federal register /vol. 66, no. 13/friday, january 19, 2001 ... · 5448 federal register/vol. 66,...
TRANSCRIPT

5447Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
involved in nuclear, missile, or militaryactivities included in Supplement No. 4to part 744 (Entity List). All licenseapplications for exports and reexports toIndia and Pakistan not meeting thesecriteria for presumption of denial willbe considered on a case-by-case basisunder other licensing policies set forthin the EAR applicable to suchcomputers.
(iv) Post-shipment verification. Thissection outlines special post-shipmentreporting requirements for exporters ofcertain computers to destinations inComputer Tier 3. Post-shipment reportsmust be submitted in accordance withthe provisions of this paragraph(b)(3)(iv), and all relevant records ofsuch exports must be kept in accordancewith part 762 of the EAR.
(A) Exporters must file post-shipmentreports for computer exports, as well asexports of items used to enhancepreviously exported or reexportedcomputers, according to the followingschedule:
(1) For exports occurring prior toFebruary 26, 2001, where the CTP isgreater than 12,500 MTOPS;
(2) For exports on or after February26, 2001, but before March 20, 2001where the CTP is greater than 28,000MTOPS; and
(3) For exports on or after March 20,2001 where the CTP is greater than85,000 MTOPS.
(B) Information that must be includedin each post-shipment report. No laterthan the last day of the month followingthe month in which the export takesplace, the exporter must submit thefollowing information to BXA at theaddress listed in paragraph (b)(3)(iv)(C)of this section:
(1) Exporter name, address, andtelephone number;
(2) License number;(3) Date of export;(4) End-user name, point of contact,
address, telephone number;(5) Carrier;(6) Air waybill or bill of lading
number;(7) Commodity description,
quantities—listed by model numbers,serial numbers, and CTP level inMTOPS; and
(8) Certification line for exporters tosign and date. The exporter must certifythat the information contained in thereport is accurate to the best of his orher knowledge.
(C) Mailing address. A copy of thepost-shipment report[s] required underparagraph (b)(3)(iv)(A) of this sectionshall be delivered to one of thefollowing addresses. Note that BXA willnot accept reports sent C.O.D.
(1) For deliveries by U.S. postal service:U.S. Department of Commerce,Bureau of Export Administration, P.O.Box 273, Washington, D.C. 20044,Attn: Office of Enforcement AnalysisHPC Team, Room 4065.
(2) For courier deliveries: U.S.Department of Commerce, Office ofEnforcement Analysis HPC Team,14th Street and Constitution Ave.,NW, Room 4065, Washington, DC20230.
* * * * *
PART 748—[AMENDED]
6. Section 748.10 is amended byrevising paragraph (b)(3) as follows:
§ 748.10 Import and end-user certificates.
* * * * *(b) * * *(3) Your transaction involves an
export to the People’s Republic of China(PRC) of a computer. You must obtaina PRC End-User Certificate, regardless ofdollar value, as follows:
(i) For exports of computers asdescribed by § 740.7(d)(2) of the EAR,regardless of value, to the People’sRepublic of China. (See paragraph (c) ofthis section for information on obtainingthe PRC End-User Certificate.) Exportersare required to obtain a PRC End-UserCertificate before exporting computersto the PRC. In addition, exporters arerequired to provide the PRC End-UserCertificate Number to BXA as part oftheir post-shipment report (see§ 740.7(d)(5)(v) of the EAR). Whenproviding the PRC End-User CertificateNumber to BXA, you must identify thetransaction in the post shipment reportto which that PRC End-User CertificateNumber applies. The original PRC End-User Certificate shall be retained in theexporter’s files in accordance with therecordkeeping provisions of § 762.2 ofthe EAR.
(ii) For exports of computers thatrequire license applications.* * * * *
Dated: January 16, 2001.
Matthew S. Borman,Acting Deputy Assistant Secretary for ExportAdministration.[FR Doc. 01–1623 Filed 1–16–01; 4:49 pm]
BILLING CODE 3510–33–P
DEPARTMENT OF HEALTH ANDHUMAN SERVICES
Food and Drug Administration
21 CFR Parts 207, 807, and 1271
[Docket No. 97N–484R]
Human Cells, Tissues, and Cellular andTissue-Based Products; EstablishmentRegistration and Listing
AGENCY: Food and Drug Administration,HHS.ACTION: Final rule.
SUMMARY: The Food and DrugAdministration (FDA) is issuing a finalrule to require human cells, tissue, andcellular and tissue-based productestablishments to register with theagency and list their human cells,tissues, and cellular and tissue-basedproducts. FDA is also amending theregistration and listing regulations thatcurrently apply to human cells, tissues,and cellular and tissue-based productsregulated as drugs, devices, and/orbiological products. These actions arebeing taken to establish a unifiedregistration and listing program forhuman cells, tissues, and cellular andtissue-based products.DATES: The regulation is effective April4, 2001, except for 21 CFR 207.20(f),807.20(d), and 1271.3(d)(2), which areeffective on January 21, 2003.FOR FURTHER INFORMATION CONTACT:Valerie A. Butler, Center for BiologicsEvaluation and Research (HFM–17),Food and Drug Administration, 1401Rockville Pike, suite 200N, Rockville,MD 20852–1448, 301–827–6210.SUPPLEMENTARY INFORMATION:
I. Introduction
We, FDA, are putting in place acomprehensive new system ofregulation for human cells, tissues, andcellular and tissue-based products. Thegoal of the new approach is to improveprotection of the public health withoutimposing unnecessary restrictions onresearch, development, or theavailability of new products. Under thenew system, the regulation of differenttypes of human cells, tissues, andcellular and tissue-based products willbe commensurate with the public healthrisks presented, enabling us to use ourresources more effectively.Consolidating the regulation of humancells, tissues, and cellular and tissue-based products into one regulatoryprogram is expected to lead to increasedconsistency and greater efficiency.Together, these planned improvementswill increase the safety of human cells,
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00021 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1
5448 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
tissues, and cellular and tissue-basedproducts, and public confidence in theirsafety, while encouraging thedevelopment of new products.
A. BackgroundIn 1997, we announced our regulatory
plans for human cells, tissues, andcellular and tissue-based products intwo documents:
• ‘‘A Proposed Approach to theRegulation of Cellular and Tissue-BasedProducts’’ (62 FR 9721, March 4, 1997)and
• ‘‘Reinventing the Regulation ofHuman Tissue’’ (Ref. 1).The proposed approach described acomprehensive plan for regulatinghuman cells, tissues, and cellular andtissue-based products that wouldinclude establishment registration andproduct listing, donor-suitabilityrequirements, good tissue practiceregulations, and other requirements.Under this tiered, risk-based approach,we proposed to exert only the type ofgovernment regulation necessary toprotect the public health. To accomplishthis goal, we planned to issue newregulations under the communicabledisease provisions of the Public HealthService Act (the PHS Act). Some humancellular and tissue-based productswould be regulated only under thesenew regulations, while other humancellular and tissue-based productswould also be regulated as drugs,devices, and/or biological drugs. Werequested written comments on theproposed approach and, on March 17,1997, held a public meeting (62 FR9721).
Since 1997, we have published threeproposed rules to implement theproposed approach. In 1998, as a firststep toward accomplishing these goals,we published the proposed rule,‘‘Establishment Registration and Listingfor Manufacturers of Human Cellularand Tissue-Based Products’’ (63 FR26744, May 14, 1998) (the ‘‘registrationproposed rule’’). That rule proposed torequire cell and tissue establishments toregister with us and submit a list of theirhuman cellular and tissue-basedproducts. We also proposedmodifications to current registration andlisting requirements for drugs anddevices under which cell and tissueestablishments already regulated underthe Federal Food, Drug, and CosmeticAct (the act) and/or section 351 of thePHS Act (42 U.S.C 262) would registerand list following the new procedures.
In addition to the registrationproposed rule, we published two moreproposed rules:
• Suitability Determination forDonors of Human Cellular and Tissue-
Based Products (64 FR 52696,September 30, 1999) (the ‘‘donor-suitability proposed rule’’); and
• Current Good Tissue Practice forManufacturers of Human Cellular andTissue-Based Products; Inspection andEnforcement (66 FR 1508, January 8,2000) (the ‘‘GTP proposed rule’’).Together, these three rules whenfinalized would establish acomprehensive regulatory program forhuman cellular and tissue-basedproducts, to be contained in part 1271(21 CFR part 1271).
In the three proposed rules, we usedthe term ‘‘human cellular and tissue-based products.’’ In this final rule, wehave changed the term to ‘‘human cells,tissues, and cellular and tissue-basedproducts’’ (abbreviated ‘‘HCT/P’s’’).This change in terminology is aclarification and does not affect thescope of the definition, which continuesto encompass an array of articlescontaining or consisting of human cellsor tissues, and intended forimplantation, transplantation, infusion,or transfer into human recipients,including investigational products. Thedefinition of ‘‘human cells, tissues, orcellular or tissue-based product’’ isintended to cover HCT/P’s at all stagesof their manufacture, from recoverythrough distribution. Some examples ofHCT/P’s include skin, tendons, bone,heart valves, corneas, hematopoieticstem cells, manipulated autologouschondrocytes, epithelial cells on asynthetic matrix, and semen or otherreproductive tissue.
B. Implementation of the NewRegulations
We had intended to finalize theregistration proposed rule with the twoother rules that would make up part1271 in its entirety, and to implementall three rules together. However, we arenow making the registration rule final,with staggered effective dates, beforefinalizing the two remaining portions ofpart 1271. We are taking this actionbecause of recent concerns raised aboutthe safety of tissue, which have led usto believe that accelerating thecollection of basic information about therapidly growing tissue industry is vital.This medical sector has grown rapidly,with a need for clearer standards andimproved accountability. TheDepartment of Health and HumanServices met in mid-2000 withrepresentatives of key tissue-relatedorganizations, who supportedfinalization of this regulation as quicklyas possible, instead of awaitingsimultaneous publication with the othertissue regulations. For these reasons, weare going to begin collecting registration
and listing information, whilecontinuing to develop the remainder ofthe final rules that will complete part1271, and we have changed the effectivedate of this rule from the proposed 180days to 75 days after the date ofpublication in the Federal Register. Aspart of completing the rulemaking forpart 1271, we would make anynecessary conforming amendments tothis regulation to make it consistentwith any changes made in theremainder of the rulemaking process,and we would revoke part 1270.
Establishments that engage in therecovery, screening, testing, processing,storage, or distribution of human tissueintended for transplantation currentlyregulated under section 361 of the PHSAct (42 U.S.C. 264) and the regulationsin part 1270 (21 CFR part 1270)(‘‘Human Tissue Intended forTransplantation’’) will be required tobegin registering with the agency andlisting their HCT/P’s within 30 daysafter the effective date of this final rule.The effective date for all other humancells, tissues, and cellular and tissue-based products (as described in§ 1271.3(d)(2)) is 2 years afterpublication, by which time we expect tohave completed rulemaking for all thesubparts of part 1271. (Someestablishments that are not required toregister and list until the secondeffective date have expressed a desire tosubmit registration and listing forms assoon as possible. In response, FDA isprepared to accept registration andlisting forms submitted in advance ofthe second effective date. However, FDAis not soliciting this information.) Oncethe entire rulemaking is complete, thenew regulatory approach would applyto a broad range of human cells, tissues,and cellular and tissue-based products,including reproductive cells and tissue;hematopoietic stem cells; and tissuesand cells regulated as devices, drugs,and/or biological products.
Staggering the effective dates of thisregulation permits us to begin collectingimportant registration and listinginformation soon from thoseestablishments currently regulatedunder part 1270, while continuing toproceed through rulemaking to developthe remainder of part 1271. We believethat this action may prevent anunintentional gap in the regulation ofcertain currently regulated HCT/P’s,permit an orderly implementationprocess, and avoid duplicativeinformation collection. If we insteadimplemented the regulationimmediately for all HCT/P’s, this actioncould have the effect of shifting theregulation of certain products (e.g.,HCT/P’s currently regulated as devices
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00022 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5449Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
that meet the criteria set out in§ 1271.10 for regulation solely undersection 361 of the PHS Act) into the newregulatory system before standards andenforcement provisions are in place.Staggering the effective dates also helpspermit an orderly implementationprocess. Establishments thatmanufacture cells and tissues that willbe regulated for the first time under newpart 1271 may require more time thanthose currently regulated to implementthe provisions of this final rule.However, we also recognize thatunanticipated delays in completing therulemaking for the remainder of part1271 could occur. Should therulemaking proceedings be delayed pastthe 2-year timeframe, we will considerwhether to maintain the 2-year effectivedate for the HCT/P’s described in§ 1271.3(d)(2) or whether to extend thatdate for some or all of those HCT/P’s.
C. Legal AuthorityWe are issuing this final rule under
the authority of section 361 of the PHSAct. Under section 361 of the PHS Act,we may make and enforce regulationsnecessary to prevent the introduction,transmission, or spread ofcommunicable diseases between theStates or from foreign countries into theStates. (See sec. 1, Reorg. Plan No. 3 of1966 at 42 U.S.C. 202 for delegation ofsection 361 of the PHS Act authorityfrom the Surgeon General to theSecretary, Health and Human Services;see 21 CFR 5.10(a)(4) for delegationfrom the Secretary to FDA.) Intrastatetransactions may also be regulatedunder section 361 of the PHS Act. (SeeLouisiana v. Mathews, 427 F. Supp. 174,176 (E.D. La. 1977).)
HCT/P’s are derivatives of the humanbody and thus pose a potential risk oftransmitting infectious disease. We havedetermined that some HCT/P’s may beeffectively regulated solely bycontrolling the infectious disease risksthey present. The regulation now beingfinalized forms the foundation for aregulatory program that will further thegoal of preventing the transmission ofcommunicable disease. To beginimplementing this regulatory program,we are publishing the registration finalrule, with staggered effective dates sothat those HCT/P establishments notcurrently subject to regulation undersection 361 of the PHS Act will haveadequate preparation time and FDA cancontinue working towards finalizing theremainder of the program.
For this regulatory system to beeffective in preventing the spread ofdisease, we must obtain basicinformation about the human cell andtissue industry and its HCT/P’s. The
information to be submitted incompliance with the registration andlisting requirements in subpart B willprovide baseline data on establishmentsthat will be subject to part 1271. Thisinformation from the registration rulewill assist us in reacting swiftly tonewly discovered or understood risks byalerting members of the industry to ourconcerns and, when appropriate, byconducting establishment inspections.Without this information, we would notbe able to effectively monitorcompliance with the proposed donor-suitability, GTP, and other regulationsthat make up the rest of the regulatoryprogram.
Authority for enforcement of section361 of the PHS Act is provided bysection 368 of the PHS Act (42 U.S.C.271). Under section 368(a) of the PHSAct, any person who violates aregulation prescribed under section 361of the PHS Act may be punished byimprisonment for up to 1 year.Individuals may also be punished forviolating such a regulation by a fine ofup to $100,000 if death has not resultedfrom the violation or up to $250,000 ifdeath has resulted (18 U.S.C. 3559 and3571(c)). In addition, Federal DistrictCourts have jurisdiction to enjoinindividuals and organizations fromviolating regulations implementingsection 361 of the PHS Act. Theregulations that we have proposedspecific to enforcement appear in theGTP proposed rule.
HCT/P’s that do not meet FDA’scriteria set forth in part 1271 forregulation solely under section 361 ofthe PHS Act are regulated as drugs,devices, and/or biological productsunder the act and/or section 351 of thePHS Act, and their manufacturers arerequired to register with the agencyunder section 510 of the act (21 U.S.C.360). Regulations implementing section510 of the act are found in parts 207 and807 (21 CFR parts 207 and 807), amongother parts. In order to consolidate ourdata base on the cell and tissue industryand thus to improve our oversightfunctions, we are amending parts 207and 807 to require registeringestablishments to follow the proceduresset out in part 1271; these amendmentsare effective in 2 years, when we projectthe remaining two proposed tissue ruleswill be ready for implementation.Section 510 of the act remains theauthority for the substantive registrationrequirement for products subject toparts 207 and 807. Because harmonizingthe registration and listing proceduresapplicable to the various HCT/P’s isintended to further the goal ofpreventing the spread of communicabledisease, we are relying on the additional
authority of section 361 of the PHS Actfor the proposed amendments to parts207 and 807.
II. Highlights of the Final Rule
A. Plain Language
On June 1, 1998, President Clintondirected Federal agencies to begin using‘‘plain language’’ in regulations andother documents. The goal of the plainlanguage initiative is to publishgovernment documents that are easier tounderstand.
In response to this initiative, we havewritten the registration regulation inplain language. We have
• Written the regulation in question-and-answer format,
• Reorganized some regulatorysections for greater clarity, and
• Followed other plain-languageconventions, such as using ‘‘must’’instead of ‘‘shall.’’The resulting codified language is easierto read and understand than theproposed regulation. These editorialchanges are for clarity only and do notchange the substance of therequirements.
B. Framework of the Final Regulationand Part 1271
When final, new part 1271 will bemade up of six subparts. This finalregulation contains subpart A (generalprovisions pertaining to the scope andapplicability of part 1271; definitions);and subpart B (registration and listingprocedures). The donor-suitabilityproposed rule contains subpart C of part1271; and the GTP proposed rulecontains subparts D, E, and F.
Section 1271.10, in subpart A, sets outthe criteria that form the foundation ofour tiered, risk-based approach toregulating HCT/P’s. HCT/P’s that meetthese criteria are subject only toregulation under section 361 of the PHSAct. When all the proposed rules thatwill make up part 1271 becomeeffective, these HCT/P’s would besubject to the regulations in part 1271,and no premarket submissions would berequired. (We sometimes refer to theseHCT/P’s as ‘‘361 HCT/P’s.’’ This termreplaces ‘‘section 361 products,’’ whichwas used in the registration proposedrule.) HCT/P’s that do not meet thecriteria for regulation as 361 HCT/P’swill be regulated as drugs, devices, and/or biological products.
