both ultrasonographers and radiologists who also provide additional services including ultrasound guided biopsy, drainage etc.
Ultrasonography as a diagnostic technique is not confined to radiology departments.
Increasingly other specialists e.g. in urology, wish to be trained in imaging for particular conditions. Such training is time-consuming and requires considerable input from consultant radiologists and senior ultrasonographers. It may, however, meet the objectives of providing diagnostics earlier in the patient pathway and improving access. The Royal College of Radiologists supports such initiatives providing sufficient resource is made available to enable adequate training, supervision and audit of performance.
Recommendation There is a significant amount of additional ultrasound equipment deployed outside
radiology departments e.g. on hospital wards, in A/E, ITU etc. Whilst this may be justified to improve accessibility some of this equipment appears to have very low utilisation and/or to be inappropriately specified. There is potentially a mismatch between equipment capability and usage, activity undertaken is unlikely to be included on any data return, the examination findings are often poorly documented and adequate maintenance and QA checks are often not in place. There appear to be significant opportunities to improve utilisation and quality of service.
Recommendation 6.8 PET- CT PET-CT is a hybrid technology that fused images from both CT and a sophisticated nuclear
medicine scan. It relies on special radioisotopes that can only be produced using a machine called a cyclotron. These are in short supply in the U.K.
A network approach to the training of other clinicians in ultrasonography should be adopted. This will need to be resourced.
That each Trust undertakes a full review of the portfolio of ultrasound equipment in their respective organisation

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 21 of 37
As the technology is relatively new its role is currently unclear and it’s effectiveness is only established for a small number of conditions. These are largely related to cancer staging where for a small number of patients it is essential in treatment planning. It is likely that as experience with this modality increases the indications will widen. The extent to which that will happen is uncertain. PET-CT is commissioned by HCW and North Wales patients are currently required to travel to Cheltenham for this service.
Recommendation A business case is currently being prepared by Conwy and Denbighshire on behalf of North Wales in respect of PET-CT scans. In the medium to long term the need to provide a service locally will depend upon changes
in referral criteria and patient need. Conwy and Denbighshire Trust are developing a business case on behalf of North Wales that will assess the available options.
Recommendation 6.9 Mammography Mammography uses dedicated radiography equipment to produce images of the breast and
is used both for screening and symptomatic diagnosis. All three Trusts provide this service, some on more than one site. Breast Test Wales also offers a screening service across North Wales using a combination of mobile and fixed equipment.
In 2009 Breast Test Wales will commence replacing existing equipment with digital
mammography. There is support from both Breast Test Wales and the North Wales Trusts to use this as an opportunity to rationalise equipment provision and improve equipment utilisation.
Recommendation
An alternative PET-CT provider that is more accessible to North Wales patients should be commissioned
The Regional Imaging Network should provide advice on the preferred option(s) for the provision of PET-CT services to North Wales patients.
North Wales Trust and Breast Test Wales should use the opportunity of equipment replacement to review service requirements.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 22 of 37
7.0 Workforce Planning Although considerable emphasis has been placed on the capital requirements for additional
imaging equipment to increase capacity, it must be understood that the current limiting factor is the workforce. Operating sophisticated diagnostic imaging equipment in a safe and effective manner requires highly trained technical staff. Radiographic staff with appropriate skills are in short supply. Similarly interpreting the images obtained requires specially trained clinical staff and again both radiologists and appropriately trained radiographers are in short supply.
This section aims to identify the staffing requirements for imaging services in North Wales
to meet future demand increases as defined in the document produced by the North Wales Diagnostic Re-Design group. Projections are based on predicted demand increases and cannot reflect unpredicted changes in demand that may ensue over the next 15 years. A series of options is included.
