Download - Facing HIV /AIDS Prevention

1
DRAFT VERSION
Facing HIV /AIDS Prevention
Cristina Pimenta1; Ivo Brito2; Pedro Chequer 3
Introduction
We are thirty years into the global epidemic and important progress has been achieved in
all areas relating to the production of knowledge on HIV and AIDS. The epidemic has been
scrutinized in terms of the social and epidemiological determinants relating to its spatial
dissemination and its dissemination among more vulnerable population groups. Knowledge
gained regarding the structure, the plasticity, and the molecular dynamics of the virus has
enabled important decisions to be taken as to the clinical management of patients and the
production of medicines such as anti-retroviral drugs (ARVs) and other pharmaceutical products.
Relevant progress has also been made in increasing the control and safety of blood and blood
products. The importance of achievements related to prevention of vertical transmission should
also be emphasized as effective and low cost prevention therapy even though it is still not
universally available to pregnant women throughout the globe.
This knowledge has provided substantial foundations for building prevention practices.
However, despite the progress achieved in these different areas, the scope of the response in
terms of behavior change and prevention have shown themselves to be clearly necessary. We
have learned that it is insufficient to deal with the complexity of cultures, sexual arrangements,
and social practices relating to drug use and the contexts of living with HIV.
Over time, such insufficiencies reinforce certain positions and bring with them a wave of
conservatism, taking the debate away from the field of science and into the field of moral beliefs.
Accumulated experience has shown us the importance of prevention as an area of knowledge
that involves both political and technical decisions in the arena of public health. It should be
remembered that initial confrontations of the disease arose with prejudice and stigma with many
people having the idea that the epidemic reproduced itself only within a restricted group of
people, who had homosexual practices, who were engaged in commercial sex or who practiced
injection drug use. For a long time prevention was, therefore, focused on the so-called high risk
groups and the measures taken were basically a combination of the promotion of safe sex and
behavior changes.

2
Notwithstanding, the strength of the community response must be recognized, especially
that of the gay movement and the movement of sex workers, drug users and, later, the networks
of people living with HIV/AIDS, who mobilized themselves to promote human rights issues and to
fight stigma and discrimination. This mobilization has been decisive for the formulation of
inclusive citizen-based public policies. It is within communities that the social movement takes the
initiative to ensure that people have attention and protection. Experiences of great significance for
prevention practices have emerged from this community experience.
This article seeks to situate the debate that has been built around prevention practices
during these thirty years of the epidemic, so as to identify major theoretical approaches,
strategies and the principal political tendencies.
1. AIDS initial moments: between silence and prevention
In the early 1980s the world came face to face with an “outbreak” of a rare and unknown
disease of epidemic proportions. The overall clinical condition of the patients seeking health
services caught the attention of medical professionals, in that it was a very special kind of total
failure of the defense system thus far not described by medical literature, and which left these
patients vulnerable to other opportunistic diseases. Initially, it was thought that it was a very
particular syndrome that affected, especially, men involved sexually with other men. Based on
this situation and the initial diagnosis of the cases, the new disease became known as the “gay
cancer”, among other terms such as, for example, “Gay-Related Immune Deficiency” (GRID),
referred in an article published in the Lancet in 19814. In the same year a case was reported
among injecting drug users5, undermining the hypothesis that the new disease was restricted to
homosexuals. Given these circumstances and the appearance of cases among hemophiliacs and
female partners of hemophiliacs, a trend arose towards seeking a more generic nomenclature
within a context of strong pressure from the gay movement.
In 1982, the Atlanta Centers for Disease Control and Prevention then adopted the
denomination of Acquired Immune Deficiency Syndrome (AIDS)6. A study indicated that the
epidemic could have begun in 1976 in Uganda. The term AIDS was used for the first time in a
new article published in the M orbidity and M ortality Weekly Report (M M WR), entitled "Current
Trends Update on Acquired Immune Deficiency Syndrome (AIDS) - United States". The CDC
linked the transmission of the disease to contact with the blood of infected people. In M ay of the
same year the New York Times published an article “New Homosexual Disorder Worries Health
3
Officials”7, stating that the appearance of the new disease was a huge threat to public health and
that its probable causes were unknown. The new disease became known as AIDS and, at least
partially, distanced itself from the concept of the “gay plague”, becoming more extensive and
associated with risk behaviors and exposure to contaminated blood.
Globally, prevention of HIV/AIDS infection policies can be seen to have become a priority
in the mid 1980s. AIDS epidemic prevention proposals in countries determined to act rapidly to
the perceived emergency involved the programming of actions through projects and proposals to
control the new epidemic. An epidemic initially understood from a purely epidemiological
viewpoint8, which linked the acquired immune deficiency syndrome to certain population groups
and associated risk behaviors, as well as the context of individual responsibility for preventing
infection which, to a certain extent, was imposed by the unexpected and devastating nature of the
epidemic itself.
Later, in the early 1990s, with the epidemic now installed and better understood, and with
the aim of responding to specific questioning from health, social and basic science professionals,
global efforts were directed by WHO Global Programme on AIDS (GPA created early 1980’s) and
then by the Joint United Nations Programme on HIV/AIDS (UNAIDS created in 1996) to build
references for government and civil society programs and actions. HIV prevention policies and
guidelines began to focus on the creation of “prevention packages” and approaches “proven” to
be able to produce foreseeable effects such as approaches based on knowledge and behavioral
changes. At the same time, in countries where social movements had been valued since the
beginning of the epidemic, prevention and protection approaches benefited from civil society
efforts to promote the citizenship and the civil and human rights of people living with HIV/AIDS.
The concept of prevention adopted in the first decade of responses to the epidemic
(1982-94) referred principally to the primary prevention of HIV infection comprised, therefore, of
two levels: health promotion involving information and education on HIV transmission routes and
specific protection, basically through the use of barrier methods (condoms) to prevent sexual
transmission, and for injecting drug users by not sharing sharp objects or needles and syringes
and, the medical services using disposable or sterilized syringes and needles. During the early
years of the epidemic integral care was neither understood nor prioritized. The emphasis of
prevention guidance was based on what one should not do: not have sex, (principally anal sex),
men not having sex with men, not using drugs, not receiving blood, etc.
As the epidemic spread above all among men through sexual contact (homo and
bisexual populations) in the early 1980s in the Americas (United States, M exico, Brazil), and in
4
other countries in Europe, Asia, public health programs and community groups launched mass
campaigns for the general population or campaigns aimed at male homosexuals about HIV
transmission and prevention in an attempt to control the disease.
In 1983 in the United States, the Centers for Disease Control and Prevention (CDC)
launched the first guide “Safer Sexual Practices” (CDC, 1983) for men having sex with men,
establishing a conceptual basis for behavior-based prevention work in several countries. At the
end of the 1980s, health educators, together with activists and representatives of gay
communities in several countries (such as San Francisco and New York in the United States and
São Paulo and Rio de Janeiro in Brazil), developed and implemented countless programs and
projects to provide information, motivation and the development of personal skills and abilities
aimed at preventing HIV/AIDS transmission, in parallel to measures to control the quality of blood
and blood products.
During this period the first explanations were provided on how the disease is transmitted
and the definition was reached that the main transmission routes were blood and contact with
secretions during unprotected sexual intercourse. Only later the presence of HIV in breast milk
was identified and the possibility of breastfeeding transmission registered. As the number of
cases reported in women increased, principally the partners of injecting drug users, the first cases
of mother-to-child transmission during pregnancy or delivery were observed.
Towards the end of the 1980s, drug user treatment and detoxification centers began to
offer information and education on HIV/AIDS. Later, community outreach programs were
implemented to reach sex workers (principally women) and injecting drug users, considered as
“risk groups” (Turner, M iller and M oses, 1989).
Two characteristics can be seen in the medical discourse of the period, differentiating
prejudice and stigma regarding the new disease when compared to other diseases and
epidemics of the past. One of these characteristics in relation to sexuality is conservative and
contrary to the trend towards sexual liberation that had begun in the 1960s and had become
consolidated politically in the feminist and gay movements in the second half of the 1970s. This
discourse saw AIDS as the “punishment” for the tendency towards sexual liberation present in
contemporary society. The second characteristic is more important, since it perceives the
problem of AIDS related to sexuality not as a generic and abstract problem, but rather as “socially
discriminated forms of sexuality”, deviant forms incompatible with normal sexual behavior. This
medical and social normalization arose as a counterpoint aimed at controlling “sexual deviants”

