Download - Postdischarge Costs in Arthroplasty Surgery
The Journal of Arthroplasty Vol. 21 No. 6 Suppl. 2 2006
Postdischarge Costs in Arthroplasty Surgery
Carlos J. Lavernia, MD,* Michele R. D’Apuzzo, MD,* Victor H. Hernandez, MD,*David J. Lee, PhD,y and Mark D. Rossi, PT, PhD*
From the *Orthopaand yDepartment ofMiami, Miami, Florid
Submitted FebruBenefits or funds
the research materMercy Hospital, Art
Reprint requestInstitute at Mercy HMiami, FL 33133.
n 2006 Elsevier0883-5403/06/19doi:10.1016/j.art
Abstract: Postdischarge costs associated with primary arthroplasty surgeries have
received limited attention in the literature. Our objective was to identify the costs
incurred after discharge in primary arthroplasty and to estimate annual post-
discharge expenditures in the United States. A cohort of 136 patients who
underwent primary arthroplasty was studied. Comprehensive rehabilitation unit
(CRU) and home care (HC) costs were obtained. The National Hospital Discharge
Survey 2003 data were used to model the national discharge cost estimates. Local
patient-oriented outcome was also compared in the patients discharged to CRU vs
HC. Total costs were significantly lower in patients discharged directly to home vs
those sent to the CRU and who subsequently received HC ($2405 vs $13435, P b
.001); both patient groups experienced similar quality of life improvements. An
estimated $3.2 billion is spent annually on postsurgical rehabilitation after
arthroplasty. Postdischarge costs are significantly higher for patients going to a
CRU vs those discharged home; yet, both groups had comparable short-term
outcomes. Key words: postdischarge, costs, rehabilitation, primary arthroplasty.
n 2006 Elsevier Inc. All rights reserved.
More than 600000 primary total joint arthroplas-
ties are performed annually in the United States
[1]. Conservative projections from the American
Academy of Orthopaedic Surgeons (Chicago, IL)
estimate that about 750000 of these procedures
will be performed annually by the year 2030 [2].
These trends, combined with life expectancy
increases, as well as the desire to maintain active
pain-free lifestyles, will lead to dramatic increases
in annual joint arthroplasty surgery expenditures
in the United States.
144
edic Institute at Mercy Hospital, Miami, Florida;Epidemiology and Public Health, University ofa.ary 27, 2006; accepted May 1, 2006.were received in partial or total support of
ial described in this article from Zimmer,hritis Surgery Research Foundation.s: Carlos J. Lavernia, MD, Orthopaedicospital, 3659 S Miami Avenue, Suite 4008,
Inc. All rights reserved.06-0004$32.00/0
h.2006.05.003
Given the continued increase in the number of
arthroplasty surgeries, it will be essential to identify
cost-effective strategies that do not diminish the
quality of patient care. Furthermore, it is extremely
important to justify post–acute care services per-
taining to joint arthroplasty surgeries given that
the current cost-containment pressures within the
Medicare system will only intensify as the baby
boom generation ages. Careful documentation of
all perioperative and associated postoperative re-
habilitative costs is a necessary first step in this
process. National acute care hospital-based esti-
mates of arthroplasty expenditures are available
[3-5], but similar data on postrehabilitative dis-
charge costs are not.
Most arthroplasty patients will require some
form of rehabilitation ranging from inpatient stays
to home care (HC) services and outpatient rehabil-
itation, or a combination of both. There have been
a limited number of studies examining the efficacy
of rehabilitation before and after joint arthroplasty
surgery [6-8]. These studies did not address cost
issues within the context of comparative outcomes.
Postsurgical rehabilitation costs can be considerable

Postdischarge Costs in Arthroplasty Surgery ! Lavernia et al 145
and yet are frequently ignored when discussing the
cost of joint arthroplasty surgery [9].
National estimates for postdischarge costs associ-
ated with arthroplasty are not available; yet,
Medicare has recently instituted changes to its
reimbursement policies, which will lead to changes
in the funding available for postdischarge care (ie,
the 75% rule) [10]. These reimbursement policy
changes could have implications in terms of access
because a number of patients live alone and have
nowhere to go after surgery. Without a bbaselineQfor postdischarge expenditures, it will be difficult to
even assess the financial implications of reimburse-
ment policies because they are phased-in. Our
objective is to document the costs incurred after dis-
charge within a single surgical practice and to apply
these cost estimates to the number of arthroplasties
completed in the United States. We also compare
surgical and quality of life outcomes in patients
according to discharge status.
