femoston vs tibolone hormone replacement therapy 1.5.15
TRANSCRIPT
1Copyright © 2014 Paras Hospitals. All rights reserved. 1
Dr Nupur GuptaDepartment of Obstetrics & Gynecology
Paras Hospital
Tackling women's midlife crisis: What's new in Hormone Therapy?

2Copyright © 2014 Paras Hospitals. All rights reserved. 2
From Menarche to Menopause
Transition

3Copyright © 2014 Paras Hospitals. All rights reserved. 3
What is Menopause?
Permanent cessation of menstruation resulting from loss of ovarian follicular activity
Perimenopause: from the first features of approaching menopause until up to 1 year after final menstrual period
Burger HG et al. Recent Prog Horm Res 2002;57:257–75.
Years around menopause
Est
rad
iol
(pm
ol/
L)
FS
H (
iu/L
)
0 1 2 3 4 5-1-2-3-4
0
20
40
60
80
100
120
0
50
100
150
200
250
300

4Copyright © 2014 Paras Hospitals. All rights reserved. 4
The Menopause - Acute Symptoms
Hot flushesHot flushes
Night sweatsNight sweats
HeadachesHeadaches
Panic attacksPanic attacks
Mood swingsMood swings
IndecisivenessIndecisiveness
Insomnia leading to:
irritability
poor short term
memory
difficulty with
concentration

5Copyright © 2014 Paras Hospitals. All rights reserved. 5
MEDIUM TERM SYMPTOMSMEDIUM TERM SYMPTOMS
Vaginal drynessVaginal dryness
DyspareuniaDyspareunia
Reduced libidoReduced libido
Thinning skin/ hairThinning skin/ hair
Skin formicationSkin formication
Urethral syndrome (frequency, nocturia & urge Urethral syndrome (frequency, nocturia & urge
incontinence)incontinence)

