ffr vs. angiography for multivessel evaluation fame 2 year follow-up william f. fearon, pim a.l....
TRANSCRIPT

FFR vs. Angiography for Multivessel Evaluation
FAME2 Year Follow-Up
William F. Fearon, Pim A.L. Tonino, Bernard De Bruyne,
Uwe Siebert and Nico H.J. Pijls,
on behalf of the FAME Study Investigators

Disclosure Statement of Financial Interest
I, William Fearon, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation.

Background
• Ischemia-producing coronary lesions cause symptoms and cardiac events.
• Coronary stenoses not responsible for ischemia can be safely treated medically.
• A primary goal of PCI is to relieve myocardial ischemia, resulting in fewer symptoms and cardiac events.

Background
• The angiographic severity of a coronary stenosis correlates poorly with its ischemic potential.
• The current strategy of performing PCI based on the angiographic appearance of a lesion may not be the most effective or efficient technique.
• Measuring fractional flow reserve (FFR) to help identify which lesions warrant PCI may be a superior method for achieving a “functionally” complete revascularization.

Background
• The FAME study is a multicenter, international, randomized trial comparing an FFR-guided approach to PCI in patients with multivessel CAD to an angiography-guided strategy.
• At TCT 2008, we presented the 1 year results from FAME demonstrating a significant decrease in MACE in the patients randomized to FFR guidance.
• The durability of this benefit is the subject of this two-year follow-up of the FAME study.

Methods
• Inclusion Criteria: Patients with lesions in 2 or all 3 major
epicardial vessels, which were ≥50% narrowed and which the operator deemed warranted PCI based on the angiographic appearance and the clinical data available.1,2
1. Fearon, et al. Am Heart J 2007;154:632-6.2. Tonino, et al. New Engl J Med 2009;360:213-24.

Methods
• Exclusion Criteria: Angiographically significant left main
disease Previous CABG Recent ST elevation MI (<5 days) Cardiogenic shock Extremely tortuous or calcified vessels
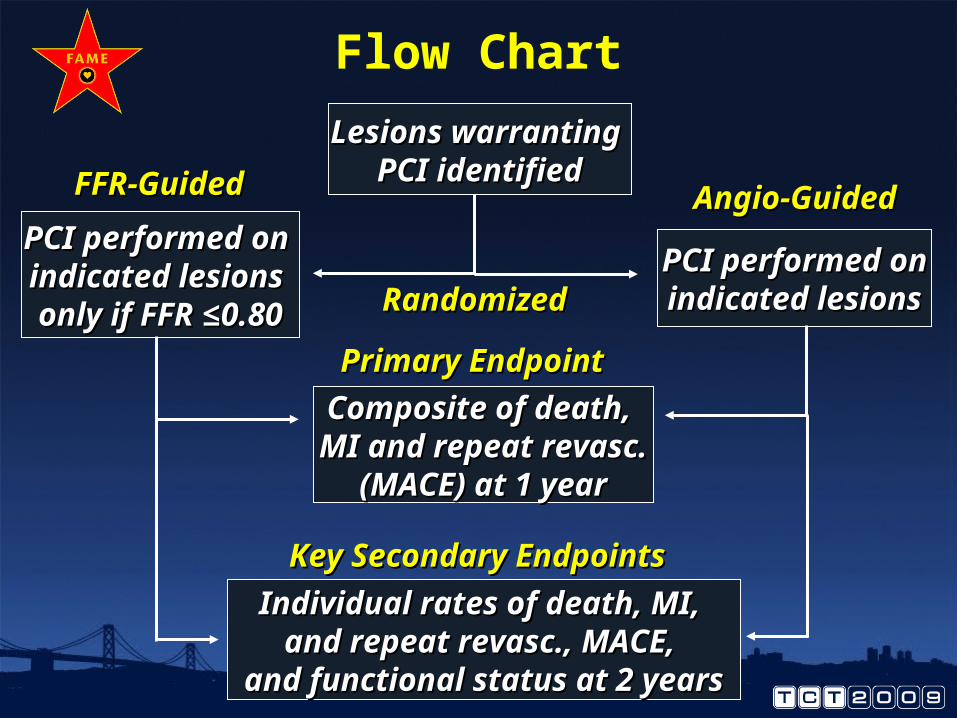
Lesions warranting Lesions warranting PCI identifiedPCI identified
PCI performed onPCI performed onindicated lesionsindicated lesionsRandomizedRandomized
PCI performed on PCI performed on indicated lesions indicated lesions only if FFR only if FFR ≤≤0.800.80
FFR-GuidedFFR-Guided Angio-GuidedAngio-Guided
Composite of death, Composite of death, MI and repeat revasc.MI and repeat revasc.
(MACE) at 1 year (MACE) at 1 year
Primary EndpointPrimary Endpoint
Individual rates of death, MI, Individual rates of death, MI, and repeat revasc., MACE, and repeat revasc., MACE,
and functional status at 2 yearsand functional status at 2 years
Key Secondary EndpointsKey Secondary Endpoints
Flow Chart

