february newsletter 2014
DESCRIPTION
ÂTRANSCRIPT

News February Issue 2014
Scientific & Medical News
More Inspirational Stories
Make a positive change!
Scleroderma Readers Top Tips
New Year New Attitude
10 NEW YEARS RESOLUTIONS
YOU SHOULD KEEP PAGE 5
KEEP ON MOVING PAGES 14-15

As I write this on New Year’s day, I look forward to the
year ahead with great excitement, despite the howling wind
and pouring rain outside! Looking back to 2013, we ended
the year on a high with the appointment of our fundraising
and volunteer coordinator, Amy Baker, who joined us in
November and many of you will no doubt have had the
pleasure of speaking and being in contact with her already.
We go into 2014 in an even stronger position as an organi-
sation, which will be further enhanced by the work of our
new project coordinator, Chloe Kastoryano, who will be
starting at the end of January, working two days a week on
much-needed projects and taking some of the burden of day
-to-day work off the trustees, whose time is needed else-
where in the Society management.
We continue to build our collaboration with the Raynaud’s
and Scleroderma Association, and will be supporting their
upcoming Raynaud’s Awareness Month in February. Chloe
will be leading us through our leaflet updates in collabora-
tion with the RSA. Our new leaflets will be jointly produced
with the costs shared by both organisations.
The next World Congress on Systemic Sclerosis in Rome is
fast approaching at the beginning of February and we’ll pro-
vide reports from that in the next newsletter. It is always a
very useful occasion with lots of interesting and relevant
information on advances into medical and scientific research
regarding scleroderma.
Finally, an extremely warm thank you from everyone at the
Society to all our members and supporters whose unprece-
dented goodwill and energy throughout 2013 enabled the
Society to continue its important work and fulfil its charita-
ble objectives of providing support, awareness and research
into scleroderma.
With warm regards and best wishes for the new year,
Susie
Editor’s Note: Hello everyone! Happy new year, and wel-
come to this winter issue of Scleroderma
News. This time of year is about casting out
the old and welcoming in the new, there is no
better time for an attitude adjustment. This
issue could change your life!
The end of 2013 brought with it a tragic shock,
with the death of my friend Richard Aransibia, known to many in the Scleroderma
Community. You can read about his journey on pages 6-7. Richard was an opti-
mist, a true inspiration. In 2014 I will be living my life as he would have, to the
fullest! I hope you enjoy reading my new year’s resolutions, on page 5! Perhaps
you have written your own resolutions, or compiled your own 2014 ‘to do’ list?
Why not share this and much more with other readers in the next issue of Scle-
roderma News which will be out in June? I am always interested in hearing what
you’ve been up to! As always, deadline for content, the first of the previous
month . Email me on [email protected]. Until next time…
Hollie xXx
The Scleroderma Society has
adopted the sunflower to repre-
sent our organisation, sunflower
pin badges are available for a
small donation, to buy one
please contact: amy@
sclerodermasociety.co.uk
Scleroderma News: Welcome Page 2
Welcome! Happy New Year! Welcome to our first edition of Scleroderma News 2014!

Scleroderma News: News Page 3
Helpline News:
Continued Professional Development
Our helpline goes from strength to
strength. We have seven well-trained and
very experienced volunteers now, most of whom are able to speak first hand about
Raynaud’s and Scleroderma. When callers
ring the helpline they don’t want to listen
to our ailments though, what they want is
help with their own individual worries and
concerns. Not all callers suffer with Sclero-
derma and Raynaud’s. They may be calling
about a friend, a loved one, or a relative.
Often we receive calls from GPs and clini-
cians. For example, physiotherapists and
occupational therapists who enquire about
the disease, or a specific issue to enable
them to improve the quality of life for
someone that they are working with or
treating. We are always looking for ways
to improve our services through training or
other accredited development. Recently,
Rosemary and Helena attended a Helpline
Partnership conference in Peterborough.