5
and “social deviants” or drug users and, based on this, established prevention measures for risk
groups (Kenneth de Camargo, 1994)9.
Despite there being sufficient evidence that the epidemic was not restricted solely and
exclusively to groups considered to be risk groups, major disease control agencies in various
countries continued to defend the argument that it was a very specific epidemic concentrated in
those groups and that, therefore, a natural gap would prevent it from spreading to the general
population. This normative and behavioral reference became incorporated into prevention
practice approaches. A set of mechanisms seeking to investigate the sexual behavior of these
groups was brought into operation with initial cohort studies and, consequently, prevention
strategies were designed mostly seeking to intervene based on a normative perspective of
sexuality.
It was based on cognitive – rational approaches centered on the concept of risk groups – that
behavioral theories were incorporated into prevention initiatives. This focus influenced prevention
practices for many years and became the theoretical reference for most national programs
throughout the world. Thus an arsenal of normative mechanisms was put into practice in the field
of prevention, aimed at disciplining and regulating people’s sexual practices10.
In the early 1990s it was recognized that information and education efforts to prevent and
reduce the risk of infection should also be extended to young adults and adolescents, as well as
to the general population, considering the extension of the epidemic in countries where
traditionally there were no homosexual relations, and to female non drug users, and that
secondary and tertiary prevention should also be incorporated11.
At the time, socially constructed concepts of sexuality and vulnerability began to be
developed by scholars and public health officials. It can been seen, however, that the prevention
measures developed in the 1980s and 1990s were directed exclusively towards meeting the
public health needs of HIV negative people. At that time, care for people living with HIV/AIDS was
primarily of a curative or social welfare nature.
Consequently, throughout the 1990s progress was observed in controlling the epidemic in
various regions of the world such as in Thailand in Asia, Uganda in Africa and Brazil in the
Americas, with the continuous practice of safer sex activities, such as reduced number of sex
partners, increased male condom use and the introduction of the female condom as an
alternative (albeit with limited access) and syringe and needle exchange for injecting drug users,
as well as the incorporation of bio-safety standards to reduce accidents in the workplace as
6
reported by UNAIDS and referred by many authors (UNAIDS Global Report 2004,2006,
M esquita & Seibel, 2000).
An annual report recently released by the Joint United Nations Programme on HIV/AIDS
(UNAIDS) and the World Health Organization (WHO) highlights that HIV prevention programs are
making a difference (UNAIDS report, 2009). As expressed by Executive Director of UNAIDS,
M ichel Sidibé: “The good news is that we have evidence that the declines we are seeing are due,
at least in part, to HIV prevention. However, the findings also show that prevention programming
is often off the mark and that if we do a better job of getting resources and programs to where
they will make most impact, quicker progress can be made and more lives saved.”
Nevertheless, at the beginning of the third decade of the epidemic, HIV infection continues to
spread and to affect poorer population groups and previously unaffected groups, including the
female population and younger people throughout the world. The UNAIDS 2009 report estimates
that 33.4 million [31.1 million–35.8 million] people are living with HIV worldwide; 2.7 million [2.4
million–3.0 million] people were newly infected in 2008; and that 2 million [1.7– 2.4 million] people
died of AIDS related illness in 2008. The data brings us to the ultimate question: what have we
done right in respect to prevention approaches and strategies and what can be done to
accelerate progress in the control of the epidemic globally?
2. Prevention Strategies and Approaches
2.1– Cognitive-behaviorist theories in the field of HIV prevention
Prevention strategies disseminated by the public health normative agencies and
incorporated by health services and non-governmental organizations particularly in the 1980s and
1990s were fundamentally based on individual behavior change with regard to sexual practices or
in relation to the sharing of syringes and needles among injecting drug users.
M any of the original works outlining the major theories that are the basis for current
knowledge about behavioural change theories were published in the 1970s and 1980s. These
include Icek Ajzen’s12 articles on the Theories of Reasoned Action and Planned Behavior, Albert
Bandura’s writings on Social Cognitive Theory, and James Prochaska and Carlo DiClemente’s
works on the Transtheoretical M odel. M ore recently, interest in behavioural change theories has
arisen due to their application in the areas of health, education, and criminology, leading to further
research backed by institutions like the National Institutes of Health and the UK Prime M inister's

7
Strategy Unit. With this renewed interest, however, there is also a shift towards research into
understanding the maintenance of behavioural change in addition to broadening the research
base for revising current theories that focus on initial change. M ost of the models used for initial
HIV prevention approaches were based on one or more of the following theoretical references: a)
Health Belief M odel - HBM - Janz, N.K., and Becker, M .H.(1984); Rosenstock, Strecher and
Becker (1994)13; b) Social Cognitive Learning Theory – Bandura, A. (1989);Castiel L.D. (1996);
and c) Theory of Reasoned Action - Ajzen and Fishbein (1975 & 1980); and d) The AIDS Risk
Reduction M odel (ARRM ) - Catania, Kegeles and Coates,( 1990) 14 .
a) Health Belief M odel - HBM -This approach assumes that people’s attitudes and beliefs
influence their health status, given that in everyday life they face situations that require decisions
in the light of the threat or risk of contracting a disease and, consequently, their evaluation of the
medical and social resources available to them, such as health services, correct information and
guidance and prevention commodities. That is to say, when an individual has been the subject of
an action intended to change behavior, they feel capable of perceiving the benefits and the
barriers with regard to their behavior.
The principal criticism to this model is that it focuses all its action on the individual,
completely ignoring other factors that influence health related behavior, such as socio-economic
factors, the social norms of the group to which a person belongs and, the social representations
of ways of coping with illness and death. This model does not allow for the comprehension of the
health-illness process as a socially experienced and shared condition and, therefore, is unable to
situate itself within the context of the culture that involves a set of social experiences, repertories
and dramas that cause great impact on the family structure, people’s emotional relationships and
networks of social interaction.
b) Social Cognitive Learning Theory is a learning theory based on the ideas that people learn by
watching what others do (modeling) and that human thought processes are central to
understanding personality. While social cognitists agree that there is a fair amount of influence on
development generated by learned behavior displayed in the environment in which one grows up,
they believe that the individual person (and therefore cognition) is just as important in determining
moral development( Bandura ,1989) 15. People learn by observing others, with the environment,
behavior, and cognition all as the chief factors in influencing development. These three factors
are not static or independent; rather, they are all reciprocal. For example, each behavior

8
witnessed can change a person's way of thinking (cognition). Similarly, the environment one is
raised in may influence later behaviors.
This model prioritizes the stages of learning in adopting safer sex practices. According to
Castiel, the learning stages include: 1) the moment when behavior change starts; 2) the
measurement of the efforts made; and 3) the duration of efforts in the face of obstacles 16. The
author points out that one of the weakest points of this approach is the fact that its inducing guilt
and victimization in individuals or “cultural” groups who have risk practices. The sequence of the
learning process is said to be directly related to the individual’s possible cognitive capacity to
judge what is right and what is wrong and, therefore, decide on the most appropriate behavior in
the face of risk situations.
Social Cognitive Theory is applied today in many different arenas, such as mass media,
public health, education, and marketing. A familiar example is the use of celebrities to endorse or
promote products or conducts suh as condom use to certain segments of the population. By
choosing the proper gender, age, and ethnicity the use of social cognitive theory is said to help
ensure the success of an AIDS campaign to urban city youth by promoting identity with a
recognizable peer, a greater sense of self-efficacy, and then imitate the actions presented in
order to learn the proper preventions and actions for a more informative AIDS aware community
17.
c) Theory of reasoned action – (TRA) was proposed by Ajzen and Fishbein (1975 & 1980). The
components of TRA are three general constructs: behavioral intention (BI), attitude (A), and
subjective norm (SN). TRA suggests that a person's behavioral intention depends on the person's
attitude about the behavior and subjective norms. A person's voluntary behavior is said to be
predicted by his/her attitude toward that behavior and how he/she thinks other people would view
them if they performed the behavior. It is also based on the principle that behavior is defined by
four components: action, objective, context, and time. It is a more comprehensive and complex
theory than the previous ones, since according to it the changing of a risk behavior is the result of
individual and collective action. Action is not the product of particular behaviors between people,
but rather human behavior that depends on the actions of others motivated by objectives and
values, in addition to being determined historically.
The great limitation of this theory is that it supposes that all behaviors and attitudes in the
face of a situation involving risk have intentionality, are rationally assimilated, and are marked by
the values of the group to which the person belongs. A human action does indeed comprise these
components, but the response on the subjective level can be very different and interspersed by
pragmatic actions without the interference of rationally given behaviors.

