final framework of outcomes for intern training in … · 2015-11-20 · executive summary the...
TRANSCRIPT

1 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
DraftFrameworkofOutcomesforInternTraininginIreland
By
Boland,J.O’Connor,P.,Offiah,G.,Byrne,D.
DocDaingeanTeoranta,Galway
CommissionedbytheMedicalCouncil
October2015

2 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
ExecutiveSummaryTheinternyearisthefirstyearofclinicalpracticefollowinggraduationfrommedicalschoolandisakeypointinthetransitionfromstudenttodoctor.Uponsatisfactorycompletionoftheinternyear,theMedicalCouncilissueaCertificateofExperienceandthisallowsprogressiontothegeneralorspecialisttraineeregister.InternshipisanimportantyearinthecontinuumofmedicaleducationandassurancesthataninternhasachievedcompetenciesrequiredtoprogresstothenextleveloftrainingarerequiredbytheMedicalCouncilandotherstakeholdersincludingtheinternnetworks,postgraduatetrainingbodies,patientsandthepublic.
In2009,withtheestablishmentofinterntrainingnetworksinIreland,theNationalInternTrainingProgrammewasdeveloped.TheNationalInternTrainingProgramme(2011)outlinesthecurriculum,standardsfortrainingandrequirementsforcertification.TheInternCurriculumisaccompaniedbyaNationalInternAssessmentFormcompletedbyclinicalsupervisorsandaligningwiththethreecoremodulesdescribedintheInternCurriculumdocument:(i)clinicaljudgment;(ii)professionaldevelopment;and(iii)communication.Atthetimeofwriting,internshiptraininginIrelandcanbebestdescribedasatimebasedapprenticeshipmodel.
TheinternyearrequiresreforminordertoalignitwithinternationalequivalentsandtoensurethattheissuingofaCertificateofExperience(CoE)isbasedontheachievementofaminimumlevelofcompetencytoensurepatientsafety.Competency-basedmedicaleducation(CBME)hasbeenadoptedinternationallytobringclarityandtransparencytoexpectationsregardingknowledge,skills,attitudesandthebehavioursnecessaryforeffectiveandsafepractice.Themovetowardsacompetencybasedframeworkisalsoaprerequisiteforcurriculumreformtoensurecomparabilityacrossinternnetworksintheeducationalexperienceandinworkbasedassessment,usingprocessessuchascurriculummappingandassessmentblueprinting.
HavingidentifiedtheneedforCBME,theprojecttodeviseadraftframeworkforoutcomesforinterntrainingwascommissionedbytheMedicalCouncil.Buildingonareviewofinterntrainingandanalysisofneedswithinthesectoranddrawingoninternationalpracticeandliterature,EntrustableProfessionalActivities(EPAs)wereadoptedastheorganisingframeworkforcompetenciesrequiredforeffectiveandsafepracticebyinternsinIrelandattheendoftheirtraining(seeAppendixE).
ThegroupingofcompetenciesintoanEPAframeworktranslateswellintoaone-yeartrainingprogrammeasitorganisescompetenciesintounitsofworkor“professionalactivities”.AnEPAisacoreunitofprofessionalpracticethatcanbefullyentrustedtoatraineeassoonasheorshehasdemonstratedthenecessarycompetencetoexecutetheactivityunsupervised.
TheseEPAsweredevelopedbyagroupofwell-informedstakeholdersandvalidatedbyalargergroup.TheseEPAswillrequirevalidationbyawidergroup.Beyondthescopeofthisreport,butrequiringconsideration,ishowdefinedcompetenciescanshapethedeliveryofanationaltrainingprogramme;howwecandeterminethatcompetencieshavebeenbeachieved;therolethatstakeholderswillhaveinenablinginternstoachievecompetenciesandhowthesestakeholderswillbesupported.Furthermore,significantinvestmentwillberequiredtosupporttheinfrastructureandinformationtechnologyrequiredtodeliveraworkinganduseablecompetencybasedframeworkthatcanmonitorinterns’progress,facilitatethecompletionofworkbasedassessmentsandsupportthecompilationofresults.

3 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
Contents
No. Section
Page
1. Introduction 4
2. NeedsAnalysis-Ireland 5
3. AppraisalofReferenceSystemsforInternship 7
4. EntrustableProfessionalActivities 8
5. ProcessofDevelopingEPAsforEndofInternship(Irl) 13
6. ValidationProcess 17
7. ForConsideration 21
Bibliography
TeamBiographies
Appendices
A. TheNationalInternEducationandTrainingAgreement(NIETA)B. NationalInternAssessmentFormC. MedicalCouncilEightDomainsofGoodProfessionalPracticeD. EntrustableProfessionalActivitiesfromOtherContextsE. DraftFrameworkofEPAsforEndofInternship(Irl)

4 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
1. Introduction
1.1 Background:
Theinternyearisakeypointoftransitionfromstudenttodoctoralongthecontinuumofmedicaleducation.In2015,theMedicalCouncilisfocusingonthequalityofinterntraininginIreland.TheMedicalCouncil’s“YourTrainingCountsReport”of2014identifiedareasforimprovementintheinternyearandtheInternNetworksExecutiveiscommittedtocurriculumreformandthedeliveryofconsistent,qualityeducationandtrainingprogrammesacrossthenetworks.Anysubsequentreformofinterntrainingneedstobebasedonclearunderstandingofwhatistobeachievedanddemonstratedbythetraineeattheendofinternship.Clarityaroundthe“signing-off“processthatcurrentlyexistsisrequiredforqualityassuranceandfortheissuanceofaCertificateofExperience(CoE)bytheMedicalCounciluponsuccessfulcompletionoftheyear,enablingthetraineetoprogresstogeneralorspecialisttraineeregistration.
1.2 MedicalCouncilspecificobjectives:
ThisreporthasbeenpreparedattherequestoftheMedicalCouncil.Thespecificobjectiveswereto:
• EstablishandappraisethecurrentapproachtodefinitionoflearningoutcomesforinterntraininginIreland
• Appraiseapproachestooutcomesforinterntraininginasmallsetofnamed“reference”healthsystems(UK,NewZealand,Australia,CanadaandtheUS)
o includingthemerits[orotherwise]ofEntrustableProfessionalActivities(EPA)• Deviseadraftframeworkofoutcomesforinterntraining(Irl)
o makerecommendationsforimplementationo reasonableassurancethatdefinedoutcomeshavebeenachievedleadingtoissue
ofCoEbytheMedicalCouncil
1.3 Tenderbrief:
Inpreparingthisreport,theteamcarriedoutathoroughreviewofthedocumentsrelatingtostandardsandtrainingofinterns(orequivalent)intheIrishcontextandinternationally.Infulfilmentofthebrief,theteamdevisedadraftframeworkofoutcomesforinterntraininginIrelandtakingaccountof:
• goodpracticeinoutcome-basedmedicaleducationandtraining;• thecurrentstateofinterntraininginIreland;and• contextoftheIrishhealthsystem
Thisdraftreportissubjecttoconsultation,finalisationandimplementationbytheMedicalCouncil.

5 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
1.4 Overviewofphasesoftheproject:
Phase1: Carryoutaneedsassessmentofoutcomesforinterntraining
Phase2: Establishcompetenciesandoutcomes
Phase3: Makerecommendationsforimplementationandassessmentstrategies
Phase4: DesignafirstdraftframeworkforreviewinconsultationwithMedicalCouncil
Postproject:
Phase5: PrepareadraftframeworkfollowingreviewandconsultationbytheMedicalCouncil
Phase6: Consultation,recommendationsandimplementationbytheMedicalCouncil
2. Needsanalysis
2.1 Methodology:
Inperformingtheneedsanalysis,theteamperformedanextensivereviewofthecurrentIrishinternshipandNationalInternTrainingProgrammeandofsimilarsystemsfromotherjurisdictions,namelyUK,NewZealand,Australia,CanadaandtheUS,takingintoconsiderationthefollowingrequirements:
• AsetofcompetenciesisrequiredtoissueaCoE,acknowledgingthatitishighstakesandatraineecannotprogresstothespecialistorgeneralregisterwithoutit
• Aframeworkisrequiredforthedesignofo locallydevisededucationandtrainingprogrammeso workbasedassessment
• Aqualityassurancesystemisnecessaryforallstakeholders(MedicalCouncil,InternNetworks,clinicalandeducationalsupervisorsandpostgraduatetrainingbodies,patientsandthepublic)
• Atransparentmethodthatidentifiestraineeswhorequiresupportisrequiredforfeedbackanddocumentationpurposesandtoimplementremediation/extensionofinternshipasrequired
IndevisingaframeworkofoutcomesforinternshipinIreland,theframeworkmustalsotakeintoaccounttheimplementationrequirementsthatwillfollow:
• Theadministrationandmanagementofaconsistentnationalprogramme• Theprovisionoflearningopportunitiestoachievecompetencies• Themanpower,trainingandsupportrequiredtofacilitateworkbasedassessment• Thetimerequiredtoimplementsuchasystem• Theadditionalworkloaddemandsonclinicalandeducationalsupervisors• Thetechnologytosupportdesign,implementation,deliveryandassessment• Themechanismforprogrammereviewandadaptationtothechanginghealthcare
environment