7.1 Background
• Diagnostic Imaging will play a central role in future modern healthcare requiring increased investment in equipment and staff to provide a timely, accurate, patient focused service • Capacity planning has identified the major increases in demand will be in CT, MRI
and Ultrasound • All 3 Trusts in North Wales currently have one CT and one MR scanner. There is a
significant risk as the scanners are a single point of failure (i.e. scanner down time and maintenance result in a loss of the service). Due to the geography of North Wales, this is a not acceptable and a second scanner is needed at each site, in order to sustain an effective emergency/trauma service • Service developments to address new National Service Frameworks and NICE
guidelines have not been considered. 7.2 Current Services
• Current operating hours on weekdays for CT, MRI and Ultrasound for each of the three North Wales Trusts are 08.30/09.00 – 17.00 hours. From April 2007 North East Wales NHS Trust will provide evening sessions for planned CT work. • All three Trusts provide 24/7 emergency cover for General Radiography, CT and
Ultrasound. • C&D Trust provide a 7 day emergency MRI cover for suspected spinal cord
compression until 21.00 hours as agreed with the Radiotherapy Service • NEWT have an extended ultrasound service
7.3 Predicted Growth in Service Demand
This is outlined in detail in the main document and summarised below:

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 23 of 37
7.3.1 MRI
• Predicted increase in demand of 50% by February 2008 requiring extended working outside normal hours (5 sessions). This will be achieved by working longer days and weekend working • This will increase capacity to absorb projected demand and will NOT provide sustainable capacity to reduce waiting times to meet the 2009 Access Targets. • To provide sustainable capacity to meet increased demand and reduce waiting times each Trust will need to purchase and staff an additional MRI scanner by 2008/9
7.3.2 CT
• Historically, a working day split in CT was split into 2 scanning sessions for both radiologists and radiographers (10 sessions per week). The speed of multi-slice CT and modernisation practices have dramatically increased patient throughput, which, added to increased scan complexity, have resulted in an increased reporting workload for radiologists. A session of scanning time now equates to 1.5 sessions of reporting, i.e. 15 reporting sessions for 10 sessions of scanning time per week. This has significant implications for workforce planning.
• Predicted increase in demand of 50% by December 2007 requiring extended working (as above) by the equivalent of 5 sessions (or 7.5 reporting sessions)
• To provide sustainable capacity to meet increased demand and reduce waiting times each Trust will need to purchase and staff an additional CT scanner by 2008/9 The provision of a 2nd MRI and CT scanner at each Trust will address the single point of failure risk 7.3.3 Ultrasound
• Predicted increase in demand of 50% by December 2008 requiring increased scanning capacity which may require extended hours of operation