The event, for the helpline sector, brought
together many organisations to share best
practice and knowledge. A good example
of this was from Loughborough University
Helpline Research Unit who talked about
their research into “improving helpline
interactions”. This was a very engaging and
informative session and we brought back
lots of information that can be passed on,
to continue improving our services. Another
session was on Helpline Self Evaluation
where we got to talk and get down to some
very practical work thinking, challenging, and
mapping out what each organisation’s help-
line really wants to achieve. We came away
with some groundwork for development
with our volunteers at the next training
session. Other sessions were on “handling
emotions”, “difficult calls”, and “best prac-
tice in supporting volunteers”. It was a busy
and informative conference and meeting
other charity helpline volunteers and staff
added to the success of the day. Watch this
space for more news and progress.
If you are interested in volunteering on the
help line p lease contact: hele-
If anyone you know is need of support or advice about scleroderma then please pass
on our helpline number: 0800 311 2756
Local Groups News: “I am delighted to be able to welcome
several new local group contacts in various
parts of the country. Alex is in Cornwall,
Anne is in Devon, Lynette joins Diana in
the Derbyshire area, Jessie is in the North
East & Jane is in the West Midlands. It is
wonderful to have so many counties cov-
ered & I must thank all of the above very
much indeed. Because there are so few people in the UK with scleroderma, it is
not an onerous job & I hope the new con-
tacts will enjoy it. Check the website or
the list in the newsletter to see if your
own area is covered, otherwise contact
me! (page 23) Best wishes to all members
for 2014.” Liz Holloway
PHD Research with UCL The trustees of the Scleroderma Society
have decided to participate in the co-
funding of PhD research in co-operation
with UCL (University College London).
We are excited about this opportunity to
become directly involved in PhD research
needed in the field of scleroderma. PhDs
usually last for three years, during which
time we will report back with updates and
news from the research and the labs. The
research at UCL will be supervised by
Prof. David Abraham and Prof. Chris Den-
ton who specialise in scleroderma re-
search. The Society will receive recogni-
tion on presentations given at scientific
meetings and symposia and in any publica-
tion arising out of the work, which will
contribute to the research puzzle in trying
to better understand and develop treat-
ments for scleroderma. We are very excit-ed about this opportunity to become in-
volved in research at grass roots level and
look forward to visiting the labs and re-
porting back on the experience. We will
let you know when the exact subject of
the PhD is decided and when it will start.
Society News The Latest News - Winter
Welcome Amy
“I am Amy Baker and I have been with the Scle-
roderma Society for three months now as a
Fundraising and Volunteer Coordinator. Since
graduating in 2010 I have worked for several
diverse charities in a similar capacity. I thorough-
ly enjoy working within the charitable sector and
look forward to bringing my skills and
knowledge to the Scleroderma Society over the
coming year. I have always enjoyed volunteering
and fundraising and have taken part in many
events in my spare time, from reaching Everest
Base Camp to jumping out of a plane, so what-
ever event you may be planning please get in
touch for advice and a helping hand. I look for-
ward to hearing from many of you during 2014.”

Scleroderma News: Inspire Feature Page 4
Paul Klee was born in Switzerland to a
German father and Swiss mother in
1879. He was a talented artist that, the
Tate recognise, cannot be described as
having one style of art – most of the
paintings we saw yesterday were so
different.
Klee lived through many difficult times.
He struggled to get recognition as an
artist. He never had the security of full
time work because his art was seen as
radical but it was also due to Klee
living in a time when there were politi-
cal, social and economic changes caus-
ing hardship to him and many others.
What we did learn about Klee was his
determination to work through hard
times and we both left the exhibition
with a great deal of respect for a great
artist.
As mentioned earlier Klee’s art has
various different styles. There are
many paintings that are dark and show
distorted figures and shapes. Others
are bright and very colourful, whereas
some are comic, highlighting Klee’s
great sense of fun.
