Download - GLOMERULAR DIS BU 2016 Lec 1 \u0026

Glomerular Diseases
Prof. Mohiuddin Alamgir


Low-power electron micrograph of renal glomerulus. CL, capillary lumen; EP, visceral epithelial cells with foot processes; END, endothelium; MES, mesangium. B, Schematic representation of a glomerular lobe.


Glomerular filter consisting, from bottom to top, of fenestrated endothelium, basement membrane, and foot processes of epithelial cells. Note the filtration slits (arrows) and diaphragm situated between the foot processes. Note also that the basement membrane consists of a central lamina densa, sandwiched between two looser layers, the lamina rara interna and lamina rara externa.

Primary glomerulopathies
Acute proliferative glomerulonephritis
Post-infectious Other
Rapidly progressive (crescentic) glomerulonephritis Membranous glomerulopathy Minimal-change disease Focal segmental glomerulosclerosis Membranoproliferative glomerulonephritis IgA nephropathy Chronic glomerulonephritis

Systemic diseases with glomerular involvment Systemic lupus erythematosus
Diabetes mellitus Amyloidosis Goodpasture syndrome Microscopic polyarteritis/polyangiitis Wegener granulomatosis Henoch-Schonlein purpura Bacterial endocarditis
Hereditary disorders Alport syndrome
Thin basement membrane disease Fabry disease
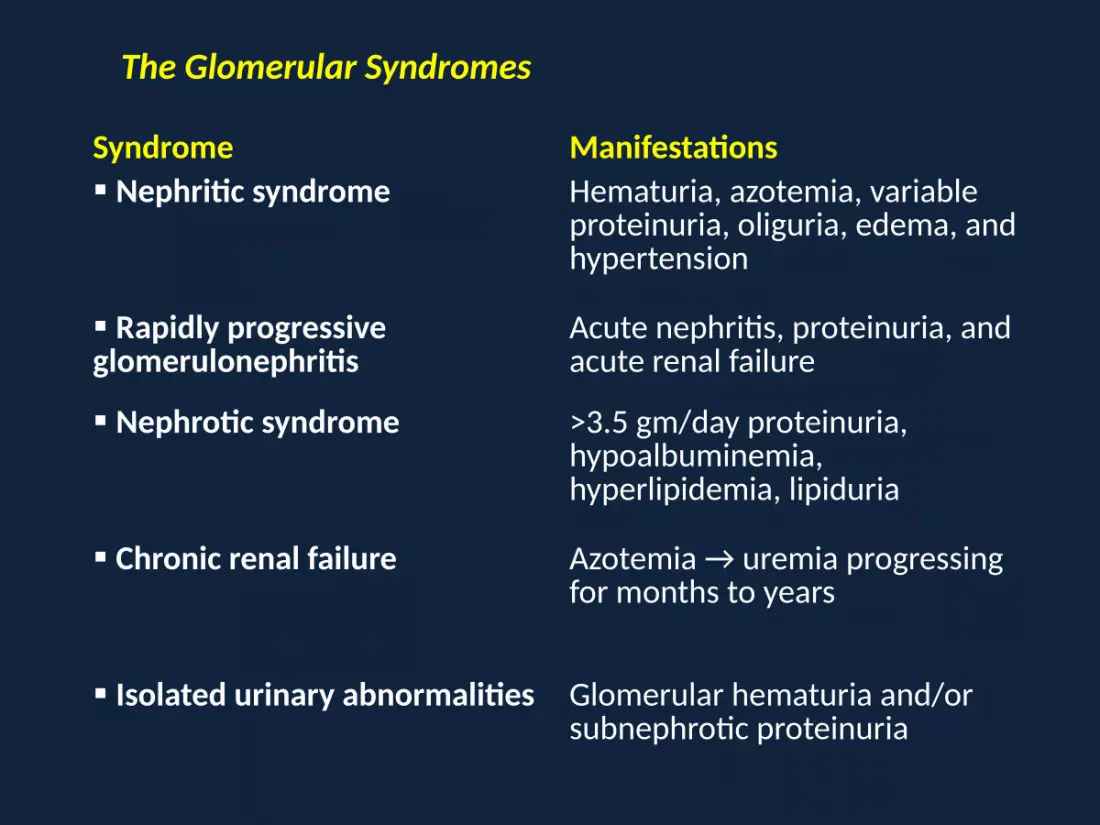
Syndrome Manifestations Nephritic syndrome Hematuria, azotemia, variable
proteinuria, oliguria, edema, and hypertension
Rapidly progressive glomerulonephritis
Acute nephritis, proteinuria, and acute renal failure
Nephrotic syndrome >3.5 gm/day proteinuria, hypoalbuminemia, hyperlipidemia, lipiduria
Chronic renal failure Azotemia → uremia progressing for months to years
Isolated urinary abnormalities Glomerular hematuria and/or subnephrotic proteinuria
The Glomerular Syndromes