In September 1999, in the donor-suitability proposed rule, we modifiedproposed §§ 1271.1, 1271.3(e), 1271.10,and 1271.20 as they appeared in theregistration proposed rule, and weadded new § 1271.15. We made some ofthese changes to clarify our meaning.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00023 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5450 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
We made other changes so that theprovisions on scope and applicabilitycontained in subpart A would apply notonly to the registration procedures insubpart B but more generally to the restof the requirements in part 1271. Thesechanges obviated the need for theaddition, in later rulemaking, of newsections dealing with scope andapplicability and were consistent withour original regulatory intent, as set outin the proposed approach.
We received comments on theregistration proposed rule, and wereceived additional comments onsubparts A and B of part 1271 inresponse to the donor-suitabilityproposed rule. To the extent possible weaddress these comments in this finalrule; however, we recognize thatadditional discussion may be necessaryas issues arise in the remaining rulesthat will makeup part 1271.
C. Staggered Effective DatesIn order to accomplish the goal of
staggering the effective dates of theregistration and listing regulation fordifferent types of HCT/P’s, we havedivided the definition of ‘‘HCT/P’’ in§ 1271.3(d) into two paragraphs.Paragraph (d)(1) of § 1271.3 identifiesthe subgroup of human tissues definedin part 1270. Paragraph (d)(2) providesthe broader definition of HCT/P basedon proposed § 1271.3(e). The definitionof the subgroup in paragraph (d)(1)incorporates the definition of ‘‘humantissue’’ set out in § 1270.3(j) and thusidentifies those tissues that are currentlyregulated under part 1270, including,for example, such tissues as corneas,bone, and skin. This represents thesubgroup of human cells, tissues, andcellular and tissue-based products forwhich this final rule will first go intoeffect. Paragraph (d)(2) of § 1271.3provides the broader definition of HCT/P and includes those HCT/P’s describedin paragraph (d)(1) as well as suchadditional HCT/P’s as reproductive cellsand tissues, hematopoietic stem cells,and cells and tissues currently regulatedas drugs, devices, and/or biologicalproducts. The definition in paragraph(d)(2) of § 1271.3 will eventually replaceparagraph (d)(1), as described below.
The effective date of § 1271.3(d)(1) is75 days after the publication of this rule.The entire definition of HCT/P in§ 1271.3(d)(2) is effective 2 years afterthe publication of this final rule in theFederal Register. The effect of thisaction is to make this final regulationapplicable first to those HCT/P’scurrently regulated under part 1270, andlater to the complete range of HCT/P’sdefined in § 1271.3(d)(2). When all ofthe regulations that make up part 1271
are final and have superseded part 1270,we will revoke § 1271(d)(1) andrenumber (d)(2) as a conformingamendment. At that time the newregulatory framework contained in part1271 will be instituted as a whole.
D. Other Highlights of This Final Rule
This final rule contains other changesfrom the proposed rule. Among thesechanges are the following:
• We have broadened ‘‘family-relatedallogeneic use,’’ as used in proposed§ 1271.10, to include first-degree andsecond-degree blood relatives.
• We have modified the definition of‘‘homologous use.’’
• We have replaced the phrase‘‘combined with or modified by theaddition of a drug or a device’’ in§ 1271.10 with new language.
• We have deleted the phrase‘‘pending scheduled’’ from theexception in § 1271.15(d) forestablishments that only receive or storeHCT/P’s.
• We have added an exception forestablishments that only recoversreproductive cells or tissues forimmediate transfer into a sexuallyintimate partner of the cell or tissuedonor. (§ 1271.15(e)).
III. Comments on the Proposed Ruleand FDA’s Responses
We received 28 comments on theproposed rule as it was published in1998. We received over 400 commentson the donor-suitability proposed rule;many of these raised issues related tosubparts A and B of part 1271.
A. General Comments
(Comment 1) Many commentsexpressed general approval of the rule.One comment stated that the proposedrule addresses the public health needsfor regulation in this area, helping toassure an adequate supply of safe andfunctional products without imposingunnecessary regulatory burdens orinhibitions to progress. Anothercomment, in support of registration,noted the importance of establishing aknown data base of the industry.Another comment stated that creation ofan official inventory of establishmentssubject to FDA regulation is importantto determine the actual level ofcompliance and to develop reliableestimates of the cost of enforcement.
We acknowledge and appreciate thesesupportive comments. The newregulation on registration and listingwill increase our knowledge andunderstanding of the HCT/P industryand will enable us to monitor industrydevelopments and communicate withindustry members. This final rule will
enhance our compliance efforts inprotecting the public from the spread ofcommunicable diseases, when theremaining tissue regulations becomeeffective.
(Comment 2) Some commentsobjected to the development of acomprehensive regulatory system. Oneof these comments objected that theapproach is based on potential, notactual, concerns, is more applicable tonew products than to such tissues ascorneal tissue offered for transplant, andis unnecessary in light of qualityassurance programs established byprofessional organizations.
We believe that this new regulatoryprogram for HCT/P’s, when it is inplace, will be superior to the confusingpatchwork of requirements that it willreplace. We have created a simpleregistration system with uniformrequirements for all HCT/P’s and a one-page registration and listing form. Theprocedures in subpart B of part 1271will be followed by all HCT/Pestablishments, along with those inproposed subparts C and D of part 1271.Together, they are intended to establisha communicable disease preventionprogram necessary to protect the publichealth.
In developing and issuing theregistration rule, we have recognizedthat, because all HCT/P’s are derivedfrom the human body, they share certaincommon characteristics, among otherthings the ability to transmit infectiousdiseases. Thus, basic requirements suchas registration, communicable diseasescreening and testing, and GTP’s mayreasonably be applied to all HCT/P’s.However, we have also recognized thatwithin the larger group of HCT/P’s,certain products may present a greaterdegree of risk, and that these HCT/P’sshould be subject to additionalpremarket requirements.
With this tiered, risk-based approach,we will be putting in place a set ofbaseline requirements for all HCT/P’s,while recognizing that different HCT/P’smay present different concerns. As thecomment points out, some concernsmay be more applicable to new productsthan to such tissues as corneal tissueoffered for transplant. We haveidentified criteria corresponding to thetypes of reduced risks that certainproducts may present. HCT/P’s that donot meet all of these criteria will beregulated under the act and/or section351 of the PHS Act (subject tosubsequent effective dates). On the otherhand, most HCT/P’s, includingcadaveric corneas, will be regulatedsolely under the communicable diseaseauthority of section 361 of the PHS Act
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00024 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5451Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
and the regulations that will make uppart 1271.
When implemented, the registration,donor-suitability, and GTP regulationsare intended to reduce the risk oftransmission of communicable diseaseby HCT/P’s. The donor-suitabilityproposed rule incorporates and expandsupon many of the requirements forhuman tissue intended fortransplantation in part 1270. The part1270 requirements were put into placeto prevent the transmission of humanimmunodeficiency virus and hepatitisthrough the transplantation of tissuefrom domestic and foreign sources,‘‘Human Tissue Intended forTransplantation,’’ final rule (62 FR40429, July 29, 1997).
Registration and listing are crucialcomponents of a regulatory program toincrease the safety of HCT/P’s. Indeed,the United States General AccountingOffice (GAO) has urged the agency toput a program in place in response tothe potential transmission of infectiousdiseases from cell and tissue donors torecipients, GAO, ‘‘Human Tissue Banks,FDA Taking Steps to Improve Safety,but Some Concerns Remain’’ (December1997).
We recognize the importance ofvoluntary quality assurance programs,and we respect the efforts andaccomplishments of professionalorganizations. We have considered theefforts of professional organizations, andwe will continue to do so as weimplement the new regulations.However, not all HCT/P establishmentsbelong to or are accredited by suchgroups, and voluntary programs are notenforceable.
(Comment 3) Another comment statedthat we should finalize the registrationrule as soon as possible, without waitingfor the other rules.
We agree that there are benefits topublishing the registration final rule inadvance of the other final rules, and weare doing so. However, as discussedearlier in this document, we arestaggering the regulation’s effectivedates. Under this approach, we will beable to promptly begin receivingregistration and listing information forHCT/P’s currently subject to part 1270.
(Comment 4) One comment assertedthat we should identify those tissuesand entities subject to part 1271 that arenot currently subject to part 1270, andinitiate rulemaking to broaden thecoverage of the substantive regulationscodified in part 1270.
Rather than broaden the scope of theregulations in part 1270, we have earliernoted that we intend to replace part1270 with the new regulations in part1271 (donor-suitability proposed rule,
64 FR 52697). Revocation of part 1270will occur at the time the GTP final rulebecomes effective. We have earlier madeclear (64 FR 52697 to 52698) that thenew rules in part 1271, when complete,will be broader in scope than those inpart 1270, will impose additional testingand screening requirements, and willcover more establishments and HCT/P’s(e.g., hematopoietic stem cells,reproductive tissue). Thus, it is notnecessary to initiate rulemaking tobroaden the coverage of the regulationsin part 1270.
(Comment 5) One comment asked theagency to clarify if it intends to requireregistered organizations to pass alongany information the agencydisseminates. Another commentcounseled against depending on asecondary dissemination system, fromthose required to register to those withwhom they interact who are notrequired to register, to get educationalinformation to all of the tissuecommunity.
We are not imposing a specificinformation-dissemination requirementat this time. The only members of thetissue community who would be subjectto the rules in part 1271 and who arenot required to register are thoseindividuals who recover cells or tissueunder contract, agreement, or otherarrangement with a registeredestablishment, but who perform noother manufacturing step (except forsending the cells or tissue to theregistered establishment). Theseindividuals would be subject to theother requirements that will becontained in part 1271, when complete,and the establishments for whom theyperform their services would beresponsible for their work. (Thisexception is discussed in greater detailbelow.) Therefore, we believe that if wedistribute information to registeredestablishments, we will be reaching thewhole of the affected tissue community.
(Comment 6) One comment expressedconcern that the proposed rule failed toidentify the party ultimately responsiblefor the tissue or for the decisionsrequired in the process of determiningdonor and tissue suitability.
We have addressed the question ofresponsibility in the GTP proposed rule.
(Comment 7) Several comments raisedthe issue of dispute resolution,particularly with respect to questionsabout homologous use and minimalmanipulation. One of these commentsurged us to develop and follow aprocess for resolving disputes in aprompt and efficient manner. Onecomment recommended that the TissueReference Group (TRG) serve as theforum for resolving any disagreements
that arise with regard to the applicationof definitions.
We recognize that, as we implementthis new regulation, there will be areasin which additional guidance may bedesirable or interpretations may differ.To help answer questions about how aparticular HCT/P will be regulated, theagency developed the TRG. If anestablishment is not sure how its HCT/P may be regulated, it should contactthe TRG.
The TRG provides a single referencepoint and makes recommendations tothe Center Directors regardingregulation of specific HCT/P’s, e.g.,regulation solely under section 361 ofthe PHS Act or additionally under theact and/or section 351 of PHS Act. TheTRG is composed of: (1) Threerepresentatives from the Center forBiologics Evaluation and Research(CBER), including the productjurisdictional officer; (2) threerepresentatives from the Center forDevices and Radiological Health(CDRH), including the productjurisdictional officer; and (3) a liaisonfrom the agency’s Office of the ChiefMediator and Ombudsman (OCMO), anonvoting member. Other FDA staffattend the TRG meetings as needed todiscuss issues related to products intheir area of expertise. Furtherinformation about the TRG can be foundon CBER’s website at http://www.fda.gov/cber/tissue/trg.htm.
In some cases, a product regulatedunder the act will fall under thejurisdiction of more than one agencycomponent, e.g., a combination deviceand biological product. Where theagency component with primaryjurisdiction is unclear or in dispute, asponsor may request designation fromthe product jurisdiction officer, who isthe FDA Ombudsman, as detailed in 21CFR part 3. In addition, the OCMO canassist in resolving disputes with theagency that may arise from decisionsmade by the Center Directors regardingthe regulation of HCT/P’s, afterconsideration of TRG recommendations,as described above.
In addition, we recognize that furtherpublic discussion of how tissueregulation would be applied to certaincategories of human cells, tissues, andcellular and tissue-based products maybe warranted due to the complexity orsensitivity of the issues. For example,we held a public meeting on August 2,2000, to discuss how proposeddefinitions for ‘‘minimallymanipulated’’ and ‘‘homologous use’’should be applied to human boneallograft products (65 FR 44485, July 18,2000). We intend to provide furtheropportunities for public discussion of
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00025 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5452 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
how the regulatory approach should beapplied to other HCT/P’s. We anticipatethat there may be additional needs fordiscussion through public meetings,public hearings, or guidance as weimplement the new regulations.
(Comment 8) One comment assertedthat we have published no documentdescribing the TRG’s currentcomposition, authoritative status,procedures, whether its decisions are orwill be made public, or how industry isexpected to communicate with thegroup. The comment also suggested thatwe should consider making the TRG’spolicy decisions routinely available tothe public.
We appreciate these comments andare committed to working on the issuesraised. Among other things, the TRG islooking into mechanisms for increasingthe transparency of its functions, whilestill protecting confidential information.Information about the TRG can be foundon CBER’s website at http://www.fda.gov/cber/tissue/trg.htm.
(Comment 9) Several commentsasserted that we are proposing toregulate the practice of medicine,especially with respect to reproductivetissue and hematopoietic stem cells.
We disagree with this comment. Thisfinal rule sets out registration and listingrequirements for establishments thatrecover, process, store, label, package, ordistribute HCT/P’s, or screen or test celland tissue donors. HCT/P’s, includinghematopoietic stem cells andreproductive tissues, fall within ourjurisdiction. Some HCT/P’s will beregulated under the act and/or the PHSAct, while other HCT/P’s will beeffectively regulated solely byregulations issued under our authorityto prevent the spread of communicabledisease. We are not attempting to governpractitioners’ use of HCT/P’s, but ratherto ensure that HCT/P’s that would beused by practitioners in their treatmentof patients are in compliance withapplicable regulations, includingregulations designed to prevent thetransmission or spread of communicabledisease.
(Comment 10) We received severalcomments on our proposed regulation ofhematopoietic stem cells. One commentsupported the proposal that allestablishments involved withhematopoietic stem cell therapy registerwith FDA. Two comments asserted thatthe proposed regulation wouldjeopardize patient treatment, impede thedevelopment of new therapies, andincrease the costs of treatment. Onecomment asserted that we lack the legalauthority to regulate intrastatehematopoietic stem cell transplants.Another comment argued that clinical
research involving the use of blood orbone marrow transplantation fortreatment of human diseases, but notinvolving an investigational drug ordevice, should not require aninvestigational new drug application orinvestigational device exemption. Thiscomment further requested thedevelopment of simplified proceduresfor evaluating those investigationaldevices or cellular biologic productsthat are more than minimallymanipulated. Two comments arguedthat there is no need for FDA regulationas industry standards suffice and FDArequirements would be duplicative.
We believe that it is necessary to bringthe regulation of hematopoietic stemcells in line with the regulation of otherHCT/P’s, and that we possess the legalauthority to take this action. Like otherHCT/P’s, hematopoietic stem cells maytransmit communicable diseases; thus,the basic communicable diseaseprevention requirements that will becontained in part 1271, including theseregistration and listing requirements, areas relevant to these cells as to any otherHCT/P’s. Intrastate activities involvinghematopoietic stem cells, as well asother HCT/P’s, can be regulated toprevent the interstate spread ofcommunicable diseases under section361 of the PHS Act. (See Louisiana v.Mathews, 427 F. Supp. 174, 176 (E.D.La. 1977).) The GAO has cited the lackof regulation of hematopoietic stem cellsas a significant gap in our oversight, andurged us to proceed with implementingnew regulations that would coverhematopoietic stem cells. We are nowclosing that gap.
Although we applaud thedevelopment of industry standardsnoted by the comments received, suchstandards are not followed by all HCT/P establishments. Moreover, voluntarystandards differ significantly fromenforceable regulations. We cannot takeenforcement actions to ensurecompliance with voluntary industrystandards and thus would be limited inour ability to protect the public healthif we relied on such standards alone.Establishments that comply withindustry standards, however, shouldhave little trouble adapting theirpractices to the new requirements.Thus, any additional burden should beminimal.
Rather than require data submissionfrom each hematopoietic stem cellestablishment, we have considered thedevelopment of standards for certainstem cell products. On January 20, 1998(63 FR 2985), we published a notice inthe Federal Register requesting thesubmission of proposed standards andsupporting data relating to certain stem
cell products by January 20, 2000,entitled ‘‘Request for ProposedStandards for Unrelated AllogeneicPeripheral and Placental/UmbilicalCord Blood Hematopoietic Stem/Progenitor Cell Products.’’ Later, weextended the deadline for submittingdata to July 17, 2000 (65 FR 20825,April 18, 2000).
(Comment 11) One commentgenerally agreed with our proposal torequire registration for certainreproductive tissue, but requestedseveral clarifications and exceptions.Several comments questioned the needfor the regulation of reproductive cellsand tissues, citing current oversightfrom professional organizations, otherFederal agencies, and States. Commentsopposed registration for programsinvolved in egg donation, egg retrieval,semen processing, semen evaluation, orin vitro fertilization (IVF) in assistedreproductive technologies. Onecomment asserted that a large number ofmedical practitioners who performinseminations would not be included inthis new regulation, lessening theireffectiveness. Another commentasserted that programs that manufacturetissue culture products for the growth ofoocytes and sperm for sale should berequired to register, but IVF programsmaking culture medium for their ownuses should be exempt.