9
One aspect of this theory should be highlighted, since it allows progress to be made in
the relationship between epidemiology and the socio-cultural dimension in terms of HIV/AIDS
prevention work. As the action is normative, it can be perceived by the individual or group, and
this enables the individual or group to recognize that other people are changing their behavior
and those with whom they interact most closely can provide support with the change. The
normative force of the group acts on people, creating feelings of self-confidence and self-esteem.
The problem resides, fundamentally, in failing to recognize that the normative structures also act
against individuals. This can be seen in the countless situations of violation of the rights of people
living with HIV and AIDS, in the widespread prejudice and in the exclusion of the group when
different opinions and views are raised against such structures.
d) The AIDS Risk Reduction M odel (ARRM ) was introduced in 1990 and provides a framework for
explaining and predicting the behavior change efforts of individuals specifically in relationship to
the sexual transmission of HIV/ AIDS. A three-stage model, the ARRM incorporates several
variables from other behavior change theories, including the Health Belief M odel, "efficacy"
theory, emotional influences, and interpersonal processes. The stages, as well as the
hypothesized factors that influence the successful completion of each stage (please see attached
diagram), are as follows (Catania, Kegeles and Coates, 1990):
Stage 1: Recognition and labeling of one's behavior as high risk
Stage 2: M aking a commitment to reduce high-risk sexual contacts
and to increase low-risk activities
Stage 3: Taking action. This stage is broken down into three phases: 1) information seeking; 2)
obtaining remedies; 3) enacting solutions. Depending on the individual, phases may occur
concurrently or phases may be skipped.
A general limitation of the ARRM model as with others is its focus on the individual. For
instance, many women feel at risk for HIV, not due to their own behavior but because of the
behaviors of their sexual partners and report it as an issue outside of their control (M cGrath et al.,
1993). Thus, when applying behavioral models there is need to take into greater consideration
the social-cultural issues that influence or limit an individual's behavior choices and ability to take
action.
The models we have presented are some of the models in practice for those working with
STD/HIV/AIDS prevention. These are theories used to seek responses in the practical field and to
guide different strategies in order to move towards safer sexual practices among the most
affected populations. Some of the early strategies adopted were: peer education approach,
10
communication campaigns capacity building and training of outreach workers to operate in
specific social networks (CSW and M SM ), training of community health workers, etc.
Nevertheless, there is lack of studies that truly evaluate the impact of these strategies and
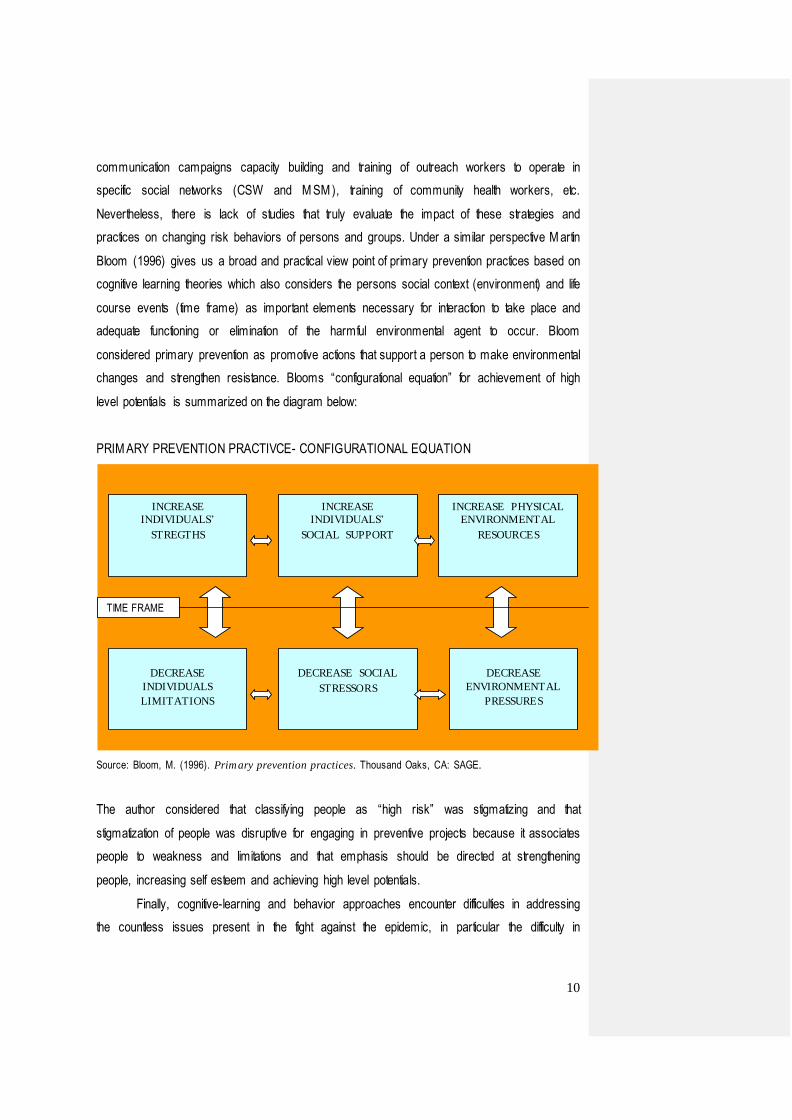
practices on changing risk behaviors of persons and groups. Under a similar perspective M artin
Bloom (1996) gives us a broad and practical view point of primary prevention practices based on
cognitive learning theories which also considers the persons social context (environment) and life
course events (time frame) as important elements necessary for interaction to take place and
adequate functioning or elimination of the harmful environmental agent to occur. Bloom
considered primary prevention as promotive actions that support a person to make environmental
changes and strengthen resistance. Blooms “configurational equation” for achievement of high
level potentials is summarized on the diagram below:
PRIM ARY PREVENTION PRACTIVCE- CONFIGURATIONAL EQUATION
Source: Bloom, M. (1996). Primary prevention practices. Thousand Oaks, CA: SAGE.
The author considered that classifying people as “high risk” was stigmatizing and that
stigmatization of people was disruptive for engaging in preventive projects because it associates
people to weakness and limitations and that emphasis should be directed at strengthening
people, increasing self esteem and achieving high level potentials.
Finally, cognitive-learning and behavior approaches encounter difficulties in addressing
the countless issues present in the fight against the epidemic, in particular the difficulty in
INCREASE
INDIVIDUALS’
STREGTHS
INCREASE
INDIVIDUALS’
SOCIAL SUPPORT
INCREASE PHYSICAL
ENVIRONMENTAL
RESOURCES
DECREASE
INDIVIDUALS
LIMITATIONS
DECREASE SOCIAL
STRESSORS
DECREASE
ENVIRONMENTAL
PRESSURES
TIME FRAME
11
applying such approaches towards reducing or eliminating stigma against people living with HIV,
partly because these strategies are based on individual responsibility, and partly because they
infer that people make enlightened decisions on risk exposure contexts, but fail to take into
consideration the structural determinants related to such situations.
Despite the many criticisms of behaviorist approaches, it is important to recognize their
crucial importance in the response to the emerging epidemic at the time, in particular with regard
to the adoption of safer sex practices by small groups and homogenous and well-established
social networks especially in developed countries. Similarly, peer education models, widely used
in HIV/AIDS prevention projects with drug users, sex workers, men who have sex with men and
youth still use elements of cognitive–learning and behavior change theories to affirm that some
people can serve as behavior models and effectively motivate others to change.
2.2 Health Education
Along with the behavior change theories and the concept of individual risk as presented
above, information and communication emerged as the major pillar of prevention during the first
decade of the epidemic. As a result, a new vision of the role of health education began to be built,
whereby providing information about HIV and its transmission routes was considered to be
sufficient for people to start protecting themselves. To give an example, in the book AIDS in the
World (M ann et. al., 1992) the authors argue in favor of a three-pronged approach to prevention
comprised of: a) information (as synonymous with education); b) health and social services, and
c) the social support environment; considered to be the globally accepted elements essential for
systematizing an effective HIV/AIDS prevention program.
During the 1990s prevention approaches gradually incorporated more complex behavior
change psychodynamics, in an attempt to offer multidimensional alternatives in support of
changes for risk behaviors. In recent decades, HIV/AIDS education, in the same way as sex
education and sexuality, has been concentrated on promoting knowledge, attitudes and safe
behaviors through targeted information campaigns and mass campaigns, and also through the
so-called IEC intervention projects (information, education and communication). Adults and young
people were “taught” the “facts” by experts about “how AIDS is or is not caught”. Or even, at best,
how to use condoms correctly in order to prevent the sexual transmission of HIV, with the belief
that people would then adopt safer behaviors as a result of the knowledge gained.

12
In a second phase, health education strategies began to offer the opportunity for young
people to reflect on the attitudes they could have, or that people around them could have – i.e.
attitudes in relation to certain sexual practices and attitudes of discrimination and prejudice with
regard to condom use and HIV positive people. In addition, at a given time, in the mid to late
1990s, new “participative” AIDS prevention methodologies were introduced, through “safe sex”
workshops with an emphasis on the development of activities capable of facilitating the
acquirement of skills – the so-called “life skills” (terminology used by UNICEF and UNESCO)18,
relating to the ability to take decisions and the capacity of sexual “communication” and
“negotiation” with partners.
However, what was most frequently seen in the use of workshops and group
methodologies with adolescents and young adults, both within schools and community
environments was the emphasis on the individual in isolation, the one who needs to be “taught”,
who needs to learn “correct attitudes”, and who needs to become “capable”. M ost of the time
expected to become capable of saying no, capable of ignoring their feelings, and ignoring their
identity and their citizenship. Rarely is concern shown with factors of affection and emotion, with
what people feel about the issues relating to their life situation, within the context of their own
social networks, their personal needs, their desires and fantasies, and what they know and do.
It is important that we recognize the limitations of logic and rational approaches in relation
to understanding people’s sex lives. Rarely are the types of action that lead to sex better
understood in terms of negotiation and structured, open, public communication, as in the
methodologies used in widespread prevention programs in the late 1980s and 1990s, of the “Just
say no” type widely applied to young people (UNAIDS, 1997). Rarely do any of us consider the
advantages and disadvantages of having sex in the manner suggested by reasoned decision -
making models and behavior change related to risk reduction. As Peter Aggleton (2003)
emphasized in a conference on “Education for Prevention” in Brazil in 2003, “how many of us
considered all the advantages and disadvantages before or during the last time we had sex?
Although actions can be reconstructed in this way, after the event, at the exact time they occur
they are responses to opportunity and chance”.
In the same way, the power of transgression – or the excitement of doing something
different, forbidden, taking a chance and following a wild or romantic impulse – is generally
underestimated. Although these issues have been discussed in the case of the apparent
abandonment of condom use by male homosexuals, namely, the phenomenon of barebacking19,
the matter has received relatively little attention. Transgression is rarely considered in safe sex

13
education in general and, principally with regard to heterosexual sex or when educating on drug
use.
On the other hand, if we look back at the progress made with HIV and AIDS prevention
we can see that the later introduced concept of vulnerability was essential for the presentation of
new forms of prevention work, enabling the understanding of the socio-cultural conditions and
factors that interfere with the adoption of certain practices, even when the initial approaches were
focused on individual behaviors. The incorporation of the concept of vulnerability has enabled us
to consider that people’s exposure to illness may result from a set of aspects and factors, some of
which are individual, but most of which are collective, structural, socio-cultural and economic. As
such, the concept of vulnerability has become increasingly accepted in academic and research
circles, as well as by civil society organizations and government bodies responsible for public
policies related to HIV/AIDS prevention and treatment.
2.3 Sexuality and HIV prevention: social and cultural constructions
Over the history of prevention approaches to HIV/AIDS there have been three phases of
theoretical guidance in relation to intervention and research: a) the first phase, in the 1980s,
focused on a more behavioral and individualist perspective where the concept of risk was
essential; b) the second phase, beginning in the early 1990s, when attention became directed
towards socio-cultural and collective determinants of the epidemic and HIV infection, such as
drug use, the number of sex partners, the type of sexual relations and gender and power
relations, having the concept of vulnerability as the explanatory and operational basis for
prevention, but with responses still centered on the individual; c) the third and more contemporary
phase which emphasizes structural factors whereby the perception of vulnerability takes into
consideration factors delineated within the context itself, such as living conditions, violence, level
of education, employment and income, the guarantee of fundamental rights and citizenship – the
experience of marginalization, stigma and discrimination on the grounds of gender, race, age or
sexual orientation and access to diagnosis, treatment and social welfare services. In this case,
the focus is also extended to the complexity of social relations in political, economic, social, and
cultural terms.