• To provide sustainable capacity to meet increased demand and reduce waiting times each Trust will need to purchase and staff additional ultrasound scanners by 2008/9 7.4 Additional Staffing Requirements
• It is assumed that the increased demand predictions are correct based on the data available. Projections for North Wales match closely those from elsewhere in the UK
• Staffing levels indicated are for EACH Trust • Assume new consultant radiologists are employed on a 7:3 contract as per the New
Welsh Consultants’ Contract • Agenda-for-change adds 2.5 hours to radiographers’ working week (phased in by
2011). Newly qualified radiographers will be employed on a 37.5 hour week • Non-clinical support staff are not included as levels will be dependant on layout
and design factors
Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 24 of 37
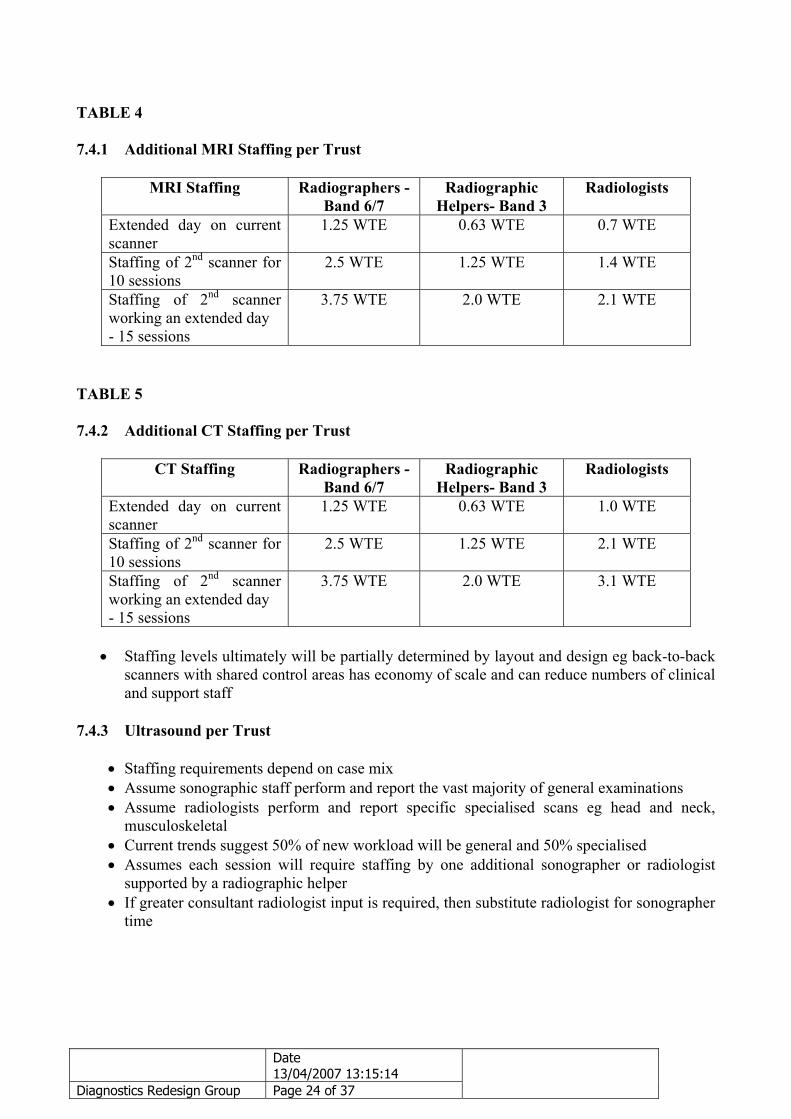
TABLE 4 7.4.1 Additional MRI Staffing per Trust
MRI Staffing Radiographers - Band 6/7
Radiographic Helpers- Band 3
Radiologists
Extended day on current scanner
1.25 WTE 0.63 WTE 0.7 WTE
Staffing of 2nd scanner for 10 sessions
2.5 WTE 1.25 WTE 1.4 WTE
Staffing of 2nd scanner working an extended day - 15 sessions
3.75 WTE 2.0 WTE 2.1 WTE
TABLE 5 7.4.2 Additional CT Staffing per Trust
CT Staffing Radiographers - Band 6/7
Radiographic Helpers- Band 3
Radiologists
Extended day on current scanner
1.25 WTE 0.63 WTE 1.0 WTE
Staffing of 2nd scanner for 10 sessions
2.5 WTE 1.25 WTE 2.1 WTE
Staffing of 2nd scanner working an extended day - 15 sessions
3.75 WTE 2.0 WTE 3.1 WTE
• Staffing levels ultimately will be partially determined by layout and design eg back-to-back
scanners with shared control areas has economy of scale and can reduce numbers of clinical and support staff
7.4.3 Ultrasound per Trust
• Staffing requirements depend on case mix • Assume sonographic staff perform and report the vast majority of general examinations • Assume radiologists perform and report specific specialised scans eg head and neck,
musculoskeletal • Current trends suggest 50% of new workload will be general and 50% specialised • Assumes each session will require staffing by one additional sonographer or radiologist
supported by a radiographic helper • If greater consultant radiologist input is required, then substitute radiologist for sonographer
time

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 25 of 37
TABLE 6 7.4.4 Additional Ultrasound Staffing per Trust
Ultrasound Staffing Radiographers - Band 7
Radiographic Helpers- Band 3
Radiologists
Extended day on one ultrasound scanner
0.63 WTE 0.63 WTE 0.5 WTE
Staffing of an additional scanner for 10 sessions
1.25 WTE 1.25 WTE 0.5 WTE
Staffing of 2nd scanner working an extended day - 15 sessions
2.0 WTE 2.0 WTE 1.0 WTE
Currently, each Trust has numerous ultrasound scanners and there is potential to extend the working day on more than one scanner. If this was the case, the number of helpers would not have to increase at the same rate as the sonographers – one helper could potential support more than one sonographer.