Methods
A cohort of 136 patients (143 procedures) from a
single surgical practice, under the direction of the
primary author, who underwent primary hip and
knee arthroplasty between January to December of
2004, was enrolled in a prospective registry study
after institutional review board approval, and
informed consent was obtained. Patient character-
istics were compared with national estimates using
weighted data from the 2003 National Hospital
Discharge Survey (NHDS) [11]. Local financial data
were obtained from 3 sources, including the
hospital cost accounting system for the compre-
hensive rehabilitation unit (CRU), and HC costs
obtained directly from the provider, and estimated
professional fees calculated using visit levels and
the 2005 Medicare fee schedule. Local data on
skilled nursing facility (SNF) costs after arthroplasty
were not available. The use of the Medicare
reimbursement rate is reasonable given that more
than 60% of arthroplasties charges in the United
States are reimbursed by this agency.
Outcome Measures
Preoperative and postoperative functional status
and quality of life scales included a Pain Visual
Analog Scale, the Western Ontario and McMaster
University Osteoarthritis Index (WOMAC) [12], and
the Short-Form 36 (SF-36) that assesses 8 domains,
including physical function, bodily pain, mental
health, social function, role limitation caused by
physical function and emotional problems, vitality
as well as general health perceptions [13,14]. The
Quality of Well-Being (QWB) Index was also
administered to assess general quality of life [15].
Postoperative measures were obtained at an average
8.6 F 3.73 SD months (range, 1-24 months).
Expenditure Definitions
Comprehensive rehabilitation unit expenditures
included both direct and indirect costs. Direct costs
included items such as devices used (ie, continuous
passive motion instrument), associated therapies
(ie, physical therapy), supplies, and medications.
Indirect costs included all support staff (ie, admin-
istration) and all ancillary services such as physical
and occupational therapies, nursing, supplies (ie,
assistive devices), and home health aides.
Estimation of National Expenditures
Total postdischarge costs included the sum of
CRU, HC, and professional fees for each patient. We
first estimated expenditures for 3 patient categories:
(1) discharged to the CRU, (2) discharged to home,
and (3) discharged to an SNF. Costs for CRU pa-
tients included CRU charges, professional fees, and
any home health care costs incurred after discharge
from the CRU. Costs for those discharged to home
were limited to HC charges only (which include
imbedded professional fees).
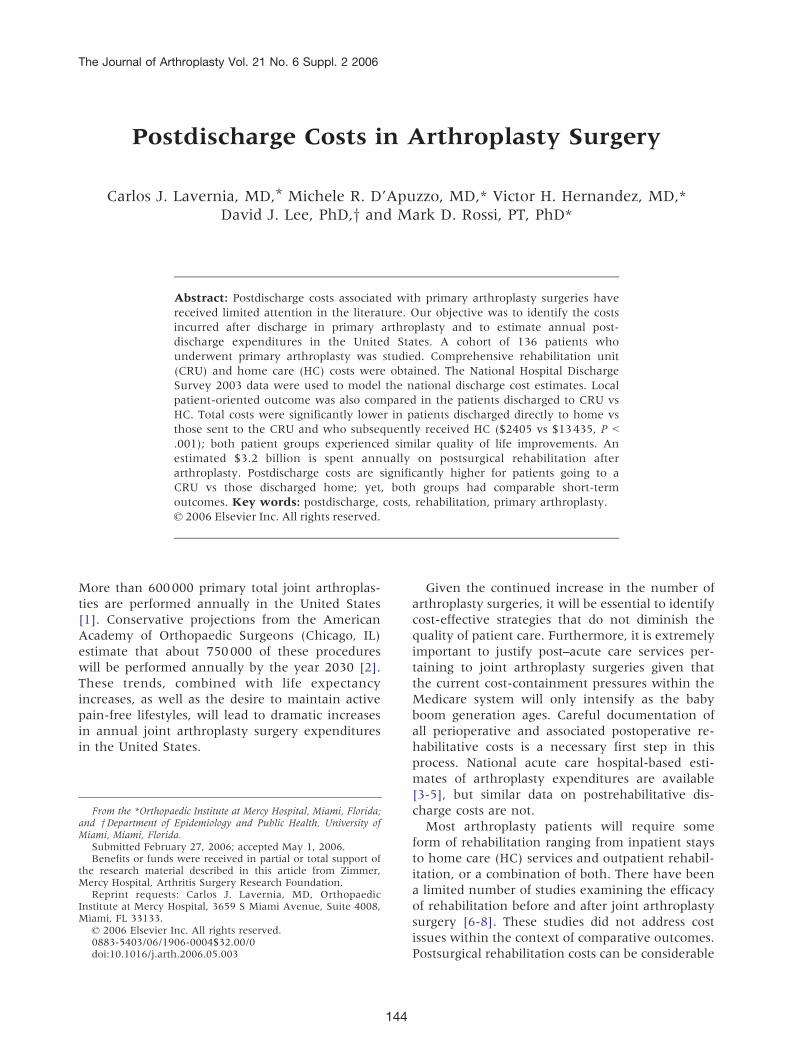
In our patient series, there were no SNF dis-
charges during the surveyed period. Because SNF
discharges can occur after arthroplasty, we estimat-
ed these costs based on the local average length of
stay for an arthroplasty patient at our local SNF
(20 days) multiplied by the local per diem Medicare
reimbursement rate (Fig. 1) [16].