14
With the aim of understanding human sexuality and sexual behavior in recent decades,
and of overcoming the challenges posed by the epidemic, several disciplines, such as sociology,
cultural anthropology, social psychology and history, have attempted to question this view and to
focus on the production of knowledge through studies based on the so-called “social and cultural
construction” of sexual behavior. In this sense, attention has been directed towards the
recognition of social, political and cultural forces that shape sexual behavior and sexuality in
different scenarios, as well as towards the complex relationship with the often contradictory
significations associated with the sexual experiences of individuals and their social groups
(Gagnon and Simon, 1973; Weeks, 1981, 1985; Parker, 1991).
The constructivist school combines the individual and the cultural levels, whereby
sexuality is constructed and not biologically defined. This does not mean that biological capacities
are not prerequisites for human sexuality, but rather that recognition is given to the force of social
relations, family and culture on the constitution of sexuality and on the organization of desire and
power. According to Vance, C. (1999), sexual identity is also the fruit of the processes of
socialization of individuals in interactions with others, but can also create its own identities and
communities. The author argues that the great achievement of social constructivism was to
provoke the questioning of ideological and pre-established assumptions about sexuality,
particularly those naturalized by essentialism, seeking to explore meanings and analyze
socialization processes. The constructivist theories on sexuality enable the distinction between
sexual acts, identities and communities, as well as the investigation of the complex and variable
ways in which these categories relate with each other.
In the 1990s, with the expansion of the field of studies on the social and cultural
construction of sexuality, HIV/AIDS research also began to place greater emphasis on examining
the social and cultural dimensions of sexuality, drug use and their relationship to the epidemic.
Reflection thus began on the importance not only of obtaining data on the frequency of a given
behavior but also of considering socio-economic contextual factors relating to behavior, so that
the subjective and inter-subjective significations associated with behavior could generate
knowledge of greater relevance for prevention (Simon and Gagnon, 1999).
The concept of social networks thus emerges as another important concept for dealing with
fundamental aspects relating to sexual health promotion and to safer sex in particular. The reality
of social networks is seen as being greater than any sex actor, individual or peers and, therefore,
the references of our sexuality can come from different sources and in different ways, ranging
from social institutions to close relatives and friends. These references can influence our sexual

15
behavior when we are alone with our partner, and can also influence our choice of partner. It is
considered that the social structure also influences the way in which partnerships are organized
in our society, and that the individual investment by the partners can influence the opportunities of
having or changing partners. For example, in a study on condom use in Thailand, Thai men
reported that what was seen as a behavioral norm among their colleagues exerted greater
influence over their own behavior (VanLandingham, Suprasert, Grandjean and Sittitrai, 1995).
Undoubtedly, progress has been made beyond the restricted and purely biological view of the
construction of sexuality, which, on the other hand, has broadened the view of a single and
epidemiological perspective of HIV transmission, and how to approach the diverse social, cultural
and subjective factors relating to the problem of the epidemic’s proliferation throughout the world.
Part of this progress is the incorporation of the concept of vulnerability in the design of public
policies on HIV/AIDS prevention, based on a review of the idea of individual responsibility. If
individual responsibility were removed from the heart of the question, “responsibility” would be
attributed to other determinants parallel to behavior, such as social and programmatic
vulnerability, in addition to individual vulnerability. The concept of vulnerability has a direct
relationship with the concept of risk and gained ground, above all, among those concerned with
the transmission of diseases through sex and drug use, such as HIV/AIDS, whilst encountering
resonance in other issues such as gender power, age, ethnic groups, and access to prevention
services and commodities.
2.4 Empowerment, Advocacy and Social Mobilization
The strengthening of social movements involved with HIV/AIDS advocacy and prevention,
the gay movement, the women’s rights movement and other social mobilization and citizenship-
based movements have brought with them the notion of empowerment, translated as
strengthening to achieve change in HIV prevention circuits. This concept considers that a change
to a protective or safer behavior is not just the result of “information + will”, but also involves
resources and limitations of a cultural, political, economic, legal and social nature, unequally
distributed between genders, social segments, ethnic and age groups (Gupta, 1996).
A limitation of this approach is directly related to the way it is used. It does not allow the
subjects of its action to truly act in an autonomous manner, because of the limitation imposed by
the socio-cultural contexts of their lives. In other words, if the concept of “empowerment” is used
only as an individual process, this excludes the dimension that a personal relationship and a

16
sexual relationship cannot be simplified as being merely a matter of power. Unprotected sex
happens between at least two people and, therefore, other variables must be taken into
consideration. For example, after taking part in capacity building and empowerment workshops
Latin American women really felt capable of claiming their rights as women, i.e. requiring their
husbands or partners (whom they knew had extramarital sex) to use condoms when having sex
with them. Consequently, they suffered verbal and physical aggression from their respective
partners when they asked them to use condoms. In other words, the men in these relationships
were not taken into consideration, nor were the social networks to which the women belonged20.
Other authors have taken this concept further and have developed approaches that value
the learning process so that raising the social and cultural awareness of the subjects and
promoting citizenship, particularly within the context of poverty, became more important initially
rather than specific knowledge about HIV/AIDS or other health care matters.
Nevertheless, the real participation of the community or target population approached is
often limited to the carrying out of activities programmed by professionals experienced in
conducting capacity building workshops and group meetings whereby the participation of the
target population goes no further than this. In this case, as no attention is paid to social networks
or the search for responses to overcome structural barriers, the target population remains without
the support necessary to help it take decisions and share concerns. As such, the responsibility for
overcoming conditions of vulnerability to HIV/AIDS such as unequal gender power relations, age
and economic power, and the responsibility for creating prevention and support responses and
alternatives for people living with HIV/AIDS, remains at the level of the individual and not at the
collective level.
Beyond the concept of empowerment is Paulo Freire’s (1968) theory of Participative
Education, also referred to as the participative education model or “collective empowerment”21.
Paulo Freire argues that the lack of power or control in a group or community, in addition to
unfavorable social and economic conditions inherent to the lack of power, are the risk factors that
most influence precarious health conditions (Amaro, 1995). This is also the process by which
socially excluded or marginalized people mobilize themselves to gain control over their health and
lives. The fight by groups against gender and racial oppression, economic exploitation, political
repression or foreign intervention, helps to build the self-confidence needed for their actions.
An empowered or strengthened community uses its resources, the skills of its members
and its organizations to meet community or collective needs. Interventions using empowerment
approaches need to consider concepts regarding practices and beliefs related to interpersonal,
community and organizational changes, whilst also focusing collective capacity building and
17
community mobilization as being crucial for more dynamic and innovative efforts in response to
the structural factors of the epidemic.
The teachings of Freire (1970) related more to the tradition of popular education in Latin
America, the raised awareness of a person or group is the result of the dialogue-based
participation of an individual or community affected by a situation in common in the collective
planning and implementation of a response to that problem or situation. Social change takes
place through collective construction and the perception of the social, cultural, economic and
political strength that structures reality, and acts against the forces perceived to be oppressive.
Under the pedagogical formulations of Paulo Freire (1970), the educational process is
described as libertarian and dialogic. It is a socio-political approach, intended to build a critical
perception of the socio-cultural and political-economic forces that structure reality, motivating and
facilitating action against oppressive forces. This view is in contrast to the model that sees
education as an act of specialists offering information and knowledge to the ignorant, without the
construction of the critical perception of socio-cultural forces or the joint identification of the needs
and vulnerabilities of the community or group, or the participatory planning of possible strategies
and local responses.
The socio-political approach considers individuals as active agents in their communities
and subcultures, capable of reaching an understanding of their symbolic universe through a
process of sensitization and awareness raising, thus being able to modify or recreate it, instead of
passively accepting it. With regard to the socio-political view, Gayle Rubin (1999), when
examining gender and race politics from a social construction point of view, also considers that
when sexuality and sex are understood through social analysis and historical comprehension, a
political and social view of sexuality becomes possible, whereby “sexual policy” is thought of in
terms of population, communities, forms of migration, settlement, conflict, marginalization,
inequality and forms of oppression.
Further developments of Freire’s reflections are presented by Paiva, V. (2000) who opts
for “libertarian education” as a means of encouraging collective organization and believes in the
production of responses by those who are directly affected and living in the context of
vulnerability. She observes that approaches to prevention and the promotion of safer sex, such
as “lectures, leaflets and campaigns do not create “sexual subjects”, nor do they improve
people’s self-esteem so that they decide to avoid risk, and they do not impose safe practices as
priorities put into everyday practice, rather than just the intention to do so ...” (op.cit., p.38).
18
Paiva (2002), emphasizes the need to politicize the psycho-educative spaces and
proposes the notion of “Psychosocial Emancipation” as one of the references for enhancing the
application of the notion of vulnerability. She states that: “in the psycho-educative spaces, the
process has gained from slow learning and from the impact of safer sex workshops on a group or
community or, more recently, the organization of interactive sessions of medication adherence
groups in reference services or non-governmental organizations”. Nevertheless, the author
observes that the sexuality dealt with in such contexts is “everyone’s sexuality”, as if everyone
had the same sexual practices, “without considering their particular aspects in each sexual scene,
in each socio-cultural context”. Furthermore, as a consequence of the simplified view, “the target
population is always considered to be HIV negative and to need to protect itself from potentially
HIV positive people” (Paiva, 2002) 22.
Pedagogical approaches that attempt to encourage the capacity of being critical and
thinking systematically, based on the individual’s own positions in life, tend to be more consistent,
long-lasting and, therefore, more successful. Such approaches generally start from matters of
everyday life and the concerns of groups and people, rather than the concerns of specialists, in
contrast to the pedagogical approach that sees the minds of those who are being educated as
“empty receptacles” waiting to be filled with the good and intelligent ideas of specialists in
intervention and communication.
In summary, the adoption of preventive or protective measures is not restricted to the
individual decision, or to access to correct information about forms of transmission and protection.
The understanding and incorporation of safer sex practices in relation to HIV/AIDS and sexual
health are the result of a dynamic process, built based on social experiences or, using the
terminology of Simon and Gagnon (1973), the result of social and cultural scenarios and
interpersonal scripts or, putting it simpler, the vision of the world by the subjects in question.
Having moved from the concepts of risk and individual responsibility to the concept of
vulnerability and, therefore, to the conceptualization of the social dimensions and dynamics of
HIV infection, we can see that there has been a fundamental transformation, over the course of
time, of the paradigms that have formed and guided the responses to the epidemic in the last
decades. A transformation in relation to the notions of education about AIDS, moving from
individualist information driven models, to more multidimensional models of collective awareness
raising and community mobilization, as potentially more effective strategies, which aims to
produce more resistant and long-lasting responses.
Further developments of this reflection includes Paulo Freire’s notion of awareness
raising as a constructive social process based on dialogue, that enables one to act with others to