Participating CentersParticipating Centers
USA (6)USA (6)Stanford University Stanford University (W. Fearon)Northeast Cardiology, Bangor, Northeast Cardiology, Bangor, MEME(P. Verlee)St Louis UniversitySt Louis University(M. Lim)University of LouisvilleUniversity of Louisville(M. Leesar)University of South CarolinaUniversity of South Carolina(E. Powers)University of VirginiaUniversity of Virginia(M. Ragosta)
EUROPE (14)EUROPE (14)
Cardiovascular Center, Aalst (B. de Bruyne)
Catharina Hospital, Eindhoven Catharina Hospital, Eindhoven (N. Pijls)
Rigshospitalet, Copenhagen Rigshospitalet, Copenhagen (T. Engstrom)
Klinikum der Universitat Munchen Klinikum der Universitat Munchen (V. Klauss)
Aarhus University Hospital Aarhus University Hospital (O. Frobert)
University Hosp Bergmannsheil University Hosp Bergmannsheil (W. Bojara)
Sodersjukhhuset, Stockholm Sodersjukhhuset, Stockholm (I. Herzfeld)
Helsingborgs Lasarett Helsingborgs Lasarett (F. Schersten)
Klinikum Darmstadt Klinikum Darmstadt (G. Werner)
Bristol Royal Infirmary Bristol Royal Infirmary (A. Baumbach)
Staedt. Krankenhaus, Bogenhausen Staedt. Krankenhaus, Bogenhausen (G. Riess)
Glasgow Western Infirmary Glasgow Western Infirmary (K. Oldroyd)
Royal Victoria Hosp, Belfast Royal Victoria Hosp, Belfast ((G. Manoharan)
King´s College Hosp, London King´s College Hosp, London (P. MacCarthy)

Organization
Major Sponsor:Major Sponsor:Radi Medical System / St. Jude MedicalRadi Medical System / St. Jude Medical
Steering Committee:Steering Committee:Nico H.J. Pijls, Eindhoven, Netherlands (PI)Nico H.J. Pijls, Eindhoven, Netherlands (PI)William F. Fearon, Stanford, CA, USA (PI)William F. Fearon, Stanford, CA, USA (PI)Bernard De Bruyne, Aalst, BelgiumBernard De Bruyne, Aalst, BelgiumPim A.L. Tonino, Eindhoven, NetherlandsPim A.L. Tonino, Eindhoven, Netherlands
Data analysis:Data analysis:Uwe Siebert, Boston, MA, USA and Hall, AUwe Siebert, Boston, MA, USA and Hall, A
Clinical Events Committee:Clinical Events Committee:Emanuele Barbato, Naples, ItalyEmanuele Barbato, Naples, ItalyEric Eeckhout, Lausanne, SwitzerlandEric Eeckhout, Lausanne, SwitzerlandMamdouh El Gamal, Eindhoven, NLMamdouh El Gamal, Eindhoven, NLMorton Kern, Irvine, CA, USAMorton Kern, Irvine, CA, USAJohn Hodgson, Wilkes Barre, PA, USAJohn Hodgson, Wilkes Barre, PA, USA

Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Age, mean Age, mean ±SD±SD 64±10 65±10 0.470.47
Male, %Male, % 73 75 0.300.30
Diabetes, %Diabetes, % 25 24 0.650.65
Hypertension, %Hypertension, % 66 61 0.100.10
Current smoker, %Current smoker, % 32 27 0.120.12
Hyperlipidemia, %Hyperlipidemia, % 73 72 0.620.62
Previous MI, %Previous MI, % 36 37 0.840.84
NSTE ACS, %NSTE ACS, % 36 29 0.110.11
Previous PCI , %Previous PCI , % 26 29 0.340.34
LVEF, mean LVEF, mean ±SD±SD 57±12 57±11 0.920.92
LVEF < 50% , %LVEF < 50% , % 27 29 0.470.47
Baseline Characteristics

Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Indicated lesions / patientIndicated lesions / patient 2.7±0.9 2.8±1.0 0.340.34
Stents / patientStents / patient 2.7 ± 1.2 1.9 ± 1.3 <0.001<0.001
Procedural Characteristics
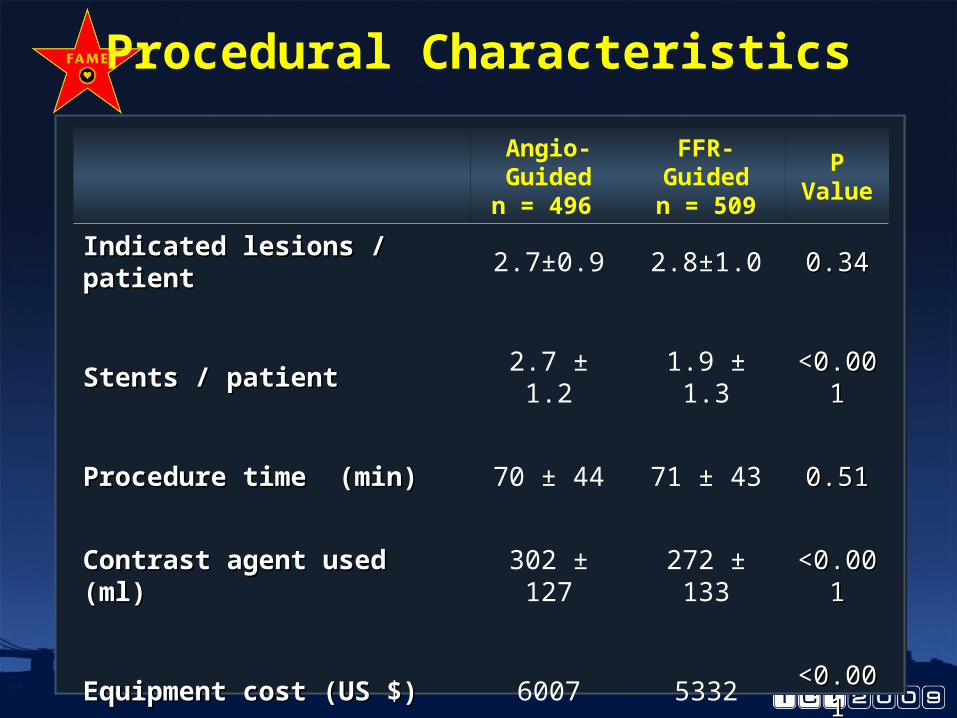
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Indicated lesions / patientIndicated lesions / patient 2.7±0.9 2.8±1.0 0.340.34
Stents / patientStents / patient 2.7 ± 1.2 1.9 ± 1.3 <0.001<0.001
Procedure time (min)Procedure time (min) 70 ± 44 71 ± 43 0.510.51
Contrast agent used (ml)Contrast agent used (ml) 302 ± 127 272 ± 133 <0.001<0.001
Equipment cost (US $)Equipment cost (US $) 6007 5332 <0.001<0.001
Length of hospital stay (days)Length of hospital stay (days) 3.7 ± 3.5 3.4 ± 3.3 0.050.05
Procedural Characteristics

Adverse Events at 1 Year
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 113 76
DeathDeath 15 (3.0) 9 (1.8) 0.190.19
Myocardial InfarctionMyocardial Infarction 43 (8.7) 29 (5.7) 0.070.07
Small / peri-PCI (CK-MB 3-5xNl)Small / peri-PCI (CK-MB 3-5xNl) 16 12
Other infarctions (“late or large”)Other infarctions (“late or large”) 27 17
CABG or repeat PCICABG or repeat PCI 47 (9.5) 33 (6.5) 0.080.08
Death or Myocardial InfarctionDeath or Myocardial Infarction 55 (11.1) 37 (7.3) 0.040.04
Death, MI, CABG, or re-PCIDeath, MI, CABG, or re-PCI 91 (18.3) 67 (13.2) 0.020.02