National postdischarge costs were estimated by
applying the averages obtained for patients dis-
charged to the CRU, home, and SNF to the 2003
NHDS estimates of the number of arthroplasty
discharges in each of these 3 categories. Discharge
status was unknown for nearly 20% of the NHDS
patients. We assumed that the distribution of
unknown discharges was equal to the distribution
of known discharge subtypes to calculate a weight-
ed cost average for this subgroup.
Statistical Analyses
The SPSS software (SPSS, Chicago, Ill) was used
for the statistical analyses. Student t tests were
used to compare costs in patients discharged to the
CRU vs directed directly to HC. We calculated
preoperative and average 8.6-month postsurgical
change scores for all quality of life measures and
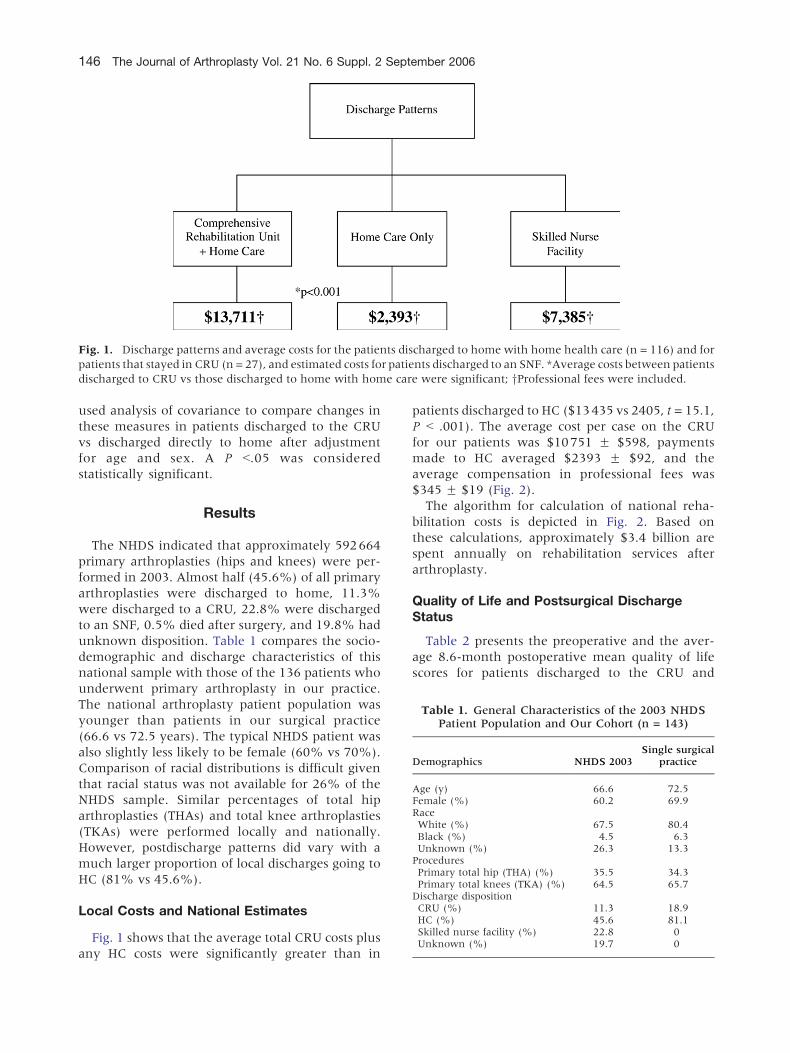
Fig. 1. Discharge patterns and average costs for the patients discharged to home with home health care (n = 116) and for
patients that stayed in CRU (n = 27), and estimated costs for patients discharged to an SNF. *Average costs between patients
discharged to CRU vs those discharged to home with home care were significant; yProfessional fees were included.