Histologic alterations
Hypercellularity
Increase in the number of cells in the glomerular tufts
• Cellular proliferation of mesangial or endo. cells
• Leukocytic infiltration consisting of neutrophils, monocytes, and, in some diseases, lymphocytes
• Formation of crescents

Acute proliferative glomerulonephritis. A, Normal glomerulus. B, Glomerular hypercellularity is due to intracapillary leukocytes and proliferation of intrinsic glomerular cells. C, Typical electron-dense subepithelial “hump” and a neutrophil in the lumen. D, Immunofluorescent stain demonstrates discrete, coarsly granular deposits of complement protein C3, corresponding to “humps” illustrated in part C.

Basement membrane thickening
Appears as thickening of the capillary walls with PAS stain By electron microscopy : two forms • Deposition of amorphous electron-dense material, most
often immune complexes, on the endothelial or epithelial side of the basement membrane or within the GBM itself. Fibrin, amyloid, cryoglobulins, and abnormal fibrillary proteins may also deposit
• Thickening of the basement membrane due to increased synthesis of its protein components, as occurs in diabetic glomerulosclerosis

Membranous nephropathy. A, Silver methenamine stain.-marked diffuse thickening of the capillary walls without an increase in the number of cells. There are prominent “spikes” of silver-staining matrix (arrow) projecting from the basement membrane lamina densa toward the urinary space, which separate and surround deposited immune complexes that lack affinity for the silver stain. B, Electron micrograph showing electron-dense deposits (arrow) along the epithelial side of the basement membrane (B). Note the effacement of foot processes overlying deposits. C, Characteristic granular immunofluorescent deposits of IgG along GBM. D, Diagrammatic representation of membranous nephropathy.

Hyalinosis
• Accumulation of material that is homogeneous and eosinophilic by light microscopy
• By EM hyalin is extracellular and amorphous, made up of plasma proteins that have insudated from circulation
• When extensive, this change contributes to obliteration of the capillary lumens of the glomerular tuft
• Hyalinosis is a consequence of endothelial or capillary wall injury and typically the end result of various forms of glomerular damage.
• It is a common feature of focal segmental glomerulosclerosis

focal segmental glomerulosclerosis (FSGS)

Sclerosis
• Accumulations of extracellular collagenous matrix, either confined to mesangial areas (DM) in diabetic glomerulosclerosis, or involving the capillary loops, or both
• Results in obliteration of some or all of the capillary lumens in affected glomeruli, leads to formation of fibrous adhesions between the sclerotic portions of glomeruli and parietal epithelium and Bowman capsules

focal segmental glomerulosclerosis (FSGS)

Immune mechanisms of glomerular injury
ANTIBODY-MEDIATED INJURY
IN SITU IMMUNE COMPLEX DEPOSITION
Fixed intrinsic tissue antigens - anti-GBM nephritis
Heymann antigen - membranous glomerulopathy
Mesangial antigens Planted antigens
Exogenous (infectious agents, drugs)
Endogenous (DNA, nuclear proteins, immuno- globulins, immune complexes, IgA)

CIRCULATING IMMUNE COMPLEX DEPOSITION
Endogenous antigens (e.g., DNA, tumor antigens)Exogenous antigens (e.g., infectious products)
CYTOTOXIC ANTIBODIES
CELL-MEDIATED IMMUNE INJURY
ACTIVATION OF ALTERNATIVE COMPLEMENT PATHWAY

Immune Complex Deposition Involving Intrinsic and in Situ Renal Antigens
Two patterns of deposition of immune complexes as seen by immunofluorescence microscopy: granular, characteristic of circulating and in situ immune complex nephritis (D), and linear, characteristic of classic anti-GBM disease (E).