Klee had his first exhibition in 1910
but was told by the curator that the
visiting public largely disliked his art
work. Klee was not put off by that and
continued to produce paintings and
was finally being recognised as an artist
in 1920. Despite having no teaching
experience he began teaching at the
famous Bauhaus in Germany in 1921
and became known world-wide by the
1930s. Despite his recognition it did
not give Klee any stability. It was very
sad to learn that Klee had to flee Ger-
many in 1933 and that the Nazis de-
stroyed much of his art work describ-
ing it as ‘degenerate’ art.
In 1935 Klee became seriously ill and
struggled with the serious symptoms
of scleroderma. his struggle with scle-
roderma is very obvious, in his works
from that time. There are many self-
portraits which show Klee coping with
the condition and although we were
dreading seeing some of Klee’s final
works (as we believed it would be
very sad) we were both in for a great
surprise. The final room at the exhibi-
tion starts by stating that Klee fought
his ‘illness’ and although he knew he
was very seriously ill did not want his
final paintings (in 1939 and 1940) re-
flecting his ill health and he produced
the most beautiful and vivid work. It
took all his strength to produce these
paintings when he felt so awful but, we
feel, they show Klee’s true character
and genius. His final painting was called
‘Vase of Flowers’ and shows the most
beautiful display of brightly coloured
flowers with huge blooms in a glass
vase. It was a wonderful end to a fasci-
nating display of imaginative art work
which at times was upsetting to see.
Klee died on the 29th of June 1940.
We would recommend this exhibition
to anyone who wishes to see how a
great artist overcame many hardships
and coped bravely with scleroderma
to produce some beautiful paintings.
By Tracey James
A Review of Paul Klee: Making Visible
16th October 2013 – March 2014, Tate Modern
“Yesterday, the 2nd of January 2014, I went with my mum to see the Paul Klee exhibition at
the Tate Modern in London. We were both at the Tate in the summer and when we learnt
that the Klee exhibition was going to be shown we were, from that moment, both very keen
to see it largely because of the connection with scleroderma – Klee had the condition. My
grandfather was diagnosed with scleroderma at the end of 2000 (the same time my mum
discovered she was having me) and through our research on Paul Klee we have discovered
many uncanny similarities between my granddad and Paul Klee which gave the trip a very
personal perspective.”
Florence James (aged 12)

Scleroderma News: Cover Story Page 5
1. Laugh every day:
Admit it, at
some po in t
we’ve all experi-
enced laughter
as the best medi-
cine. Patch Ad-
ams once said:
“ R e m e m b e r
laughing? Laugh-
ter enhances the
blood flow to the body’s extremities and
improves cardiovascular function. Laughter
releases endorphins and other natural
mood elevating and pain-killing chemicals,
improves the transfer of oxygen and nutri-
ents to internal organs. Laughter boosts
the immune system and helps the body
fight off disease, cancer cells as well as
viral, bacterial and other infections.”
2. Spend time with family:
Princess Diana once said: “Family is the
most important thing in the world.” In
2014 we should all take some time to let
our families know how much they are
loved and appreciated beyond words.
3. Appreciate your friends:
I have a close group of best friends who
have been by my side throughout the dark-
est and happiest points of life, they have
always been exceptional, and continue to
never stray more than a phone call away.
However, like so many, when it comes to
those further afield, I am guilty of leaving it
too long in between catch ups! Life moves
at an alarming pace, and that’s why in 2014
we should all make a conscious effort to
see our distant friends!
4. Have some YOU time!
Do something that’s all for you! Whether
it is going for a stroll in the park, or taking
ten minutes out of your day to have a qui-
et cup of tea and a read of a good book.
Find some time to be alone. I have found
that since I started dedicating some time
to be by myself, I am an altogether calmer
more composed person. Give it a try in
2014!
5. Do something unfamiliar!
In 2014 why not try mixing it up a little?