We stand by our decision to extendregulatory requirements to reproductivecells and tissue. Currently, FDA doesnot have regulations in place to addressthe infectious disease risk of donating,processing, and storing reproductivecells and tissue. Because there has beenno registration or listing requirement,we have not had accurate informationabout the industry. We agree with theGAO that extending regulation toreproductive cells and tissues willremedy a significant gap in oversight.
Although we recognize the value ofprofessional efforts to self-regulate, andof regulatory efforts of other agenciesand the States, we disagree that thesepiecemeal, often voluntary, efforts areadequate. Nor will the new regulationsin part 1271 be duplicative. Stateregulation varies from State to State anddoes not consistently address ourconcerns about the transmission ofcommunicable disease. The modelcertification program for embryolaboratories developed by the Centersfor Disease Control and Prevention(CDC) is a voluntary program that Statesmay or may not choose to adopt; itsprimary focus is not on preventing thetransmission of communicable disease.No State has yet adopted CDC’s modelcertification program. Membership inprofessional societies is voluntary.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00026 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5453Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
Moreover, many establishments do notreport to the Society for AssistedReproductive Technology. The ClinicalLaboratories Improvement Amendmentof 1988 (CLIA) covers clinical laboratorytesting, including certain proceduresperformed in embryo laboratories;however, as discussed later in thisdocument, CLIA certification is notequivalent to the requirements we areputting in place.
We disagree that establishments thatonly deal with egg donation, retrieval,semen processing, or IVF should beexempt from the new regulations. Theseactivities are vital to the handling ofreproductive tissues. Performing theseactivities appropriately in order toprevent cross-contamination and mix-ups requires proper recordkeeping,storage practices, and accountability.Moreover, registration of theseestablishments is consistent with agencypractice in other areas; e.g.,establishments where only blooddonation or processing occurs arerequired to register.
As discussed later in this document,however, this final rule contains a newexception for certain reproductive tissueestablishments that perform only certainlimited activities that raise limitedcommunicable disease concerns. Underthe exception, an establishment thatonly recovers reproductive cells ortissue for immediate transfer into asexually intimate partner of the cell ortissue donor is not required to complywith the requirements that will becontained in part 1271, includingregistration and listing.
With respect to the comment abouttissue culture media, these products arenot considered HCT/P’s. Rather, embryoculture media and other such productsare regulated as medical devices byFDA, and establishments thatmanufacture embryo culture media aresubject to the device regulations.
(Comment 12) Several commentsresponded to our discussion ofregulating dura mater and human heartvalve allografts as 361 HCT/P’s ratherthan as devices, if they meet the criteriain § 1271.10 (63 FR 26744 at 26747).Three comments supported theregulation of heart valves as 361 HCT/P’s. One comment suggested that, toprevent a regulatory ‘‘open window,’’the regulatory change should not takeplace until GTP requirements areeffective or other steps are taken. Onecomment asked whether the transfer ofheart valves would be reflected in acodified regulation. A fourth commentsupported regulating dura mater as a361 HCT/P and strongly suggested that‘‘special controls’’ be included in theGTP requirements. No comments
objected to regulating heart valveallografts and dura mater as 361 HCT/P’s.
We agree that we should avoid an‘‘open window’’ where possible.Therefore, we have staggered effectivedates for this rule to prevent such anoutcome. We do not intend to beginregulating human heart valve allograftsand dura mater that meet the criteria in§ 1271.10 as 361 HCT/P’s until thedonor-suitability and GTP componentsof part 1271 become effective, or otherappropriate steps have been taken. TheGTP proposed rule contains specialrequirements for dura mater intended toaddress the communicable diseaseconcerns about that product. Because§ 1271.10 contains the criteria forregulation of HCT/P’s as 361 HCT/P’s,and we are now reiterating our view thatheart valves meeting those criteria willnot be regulated as devices, we do notintend to issue a separate regulation tochange regulatory authority on thatspecific point.
(Comment 13) One commentsuggested that we consider voluntaryaccreditation and inspection programsin implementing our regulatory strategy.The comment further requested that weaccord ‘‘deemed status’’ to certainaccredited facilities.
We are exploring various options forinspections and compliance actions toenforce the new regulations. Amongother ideas, we are looking into thosesuggested by this comment, includingthe legal issues raised. At present, wehave in place a tiered inspectionapproach to enforce the regulations inpart 1270 that takes into considerationsuch factors as professionalaccreditation. We intend to provide amore detailed discussion of ourregulatory intentions after considerationof comments to the GTP proposed rule.
(Comment 14) One comment notedthat tissue recovery is frequentlyperformed by organ procurementorganizations, and that the requirementswith regard to the prevention ofinfectious disease transmission areappropriately much less stringent fororgan donation than are comparablerequirements for tissues. The commentasserted that exempting theseorganizations from regulation wouldimmeasurably weaken the public healthprotection provided by this regulation.
An organ procurement organizationthat also recovers cells or tissues inaddition to organs is not exempt fromthese regulations, and must register withthe agency and follow all otherregulations applicable to its actions withrespect to HCT/P’s. An organprocurement establishment is notrequired to submit a list of the
vascularized human organs fortransplantation that it recovers, becausethese organs are not covered by thedefinition of HCT/P (see§ 1271.3(d)(2)(i)). However, such anorganization must list with the agencyany HCT/P’s that fall within the scopeof part 1271 that the organizationrecovers or otherwise manufactures.
B. Comments on Subpart A of Part 1271:Definitions
We received comments on many ofthe proposed definitions in § 1271.3(a)through (h). We did not receivecomments on the definitions of‘‘autologous’’ and ‘‘transfer.’’ Weaddress many of these comments below.Comments on the definitions of‘‘homologous use’’ and ‘‘minimalmanipulation’’ are addressed in sectionIII.C of this document.
(Comment 15) The definition ofestablishment in proposed § 1271.3(b)reads as follows:
Establishment means a place of businessunder one management, at one generalphysical location, that engages in themanufacture of human cellular or tissue-based products. The term includes, amongothers, facilities that engage in contractmanufacturing services for a manufacturer ofhuman cellular or tissue-based products. Theterm also includes any individualpartnership, corporation, association, orother legal entity engaged in the manufactureof human cellular or tissue-based products,except that an individual engaged solely inthe procurement or recovery of cells ortissues or under contract to a registeredestablishment is not required toindependently register (emphasis added).
Comments raised issues about theproposed exception in the last sentenceof the definition. Some commentsasserted that individuals ororganizations engaged solely inprocurement under contract should berequired to register. One commentpointed to the critical role in thesuitability assessment of a cell andtissue donor that such organizationsplay. Another comment asserted thatregistration and listing should beapplied to those who screen donors andthat procurement of tissue that is notdone in an aseptic manner places tissuerecipients at risk. One commentexpressed confusion about theexception and suggested that ‘‘or undercontract’’ should read ‘‘and undercontract.’’ This comment furthersuggested that individuals and otherlegal entities engaged solely inprocurement or recovery be required toregister unless contracted for thatactivity to a registered establishment.
Three comments argued for anexpanded exception. One commenturged us to clarify that the ‘‘under
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00027 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5454 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
contract to’’ language can apply to othercontracting individuals, not just tocontractors engaged in procurement orrecovery (e.g., sales representatives whodistribute HCT/P’s). Two othercomments requested clarification thatclinical laboratories who perform testingare excluded from the registration andlisting requirements.
We have rewritten the exception andmoved it to § 1271.15(f). The relevantlanguage now states:
(f) You are not required to register or listyour HCT/P’s independently, but you mustcomply with all other applicablerequirements in this part, if you are anindividual under contract, agreement, orother arrangement with a registeredestablishment and engaged solely inrecovering cells or tissues and sending therecovered cells or tissues to the registeredestablishment.
We believe this new languageaddresses many of the comments’concerns. We have replaced ‘‘or undercontract’’ with ‘‘and under contract,agreement, or other arrangement.’’ Inaddition, because ‘‘procurement’’ and‘‘recovery’’ refer to the same action—theremoval of cells or tissue from a donor—we have decided that it is redundantand possibly confusing to use bothwords. Instead, the exception now usesthe term ‘‘recovery,’’ the same term usedin the definition of ‘‘manufacture’’ in§ 1271.3(e). Therefore, the exceptiononly applies to those individualsengaged solely in recovery of HCT/P’sand who are under contract, agreement,or other arrangement with a registeredestablishment. We believe this is anappropriate way of easing the regulatoryburden on individuals while ensuringthe protection of the public health.
This exception does not extend to anindividual who does more than recovertissue and send it to the contractingestablishment. (Thus, for example, anindividual engaged in any aspect ofdonor screening is not covered by theexception and must register.) Further,an individual who meets the terms ofthe exception would be excepted onlyfrom registration and listingrequirements and would be required tocomply with all other requirements tobe contained in part 1271.
We are not extending the exception to‘‘other legal entities.’’ Only individualsare covered. Examples of suchindividuals not required to registermight include certain medicalexaminers, morticians, or physicianswho recover hematopoietic stem cells ortissues (e.g., corneas, cord blood).Laboratories that perform donor testingare not excluded from registration,listing, or other requirements in part1271.
(Comment 16) We proposed to definefamily-related allogeneic use inproposed § 1271.3(c) as ‘‘theimplantation, transplantation, infusion,or transfer of a human cellular or tissue-based product into a first-degree bloodrelative of the individual from whomcells or tissue comprising such productwere removed.’’ Under § 1271.10(d), asproposed, HCT/P’s with a systemiceffect that are for family-relatedallogeneic use would be regulated undersection 361 of the PHS Act (providedthat the HCT/P meets all other criteriaset out in § 1271.10). This limitedexception from the requirement forinvestigational use exemptions andpremarketing submissions was firstproposed in the proposed approach (62FR 9721). In the registration proposedrule, we specifically requested furthercomments on the issue (63 FR 26744 at26750).
We received approximately 13comments on our proposed definition of‘‘family-related allogeneic use,’’ mostfrom individuals and organizationsinvolved in hematopoietic stem celltransplantation. One comment praisedthe proposed definition as clearer andmore consistent than that used in theproposed approach, but cautioned thatour terminology might create confusion.Other comments argued that we shouldexpand the definition to more distantlyrelated family members. Severalcomments suggested that the terminclude all ancestral relations, siblings,and collateral relations to the fourthdegree by blood, marriage, or adoption.Another comment objected todistinguishing between family-relateddonors and other donors, stating that thesame principles apply in bothsituations. This comment argued thatthe clinical use of unrelated versusrelated allogeneic transplants fallswithin the practice of medicine andshould not be regulated by FDA.
We have decided to change the termfrom ‘‘family-related allogeneic use’’ to‘‘allogeneic use in a first-degree orsecond-degree blood relative.’’ Parents,children, and siblings are consideredfirst-degree relatives. Aunts, uncles,nieces, nephews, first cousins,grandparents, and grandchildren aresecond-degree relatives. Relations byadoption or marriage are not included.Because we are using the phrase ‘‘first-degree or second-degree blood relative’’in its ordinary sense, the final regulationdoes not contain a definition of thisphrase.
Our decision to broaden the scope ofrelated donors to include second-degreeblood relatives, rather than just first-degree, is based upon several factors. Inthe absence of a human leukocyte
antigen (HLA) identical sibling, thesearch for donors in extended familiesis occurring now to a very limiteddegree, but is likely to increase with thecontinuing advances indeoxyribonucleic acid technology. Thelikelihood of finding a donor with ahaplotype identical to that of therecipient is greater among blood-relatedindividuals than among unrelatedindividuals. Indeed, statistical methodshave been proposed to measure thisprobability (Refs. 2 and 3).
In addition, for certain ethnic groups,it is extremely difficult to find anappropriate unrelated donor. Success atfinding a match among the extendedfamily can be equal to or even greaterthan the chance of finding a matchusing a single sibling search, if thehaplotype is a common one within thepatient’s ethnic population, and thefamily members are of the same ethnicorigin.
Registry outcome data for somehematologic malignancies suggest thatperipheral blood and bone marrowtransplant recipients may have a bettersurvival rate when transplanted withhematopoietic stem cells from relateddonors. One possible reason is that arelated donor is likely to share identicalhaplotypes with the patient (thegenotypic level), whereas an unrelateddonor is matched at the phenotypiclevel. Also, family donors may be bettermatched for minor histocompatabilityloci for which testing is not routinelyperformed.
We initially proposed a more limitedexception. Having reviewed thecomments on this issue, we believethere is some scientific merit inexpanding the exception to second-degree blood relatives. This change isconsistent with our goal of keepingregulatory burden to a minimum. Thesame scientific justification does notexist for expanding the exception torelatives by marriage or adoption, and isweaker for blood relatives beyond thesecond degree. In addition, theexception in § 1271.10(a)(4)(ii)(b) forallogeneic use in a first-degree orsecond-degree blood relative does notextend to those situations where theHCT/P is more than minimallymanipulated, is advertised, labeled orotherwise objectively intended by themanufacturer for a nonhomologous use,or is combined with a drug or device(except as described in § 1271.10(a)(3)).
(Comment 17) One of the commentson ‘‘family-related allogeneic use’’asserted that, in the context ofreproductive medicine, the notion ofappropriate use of family-relatedmaterials must include the close bloodrelatives of either partner. This
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00028 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5455Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
comment proposed that those facilitiescollecting or using reproductive tissuesfrom sexually intimate partners or closerelatives should not be required toregister.
Later in this document, we addressthe question of registration forreproductive tissue facilities. Thechange in terminology from ‘‘family-related allogeneic use’’ to ‘‘allogeneicuse in first-degree or second-degreeblood relatives’’ does not affect theregistration of reproductive tissueestablishments.
(Comment 18) Several commentsobjected to the word ‘‘product’’ in theterm human cellular or tissue-basedproduct, defined in proposed§ 1271.3(e). These comments assertedthat human cells and tissues aredonations, not goods manufactured forsale. Some comments argued that theuse of the word ‘‘product’’ might havelegal implications; e.g., subjecting eyebanks to inappropriate product liabilitylitigation. Comments also noted that theword ‘‘product’’ is inconsistent withterms used in the tissue and eye bankingfield. We also received an objection todescribing embryos and germ cells as‘‘products.’’
In choosing ‘‘human cellular or tissue-based product,’’ we were seeking a termthat would describe everything that willbe subject to the regulations in part1271. We needed a term broad enoughto cover both cells and tissues, and onethat would include within its scopesuch diverse articles as unprocessedtissue, highly processed cells, andtissues that are combined with certaindrugs or devices. Although we haveconsidered removing the word‘‘product’’ from the definition, we areconcerned that another term (e.g.,‘‘human cells and tissues’’) would notbe understood to include many of thehighly manufactured products to whichthe regulations apply, or might bemisconstrued to apply only to the cellor tissue component of such a product.Moreover, the term ‘‘product’’ isconsistent with the language of thestatutes under which we operate; forexample, blood (which is also routinelydonated) is a ‘‘biological product’’ undersection 351 of the PHS Act. We do notbelieve that the use of the word‘‘product’’ will affect the manner inwhich state laws apply to HCT/P’s; ourexperience with the regulation of bloodand blood products supports this view.
We recognize, however, thatconceptual difficulties may arise incalling certain cells or tissues‘‘products.’’ Thus, as noted earlier inthis document, we have expanded theterm to ‘‘human cells, tissues, andcellular and tissue-based products,’’
abbreviated as ‘‘HCT/P’s.’’ We havemade appropriate substitutionsthroughout the regulation. Thedefinition itself has not changed, andthe scope of the term remains the same.
Proposed § 1271.3(e) has beenredesignated as § 1271.3(d)(2).
(Comment 19) One comment statedthat the proposed rule leaves vagueperipheral blood lymphocytes that arenot cultured or manipulated, but areused for their immunological effects forthe treatment of disease. According tothe comment, the definition in proposed§ 1271.3(e)(2) (final§ 1271.3(d)(2)(ii))implies that these cells are subject toregulation under 21 CFR part 607. Thecomment recommends that these cellsbe specifically included in this proposaland not be considered mature bloodcells subject to regulation under othersections of title 21 of the CFR.
We believe that the commenter isaddressing donor lymphocytes(leukocytes) for infusion (DLI), whichare the lymphocyte-rich cellularfractions obtained by leukapheresis ofthe peripheral blood of donors of bonemarrow or peripheral bloodhematopoietic stem/progenitor cells.Many DLI products are not furthermanipulated. These minimallymanipulated products are administeredto select patients to elicit a graft-versus-leukemia effect and to treat othertransplant-associated complications.
DLI, regardless of the level ofmanipulation, meet the definition ofHCT/P in this rule. FDA intends toregulate all DLI as HCT/P’s, rather thanas traditional blood products.
(Comment 20) One comment onproposed § 1271.3(e) requestedclarification that an extract would notfall under the definition of humancellular or tissue-based product. Thecomment noted that the words ‘‘any cellor tissue-based component of such aproduct’’ may imply that an extractcould fall within the definition.
We do not consider extracts to beHCT/P’s. When we revised thedefinition of human cellular or tissue-based product in the donor-suitabilityproposed rule (64 FR 52696 at 52719),we deleted the phrase ‘‘or any cell ortissue-based component of such aproduct.’’ Moreover, we listed ‘‘anysecreted or extracted human products’’as an exception to the definition ofHCT/P in proposed § 1271.3(e)(3). Thesechanges are codified in this rule at§ 1271.3(d)(2)(iii).
(Comment 21) One comment onproposed § 1271.3(e)(4) objected to theexclusion of bone marrow from thedefinition of HCT/P, since all threesources of hematopoietic stem cells(cord, peripheral blood, bone marrow)
have the same risk of infectious diseasetransmission.