6 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
2.2 Ireland–CurrentNationalInternTrainingProgramme(NITP)overview:
InIreland,internshipis12monthsandconsistsoffour3-monthrotations.TheeligibilitycriteriaforapplicationforinternshipinIrelandaredeterminedbytheDepartmentofHealth,HealthServiceExecutive(HSE)andNationalRecruitmentServiceHSE.Currentlythereare727one-yearinternpostsinsixInternNetworks(2015)centeredaroundthesixmedicalschools.EachInternNetworkisoverseenbyoneInternCoordinatorandinterntutors/lecturersateachtrainingsite.Mostinternrotationsareingeneralhospitals,withasmallnumberingeneralpractice(11)andafewinspecialisedunits(e.g.orthopaedics,rheumatology,psychiatry).
Uponcompletionofinternshipalistofnamedinternswhohavebeen“signedoff”(seebelowforprocess)bytheirinternnetworkissentbytheInternCoordinatorstotheMedicalCouncilwhothenissuetheCoEtotheinternsonthelist.
Atthetimeofwriting,internshiptraininginIrelandcanbebestdescribedasatimebasedapprenticeshipmodel.
Therequirementsandstandardsforinterneducationandtrainingareoutlinedinthefollowingdocuments:
• StandardsforTrainingandExperienceRequiredforGrantingofaCertificateofExperience2011(https://www.medicalcouncil.ie/Education/Career-Stage-Intern/Standards-of-training.pdf)
• GuidelinesforMedicalEducationandTrainingforInterns2011(https://www.medicalcouncil.ie/Education/Career-Stage-Undergraduate/Your-Questions-Answered/Guidelines-on-Medical-Education-and-Training.pdf)
• NationalInternTrainingProgramme(NITP)InternCurriculum2011(http://www.medicalcouncil.ie/Education/Career-Stage-Intern/National-Intern-Training-Programme-.pdf)
• TheNITPInternCurriculumisorganisedaroundtheMedicalCouncil’s8domainsofGoodProfessionalPractice(seeAppendixC),intothreemodules:
o clinicaljudgmento professionaldevelopmento communication
• TheNationalInternEducationandTrainingAgreement(NIETA)(seeAppendixA)is
signedbyeachinternatthebeginningofinternshipanditoutlinestheeducationalrequirements(prescribedcoursesandworkshopsthatmustbeattended,e.g.ACLS,proceduralskillstrainingworkshops)foreachinterntoachieve“signoff”bythenetwork.
2.3 Ireland–NationalInternTrainingProgramme(NITP)-Currentassessmentprocess:
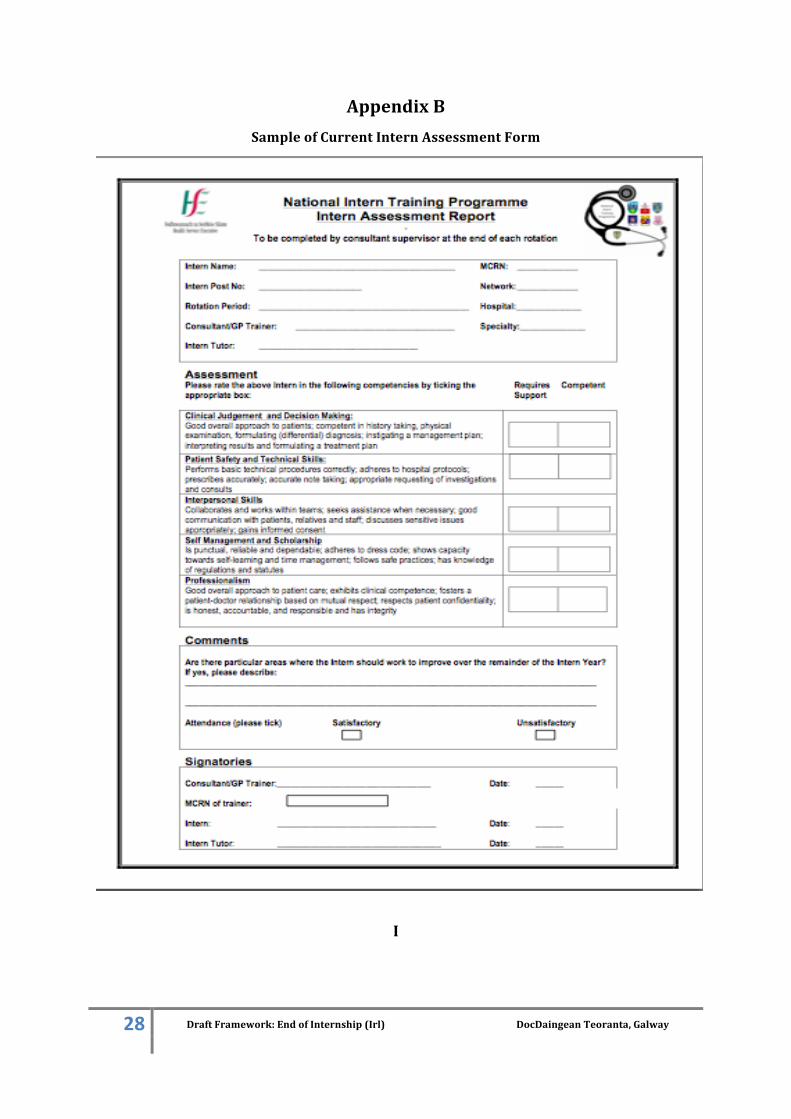
ANationalInternTrainingProgrammeAssessmentForm(seeAppendixB)iscompletedbytheclinicalsupervisorattheendofeachrotationandsignedbytheinterntutor/coordinator.The
7 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
assessmentformrequirestheclinicalsupervisortorecordtheinternas“competent”or“requiringsupport”infiveareasbroadlyrelatedtotheMedicalCouncil’s8DomainsofGoodProfessionalPracticeandtheInternCurriculum’sthreemodules.
Insummary,therequirementsforaninterntobe“signedoff”attheendofinternshipandsubsequentlybeissuedwithaCoEbytheMedicalCouncilare:
• FoursatisfactoryNITPassessmentforms• Evidenceofattendanceatanetworks’prescribedrequirementsforteaching/courses
outlinedintheNIETAdocument
Currentlytherearenoe-portfolios,technologytosupporttheeducationalprogramme,centraladministrativeorganization/bodyorworkbasedassessmentsinuseandtheassessmentformsarepaperbased.
3.Appraisalofreferencesystemsforinternship
3.1 Referencesystems:
Specificinternationalsystemsandprogrammeswereidentifiedforappraisalinthetermsofreferenceforthisproject.Theywere:
(i) UnitedKingdom(FoundationProgrammeF1andF2)www.foundationprogramme.nhs.uk/
(ii) NewZealand(Pre-VocationalYear1)https://www.mcnz.org.nz/news-and-publications/prevocational-training/
(iii) AustralianInternshiphttp://www.amc.org.au/accreditation/prevoc-standards
(iv) Canadian(PGY1)Note:MDgraduatesproceeddirectlyintoresidencywithoutaninternshipstephttp://www.carms.ca/en/
3.1 Summaryoftheappraisalofthereferencesystems:
Theaboveprogrammesareofoneortwoyearsdurationandarecompetencybased.Outcomesandcompetenciesareclearlydefinedandaregroupedinavarietyofwaysforclarity.Therearebetween20(Australia)and397(UK)competenciesdefined.Thesecompetenciesaremappedtorolesordomainsdefinedbymedicalcouncilsorsimilargoverningortrainingbodies.Competenciescanbemapped,forexample,topredefineddomainssuchasscholarship,communication,professionalism,skills,safetyandmanagement.Allofthereferencedinternationalsystemshaveverydetailedprogrammeoperationaldocumentsinplacesuchasorganisationaldocuments,curriculumdocumentsandintendedoutcomesdocuments.Largeprogrammeoffices,operationalsupportsandstaffareinplacewithdefinedroles(i.e.programmeadministrators,clinicalsupervisors,educationalsupervisors,tutorsetc.)toadministeranddelivertheprogramme.Furthermore,theassociatedworkbasedassessmentprogrammeanddocumentationthatcomeswithacompetencybasedprogrammeissupported

8 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
byanITteam,programmeofficeandcomplexadministrativeplatforms;inmostcasesviaane-portfoliothatiscompatiblewithallmobiledevices.Theprogrammesarereviewedonaregular(annualorbiennial)basisandadjustedtoalignwithchanginghealthcaredemands.
4. EntrustableProfessionalActivities
4.1 EntrustableProfessionalActivitiesasaresponsetochallengesofimplementingcompetencybasedmedicaleducation:
Thetermsofreferenceforthestudydescribedinthisreportincludeappraisingapproachestooutcomesforinterntrainingincludingthemerits[orotherwise]ofEntrustableProfessionalActivities(EPA).
Competencybasedmedicaleducation(CBME)hasbeenadoptedinternationallytobringclarityandtransparencytoexpectationsregardingtheknowledge,skills,attitudesandbehaviournecessaryforeffectiveandsafepractice(Mulderetal,2010;Chenetal,2015).Competencybasedmedicaleducationhasbeendescribedasanapproachtopreparingphysiciansforpracticethatisfundamentallyorientatedtowardsgraduateoutcomesandabilities.Itisorganisedaroundcompetenciesderivedfromananalysisofsocietalandpatientneeds.Itde-emphasisestime-basedtrainingandpromisesgreateraccountability,flexibilityandlearnercentredness(Franketal,2010).Theprocessofimplementingacompetencybasedtrainingprogramme,however,hasprovedchallenginginternationally,becauseofdifficultiesintranslatingcompetenciesintopracticeandinthedesignofarobustassessmentsystem.
ChallengesassociatedwithimplementingCBME
• Competenciesareoftenverybroadlydefined• Sub-competencedescriptionsaretooanalytical• Riskoftick-boxapproachtoassessment• Riskofinstrumentalistlearning• Onerouslevelofpaperworkandbureaucracy• Disconnectednessfromclinicalpractice
ItisinthiscontextthattheconceptofEntrustableProfessionalActivities(EPAs)hasdevelopedandgainedgroundinrecentyearsinbothundergraduateandpostgraduatetraining(Aylwardetal,2014;EnglanderR.,2014,Gilhooltetal,2014;Rachid,2015).AnEntrustableProfessionalActivityisacoreunitofprofessionalpracticethatcanbefullyentrustedtoatraineeassoonasheorshehasdemonstratedthenecessarycompetencetoexecutetheactivityunsupervised(tenCate,O.etal,2015).EPAsaddresssomeoftheoperationalissuesassociatedwiththeimplementationofcompetencyframeworks.Themodelprovesintuitivetocliniciansasmuchoftheirworkcanbecapturedbytasksorresponsibilitiesthatcanbeentrustedtoindividuals,withdefinedlevelsofsupervision,fromnovicethroughtoindependentpractice.