146 The Journal of Arthroplasty Vol. 21 No. 6 Suppl. 2 September 2006
used analysis of covariance to compare changes in
these measures in patients discharged to the CRU
vs discharged directly to home after adjustment
for age and sex. A P b.05 was considered
statistically significant.
Table 1. General Characteristics of the 2003 NHDSPatient Population and Our Cohort (n = 143)
Demographics NHDS 2003Single surgical
practice
Age (y) 66.6 72.5Female (%) 60.2 69.9RaceWhite (%) 67.5 80.4Black (%) 4.5 6.3Unknown (%) 26.3 13.3
ProceduresPrimary total hip (THA) (%) 35.5 34.3Primary total knees (TKA) (%) 64.5 65.7
Discharge dispositionCRU (%) 11.3 18.9HC (%) 45.6 81.1Skilled nurse facility (%) 22.8 0Unknown (%) 19.7 0
Results
The NHDS indicated that approximately 592664
primary arthroplasties (hips and knees) were per-
formed in 2003. Almost half (45.6%) of all primary
arthroplasties were discharged to home, 11.3%
were discharged to a CRU, 22.8% were discharged
to an SNF, 0.5% died after surgery, and 19.8% had
unknown disposition. Table 1 compares the socio-
demographic and discharge characteristics of this
national sample with those of the 136 patients who
underwent primary arthroplasty in our practice.
The national arthroplasty patient population was
younger than patients in our surgical practice
(66.6 vs 72.5 years). The typical NHDS patient was
also slightly less likely to be female (60% vs 70%).
Comparison of racial distributions is difficult given
that racial status was not available for 26% of the
NHDS sample. Similar percentages of total hip
arthroplasties (THAs) and total knee arthroplasties
(TKAs) were performed locally and nationally.
However, postdischarge patterns did vary with a
much larger proportion of local discharges going to
HC (81% vs 45.6%).
Local Costs and National Estimates
Fig. 1 shows that the average total CRU costs plus
any HC costs were significantly greater than in
patients discharged to HC ($13435 vs 2405, t = 15.1,
P b .001). The average cost per case on the CRU
for our patients was $10751 F $598, payments
made to HC averaged $2393 F $92, and the
average compensation in professional fees was
$345 F $19 (Fig. 2).
The algorithm for calculation of national reha-
bilitation costs is depicted in Fig. 2. Based on
these calculations, approximately $3.4 billion are
spent annually on rehabilitation services after
arthroplasty.
Quality of Life and Postsurgical DischargeStatus
Table 2 presents the preoperative and the aver-
age 8.6-month postoperative mean quality of life
scores for patients discharged to the CRU and

Fig. 2. Algorithm for estimation of national arthroplasty postdischarge expenditures.
Postdischarge Costs in Arthroplasty Surgery ! Lavernia et al 147
patients discharged directly to home. There were
significant improvements in WOMAC function and
corresponding reductions in pain and stiffness
reported in both discharge groups. Quality of life
as measured by the QWB and the SF-36 also tended
Table 2. Changes in Presurgical and Postsurgical QualityPatients Dischar
Outcomes
CRU
Pre Post D
QWBy 0.552 0.576 0.023VASz pain intensity 6.5 0.9 5.6SF-36Physical function 25.8 50.0 24.1Role playing 31.3 58.3 27.1Bodily pain 52.7 61.8 9.1General health 65.7 75.2 9.5Vitality 67.5 62.5 5.0Social function 67.8 59.5 8.3Role emotional 61.1 61.1 0Mental health 61.0 73.3 12.3
WOMACFunction 33.7 8.2 25.5Pain 9.7 1.9 7.8Stiffness 3.3 1.0 2.3Total 46.7 11.1 35.6
*F test compares preoperative to postoperative change in CRU vs HyQuality of Well-Being Scale.zVisual Analog Scale.§P b .05.