19
correct social injustices and inequalities as the essence of community “qualification” and
mobilization as a strategy for fighting AIDS. The participatory working methodology, which sees a
person as the “subject and protagonist” of their responses and which promotes the commitment
of local networks, is capable of generating a sense of solidarity and fighting for a common
objective and for citizenship.
We therefore reach the conclusion that, in order for us to advance and be more effective
with prevention work, prevention models need to be built by integrating various levels of
theoretical frameworks and concepts. It needs to work on the diverse dimensions of vulnerability
(individual, social and programmatic), through proposals for structural and cultural interventions
that take into consideration the subject and their peers in their social and collective environment,
but which also consider the subject on the individual level, with feelings and subjectivities, as the
owner of their own personal history, and with their own interpersonal and sexual scripts and
scenarios.
2.5 Community Participation and Solidarity
The discussion on how to reduce social exclusion and social inequalities as factors of
vulnerability to HIV is present in current national and international debates in various areas, such
as the academic world, civil society, government bodies and international agencies. Building an
AIDS prevention program in low and middle income countries or communities requires
recognition that AIDS is a multi-dimensional social problem and that the approach to effective
program implementation must be based on integrating multi-sector strategies based on a shared
participative vision.
Considering the need to develop new prevention and health promotion strategies,
particularly in the countless disadvantaged social and economic contexts in the majority of
countries or cities with high levels of HIV infection, there is currently growing interest in
strengthening community systems with the aim of developing healthy communities and promoting
environmental and structural change23.
From this perspective, the way in which a society or a community is organized, the extent
to which interaction between community members is encouraged and the degree of association
and trust between individuals are important factors in determining health. A community that can
be described as “facilitating or enabling health” is, therefore, one that structurally encourages
individuals in their efforts to maximize their welfare (Aggleton,2001). Health enabling communities

20
are those that have what is called “social capital”. Social capital refers to the social and
interpersonal ties that promote a person’s growth – complicity, harmony and trust among
members of a society.
Work done using new research methodologies in the social sciences (Putnam, 1996)24
demonstrate the development in several social questions of “intangible” factors as a consequence
of the “atmosphere of trust” that is created between the members of a society which, in turn,
influence directly the degree of associability and the level of “civic consciousness” of its members.
Whereas the concept of “civic consciousness” is understood to refer to basic attitudes of the
members of a society in relation to that society as a whole (e.g. correctly fulfilling their personal
and social obligations), the degree of associability according to Bernardo Kliksber (2000), refers
to: “the extent to which the members of a society form all kinds of associations, take an active
part in them, have the abili ty to make associative efforts of all kinds and to develop synergies”. In
this way, these ties create certain conditions that enable a degree of community sustainability
from several political and social perspectives25. As such, in relation to the community of HIV/AIDS
prevention work, particularly among resource limited populations, social capital is the social or
community cohesion that results from:
- Local horizontal community networks in voluntary, state and personal spheres.
- High levels of civic engagement and participation in these local networks.
- A positive local identity and a sense of solidarity, commitment and equality in relation
to other community members.
- Standards of mutual trust and help, support and cooperation.
Some authors argue that these are the principal characteristics that prevailed in some of
the first and most successful prevention and care efforts for people living with HIV.
Kerrigan, D. and colleagues (2006), assessed the effectiveness of 2 environmental–
structural interventions in reducing risks of HIV and sexually transmitted infections (STIs) among
female sex workers in the Dominican Republic. Significant increases in condom use with new
clients; significant increases in condom use with regular partners; and reductions in STI
prevalence were documented, as were significant increases in sex workers’ verbal rejections of
unsafe sex. Authors concluded that Interventions that combine community solidarity and public
(government) policy show positive effects on HIV and STI risk reduction among sex workers.26
Implications for programming emphasize that the importance of strengthening the so-
called community systems or, in other words, community support, networks and groups lies
above all in the fact that the ability of community leadership to act is the principal strength of the
social action undertaken.

21
The strengthening of community systems and the community participation approach is
based on the principal of effective integration and participation of community members’ rights
from the beginning. Community leaders, community educators, health workers, youth, women,
and men are encouraged to form groups to undertake community needs assessment even before
work proposals or projects are planned and, later, to organize activities of health promotion,
protection, education, sports, cultural, and leisure activities.
Organized communities and networking enables the exchange of experiences that
complement the technical knowledge acquired through ad hoc intervention projects, drives the
gaining of new knowledge and favors interinstitutional relations between governmental and non-
governmental sectors, representing progress on the scenario imposed by poverty and economic
exploitation, gender and sexual oppression, racism and ethnic discrimination, or other situations
of structural violence. Such violence can be expressed as domestic violence, sexual violence or
be related to intolerance of sexual diversity against homosexual men and women and
transgender persons, or even resulting from organized crime such as the trafficking of drugs or
people.
Community involvement is of major importance because it enables actions to be
introduced based on local culture and it drives collective commitment. Given that cultural
scenarios influence collectivity or the group, as well as individual behavior, environmental cues
for safer sex practices, for example, can be introduced into various social contexts ranging from
leisure, cultural, and sport activities to neighborhood association meetings. In this way, there are
a larger number of possible social contexts and representations that influence the ways of
achieving the desired sexual behavior – in this case safer sex and condom use, the use of health
services for prenatal care, STIs and HIV/AIDS diagnosis and treatment. Furthermore, the specific
population or community also begins to discuss its needs and alternatives with regard to leisure,
work as well as to organize and articulate compensatory and support programs for more far-
reaching community development.
In summary, community based participatory models are integrated into human
development processes and facilitate interventions that work aspects of structural violence from
alternative life and educational perspectives, cultural, and productive activities. These
approaches propose to influence social norms and social inclusion of the most vulnerable;
combat stigma and discrimination of people living with HIV and AIDS; promote equal gender
power relations; facilitate protection and promotion of fundamental human rights including sexual
rights and respect for sexual diversity; and racial/ethnical equality. Participatory and inclusive
approaches consider vulnerability factors for HIV/AIDS transmission as well as social, economic,
22
and cultural aspects of communities in order to plan for the development of multidisciplinary and
integral interventions.
3. Promising Biomedical Methods of Prevention: Pre and post HIV prophylaxis with ARVs , circumcision and microbicides
The response range of HIV/AIDS prevention does not exclude the clinical or the
epidemiological fields. The synergic relation between prevention, assistance and treatment is
fruitful and necessary. Today there is no question about the combination of biomedical methods,
cognitive-behavioral methods, or even structural interventions as strategic alternatives for the
control of the epidemic (UNAIDS,2005)27 .
In this respect, measures that have shown to be adequate and widely accepted without
many difficulties through-out public health service networks in general has to do with the
expansion of early diagnosis to HIV infection, universal access to treatment with antiretroviral
drugs, and the expansion of promotion and access to condoms (female and male). These
combined measures and approaches constitute a strong reference for the stabilization and
control of the epidemic. These three references have more recently been complemented by other
biomedical measures in many parts of the world of which we can highlight: adult male
circumcision, post-exposure (PEP) and pre-exposure prophylaxis (PreP), and treatment
measures to lower viral loads of patients with HIV and AIDS.
3.1 Treatment with ARV Medication
There are innumerous benefits that ARV treatment brings to AIDS patients and society as
a whole. ARV medications in addition to providing a better quality of life to patients in respect to
their health standard (reduction of opportunistic infections), to their life extension, and the
reduction of stigma and discrimination associated to AIDS, ARV treatment also contributes to the
reduction of HIV transmission.
According to Swiss medical specialists, Pietro Vernazza; Bernard Hirschel; Enos
Bernasconi and M arkus Flepp (Jan. 2008) after a review of the medical literature and extensive
discussion they published in the weekly Bulletin of Swiss Medicine (Bulletin des Médecins
Suisses) on behalf of the Swiss Federal Commission for HIV / AIDS, a statement that states that