Try doing the opposite of what is expected
of you! I’m not suggesting we all hurtle out
of a plane or unite in a synchronised
bungee jump, (though if you’ve got it in
you – fabulous!) But why not attend an
event that you’ve previously thought might
not be your cup of tea – you may be sur-
prised!
6. Join a support group:
Scleroderma can be an extremely lonely
illness, but it doesn’t have to be. As sup-
portive as friends and family can be, and
with all the compassion in the world, no
one truly empathises with your scleroder-
ma journey like a fellow sufferer. In 2014,
why not embrace the opportunity to make
new friends through a Scleroderma sup-
port group? From pages on social media
sites like Facebook (search for the Sclero-
derma Society) to specialist health based
social networks (try inspire.com) there are
people out there, just like you, willing to
offer unprecedented support and advice,
free of charge! You can also see page XXX
to discover your nearest local group.
7. Get fit!
So, the clock
hasn’t finished
chiming twelve
and I’m already
subscribed to my local gym,
with the best
intent at the
forefront of my
mind, but deep
down knowing
I’ll have can-
celled it by February! Let’s make 2014 the
exception. Exercise is particularly im-
portant for people with Scleroderma: Stud-
ies have found that people who are physi-
cally fit have increased assertiveness, bet-
ter perception, and are able to make
sound decisions. They are more confident
in their ability to do things. Emotionally fit
people are more ‘stable’ and less troubled
by life's challenges and disappointments.
People who are fit are more independent,
have a better memory and more frequently
experience a positive mood. Needless to
say, they also have a better body image and
heightened feelings of well-being. In 2014
why not try a new exercise regime that
suits you and your needs?
8. Help a charity!
I will never forget my first fundraiser. The
gratification I felt knowing that I had helped
so many others, is a feeling that should be felt by all in 2014. Organising a fundraiser
is not as daunting as it might seem. There
are so many ways in which you can arrange
to collect money for your chosen charity,
from simple ‘whip rounds’ (we can provide
collection boxes) to events such as walks,
bike rides and marathons, sponsored beard
shaves, leg waxes and hair growing, to
quizzes, discos, auctions, raffles and fashion
shows. The possibilities are endless. If you
would like to support the Scleroderma
Society, in ANY way, please email fundrais-
9. Speak your mind!
Morrissey once
sang: “Don't
leave it all un-
said, somewhere
in the wasteland
of your head.”
Embrace your
ability to ex-
press yourself! If
you feel passion-
ate about something, anything, speak up!
Why not offer feedback? Leave a comment
on a post? Write a letter or keep a blog?
Finally, and perhaps most importantly.:
10. Say YES more:
There are so many reasons why we say no
in life, so many reasons why we shouldn’t
do things, and perhaps only one why we
should – life is too short.
2014 is your year! Make it count!
Love and best wishes,
Hollie
10 New Year’s Resolutions
For a Happier Scleroderma Life

My Scleroderma Journey:
‘We all shine on, like the moon,
and the stars, and the sun...’ John Lennon America is home to an estimated 80,000
to 100,000 sufferers of Systemic Sclero-
derma. Sounds like a relatively large
number huh? Not when you consider
that 314 million people call it home. A
reliable source informs me, that are less
than 0.03% people in America suffering
with Systemic forms of Scleroderma.
It’s impossible to say how many people
are battling Scleroderma globally. Per-
haps all we can say with any certainty is
that it is rare. Couple that with this:
How many people does one meet in a
lifetime? Studies have estimated the
number to be an average of 10,000 peo-
ple. What are the chances of one of
those people being a sufferer of Sclero-
derma? The number is getting smaller
right? Finally, consider this. What are the
chances of meeting a fellow sufferer of
Scleroderma, at home in Essex, in a
completely, unrelated social setting?