to show improvement after surgery in both groups,
although there was a trend toward greater
improvements for patients discharged to home
health care on many of the SF-36 measures. With
1 exception, there were no significant differences in
of Life Indicators in Patients Discharged to a CRU vsged to HC
HC
F*Pre Post D
0.560 0.590 0.030 0.87.5 1.4 6.1 0.2
23.3 59.7 36.4 1.232.4 74.0 41.6 1.255.8 70.3 14.5 1.076.2 72.9 3.3 0.057.1 65.6 8.4 1.064.1 84.9 20.8 4.7§76.6 83.8 7.2 0.267.5 76.9 9.4 0.4
35.6 10.7 24.9 0.010.7 2.3 8.4 0.03.2 1.3 1.9 0.9
49.6 14.3 35.3 0.0
C patients after adjustment for age and sex.

148 The Journal of Arthroplasty Vol. 21 No. 6 Suppl. 2 September 2006
the relative rate of improvement on the WOMAC
and quality of life measures when comparing
patients discharged to the CRU and patients dis-
charged directly to home. Age- and sex-adjusted
SF-36 social function scores did improve signifi-
cantly more in home-discharged patients relative to
the CRU-discharged patients (t = 4.7, P b .05).
Discussion
Arthritis remains the leading cause of disability
in the United States; in addition, the number of
Americans with doctor-diagnosed arthritis contin-
ues to increase [17,18]. In individuals for whom
medical therapy has failed, joint arthroplasty sur-
gery has been shown to be a cost-effective inter-
vention resulting in pain relief and improved
quality of life [19-23]. After joint arthroplasty
surgeries, most individuals undergo some form of
rehabilitation, with treatment strategies focusing
on improving range of motion, increasing strength,
and improving ability to complete activities of daily
living safely and efficiently. Moreover, other allied
health professions such as physical and occupa-
tional therapy, nursing, and social services all play
a vital role in postsurgical rehabilitation.
A number of cost-effectiveness studies have
been published on specific interventions during
the acute phase of the arthroplasty procedures.
Lavernia et al [24] demonstrated that perioperative
x-rays in joint arthroplasty generated more than a
million dollars in radiologist’s fees with no apparent
influence on patient outcomes. Kocher et al [25]
demonstrated that pathologic analysis of postsurgi-
cal total joint arthroplasty specimens did not
contribute to patient outcomes; yet, it generated
costs in excess of $233 per case for THA surgeries
and $304 per case for TKA surgeries. Several other
studies have demonstrated the cost utility of
interventions in the acute phase of the arthroplasty
procedures [24-28]. To our knowledge, no infor-
mation exists on the rehabilitation costs and their
respective cost utility.
Some studies have focused on the timing of
rehabilitation and comparison of HC and outpa-
tient therapies. Mitchell et al [8] compared the
effectiveness of HC vs outpatient hospital rehabil-
itation services in individuals before and after
unilateral knee joint arthroplasty surgery. The
authors reported that similar outcomes, which
included WOMAC, SF-36, and patient satisfaction,
were achieved in both rehabilitation groups;
however, rehabilitation was more expensive when
administered at home. In contrast to this report,
there are 2 Canadian studies that documented
similar functional outcomes between home and
hospital groups, but that home-based rehabilita-
tion was less costly [7,29]. Our cost findings are
also consistent with those reported by Tran et al
[30]. They reported that 37 individuals of 97 pa-
tients discharged to home after joint arthroplasty
surgery had an average cost of $2479 per patient.
The authors also reported that in those discharged
to a rehabilitation hospital after joint arthroplasty
surgery, 42 of 51 individuals had an average cost
of $7768 per patient. In our study, we found that
HC services were less expensive when compared
with an acute care facility by approximately $8300
per patient, findings which are consistent with
these studies.
The literature on the postdischarge costs after
arthroplasty is extremely limited. In our study,
we found that the average cost per case on CRU
was $10751, and payments made to HC aver-
aged $2393.
Differences between SNF and CRU units include
the amount of time spent in therapy per day, the
nursing-to-patient ratio (CRU 5:1, SNF 30:1 in our
institution), and the number of allowed profes-
sional visits per stay by physical medicine and
rehabilitation specialists. All of the previously
mentioned factors increase the cost of these inter-
ventions. According to our estimates, approximate-
ly $3.2 billion are spent annually in rehabilitation
services after primary arthroplasty.