23
HIV-positive individuals on effective antiretroviral therapy and without sexually transmitted
infections (STI) are sexually non-infectious. 28 As stated: “An HIV-infected person on antiretroviral
therapy with completely suppressed viraemia (“effective ART”) for a period of six months, with no
other STI is not sexually infectious, i.e. cannot transmit HIV through sexual contact”. This of
course brings new light into the alternatives for prevention of sexual transmission, especially in
the case of stable serodiscordant homosexual couples, or, heterosexual couples who intend to
reproduce. In this case the authors consider issues related to persons who are not into stable
relationships and are not certain of treatment adherence or suppressed viraemic levels of
partners.
This data also adds to the evaluation that treatment with ARVs has contributed to
prevention effectiveness and the relative slow growth or “stabilization” of epidemics in countries
that have implemented early universal access to treatment in both developing (Brazil, Cuba) and
developed countries (Switzerland). According to a WHO Report (2009), by 2008 around 4 million
people in low and middle income countries were receiving antiretroviral therapy. This is
considered a 10-fold increase since 200329. Nevertheless, only 42% of those persons in need of
treatment globally have access. Fifty-eight percent of patients have their needs for treatment
unmet. In order to move towards universal access and cover the remaining 58% there is a need
for drastic measures to be undertaken with respect to price reduction as well as increases in
production. This includes promoting flexibilities regarding patents and intellectual property and
support for generic production of AIDS medications. Guaranteeing price reduction of ARVs is
necessary for sustaining people already on treatment as well as providing universal access to
those in need and for supporting ethical clinical trials without conflict of interests.
3.2 Post - Exposure Prophylaxis (PEP)
Prevention of Vertical Transmission – Mother to Child In 1994, the results of Protocol 076 from Aids Clinical Trial Group (PACTG 076)
demonstrated the reduction in 67.5% of vertical transmissions of HIV from HIV-positive mothers
to their babies with the use of zidovudine (AZT) during pregnancy, at time of labor and by new
born babies fed with infant formulas30. After this protocol several other studies conducted in the
Unites states, Europe, Africa and Asia confirmed the efficacy of AZT in the reduction of vertical
transmission (Dabis F, M sellati P, M eda N. et al 1999); (Dickover RE et al.1996); (Newell M -L,

24
Gray G, Bryson YJ, 1997) even when the intervention with AZT is conducted later in pregnancy or
even just to the newborn baby (31) (32)( 33) and many others followed. Since then millions of
babies and mothers have benefited from the use of prevention of vertical transmission (M CT and
M TCT) with the use of a relative low-cost antiretroviral therapy.
According to the last UNAIDS Report (2009), coverage of prevention of vertical
transmission services has increased from 10% (2004) to 45% (2008) and is considered a
feasible, successful and cost – effective method of HIV transmission control of universal
affordability. The principal barrier in this case is in the organization of primary heath care services
and maternities (lack of availability to offer diagnostic testing during prenatal care and lack of
treatment for positive women), including the fact that many still don’t have medication (AZT) to
offer women at delivery.
Health Care Workplace Exposure and Sexual Exposure PEP
It is important to emphasize that the use of post- exposure prophylaxis with ARV has
proven efficacy in cases of health worker accidents at hospitals, laboratories and clinics34 . Post-
exposure prophylaxis (or PEP) means taking antiretroviral medications (ARVs) as soon as
possible after exposure to HIV, so that the exposure will not result in HIV infection. PEP should
begin as soon as possible after exposure to HIV but certainly within 72 hours. PEP has been
standard procedure since 1996 for healthcare workers exposed to HIV and it has a 79% rate of
efficacy.
The Centers for Disease Control (CDC, 2005) after review of literature on PEP concluded
that it should also be available for use after HIV exposures that are not work-related. Considering
that people can be exposed to HIV during unsafe sexual activity (when a condom breaks during
sex), or if they share needles for injecting drugs, or infants that are breast fed by an infected
woman and in cases of sexual abuse and rape.
PEP is a four-week program involving two or three ARVs, several times a day. The
medications have serious side effects that can make it difficult to finish the program. PEP is not
100% effective, and it can not guarantee that exposure to HIV will not become a case of HIV
infection35.
Benefits of ARV Therapy Improved quality of life for HIV+ persons Integration of primary prevention and treatment
Contributes to lower stigma and discrimination against persons living with HIV and AIDS
[A-ABIdA1] Comentário: OK

25
Positive impact on the control of dissemination of the virus through sexual and vertical transmission
3.3 Pre-exposure prophylaxis - PrEP
ARVs
Pre-exposure prophylaxis (PrEP) is still under study with the use of the antiretroviral
(ARV) Tenofovir and its efficacy has not been proven yet. Concerns are related to collateral
effects not dimensioned and the possibilities for creating therapeutic resistance in the future.
The extension of the pre-exposure prophylaxis is due in most part to the results
obtained in the last decade with HAART therapy in general and prevention of vertical
transmission in particular. In view of the fact that pre-exposure prophylaxis involves some level of
risk, its result may well be limited and thus its application be directed for specific situations, for
example, in contexts of reproductive rights of persons living with HIV and in the case of
serodiscordant couples that don’t use condoms in all sexual relations, or with injected drug
users.
Considering that new approaches to prevention of HIV transmissiona are needed, many
clinical studies are presently being conducted in many regions of the world by many agencies.
The CDC for example is presently sponsoring trials designed to answer safety and efficacy
questions of a tenofovir or tenofovir plus emtricitabine pill taken as a daily oral HIV preventative
among three populations at high risk for infection: heterosexuals in Botswana, injection drug
users in Thailand, and men who have sex with men (M SM ) in the United States. The CDC also
co-manages trial sites in Uganda as part of the University of Washington Partners PrEP Study,
which is examining the safety and efficacy of PrEP among serodiscordant heterosexual couples.
All trials will also assess the effects of taking a daily pill on HIV risk behaviors, adherence to and
acceptability of the regimen, and in cases where participants become HIV-infected, the resistance
characteristics of the acquired virus. This information will be critical to guide future studies and
HIV prevention programs.
Similar PrEP trials are also being conducted by other agencies. In 2006, Family Health
International (FHI), with funding from the Bill and M elinda Gates Foundation, completed a safety
trial of tenofovir for HIV prevention among young women in Ghana, Nigeria, and Cameroon. The
study provided the first data showing PrEP with tenofovir to be both safe and acceptable for use
by HIV-negative individuals. The National Institutes of Health (NIH) is currently evaluating the

26
safety and efficacy of PrEP among M SM in Peru, Ecuador, South Africa, Brazil, Thailand, and the
United States, and additional trials investigating PrEP among women have been launched in
Africa 36.
It is important to call attention to the fact that pre-exposure prophylaxis more than any
other of the previously mentioned prevention strategies has clear ethical, economic and political
implications that go beyond the possible favorable clinical results. Clinical evidence encounters
large barriers if we begin to consider the present deficit to treatment access of persons in need of
ARV globally regardless of the recent advancements obtained with the support of international
financial institutions and cooperation, and the more recent expansion of investments made in the
production of generic drugs with more accessible prices. There is not enough ARV medication
available globally for the implementation of such an approach today which brings us not only to
the economical and political issues related to production capacity, patents and prices involved but
also to ethical dilemmas. For example is it ethical to provide ARVs for PrEP in rich countries and
let people die without treatment in less resourceful ones? Is it ethical not to make an alternative
method of prevention (when proven effective) available to those who can afford it?
Herpes Simplex Virus Type2 (HSV-2) Suppression
HSV-2 suppression is another promising biomedical internvention under study based on
the fact that genital herpes is caused by the sexually transmitted virus herpes simplex virus type
2. There is a possibility that prevention of HSV-2 or suppressive use of antivirals—acyclovir and
valcyclovir—can reduce the recurrence of HSV-2 lesions. This may have the added benefit of
reducing the risk of HSV-2 infected/HIV-uninfected people acquiring HIV, and of HSV-2/HIV
dually-infected people transmitting HIV to their sexual partners. HSV-2 is found in 20 to 30
percent of HIV-uninfected people in industrialized world compared to 40 to 70 percent of HIV-
uninfected people in resource-limited settings. HSV-2 prevalence is highest (>80%) in HIV-
infected people. Therefore, preventing HSV-2 or treating HSV-2 in both HIV negative and positive
people could potentially have an impact on the HIV epidemic.
Nicolas Nagot and colleagues from London School of Hygiene and Tropical M edicine,
investigated whether suppressive treatment for herpes simplex virus (HSV) associated with
genital herpes could have an impact on HIV transmission (Nagot N, et al. 2006)37. The study
found that reduction in HIV-1 RNA genital shedding was significantly greater in the treated group
than in the placebo group. HIV-1 shedding was significantly less persistent in the treated group.