7.5 Skill-Mix
• Healthcare professionals are being asked to redefine and review their roles as it is widely accepted that there will be insufficient numbers of suitably qualified staff to fill the posts in the timeframe being considered • Radiographers have developed their role to report on images and undertake fluoroscopic procedures to allow radiologists to spend more time dealing with the more complex problems • Assistant practitioners are undertaking roles previously performed by radiographers • Medical and clinical disciplines are expanding their roles to include imaging, especially ultrasound. For example, ultrasound is now formally included in the training of urologists. This is placing an additional burden on ultrasound staff to provide the training. • Possible further role extensions may have some impact on the staffing requirements outlined above. • Radiographers may in future report on some of the more straightforward imaging examinations. The time saving to radiologists may become significant although complex cases account for a far greater proportion of reporting time. • Any extension of the Radiographer’s role will require ‘backfilling’ of their traditional role. This may be achieved by assistant practitioners. • There is a significant ‘lag time’ to allow for training staff to fulfil any new role and in many cases this may be several years

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 26 of 37
Recommendation Recommendation Consideration will need to be given to the workforce infrastructure required to support new
models of service delivery, as identified within the sub-groups of the imaging project. Extended hours of service (incorporating extended day and 6/7 day services) will require consideration of the impact of roles across the wider healthcare team, including:
• Reception staff • Portering staff • Secretarial staff • Appointment clerks
Some of the potential additional reception, secretarial and appointment staffing required
will be available from the implementation of PACS. This process has already occurred to varying degrees across the North Wales Trusts.
7.6 Portering Portering is provided to imaging departments through many different models with some
departments employing porters directly and others having to call porters from a hospital wide pool. The ability to access prompt, efficient and reliable portering services is vital to effective utilisation of expensive imaging equipment. All clinical radiology departments have previously reported difficulties with existing portering arrangements.
Recommendation All organisations should review portering arrangements to ensure the delivery of a prompt and efficient portering service 7.7 Medical Physics Medical Physics staff play a vital role in ensuring the safety and effective use of imaging
equipment. In some departments they also play a direct role in providing and / or
The North Wales School of Radiography reviews its SLA to ensure it is aligned with service needs.
The opportunities afforded by training of additional Assistant Practitioners should be fully exploited

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 27 of 37
interpreting imaging tests. A significant increase in the equipment base for diagnostic imaging will require additional resource for medical physics which is provided to North Wales hospitals by the North Wales Medical Physics Service.
Recommendation 5. FINANCIAL CASE 8 Finance and Activity
This section has not yet been signed off by the finance and activity group. As such, the figures remain provisional and may be subject to change. It is included in order to give an indication as to the financial and activity implications of the group’s work.
8.1 Table 2 in section 5.6 sets out the estimated total activity delivered across North Wales by radiology services during 2005/06. 8.2 This activity utilised the following resources amounting to £14.6 million as detailed in table
B. Table B
Radiology expenditure 2005-2006 North West Wales
Conwy & Denbighshire
North East Wales Total
£m £m £m £m Pay 2.728 4.176 4.086 10.99Non Pay 1.336 0.996 1.255 3.587Total 4.064 5.172 5.341 14.577 8.3 Demography Whilst the population of North Wales in total will stay relatively stable over the next twenty years, there will be considerable increase in the number of people over the age of 65. Since older people are the heaviest user of health services this will bring it with increased demand on services. The change in demographic profile is shown in the graph below.