6Copyright © 2014 Paras Hospitals. All rights reserved. 6
LONG TERM SYMPTOMS
CARDIOVASCULAR DISEASE
OSTEOPOROSIS
CEREBROVASCULAR DISEASE
7Copyright © 2014 Paras Hospitals. All rights reserved. 7
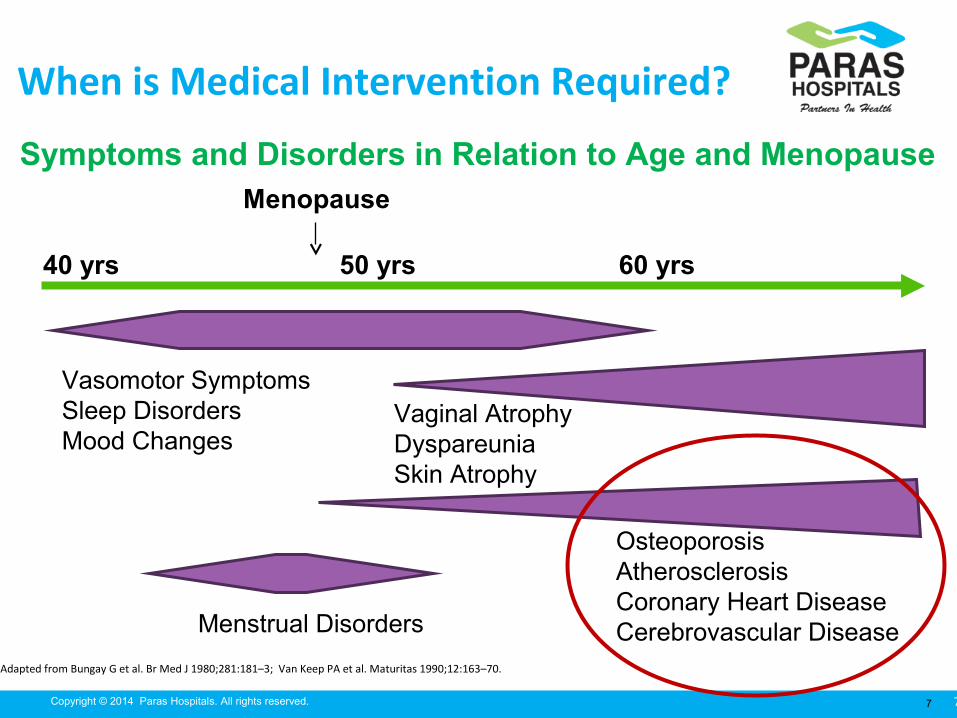
When is Medical Intervention Required?
Adapted from Bungay G et al. Br Med J 1980;281:181–3; Van Keep PA et al. Maturitas 1990;12:163–70.
Vasomotor SymptomsSleep DisordersMood Changes
Vaginal AtrophyDyspareuniaSkin Atrophy
OsteoporosisAtherosclerosisCoronary Heart DiseaseCerebrovascular Disease
40 yrs 50 yrs
Menopause
60 yrs
Symptoms and Disorders in Relation to Age and Menopause
Menstrual Disorders
8Copyright © 2014 Paras Hospitals. All rights reserved. 8
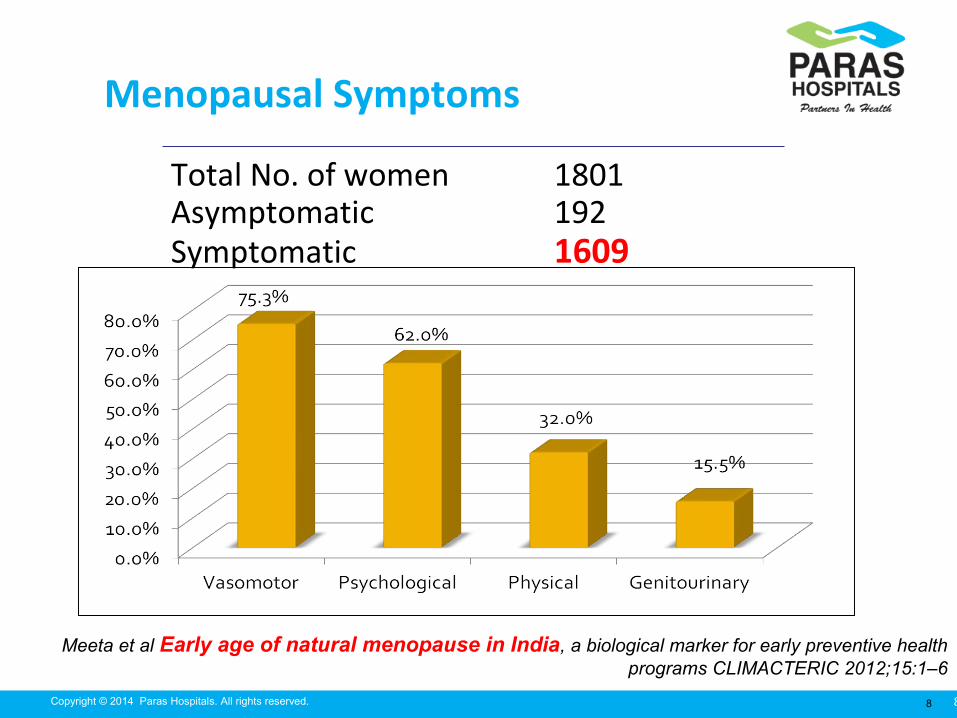
Menopausal Symptoms
Total No. of women 1801Asymptomatic 192Symptomatic 1609
Meeta et al Early age of natural menopause in India, a biological marker for early preventive health programs CLIMACTERIC 2012;15:1–6

9Copyright © 2014 Paras Hospitals. All rights reserved. 9
Attitude of Gynecologists for HT prescription in India
Meherishi S, Khandelwal S; Jr of Midlife Health 2012

10Copyright © 2014 Paras Hospitals. All rights reserved. 10
Rise in female life expectancy over the last 100 years
0
10
20
30
40
50
60
70
80
90
1850 1900 1950 2000
Lifeexpectancy
Age atmenopause

11Copyright © 2014 Paras Hospitals. All rights reserved. 11
a. Counseling: Diet; Exercise
b. Common Indications of Hormone therapy - estrogens,
progestogens, combined therapies and tibolone
– Symptom relief (Vasomotor symptoms)
– Urogenital atrophy
– Bone
MANAGEMENT OPTIONS
Meeta, et al.: Guidelines on menopause. Journal of Mid-life Health ¦ Apr-Jun 2013 ¦ Vol 4 ¦ Issue 2

12Copyright © 2014 Paras Hospitals. All rights reserved. 12
Prescription of HRT: ROUTES
OralOralTransdermal: Transdermal: patch or gelpatch or gel
SubcutaneousSubcutaneous(implant)(implant)
Intramuscular Intramuscular (depot)(depot)
Intra-uterine Intra-uterine (Mirena)(Mirena)
Intra-vaginal Intra-vaginal (tablets, ring (tablets, ring or cream)or cream)