Antibodies against Planted Antigens
• Planted antigens include cationic molecules that bind to anionic components of the glomerulus
• e.g., DNA, nucleosomes, and other nuclear proteins, bacterial products, large aggregated proteins e.g., aggregated immunoglobulins.
• Viral, bacterial, and parasitic products and drugs
• Detected as granular staining by immunofluorescence microscopy, as in circulating immune complex nephritis

Anti-GBM Antibody–Induced Glomerulonephritis
• Antibodies are directed against intrinsic fixed antigens that are normal components of the GBM proper
• Abs bind along the entire length of the GBM, resulting in a diffuse linear pattern on immuno-fluorescence
• Cross-react with other basement membranes, e.g. lung alveoli, resulting in simultaneous lung and kidney lesions (Goodpasture syndrome)
• Accounts for < 5% of cases of glomerulonephritis.

Circulating Immune Complex Glomerulonephritis
• Trapping of circulating antigen-antibody complexes within glomeruli.
Microbial antigens: • bacterial products (streptococci)• surface antigen of hepatitis B virus• hepatitis C virus antigens• antigens of Treponema pallidum• Plasmodium falciparum antigen• viruses & some tumor antigens• Unknown antigen

Localization of immune complexes in the glomerulus
(1) Subepithelial humps, as in acute glomerulonephritis
(2) Epimembranous deposits, as in membranous nephropathy
and Heymann glomerulonephritis
(3) Subendothelial deposits, as in lupus nephritis and
membranoproliferative glomerulonephritis
(4) Mesangial deposits, as in IgA nephropathy

Localization of immune complexes in the glomerulus: (1) subepithelial humps, as in acute glomerulonephritis; (2) epimembranous deposits, as in membranous nephropathy and Heymann glomerulonephritis; (3) subendothelial deposits, as in lupus nephritis and membranoproliferative glomerulonephritis; (4) mesangial deposits, as in IgA nephropathy; (5) basement membrane.

Antibodies in Glomerular Dis.
• Abs to mesangial cell antigens cause mesangial cell prolif.
• Abs to endothelial cell antigens cause intravascular thrombosis
• Abs to certain visceral epithelial cell components cause proteinuria

Cell-Mediated Immunity in GN
• Abs to GBM may initiate glomerular injury but activated T lymphocytes propagate the inflammation
• Sensitized T cells are involved in the progression of many glomerulonephritides.
• Presence of activated macrophages and T cells and their products in the glomerulus in e.g. Crescentic glomerulonephritis

Activation of Alternative Complement Pathway
• Alternative complement pathway activation occurs in the
clinico-pathologic entity called dense-deposit disease,
also referred to as membranoproliferative
glomerulonephritis (MPGN type II)
• It may also occur in some forms of proliferative GN

Soluble Mediators
The chemotactaxis - C5b-C9 (MAC)
C5b-C9 causes cell lysis & stimulates mesangial cells to produce oxidants, proteases. Cause proteinuria as in MGN
Eicosanoids, nitric oxide, angiotensin, endothelin → hemodynamic changes
Chemokines promote monocyte & lymphocyte influx
Growth factors: PDGF → mesangial cell proliferation TGF-β, connective tissue GF & FGF → ECM deposition and hyalinization The coagulation system : Fibrin – parietal epithelial cell proliferation (crescent formation).
• Currently, the most successful interventions to interrupt these mechanisms of progressive glomerulosclerosis involve treatment with inhibitors of the renin-angiotensin system.
• There is inability of mature visceral epithelial cells (podocytes) to proliferate after injury .
• Remaining podocytes are either abnormally stretched to maintain an appropriate filtration barrier or unable to cover portions of the GBM.