9 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
EntrustableProfessionalActivities:
• aredescriptorsofwork(inaclinicalsetting),ratherthanattributesofadoctor
• requireintegrationofmultiplecompetenciesacrossarangeofdomains
• provideameansoftranslatingcompetenciesintoclinicalpractice
• involvestatingthelevelofproficiencyexpected• providethebasisforwork-basedassessment
4.2 RelationshipbetweencompetencyandEPAs:
TherelationshipbetweencompetencyandEPAshasbeensubjecttoconsiderablescrutiny.OneofthereferencesystemsreviewedforthisstudywastheAmericanAssociationofMedicalColleges(2014)“CoreEntrustableProfessionalActivitiesforEnteringResidency”.Agreeingaconceptualframeworkinvolvedgainingconsensusonshareddefinitionsfor:
1.Competency:Anobservableabilityofahealthprofessional,integratingmultiplecomponentssuchasknowledge,skills,valuesandattitudes.Sincecompetenciesareobservable,theycanbemeasuredandassessedtoensuretheiracquisition.
2.EntrustableProfessionalActivity(EPA):EPAsareunitsofprofessionalpractice,definedastasksorresponsibilitiesthattraineesareentrustedtoperformunsupervisedoncetheyhaveattainedsufficientspecificcompetence.EPAsareindependentlyexecutable,observableandmeasurableintheirprocessandoutcome,andarethereforesuitableforentrustmentdecisions.
ThedistinctionbetweenEPAsandcompetencieshasbeendescribedbytenCateasfollows:
Competencies EPA
PersondescriptorsKnowledge,skill,attitudes,values
WorkdescriptorsEssentialtaskinprofessionalpractice
e.g.Contentexpertise
CommunicationabilityManagementabilityProfessionalattitude
Scholarship
e.g.DischargeapatientCounselapatient
LeadafamilymeetingDesignatreatmentplanLeadaresuscitation
AnumberofwritershaveemphasisedthatEPAsandcompetenciesarenotmutuallyexclusive.Onthecontrary,EPAs,bydefinition,requiresuccessfulintegrationofarangeofcompetencies.Thesecompetenciesarebestassessedinthecontextofspecificperformance,asprovidedforby
10 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
anEPAframework.WhiletenCatesuggeststhatgeneralcompetenciesarethefocusofmostgoverningbodiesandeducationalleadersresponsibleforphysiciantraining,
“itisnotnecessarytochoosebetweencompetenciesandactivities.Rather,byacknowledgingthatbotharerelevantpiecesofthetrainingprocessandthateachrepresentsadifferentdimensionofthesameoverallobjectiveofprofessionaltraining,wecanreconciletheconceptsofcompetenceandclinicalpractice.”
tenCateandScheele,2007
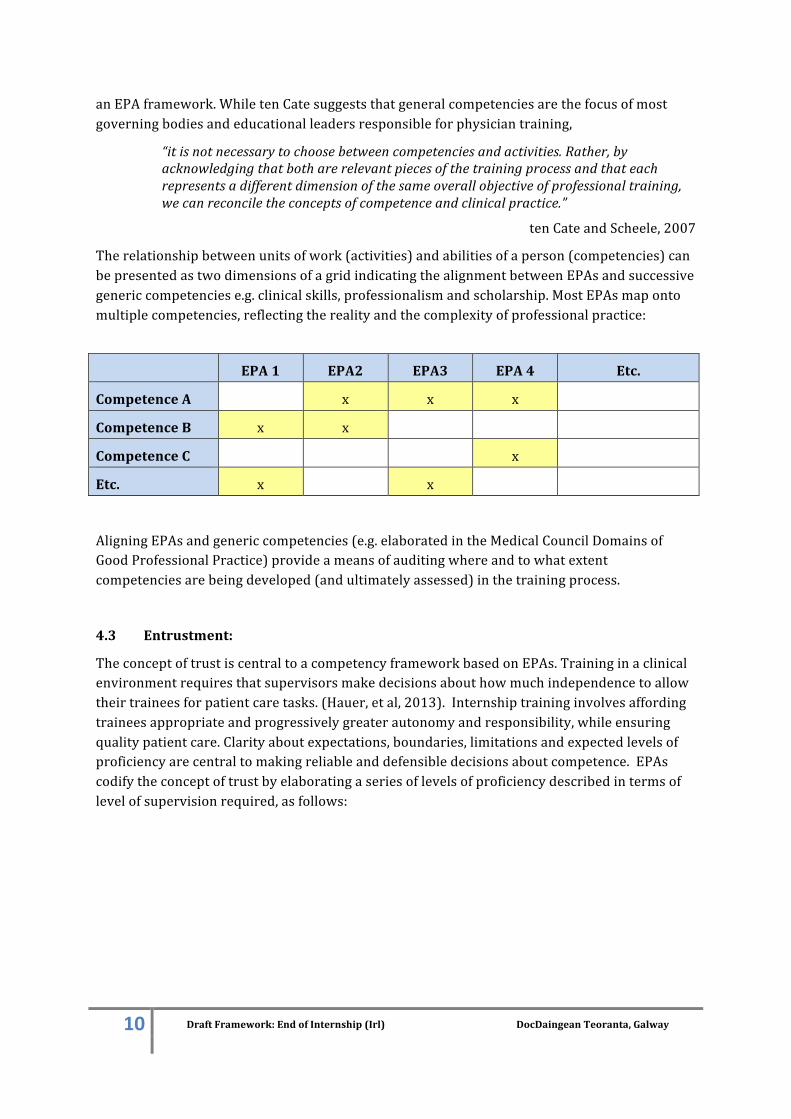
Therelationshipbetweenunitsofwork(activities)andabilitiesofaperson(competencies)canbepresentedastwodimensionsofagridindicatingthealignmentbetweenEPAsandsuccessivegenericcompetenciese.g.clinicalskills,professionalismandscholarship.MostEPAsmapontomultiplecompetencies,reflectingtherealityandthecomplexityofprofessionalpractice:
EPA1 EPA2 EPA3 EPA4 Etc.
CompetenceA x x x
CompetenceB x x
CompetenceC x
Etc. x x
AligningEPAsandgenericcompetencies(e.g.elaboratedintheMedicalCouncilDomainsofGoodProfessionalPractice)provideameansofauditingwhereandtowhatextentcompetenciesarebeingdeveloped(andultimatelyassessed)inthetrainingprocess.
4.3 Entrustment:
TheconceptoftrustiscentraltoacompetencyframeworkbasedonEPAs.Traininginaclinicalenvironmentrequiresthatsupervisorsmakedecisionsabouthowmuchindependencetoallowtheirtraineesforpatientcaretasks.(Hauer,etal,2013).Internshiptraininginvolvesaffordingtraineesappropriateandprogressivelygreaterautonomyandresponsibility,whileensuringqualitypatientcare.Clarityaboutexpectations,boundaries,limitationsandexpectedlevelsofproficiencyarecentraltomakingreliableanddefensibledecisionsaboutcompetence.EPAscodifytheconceptoftrustbyelaboratingaseriesoflevelsofproficiencydescribedintermsoflevelofsupervisionrequired,asfollows:

11 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
Level Proficiency-levelof‘entrustability’
1Hasacquiredknowledgeandskills,butinsufficienttoperform;notallowedtoenacttheEPA
2Mayperformanactivityunderfull,proactivesupervisioninthesameroom;thesupervisordecidestheintensityofsupervision
3Mayperformanactivityunderqualified,reactivesupervision;thetrainee(intern)asksforsupervision
4Mayperformanactivityindependentlywithbackstage,mainlyinformalsupervision
5Mayprovidesupervisionandinstructiontojuniorlearners
4.4 Overviewofmeritsandlimitations:
TherelativebenefitsandlimitationsofEPAsandcompetencieshavebeensummarisedbytheAssociationofAmericanMedicalColleges(AAMC,2014)asfollows:

12 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
Buildingonourreviewofinterntrainingandanalysisofneedswithinthesector,anddrawingoninternationalpracticeandliterature,EPAswereadoptedastheorganisingframeworkforcompetencesrequiredforeffectiveandsafepracticebyinternsattheendoftheirtraining.Finally,oneofthepromisingfeaturesofanEPAapproachinanysinglecontext(e.g.enteringresidencyorinternship)isthepotentialithasforshapingrequirementsatpreviousandsuccessivestageswithinthecontinuumofmedicaleducationandtraining.ThisrelationshiphasbeenrepresentedbytheAAMC(2014)asfollows:
MakingexpectationsforinternshipinIrelandmoreexplicit,intermsofcoreEPAshasthepotentialforinformingexpectationsofundergraduateprogrammes.
13 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
5. DevelopingendofinternshipEPAsforIreland
5.1 AnEPAtemplate:
ThefirststageintheprocesswastodevelopabespoketemplatewithguidelinesforEPAdevelopers.DrawingonguidelinesfromtheinternationalliteratureandexistingpracticeinIreland,(tenCate,2014,tenCate,2015,AAMC,2014)anEPAtemplatefordevelopmentofEPAsatendofinternshipwasdraftedandrefined.
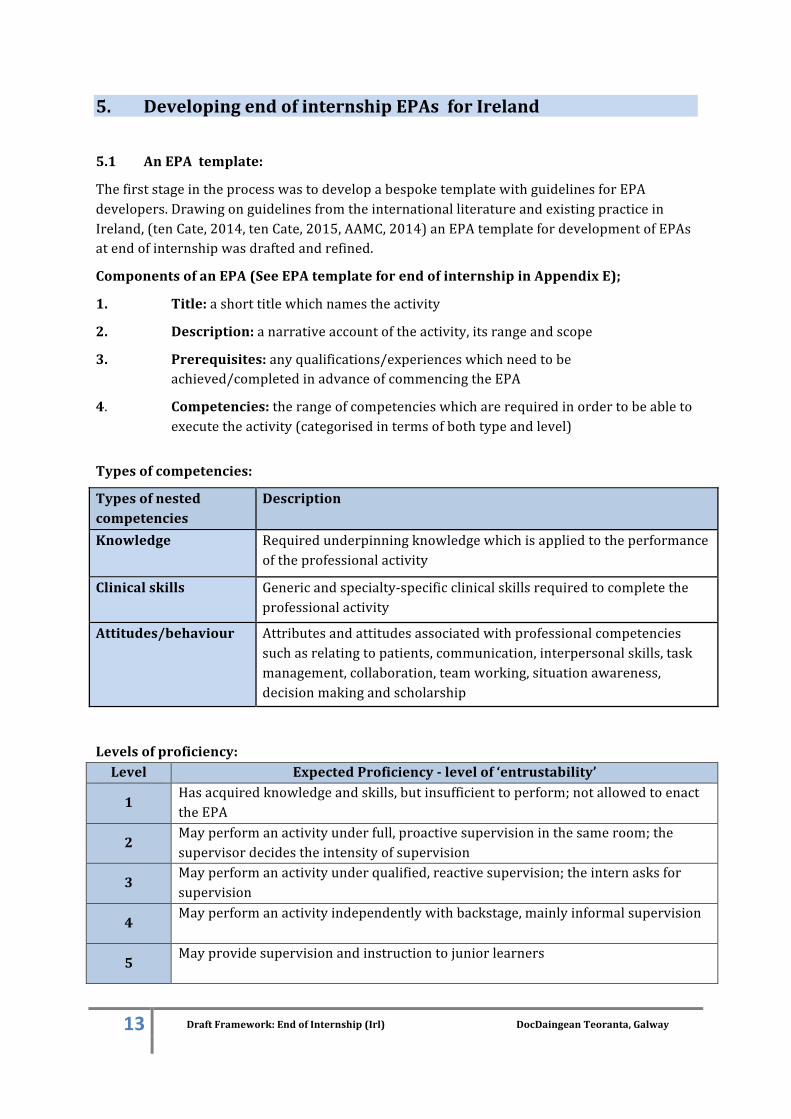
ComponentsofanEPA(SeeEPAtemplateforendofinternshipinAppendixE);
1. Title:ashorttitlewhichnamestheactivity
2. Description:anarrativeaccountoftheactivity,itsrangeandscope
3. Prerequisites:anyqualifications/experienceswhichneedtobeachieved/completedinadvanceofcommencingtheEPA
4. Competencies:therangeofcompetencieswhicharerequiredinordertobeabletoexecutetheactivity(categorisedintermsofbothtypeandlevel)
Typesofcompetencies:
Typesofnestedcompetencies
Description
Knowledge Requiredunderpinningknowledgewhichisappliedtotheperformanceoftheprofessionalactivity
Clinicalskills Genericandspecialty-specificclinicalskillsrequiredtocompletetheprofessionalactivity
Attitudes/behaviour Attributesandattitudesassociatedwithprofessionalcompetenciessuchasrelatingtopatients,communication,interpersonalskills,taskmanagement,collaboration,teamworking,situationawareness,decisionmakingandscholarship
Levelsofproficiency:Level ExpectedProficiency-levelof‘entrustability’
1Hasacquiredknowledgeandskills,butinsufficienttoperform;notallowedtoenacttheEPA
2Mayperformanactivityunderfull,proactivesupervisioninthesameroom;thesupervisordecidestheintensityofsupervision
3Mayperformanactivityunderqualified,reactivesupervision;theinternasksforsupervision
4Mayperformanactivityindependentlywithbackstage,mainlyinformalsupervision
5Mayprovidesupervisionandinstructiontojuniorlearners
14 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
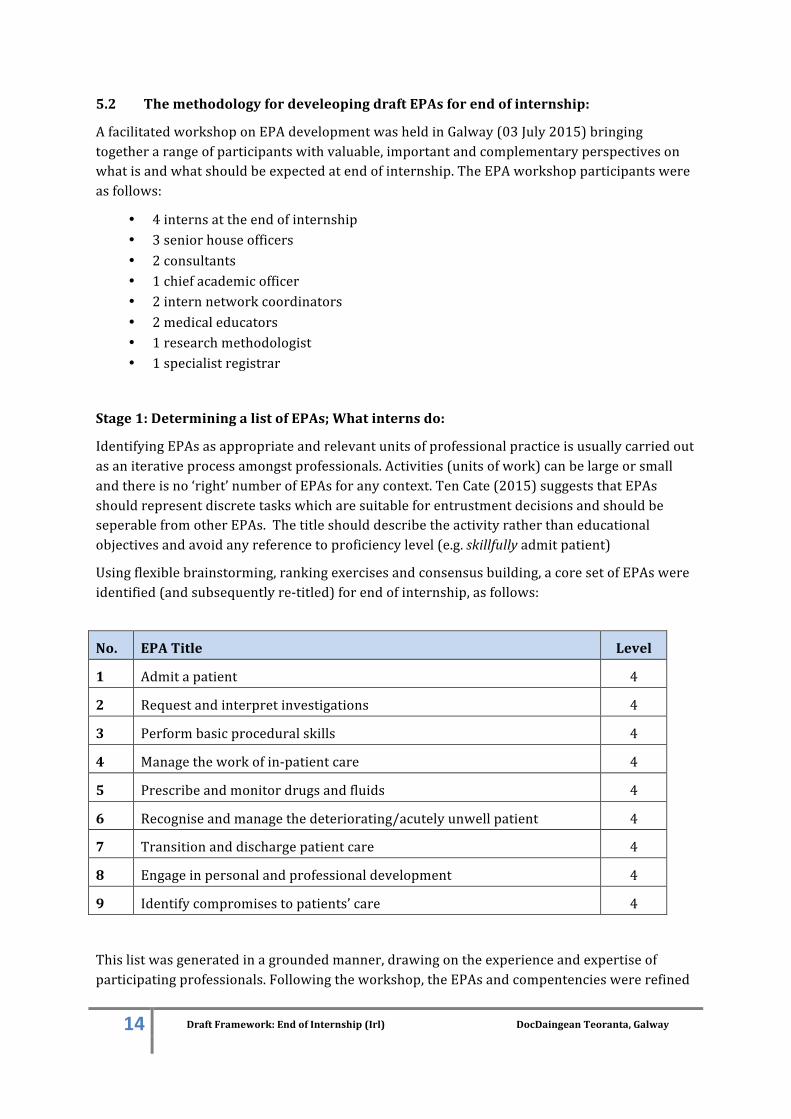
5.2 ThemethodologyfordeveleopingdraftEPAsforendofinternship:
AfacilitatedworkshoponEPAdevelopmentwasheldinGalway(03July2015)bringingtogetherarangeofparticipantswithvaluable,importantandcomplementaryperspectivesonwhatisandwhatshouldbeexpectedatendofinternship.TheEPAworkshopparticipantswereasfollows:
• 4internsattheendofinternship• 3seniorhouseofficers• 2consultants• 1chiefacademicofficer• 2internnetworkcoordinators• 2medicaleducators• 1researchmethodologist• 1specialistregistrar
Stage1:DeterminingalistofEPAs;Whatinternsdo:
IdentifyingEPAsasappropriateandrelevantunitsofprofessionalpracticeisusuallycarriedoutasaniterativeprocessamongstprofessionals.Activities(unitsofwork)canbelargeorsmallandthereisno‘right’numberofEPAsforanycontext.TenCate(2015)suggeststhatEPAsshouldrepresentdiscretetaskswhicharesuitableforentrustmentdecisionsandshouldbeseperablefromotherEPAs.Thetitleshoulddescribetheactivityratherthaneducationalobjectivesandavoidanyreferencetoproficiencylevel(e.g.skillfullyadmitpatient)
Usingflexiblebrainstorming,rankingexercisesandconsensusbuilding,acoresetofEPAswereidentified(andsubsequentlyre-titled)forendofinternship,asfollows:
No. EPATitle Level
1 Admitapatient 4
2 Requestandinterpretinvestigations 4
3 Performbasicproceduralskills 4
4 Managetheworkofin-patientcare 4
5 Prescribeandmonitordrugsandfluids 4
6 Recogniseandmanagethedeteriorating/acutelyunwellpatient 4
7 Transitionanddischargepatientcare 4
8 Engageinpersonalandprofessionaldevelopment 4
9 Identifycompromisestopatients’care 4
Thislistwasgeneratedinagroundedmanner,drawingontheexperienceandexpertiseofparticipatingprofessionals.Followingtheworkshop,theEPAsandcompentencieswererefined

15 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
bythereportauthorsandauditedagainstthetwomostcomparableEPAframeworks(EPAsidentifiedbytheAAMCforendofresidencyandthepan-CanadianEPAsforendofclerkship-seeAppendixD).Morecommonalitiesthandifferencescanbediscerned.CertainAAMCEPAshavebeensubsumedwithinEPAsfortheIrishframeworke.g.competencesassociatedwithEPA10(AAMC)“obtaininginformedconsent”areincludedinEPA1(Irl)“admittingapatient”.
AllEPAsfortheendofinternshipinIrelandweredesignatedasLevel4,reflectingthelevelofresponsibilityaffordedi.e.internsshouldbeabletoperformtheactivitiesindependentlywithbackstage,mainlyinformalsupervision.
Stage2:DraftingindividualEPAs:
Smallgroupsof2-3participantsworkedoneachEPAtoprepareadraftincluding:
• EPAnarrativedescription• Competencies(knowledge,skillsandattitudes/behaviour)• Proficiencylevelforeachcompetence
SomecompetencieswithinindividualEPAsweredesignatedatalevelotherthanlevel4,whereappropriate;level3whereahigherlevelofsupervisionwasrequired(qualified,reactivesupervisionwheretheinternasksforsupervision)orlevel5whereitwasdeemedreasonabletoexpectinternstoprovidesupervisionandinstructiontojuniorlearnerse.g.medicalstudents.(seeAppendixEfordetailsofeachEPA.)
Stage3:AligningEPAswithMedicalCouncilDomainsofGoodProfessionalPractice:
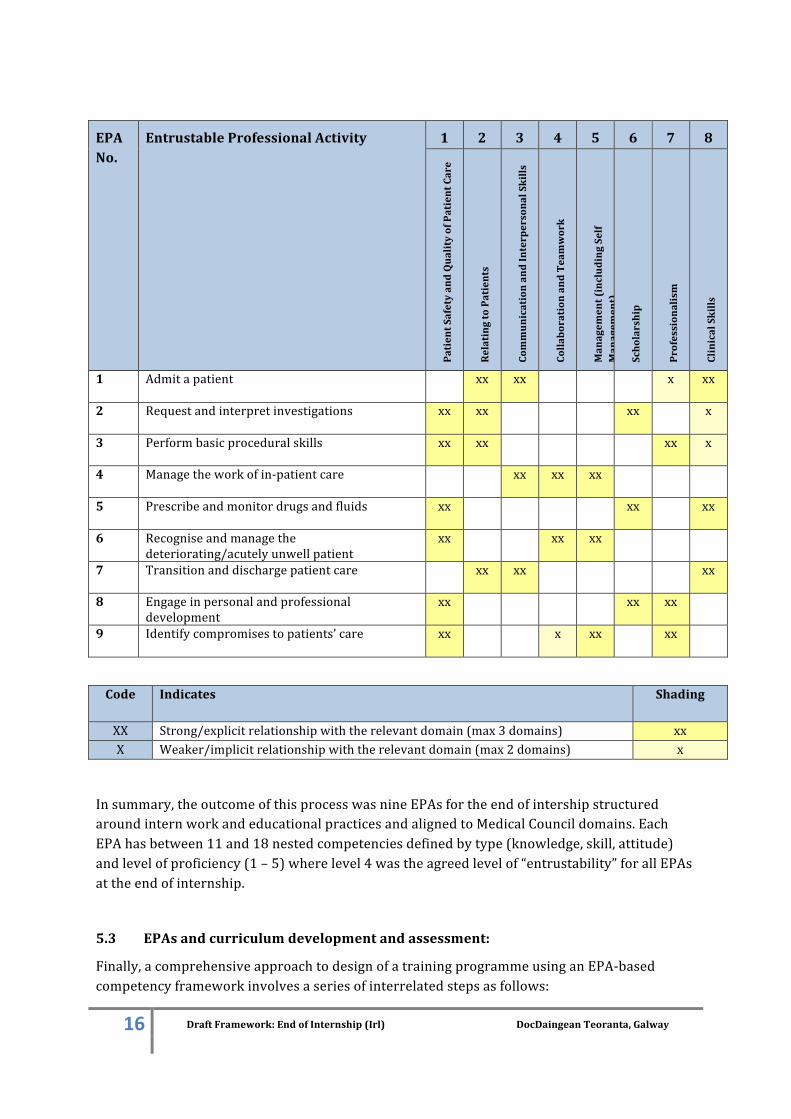
AligningEPAsforendofinternshipandthegenericcompetencieselaboratedintheMedicalCouncilDomainsofGoodProfessionalPracticeprovidesameansofauditingwhereandtowhatextentcompetenciesarebeingdeveloped(andultimatelyassessed)inthetrainingprocess:
16 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
EPANo.
EntrustableProfessionalActivity
1 2 3 4 5 6 7 8
PatientSafetyandQualityofPatientCare
RelatingtoPatients
CommunicationandInterpersonalSkills
CollaborationandTeamwork
Managem
ent(includingSelf
Managem
ent)
Scholarship
Professionalism
ClinicalSkills
1 Admitapatient
xx xx x xx
2 Requestandinterpretinvestigations
xx xx xx x
3 Performbasicproceduralskills
xx xx xx x
4 Managetheworkofin-patientcare
xx xx xx
5 Prescribeandmonitordrugsandfluids
xx xx xx
6 Recogniseandmanagethedeteriorating/acutelyunwellpatient
xx xx xx
7 Transitionanddischargepatientcare
xx xx xx
8 Engageinpersonalandprofessionaldevelopment
xx xx xx
9 Identifycompromisestopatients’care
xx x xx xx
Code Indicates
Shading
XX Strong/explicitrelationshipwiththerelevantdomain(max3domains) xxX Weaker/implicitrelationshipwiththerelevantdomain(max2domains) x
Insummary,theoutcomeofthisprocesswasnineEPAsfortheendofintershipstructuredaroundinternworkandeducationalpracticesandalignedtoMedicalCouncildomains.EachEPAhasbetween11and18nestedcompetenciesdefinedbytype(knowledge,skill,attitude)andlevelofproficiency(1–5)wherelevel4wastheagreedlevelof“entrustability”forallEPAsattheendofinternship.
5.3 EPAsandcurriculumdevelopmentandassessment:
Finally,acomprehensiveapproachtodesignofatrainingprogrammeusinganEPA-basedcompetencyframeworkinvolvesaseriesofinterrelatedstepsasfollows:

17 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
1. Determiningtheworktobedone.Ø Describingtheactivity
2. Statingwhattrainees(interns)mustdemonstratebeforewecantrustthemtodothework.
Ø Identifyingcompetenciesassociatedwiththatactivity
3. Decidinghowtraineesshouldbepreparedtomeettheserequirements.
Ø Designingthecurriculum:whatkindofteachingandlearningopportunitiesneedtobeprovidedinordertoenabletraineestoachievetheEPA
4. Determininghowweassesstrainees’readinesstopassthethresholdofentrustment.
Ø DevelopingtoolsofassesmenttodetermineifEPAshavebeenachievedtorequiredlevelofproficiency
AgreementontherangeandcontentofEPAsforendofinternshipisanessentialprerequisitetothedevelopmentofaNationalInternTrainingProgrammewithaqualityassuredsystemofworkbasedassessment.Stages1and2above,however,havebeenthefocusofthisproject.
ThedescriptionandelaborationofanEntrustableProfessionalActivityshouldprovidesufficientinformationtofacilitaterobustanddefensibledecisionsaboutcompetenceoftrainees.Ultimately,withtheuseofappropriateworkbasedassessment,theassessorshouldbeabletouseEPAsforbothformativefeedbackandsummativedecisions.OptionsforprovidingfeedbackonEPAsincludeusinga‘trafficlight’systemtoindicate:
Competent Wherethetrainee(intern)hasachievedthecompetenciestothelevel
ofentrustabilityrequiredatendofinternshipNotthereyet Wherethetrainee(intern)ismakingappropriateprogresstowards
thelevelofentrustabilityrequired,butisnotthereyet.Notcompetent/causeforconcern
Wherethecompetencieshavenotbeenmetandyouhavecauseforconcernaboutthelevelofprogressbeingmadebythetrainee(intern)
N/A Notapplicable/Noopportunitytoassess
Note: Identificationofassessmentstrategiesisoutsidethescopeofthisproject
6. ValidationProcess
6.1 Overviewofvalidationprocess:
AnimportantpartoftheEPAdevelopmentprocesswasthevalidationoftheworkbyawidergroupofstakeholders.ThedraftEPAs,nestedcompetencies,typesofcompetenciesandlevelsofproficiencywerecirculatedelectronicallyin2separatesurveys,toworkshopattendees,interncoordinatorsandinterntutorsforcomment.EachofthesurveyswasaccompaniedbyashortexplainervideooutliningtheEPAframework,thedraftingprocessandwhatwasrequiredofeachstakeholder/respondentduringeachsurvey.

18 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
6.2 Surveyround1:
ThepurposeofthesurveywastoobtainfeedbackfromstakeholdersonthedraftframeworkofnineEPAsand124competenciesdevelopedattheworkshop.Theparticiantswereaskedwhether:
• theythoughteachofthenineEPAswasakeyactivitywhichaninternshouldbeabletoperformindependentlybytheendoftraining;
• anyoftheEPAswereinappropriate,andtheirreasonforthisopinion;• theythoughttherewasaneedforadditionalEPAs;• eachcompetencywasappropriatefortheEPAwithwhichithadbeenlinked;• anyofthecompetencieswereinappropriate,andtheirreasonforthisopinionand• theythoughtherewasaneedforadditionalcompetencies
Results: Atotalof9doctorscompletedthesurvey(2interns,2SHOs,2registrarsand3consultants)-3wereinternnetworkcoordinatorsandoneaninterntutor.
EPA%agreethatEPAisacorecompetency
%ofcompetenciesforwhich>90%ofrespondentsagreedshouldbeperformed
byanintern
1 Admitapatient 90.9% 85.2%
2 Requestandinterpretinvestigations 100% 100%
3 Performbasicproceduralskills 100% 81.4%
4 Managetheworkofin-patientcare 100% 88.2%
5 Prescribeandmonitordrugsandfluid 100% 82.3%
6 Recogniseandmanagethedeteriorating/acutelyunwellpatient
100% 84.6%
7 Transitionanddischargepatientcare 90.9% 54.5%
8 Engageinpersonalandprofessionaldevelopment 100% 100%
9 Identifycompromisestopatientcare 100% 100%
ItcanbeseenfromtheabovetablethattherewerehighlevelsofagreementfromthesurveyrespondentsthattheEPAswereappropriateforinterns.AdditionalEPAsthatweresuggestedincluded:
• Workaspartofateam• Abilitytoformclinicalquestionsthatwillaffect/improvepatientcare• Communicatingwithfamilies• Interdisciplinary/interprofessionalrelations• Presentandcommunicatewithinateamstructure• Capableofworkingwithinamultidisciplinaryteam

19 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
• Communicationwithfamily/nextofkin• Prescribing• Assesspatients’ongoingcareneeds
Summaryofcommentsoncompetencies;therewasalsobroadagreementwiththecompetencies:
• ForEPA1‘admitapatient’thefivecommentswereconcernedwithissuesregardingduplicationofcompetencies,thefactthatconsentshouldbelimitedtoparticularproceduresandthatprescribingshouldbeanindividualEPA.
• ForEPA3‘performbasicproceduralskills,’thesixcommentswerecentredonwhetherornottheinternhastheexpertisetoperformcertaintasks(e.g.‘shouldinternsbeabletodoalumbarpuncture?’;‘Idon'tthinkinternsshouldbeinstigatingNIVwithoutsenior/anaestheticinput’).
• ForEPA4‘managetheworkofin-patientcare,’thethreecommentswereconcernedwiththefactthattheinternwasunlikelytoleadawardround(e.g.‘seniormemberofteamshouldleadround’).
• ForEPA5‘prescribeandmonitordrugsandfluid,’thethreecommentswereconcernedthatnon-invasiveventilation(NIV)wasaskillthataninternwouldnotbeexpectedtocarryout(e.g.‘NIVisunlikelytobeatanindependentskilllevel’).
• ForEPA6‘recogniseandmanagethedeteriorating/acutelyunwellpatient,’thethreecommentswereconcernedwithpatienttransferbeingtheresponsibilityofmoreseniormembersofstaff(e.g.‘seniormemberofstaffshouldbeinvolvedintransferofpatient’).
• ForEPA7‘transitionanddischargepatientcare,’thethreecommentswereconcernedwithissuesaroundlimitingtheroleoftheinternaroundpatientdeath(e.g.‘notappropriateforinterntoberingingthecoronerorarrangingpost-mortem’).
• NocommentsweremadeonthecompetenciesfortheremainingtwoEPAs(‘engageinpersonalandprofessionaldevelopment’and‘identifycompromisestopatientcare’).
Basedupontheresponsestothissurvey,someamendmentsweremadetotheEPAsbutnoadditionalEPAswereincluded.Theamendmentsmadeincludedaddingsomeadditionalcompetenciesandalterationstosometerminologyandthelevelsofproficiency.
6.3 Surveyround2:
Thepurposeoftheroundtwosurveywastoobtaininformationfromstakeholdersontheclassificationofthetypeandlevelofcompetenciesmadebytheresearchteam,foreachofthe129competenciesintherevisedframework.Eachcompetencywasclassifiedasoneormoreofthefollowingtype(s)ofcompetency:
• Knowledge:Requiredunderpinningknowledgewhichisappliedtotheperformanceoftheprofessionalactivity
• Clinicalskills:Genericandspecialty-specificskillsrequiredtocompletetheprofessionalactivity
• Attitudes/behaviours:Attributesandattitudesassociatedwithprofessionalcompetenciessuchasrelatingtopatients,communication,interpersonalskills,task

20 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
management,collaboration,teamworking,situationawareness,decisionmakingandscholarship
Eachcompetencywasalsoclassifiedatoneoffivelevels(seelevelsofproficiencytablepage13).Forexample,thecompetency‘establishrapportwithpatient’wasclassifiedasanattitudinalcompetencyatlevel4(mayperformanactivityindependentlywithbackstage,mainlyinformalsupervision).
Therespondentswerepresentedwiththeclassificationofthetypeofcompetencyandlevelandaskedwhethertheyagreedordisagreedwiththeopinionsoftheresearchteam.Iftheydisagreed,theywereaskedtoprovideamoreappropriateclassificationoftypeand/orlevel.
Results:Atotalof10doctorscompletedthesurvey(2interns,2SHOs,4registrars,and2consultants).Oftheserespondents,2wereinternnetworkcoordinators,and1aninterntutor.ThetablebelowshowsthepercentageoftherespondentswhoagreedwiththeproficiencyandratingofthetypeofcompetencyineachEPA.Itcanbeseenfromthetablethatthelevelsofagreementbetweentheratingscarriedoutbythebrainstorminggroupandthestakeholderswasrelativelyhigh.Anycommentsthatweremadebytheparticipantsgenerallyreferredtoaddinganothertypeofrating,and/oradjustingthelevelupordownonelevel.
EPA %ofrespondentwhoagreedwithalloftheproficiencyratingsofthe
competenciesintheEPA
%ofrespondentwhoagreedwiththeratingsofthetypeofcompetency
ineachEPA
1 Admitapatient 83.3% 58.3%
2 Requestandinterpretinvestigations 90.9% 90.9%
3 Performbasicproceduralskills 72.7% 81.8%
4 Managetheworkofin-patientcare 70.0% 90.0%
5 Prescribeandmonitordrugsandfluid 90.0% 90.0%
6 Recogniseandmanagethedeteriorating/acutelyunwellpatient
90.0% 90.0%
7 Transitionanddischargepatientcare 100.0% 90.0%
8 Engageinpersonalandprofessionaldevelopment 90.0% 90.0%
9 Identifycompromisestopatientcare 80.0% 90.0%