27
HIV-1 plasma viral load was also reduced as was HSV DNA shedding. The proportion of women
shedding HSV at least once was 18.6% in the treated arm and 54.3% in the placebo arm.
On the other hand, the results from the Partners in Prevention trial released in M ay 2009,
conducted at 14 sites in seven African countries, found that on going suppressive valcyclovir
therapy for HSV-2 in HIV-positive people did not reduce their risk of transmitting HIV to their HIV-
negative partners. The study also demonstrated that a modest reduction in plasma HIV level with
valcyclovir suppression did not translate into reduced HIV transmission, but that there was a
reduction in CD4 decline and HIV disease progression.
A recent meta-analysis conducted by Freeman et al. (2006) of studies in this area
concluded that a person with genital herpes has an approximately threefold greater risk of
acquiring HIV infection after sexual exposure.38 Based on study results we may conclude that
suppression of HSV-2 can be an important additional form of reducing HIV transmission.
Circumcision M ale circumcision is probably the biomedical intervention that has been most exposed to
extensive discussions and attracted as much opposition as supporters during the last few years.
The discussion around the role of circumcision has been in play since the beginning of the 1990s
but has more recently become appreciated at scientific conferences especially after the recent
randomized clinical trials conducted in Uganda, Kenya and South Africa in 2007-2008.
M any considerations have been raised around circumcision and the first is that there has
been sufficient evidence to state that male circumcision can be a protecting factor for men in
heterosexual relationships and that in the case of generalized epidemics it can constitute an
additional protecting factor. Nevertheless, barriers to large scale applications exist and also need
to be taken into consideration39. The most important are: a) proper organization of services to
provide safe adult male circumcision procedures with adequate supervision of trained health
professionals; b) reduction of cultural and religious resistances without conflict with traditional
authorities; c) establishment of a sufficient bond to men that will undergo the procedure to ensure
effective adherence and abstinence during initial healing phase; d) strong social communication
to demonstrate that circumcision does not provide 100% protection, and that it should be
associated with other prevention methods such as consistent condom use.
In respect to female protection, male circumcision has shown to be very little effective
and direct benefits to the female population are mostly related to the possibilities of long term
reduction of male HIV incidence. On the other hand, issues related to conditions of vulnerability

28
of women and unequal power relations could produce an opposite effect where men adopt higher
risk practices, such as an increase in number of sexual partners or a refusal to use condoms40.
Nonetheless, male circumcision has been associated with a lower risk for HIV infection in
international observational studies and in 3 randomized controlled clinical trials. Although there
are risks to male circumcision, serious complications are not common. Accordingly, male
circumcision, together with other prevention interventions, could play an important role in HIV
prevention 41 . Robert C. Bailey(2007), from the Public Health School of Univ. of Illinois, Chicago,
stated during the International AIDS Conference (IAS 2007) that 45 research studies, 3 clinical
trials and several biological studies demonstrated sufficient evidence that adult male circumcision
lowers sexual transmission from females to males in approximately 60%. A meta-analysis
conducted on the status of circumcision and the risk of HIV infection among men who have sex
with men (M SM ) showed low effectiveness in lowering HIV transmission42. A study by Templeton,
DJ et al. (2009) showed that overall, circumcision did not significantly reduce the risk of HIV
infection in the M SM cohort. However, it was associated with a significant reduction in HIV
incidence among those participants who reported a preference for the insertive role in anal
intercourse. Thus circumcision may have a role as an HIV prevention intervention with this subset
of homosexual men43.
A possible set-back related to circumcision is the possibility for men to believe they are
free of infection when circumcised and then relax with respect to other proven effective safer sex
methods such as male and female condom use.
Issues on Circumcision – Adult Males
• Randomized clinical studies clearly indicate the benefit for prevention of HIV transmission from female population to circumcised men (51-63% reduction).
• Cultural, religious and social factors need to be taken into consideration.
• Concern of increased female difficulty in negotiating condom use may occur. • WHO and UNAIDS recommend that circumcision be offered to men in countries where
the epidemics are high (>15%) or generalized and with low levels of circumcision.
29
Microbicides - The use of microbicides for HIV prevention is one of the most discussed and anticipated
methods of prevention considering that it can be a “user controlled” method and thus reverse the
underprivileged place women hold in the scene of sexual transmission of HIV prevention in most
countries. The possibility to use microbicides for anal sex is being studied as well. Scientists are
currently testing many substances to see whether they help protect against HIV and/or other
STIs, but no safe and effective microbicide is currently available to the public. However, scientists
are seriously pursuing more than 50 product leads, including about a dozen that have proven
safe and effective in animals and are now being tested in people44.
In summary, the combination of small doses of a variety of ARV medications is promising
and could be effective in situations where there might be sexual exposure to HIV without the use
of condoms. Nevertheless, there is a need to wait for more consistent clinical evaluations of its
effectiveness and possible collateral effects in the near future. In any case, biomedical methods
and interventions should be considered as complementary methods for prevention of sexual
transmission.
Nevertheless, even considering the many possibilities for prevention with the promising
advancements of medical methods and procedures careful thought must be directed at the
present trend towards the “medicalization” of prevention. Concern is expressed when we look at
the global discourses and responses to the AIDS epidemic - the present tendency to see
biomedical interventions as “quick or magic solutions” to HIV/AIDS prevention. Unfortunately, the
most effective antiretroviral therapies we have today are still not a solution to HIV infection nor a
cure for AIDS – millions of people are still dying – and treatment related side effects as well as
health debilitating advents are cumulative and sometimes acute and of extreme concern for those
under treatment. Thus, the promotion of biomedical methods when unaccompanied by culturally
appropriate educational actions and access to proven barrier methods such as condom use, it
interferes with the principles of comprehensive and integral approaches to prevention.
4. Conclusions: Towards universal access in the field of prevention – combined and powerful interventions
In concluding it is important to point out that results obtained in the prevention field are
very promising, however there is a lot of work still to be done. In our viewpoint, one of the most
important questions to be addressed today by prevention program officials in the face of a

30
complex global epidemic is related to what the social and epidemiological determinants of the
epidemic (or epidemics) are, and, their differences and extensions (including populations and
geographical territories) in order to allow for planning and implementation oriented towards each
of their expressions.
To combine means of control based on the opportunities for early diagnosis, condom
use (male and female) and universal access to treatment is in fact possible, and in reach of many
countries. There are innumerous possibilities and alternative actions and approaches that can be
combined which are believed to be more effective than betting on a single or exclusive alternative
in the field of prevention with the potential to reach everyone. Beyond isolated or pilot actions it
is important for prevention agendas to be based on the right to a broad and universal prevention
approach. We need to look for alternatives that focus on the most vulnerable groups with
extension of coverage, improvement of health service delivery systems (prevention and
assistance) making them more receptive and inclusive, and be able to reach the economic and
social basis under which the epidemic reproduces.
In summary, in the third decade of the epidemic, in order for us to advance and truly
scale up effective prevention strategies, we need to propose the construction of a paradigm that
enables prevention frameworks to be integrated on several levels - individual, social and
structural, based on concepts of social construction of sexuality, social influence and collective
empowerment as the key to reduction of vulnerability factors and risk for HIV infection. We must
also promote frameworks and strategies that encourage critical thinking and the use of
participative methodologies and community mobilization so as to develop local and long lasting
responses in the fight against the HIV/AIDS epidemic45. A proposal capable of reducing prejudice
and discrimination, of promoting respect for human rights and gender equality promoting access
to social services and structures and to health protection and care facilities with freedom and
choice, allowing decisions to be taken on the exercise of sexuality and reproduction46.
Another difficult subject area for program officials and normative agencies to respond to,
and, which creates a huge challenge in the field is related to the need to evaluate results and
outcomes of prevention actions and programs and the costs for services offered.
Impact evaluation and cost variations of prevention efforts are difficult to measure due to
a combination of programmatic inputs that usually occur concurrently, and at different levels (local
and national) and at different time lines.
As Robert Greener (2010)47 says, when prevention programs and actions are evaluated it
is difficult to attribute outcomes to specific inputs and to measure changes in outcomes, in view of
the fact that outcomes are not necessarily related to the inputs in a linear way. On the other hand,