The requirement for Medical Physics Services should be reviewed on a regular basis as diagnostic imaging capacity is increased.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 28 of 37
Estimated and Forecast Population for North Wales
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
2006 2009 2014 2020 2025
Years
Popu
latio
n Fi
gure 0-15
16-64
65-84
85+
This, along with changing clinical practice, will bring with it an increase in demand for services. 8.4 Investment required As set out in section 5.6 above the demand for radiology services is expected to continue to rise year on year at a level greater than that driven purely by the demographic factors set out in 8.3 above. This reflects the increasing importance of early diagnosis in preventing and managing illness.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 29 of 37
TABLE C Scenario 2 growth at mid point of growth estimates
Estimated growth rates
Projected growth rates 2005/06 2006/07 2007/08 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15
Modality Conversion rate Exams Exams Exams Exams Exams Exams Exams Exams Exams ExamsX ray including mobiles and theatres 2 1.1.2 370,313 378,608 376,904 350,200 383,496 386,791 390,088 393,383 396,679 399,975Fluroscopy 1 1.54 24,252 28,861 33,468 38,077 42,927 43,309 43,309 43,309 43,309 43,309Obs % Gyny ultrasound 3 1.09 37,095 37,425 37,755 38,085 38,415 38,745 39,076 39,406 39,736 40,066General ultrasound 4 1.28 60,605 69,696 78,787 87,877 96,968 97,831 98,702 99,580 100,467 101,361CT 1.20 22,297 28,986 35,675 42,364 49,053 49,490 49,930 50,374 50,823 51,275MRI 1.01 10,644 14,689 18,733 22,778 26,823 27,062 27,302 27,545 27,791 28,038RNI 1.41 4,505 4,505 4,505 4,505 4,505 4,505 4,370 4,229 4,088 3,947 The English tariffs at 50% for 2006/07 have been used to estimate the cost impact of this
increasing demand, which is set out in the table below. Resources to fund the additional investment will need to be released by bring forward imaging to earlier in the patient pathway thereby reducing admissions, lengths of stay and outpatients visits.
TABLE D Increment Cost Increases
Average Prices per exam
Projected growth rates 2005/06 2006/07 2007/08 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15
Modality £ £m £m £m £m £m £m £m £m £m £mX ray including mobiles and theatres 2 13 0.00 0.04 0.04 0.04 0.04 0.04 0.04 0.04 0.04 0.04Fluroscopy 1 13 0.00 0.06 0.06 0.06 0.06 0.00 0.00 0.00 0.00 0.00Obs % Gyny ultrasound 3 26 0.00 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01General ultrasound 4 26 0.00 0.24 0.24 0.24 0.24 0.02 0.02 0.02 0.02 0.02CT 63 0.00 0.42 0.42 0.42 0.42 0.03 0.03 0.03 0.03 0.03MRI 97 0.00 0.39 0.39 0.39 0.39 0.02 0.02 0.02 0.02 0.02RNI 29 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00Total 0.00 1.2 1.2 1.2 1.2 0.1 0.1 0.1 0.1 0.1 8.5 Capital Investment The capital investment required to support the recommendations in this report have been included in the North Wales SOP submission in January 2007. 8.6 Conclusion The report has identified the need for investment in radiology services, estimated at £4.1
million to 2015, to underpin the new model of more community based care. This report highlights the financial and activity elements most directly related to the
changes in radiology practice described in this report. However, to get a full picture of the financial implications reference needs to be made to the report of the finance and activity group.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 30 of 37
9 Recommendations Ref
Item
Action
Timescale
5.0 North Wales Context
That the provision of diagnostic imaging services at each level should be based on table 1.