Mechanism of progression in glomerular diseases

Mechanisms of progression in glomerular diseases
• Glomerular hypertrophy → increases in glomerular blood flow, filtration, → glomerular hypertension & often systemic HTN
• Endothelial/ epithelial cell injury → increased glomerular permeability to proteins, and accumulation of proteins in the mesangial matrix.
• Proliferation of mesangial cells, infiltration by macrophages, increased accumulation of extracellular matrix (ECM),
→ segmental and eventually global sclerosis of glomeruli

Tubulointerstitial Fibrosis
• Indeed, there is often a much better correlation of decline in renal function with the extent of tubuloin-terstitial damage than with the severity of glomerular injury
• Contributing factors are ischemia of tubule segments downstream from sclerotic glomeruli, acute and chronic inflammation in the adjacent interstitium, and damage or loss of the peritubular capillary blood supply

Disease
Most Frequent Clinical Presentation Pathogenesis
Light Microscopy
Fluorescence Microscopy
Electron Microscopy
Postinfectious glomerulonephritis
Nephritic syndrome
Immune complex mediated; circulating or planted antigen
Diffuse endocapillary proliferation; leukocytic infiltration
Granular IgG and C3 in GBM and mesangium
Subepithelial humps
Goodpasture syndrome
Rapidly progressive glomerulonephritis
Anti-GBM COL4-A3 antigen
Extracapillary proliferation with crescents; necrosis
Linear IgG and C3; fibrin in crescents
No deposits; GBM disruptions; fibrin
Chronic glomerulonephritis
Chronic renal failure
Variable Hyalinized glomeruli
Granular or negative
Membranous glomerulopathy
Nephrotic syndrome
In situ immune complex formation; antigens mostly unknown
Diffuse capillary wall thickening
Granular IgG and C3; diffuse
Subepithelial deposits
Minimal-change disease
Nephrotic syndrome
Unknown; loss of glomerular polyanion; podocyte injury
Normal; lipid in tubules
Negative Loss of foot processes; no deposits

Case-1
A 25 year old woman experiences sudden onset of fever,
malaise and nausea. On physical examination, temp. 38.2°C,
pulse 85/min., RR 18/min., and BP: 140/90 mmHg. Urine
analysis shows 1+proteinuria, 4+ hematuria, & no ketones or
glucose. RBC casts are seen. Renal biopsy reveals marked
glomerular hypercellularity with neutrophils in glomerular
capillary loop. Immunoflourescence microscopy shows
granular deposition of IgG & C3 in GBM. Electron
microscopy shows electron-dense subepithelial “humps”.

Acute proliferative glomerulonephritis. A, Normal glomerulus. B, Glomerular hypercellularity is due to intracapillary leukocytes and proliferation of intrinsic glomerular cells. C, Typical electron-dense subepithelial “hump” and a neutrophil in the lumen. D, Immunofluorescent stain demonstrates discrete, coarsly granular deposits of complement protein C3, corresponding to “humps” illustrated in part C.

Case-2
A 7-year old boy is recovering from impetigo. Physical examination shows a few honey-colored crusts on his face. The crusts are removed, and a culture of lesions grows group A Streptococcus pyogenes. He is treated with a course of antibiotics. One week later he develops malaise with nausea and a slight fever and passes dark brown urine. Lab. shows a serum anti-streptolysin O (ASO) titre of 1:1024. Subsequently, the boy shows complete recovery without treatment.

Nephritic syndromeGlomerular diseases presenting with a nephritic syndrome are oftencharacterized by inflammation in the glomeruli
Hematuria, red cell casts in the urine, azotemia, oliguria, and mild tomoderate hypertension
Proteinuria and edema are common, but these are not as severe asin nephrotic syndrome
It is characteristic of acute proliferative glomerulonephritis and is animportant component of crescentic glomerulonephritis

Acute Proliferative (Poststreptococcal, Postinfectious) Glomerulonephritis
Diffuse proliferation of glomerular cells, associated with influx of leukocytes
Lesions are typically caused by immune complexes
The inciting antigen may be exogenous or endogenous.
Exogenous antigen -- post-infectious glomerulonephritis
Endogenous antigen-- nephritis of SLE
The most common underlying infections are streptococcal
Disorder also has been associated with other infections

Clinical course
• A young child abruptly develops malaise, fever, nausea, oliguria, and hematuria (smoky or cola-colored urine) 1 to 2 weeks after recovery from a sore throat
• The patients have red cell casts in the urine, mild proteinuria (usually less than 1 gm/day), periorbital edema, and mild to moderate hypertension.
• In adults the onset is more likely to be atypical, such as the sudden appearance of hypertension or edema, frequently with elevation of BUN
• Important laboratory findings include elevations of antistreptococcal antibody titers and a decline in the serum concentration of C3 and other components of the complement cascade.