31
as the author further states, costs for prevention interventions and services suffer a wide range of
variations throughout countries and regions complicating further the establishment of cost –
effectiveness (CE) ratios for effective prevention interventions given that “they confound many
factors such as epidemiology, population targeted, coverage, unit prices, and technical
efficiency”48. Nevertheless, specialists and financial agencies agree that there is a need to
improve the efficiency and effectiveness of services and interventions, but also to ensure
sustainable financing of programs.
1 PhD in Collective Health, Ex ecutive Director, Brazilian Interdisciplinary AIDS Association(ABIA).
2 Sociologist, Chief of Prevention, Brazilian National AIDS Program, Ministry of Health
3 MD, MPH, UNAIDS Country Coordinator, Brazill.
4 Brennan, R.O. and Durack, D.T., (1981) 'Gay compromise syndrome', the Lancet, 2 1338-1339.
5 Masur H., Michelis M.A., Greene J.B., Onorato I., Stouwe R.A., Holzman R.S., Wormser G., Brettman L., Lange M., Murray H.W. and
Cunnigham-Rundles S. (1981) 'An Outbreak of community acquired Pneumocystis carinii pneumonia: initial manifestation of cellular immune
dysfunction' (1981), The New England Journal Of Medicine, vol 305:1431-1438, December 10, Number 24
6MMWR Weekly (1982) 'Current Trends Update on Acquired Immune Deficiency Syndrome (AIDS) - United States', September 24, 31(37); 507-
508, 513-514.
7 Altman, L.K. (1982) 'New homosex ual disorder worries officials', the New York Times, May 11
8 During the 12th International Scientific Meeting of the International Epidemiology Association (1990) the then director of the World Health
Organization (WHO), Hiroshi Nakajima, commented that: “ We owe the discovery of this disease to epidemiology. AIDS was recognized in 1981,
two years before the human immune deficiency virus was identified” . Epidemiological observation noted the prevalence of a combination of clinical
manifestations and other pathological conditions: asthenia, weight loss, dermatosis, immune system deterioration and Kaposi’s sarcoma, as well
as opportunistic infections such as Pneumocystis carinii pneumonia.
9 Camargo Jr, Kenneth R (1994) The Sciences of AIDS and the AIDS of Sciences: The medical discourse and the construction of A IDS.[ As
Ciências da Aids & A AIDS das Ciências. O discurso médico e a construção da AIDS.] ABIA-IMS-UERJ and Relume Dumará Editora, Rio de
Janeiro.
10 Foucault, Michel (1980) The Microphysics of Power [A Microfísica do Poder]. Editora Graal, RJ.
32
11 In the 1990s studies demonstrated the effectiveness of preventing vertical transmission (from the mother to the baby) through AZT caps ules
for pregnant women and AZT oral solution for babies during the first six weeks of life.
12 Ajzen and Fishbein (1975 & 1980)
13 AIDSCAP (1996) Behavior Change – a summary of four major theories: Health Belief Model; AIDS Risk Reduction Model; Stages of Change
and Theory of Reasoned Action.
14 Catania, J.A., Kegeles, S. M., and Coates T.J. (1990). Towards an understanding of risk behavior: An AIDS risk reduction model (ARRM).
Health Education Quarterly, 17(1), 53-72.
15 Bandura, A. (1989). Human Agency in Social Cognitive Theory. American Psychologist, 44, 1175-1184.
16 Castiel, L.D. (1996) Força e vontade: aspectos teórico-metodológicos do risco em epidemiologia e prevenção do HIV-AIDS. Revista de Saúde
Pública, 30 (1): 91-100.
17 Miller, Katherine (2005). Communication Theories: Perspectives, Processes, and Contex ts (2nd ed.). New York, New York: McGraw -Hill
18 See UNAIDS Report on the Global HIV/AIDS Epidemic. Geneva. Switzerland: UNAIDS, June 2000. www.unaids.org.
19 Barebacking is characterized by sex ual activity involving penetration (usually in group sex ) between homosexuals without cond om use. In this
contex t, seropositivity is valued as a gift or a present. There are various forms of interaction between HIV positive and neg ative men, and
seroconversion is highly valued (cf. Cypriano, 2003 and Gregório, 2003).
20 For further information on empowerment and gender relations, see Paiva, V.1996. Sex ualidades adolescentes: escolaridade, gênero e o
sujeito sex ual, In: Parker, R.; Barbosa, M.R. Sex ualidades Brasileiras.
21 See Parker, 2000. Teorias de intervenção e de prevenção ao HIV/AIDS pp.92-93. The author refers to the works of Paulo Freire and of popular
educators and ex amines HIV/AIDS-related activities based on Social Transformation and Collective Empowerment theories, with the aim of
analysing issues relating to power and oppression. Parker goes beyond these works and refers (op.cit. p.105) to empowerment and community
mobilization as strategic forms of capacity building essential in the fight against AIDS.
22 PAIVA, V. Sem mágicas soluções: A prevenção e o cuidado em HIV/AIDS e o processo de emancipação psicossocial. Interface. Botucatu: v.
6, n. 11, p. 25-38, 2002.
24 See Robert Putnam for further information on the methodology used in the Italian ex perience. Putnam developed a methodology that enabled
him to “ measure” certain social actions that favored the development of industrial northern Italy. Putnam, R.D., Community and democracy: the
ex perience of modern Italy. [Comunidade e Democracia: a ex periência da Itália Moderna.] Rio de Janeiro, Editora Fundação Getú lio Vargas,
1996.
25 See Kliksber, B. América Latina: Uma região de risco – pobreza, desigualdade e institucionalidade social. Brasília: Cadernos UNESCO Brasil,
2000, p.36. See also: Kliksberg, Tomassini and Iglesias (2000) “ capital social y cultura:claves estrategicas para el desarrol lo (Mundo
Contemporaneo) ( Spanish Edition).
26Deanna Kerrigan et al. Environmental–Structural Interventions to Reduce HIV/STI Risk Among Female Sex Workers in the Dominican Republic.
American Journal of Public Health 120-125 .© 2006.
27 See “ Essential Programatic Actions for HIV Prevention” . UNAIDS Prevention Policy Paper “ Intensifying HIV prevention” . ( August 2005).
28 The statement, published in the January 30, 2008 week’s Bulletin of Swiss Medicine (Bulletin des médecins suisses on behalf o f the Swiss
Federal Commission for HIV / AIDS was authored by four of Switzerland’s foremost HIV ex perts: Prof Pietro Vernazza, of the Cantonal Hospital in
St. Gallen, and President of the Swiss Federal Commission for HIV / AIDS; Prof Bernard Hirschel from Geneva University Hospital; Dr Enos
Bernasconi of the Lugano Regional Hospital; and Dr Markus Flepp, president of the Swiss Federal Office of Public Health’s Sub -committee on the
clincal and therapeutic aspects of HIV / AIDS, discusses the implications for doctors; for HIV-positive people; for HIV prevention; and the legal

33
system. http://aidsmap.com/en/news accessed 4-14-2010.
29 Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. Progress report. September 2009. Available at
www.who.int/hiv/pub/2009 progress report/en/.
30 Connor EM et al. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. N Engl J Med,
1994, 331 (18):1173-1180.
31 Dabis F, Msellati P, Meda N. et al. 6-Month efficacy, tolerance, and acceptability of a short regimen of oral zidovudine to reduce vertical
transmission of HIV in breast-fed children in Cote d'Ivoire and Burkina Faso: a double-blind placebo-controlled multicentre trial. Lancet 1999, 353:
786 -792.
32 Dickover RE et al. Identification of levels of maternal HIV-1 RNA associated with risk of perinatal transmission: effect of maternal zidovudine
treatment on viral load. JAMA, 1996, 275:599-605
33 Newell M-L, Gray G, Bryson YJ. Prevention of mother-to-child transmission of HIV-1 transmission. AIDS,1997,11(Suppl A):S165-S172.
34 X De La Tribonniere; M D Dufresneet.al (1998) . Tolerance, compliance and psychological consequences of post-ex posure prophylaxis in
health-care workers . International Journal of STD AIDS 1998;9:591-594 doi:10.© 1998 Royal Society of Medicine Press.
35 For further information CDC PREP Guidelines see: Occupational exposure: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5409a1.htm and
Non-occupational ex posure: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5402a1.htm source: The AIDS Infonet viewed April 20, 2010.
36 A full list of current trials, researchers, and sponsors is available at the PrEP Watch website.
37 (Nagot N, Ouedraogo A, Mayaud P et al. Effect of HSV-2 suppressive therapy on HIV-1 genital shedding and plasma viral load: a proof of
concept randomized double-blind placebo controlled trial (ANRS 1285 Trial). 13th CROI, Denver 2006. Abstract 33LB.)
38 Freeman EE, Weiss HA, Glynn JR et al. Herpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and
meta-analysis of longitudinal studies. AIDS 2006;20:73-83.
39 Gostin, L.O and Hankins, C. A. Male Circumcision as an HIV Prevention Strategy in Sub-Saharan Africa. Sociolegal Barriers. JAMA.
2008;300(21):2539-2541.
40 Auvert B, Taljaard D, Lagarde E, et al. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the
ANRS 1265 trial. PLoS Med. 2005;2(11):e298.
41 World Health Organization and UNAIDS. New data on male circumcision and HIV prevention: policy and programme implications. 2007 Mar.
Accessed Jan 24, 2008.; Williams BG, Lloyd-Smith JO, Gouws E, et al. The potential impact of male circumcision on HIV in sub-Saharan Africa.
PLoS Med. 2006;3(7):e262. Accessed Jan 24, 2008. Source: Divisions of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis,
STD, and TB Prevention.
42 Gregorio A. ,Millett, et al. Circumcision Status and Risk of HIV and Sex ually Transmitted Infections Among Men Who Have Sex With Men: A
Metaanalysis” .JAMA (2008;300[14]:1674-1684).
43 Templeton, D. J; Jin, Fengyi; Mao, Limin; et al..Circumcision and risk of HIV infection in Australian homosex ual men,(2009) @Lippincott
Williams & Wilkins, Inc. viewed march 10, 2010.
http://journals.lww.com/aidsonline/Abstract/2009/11130/Circumcision_and_risk_of_HIV_infection_in.12.aspx
44 For more information on microbicides see http://www.global-campaign.org/more_microbicides.htm.
45 Pimenta, M.C. ‘HIV/AIDS Prevention Paradigms’. Conference paper presented at the XVI International AIDS Conference.Toronto, 2006.
34
46 For references on current guidelines for comprehensive national strategies based on global efforts see: a) UNESCO, 2010. ‘International
Guidelines on Sex uality Education: an evidence informed approach to effective sex , relationships and HIV/STI education’. Viewed April 15, 2010.
http://unesdoc.unesco.org/images/0018/001832/183281e.pdf and,
b) UNAIDS,2009. ‘Joint action for results: UNAIDS outcome framework, 2009–2011’. Viewed April 15,2010.
http://data.unaids.org/Publications/Fact- Sheets02/jc1713_joint_action_from20printer_en.pdf
47 Dr. Robert Greener is senior economics advisor to UNAIDS.
48 Greener, R. 2010. ‘Economics and HIV’. Proceedings from UNAIDS HIV Prevention Seminar Series. Geneva April 12, 2010.