21 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
7. ForConsideration
Thegoalofthisprojectwastodeviseaframeworkofoutcomesforinternship.Thisreportrepresentsadraftofapotentialframeworkdevelopedinconsultationwithasmallgroupofwellinformedstakeholders.Whileaoneyearinternshipprogramme,wheretheinternhasawelldefinedrole,lendsitselfwelltoCBMEorganisedasanEPAframework,theimplementationofthiswillrequireconsiderablebuy-inandresources.
Firstly,thereisaneedforcommentandfeedbackfromawiderrangeofstakeholdersbeforeadoptinganEPAframeworkforinterntraining.UponagreementofEPAsandcompetenciesforinternship,thenextstepwillbetoseehowthiscanshapethedeliveryofaNationalInternTrainingProgrammethatiscomparableacrossallnetworks.ThisrequiresconsiderationofhowlocalproviderscanbesupportedinthedesignoftrainingprogrammestoensureinternshaveappropriatelearningexperiencestoenablethemtoachievethenestedcompetenciesforeachEPA.Further,thekindsofteachingandlearningopportunitiesrequiredandtobeprovidedtoalignwithcompetencieswillrequirediscussionandinvestment.
Inadditiontoobtainingabroadlevelofagreementfromstakeholders,therearegovernanceimplicationswhenadoptingacompetencybasedEPAframework.TheMedicalCouncilasthegoverningbodywillhavetoconsiderhowthisframeworkmightbeusedasafoundationforstandards,trainingandworkbasedassessment.
Tobeassuredthatcompetenciesareachievedrequiresrobustworkbasedassessmenttoolsandconsiderationshouldbegiventothedevelopment,useabilityandalignmentofthesewithEPAsandcompetencies.Thedevelopmentofthesewilltaketimeandconsultationandiftheyaretobeused,theymustbefitforpurpose,appropriatelytimedandaccessibleonmobiledevices.
Theinternsthemselvesarestakeholdersandwillbeexpectedtohavesomeresponsibilityforengaginginandseekinglearningopportunitiesandworkbasedassessment.
Theroleofkeystakeholdersintheimplementation,organisationanddeliveryofacompetencybasedprogrammethatincludesworkbasedassessmentneedstobeclear.Thetrainingandinfrastructurerequiredtosupportthemisacriticalpartofimplemetation.TherolesoftheHSENationalDoctorsTrainingandPlanning,theInternNetworksExecutive,interncoordinators,clinicalandeducationalsupervisorsandinternadministratorsneedtobedefinedandsupported.Additionaladministrativeandorganisationalstaffwillberequiredandconsiderationshouldbegiventoanationalprogrammeoffice.
Theresourcingofinformationtechnologyisrequiredtofacilitateinternsandsupervisors.Toillustrate,someinternationaltrainingbodieshavedevelopedelectroniclogbooks,portfoliosandmobiletechnologytosupportbothsupervisedlearningactivitiesandworkbasedassessment.
Insummary,thedevisingofadraftframeworkofcompetencybasedtrainingforinternshipisnotsomethingthatcanbedoneinisolation.Thereneedstobeconsiderationgiventoteachingandlearningopppotunitiesandtheworkbasedassessmentthatwillfollow.Moreover,theimpactofthisonallstakeholders,theresourcesandeducationalsupportsrequiredandthegovernanacestructuresnecessarytoensuredeliveryoftheprogrammeareequallyimportantelements.

22 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
TeamBiographies
DocDaingeanTeorantaisahealthcaresolutionscompanybasedinGalway.Thefollowingteammemberswerecontractedtofulfilstrategicprojectroles.Dr.DaraByrneFRCSI,MCh,MMedEd,CHSEDrByrneistheprojectlead.SheisCEOofDocDaingeanTeorantaandInternCoordinatorfortheWestNorthwest InternNetwork.She isaSeniorLecturer inMedicalEducationatNUIGalwayandDirectorofSimulationfortheSaoltaUniversityHealthCareGroup.Shehasauthoredover50conferencepapersandpublicationsintheareaofinterneducationandtraining.Dr.JosephineBolandPhDDrJosephineBolandisanindependentmedicaleducationalistandresearcher,withaDoctorateinEducation(EdinburghUniveristy)andoverthirtyyearsexperienceinfurther,higher,teacherandmedicaleducation.Shespecialisesincurriculumdevelopment,assessmentdesign,qualityassuranceandfacultydevelopment.AsSeniorLecturerinEducationintheSchoolofMedicine,NUIGalway(2011-2015)shewasdirectoroftheMastersinClinicalEducationandacademicleadforcurriculummappingandtechnologyenhancedlearning.AsmedicaleducationalistwiththeCollegeofAnaesthetists(2014-present)shesupportsthedevelopmentandimplementationofacompetencybasedcurriculumandworkbasedassessment.
Dr.GozieOffiahFRCSI,MMedEdDr. Offiah is a Senior Clinical Lecturer in Surgery in the RCSI, Dublin. Dr. Offiah studied atQueen’s University Belfast and was awarded a Masters in Medical Education. She is internlecturerintheDublinNorthEastInternNetwork.Asafulltimemedicaleducationalist,sheisamemberofthecurriculumreviewcommitteeintheundergraduateprogrammeinRCSIandalsoinvolved in the development of a competency based curriculum for the Human Factors inPatientSafetyprogrammedeliveredintheNationalSurgicalTrainingCentre.Dr.PaulOConnorPhDDr.PaulO’Connor isaLecturer inPrimaryCare inNUIGalwayandaResearchMethodologist.He has a Ph.D. in Psychology from the University of Aberdeen,M.Sc. in ResearchMethods inPsychologyfromtheUniversityofStrathclyde,ScotlandandB.Sc.(Hons)inPsychologyfromtheUniversity of Aberdeen, Scotland. His research is concerned with improving humanperformanceandsafetyinhighriskworkenvironments.Hehascarriedoutresearchinawiderangeofhighriskindustriesandthemilitary.Morerecentlyhehasbeencarryingoutresearchinhealthcarewithinterns.

23 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
Bibliography
AssociationofAmericanMedicalCollege(2014)CoreEntrustableActivitiesforEnteringResidency:CurriculumDevelopers’Guide.WashingtonDC:AAMC
AustralianMedicalCouncilLimited(2014)NationalInternshipFramework-http://www.amc.org.au/accreditation/prevoc-standards
Aylward,M.,Nixon,J.,&Gladding,S.(2014).Anentrustableprofessionalactivity(EPA)forhandoffsasamodelforEPAassessmentdevelopment.AcadMed,89(10),1335.doi:10.1097/ACM.0000000000000317
Boyce,P.,Spratt,C.,Davies,M.,&McEvoy,P.(2011).Usingentrustableprofessionalactivitiestoguidecurriculumdevelopmentinpsychiatrytraining.BMCMedicalEducation,11,96-96.doi:10.1186/1472-6920-11-96
CanadianResidentsMatchingService.(2015).CanadianResidentsMatchingService.Retrievedfrom:http://www.carms.ca/en/
ChenHcChen(2015).Thecaseforuseofentrustableprofessionalactivitiesinundergraduatemedicaleducation.AcademicMedicine,90(4),431-436.
Englander,R,(2014).Fromtheorytopractice:makingentrustableprofessionalactivitiescometolifeinthecontextofmilestones.AcademicMedicine,89(10),1321-1323.
Frank.J.R.,Mungroo,R.,Ahmad,Y.Wang.M,DeRossi,S.HorsleyT.(2010)Towardadefinitionofcompetency-basededucationinmedicine:asystematicreviewofpublisheddefinitions.MedicalTeacher32(8):631-7.doi:10.3109/0142159X.2010.500898
GeneralMedicalCouncil(2014)UnitedKingdomFoundationProgrammeCurriculumwww.foundationprogramme.nhs.uk/
Gilhooly,J.,Schumacher,D.J.,West,D.C.,&Jones,M.D.(2014).Thepromiseandchallengeofentrustableprofessionalactivities.Pediatrics,133(2),S78-S79.doi:10.1542/peds.2013-3861H
Glass,J.M(2014)Competencybasedtrainingisaframeworkforincompetence.BMJdoi:10.1136/bmj.g2909.
Hauer,K.E.,Soni,K.,Hollander,H.,Ranji,S.R.,TenCate,O.,Calton,B.Widera,E.(2013).Developingentrustableprofessionalactivitiesasthebasisforassessmentofcompetenceinaninternalmedicineresidency:Afeasibilitystudy.JGenInternMed,28(8),1110-1114.doi:10.1007/s11606-013-2372-x
HealthServiceExecutive(2015)TheNationalInternEducationandTrainingAgreementDublin:HSE
HirshDaHirsh,(2014).Timetotrust:longitudinalintegratedclerkshipsandentrustableprofessionalactivities.AcademicMedicine,89(2),201-204.
MedicalCouncil(2011)GuidelinesforMedicalEducationandTrainingforInterns(https://www.medicalcouncil.ie/Education/Career-Stage-Undergraduate/Your-Questions-Answered/Guidelines-on-Medical-Education-and-Training.pdf)
24 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
MedicalCouncil(2011)NationalInternTrainingProgrammeInternCurriculum(http://www.medicalcouncil.ie/Education/Career-Stage-Intern/National-Intern-Training-Programme-.pdf)
MedicalCouncil(2011)StandardsforTrainingandExperienceRequiredforGrantingofaCertificateofExperience(https://www.medicalcouncil.ie/Education/Career-Stage-Intern/Standards-of-training.pdf)
MedicalCouncil(2014)YourTrainingCountsReport:ResultsoftheNationaltraineeExperienceSurveyDublin:MedicalCouncil
MedicalCouncil(2015)Doctors’Education,TrainingandLifelongLearningin21stCenturyIrelandDublin:MedicalCouncil
MedicalCouncilofNewZealand(2014)CurriculumFrameworkforPre-VocationalMedicalTraining:https://www.mcnz.org.nz/news-and-publications/prevocational-training/
Mulder,H.,tenCate,O.,Daalder,R.,&Berkvens,J.(2010).Buildingacompetency-basedworkplacecurriculumaroundentrustableprofessionalactivities:Thecaseofphysicianassistanttraining.MedicalTeacher,32(10),E453-E459.doi:10.3109/0142159X.2010.513719
Rashid,P.(2015).Entrustableprofessionalactivities:Timetobetrusted?ANZJournalofSurgery,85(5),298-299.doi:10.1111/ans.12946
Sklar,D.P.(2015).Competencies,milestones,andentrustableprofessionalactivities:whattheyare,whattheycouldbe.AcadMed,90(4),395-397.doi:10.1097/ACM.0000000000000659
Talbot,M.(2004)Monkeysee,monkeydo:acritiqueofthecompetencymodelingraduatemedicaleducation.MedicalEducaiton38(6):587-92
tenCate,O.(2014)Thepatienthandoverasanentrustableprofessionalactivity:addingmeaninginteachingandpracticeBMJQualSaf2012;21:i9–i12.doi:10.1136/bmjqs-2012-001213
tenCate,O.,&Scheele,F.(2007).Competency-basedpostgraduatetraining:canwebridgethegapbetweentheoryandclinicalpractice?AcadMed,82(6),542.
tenCate,O.,Chen,H.C.,Hoff,R.G.,Peters,H.,Bok,H.,&vanDerSchaaf,M.(2015).CurriculumdevelopmentfortheworkplaceusingEntrustableProfessionalActivities(EPAs):AMEEGuideNo.99.MedicalTeacher,1-20.doi:10.3109/0142159X.2015.1060308
VanLoon,K.A.,Driessen,E.W.,Teunissen,P.W.,&Scheele,F.(2014).ExperienceswithEPAs,potentialbenefitsandpitfalls.MedicalTeacher,2014,Vol.36(8),p.698-702,36(8),698-702.doi:10.3109/0142159X.2014.909588