I didn’t believe in fate, until the day I met
Richard Aransibia. It was the spring of
2011 when I was introduced to Richard
through a mutual friend, who at the time
didn’t comprehend that we were suffer-
ers of the same illness. We were watch-
ing a wrestling match, when Richard
casually commented that he was due a
blood test the following day. I asked him
what i t was for and he sa id
‘methotrexate’ - you could have
knocked me over with a feather as I
realised we were both having our blood
monitored for the same reasons!
I learned that when he wasn’t working as
a Specialist at the Apple store, skate-
boarding, playing Frisbee (and as he put
it “generally running about doing things I
look a little too old to do,”) Richard, like
myself, was a patient at The Royal Free
Hospital in London. We were both un-
der the care of Professor Christopher
Denton. For years to come we would
meet up during hospital stays and visits,
to share a bottle of fizzy lime water and
have a chat. Richard explained to me
that he first noticed that something was-
n’t right when his knees became stiff
when crouching. Speaking to me in the
summer of 2013, he told me: “I thought
nothing of it as I skateboard, but soon
after I noticed swelling in my fingers at
work. I'm a pretty healthy guy so I ig-
nored it, thinking it would go away. The
first time I knew something was really up
was the gradual increase in fatigue when
moving around. In hindsight, this was
odd as my mobility and range of move-
ment was still completely intact.” Rich-
ard went to his GP who quickly read the
symptoms as Scleroderma due to the
fact he had seen a woman with it before,
over a decade prior! Richard was re-
ferred to a specialist who diagnosed
Systemic Diffused Sclerosis. Richard
explained “this meant Scleroderma that
was not localised. It affects multiple as-
pects of the body inside and out. Name-
ly, tightening of the skin, contractures of
the limbs, Raynauds, poor circulation,
myositis (inflammation of muscles
around internal organs) gut problems,
and weakness etc.” Over the course of
three years Richard visited his local hos-
pital in Basildon, and London’s Royal free
where he received a multitude of treat-
ments. He said: “Cyclophosphamide
helped, as did laxatives, but everything
else, like steroids, immunosuppressors
and antibiotics must simply manage scle-
ro as I didn’t feel any improvement after
taking them.”
Richard rapidly became a huge source of
strength to me. He was never more than
a text message away, even if I needed
someone to confide in at 4am! It was
during one of these late night heart-to-
hearts that I asked him what he thought
his future looked like, to which he re-
plied “Sclero is supposed to level out
and start to revert. That’s what I am
looking forward to.” Richard had tips to
help me cope. One night he told me:
“No matter how tired you get, don’t
give up, push through the tiredness.
Don’t rest in bed too much like I did.
Stretch your limbs and fingers a lot.
Have hot baths, wear gloves in cold
weather even if it’s not THAT cold.
Keep your chin up, even if things start to
get difficult…” I remember his reminder
that “you’re already fighting it so it
won’t hit as hard.”
Richard was famous for his (sometimes
unusual) sense of humour; “Every con-
versation I have, somewhere in there, is
Richard.” Said his friend, Tony Wells;
“The jokes we make and the way in
which we make them, at the very core
of it all, is Richard. His comical nature
was contagious and his timing
of punch-lines was impecca-
Scleroderma News: Inspire Feature Page 6

ble. He had the best sense of humour
we have ever come across. If you were
in a bad mood before seeing him, within
minutes you'd be smiling from ear to ear
and you'd forget why you were upset in
the first place.”
“Scleroderma is bloody *** isn’t it? If it
was a person I would have definitely
deleted them off Facebook,” Richard
complained to me one day. I couldn’t
help but smile. Richard had a way of
making serious problems feel less in-
tense.