Minimally manipulated bone marrowfalls under the purview of the HealthResources and Services Administration(section 379 of the PHS Act (42 U.S.C.274(k)). For this reason, we haveexcepted it from the definition of HCT/P’s, and thus from the scope of thisregulation issued under section 361 ofthe PHS Act authority.
The exception for bone marrow infinal § 1271.3(d)(2)(iv) extends only to‘‘minimally manipulated bone marrowfor homologous use and not combinedwith a drug or a device (except for asterilizing, preserving, or storage agent,if the addition of the agent does notraise new clinical safety concerns withrespect to the bone marrow).’’ Bonemarrow would meet the definition of anHCT/P if it is: More than minimallymanipulated; advertised, labeled, orotherwise objectively intended by themanufacturer for a nonhomologous use,or combined with certain drugs ordevices.
(Comment 22) In the proposed rule,we stated in proposed § 1271.3(f) that‘‘manufacture means, but is not limitedto, any or all steps in the recovery,screening, testing, processing, storage,labeling, packaging, or distribution ofany human cellular or tissue-basedproduct’’ (63 FR 26744 at 26754).Approximately 10 comments objectedthat the term ‘‘manufacture’’ isinappropriate. Some comments assertedthat fertility clinics are not‘‘manufacturers’’ of human tissue.Comments from the eye banks assertedthat it is inaccurate to use the word‘‘manufacture’’ with respect to cornealtissue; along with ‘‘product,’’ the termcould raise legal issues (e.g., subjectingeye banks to inappropriate productliability litigation). Another commentasserted that tissue banks do notmanufacture tissue, but rather processit.
We have considered substituting adifferent term for ‘‘manufacture,’’ buthave been unable to find a satisfactoryreplacement. Most of the terms that weconsidered (e.g., produce, handle) weretoo limited in scope. Moreover,comments that objected to the term didnot suggest alternatives. For thesereasons, we continue to use the word‘‘manufacture’’ as an umbrella term tocapture the many different actions thatHCT/P establishments might take inpreparing HCT/P’s for use. These stepsmay include, but are not limited to,recovery, screening, testing, processing,storage, labeling, packaging, anddistribution. No comments disagreedwith or objected to any of the actionslisted in the definition of manufacture.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00029 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5456 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
Rather than list each of these activitiesrepeatedly throughout this preambleand the regulation, we have decided tomaintain the term ‘‘manufacture,’’ asdefined in this rule (proposed§ 1271.3(f) is codified at § 1271.3(e)).
(Comment 23) One comment onmanufacture questioned the rationalefor requiring testing establishments toregister. Three comments asserted thattesting laboratories should not berequired to register because CLIAcertification is sufficient. One commentasked if labs that test for other diseasesor that perform bacterial cultures needto register.
The definition of ‘‘manufacture’’ isintended to cover all steps in theprocess of handling HCT/P’s. Testingdonors for communicable diseases is acritical step in this process and for thatreason is included the definition ofmanufacture. The registrationrequirement for testing laboratoriesenables us to have a list of all partiesinvolved in manufacturing activities.
Having a list of testing laboratoriesenables us to inspect laboratories toensure that testing is performed in acorrect manner according to test kitinstructions. The CLIA certificationreferred to in the comments isimportant, and in fact we are requiringCLIA certification. However, becausethere are differences betweeninspections under CLIA and inspectionscarried out by FDA, CLIA certificationalone is not adequate for our purposes.CLIA requirements address only alimited spectrum of laboratory testingand personnel requirements and do notfocus on donor testing. Moreover, ourexperience with inspecting testinglaboratories indicates that significantviolations have been found. To excludetesting laboratories from the scope ofthis regulation would not be consistentwith our goal of preventing thetransmission of communicable diseases.
The registration requirement fortesting laboratories extends to thoselaboratories that test donor specimensfor communicable disease. Onlylaboratories that test for relevantcommunicable diseases as defined inthe proposed donor-suitability rule arerequired to register. We have clarifiedthe definition of ‘‘manufacture’’ to referto ‘‘screening or testing of the cell ortissue donor’’ rather than to screening ortesting of the cell or tissue. In thesituation where communicable diseasetesting to determine donor suitabilitymight be appropriately performed onthe cells or tissues, rather than on thedonor (as might be the situation withcord blood), such testing would beincluded within the meaning of donortesting.
(Comment 24) One comment notedthat entities engaged only in labelingand packaging are not explicitly withinthe scope of part 1270, but are coveredby this new rule.
Part 1271 covers more activities thanpart 1270.
(Comment 25) In the preamble to theproposed rule, we noted thatdistribution ‘‘includes any conveyanceor shipment of human cellular or tissue-based product (including importationand exportation), whether or not suchconveyance or shipment is entirelyintrastate and whether or not possessionof the human cellular or tissue-basedproduct is taken’’ (63 FR 26750). Wehave proposed a codified definition of‘‘distribution’’ in the GTP proposedrule.
For purposes of the regulations in part1271 only, we have proposed in the GTPrule to define ‘‘distribute’’ to mean theconveyance or shipment of an HCT/P. Inother contexts, FDA has defined‘‘distribution’’ more broadly. Under theact, FDA has interpreted the term‘‘distribute’’ to include the delivery,transfer, and dispensing of products.Moreover, the ordinary, dictionarymeaning of the term ‘‘distribute’’includes acts such as delivering,dispensing, supplying, and giving out.In this rule, we do not intend the termto include the dispensing or the transferof an HCT/P to or in a patient.
Two comments on the registrationproposed rule disagreed with the phrase‘‘whether or not possession is taken.’’They asserted that merely taking ordersfor a product should not be includedwithin the meaning of ‘‘distribution,’’and thus should be excluded from‘‘manufacture.’’ One of these commentsdescribed its ‘‘service and distribution’’agreement with a tissue processor,noting that although it does not ship ortake possession of the product, its nameappears on the product label along withthat of the processor. A third commentrecommended that the term‘‘distributes’’ be clarified to exclude‘‘distributors’’; i.e., organizations thatreceive processed/manufacturedallografts and ship them to hospitals.Another comment noted that hospitalsand other establishments sometimesprovide tissue to other institutions inemergencies or in cases of special need.The comment requested that theselimited activities not be considereddistribution.
We agree that an entity that does nottake possession of HCT/P’s is notdistributing them for the purposes ofthis rule. However, we disagree thatdistributors should be excluded fromthe terms of the definition of‘‘distribution.’’ We agree that the
occasional provision of HCT/P’s to otherinstitutions on an emergency basis doesnot fall within the meaning of‘‘distribution.’’
We will consider any additionalcomments on the definition of‘‘distribution’’ when finalizing the otherproposed rules that will make up part1271.
C. Comments on Subpart A: Proposed§§ 1271.10 and 1271.15 (Final§§ 1271.10 and 1271.20)
In proposed § 1271.10, we set out thecriteria for regulating certain HCT/P’ssolely under section 361 of the PHS Actand the regulations to be contained inpart 1271. An HCT/P would be subjectto this level of regulation if it: (1) Wasminimally manipulated; (2) was notpromoted or labeled for any use otherthan a homologous use; (3) was notcombined with or modified by theaddition of any component that is adrug or a device; and (4) either does nothave a systemic effect, or has a systemiceffect and is for autologous, family-related allogeneic, or reproductive use(64 FR 52720).
Proposed § 1271.15 was intended todescribe the HCT/P’s that did not meetthe criteria set out in § 1271.10 and forwhich we therefore did not considerregulation solely under section 361 ofthe PHS Act to be justified (64 FR52699). The section set out the ‘‘mirrorimages’’ of the criteria in § 1271.10 toassist readers in understanding whichHCT/P’s would not be regulated solelyunder part 1271. However, rather thanproviding clarification, the proposedsection could have been interpreted tocreate an additional hurdle forregulation of certain HCT/P’s as drugs,devices, and/or biological products.
Our ability to regulate an HCT/P as adrug, device, and/or biological productderives from the act and section 351 ofthe PHS Act, authorities that are distinctfrom our authority to issue regulationsto prevent the transmission ofcommunicable disease under section361 of the PHS Act. If an HCT/P doesnot meet the criteria in § 1271.10 forregulation solely under section 361 ofthe PHS Act, and the establishment doesnot qualify for any of the exceptions infinal § 1271.15, the HCT/P will beregulated under the act and/or the PHSAct and applicable regulations. As partof this rulemaking process, we areamending certain drug and deviceregulations (e.g., §§ 207.20, 807.20) torequire compliance with certainsubparts of part 1271.
Therefore, we have modifiedproposed § 1271.15 and renumbered it§ 1271.20. That section now refers to‘‘an HCT/P that does not meet the
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00030 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5457Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
criteria set out in § 1271.10(a),’’ ratherthan setting out the mirror images ofthose criteria. As before, the sectioncontains cross-references to those drugand device regulations (e.g., §§ 207.20and 807.20) that will directestablishments to follow the proceduresset out in subparts B, C, and D of part1271. The section now also clarifies thatthe referenced drug and deviceregulations apply if the establishmentdoes not qualify for any of theexceptions in § 1271.15.
We address below the commentsreceived on proposed § 1271.10 and onthe proposed definitions of‘‘homologous use’’ and ‘‘minimalmanipulation.’’
(Comment 26) One commentrequested that we schedule a publicmeeting to discuss the appropriateness,legality, and practicality of using thecriteria in § 1271.10 to reachjurisdictional determinations.
We value public input on the criteriain § 1271.10. In February 1997 we madeavailable the proposed approach, whichamong other things described the factorsthat we would consider in choosing toregulate certain HCT/P’s solely underthe authority of section 361 of the PHSAct rather than as drugs, devices, and/or biological products. On March 17,1997, we held a public meeting to solicitinformation and views on the proposedapproach from the interested public,and we opened a docket for thesubmission of comments (Docket No.97N–0068).
We have published three proposedrules in the Federal Register. Two ofthose rules specifically solicitedcomments on the criteria for regulatingcertain HCT/P’s solely under section361 of the PHS Act. On August 2, 2000,we held an open public meeting tosolicit information on current practicesrelated to the manipulation andhomologous use of human bone allograftin the spine and other orthopedicreconstruction and repair. Many of thecomments presented at the meetingindicated that there weremisunderstandings about how thecriteria set out in § 1271.10 would beapplied, and about the meaning of theterms ‘‘minimal manipulation’’ and‘‘homologous use.’’ This final rulecontains clarifications and additionalexamples that we believe will clear upmuch of the confusion expressed at themeeting. We will consider issuing aguidance document if establishmentsneed additional help in understandingthe terms.
We intend to schedule additionalpublic meetings as necessary. Forexample, FDA believes that additionalpublic discussion of how the criteria in
§ 1271.10 would apply to reproductivetissues would be helpful, and furtherdevelopment of policy in this area maybe warranted.
(Comment 27) We received numerouscomments on the definition of minimalmanipulation. The proposed definitionreads as follows:
Minimal manipulation means:(1) For structural tissue, processing that
does not alter the original relevantcharacteristics of the tissue relating to thetissue’s utility for reconstruction, repair, orreplacement; and
(2) For cells and nonstructural tissues,processing that does not alter the relevantbiological characteristics of cells or tissues.
One comment urged us to state in thepreamble of the final rule thoseactivities that FDA presently considersto be minimal manipulation. Twocomments recommended that thefollowing procedures be consideredminimal manipulation: Selectiveremoval of B-cells, T-cells, or malignantcells; blood or platelet depletion;centrifugation; density gradientseparation; and cryopreservation. Twocomments supported the use of clinicaland scientific data to determine whethera tissue-processing method isappropriately considered to be minimalmanipulation or more than minimalmanipulation.
Eight comments asserted that‘‘minimal manipulation’’ is vague andopen to subjective interpretation, andshould be eliminated. Two commentsasserted that it is difficult to draw ameaningful distinction between tissuesthat are minimally manipulated andthose that are more than minimallymanipulated. One of these commentssuggested that instead of the minimalmanipulation criterion, FDA shouldpropose that tissue products labeled orpromoted for tissue replacement,reconstruction, or restoration offunction be regulated as tissue. Anothercomment requested the development ofguidance and noted that, in light offuture technological advances, a broaderdefinition of minimal manipulation maybe more appropriate. One commentrecommended that the TRG serve as theliaison for communicating withmanufacturers concerning FDA’sintended application of the definition ofminimal manipulation to particulartissues.
We received many comments on theregulation of bone allografts,INCLUDING bone dowels, submitted inresponse to the donor-suitabilityproposed rule. (The agency hadpreviously considered regulating certainbone dowels as medical devices.) Manyof these comments addressed theconcept of minimal manipulation.
Several comments supported regulatingmachined bone allografts as medicaldevices in order to evaluate their safetyand efficacy and protect the publichealth. However, most commentsopposed such regulation, pointing to thelong history of safe use of boneallografts and citing concerns aboutdecreased supply, among other issues.
Comments did not suggest changes tothe definition of minimal manipulation,and we have not changed theregulation’s wording. We disagree thatthe term should be eliminated, however,as it serves as a valid indicator of thoseHCT/P’s that present fewer risks andthat are most appropriately regulatedsolely under section 361 of the PHS Actand part 1271 (so long as other criteriaare also met).
We agree that the TRG will continueto play a role in providingrecommendations for certain decisionsmade by the Center director interpretingthe term ‘‘minimal manipulation.’’ Atthis time, examples of HCT/P’s that weconsider to be minimally manipulatedinclude those that have been subjectedto the following procedures: Densitygradient separation; selective removal ofB-cells, T-cells, malignant cells, redblood cells, or platelets; centrifugation;cutting, grinding, or shaping; soaking inantibiotic solution; sterilization byethylene oxide treatment or irradiation;cell separation; lyophilization;cryopreservation; or freezing. We do notagree that the expansion ofmesenchymal cells in culture or the useof growth factors to expand umbilicalcord blood stem cells are minimalmanipulation.
Most of the comments we received onthe regulation of bone allografts andbone dowels assumed that we plannedto regulate all bone allografts as medicaldevices. This is a misunderstanding. Weare not considering regulating all boneallografts as medical devices. Like allother HCT/P’s, the regulation of boneallografts depends on the four factors setout in § 1271.10. If the allograft isminimally manipulated, is notadvertised, labeled, or otherwiseobjectively intended by themanufacturer for a nonhomologous use,and is not combined with a drug ordevice (except as described in§ 1271.10(a)(3)), then it will be regulatedas a 361 HCT/P and subject only to theregulations in part 1271. (Bone allograftsdo not have a systemic effect, so thefourth factor is not at issue.) Weconsider cutting, shaping and grindingof bone minimal manipulation.Threading and other machiningprocedures that are performed to createbone dowels, screws, and pins are alsoconsidered minimal manipulation.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00031 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5458 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
(Comment 28) We received manycomments on the term homologous use,which we defined in proposed§ 1271.3(d) as follows:
Homologous use means the use of acellular or tissue-based product forreplacement or supplementation and:
(1) For structural tissue-based products,occurs when the tissue is used for the samebasic function that it fulfills in its nativestate, in a location where such structuralfunction normally occurs; or
(2) For cellular and nonstructural tissue-based products, occurs when the cells ortissue is used to perform the function(s) thatthey perform in the donor.
One comment praised the definitionas reasonable, but urged us to developa process for resolving differences ofopinion between FDA and tissuemanufacturers. Another commentsupported our preamble statement thatthe ‘‘[b]asic function of a structuraltissue is what the tissue does from abiological/physiological point of view,or is capable of doing when in its nativestate’’ (63 FR 26744 at 26749). As anexample, this comment pointed tosurgical use of fascia lata or pericardiumallografts to replace or repair damageddura mater or to construct a bladdersupport sling from a fascia lata allograftto prevent incontinence. Anothercomment questioned whether thehomologous/nonhomologous criterion isa meaningful indicator of the need forpremarket review; this comment citedfascia lata as an example of a tissue thathas been used safely and effectively foryears in ways that may be considerednonhomologous. One comment inresponse to our statement (63 FR 26744at 26749) that the use of hematopoieticstem cells for treatment of adrenalleukodystrophy is an example ofnonhomologous use stated that logicalapplication of hematopoietic stem cellsfor their known hematologic,immunologic or metabolic effects astreatment of human disease should beconsidered within the practice ofmedicine and not subject to regulationby FDA.
Approximately 10 comments arguedthat the term ‘‘homologous use’’ shouldbe eliminated. Many of these commentsasserted that the term is vague and opento subjective interpretation. Onecomment stated that the phrase ‘‘fulfillsin its native state’’ implies that tissuemust be used in the identical place andfor identical purposes, which ignoresthe realistic use of most tissue products.Many comments questioned theapplication of the term ‘‘homologoususe’’ to bone allografts. One assertedthat it is unusual for allograft tissues tobe used in a homologous location,especially with regard to the spine.
Below, in comment 29, we discussour decision to look not at the actual useof an HCT/P, but at the manufactuer’sobjective intent for a nonhomologoususe. Under this approach, a practitionercould use an HCT/P, such ashematopoietic stem cells or fascia lata,for a nonhomologous use in thetreatment of the physician’s patients.Thus, we would not look at the surgicaluse of HCT/P’s such as fascia lata orpericardium allografts, but instead atwhether they were advertised, labeled,or otherwise objectively intended by themanufacturer for a nonhomologous use.In the absence of advertising, labeling,or other indications of themanufacturer’s intent for such use, wewould not require premarketsubmissions. Should such review berequired for a product that has beenused safely and effectively for years innonhomologous ways, and that isintended for a nonhomologous use, wewould expect that data would alreadyexist to facilitate the review process.