Constant surgical advances (ie, minimal invasive
surgery, pain management) have lowered the
average length of stay for primary arthroplasty.
New strategies that lower the cost and use of
hospital supplies have also contributed to decreased
intrahospital costs. Despite this focus on improved
outcomes and lower in-hospital costs, orthopedic
surgeons as well as hospital administrators are
generally unaware of arthroplasty postdischarge
expenditures. Cost utility studies are needed to
assess interventions in the post–acute care setting.
Our study raises the possibility that reducing
postdischarge costs by only 10% would result in
more than $250 million dollars in savings per year.
These cost-utility studies therefore could result in
substantial savings to partially offset costs associat-
ed with the increasing number of procedures.
A drawback in our study was that we estimated
national arthroplasty costs based on financial data
from a single surgical practice. Medical cost studies
in general have noted substantial geographic var-
iation with respect to expenditures [31]. It is
therefore possible that these costs at our institution
do underestimate or overestimate costs for the

Postdischarge Costs in Arthroplasty Surgery ! Lavernia et al 149
nation as a whole. Also, the average age of our
patient population was higher than was noted in
the NHDS, although we found no correlation
between age and postdischarge expenditures. Fi-
nally, we lacked direct cost data for patients
discharged to skilled nursing home facilities. Our
national cost estimates for this type of discharge
may be imprecise.
Clearly, postrehabilitative outcomes after joint
arthroplasty surgeries must be better defined in an
effort to provide meaningful treatments that are
efficient and cost-effective. In the coming years, it
will be necessary to identify evidence-based reha-
bilitation strategies that will promote functional
recovery after knee and hip joint arthroplasty as
quickly and safely as possible while maximizing
functional abilities. It is also important to select
the least expensive option under the scenario of
equally effective rehabilitative approaches. The
only way to truly evaluate the utility and cost-
effectiveness of these postsurgical rehabilitative
strategies is to perform well-designed multicenter
randomized clinical trials. These trials are not only
critical for maximizing patient outcomes, but may
also help to at least slow the growth of annual
expenditures associated with arthroplasty.
References
1. Kurtz S, Mowat F, Ong K, et al. Prevalence of
primary and revision total hip and knee arthroplasty
in the United States from 1990 through 2002. J Bone
Joint Surg Am 2005;87:1487.
2. Frankowski JJ, Watkins-Castillo S. Primary total
knee and hip arthroplasty projections for the
U.S. population to the year 2030. www.aaos.org/
wordhtml/research/stats/TJR_Projections.pdf [Last
accessed Sep 15, 2005].
3. Antoniou J, Martineau PA, Filion KB, et al. In-
hospital cost of total hip arthroplasty in Canada and
the United States. J Bone Joint Surg Am 2004;
86-A:2435.
4. Bozic KJ, Katz P, Cisternas M, et al. Hospital resource
utilization for primary and revision total hip arthro-
plasty. J Bone Joint Surg Am 2005;87:570.
5. Lavernia CJ, Drakeford MK, Tsao AK, et al. Revision
and primary hip and knee arthroplasty. A cost
analysis. Clin Orthop Relat Res 1995;136.
6. Coyte PC, Young W, Croxford R. Costs and outcomes
associated with alternative discharge strategies fol-
lowing joint replacement surgery: analysis of an
observational study using a propensity score. J Health
Econ 2000;19:907.
7. Kramer JF, Speechley M, Bourne R, et al. Compar-
ison of clinic- and home-based rehabilitation pro-
grams after total knee arthroplasty. Clin Orthop Relat
Res 2003;225.
8. Mitchell C, Walker J, Walters S, et al. Costs and
effectiveness of pre- and post-operative home phys-
iotherapy for total knee replacement: randomized
controlled trial. J Eval Clin Pract 2005;11:283.
9. Forrest GP, Roque JM, Dawodu ST. Decreasing
length of stay after total joint arthroplasty: effect on
referrals to rehabilitation units. Arch Phys Med
Rehabil 1999;80:192.
10. Department of Health and Human Services D and
Centers for Medicare & C. Medicaid Services, CMS.
Medicare IRF Classification Requirements. CMS
Manual System; 2004. Centers for Medicare &
Medicaid Services (CMS). Inpatient Rehabilitation
Facility Prospective Payment System and The 75
Percent Rule. www.cms.hhs.gov/InpatientRehab-
FacPPS/Downloads/DLSumIRFPPS_75pcrule.pdf
[Last accessed May 26, 2006].