NWHPF April 2006
5.2 Service Strategy
Evidence based care pathways clearly specifying relent imaging tests and their timing should be developed and adopted for all common conditions. The role of the Map of Medicine in achieving the above should be formally investigated. Additional imaging capacity should be based around the three acute level 3 sites as set out in Designed for North Wales.
North Wales Imaging Network North Wales Imaging Network Trusts
Autumn 2007 Autumn 2007 Autumn 2007
5.4 Existing Services
Each trust should agree a formal rolling equipment replacement programme supported by advice from the Regional Imaging Network. Rolling equipment replacement programmes should be adequately resourced across the region.
Trusts LHBs/Trusts
Autumn 2007 Ongoing
5.5 Information Technology
Trusts should consider the need to upgrade to RaDIS 2 system offered by Health Solution Wales. North Wales Trusts and the North Wales Planning Forum should ensure that the specification and procurement of the replacement national RIS is fully compatible with systems in Trust in England and providing services to Welsh patients.
Trusts Trusts
Autumn 2007 Autumn 2007

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 31 of 37
Ref
Item
Action
Timescale
5.6 Capacity Planning
Services should be planned around the following changes in activity detailed in table 3.
NWHPF April 2007
6.1 Interventional Radiology
Extended provision of interventional radiology should be considered using a networked approach.
North Wales Imaging Network
Autumn 2007
6.2 MRI Scanning
MRI capacity in each Trust should be increased by moving to extended working hours. Each acute hospital site should consider, with advice from the Regional Imaging Network, how it will meet future demand additional to that provided by extended working hours.
Trusts Trusts
Autumn 2007 Autumn 2007
6.3 CT Scanning
CT capacity in each Trust should be increased by moving to extended working hours. Each acute hospital site admitting major trauma and/or unselected emergency care patients should have available on suite two multi-slice CT scanners based on clinical risk and forecast demand.
Trusts Trusts
Autumn 2007 Autumn 2007
6.4 Fluoroscopy
Investment in fluoroscopy capacity should reduce in line with decreasing demand. Trusts should not replace fluoroscopy equipment without careful consideration and advice form the Regional Imaging Network. Each Trust should ensure fluoroscopy provision is adequate to support interventional radiology procedures.
Trusts Trusts Trusts
Ongoing Ongoing Ongoing

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 32 of 37
Ref
Item
Action
Timescale
6.5 Nuclear Medicine
At present each Trust will need to maintain nuclear medicine facilities at roughly current levels. The Regional Imaging Network should co-ordinate a network approach to ensure nuclear medicine across North Wales meet clinical governance requirements and that departments in each Trust are appropriately supported by ARSAC licence holders.
Trust R/N
Ongoing Ongoing
6.6 General Radiography
General radiography facilities should be provided in community settings based on population need and access. Such facilities should have direct links to Trust PACS. Busy sites should carefully consider the cost benefit ratio of investing in MR when replacing conventional general radiology equipment.
Trusts Trusts
Ongoing Ongoing
6.7 Ultrasound scanning
Ultrasonongraphy facilities should be provided in community settings based on population need and access. Such facilities should have direct links to Trust PACS. A network approach to the training of other clinicians in ultrsonongraphy should be adopted. This will need to be resourced. That each Trust undertakes a full review of the portfolio of ultrasound equipment in their respective organisation.
Trusts R/N Trusts
Ongoing Ongoing Autumn 2007
6.8 PET CT
An alternative PET CT provider that is more accessible to North Wales patients should be commissioned. The Regional Imaging Network should provide advice on the preferred option (s) for the provision of PET CT services to North Wales patients.
C&D Trust R/N
December 2008 April 2007

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 33 of 37
Ref
Item
Action
Timescale
6.9 Mammography
North Wales Trust and Breast Test Wales should use the opportunity of equipment replacement to review service requirements.
NWWT and BTW
2009
7.5 Skill Mix
The North Wales School of Radiography reviews its SLA to ensure it is aligned with service needs. The opportunities afforded by training of additional Assistant Practitioners should be fully exploited.