13Copyright © 2014 Paras Hospitals. All rights reserved. 13
Oestrogen Only HRT (ERT)
women who have had a total hysterectomy
If the hysterectomy was subtotal, then may need to use
progestogens as well (some endometrium may be left behind)
If the hysterectomy was for endometriosis, then progestogens
continuously along with oestrogen should be used at least
initially
14Copyright © 2014 Paras Hospitals. All rights reserved. 14
Estrogens
Most Potent
15Copyright © 2014 Paras Hospitals. All rights reserved. 15
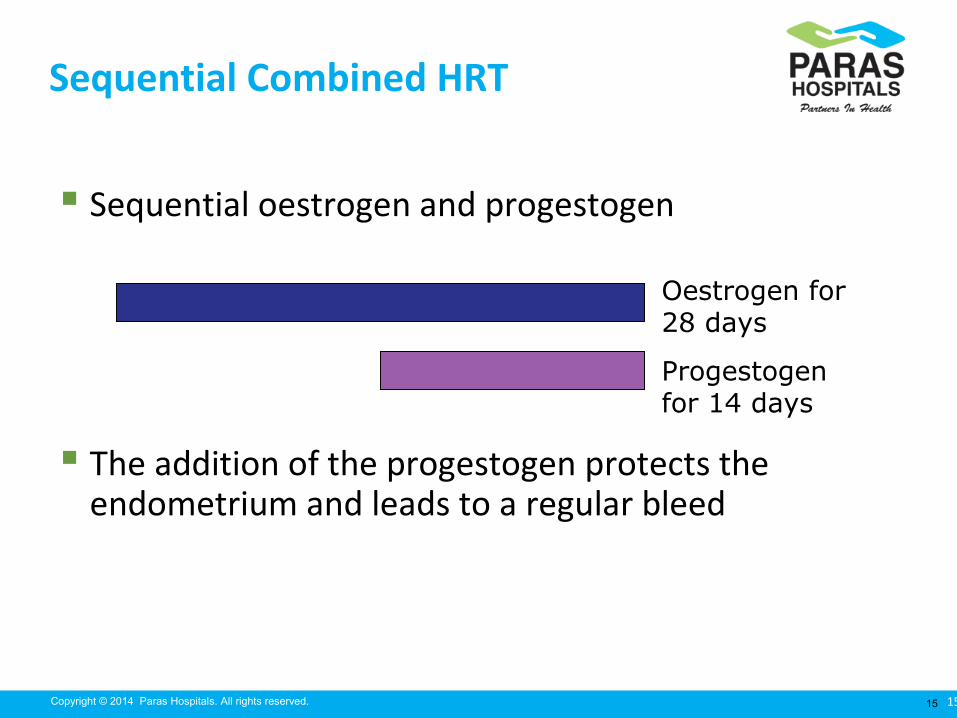
Sequential Combined HRT
Sequential oestrogen and progestogen
The addition of the progestogen protects the endometrium and leads to a regular bleed
Oestrogen for 28 days
Progestogen for 14 days
16Copyright © 2014 Paras Hospitals. All rights reserved. 16
Continuous Combined HRT
This should not be started until 1 year after the LMP
No monthly bleed
Oestrogen combined with progestogen for 28 days

17Copyright © 2014 Paras Hospitals. All rights reserved. 17
Estrogens Used in MHT
Equivalent dose for bone endpoints*
Estrogen Ultra Low Low Standard High
Conjugated equine estrogens (mg) 0.151 0.3 0.625 1.25
17β-estradiol (mg) 0.52 1 2 4
Estradiol valerate (mg) 1 2
Transdermal 17β-estradiol (μg) 143 25 50 100
*Estrogenic effects may vary for other endpoints
The Estrogen Dose Counts
Note: For many women, low-doses of estrogen provide adequate relief of symptoms with high rates of amenorrhea

18Copyright © 2014 Paras Hospitals. All rights reserved. 18
Role of Progestogens in HRT For women with intact uterus, the addition of a progestogen
protects the endometrium from the stimulatory effects of unopposed estrogen
PEPI Trial: Results of Endometrial Biopsy
Conclusion: Adding a progestogen is needed to safeguard the endometrium
Placebo CEE alone CEE+MPA sequential
CEE+MPA continuous
N 119 119 118 120
Normal 98% 38% 95% 99%
Simple hyperplasia 1% 28% 3% 1%
Complex hyperplasia 1% 23% 2% 0%
Atypia 0% 12% 0% 0%
Adenocarcinoma 1% 0% 0% 0%