1 Year Event-Free Survival
FFR-guided
30 days2.9% 90 days
3.8% 180 days4.9% 360 days
5.1%
Angio-guided
Absolute Difference in MACE-Free Survival
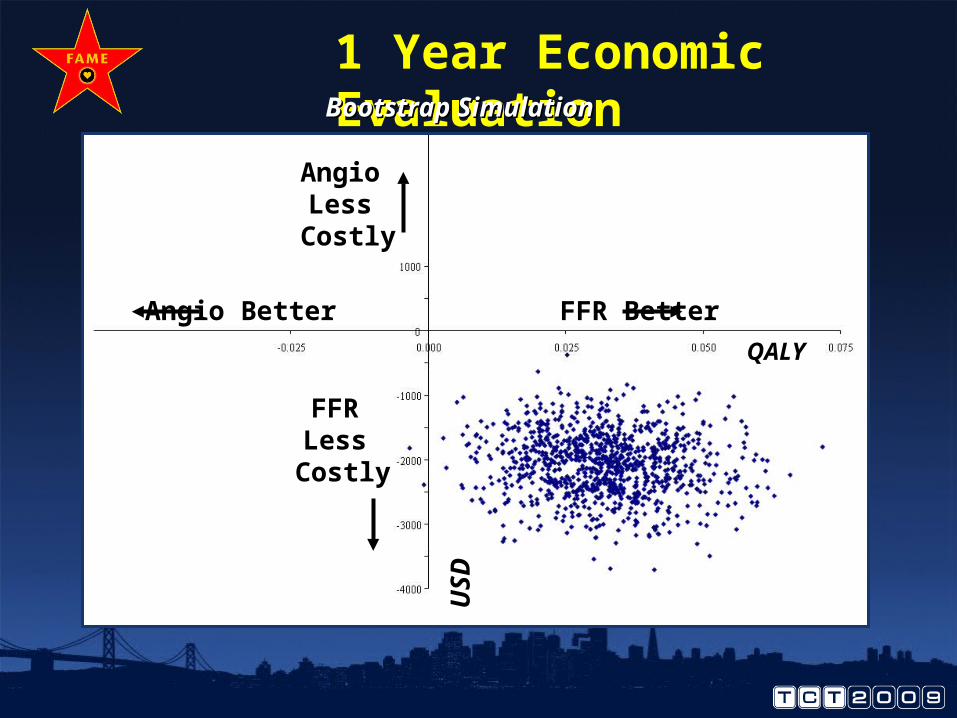
1 Year Economic Evaluation
Angio Better FFR Better
FFR Less Costly
Angio Less Costly
QALY
US
D
Bootstrap SimulationBootstrap Simulation

Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value

Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105

Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105
Individual EndpointsIndividual Endpoints

Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105
Individual EndpointsIndividual Endpoints
DeathDeath 19 (3.8) 13 (2.6) 0.250.25

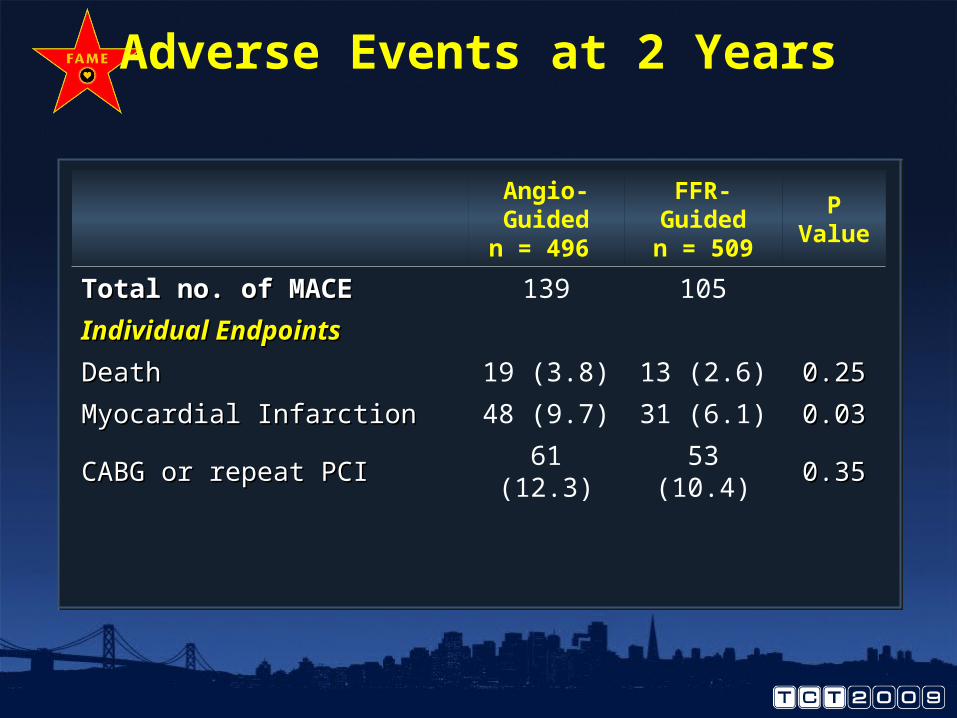
Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105
Individual EndpointsIndividual Endpoints
DeathDeath 19 (3.8) 13 (2.6) 0.250.25
Myocardial InfarctionMyocardial Infarction 48 (9.7) 31 (6.1) 0.030.03
Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105
Individual EndpointsIndividual Endpoints
DeathDeath 19 (3.8) 13 (2.6) 0.250.25
Myocardial InfarctionMyocardial Infarction 48 (9.7) 31 (6.1) 0.030.03
CABG or repeat PCICABG or repeat PCI 61 (12.3) 53 (10.4) 0.350.35

Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105
Individual EndpointsIndividual Endpoints
DeathDeath 19 (3.8) 13 (2.6) 0.250.25
Myocardial InfarctionMyocardial Infarction 48 (9.7) 31 (6.1) 0.030.03
CABG or repeat PCICABG or repeat PCI 61 (12.3) 53 (10.4) 0.350.35
Composite EndpointsComposite Endpoints

Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105
Individual EndpointsIndividual Endpoints
DeathDeath 19 (3.8) 13 (2.6) 0.250.25
Myocardial InfarctionMyocardial Infarction 48 (9.7) 31 (6.1) 0.030.03
CABG or repeat PCICABG or repeat PCI 61 (12.3) 53 (10.4) 0.350.35
Composite EndpointsComposite Endpoints
Death or Myocardial InfarctionDeath or Myocardial Infarction 63 (12.7) 43 (8.4) 0.030.03

Adverse Events at 2 Years
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Total no. of MACETotal no. of MACE 139 105
Individual EndpointsIndividual Endpoints
DeathDeath 19 (3.8) 13 (2.6) 0.250.25
Myocardial InfarctionMyocardial Infarction 48 (9.7) 31 (6.1) 0.030.03
CABG or repeat PCICABG or repeat PCI 61 (12.3) 53 (10.4) 0.350.35
Composite EndpointsComposite Endpoints
Death or Myocardial InfarctionDeath or Myocardial Infarction 63 (12.7) 43 (8.4) 0.030.03
Death, MI, CABG, or re-PCIDeath, MI, CABG, or re-PCI 110 (22.2) 90 (17.7) 0.070.07