NWSR Directors of HR
Autumn 2007 Ongoing
7.6 Portering
All organisations should review portering arrangements to ensure the delivery of a prompt and efficient portering service.
Trusts Autumn 2007
7.7 Medical Physics
The requirement for Medical Physics Services should be reviewed on a regular basis as diagnostic imaging capacity is increased.
Trusts Ongoing

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 34 of 37
Appendix 1 SERVICE RE-DESIGN GROUPS
DIAGNOSTICS
Introduction The group will build upon the vision for services put forward in the consultation document ‘Designed for North Wales’, its supporting work including the benchmarking against UK best practice undertaken by Teamwork. It will develop a sufficiently detailed picture of services to inform the Regional Strategic Outline Plan and the local health economy Strategic Outline Cases. The work of the group will inform the regional chronic disease management plan to be submitted as part of the delivery programme for Designed for Life. Terms Of Reference The group needs to look at services for diagnostics in the round but it will focus particularly on
1. To link closely with the work of the national and regional radiology networks. 2. The facilitation of long-term condition management in the community. 3. The facilitation of optimising the use of day surgery and minor outpatient
procedures. 4. Minimising the number of visits to a hospital site for diagnostic tests. 5. Minimising the duplication in tests/screening. 6. Exploiting the potential offered by IT developments 7. The groups work needs to link to the Access 2009 work (but not to duplicate it). 8. The need to shorten patient pathways. 9. The exploration of models of diagnostic delivery eg out of hours, planned and
unplanned work. Timescale The group needs to produce work to inform
1 The Strategic Outline Plan – final report by the 31st October 2006. 2 Three health economies Strategic Outline Cases estimated date for completion
the 31st March 2007. 3 The regional Chronic Disease Management Plan due for completion by the
31st March 2007.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 35 of 37
Meetings The first meeting will take place on the 11th September at 5 pm in the Boardroom, Glan Clwyd.

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 36 of 37
Appendix 2
DIAGNOSTICS SERVICE REDESIGN GROUP Name Title Organisation Dr David Gozzard - Chair Medical Director Conwy and Denbighshire Geoff Lang Chief Executive Wrexham LHB Robin Wigg Directorate
Manager North East Wales NHS Trust
Mr Adrian Thomas Directorate Manager
Conwy and Denbighshire NHS Trust
Ms Tina Bailey Directorate Manager
North West Wales NHS Trust
Dr N Looker NPHS Glanville Owen CHC representative Mrs P Nash CHC representative David Owen CHC representative Radiology Dr Paul Birch – Sub Group Chair
Clinical Director North West Wales NHS Trust
Dr Catrin Barwick Consultant North West Wales NHS Trust Dr R Byrne Consultant Conwy and Denbighshire NHS
Trust Dr David Parker Consultant North East Wales NHS Trust Dr Malcolm Greensmith Clinical Director North East Wales NHS Trust Mrs Bethan Wynn Owen Radiology Services
Manager Conwy and Denbighshire NHS Trust
Mrs Helen Hughes Imaging Manager North East Wales NHS Trust Mrs Jill Newman Modernisation
Manger North East Wales NHS Trust
Mrs Pat Youds Modernisation Manager
Conwy and Denbighshire NHS Trust
Colin Heath North West Wales NHS Trust David Nuttall Conwy and Denbighshire NHS
Trust

Date 13/04/2007 13:15:14
Diagnostics Redesign Group Page 37 of 37
Appendix 3
Acronyms Acronyms
Meaning
CT Computed Tomography D4L Designed for Life HSW Health Solution Wales LDP Local Delivery Plan MRI Magnetic Resonance Imaging NICE National Institute of Clinical Effectiveness NLIAH National Leadership Innovation Agency for
Healthcare PACS Picture Archiving and Communication System RIS Radiology Information System SOP Strategic Outline Plan WHC Welsh Health Circular WTE Whole Time Equalivents