11. DeFrances C, Hall M, Podgomik M. 2003 National
hospital discharge survey. http://www.cdc.gov/nchs/
data/ad/ad359.pdf [Last accessed Sep 23, 2005].
12. Bellamy N, Buchanan WW, Goldsmith CH, et al.
Validation study of WOMAC, a health status instru-
ment for measuring clinically important patient
relevant outcomes to antirheumatic drug therapy in
patients with osteoarthritis of the hip or knee.
J Rheumatol 1988;15:1833.
13. Arocho R, McMillan CA, Sutton-Wallace P. Con-
struct validation of the USA-Spanish version of the
SF-36 health survey in a Cuban-American popula-
tion with benign prostatic hyperplasia. Qual Life Res
1998;7:121.
14. Lieberman JR, Dorey F, Shekelle P, et al. Outcome
after total hip arthroplasty. Comparison of a tradi-
tional disease-specific and a quality-of-life measure-
ment of outcome. J Arthroplasty 1997;12:639.
15. Kaplan R, Bush J. Health-related quality of life
measurement for evaluation research and policy
analysis. Health Psychol 1982:1.
16. Feliz M. Personal Communication, C. Lavernia,
Editor. 2005: Miami.
17. Brooks PM. Impact of osteoarthritis on individuals
and society: how much disability? Social consequen-
ces and health economic implications. Curr Opin
Rheumatol 2002;14:573.
18. Buckwalter JA, Saltzman C, Brown T. The impact of
osteoarthritis: implications for research. Clin Orthop
Relat Res 2004;(427 Suppl):S6.
19. Laupacis A, Bourne R, Rorabeck C, et al. The effect
of elective total hip replacement on health-
related quality of life. J Bone Joint Surg Am 1993;
75:1619.
20. Liang MH, Cullen KE, Larson MG, et al. Cost-
effectiveness of total joint arthroplasty in osteoar-
thritis. Arthritis Rheum 1986;29:937.
21. Liang MH, Larson M, Thompson M, et al. Costs and
outcomes in rheumatoid arthritis and osteoarthritis.
Arthritis Rheum 1984;27:522.

150 The Journal of Arthroplasty Vol. 21 No. 6 Suppl. 2 September 2006
22. Rorabeck CH, Bourne RB, Laupacis A, et al. A
double-blind study of 250 cases comparing
cemented with cementless total hip arthroplasty.
Cost-effectiveness and its impact on health-related
quality of life. Clin Orthop Relat Res 1994;156.
23. Lavernia CJ, Guzman JF, Gachupin-Garcia A. Cost
effectiveness and quality of life in knee arthroplasty.
Clin Orthop Relat Res 1997;134.
24. Lavernia CJ, Hernandez RA, Rodriguez JA. Perioper-
ative X-rays in arthroplasty surgery: outcome and
cost. J Arthroplasty 1999;14:669.
25. Kocher MS, Erens G, Thornhill TS, et al. Cost and
effectiveness of routine pathological examination of
operative specimens obtained during primary total
hip and knee replacement in patients with osteoar-
thritis. J Bone Joint Surg Am 2000;82-A:1531.
26. Healy JC, Frankforter SA, Graves BK, et al. Preoper-
ative autologous blood donation in total-hip arthro-
plasty. A cost-effectiveness analysis. Arch Pathol Lab
Med 1994;118:465.
27. Iorio R, Whang W, Healy WL, et al. The utility of
bladder catheterization in total hip arthroplasty. Clin
Orthop Relat Res 2005:148.
28. Sonnenberg FA, Gregory P, Yomtovian R, et al. The
cost-effectiveness of autologous transfusion revisited:
implications of an increased risk of bacterial infection
with allogeneic transfusion. Transfusion 1999;
39:808.
29. Williams JI, Mahomed N, Chapeskie KK. Shorter
waiting times for hip and knee replacement on the
horizon. Hosp Q 2000;4:21.
30. Tran V, Doctor D, Nelson C, et al. The cost of
postoperative home health extended care rehabili-
tation facilities for total joint replacement patients.
American Academy of Orthopaedic Surgeons An-
nual Meeting; 1999.
31. Fisher ES, Wennberg DE, Stukel TA, et al. The
implications of regional variations in Medicare
spending. Part 1: The content, quality, and accessi-
bility of care. Ann Intern Med 2003;138:273.