19Copyright © 2014 Paras Hospitals. All rights reserved. 19
Progestogens: Receptor-binding Activity
ProgestogenProgestog
enicEstroge
nicAndroge
nicAnti-
androgenicGlucocort
icoid
Anti-mineralo-corticoid
Dydrogesterone1 + – – ± – ±
Progesterone1 + – – ± + +
MPA1 + – ± – + –
Norethisterone1 + + + – – –
Drospirenone1 + – – + – +
CPA1 + – – ++ + –
Dienogest1 + ± – + – –
Levonorgestrel1 + – + – – –
Norgestrel1 + – + – – –
Tibolone2 + ± + – – –1. Schindler AE. Maturitas 2003;46(S1):7–16; 2. De Gooyer ME et al. Steroids 2003;68:21–30.
+ Effective; ± Weakly effective; – Not effective.

20Copyright © 2014 Paras Hospitals. All rights reserved. 20
Guidelineson MHT
(Menopausal Hormone Therapy)

21Copyright © 2014 Paras Hospitals. All rights reserved. 21
Guidelines Indian Menopause
Society, 2013
International Menopause
Society, 2013
North American
Menopause Society,
2012
Indication • Most effective for Vasomotor symptoms
• For sleep disturbances & urogenital atrophy
Potential
Benefits
• Positive effects on lipid profile
• Metabolic syn (Type 2 DM, abdominal obesity)

22Copyright © 2014 Paras Hospitals. All rights reserved. 22
Guidelines Indian Menopause
Society, 2013
International Menopause
Society, 2013
North American
Menopause Society,
2012
Age of
Initiation
• Begins within 10 years of menopause or <60 years of age
“Window of opportunity”
Duration
of Use
• Premature menopause: MHT up to natural age of menopause
• 3‑5 years

23Copyright © 2014 Paras Hospitals. All rights reserved. 23
Guidelines
Indian Menopause
Society, 2013
International Menopause
Society, 2013
North American
Menopause Society,
2012
Monitoring • Pre HT work up (Indian MS)‑ ‑• Initial follow-up at 3 months (NAMS)
• Annual follow up – physical, laboratory/imaging (All)‑• Discussion on lifestyle strategies to prevent or
reduce chronic disease

24Copyright © 2014 Paras Hospitals. All rights reserved. 24
Guidelines: Safety Profile of MHT Events Indian Menopause
Society, 2013
International
Menopause
Society, 2013
The North American
Menopause Society,
2012/The Endocrine
Society 2010
CVD • No/lower risk in healthy women <60 years of age or within 10
years of menopause
Breast
CancerIt does not
increase risk if
given for <5 yrs
Small increase in
risk (incidence of
<1.0/1000 women
/year of use)
Risk of events in younger
women is lower than that for
older women
Does not increase
breast cancer risk
if given for <5 yrs
Santen R et al. J Clin Endocrinol Metab 2010;95(Suppl1):S1–S66.

25Copyright © 2014 Paras Hospitals. All rights reserved. 25
MANAGEMENT OF HRT
Initial visitInitial visit
3 months3 months
6 months6 months
Yearly: BP, breast examination and vaginal Yearly: BP, breast examination and vaginal examination (3 yearly smears to age 60 and 3 examination (3 yearly smears to age 60 and 3 yearly mammography aged 50-64)yearly mammography aged 50-64)
Invite earlier visit for specific problemsInvite earlier visit for specific problems