25 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
AppendixATheNationalInternEducationandTrainingAgreement(NIETA)
NationalInternEducationandTrainingAgreement
(Forperiod13July2015to10July2016)
InternName: XXXXXXXXXXXX
TrainingProgramme: NationalInternTrainingProgrammeInternTrainingNetwork: AdministrativeBody: InternNetworkCoordinator: TrainingPeriod: 13July2015–10July2016TrainingPostNumber: XXXXXXMedicalCouncilRegistrationNumber: Manycongratulationsonyourgraduationandwelcometothemedicalworkforce.Mostdoctorshavegoodandhappymemoriesoftheirinternshipyearandhopefullyyourexperiencewillbenodifferent.InsigningthisNationalInternEducationandTrainingAgreement(NIETA)youandtheschoolofMedicine,NUIG(theadministrativebodyfortheWestNorthwestInternTrainingNetwork)committotheeducationandtrainingprinciplescontainedtherein.EachInternisbeingaskedtosigntheagreementatthecommencementofinternship.InternswhohavecompletedsomeinternshippriortoJuly2015arerequiredtosigntheNIETAinrespectofthedefinedperiodoftrainingremaining.PleasenotethatthisNIETAdoesnotrelatetoemploymentmatters,whicharegovernedbytheNCHDContract2010,betweentheInternandtheirindividualemployer(s).InternsshouldconsulttheNationalInternTrainingProgramme(NITP):EducationandTrainingintheInternYear,approvedbytheMedicalCouncilinMay2011,,andrevisedinMay2012,whichoutlinestheprofessionalcompetencerequirementsforinterns.TheNITPisappendedtothisAgreementinAppendixA.TheInternNetworkCoordinatorscoordinatetheirresponsibilitiesonanationalbasisthroughtheInternNetworksExecutive(INE)establishedin2011.TheINE,incollaborationwiththeCouncilofDeansfortheMedicalSchoolsinIreland(CDFMSI),ensuresthatthereisacoordinatedapproachtointeractionwiththosebodieshavinganinterestandresponsibilityintheprovisionofmedicaleducationandtrainingincludingtheMedicalCouncil,theHealthServiceExecutive,theForumof
26 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
PostgraduateTrainingBodiesandtheDepartmentofHealth&Children.TheInternNetworksExecutivemeetsatleastsixtimesperannum.TheWestNorthwestInternTrainingNetworkisresponsiblefortheprovisionandcoordinationofthistrainingprogrammeandisaccreditedbytheMedicalCouncil(ofIreland)forthispurpose.IntheWestNorthwestInternNetwork,NUIGisthebodyresponsiblefortheadministrationoftheprogramme.EachInternTrainingNetworkisledbyaconsultant-gradeInternNetworkCoordinatorwho,incollaborationwiththeInternTutors,isresponsibleforoverseeinginterntrainingintheirNetwork.ThecontactdetailsfortheInternNetworkCoordinator,theInternTutorsandtheAdministrativeofficeintheWestNorthwestInternNetworkareprovidedinAppendixB.The12-monthinternshipintheWestNorthwestInternTrainingNetworkcomprises4x3-monthrotationsTheWestNorthwestInternTrainingNetworkiscommittedtosupportingyouthroughouttheyear.Ifdifficultiesdoariseyoushouldseeksupport,inthefirstinstance,fromyourdesignatedspecialistTrainer,nextyourInternTutorand,ifnecessary,theInternNetworkCoordinator.ThepurposeofinterntrainingistoeducateandtrainthenewlyqualifiedmedicalgraduatetoalevelwhichwillleadtobeingawardedaCertificateofExperiencebytheMedicalCouncilofIreland.Thegrantingofacertificateofexperienceisdependentontheinternsatisfactorilycompletingtheeducationandtrainingprogramme.TheInternNetworkCoordinatorwillrecommendinternstotheMedicalCouncilfortheawardoftheCertificateofExperiencebasedontheintern’sprogressionthroughtheInternTrainingProgramme,includingthecompletionofmandatoryandothertrainingelementsandthecompletionofassessmentstotherequiredstandardasoutlinedbelow.TheissuanceoftheCertificateofExperiencebytheMedicalCounciltestifiesthattheInternhassatisfactorilycompletedtheInternTrainingProgramme.Theareasthatwillbeincludedintheassessmentofeachintern’soverallperformanceinclude:
1. Attendingthe5/7-dayinductionprogrammeinGalwayUniversityHospital(GUHs),GalwayClinic,BonSecoursHospitalorinSligo.Letterkenny,Mayo,RoscommonorPortiunculaHospitalspriortocommencinginternship.Thedetailsofthiswillbesenttoyouatthetimeofjoboffer.Theface-to-faceinductionismandatoryandincludesmanualhandling,occupationalhealthappointmentandspecifictraining.AllinternsintheWNWwillberequiredtocompleteanonlineinductionprogrammePRIORtotheface-to-aceinduction–thelinktothiswillbesenttoyouatthetimeofjoboffer.
2. Achievinga70%attendancerateatthededicatedintern-specificlunchtimeteachingsessions.Thetimingandnumberofthesesessionsinanyone-weekvaryfromsitetosite.IntheWestNorthwestNetworktheyareeveryMonday,TuesdayandWednesdaybetween1pmand2pmandarevideo-conferencedtoallsitesinthenetwork.Asigninsheetisinoperation.
3. Attainingcompetencyinthe8DomainsofGoodProfessionalPracticeandcapturedintheInternAssessmentForm(acopyofwhichisprovidedinAppendix4oftheNationalInternTrainingProgrammealreadyreferredtoinAppendixAbelow).
4. Acquiring sign-off, to thegreatestpossibleextent, in thedomainsdetailed in theNationalInternTrainingProgramme(seeAppendixA);theyinclude:
a. ClinicalJudgementi. ClinicalHistoryandExaminationii. ClinicalSkillsiii. InfectionControliv. ManagingtheAcutelyIllv. Prescribingvi. ContinuousLearning