We disagree that the term‘‘homologous use’’ should be eliminatedas a criterion for regulation of humancells or tissues under section 361 of thePHS Act. Regulation solely undersection 361 and part 1271 is notwarranted unless it is clearlydemonstrated that the use of an HCT/Pin the recipient is homologous to thefunction the HCT/P would carry out inthe donor. We continue to considernonhomologous use to be a meaningfulindicator that regulation solely undersection 361 of the PHS Act is notsufficient. For example, promotion of anHCT/P for an unproven therapeutic use,such as curing cancer, would clearlymake it inappropriate to regulate theHCT/P solely under section 361 of thePHS Act and the regulations that will bein part 1271.
We have, however, rewritten thedefinition of homologous use inresponse to the comments’ concerns.The new definition (codified at§ 1271.3(c)) reads: ‘‘Homologous usemeans the replacement orsupplementation of a recipient’s cells ortissues with an HCT/P that performs thesame basic function or functions in therecipient as in the donor.’’ Therewording eliminates the distinctionbetween, on the one hand, structuraltissues and, on the other, nonstructuraltissues and cells. The new wording doesnot include the statement that, forstructural tissues, homologous useoccurs ‘‘in a location where suchstructural function normally occurs.’’This language was understood, contraryto our intention, to limit the use ofstructural tissue to the same locationfrom which is was derived. However, a
use of a structural tissue may behomologous even when it does notoccur in the same location as it occurredin the donor. For example, the use ofbone for repair, replacement, orreconstruction anywhere in the skeletonof the recipient (including the vertebralcolumn) would be consideredhomologous use. However, it should beunderstood that, for the use of astructural tissue to be consideredhomologous, the HCT/P must performthe same basic function or functions inthe recipient as it did in the donor; theuse of structural tissue in a locationwhere it does not perform the samebasic function as it did in the donorwould not be homologous.
We intend to interpret‘‘nonhomologous’’ narrowly. Examplesof uses that would be considerednonhomologous include: The use ofdermis as a replacement for dura mater,the use of amniotic membrane in theeye, and the use of cartilage in thebladder. As noted above, an HCT/P thatis intended by the manufacturer for oneof these uses would not be regulatedsolely under section 361 of the PHS Actand these regulations, but as a drug,device, and/or biological product.
(Comment 29) We receivedapproximately six comments agreeingwith our focus in proposed § 1271.10(b)on the promotion or labeling of HCT/P’sfor nonhomologous uses, rather than ontheir actual use. One of these commentsnoted that the use of a product shouldbe determined not by the practice ofsurgeons but by the promotion, labeling,and objective intent of themanufacturer. Another noted that themanner in which we intend todetermine homologous use is consistentwith the way we determine the intendeduse of other products under ourjurisdiction. Two comments interpretedproposed § 1271.10(b) as relievingclinicians from restrictions on use oftissue, and one of these commentsasserted that the exception should beextended to certain clinical transplantprograms.
Another supportive commentquestioned how we will regulate thelabeling of 361 HCT/P’s. Among otherthings, the comment asked whether wewill require 361 HCT/P’s to be labeledfor their homologous use. The commentalso queried whether cutting, shaping,or processing a product in a manner thatmakes it amenable to nonhomologoususe would be considered promotion, inthe absence of labeling or advertising.
We appreciate the comments on thisissue, and we have decided to maintainthe regulation’s focus on the objectiveintent of the HCT/P’s manufacturer fora nonhomologous use, rather than on
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00032 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5459Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
the intent of the practitioner who usesthe HCT/P. We believe this approachwill lead to more efficient use of ourresources. The focus on labeling,advertising, and other indications of themanufacturer’s objective intent does notrelieve clinicians from all restrictions onthe use of HCT/P’s. However, it doesmean that clinical use of an HCT/P ina nonhomologous manner, whether byan individual practitioner or atransplant program, can be consistentwith regulation of the HCT/P solelyunder section 361 of the PHS Act andthe regulations to be contained in part1271. In order to clarify this provison,we are revising proposed § 1271.10(b) toread, in new § 1271.10(a)(2), as follows:‘‘The HCT/P is intended for homologoususe only, as reflected by the labeling,advertising, or other indications of themanufacturer’s objective intent.
By labeling, we refer to the HCT/Plabel and any written, printed, orgraphic materials that supplement,explain, or are textually related to theproduct, and which are disseminated byor on behalf of its manufacturer. We willaddress specific labeling requirementsafter reviewing comments to the GTPproposed rule.
In order to be more consistent withterminology used by the rest of theagency, we have replaced the word‘‘promoted’’ with ‘‘advertised.’’ Theterms ‘‘advertised,’’ ‘‘advertisement,’’and ‘‘advertising’’ include information,other than labeling, that originates fromthe same source as the product and thatis intended to supplement, explain, orbe textually related to the product (e.g.,print advertising, broadcast advertising,electronic advertising (including theInternet), statements of companyrepresentatives).
(Comment 30) As originally proposed,§ 1271.10(c) contained the followingcriterion for regulation of an HCT/Psolely under section 361 of the PHS Act:‘‘Not combined with or modified by theaddition of any nontissue or noncellularcomponent that is a drug or a device.’’We modified that wording in the donor-suitability proposed rule by deleting thephrase ‘‘nontissue or noncellular.’’
Two comments questioned themeaning of § 1271.10(c) and requestedadditional explanation. For example,the comments asked whether we wouldregard a component as being a drug ordevice based on its actual function inthe product, or based on how thecomponent is already regulated. Thecomments also questioned whether allproducts containing a ‘‘nontissue ornoncellular component that is a drug ordevice’’ would automatically be subjectto regulation and premarket review asdrugs or devices, and expressed concern
that application of the criterion mightresult in unnecessary regulation of HCT/P’s as drugs or devices. Anothercomment asserted that we should notregulate a product containing a drug ordevice component unless it could affectrecipient safety, and that themanufacturer should make the initialdetermination of whether this thresholdhas been crossed. One comment statedthat hematopoietic stem cellcomponents are routinely processedusing centrifuges and other laboratoryequipment, combined withdimethylsulfoxide (DMSO) and otherreagents for cryopreservation, andseparated using devices approved forthe processing of hematopoietic stemcells components, and that we havepreviously classified these steps asminimal manipulation. The commentexpressed concern that these stepsmight be considered to combine thecells with a drug or device component.
In response to the concerns expressedby these comments, we have rewrittenthe proposed language. Proposed§ 1271.10(c) has been renumbered as§ 1271.10(a)(3), and now reads: ‘‘Themanufacture of the HCT/P does notinvolve the combination of the cell ortissue component with a drug or adevice, except for a sterilizing,preserving, or storage agent, if theaddition of the agent does not raise newclinical safety concerns with respect tothe HCT/P.’’
The addition of a drug or a device tothe cell or tissue component of an HCT/P may ordinarily be expected to add atherapeutic effect and may also raisesafety concerns. For these reasons, theaddition of a drug or a device to a cellor tissue makes it no longer appropriateto regulate the HCT/P solely undersection 361 of the PHS Act. (As used,the terms drug and device are defined insection 201(g) of the act (21 U.S.C.321(g)).
However, we recognize that the use ofcertain sterilizing, preserving, andstorage agents do not raise the sameconcerns. For this reason, we haveexcepted sterilizing, preserving, andstorage agents, but only if the additionof the agent does not raise new clinicalsafety concerns with respect to the HCT/P. Examples of substances that wouldgenerally be acceptable include: (1)Cryoprotectants (e.g., DMSO); (2)chemicals used for sterilization (e.g.,ethylene oxide); and (3) storagesolutions. We encourage thedevelopment of industry standards thatdescribe the safe use of sterilization,preserving, and storage agents.
Some drugs or devices that have astheir principal purpose sterilizing,preserving, or storage may also have a
therapeutic effect or may be claimed tohave such an effect. The addition ofsuch drugs or devices would not fallwithin the exception for sterilizing,preserving, and storage agents. We agreethat the establishment thatmanufactures the HCT/P should makethe initial determination of whether theaddition of a drug or device that is asterilizing, preserving, or storage agentto an HCT/P raises new clinical safetyconcerns.
(Comment 31) We received onecomment in response to our request forcomments on whether the term‘‘systemic effect’’ adequatelycharacterizes those HCT/P’s that shouldbe regulated under section 351 of thePHS Act, such as neural-derived tissuesand cells used to replace or supplementneurons in the brain (donor suitabilityproposed rule, 64 FR 52699). Thiscomment expressed concern that theintent of the proposed change is vagueand that currently there is little or noevidence that supports such cells ortissues having any systemic effect whenimplanted in the brain.
After further consideration, we agreethat the term ‘‘systemic effect’’ may notcover all of the HCT/P’s that weintended to cover. Because the effect ofimplanted neurons or neural tissue intothe brain would likely be restricted tothe site where the tissue/cells wereplaced, this effect might not be includedwithin the meaning of systemic.However, as discussed in the proposedapproach, HCT/P’s that rely on livingcells for their primary function, such asneuronal tissue, raise clinical safety andeffectiveness concerns that are notappropriately addressed solely undersection 361 of the PHS Act. Suchconcerns include viability, efficacy,malignant transformation, or rejectionafter transplantation. Thus, althoughneuronal cells may not be considered tohave a systemic effect, they nonethelessrequire regulation under the act and/orsection 351 of the PHS Act.
Therefore, we have clarified§ 1271.10(a)(4) to indicate that an HCT/P that either has systemic effect ordepends upon the metabolic activity ofliving cells for its primary functionwould not be appropriately regulatedsolely under section 361 of the PHS Act,and therefore will be regulated as adrug, device, and/or biological product.Cells or tissues such as pancreatic isletcells, which have effects on manydifferent organs throughout the bodythrough the secretion of insulin, areappropriately characterized by the term‘‘systemic effect.’’ Neurons forimplantation in the brain would fall intothe category of HCT/P’s that dependupon the metabolic activity of living
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00033 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5460 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
cells for their primary function. Incontrast, some HCT/P’s (such ascorneas, skin, or osteochondralallografts) may contain living cells, butdo not depend on them for their primaryfunction, which is structural.
(Comment 32) Two comments onproposed § 1271.10 suggested thatisolated human hepatocytes intendedfor transplantation be considered tomeet the criteria in § 1271.10 andtherefore be regulated as 361 HCT/P’s.
We do not consider humanhepatocytes, isolated in tissue culturemedium, infused into the spleen, andintended for temporary treatment ofliver failure to be suitable for regulationsolely under section 361 of the PHS Act.Human hepatocytes have a systemiceffect. Therefore, regardless of the levelof manipulation of the hepatocytes,these cells would be regulated under theact and section 351 of the PHS Act.
D. Comments on Subpart A: Proposed§ 1271.20 (Final § 1271.15)
Proposed § 1271.20, as modified inthe donor-suitability proposed rule, setout four specific exceptions from therequirements of part 1271. We addresscomments on these proposed exceptionsbelow. In this final rule, we haverenumbered proposed § 1271.20 as§ 1271.15.
(Comment 33) We received onecomment on the proposed exception in§ 1271.20(b) for establishments thatremove human cells or tissues from anindividual and implant such cells ortissues into the same individual duringthe same surgical procedure. Thecomment assumed that hospitalsretaining autologous tissue, not used ina scheduled surgical procedure, to beused in a subsequent application on thesame patient, are exempt fromregistration and listing because the twoapplications are essentially a singlecontinuous procedure.
We agree that, so long as the hospitaldoes not engage in any other activityencompassed with in the definition of‘‘manufacture,’’ the hospital would notbe required to register or comply withthe other provisions to be codified inpart 1271. For example, if the hospitalexpanded the cells or tissues, it wouldnot meet the terms of the exception. Inreaching this conclusion, we note thathospitals that store autologous cells ortissues for subsequent application in thesame patient must follow the guidelinesof the Joint Commission onAccreditation of HealthcareOrganizations (JCAHO) for tissuestorage, monitoring of storage devices,and tracking in order to obtain ormaintain accreditation.
(Comment 34) We received commentsquestioning the proposed exception in§ 1271.20(d) for establishments that‘‘receive or store human cellular ortissue-based products solely for pendingscheduled implantation,transplantation, infusion, or transferwithin the same facility.’’Approximately eight comments assertedthat hospitals and other surgicalfacilities keep tissue allografts on handfor future use and suggested that thephrase ‘‘pending scheduled’’ be deletedfrom the exception. One commentprojected that institutions woulddiscontinue stocking tissue in order toavoid the registration requirement,leading to the denial to patients ofappropriate implants. Another commentnoted that thousands of hospitals andphysician’s offices store cells and tissue,and argued that registration could causean unnecessary burden for facilities andFDA. One comment asserted thathospitals must follow the JCAHOguidelines for storage of tissues,monitoring of storage devices, andtracking of tissue use to provide for thesafe storage of tissue. Another commentquestioned whether physicians whoreceive sperm from a sperm bank andexamine it for viability would becovered by the exception.
In response to many of thesecomments, we have deleted the phrase‘‘pending scheduled.’’ The exception,codified at § 1271.15(d), now reads:
You are not required to comply with therequirements of this part if you are anestablishment that does not recover, screen,test, process, label, package, or distribute, butonly receives or stores human cells or tissuesolely for implantation, transplantation,infusion, or transfer within your facility.
As we noted in the preamble to theregistration proposed rule (63 FR 26744at 26748), this exception is intendedonly for end-user establishments; that is,establishments that do not recover,distribute, or otherwise manufacturehuman cells or tissue. Examples of suchestablishments might include somehospitals, dental offices, and physicians’offices. Physicians who do not recoversperm from donors but only receivesperm from a sperm bank would fallwithin the exception; examining thereceived sperm sample for viabilitywould not be considered screening.
We believe that expanding thisexception will ease the regulatoryburden without posing public healthconcerns. To date, we have not becomeaware of problems with the types offacilities that will fall under theexception. However, should thatsituation change—e.g., should weencounter problems with trackingsystems or learn of storage problems—
we will consider narrowing theexception through rulemaking to bringthese establishments within the scope ofthe regulation.
(Comment 35) One comment arguedthat registration should not be requiredfor facilities collecting or usingreproductive tissues from sexuallyintimate partners or close relatives. Thecomment strongly urged us to expandproposed § 1271.20(d) to includeestablishments that collect reproductivematerials for use between sexuallyintimate partners or close relatives.
We agree with this comment, in part,and have added new paragraph (e) tothe exceptions in § 1271.15. Thisexception is limited to establishmentsthat recover reproductive materials forimmediate use between sexuallyintimate partners. (By ‘‘immediate use,’’we mean that the reproductive materialsare used promptly enough thatcryopreservation is not necessary and isnot performed.) The exception isintended to cover an establishment thatrecovers semen for use in the artificialinsemination of the donor’s sexuallyintimate partner. We believe that thissituation raises few new infectiousdisease concerns. For this reason, we areexcepting these establishments fromregistering and from the otherrequirements that will be contained inpart 1271. The exception does notextend to the recovery of cells or tissuesfrom close relatives who are notsexually intimate partners, since anincreased risk of communicable diseasetransmission exists in this situation.
E. Comments on Subpart B of Part 1271:Procedures for Registration and Listing
Many comments expressed generalagreement with the proposedregistration and listing procedures. Onecomment stated that the rule set forth areasonable structure of requirements tobe applied uniformly.
(Comment 36) One commentexpressed concern that we mightimpose a registration fee.
We stated in the preamble to theregistration proposed rule that we wereevaluating our authority to assess a feeand the impacts of such a fee (63 FR26744 at 26751). At this time, we haveno plans to impose a registration fee.
(Comment 37) Comments opposed theproposed requirement in § 1271.21 fortwice yearly reporting as excessive andsupported annual listing updatesinstead. One comment noted that it isunlikely that the components processedby individual laboratories will changegreatly over a 12-month period.
We disagree that the requirement forupdating HCT/P lists is excessive.Establishments are required to update
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00034 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5461Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
their listings with information onchanges that have occurred since thepreviously submitted list. Thesechanges include the introduction of newHCT/P’s, the discontinuation of HCT/P’s, the reintroduction of previouslydiscontinued HCT/P’s, and materialchanges in information previouslysubmitted. However, if no such changehas occurred since the previouslysubmitted list, the establishment is notrequired to submit an update.
Those establishments that mustupdate their lists will likely find thetask relatively simple. As discussed insection III.G of this document, FormFDA 3356 was designed with ease ofcompletion in mind. Yet theinformation to be submitted on thoseupdates is crucial if we are to keepabreast of developments in the cell andtissue industry. Without currentinformation, we will be restricted in ourability to understand the industry andachieve our public health goals.
In setting up a unified registrationsystem for all HCT/P’s, we incorporatedcertain components from currentregistration and listing regulations fordrugs and devices, such as the updaterequirements. By doing so, we made itpossible for establishments thatmanufacture HCT/P’s regulated asdevices, drugs, and/or biological drugsto register and list their products withthe agency using the same form asmanufacturers of 361 HCT/P’s. Thus,the requirement for updating is similarto the requirements in §§ 207.30 and807.30 and is consistent with therequirements of section 510(j)(2) of theact.
We have rewritten the requirement forupdates for greater clarity. Section1271.21(c) now contains timeframes forupdating. Section 1271.25(c) lists thechanges that must be reported. Thelisted events to be reported have beencorrected to reflect the type ofinformation required to be included inthe initial listing. Thus, for example,just as a listing includes the names ofHCT/P’s that an establishment recovers,processes, stores, labels, packages,distributes, or for which it performsdonor screening or testing, so theupdated listing would reflect anychanges in the HCT/P’s for which anyof these activities are performed.
We have made an additional changeto proposed § 1271.25(c), which wouldhave required that copies of all contractservice agreements be available at thetime of inspection of the establishment.In order to avoid duplicating a similarrequirement proposed in the GTPregulations, we have deleted therequirement from § 1271.25(c).