26Copyright © 2014 Paras Hospitals. All rights reserved. 26
Schematic representation of lifetime changes in bone mass
0
10
20
30
40
50
60
70
80
0 25 40 70
Women
Men
Attainment of Consolidation Age related
peak bone mass bone loss
Climacteric
27Copyright © 2014 Paras Hospitals. All rights reserved. 27
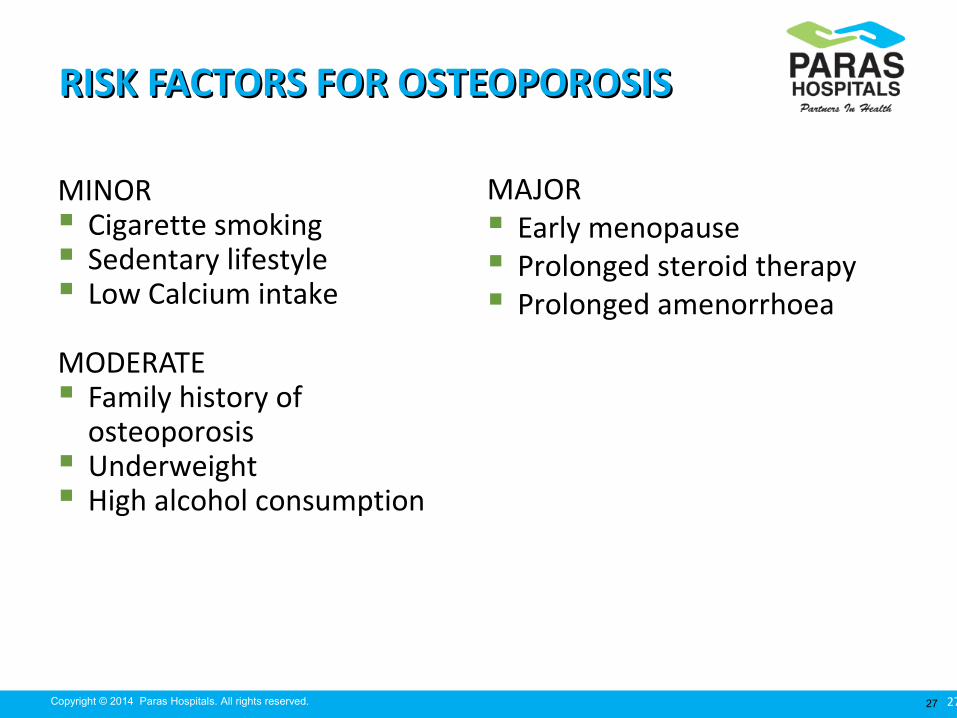
RISK FACTORS FOR OSTEOPOROSISRISK FACTORS FOR OSTEOPOROSIS
MINOR Cigarette smoking Sedentary lifestyle Low Calcium intake
MODERATE Family history of
osteoporosis Underweight High alcohol consumption
MAJOR Early menopause Prolonged steroid therapy Prolonged amenorrhoea

28Copyright © 2014 Paras Hospitals. All rights reserved. 28
Benefits and HRT: Osteoporosis
Its beneficial effect on bone Its beneficial effect on bone diminishes soon diminishes soon
after stopping treatmentafter stopping treatment
However HRT remains the treatment of choice However HRT remains the treatment of choice
in women with in women with premature ovarian failurepremature ovarian failure
29Copyright © 2014 Paras Hospitals. All rights reserved. 29
Hormonal Therapy for OsteoporosisInternational Menopause Society Global Consensus 2013 Statement
MHT is an effective
treatment for the prevention
of fracture (vertebral/hip) in
at-risk women before age
60 years or within 10 years
after the menopause
De Villiers TJ et al. Climacteric 2013;16:316–37.

30Copyright © 2014 Paras Hospitals. All rights reserved. 30
What’s New in MHT?

31Copyright © 2014 Paras Hospitals. All rights reserved. 31
Fournier A et al. Breast Cancer Res Treat 2008;107:103–11; Fournier A et al. J Clin Oncol. 2008 ;26:1260–1268.
Choice of Progestogen & Breast Cancer Risk:E3N French Cohort Study: 2007
Risk of breast cancer
N = 80,377 womenDuration = 8.1 years
Risk elevation may not be uniform
for all progestogens
E/D - 17ß-Estradiol + Dydrogesterone