27 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
b. Communicationi. Patientconfidentialityii. ClinicalNoteTakingiii. InformedConsent
c. ProfessionalDevelopmenti. UnderstandthelegalframeworkformedicalpracticeinIrelandii. RegistrationwiththeMedicalCouncilofIrelandiii. ProfessionalApproachiv. Maintainingcompetencev. Ensureappropriateprofessionalindemnityvi. DisciplinaryActionvii. Adheretohighethicalstandardsviii. CompletionofFormalDocumentsix. Developaninformedcareerplanx. EnhanceTeamworkSkillsxi. RecogniseLimitationsandManageStress
5. CurrentcertificationinBasicLifeSupport(BLS)6. AttainingcertificationinAHA/IHFapprovedAdvancedCardiacLifeSupport(ACLS)-tobe
completedatinduction.7. CompletionandcertificationofattendanceattheEarlyWarningScoringSystemcourse
(COMPASS)–theacutemedicalemergencyrecognitionandtreatmentworkshopscurrentlybeingrolledoutthroughoutthecountry.
8. Currentcertificationinamanualhandlingcourse,orcertificationwithin6monthsofemployment
9. EvidenceofsatisfactoryparticipationintheOn-LineNationalInternEducation&Trainingprogramme.TheClinicalJudgementmoduleofthiseLearninginitiativethatincludestutorialsandMCQscoveringthe6headingsoutlinedin4(a)abovearecompleted.ThisOn-LineeducationtoolwillbeavailabletoALLinternsnationwide;eachwillhavetheirownuniqueaccesscode.Participationwillformpartofeachintern’soverallassessmentattheendoftheyear.
10. DetailedinAppendixCareadditionaltrainingcourses/workshopscurrentlybeingprovidedbysomebutnotallInternNetworks.ParticipationintheseeducationalactivitiesismandatoryforInternsaffiliatedtotheseNetworks.AsthenationalprogrammeevolvesandtherequiredfundingismadeavailableitisintendedthatALLInternswillhaveaccessthesetrainingworkshops,regardlessofNetworkbase.
11. Satisfactoryattendanceintheworkplace,withnounexplainedperiodofabsenteeism.12. AsaninternYOUareresponsibleforensuringthattheInternAssessmentFormis
completedandsignedbythesupervisingconsultantandyouattheendofeachrotation.YOUarealsorequiredtobringthisformtotheInternTutorinyourclinicalsiteforreviewandfinalsign-off.IntheWestNorthwestInternTrainingNetworkyouwillhaveaminimumof4InternAssessmentFormstocompleteduringyour12-monthinternship.FailuretocomplywiththisrequirementwilldelayprocessingyourfullregistrationwiththeMedicalCouncil.
I(printnameinBLOCKCAPITALS),............................................................................,agreetoaccepttheconditionsoutlinedabove,formyperiodofinternshipinWestNorthwestInternNetworkSigned:__________________________ Date:______________________________Signed:__________________________ Date:________________________________ InternNetworkCoordinator
28 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
AppendixBSampleofCurrentInternAssessmentForm
I
29 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
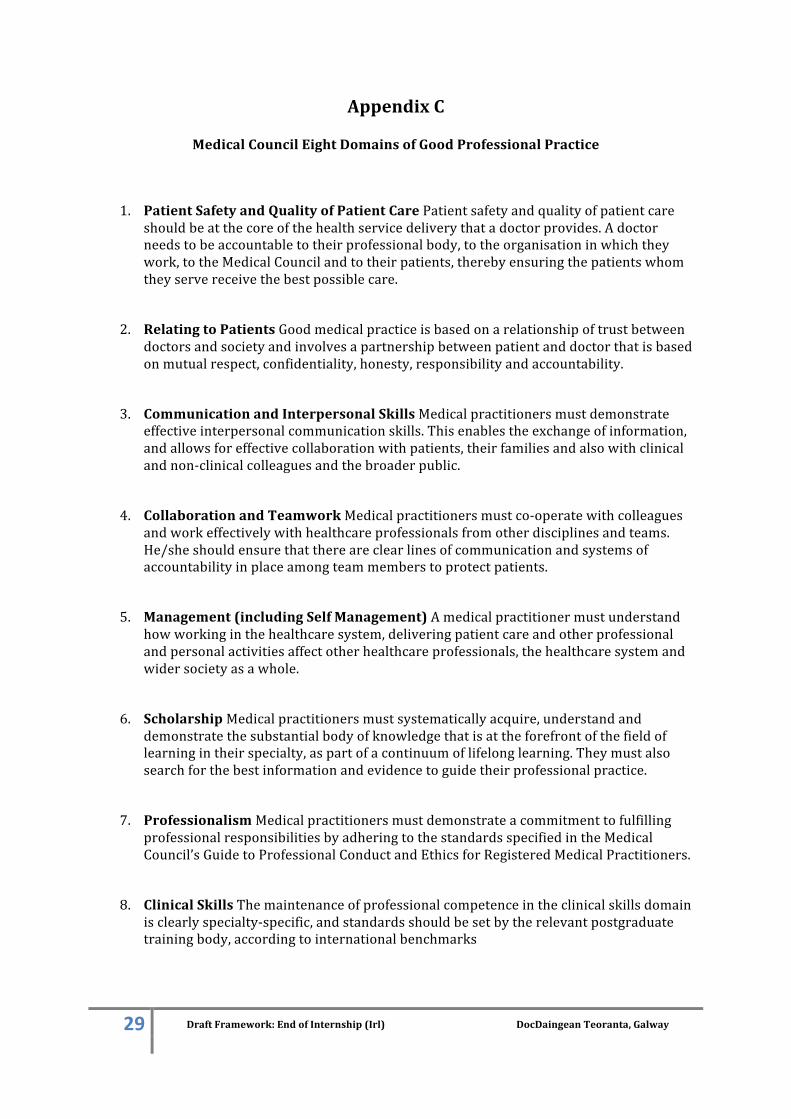
AppendixC
MedicalCouncilEightDomainsofGoodProfessionalPractice
1. PatientSafetyandQualityofPatientCarePatientsafetyandqualityofpatientcareshouldbeatthecoreofthehealthservicedeliverythatadoctorprovides.Adoctorneedstobeaccountabletotheirprofessionalbody,totheorganisationinwhichtheywork,totheMedicalCouncilandtotheirpatients,therebyensuringthepatientswhomtheyservereceivethebestpossiblecare.
2. RelatingtoPatientsGoodmedicalpracticeisbasedonarelationshipoftrustbetweendoctorsandsocietyandinvolvesapartnershipbetweenpatientanddoctorthatisbasedonmutualrespect,confidentiality,honesty,responsibilityandaccountability.
3. CommunicationandInterpersonalSkillsMedicalpractitionersmustdemonstrateeffectiveinterpersonalcommunicationskills.Thisenablestheexchangeofinformation,andallowsforeffectivecollaborationwithpatients,theirfamiliesandalsowithclinicalandnon-clinicalcolleaguesandthebroaderpublic.
4. CollaborationandTeamworkMedicalpractitionersmustco-operatewithcolleaguesandworkeffectivelywithhealthcareprofessionalsfromotherdisciplinesandteams.He/sheshouldensurethatthereareclearlinesofcommunicationandsystemsofaccountabilityinplaceamongteammemberstoprotectpatients.
5. Management(includingSelfManagement)Amedicalpractitionermustunderstandhowworkinginthehealthcaresystem,deliveringpatientcareandotherprofessionalandpersonalactivitiesaffectotherhealthcareprofessionals,thehealthcaresystemandwidersocietyasawhole.
6. ScholarshipMedicalpractitionersmustsystematicallyacquire,understandanddemonstratethesubstantialbodyofknowledgethatisattheforefrontofthefieldoflearningintheirspecialty,aspartofacontinuumoflifelonglearning.Theymustalsosearchforthebestinformationandevidencetoguidetheirprofessionalpractice.
7. ProfessionalismMedicalpractitionersmustdemonstrateacommitmenttofulfillingprofessionalresponsibilitiesbyadheringtothestandardsspecifiedintheMedicalCouncil’sGuidetoProfessionalConductandEthicsforRegisteredMedicalPractitioners.
8. ClinicalSkillsThemaintenanceofprofessionalcompetenceintheclinicalskillsdomainisclearlyspecialty-specific,andstandardsshouldbesetbytherelevantpostgraduatetrainingbody,accordingtointernationalbenchmarks
30 DraftFramework:EndofInternship(Irl)DocDaingeanTeoranta,Galway
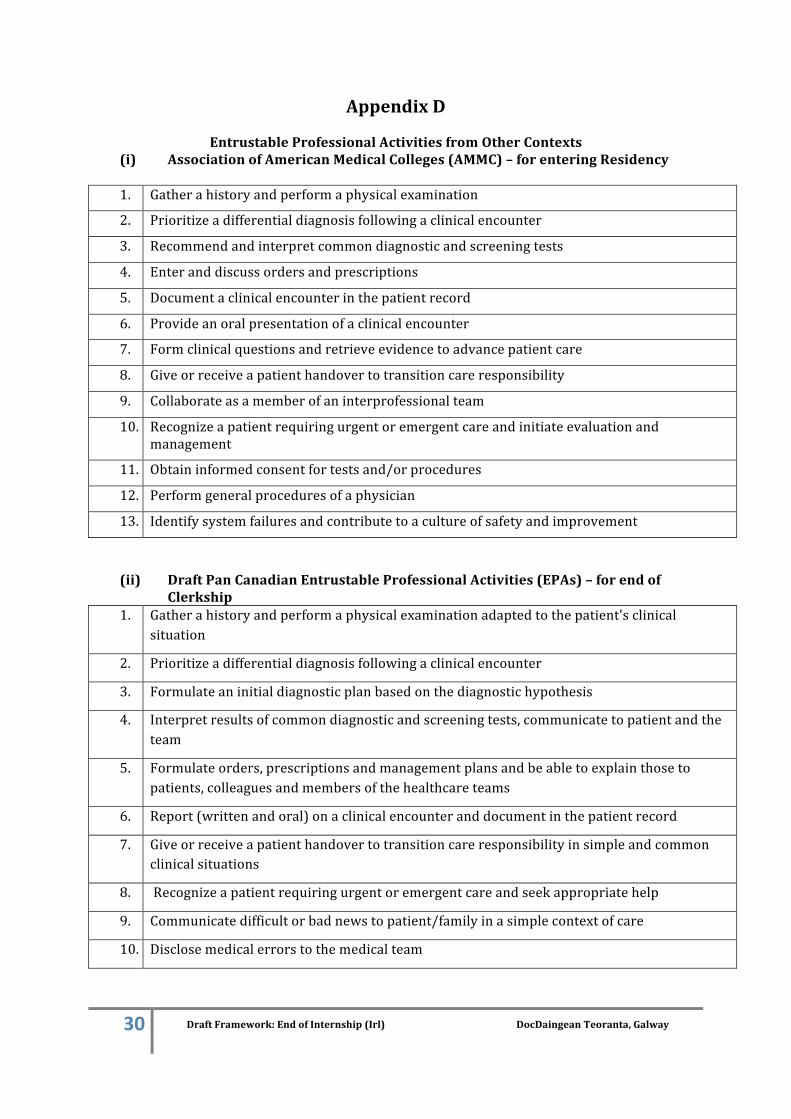
AppendixD
EntrustableProfessionalActivitiesfromOtherContexts(i) AssociationofAmericanMedicalColleges(AMMC)–forenteringResidency
1. Gatherahistoryandperformaphysicalexamination
2. Prioritizeadifferentialdiagnosisfollowingaclinicalencounter
3. Recommendandinterpretcommondiagnosticandscreeningtests
4. Enteranddiscussordersandprescriptions
5. Documentaclinicalencounterinthepatientrecord
6. Provideanoralpresentationofaclinicalencounter
7. Formclinicalquestionsandretrieveevidencetoadvancepatientcare
8. Giveorreceiveapatienthandovertotransitioncareresponsibility
9. Collaborateasamemberofaninterprofessionalteam
10. Recognizeapatientrequiringurgentoremergentcareandinitiateevaluationandmanagement
11. Obtaininformedconsentfortestsand/orprocedures
12. Performgeneralproceduresofaphysician
13. Identifysystemfailuresandcontributetoacultureofsafetyandimprovement
(ii) DraftPanCanadianEntrustableProfessionalActivities(EPAs)–forendofClerkship
1. Gatherahistoryandperformaphysicalexaminationadaptedtothepatient'sclinicalsituation
2. Prioritizeadifferentialdiagnosisfollowingaclinicalencounter
3. Formulateaninitialdiagnosticplanbasedonthediagnostichypothesis
4. Interpretresultsofcommondiagnosticandscreeningtests,communicatetopatientandtheteam
5. Formulateorders,prescriptionsandmanagementplansandbeabletoexplainthosetopatients,colleaguesandmembersofthehealthcareteams
6. Report(writtenandoral)onaclinicalencounteranddocumentinthepatientrecord
7. Giveorreceiveapatienthandovertotransitioncareresponsibilityinsimpleandcommonclinicalsituations
8. Recognizeapatientrequiringurgentoremergentcareandseekappropriatehelp
9. Communicatedifficultorbadnewstopatient/familyinasimplecontextofcare
10. Disclosemedicalerrorstothemedicalteam