(Comment 38) We earlier stated thatwe were developing an electronicversion of Form FDA 3356 (registrationproposed rule, 63 FR 26750). Onecomment strongly supported theseefforts and asserted that manufacturersshould also be able to submitregistration and listing informationelectronically.
We understand that it would beconvenient to submit registration andlisting information electronically overthe Internet. We intend to rely on ourexperience in developing electronicsubmission capability in other areas(e.g., biological product deviations inmanufacturing reports) to develop anelectronic submission process for HCT/P registration and listing. Whenelectronic submissions of Form FDA3356 are possible, we will make anannouncement to that effect.
(Comment 39) Two commentsdisagreed with the requirementproposed in § 1271.25(a)(4) for astatement affirming the truth andaccuracy of all information in theregistration and listing form. Thecomments argued that no similarrequirement exists in the registrationand listing regulations for drugs anddevices, parts 207 and 807. Thecomments proposed that, if therequirement is maintained, thestatement be qualified with a phrasesuch as ‘‘to the best of my knowledge.’’
To be of use, information submittedon the registration and listing form mustbe truthful and accurate. Moreover, thereporting official who completes andsigns the form should be aware of theobligation to report truthfully andaccurately. Although, as the commentpoints out, the registration and listingregulations for drugs and devices do notcontain a similar statement, the actspecifically prohibits the submission offalse or misleading reports with respectto any device (section 301(q)(2) of theact (21 U.S.C. 331(q)(2)). Furthermore, awillfully false statement to a Federalagency is a criminal offense, and it isnot uncommon for forms submitted tothe agency to so note (18 U.S.C. 1001).
For these reasons, we are maintainingthe requirement for a statementaffirming the truth and accuracy of theinformation submitted on theregistration and listing form. However,the reporting official may reasonablyobtain the reported information fromreliable sources rather than firsthand.For this reason, we believe it isreasonable to modify the requiredstatement with the language ‘‘to the bestof my knowledge.’’ We have made thischange to the regulation and to the form.
(Comment 40) Two commentsquestioned the requirement proposed in
§ 1271.25(b) for a statement of whethereach listed product meets the criteria setout in § 1271.10. One comment queriedwhether we plan to regard thisstatement as an admission that aproduct is or is not a 361 HCT/P. Thiscomment suggested the addition oflanguage consistent with that of otherproduct registration and listingregulations clarifying that registrationand listing under part 1271 does notconstitute such an admission of productregulatory status. Both comments notedthat only the statement is required, notan explanation or summary of why aproduct does or does not meet thecriteria or which criteria are not met.
The categorization of HCT/P’s as 361HCT/P’s or as drugs, devices, and/orbiological products is a fundamentalcomponent of the new tiered, risk-basedsystem. We are requiring thisinformation for each HCT/P type to helpus understand the HCT/P industry.Establishments need to know how theirproducts are regulated in order tocomply with appropriate requirements;therefore, the information requiredshould be readily available. Weunderstand that there may be instanceswhere an establishment is unsure intowhich category its HCT/P falls; theestablishment should contact theexecutive secretariat of the TRG in thesesituations. (For more information on theTRG, see CBER’s website at http://www.fda.gov/cber/tissue/trg.htm.)
The requirement in § 1271.25(b) is fora statement only, not an explanation.The statement will inform the agency ofthe manufacturer’s opinion, but will notbe an ‘‘admission’’ with respect to howan HCT/P will be regulated. To beregulated solely under section 361 of thePHS Act and part 1271, an HCT/P mustmeet the criteria set forth under§ 1271.10.
(Comment 41) Two commentsrequested that we clarify whetherindividual sizes or configurations oftissues should be listed separately, orinstead under more general headings.One of these comments questionedwhether a ‘‘new’’ product wouldinclude a new size of a product.
The information currently required onthe registration and listing form is of amore general nature. Because the formdoes not ask for sizes, a new productwould not include a new product size.
(Comment 42) One commentencouraged the use of standard productnames for hematopoietic progenitor celltherapies in order to make productlisting consistent.
We encourage the development ofstandard names. However, at this pointwe are requesting more generalinformation on Form FDA 3356. In the
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00035 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5462 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
future, we may ask for more detailedinformation.
(Comment 43) One commentrecommended that required listinginformation include, with respect toeach listed type of tissue, the specificmanufacturing activities conducted ateach registered establishment.
To simplify the registration andlisting form, we are not asking forspecific manufacturing information foreach product but for the establishmentin general. If there is a need, we maypossibly ask for more specificinformation in the future.
(Comment 44) One commentquestioned whether the addition of anadjacent building with a differentaddress would be considered a newlocation, requiring an amendment toregistration under § 1271.26.
No. Adding an adjacent buildingwould not require an amendment toregistration.
(Comment 45) No comments werereceived on proposed § 1271.27, whichdeals with the assignment of aregistration number. We wish, however,to note that establishments that arecurrently registered under the drug ordevice registration and listingrequirements, and who would in thefuture register and list using theprocedures in part 1271, when that partis fully effective, would keep the sameregistration number that was issuedpreviously. Those establishmentsshould provide that number to us whenregistering for the first time using thenew procedures.
(Comment 46) One commentsupported the release of registration andlisting information under § 1271.37, butquestioned how we would determinewhich information to disclose to thepublic.
The information submitted on FormFDA 3356 is not proprietary orconfidential in nature and may bereleased to the public. Section1271.37(a)(4) notes that the agency mayalso release all data or information thathas already become a matter of publicrecord. The agency will follow theprocedures and requirements set out in21 CFR part 20 to determine whichinformation has become a matter ofpublic record and may be released.
F. Comments on the ProposedAmendments to §§ 207.20 and 807.20
(Comment 47) No comments weresubmitted on the proposed amendmentsto §§ 207.20 and 807.20.
We have modified the languageproposed for §§ 207.20(f) and 807.20(e)to clarify that establishments thatmanufacture HCT/P’s regulated asdevices, drugs, and/or biological
products will register and list theirproducts following the procedures inpart 1271 instead of the procedures inparts 207 and 807. Thus, when this ruleis effective for HCT/P’s regulated asdevices, drugs, and or biologicalproducts, these establishments willsubmit Form FDA 3356 according to theprocedures set out in subpart B of part1271, at the same time as other cell andtissue establishments, and will nolonger have to submit other registrationand listing forms. We have alsorenumbered proposed § 807.20(e) as§ 807.20(d).
The effective date of §§ 207.20(f) and807.20(d) is 2 years after the publicationof this rule.
G. Comments on the Registration andListing Form (Form FDA 3356)
We asked nine manufacturers toparticipate in a pilot study to evaluateFDA Form 3356 in draft form, asallowed by the Office of Managementand Budget (OMB) before we finalizedthe paperwork burden analysis. Thepilot study had two purposes: Toevaluate the ease of use of Form FDA3356, and to validate the data basesoftware developed for FDA undercontract. The pilot study took place inMay 1998, and in August 1998 wesubmitted to the docket a summary ofthe results of the study.
Six of the participating establishmentsnoted that the draft form was easy to useand required less than 1 hour tocomplete. Other comments on the formnoted several areas of potentialconfusion. We have addressed many ofthese issues elsewhere in thisdocument, in response to commentssubmitted to the docket. We haveaddressed other issues by modifying theinstructions for completing the form.
We have made minimal changes toForm FDA 3356 and its instructions toconform to the revised requirements inpart 1271, subpart B. We have not addedany additional informationrequirements.
IV. Analysis of Economic ImpactsFDA has examined the impacts of the
rule under Executive Order 12866 andthe Regulatory Flexibility Act (5 U.S.C.601–612) as amended by subtitle D ofthe Small Business Regulatory FairnessAct of 1996 (Public Law 104–121) andunder the Unfunded Mandates ReformAct of 1995 (Public Law 104–4).Executive Order 12866 directs agenciesto assess all costs and benefits ofavailable regulatory alternatives and,when regulation is necessary, to selectregulatory approaches that maximizenet benefits (including potentialeconomic, environmental, public health
and safety, and other advantages;distributive impacts; and equity). Theagency believes the final rule isconsistent with the regulatoryphilosophy and principles identified inthe Executive Order. OMB hasdetermined that the final rule is asignificant action as defined inExecutive Order 12866.
The Regulatory Flexibility Actrequires agencies to analyze whether arule may have a significant impact on asubstantial number of small entitiesand, if it does, to analyze regulatoryoptions that would minimize theimpact. The Unfunded MandatesReform Act requires that agenciesprepare an assessment of anticipatedcosts and benefits before proposing anyrule that may result in an expenditureby State, local, and tribal governments,in the aggregate, or by the private sector,of $100,000,000 (adjusted annually forinflation) in any one year. We have alsodetermined that this rule will not resultin aggregate expenditures for State,local, and tribal governments, or theprivate sector of $100 million in any oneyear (adjusted for inflation).
An analysis of available informationsuggests that costs to the entities mostaffected by this rule, including smallentities, are not expected to besignificant, as described in the analysisbelow. Therefore, the agency certifiesthat this rule will not have a significantimpact on a substantial number of smallentities.
A. Objective and Basis of the ActionThis action is a first step in the
regulation of the rapidly evolvingindustry of human cells and tissue. Theentire industry has not been previouslyregulated under a single comprehensiveregulatory program by FDA or otherpublic health authorities. Lack of asingle regulatory approach orregistration system has prevented theagency from acquiring informationregarding the full size of the cell andtissue industry and the scope of humancells, tissues, and cellular and tissue-based products (HCT/P’s) that are usedby the industry. The rule will require allmanufacturers of HCT/P’s to registerwith the agency and to submit to theagency a list of their HCT/P’s. Throughregistration and listing, FDA will be ableto identify industry participants and thescope of the HCT/P’s produced. Thiswill enable the agency to moreefficiently monitor the industry,distribute new information such asguidances, policies, or requirements,and identify entities that may be subjectto FDA oversight. This action is takensolely under the authority of section 361of the PHS Act. Section 361 of the PHS
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00036 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5463Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
Act is also used as authority to amendparts 207 and 807 so that theregistration and data bases for all humancells, tissues, and cellular and tissue-based products may be consolidated.FDA has reviewed related Federal rulesand has not identified any rules thatduplicate, overlap, or conflict with therule.
B. Small Entities AffectedThis rule affects both establishments
that currently register with FDA andsubmit product lists to the agency underapplicable sections of the act (parts 207and 807), and those establishments thatare not presently required to register orlist with the agency. FDA has structuredregistration and listing for HCT/P’s tohave a minimal impact on affectedestablishments. However, the agencyanticipates that the impact will begreater for those establishments that donot currently register or list. Because thefinal rule is effective 75 days afterpublication of this document for thoseestablishments currently regulatedunder part 1270, and is effective in 2years for all other HCT/Pestablishments, the economic impact onthe industry will be staggered.
The total number of establishmentsthat are required to register and listunder part 1271 in 2 years after thepublication of this rule is estimated tobe 1,225. The registration and listinginitiative will, in part, help the agencyobtain more accurate numbers of HCT/P’s establishments. In calculating theburden, the agency has relied oninformation obtained from tradeorganizations related to the human cells,tissue, and cellular and tissue-basedproducts industry, several of which alsoprovided estimates of what portion ofthe industry their membershiprepresented. Along with thisinformation and from our own research,we determined that 65 manufacturers ofhuman cells, tissue, and cellular andtissue-based products are registeredwith the agency as required by part 807.The agency also determined that onemanufacturer of an HCT/P drug isregistered as required by part 207
According to the U.S. Small BusinessAdministration, a tissue bank is a smallentity if it has annual revenues less than$5 million. FDA estimates that 110tissue banks are involved in themanufacture of conventional tissue andthat approximately 77.5 percent (or 85)of these banks are small entities. FDAestimates that there are 425 stem cellfacilities (400 peripheral blood stem cellfacilities and 25 cord blood facilities),and that all are small entities. FDAestimates that approximately 114 eyebanks are currently operating in the
United States, and industry expertsestimate that virtually all facilitieswould be classified as small. FDAestimates that there are approximately400 assisted reproductive technology(ART) facilities. This estimate isconsistent with industry comments.Consultants estimate that two-thirds ofall ART facilities (or 267establishments) would be classified assmall entities. In addition, the AmericanSociety of Reproductive Medicine(ASRM) has a 1996 list of approximately110 sperm banks operating in the U.S.Information about sperm banks from areport by Eastern Research Group (ERG)indicates that 95 percent (or 105) ofthese sperm banks are small. Thus,approximately 996 (85 + 425 + 114 +267 + 105) of all 1,225 establishmentswould be considered small entities. Inaddition, 66 establishments arecurrently regulated as drugs, devices, orbiological products under parts 207 and807. Approximately 90 percent of these(or 60 establishments) are small entities.Therefore, we estimate that a total 1,056establishments (996 + 60) are smallentities.
C. Nature of the ImpactThe main cost in implementing this
final rule is staff time, which weestimate to cost $38.00 per hour, basedon 1997 Bureau of Labor Statisticsestimates.
Out of a total 1,225 establishmentsaffected by this rule, 66 HCT/P drug anddevice establishments currently submitregistration and product listinginformation under parts 207 and 807. Inthe proposed rule, we incorrectlyestimated both the time and the scopeof annual information collection forthese establishments. Our estimateinaccurately lumped the submission ofall required information into one yearand concluded that 2 hours would beneeded annually to register and listinitially, submit a subsequent annualregistration, update HCT/P listings, andamend ownership or locationinformation.
As proposed, however, this final rulerequires that HCT/P drug and devicemanufacturers use a new, single form toregister and list their HCT/P products.This rule does not impose any newregistration or listing requirements forestablishments regulated under parts207 and 807. To avoid duplication, therule provides HCT/P drug and devicemanufacturers a single, new form toreplace the multiple forms currentlyrequired under parts 207 and 807.Therefore, we now estimate only thetime needed to transition from the useof multiple forms to the use of the oneform. Based on results from the pilot
study described above in section III.G ofthis document, we estimate thatestablishments will need approximately0.5 hour to transition to Form FDA 3356at a one-time transition cost ofapproximately $19 [$38 x 0.5]. Weestimate that the total impact for all 66establishments will be approximately$1,254 [66 x $38 x 0.5].
For the 1,159 HCT/P manufacturersnot regulated under parts 207 and 807,the costs are based upon the staff timeneeded to obtain the form, read theinstructions, and complete and submitthe form for the initial registration andHCP/T listing, subsequent annualregistration, and, as needed, listingupdates and location/ownershipamendments. Based on the pilot studydescribed above, FDA estimates that itwill take an average of 0.75 hour of stafftime per establishment for the initialsubmission. At $38.00 per hour of stafftime, each establishment is expected toincur an initial one-time cost ofapproximately $28 [$38 x 0.75]. Weestimate the total impact for all 1,159establishments for the submission ofinitial registration and HCT/P listing tobe approximately $33,032 [1,159 x $38x 0.75].
After the initial registration, the finalrule requires annual registration, whichwe estimate will take 0.5 hour tocomplete and submit to FDA. Weestimate that the annual cost of thesesubmissions will be approximately$22,021 [1,159 x $38 x 0.5] or $19 perestablishment.
The final rule also requires HCT/Plisting updates twice a year, asubmission that is required only whena change has been made since theprevious listing submission. FDAassumes that in any given year, 5percent or 58 of the 1,159establishments [1,159 x 0.05] willsubmit one listing. The listing update isestimated to take about 0.5 hours tocomplete and submit to FDA. Weestimate that each establishment willincur an annual cost of approximately$19 [$38 x 0.5], for a total of $1,102 forall 58 establishments.
The rule also requires changes inownership or location to be reported asan amendment within 5 days of suchchanges. FDA expects that this will bea rare event and that in any given year,no more than 5 percent or 58 of the1,159 establishments [1,159 x 0.05] willchange location or ownership andsubmit an amendment. This amendmentis estimated to take 0.25 hours of stafftime. We estimate that eachestablishment will incur a cost ofapproximately $10 [$38 x 0.25], totaling$580 for all 58 establishments.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00037 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5464 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
In sum, we estimate the total annualfor all submissions subsequent to theinitial registration and listing (annualregistration and, as needed, listingupdates and location/ownershipamendments) to be $23,702 [$22,021 +$1,101 + $580].
There are no specific educational ortechnical skills required to completeand submit the registration and listingform. Trained and qualified employeesof an establishment who are involvedwith its operations generally completesimilar activities.
This final rule is the first step increating a tiered, risk-based regulatoryscheme that will tailor the degree ofscrutiny afforded to different HCT/P’s tothe risks associated with each of them.Through registration and listing, FDAwill acquire the information needed tocharacterize the nature and extent ofHCT/P’s. This information will enableFDA to efficiently and effectivelyrespond to emerging public healthconcerns related to human cells ortissue. Lists of industry members andtheir HCT/P’s will also help FDAdisseminate educational materials andother important information regardingFDA policies, guidances, andrequirements.
D. Minimizing the Impact on SmallEntities
FDA recognizes that a large number ofthe establishments that would berequired to register and list under therule will be small entities with limitedresources. In recognition of this, theagency is proposing that the informationto be provided during registration andlisting be only that which is necessaryto achieve the agency’s goals of industrycharacterization and identification of itsparticipants. To alleviate the impact onentities, especially small entities, FDAwill consider the use of electronicsubmissions (e-mail or Internet) andelectronic signatures.
V. Environmental ImpactThe agency has determined under 21
CFR 25.30(h) that this action is of a typethat is categorically excluded from thepreparation of an environmentalassessment because these actions, as aclass, will not result in the productionor distribution of any substance andtherefore will not result in theproduction of any substance into theenvironment.