• More than 95% of affected children eventually recover totally with conservative therapy
• A small minority of children (perhaps fewer than 1%) do not improve, become severely oliguric, and develop a rapidly progressive form of glomerulonephritis
• In adults only about 60% of sporadic cases do the patients recover promptly
• In the remainder the glomerular lesions fail to resolve quickly, as manifested by persistent proteinuria, hematuria, and hypertension.
• In some of these patients, the lesions eventually clear totally, but others develop chronic glomerulonephritis.

Case-3
A 47-year old man has had a decreased urine output over
the past 10 days accompanied by hemoptysis. On physical
examination, he is afebrile. Urinalysis shows 1+ proteinuria,
4+ hematuria, urobilinogen, and no glucose or ketones.
Microscopic examination of urine shows few WBCs and
some RBCs with RBC casts. A renal biopsy is performed
which shows collapsed glomerular tufts and the crescent-
shaped mass of proliferating parietal epithelial cells and
leukocytes internal to Bowman capsule.

Crescentic glomerulonephritis (PAS stain). Note the collapsed glomerular tufts and the crescent-shaped mass of proliferating parietal epithelial cells and leukocytes internal to Bowman capsule.

RAPIDLY PROGRESSIVE (CRESCENTIC) GLOMERULONEPHRITIS
• RPGN is a syndrome associated with rapid and progressive loss of renal function associated with severe oliguria and signs of nephritic syndrome
• If untreated, death from renal failure occurs within weeks to months.
• Crescents are produced by the proliferation of the parietal epithelial cells lining Bowman capsule and by the infiltration of monocytes and macrophages

Rapidly Progressive Glomerulonephritides
TYPE I (ANTI-GBM ANTIBODY)Renal limited Goodpasture syndrome
TYPE II (IMMUNE COMPLEX)Idiopathic Post-infectious glomerulonephritis Lupus nephritis Henoch-Schönlein purpura (IgA nephropathy) Others
TYPE III (PAUCI-IMMUNE)
ANCA-associated Idiopathic Wegener granulomatosis Microscopic polyangiitis

The first type of RPGN is anti-GBM antibody–induced disease, characterized by linear deposits of IgG and, in many cases, C3 in
the GBM that are visualized by immunofluorescence
The second type of RPGN is the result of immune complex deposition
The third type of RPGN, also called pauci-immune type, is defined by the lack of anti-GBM antibodies or immune complexes but having circulating antineutrophil cytoplasmic antibodies (ANCAs)

MORPHOLOGY
Kidneys are enlarged, pale, with petechial hemorrhages on corticalsurfaces
The crescents eventually obliterate Bowman space & compress theglomerular tuft
By immunofluorescence microscopy:
- Immune complex–mediated cases show granular immune deposits- Goodpasture syndrome cases show linear GBM fluorescence for
Ig & complement- Pauci-immune cases -- little or no deposition of immune reactants
Clinical course
Renal involvement is usually progressive over a matter ofweeks and culminates in severe oliguria
Recovery of renal function may follow early intensiveplasmapheresis (plasma exchange) combined withsteroids and cytotoxic agents

Case-4
A 6-year-old previously healthy girl has become increasingly
lethargic over the past two weeks. On physical examination,
she as puffiness around her eyes. Her temp. is 37°C, and BP:
100/60 mmHg. Labs show serum creatinine of 0.7mg/dl &
urea nitrogen of 12mg/dl. Urinanalysis shows pH of 6.5, Sp gr.
1.1011, 4+ proteinuria, no blood or glucose. 24-hour urine
protein of 3.8 g. EM shows effacement of podocyte foot
process. This child’s condition improves after a course of
corticosteroid therapy.

PRIMARY GLOMERULAR DISEASE % age in children % age in Adults
Membranous glomerulopathy 5 30
Minimal-change disease 65 10
Focal segmental glomerulosclerosis 10 35
Membranoproliferative 10 10
Nephrotic syndrome in children & adults