In 2013 Richard grew increasingly frus-
trated with Scleroderma as it began to
limit his ability to drive his prized Audi
RS5. He once confided in me that a lack
of mobility prevented him getting to and
from the vehicle. He said: “Fatigue stops
me driving far. Weight loss means I need
a cushion. Contractures mean I am not
as nimble on the wheel. This is quite
frustrating, but when I can manage it,
driving is a huge release for me.” I’ve
never met someone as passionate about
cars as Richard. In the summer of 2013
he arranged a surprise for his mum, Ber-
nice, when he gave her BMW a makeo-
ver. Uploading the photographs to Face-
book, he wrote: ‘Expecting just refur-
bished wheels, Mum is kinda shocked to
see zenons, running boards, chrome
grille, a roof aerial and pearl effect vinyl
body wrap - And a Bluetooth hands-free
kit & iPhone charger. Result.’
Richard valued the people around him,
and once explained to me how his mum
was his main source of strength, he said:
“I guess the person who has made the
biggest difference, even though we get
under each other's toes a lot, is my
mum. She has been so helpful and I
should be grateful for that. She must be
as stressed as I am in a different way.”
He said: “My friends and family are very
supportive. Some of my friends are very
active in the scleroderma community
and that’s inspiring.”
But he was also, himself, extremely en-
couraging of his own friends. Upon
learning of my new role as Editor of
Scleroderma News, Richard expressed
an interest in sharing his personal story,
in order to spread scleroderma aware-
ness.
In October 2012, he once again showed
me his support when he discharged him-
self from a hospital stay to attend a char-
ity autograph auction that I had organ-
ised in aid of The Scleroderma Society. I
was shocked and delighted to see him
attend, and I will never forget his kind
words of appreciation. Sadly, and unbe-
known to so many, that was to be the
last time I saw my friend.
Richard died on the 30th October 2013,
exactly one month after his 26th birth-
day. His Mum, Bernice, was by his bed-
side at the Royal Free Hospital in Lon-
don.
Richard enjoyed reading and talking
about science. He found it fascinating. ,
whether it was strange facts, astounding
accomplishments or pondering the mys-
teries of the Universe. Tonight, if you
happen to look up at the night sky, like
Richard so often did, you may notice
that there’s one more star watching
over us.
Do you have a story to tell? Do you want to share it with others? Email: [email protected]
Scleroderma News: Inspire Feature Page 7
Richard’s friend, Tony Wells, said: “There will never be another like him and for that we are eternally
grateful. A truly remarkable human being with many good traits and few flaws. To say he influenced all
of us is an understatement. We've never met anyone who loved life as much as he did, and we don't
think Richard realized it himself. Music, fashion, cars, sport, and films - He enjoyed all of them. He
loved all kinds of food and constantly immersed himself in the ever evolving world of technology.
Thinking back, it's hard to find anything he didn't have an interest in. We've barely begun to scratch the
surface of this incredible person, how much he meant to us, and how hollow life will be without him
here to share it. He'll be in our hearts through the good times and the bad, and that out of the 107.6
billion people to have lived, we couldn't have picked a better man to have as our best friend.”
“He used to call me Gambit and he was Wizard.” Laughs his friend Rikki Piercy: “I met Richard out
skating. We couldn't have been much older than 15, he was so healthy and a great skate border. He
was always so funny and his laugh was infectious! Everyone who knew or had met Richard always com-
mented on how full of life he was and you could never say a bad thing about him. You could always find
something in common with him. He would always beat me in a running race. He would always show
me new music he thought I would like too. We would watch films on his big high definition TV and try
to spot mistakes and silly things like that. He could take something terrible and turn it in to something
comical. He was the greatest friend anyone could ask for!”

Start 2014 in style and snap up one of
our 13 places for this perfect ride!
Follow in the footsteps of our 2013
riders Peter Marsh, Amy McCallin and
Martin Billman who raised a whopping
£2636.99! The Prudential Ride London
100 follows a route made famous by
the world’s best cyclists at the London
2012 Olympics. Start in Queen Eliza-
beth Olympic Park, then follow a 100
mile route on closed roads through
the capital and into Surrey’s stunning
countryside, finishing at The Mall in
central London. This is a truly spectac-
ular event to be involved in. In the
next issue we will read about Peter
Marsh’s (right) experience of the ride.