VI. FederalismFDA has analyzed this final rule in
accordance with the principles set forthin Executive Order 13132. FDA hasdetermined that the rule does notcontain policies that have substantial
direct effects on the States, on therelationship between NationalGovernment and the States, or on thedistribution of power andresponsibilities among the variouslevels of government. Accordingly, theagency has concluded that the rule doesnot contain policies that havefederalism implications as defined inthe order and, consequently, afederalism summary impact statement isnot required.
VII. The Paperwork Reduction Act of1995
This final rule contains informationcollection requirements that are subjectto review by the Office of Managementand Budget (OMB) under the PaperworkReduction Act of 1995 (PRA) (44 U.S.C.3501–3520). The title, description, andrespondent description of theinformation collection requirements areshown below with an estimate of theinitial one-time reporting burden andthe annual reporting burden. Includedin the estimate is the time for reviewingthe instructions, searching existing datasources, gathering and maintaining thedata needed, completing and reviewingeach collection of information.
Title: Establishment Registration andListing Requirements for Human Cells,Tissues, and Cellular and Tissue-BasedProducts.
Description: The final rule requiresestablishments that recover, process,store, label, package, or distribute anyhuman cell, tissue, and cellular andtissue-based product (HCT/P), or thatperform donor screening or testing, tosubmit an initial establishmentregistration and HCT/P list to FDA.Subsequently, establishments mustsubmit an annual update to theirestablishment registration. In addition,establishments are required to submitHCT/P list updates, if any, andamendments whenever anestablishment changes ownership orlocations. FDA provides a registrationand listing form (Form FDA 3356) tofacilitate the ease and speed ofsubmissions. Form FDA 3356 is anapproved information collection formatunder OMB control number 0910–0372.The approval expires July 31, 2001.
Description of Respondents:Establishments that recover, process,store, label, package, or distribute anyhuman cells, tissue, and cellular andtissue-based product.
As required by section 3506(c)(2)(B)of the PRA, FDA provided anopportunity for public comment on May14, 1998 (63 FR 26744), on theinformation collection requirements ofthe proposed rule.
Table 1 of this document lists theestimated one-time reporting burden forthe initial establishment registration andHCT/P listing, which is required under§ 1271.10(b). Section 1271.25(a) and (b)identify the initial establishment andHCT/P listing information required.Sections 207.20(f) and 807.20(d) requireHCT/P establishments to use Form FDA3356 for providing registration andlisting information required under parts207 and 807.
Table 2 of this document provides theestimate of the ongoing annual reportingburden for establishment registration. Inaddition, table 2 of this document setsout estimated reporting burdens forHCT/P listing updates andestablishment location or ownershipamendments that would occur duringany given year. If there is no change toan HCT/P listing, establishment locationor ownership, a submission is notrequired.
Sections 1271.21(b) and 1271.10(b)require the annual establishmentregistration by domestic and foreignHCT/P establishments that are solelyregulated under section 361 of the PHSAct and this part.
Sections 1271.21(c)(ii), 1271.25(c),and 1271.10(b) require domestic andforeign HCT/P establishments to submitHCT/P listing updates only when anHCT/P is changed, added, ordiscontinued, and when there has beena material change to informationsubmitted previously to the agency. Ifno change has occurred since theprevious submission, an update is notrequired.
Sections 1271.26 and 1271.10(b)require domestic and foreign HCT/Pestablishments to submit anamendment, but only when theestablishment makes a change inlocation or ownership.
Sections 207.20, 207.26, 207.30,807.20, 807.26, and 807.30 alreadyrequire establishments that manufacturedrug or device products to submit initialestablishment registration and productlisting, as well as annual establishmentregistration, product listing updates,and location and ownershipamendments. This final rule adds§§ 207.20(f) and 807.20(d), whichrequire that manufacturers of HCT/Pdrugs and devices submit thisregistration and listing informationusing Form FDA 3356 instead of themultiple forms identified under parts207 and 807. Therefore, theseestablishments will incur only a one-time burden to transition from the useof several forms to the use of one form(see table 1 above). This rule adds nonew registration and listingrequirements.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00038 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1
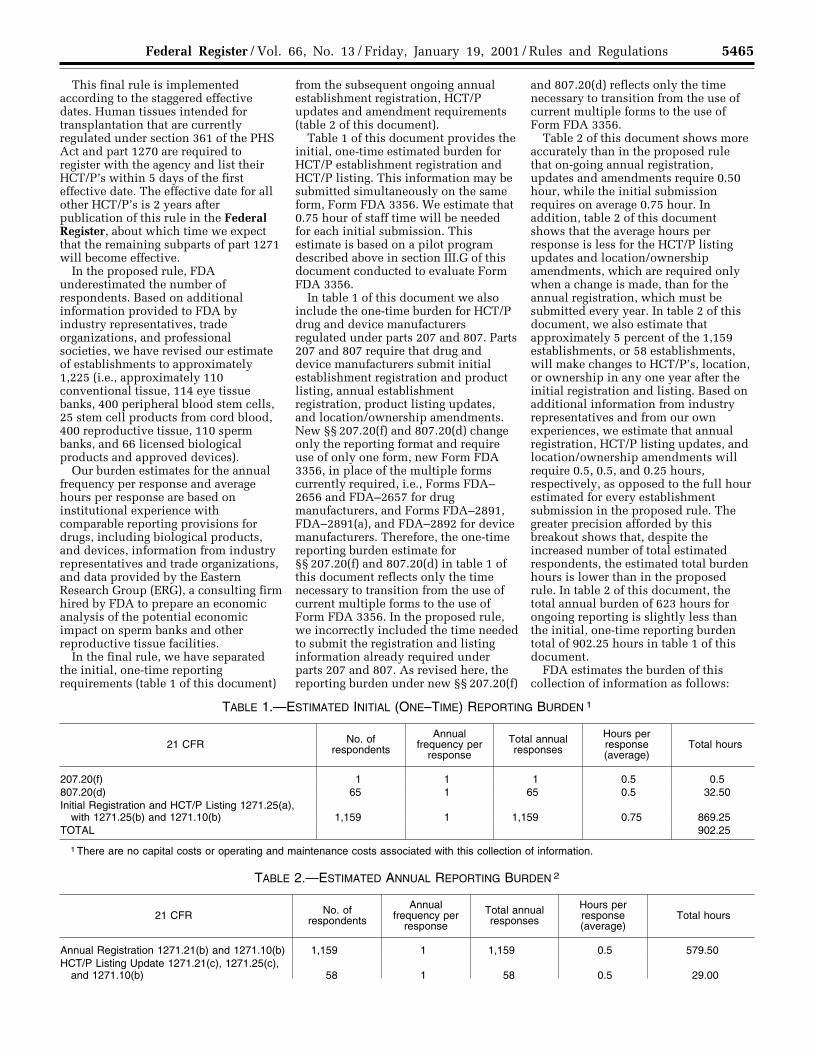
5465Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
This final rule is implementedaccording to the staggered effectivedates. Human tissues intended fortransplantation that are currentlyregulated under section 361 of the PHSAct and part 1270 are required toregister with the agency and list theirHCT/P’s within 5 days of the firsteffective date. The effective date for allother HCT/P’s is 2 years afterpublication of this rule in the FederalRegister, about which time we expectthat the remaining subparts of part 1271will become effective.
In the proposed rule, FDAunderestimated the number ofrespondents. Based on additionalinformation provided to FDA byindustry representatives, tradeorganizations, and professionalsocieties, we have revised our estimateof establishments to approximately1,225 (i.e., approximately 110conventional tissue, 114 eye tissuebanks, 400 peripheral blood stem cells,25 stem cell products from cord blood,400 reproductive tissue, 110 spermbanks, and 66 licensed biologicalproducts and approved devices).
Our burden estimates for the annualfrequency per response and averagehours per response are based oninstitutional experience withcomparable reporting provisions fordrugs, including biological products,and devices, information from industryrepresentatives and trade organizations,and data provided by the EasternResearch Group (ERG), a consulting firmhired by FDA to prepare an economicanalysis of the potential economicimpact on sperm banks and otherreproductive tissue facilities.
In the final rule, we have separatedthe initial, one-time reportingrequirements (table 1 of this document)
from the subsequent ongoing annualestablishment registration, HCT/Pupdates and amendment requirements(table 2 of this document).
Table 1 of this document provides theinitial, one-time estimated burden forHCT/P establishment registration andHCT/P listing. This information may besubmitted simultaneously on the sameform, Form FDA 3356. We estimate that0.75 hour of staff time will be neededfor each initial submission. Thisestimate is based on a pilot programdescribed above in section III.G of thisdocument conducted to evaluate FormFDA 3356.
In table 1 of this document we alsoinclude the one-time burden for HCT/Pdrug and device manufacturersregulated under parts 207 and 807. Parts207 and 807 require that drug anddevice manufacturers submit initialestablishment registration and productlisting, annual establishmentregistration, product listing updates,and location/ownership amendments.New §§ 207.20(f) and 807.20(d) changeonly the reporting format and requireuse of only one form, new Form FDA3356, in place of the multiple formscurrently required, i.e., Forms FDA–2656 and FDA–2657 for drugmanufacturers, and Forms FDA–2891,FDA–2891(a), and FDA–2892 for devicemanufacturers. Therefore, the one-timereporting burden estimate for§§ 207.20(f) and 807.20(d) in table 1 ofthis document reflects only the timenecessary to transition from the use ofcurrent multiple forms to the use ofForm FDA 3356. In the proposed rule,we incorrectly included the time neededto submit the registration and listinginformation already required underparts 207 and 807. As revised here, thereporting burden under new §§ 207.20(f)
and 807.20(d) reflects only the timenecessary to transition from the use ofcurrent multiple forms to the use ofForm FDA 3356.
Table 2 of this document shows moreaccurately than in the proposed rulethat on-going annual registration,updates and amendments require 0.50hour, while the initial submissionrequires on average 0.75 hour. Inaddition, table 2 of this documentshows that the average hours perresponse is less for the HCT/P listingupdates and location/ownershipamendments, which are required onlywhen a change is made, than for theannual registration, which must besubmitted every year. In table 2 of thisdocument, we also estimate thatapproximately 5 percent of the 1,159establishments, or 58 establishments,will make changes to HCT/P’s, location,or ownership in any one year after theinitial registration and listing. Based onadditional information from industryrepresentatives and from our ownexperiences, we estimate that annualregistration, HCT/P listing updates, andlocation/ownership amendments willrequire 0.5, 0.5, and 0.25 hours,respectively, as opposed to the full hourestimated for every establishmentsubmission in the proposed rule. Thegreater precision afforded by thisbreakout shows that, despite theincreased number of total estimatedrespondents, the estimated total burdenhours is lower than in the proposedrule. In table 2 of this document, thetotal annual burden of 623 hours forongoing reporting is slightly less thanthe initial, one-time reporting burdentotal of 902.25 hours in table 1 of thisdocument.
FDA estimates the burden of thiscollection of information as follows:
TABLE 1.—ESTIMATED INITIAL (ONE–TIME) REPORTING BURDEN 1
21 CFR No. ofrespondents
Annualfrequency per
response
Total annualresponses
Hours perresponse(average)
Total hours
207.20(f) 1 1 1 0.5 0.5807.20(d) 65 1 65 0.5 32.50Initial Registration and HCT/P Listing 1271.25(a),
with 1271.25(b) and 1271.10(b) 1,159 1 1,159 0.75 869.25TOTAL 902.25
1 There are no capital costs or operating and maintenance costs associated with this collection of information.
TABLE 2.—ESTIMATED ANNUAL REPORTING BURDEN 2
21 CFR No. ofrespondents
Annualfrequency per
response
Total annualresponses
Hours perresponse(average)
Total hours
Annual Registration 1271.21(b) and 1271.10(b) 1,159 1 1,159 0.5 579.50HCT/P Listing Update 1271.21(c), 1271.25(c),
and 1271.10(b) 58 1 58 0.5 29.00
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00039 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5466 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
TABLE 2.—ESTIMATED ANNUAL REPORTING BURDEN 2—Continued
21 CFR No. ofrespondents
Annualfrequency per
response
Total annualresponses
Hours perresponse(average)
Total hours
Location/Ownership Amendment 1271.26 and1271.10(b) 58 1 58 0.25 14.50
TOTAL 623
2 There are no capital costs or operating and maintenance costs associated with this collection of information.
Individuals and organizations maysubmit comments on these burdenestimates or on any other aspect of theseinformation collection requirements,including suggestions for reducing theburden. Comments should be directedto the Food and Drug Administration,Center for Biologics Evaluation andResearch, Tissue EstablishmentRegistration Coordinator (HFM–305),1401 Rockville Pike, suite 200N,Rockville, MD 20852.
The information collectionrequirements of the final rule have beensubmitted to OMB for review. Prior tothe effective date of the final rule, FDAwill publish a document in the FederalRegister announcing OMB’s decision toapprove, modify, or disapprove theinformation collection requirements inthe final rule. An agency may notconduct or sponsor, and a person is notrequired to respond to, a collection ofinformation unless it displays acurrently valid OMB control number.
VIII. References
The following references have beenplaced on display in the DocketsManagement Branch (address above)and may be seen by interested personsbetween 9 a.m. and 4 p.m., Mondaythrough Friday.
1. Vice President’s National PerformanceReview report, ‘‘Reinventing the Regulationof Human Tissue,’’ February 1997.
2. Schipper, R. F., D’Amaro, J., andOudshoorn, M., ‘‘The Probability of Findinga Suitable Related Donor for Bone MarrowTransplantation in Extended Families,’’Blood, 87:800–804, 1996.
3. Kaufman, R., ‘‘A Generalized HLAPrediction Model for Related DonorMatches,’’ Bone Marrow Transplantation,17:1013–1020, 1996.
List of Subjects
21 CFR Part 207
Drugs, Reporting and recordkeepingrequirements.
21 CFR Part 807
Confidential business information,Imports, Medical devices, Reporting andrecordkeeping requirements.
21 CFR Part 1271
Human cells, Reporting andrecordkeeping requirements, tissue-based products.
Therefore, under the Federal Food,Drug, and Cosmetic Act and the PublicHealth Service Act, and under authoritydelegated to the Commissioner of Foodand Drugs, chapter I of title 21 of theCode of Federal Regulations is amendedas follows:
PART 207—REGISTRATION OFPRODUCERS OF DRUGS AND LISTINGOF DRUGS IN COMMERCIALDISTRIBUTION
1. The authority citation for 21 CFRpart 207 is revised to read as follows:
Authority: 21 U.S.C. 331, 351, 352, 355,356, 360, 360b, 371, 374; 42 U.S.C. 262, 264,271.
2. Section 207.20 is amended byrevising the heading and addingparagraph (f) to read as follows:
§ 207.20 Who must register and submit adrug list?
* * * * *(f) Owners and operators of
establishments or persons engaged inthe recovery, screening, testing,processing, storage, or distribution ofhuman cells, tissues, and cellular andtissue-based products, as defined in§ 1271.3(d) of this chapter, that areregulated under section 351 of thePublic Health Service Act and/or theFederal Food, Drug, and Cosmetic Actmust register and list those human cells,tissues, and cellular and tissue-basedproducts with the Center for BiologicsEvaluation and Research on Form FDA3356 following the procedures set out insubpart B of part 1271 of this chapter,instead of the procedures for registrationand listing contained in this part, exceptthat the additional listing informationrequirements in § 207.31 remainapplicable.
PART 807—ESTABLISHMENTREGISTRATION AND DEVICE LISTINGFOR MANUFACTURERS ANDDISTRIBUTORS OF DEVICES
3. The authority citation for 21 CFRpart 807 is revised to read as follows:
Authority: 21 U.S.C. 331, 351, 352, 360,360c, 360e, 360i, 360j, 371, 374; 42 U.S.C.264, 271.
4. Section 807.20 is amended byrevising the heading and addingparagraph (d) to read as follows:
§ 807.20 Who must register and submit adevice list?
* * * * *(d) Owners and operators of
establishments or persons engaged inthe recovery, screening, testing,processing, storage, or distribution ofhuman cells, tissues, and cellular andtissue-based products, as defined in§ 1271.3(d) of this chapter, that areregulated under the Federal Food, Drug,and Cosmetic Act must register and listthose human cells, tissues, and cellularand tissue-based products with theCenter for Biologics Evaluation andResearch on Form FDA 3356 followingthe procedures set out in subpart B ofpart 1271 of this chapter, instead of theprocedures for registration and listingcontained in this part, except that theadditional listing informationrequirements of § 807.31 remainapplicable.
5. Part 1271 is added to read asfollows:
PART 1271—HUMAN CELLS, TISSUES,AND CELLULAR AND TISSUE–BASEDPRODUCTS
Subpart A—General Provisions
Sec.1271.1 What are the purpose and scope of
this part?1271.3 How does FDA define important
terms in this part?1271.10 Are my HCT/P’s regulated solely
under section 361 of the PHS Act and theregulations in this part, and if so whatmust I do?
1271.15 Are there any exceptions from therequirements of this part?
1271.20 If my HCT/P’s do not meet thecriteria in § 1271.10, and I do not qualify
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00040 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1
5467Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
for any of the exceptions in § 1271.15,what regulations apply?
Subpart B—Procedures for Registrationand Listing
1271.21 When do I register, submit an HCT/P list, and submit updates?
1271.22 How and where do I register andsubmit an HCT/P list?
1271.25 What information is required forestablishment registration and HCT/Plisting?
1271.26 When must I amend myestablishment registration?
1271.27 Will FDA assign me a registrationnumber?
1271.37 Will establishment registrationsand HCT/P listings be available forinspection, and how do I requestinformation on registrations and listings?
Authority: 42 U.S.C. 216, 243, 264, 271.
Subpart A—General Provisions
§ 1271.1 What are the purpose and scopeof this part?