32Copyright © 2014 Paras Hospitals. All rights reserved. 32

33Copyright © 2014 Paras Hospitals. All rights reserved. 33
Invasive Breast Cancer associated with Different types & Times since last use of MHT
Mean duration of use
N -169N - 638
N - 931
5.1 yrs 6.1 yrs 6.1 yrs
Fournier A et al. Breast Cancer Res Treat (2014) 145:535–543
78,353 women
Haz
ard
Rat
io
34Copyright © 2014 Paras Hospitals. All rights reserved. 34
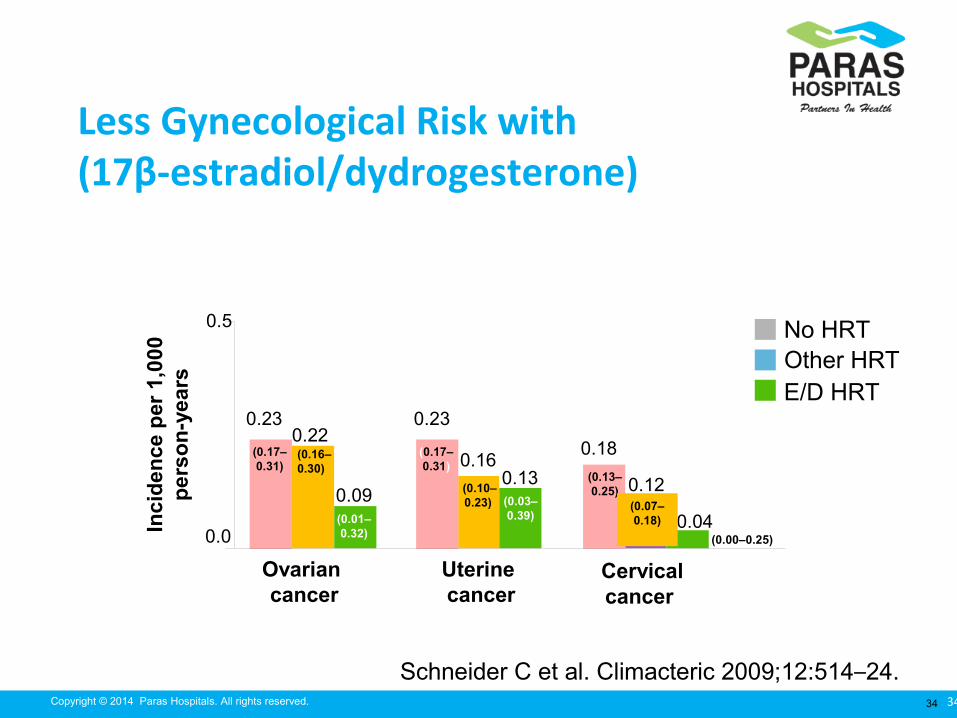
Less Gynecological Risk with (17β-estradiol/dydrogesterone)
Schneider C et al. Climacteric 2009;12:514–24.
Inci
den
ce p
er 1
,000
per
son
-yea
rs
Ovarian cancer
Uterine cancer
Cervical cancer
0.0
0.5
0.23
0.180.22
0.160.12
0.090.13
0.04
0.23
(0.17–0.31)
(0.16–0.30)
No HRTOther HRTE/D HRT
(0.01–0.32)
(0.17–0.31)
(0.10–0.23) (0.03–
0.39)
(0.13–0.25)
(0.07–0.18)
(0.00–0.25)

35Copyright © 2014 Paras Hospitals. All rights reserved. 35
Risks and HRT: Stroke
In RCT’s HRT In RCT’s HRT increased the risk of stroke increased the risk of stroke (mostly (mostly ischaemic) compared with placeboischaemic) compared with placebo
Older womenOlder women have a greater absolute risk of stroke have a greater absolute risk of stroke
Risk may depend on Risk may depend on oestrogen doseoestrogen dose

36Copyright © 2014 Paras Hospitals. All rights reserved. 36
No Increased CV Risk Demonstrated with (17β estradiol/dydrogesterone)
Schneider C et al. Climacteric 2009;12:445–53.
0.0
0.2
0.4
0.6
0.8
1.0
1.2
0.58
0.93
0.660.68
1.10
0.95
0.40
0.27 0.31
Myocardial
infarctionStroke
Venous thromboembolism
Inci
den
ce p
er 1
000
per
son
-yea
rs
No MHT
Other MHT
E/D MHT
(0.48–0.70)
(0.57–0.82)
(0.18–0.76)
(0.80–1.07)
(0.95–1.26)
(0.10–0.58)
(0.56–0.79)
(0.82–1.11)
(0.13–0.64)
37Copyright © 2014 Paras Hospitals. All rights reserved. 37
Risks and HRT: Venous Thromboembolism
Oral HRT has been associated with an increased risk of DVT
and PE in RCT’s and observational studies.
Evidence suggests that it is higher with combined HRT than
oestrogen-only HRT and that these events are more likely in
the first year of use

38Copyright © 2014 Paras Hospitals. All rights reserved. 38
Risk of Thromboembolism with Different ProgestogensESTHER case-control study 271 consecutive VTE cases (mean age: 61.6 years) and 610 controls (mean age: 61.5 years)
Canonico M. Circulation 2007;115:840–5.
Ad
just
ed O
Rs
(95%
CI)
fo
r V
TE
wit
h o
ral a
nd
tra
nsd
erm
al
estr
og
en v
s. n
on
-use
rs
(e.g. dydrogesterone)
Pregnane derivatives & micronized progesterone appear to have the least thrombotic risk profile
(1.5–11.6)
(0.3–1.9) (0.4–2.3)
(1.5–10.0)