2 Year Survival Free of MACE
FFR-GuidedFFR-Guided
Angio-GuidedAngio-Guided
730 days730 days4.5%4.5%

2 Year Survival Free of Repeat Revascularization
FFR-GuidedFFR-Guided
Angio-GuidedAngio-Guided
730 days730 days1.9%1.9%

2 Year Survival Free of MI
FFR-GuidedFFR-Guided
Angio-GuidedAngio-Guided 730 days730 days3.6%3.6%
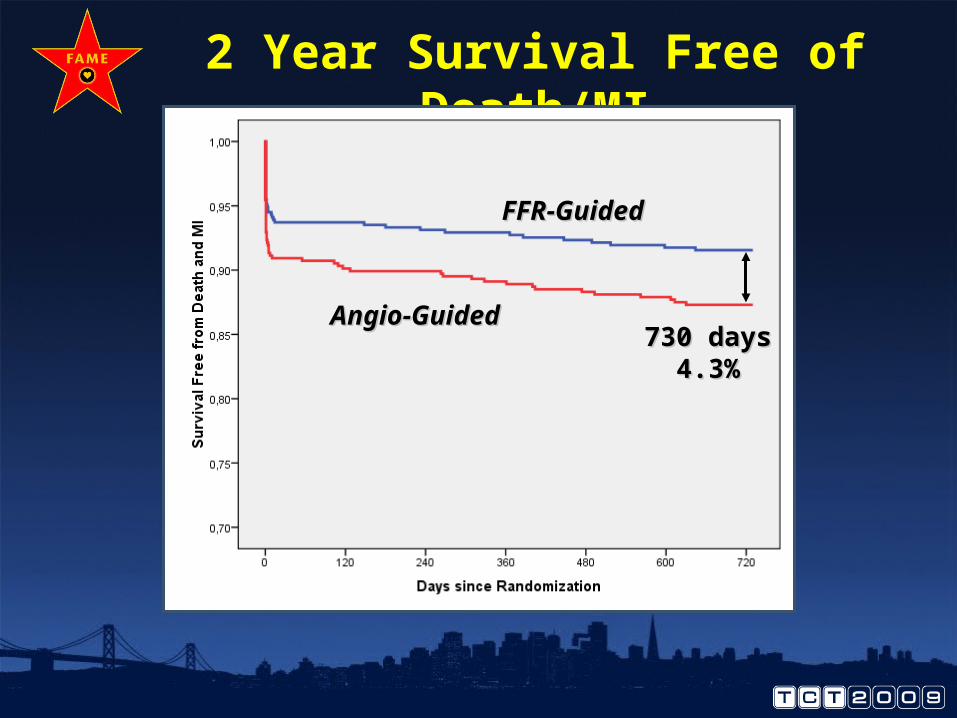
2 Year Survival Free of Death/MI
FFR-GuidedFFR-Guided
Angio-GuidedAngio-Guided730 days730 days
4.3%4.3%

Other 2 Year Outcomes
Angio-Guidedn = 496
FFR- Guidedn = 509
P Value
Follow-up (%)Follow-up (%) 92.7 94.5 0.310.31
Anti-anginal Medications, No.Anti-anginal Medications, No. 1.2 ±0.8 1.2 ±0.7 0.660.66
Dual Antiplatelet Therapy (%)Dual Antiplatelet Therapy (%) 33.6 31.4 0.490.49
Freedom from Angina, (%)Freedom from Angina, (%) 75.8 79.9 0.140.14

Outcome of Deferred Lesions
513 Deferred Lesions in513 Deferred Lesions in509 FFR-Guided Patients509 FFR-Guided Patients
2 Years2 Years
31 31 Myocardial InfarctionsMyocardial Infarctions2222
Peri-proceduralPeri-procedural
99Late Myocardial InfarctionsLate Myocardial Infarctions
88Due to a New Lesion Due to a New Lesion
or Stent-Relatedor Stent-Related
11Myocardial Infarction due toMyocardial Infarction due to
an Originally Deferred Lesionan Originally Deferred Lesion
Only 1/513 or 0.2% of deferred Only 1/513 or 0.2% of deferred lesions resulted in a late lesions resulted in a late
myocardial infarctionmyocardial infarction

Outcome of Deferred Lesions
513 Deferred Lesions in513 Deferred Lesions in509 FFR-Guided Patients509 FFR-Guided Patients
2 Years2 Years
5353 Repeat Revascularizations Repeat Revascularizations3737
in a New Lesion orin a New Lesion orin a Restenotic Onein a Restenotic One
1616Originally Deferred LesionsOriginally Deferred Lesions
66Without FFR or Without FFR or
Despite an FFR > 0.80Despite an FFR > 0.80
1010Originally Deferred LesionsOriginally Deferred Lesions
with Clear Progressionwith Clear Progression
Only 10/513 or 1.9% of deferred Only 10/513 or 1.9% of deferred lesions clearly progressed lesions clearly progressed
requiring repeat revascularizationrequiring repeat revascularization

Conclusions
• At 2 years, there is now a significant decrease in the rate of MI in the FFR-guided arm. There continues to be a significant decrease in death and MI favoring the FFR-guided approach. Lastly, there is a strong trend towards a lower rate of death, MI or the need for repeat revascularization in the FFR-guided arm.
• There is no signal to suggest that deferred lesions are likely to be responsible for late myocardial infarctions or to progress and require repeat revascularizations.
Conclusions
• The 2 year follow-up of the FAME study demonstrates durability of the improved outcomes noted at 1 year with an FFR-guided approach to PCI in patients with multivessel CAD
• These results continue to support the evolving paradigm of:
““Functionally Complete Revascularization”Functionally Complete Revascularization”
i.e. stenting of ischemic lesions and i.e. stenting of ischemic lesions and medical treatment of non-ischemic onesmedical treatment of non-ischemic ones