(a) Purpose. The purpose of this part,in conjunction with §§ 207.20(f),210.1(c), 210.2, 807.20(d), and 820.1(a)of this chapter, is to create a unifiedregistration and listing system forestablishments that manufacture humancells, tissues, and cellular and tissue-based products (HCT/P’s) and toestablish donor-suitability, current goodtissue practice, and other procedures toprevent the introduction, transmission,and spread of communicable diseasesby HCT/P’s.
(b) Scope. (1) If you are anestablishment that manufactures HCT/P’s that are regulated solely under theauthority of section 361 of the PublicHealth Service Act (the PHS Act), thispart requires you to register and listyour HCT/P’s with the Food and DrugAdministration’s (FDA’s) Center forBiologics Evaluation and Research andto comply with the other requirementscontained in this part, whether or notthe HCT/P enters into interstatecommerce. Those HCT/P’s that areregulated solely under the authority ofsection 361 of the PHS Act are describedin § 1271.10.
(2) If you are an establishment thatmanufactures HCT/P’s that are regulatedas drugs, devices and/or biologicalproducts under section 351 of the PHSAct and/or the Federal Food, Drug, andCosmetic Act, §§ 207.20(f) and 807.20(d)of this chapter require you to registerand list your HCT/P’s following theprocedures in subpart B of this part.Sections 210.1(c), 210.2, 211.1(b), and820.1(a) of this chapter require you tocomply with the donor-suitabilityprocedures in subpart C of this part andthe current good tissue practiceprocedures in subpart D of this part, in
addition to all other applicableregulations.
§ 1271.3 How does FDA define importantterms in this part?
The following definitions apply onlyto this part:
(a) Autologous use means theimplantation, transplantation, infusion,or transfer of human cells or tissue backinto the individual from whom the cellsor tissue were recovered.
(b) Establishment means a place ofbusiness under one management, at onegeneral physical location, that engagesin the manufacture of human cells,tissues, and cellular and tissue-basedproducts. ‘‘Establishment’’ includes:
(1) Any individual, partnership,corporation, association, or other legalentity engaged in the manufacture ofhuman cells, tissues, and cellular andtissue-based products; and
(2) Facilities that engage in contractmanufacturing services for amanufacturer of human cells, tissues,and cellular and tissue-based products.
(c) Homologous use means thereplacement or supplementation of arecipient’s cells or tissues with an HCT/P that performs the same basic functionor functions in the recipient as in thedonor.
(d)(1) Human cells, tissues, or cellularor tissue-based products (HCT/P’s)means any human tissue derived from ahuman body and intended fortransplantation into another human, asdefined under § 1270.3(j). Examples ofHCT/P’s include, but are not limited to,bone, ligament, skin, and cornea.
(2) Human cells, tissues, or cellular ortissue-based products (HCT/P’s) meansarticles containing or consisting ofhuman cells or tissues that are intendedfor implantation, transplantation,infusion, or transfer into a humanrecipient. Examples of HCT/P’s include,but are not limited to, bone, ligament,skin, dura mater, heart valve, cornea,hematopoietic stem cells derived fromperipheral and cord blood, manipulatedautologous chondrocytes, epithelialcells on a synthetic matrix, and semenor other reproductive tissue. Thefollowing articles are not consideredHCT/P’s:
(i) Vascularized human organs fortransplantation;
(ii) Whole blood or blood componentsor blood derivative products subject tolisting under parts 607 and 207 of thischapter, respectively;
(iii) Secreted or extracted humanproducts, such as milk, collagen, andcell factors; except that semen isconsidered an HCT/P;
(iv) Minimally manipulated bonemarrow for homologous use and not
combined with a drug or a device(except for a sterilizing, preserving, orstorage agent, if the addition of the agentdoes not raise new clinical safetyconcerns with respect to the bonemarrow);
(v) Ancillary products used in themanufacture of HCT/P;
(vi) Cells, tissues, and organs derivedfrom animals other than humans; and
(vii) In vitro diagnostic products asdefined in § 809.3(a) of this chapter.
(e) Manufacture means, but is notlimited to, any or all steps in therecovery, processing, storage, labeling,packaging, or distribution of any humancell or tissue, and the screening ortesting of the cell or tissue donor.
(f) Minimal manipulation means:(1) For structural tissue, processing
that does not alter the original relevantcharacteristics of the tissue relating tothe tissue’s utility for reconstruction,repair, or replacement; and
(2) For cells or nonstructural tissues,processing that does not alter therelevant biological characteristics ofcells or tissues.
(g) Transfer means the placement ofhuman reproductive cells or tissues intoa human recipient.
§ 1271.10 Are my HCT/P’s regulated solelyunder section 361 of the PHS Act and theregulations in this part, and if so what mustI do?
(a) An HCT/P is regulated solelyunder section 361 of the PHS Act andthe regulations in this part if it meets allof the following criteria:
(1) The HCT/P is minimallymanipulated;
(2) The HCT/P is intended forhomologous use only, as reflected by thelabeling, advertising, or otherindications of the manufacturer’sobjective intent;
(3) The manufacture of the HCT/Pdoes not involve the combination of thecell or tissue component with a drug ora device, except for a sterilizing,preserving, or storage agent, if theaddition of the agent does not raise newclinical safety concerns with respect tothe HCT/P; and
(4) Either:(i) The HCT/P does not have a
systemic effect and is not dependentupon the metabolic activity of livingcells for its primary function; or
(ii) The HCT/P has a systemic effector is dependent upon the metabolicactivity of living cells for its primaryfunction, and:
(a) Is for autologous use;(b) Is for allogeneic use in a first-
degree or second-degree blood relative;or
(c) Is for reproductive use.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00041 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1

5468 Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
(b) If you are a domestic or foreignestablishment that manufactures anHCT/P described in paragraph (a) of thissection:
(1) You must register with FDA;(2) You must submit to FDA a list of
each HCT/P manufactured; and(3) You must comply with the other
requirements contained in this part.
§ 1271.15 Are there any exceptions fromthe requirements of this part?
(a) You are not required to complywith the requirements of this part if youare an establishment that uses HCT/P’ssolely for nonclinical scientific oreducational purposes.
(b) You are not required to complywith the requirements of this part if youare an establishment that removes HCT/P’s from an individual and implantssuch HCT/P’s into the same individualduring the same surgical procedure.
(c) You are not required to complywith the requirements of this part if youare a carrier who accepts, receives,carries, or delivers HCT/P’s in the usualcourse of business as a carrier.
(d) You are not required to complywith the requirements of this part if youare an establishment that does notrecover, screen, test, process, label,package, or distribute, but only receivesor stores HCT/P’s solely forimplantation, transplantation, infusion,or transfer within your facility.
(e) You are not required to complywith the requirements of this part if youare an establishment that only recoversreproductive cells or tissue andimmediately transfers them into asexually intimate partner of the cell ortissue donor.
(f) You are not required to register orlist your HCT/P’s independently, butyou must comply with all otherapplicable requirements in this part, ifyou are an individual under contract,agreement, or other arrangement with aregistered establishment and engagedsolely in recovering cells or tissues andsending the recovered cells or tissues tothe registered establishment.
§ 1271.20 If my HCT/P’s do not meet thecriteria in § 1271.10, and I do not qualify forany of the exceptions in § 1271.15, whatregulations apply?
If you are an establishment thatmanufactures an HCT/P that does notmeet the criteria set out in § 1271.10(a),and you do not qualify for any of theexceptions in § 1271.15, your HCT/Pwill be regulated as a drug, device, and/or biological product under the act and/or section 351 of the PHS Act, andapplicable regulations in title 21,chapter I. Applicable regulationsinclude, but are not limited to,
§§ 207.20(f), 210.1(c), 210.2, 211.1(b),807.20(d), and 820.1(a) of this chapter,which require you to follow theprocedures in subparts B, C, and D ofthis part.
Subpart B—Procedures forRegistration and Listing
§ 1271.21 When do I register, submit anHCT/P list, and submit updates?
(a) You must register and submit a listof every HCT/P that your establishmentmanufactures within 5 days afterbeginning operations or within 30 daysof the effective date of this regulation,whichever is later.
(b) You must update yourestablishment registration annually inDecember, except as required by§ 1271.26. You may accomplish yourannual registration in conjunction withupdating your HCT/P list underparagraph (c) of this section.
(c)(i) If no change described in§ 1271.25(c) has occurred sinceyoupreviously submitted an HCT/P list,you are not required to update yourlisting.
(ii) If a change described in§ 1271.25(c) has occurred, you mustupdate your HCT/P listing with the newinformation:
(a) At the time of the change, or(b) Each June or December, whichever
month occurs first after the change.
§ 1271.22 How and where do I register andsubmit an HCT/P list?
(a) You must use Form FDA 3356 for:(i) Establishment registration,(ii) HCT/P listings, and(iii) Updates of registration and HCT/
P listing.(b) You may obtain Form FDA 3356:(i) By writing to the Center for
Biologics Evaluation and Research(HFM–305), Food and DrugAdministration, 1401 Rockville Pike,Rockville, MD 20852–1448, Attention:Tissue Establishment RegistrationCoordinator;
(ii) By contacting any Food and DrugAdministration district office;
(iii) By calling the CBER VoiceInformation System at 1–800–835–4709or 301–827–-1800;
(iv) By calling the Fax InformationSystem at 1–888–CBER–FAX or 301–827–3844; or
(v) By connecting to http://forms.psc.gov/forms/FDA/fda.html onthe Internet.
(c)(i) You may submit Form FDA 3356to the Center for BiologicsEvaluationand Research (HFM–305), Food andDrug Administration, 1401 Rockville,Pike, Rockville, MD 20852–1448,Attention: Tissue EstablishmentRegistration Coordinator; or
(ii) You may submit Form FDA 3356electronically in accordance with theinstructions provided with the form.
§ 1271.25 What information is required forestablishment registration and HCT/Plisting?
(a) Your establishment registrationForm FDA 3356 must include:
(1) The legal name(s) of theestablishment;
(2) Each location, including the streetaddress of the establishment and thepostal service zip code;
(3) The name, address, and title of thereporting official; and
(4) A dated signature by the reportingofficial affirming that all informationcontained in the establishmentregistration and HCT/P listing form istrue and accurate, to the best of his orher knowledge.
(b) Your HCT/P listing must includeall HCT/P’s (including the establishedname and the proprietary name) thatyou recover, process, store, label,package, distribute, or for which youperform donor screening or testing. Youmust also state whether each HCT/Pmeets the criteria set out in § 1271.10.
(c) Your HCT/P listing update mustinclude:
(1) A list of each HCT/P that you havebegun recovering, processing, storing,labeling, packaging, distributing, or forwhich you have begun donor screeningor testing, that has not been included inany list previously submitted. You mustprovide all of the information requiredby § 1271.25(b) for each new HCT/P.
(2) A list of each HCT/P formerlylisted in accordance with § 1271.21(a)for which you have discontinuedrecovery, processing, storage, labeling,packaging, distribution, or donorscreening or testing, including for eachHCT/P so listed, the identity byestablished name and proprietary name,and the date of discontinuance. Werequest but do not require that youinclude the reason for discontinuancewith this information.
(3) A list of each HCT/P for which anotice of discontinuance was submittedunder paragraph (c)(2) of this sectionand for which you have resumedrecovery, processing, storage, labeling,packaging, distribution, or donorscreening or testing, including theidentity by established name andproprietary name, the date ofresumption, and any other informationrequired by § 1271.25(b) not previouslysubmitted.
(4) Any material change in anyinformation previously submitted.Material changes include any change ininformation submitted on Form FDA3356, such as whether the HCT/P meetsthe criteria set out in § 1271.10.
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00042 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1
5469Federal Register / Vol. 66, No. 13 / Friday, January 19, 2001 / Rules and Regulations
§ 1271.26 When must I amend myestablishment registration?
If the ownership or location of yourestablishment changes, you must submitan amendment to registration within 5days of the change.
§ 1271.27 Will FDA assign me aregistration number?
(a) FDA will assign each location apermanent registration number.
(b) FDA acceptance of anestablishment registration and HCT/Plisting form does not constitute adetermination that an establishment isin compliance with applicable rules andregulations or that the HCT/P is licensedor approved by FDA.
§ 1271.37 Will establishment registrationsand HCT/P listings be available forinspection, and how do I requestinformation on registrations and listings?
(a) A copy of the Form FDA 3356 filedby each establishment will be availablefor public inspection at the Office ofCommunication, Training, andManufacturers Assistance (HFM–48),Center for Biologics Evaluation andResearch, Food and DrugAdministration, 1401 Rockville Pike,suite 200N, Rockville, MD 20852–1448.In addition, there will be available forinspection at each of the Food and DrugAdministration district offices the sameinformation for firms within thegeographical area of such district office.Upon request and receipt of a self-addressed stamped envelope,verification of a registration number orthe location of a registeredestablishment will be provided. Thefollowing information submitted underthe HCT/P requirements is illustrative ofthe type of information that will beavailable for public disclosure when itis compiled:
(1) A list of all HCT/P’s;(2) A list of all HCT/P’s manufactured
by each establishment;(3) A list of all HCT/P’s discontinued;
and(4) All data or information that has
already become a matter of publicrecord.
(b) You should direct your requestsfor information regarding HCT/Pestablishment registrations and HCT/Plistings to the Office of Communication,Training and Manufacturers Assistance(HFM–48), Center for BiologicsEvaluation and Research, Food andDrug Administration, 1401 RockvillePike, suite 200N, Rockville, MD 20852–1448.
Dated: January 2, 2001.Jane E. Henney,Commissioner of Food and Drugs.Donna E. Shalala,Secretary of Health and Human Services.[FR Doc. 01–1126 Filed 1–18–01; 8:45 am]BILLING CODE 4160–01–F
DEPARTMENT OF THE TREASURY
Bureau of Alcohol, Tobacco andFirearms
27 CFR Parts 17 and 18
[T.D. ATF–436]
RIN 1512–AB99
Delegation of Authority for Parts 17and 18
AGENCY: Bureau of Alcohol, Tobaccoand Firearms (ATF), Treasury.ACTION: Treasury decision, final rule.
SUMMARY: Authority delegation. Thisfinal rule places most ATF authoritiescontained in parts 17 and 18, title 27Code of Federal Regulations (CFR), withthe ‘‘appropriate ATF officer’’ andrequires that persons file documentsrequired by parts 17 and 18, title 27Code of Federal Regulations (CFR), withthe ‘‘appropriate ATF officer’’ or inaccordance with the instructions on theATF form. Also, this final rule removesthe definitions of, and references to,specific officers subordinate to theDirector. Concurrently with thisTreasury Decision, ATF Order 1130.13is being published. Through this order,the Director has delegated most of theauthorities in 27 CFR parts 17 and 18 tothe appropriate ATF officers andspecified the ATF officers with whomapplications, notices and other reports,which are not ATF forms, are filed.EFFECTIVE DATE: January 19, 2001.FOR FURTHER INFORMATION CONTACT:Robert Ruhf, Regulations Division,Bureau of Alcohol, Tobacco andFirearms, 650 Massachusetts AvenueNW, Washington, DC 20226 (202–927–8210).SUPPLEMENTARY INFORMATION:
Background
Pursuant to Treasury Decision 120–01(formerly 221), dated June 6, 1972, theSecretary of the Treasury delegated tothe Director of the Bureau of Alcohol,Tobacco and Firearms (ATF), theauthority to enforce, among other laws,the provisions of chapter 51 of theInternal Revenue Code of 1986 (IRC).The Director has subsequentlyredelegated certain of these authorities
to appropriate subordinate officers byway of various means, including byregulation, ATF delegation orders,regional directives, or similar delegationdocuments. As a result, to ascertainwhat particular officer is authorized toperform a particular function underchapter 51, each of these variousdelegation instruments must beconsulted. Similarly, each time adelegation of authority is revoked orredelegated, each of the delegationdocuments must be reviewed andamended as necessary.
ATF has determined that thismultiplicity of delegation instrumentscomplicates and hinders the task ofdetermining which ATF officer isauthorized to perform a particularfunction. ATF also believes thesemultiple delegation instrumentsexacerbate the administrative burdenassociated with maintaining up-to-datedelegations, resulting in an undue delayin reflecting current authorities.
Accordingly, in this final rule, theDirector of ATF is rescinding allauthorities of the Director in parts 17and 18 which were previously delegatedto a specified ATF officer and placingall authorities of the Director with the‘‘appropriate ATF officer.’’ Along withthis final rule, ATF is publishing ATFOrder 1130.13, Delegation Order—Delegation of the Director’s Authoritiesin parts 17 and 18, in which certain ofthese authorities are then delegateddown to the appropriate organizationallevel. The effect of these changes is toconsolidate all delegations of authorityin parts 17 and 18 into one delegationinstrument. This action both simplifiesthe process for determining what ATFofficer is authorized to perform aparticular function and facilitates theupdating of delegations in the event ofa change in delegation or in the eventof a restructuring. As a result,delegations of authority will be reflectedin a more timely and user-friendlymanner.
In addition to the above, this finalrule also eliminates all references in theregulations which identify the ATFofficer with whom an ATF form is filed.Thus, in lieu of identifying theauthorized officer in the regulations, theform itself will indicate the officer withwhom it shall be filed. Similarly, thisfinal rule also amends parts 17 and 18to provide that documents other thanATF forms (such as letterheadapplications, notices and reports) willbe filed with the ‘‘appropriate ATFofficer.’’ The ‘‘appropriate ATF officer’’is the Director’s delegate and will beidentified in the accompanying ATFOrder (ATF Order 1130.13, DelegationOrder—Delegation of the Director’s
VerDate 11<MAY>2000 15:50 Jan 18, 2001 Jkt 194001 PO 00000 Frm 00043 Fmt 4700 Sfmt 4700 E:\FR\FM\19JAR1.SGM pfrm01 PsN: 19JAR1