39Copyright © 2014 Paras Hospitals. All rights reserved. 39
N – 362; Healthy postmenopausal women; 39–74 years
Continuous E/D 1/5 mg vs. CEE/MPA
A.T. de Kraker et al. / Maturitas 49 (2004) 253–263
HDL-C

40Copyright © 2014 Paras Hospitals. All rights reserved. 40
N = 193; Duration = 24 weekN = 193; Duration = 24 week
E/D - ↑ HDL E/D - ↑ HDL
CEE/N - ↓ CEE/N - ↓ HDLHDL
CEE/N - ↑ incidence, duration & severity of bleedingCEE/N - ↑ incidence, duration & severity of bleeding
Sequential E/D 1/10mg vs. CEE/Norgestrel (0.625/0.15 mg)
Cieraad D et al. Arch Gynecol Obstet 2006;274:74–80.
HDL-C

41Copyright © 2014 Paras Hospitals. All rights reserved. 41
Sequential E/D1/10 and 2/10: HDL Profile
Stevenson JC, Rioux JE, Komer L, Gelfand M. Climacteric 2005;8:352–9. ©2005 Informa Healthcare. Figure reproduced with permission of Informa Healthcare.
Placebo (n=54)1/5 mg (n=62)1/10 mg (n=74)
Cycle 13 Cycle 26
0
5
10
15
20
25
*
* *
Increase in HDL cholesterol (%)
*p≤0.05 vs. placebo

42Copyright © 2014 Paras Hospitals. All rights reserved. 42
Low-Dose Sequential E/ D: Blood Glucose and Insulin
• E/D can affect menopausal changes in insulin secretion/elimination
Fasting glucose (mmol/L)
Fasting insulin (mU/L)
0
1
2
3
4
5
6
Baseline Year 1 Year 2
4.14
5.13
3.12* 2.88**
4.96* 4.87**
Mea
n co
ncen
trat
ion
of
gluc
ose
or in
sulin
Godsland IF et al. Clin Endocrinol (Oxf) 2004;60:541–9.

43Copyright © 2014 Paras Hospitals. All rights reserved. 43
-15
-10
-5
0
5
10
15
0 3 12 months
Am
bu
lato
ry s
ysto
lic B
P
chan
ge
fro
m b
asel
ine
(%)
Estradiol/Dydrogesterone 1/10 (n=14)
No treatment (n=15)
Normotensive women
Van Ittersum FJ et al. Am J Hypertens 1998;11:1147–52.
Sequential E/D 1/10: Decreased Systolic BP During Long-Term Therapy
6 9
*
*
*p<0.05 vs. baseline

44Copyright © 2014 Paras Hospitals. All rights reserved. 44
Fact - MHT users gain less weight or body fat than nonusers)1
2 years, body fat mass (N=100)2
17β-Estradiol/Dydrogesterone reduced the body fat
mass (↓ –1.2%)
Women not taking MHT (↑ +3.6%)
Transdermal MHT (↑ +4.7%)
Tibolone users (no change)
Is there a risk of weight gain with MHT?
1. Santen RJ et al. J Clin Endocrinol Metab 2010;95(7 Suppl 1):s1–66.2. Hänggi W et al. Clin Endocrinol (Oxf) 1998;48:691–9.

45Copyright © 2014 Paras Hospitals. All rights reserved. 45
Conclusion
Used by the right woman, at the right dose & right age, Used by the right woman, at the right dose & right age, Femoston:Femoston:
Relieve vasomotor and other menopausal symptomsRelieve vasomotor and other menopausal symptoms
Provide protection against bone loss (second line)Provide protection against bone loss (second line)
Provide acceptable bleeding patternsProvide acceptable bleeding patterns

46Copyright © 2014 Paras Hospitals. All rights reserved. 46
Tibolone
Dr Rama YadavJunior Consultant,
Dr Nupur GuptaDepartment of Obstetrics & Gynecology
PARAS HOSPITALS

47Copyright © 2014 Paras Hospitals. All rights reserved. 47
Tibolone
oestrogenic oestrogenic
androgenic androgenic
progestogenic agentprogestogenic agent
STEAR ( Selective Tissue Estrogen Activity STEAR ( Selective Tissue Estrogen Activity
Regulator)Regulator)
48Copyright © 2014 Paras Hospitals. All rights reserved. 48
Tibolone for Menopausal symptoms
↓ hot flushes
↓ headache, insomnia, fatiguability
Mood changes[increases endorphins]
Increases sexual function[libido]
Improves vaginal atrophy
Improves urogenital symptoms

49Copyright © 2014 Paras Hospitals. All rights reserved. 49
Tibolone and Bone
↑ BMD 2.6% vs -2.3% in placebo after 2 years
(Gallagher et al,2001; J Clin Endo Metab)
Other RCTs show ↑BMD.
No data from RCT on fracture risk available
Consensus: Tibolone as effective as EPT/ET in preventing bone
loss.
International Tibolone Consensus Group; Maturitas,2005

50Copyright © 2014 Paras Hospitals. All rights reserved. 50
Tibolone and Cardiovascular system
Favorable effect on lipid profile:
↓Triglyceride- 25%
↓ HDL-C 34%
No effect on LDL and Lipoprotein(a)
No effect- Antithrombin3, Plasminogen, CRP
–J Clin Endo Metab; 2002
Inconclusive evidence on cardiovascular clinical outcomes and
VTE with regard to risk or benefit.
International Tibolone Consensus Group; Maturitas,2005
51Copyright © 2014 Paras Hospitals. All rights reserved. 51
Tibolone and Breast
Inhibits formation of active estrogen in breast
Antiproliferative and antiapoptotic
↓ breast tenderness
↓ mammographic density
Inconclusive evidence on breast cancer incidence. RCTs
awaited.
International Tibolone Consensus Group; Maturitas,2005

52Copyright © 2014 Paras Hospitals. All rights reserved. 52
Tibolone and Endometrium
Prevents endometrial proliferation
(Volker et al,2001; Climacteric)
No increase in size or volume of myomas
Addition of progestogen not required[as progestogenic]
Standard endometrial surveillance not required
(International Tibolone Consensus Group;
Maturitas,2005)

53Copyright © 2014 Paras Hospitals. All rights reserved. 53
Tibolone or Livial This is an alternative CC HRT
It is a gonadomimetic containing oestrogen, progestogens & androgens
Licensed for vasomotor symptoms and osteoporosis
The risk: benefit ratio similar to HRT in women under 60, but over 60 increased risk of stroke
Slightly increased risk for endometrial cancer
Less risk of breast cancer compared with CCT but increased over ERT
May help libido due to androgen content

54Copyright © 2014 Paras Hospitals. All rights reserved. 54
Side-effects Leucorrhoea
Abdominal pain
Weight gain
Vaginal bleeding( less than with continuous EPT)
Breast pain( less than with continuous EPT)

55Copyright © 2014 Paras Hospitals. All rights reserved. 55
Indication
Tibolone may have added value in
Women with low sex drive
Women with mood disorders
Women with risk of accelerated bone loss
Women with premenopausal breast tenderness
Women with high breast density
Women with fibroids
Women with urogenital complaints

56Copyright © 2014 Paras Hospitals. All rights reserved. 56
Contraindications
Pregnancy n lactation [teratogenic]
Estrogen dependant cancer
Thrombophilic disorders
VTE/CAD
Liver diseases
Porphyria
Known/suspected ca breast/Ovary

57Copyright © 2014 Paras Hospitals. All rights reserved. 57
Tibolone vs Combined HT: Cochrane 2012
Formoso G, Perrone E,Maltoni S, Balduzzi S, D’Amico R, Bassi C, Basevi V,Marata AM,Magrini N,Maestri E. Short and long term effects of tibolone in postmenopausal women. Cochrane Database of Systematic Reviews 2012, Issue 2
p = .015
p = .0006
Total no. of Events

58Copyright © 2014 Paras Hospitals. All rights reserved. 58
Tibolone vs 17β-Estradiol/dydrogesterone
Hänggi et al. 1997. British Journal of Obstetrics and Gynaecology. 1997;104:708–17

59Copyright © 2014 Paras Hospitals. All rights reserved. 59
Long term safety
Symptomatic benefits of tibolone appear
questionable compared to those of combined HT
More concerning is uncertainty about Tibolone’s
risk profile
Tibolone vs Combined HT: Cochrane 2012
Formoso G, Perrone E,Maltoni S, Balduzzi S, D’Amico R, Bassi C, Basevi V,Marata AM,Magrini N,Maestri E. Short and long term effects of tibolone in postmenopausal women. Cochrane Database of Systematic Reviews 2012, Issue 2

60Copyright © 2014 Paras Hospitals. All rights reserved. 60
Take home message
Better effects than HRT/ERT
LIVIAL 2.5mg starting dose
Best for women with estrogen contraindication
Better improvements in vasomotor symptoms, osteoporosis
No known toxicity
.

61Copyright © 2014 Paras Hospitals. All rights reserved. 61Thank you