Thank You...
Since our last newsletter in No-
vember our members and sup-
porters have been supporting
us through a variety of events.
An extra special thank you to:
Paul Robins and team who held
a Golf Day in Dubai raising a
huge £6,900.
Natalie for throwing herself out
of a plane in the name of charity.
Becky and colleagues for fund-
raising through a book sale and
office collection.
De Ruddick and the Ladies at
Workington Golf Club for rais-
ing £ 785.
Claire Erte for running the Car-
diff Half Marathon and raising
over £1000.
(Right) Ian Drury and team for
hosting their annual Brian Nor-
ris Charity Dinner.
If you are fundraising on our be-
half then please let us know so
we can assist and credit you for
supporting our vital work: fund-
or call us on: 020 7000 1925
Scleroderma News: Fundraising Page 8
Fundraising Stars: Prudential Ride London 100
“I am close to finishing a
whole year without having a
shave or a haircut all in aid
of raising funds for the Scle-
roderma Society. My moth-
er Wendy was diagnosed
with the disease several
years ago and, along with
various other members of
my family and friends was
completely unaware that
such a condition existed, so
taking part in this fund rais-
er was also to raise aware-
ness. You may not know
mum personally but she is
the heart of our family, and
has us all round twice a
week to cook us a family
meal (usually about 12 of
us!!!) She would do anything
for anyone and always puts
others before herself.” Paul
plans to shave at a New
Year’s Eve party where fur-
ther money will be raised
via raffles and games. Please
help Paul to raise as much
as possible:
www.justgiving.com/
Paul-Le-Grave,
Hair Today, Gone Tomorrow

“Hi readers. My name is
Becky Pearson and I am a
Work Experience Officer at
Bradford Metropolitan Dis-
trict Council. I am also a
member of the Education,
Employment & Enterprise
Activity Hub.
In 2013, 4 col-
leagues and I formed an Ac-
tivity Hub for our overall
team. On a monthly basis
we get together to arrange
team activities and look at
ideas where we can raise
money for various charities.
We try to do a team build-
ing fundraiser every term.
Earlier this year our colleague
Janet Knowles and her family were
going through a terrible time with her
sister Dianne’s illness. Sadly Dianne
lost her life to Scleroderma. Janet’s
family arranged a number of fund rais-
ing events including The Three Peaks
Challenge and I asked Janet if there
was anything that we could do to help
raise some more funds for the charity
and if we could do our next fundraising
day in memory of Dianne.
We planned a date after the
summer school holidays and as it fell
around Halloween we decided to give
it a Halloween theme so we could
dress up. I contacted Susie at the Scle-
roderma Society to inform her that we
would be raising money and also to see
if she would be able to send me logos
for us to use for our poster that we
were designing. Susie was a great help
and it was lovely that she knew from
the basic information I had put in my
email who we were raising money for
and how the family had already raised
money doing the three peaks chal-
lenge. Susie arranged sending merchan-
dise for us to use to raise awareness
including pens, pin badges and wrist
bands which was so generous.
We asked for people to do-
nate cakes so we could sell them
across the 5 floors in our building.
Vicky, who is also a member of the
activity hub arranged for her partner
to put a Halloween Quiz together to
continue the theme. We had also ar-
ranged for the Book People to come
into our extension area at the end of
September to sell books and 10% of
the sales was donated to a charity of
our choice so on this occa-
sion it was the Scleroderma
Society.
October 25th ar-
rived and several of us came
in fancy dress. We had loads
of cakes donated by members
of our team and also Janet’s
family. At 10am, dressed at
witches, cats, wizards and
devils we tackled a couple of
floors between us selling
cakes, badges and wrist bands
and raising the awareness of
the charity. We even had an
18 month old witch selling
cakes with us! A few others
went round selling quiz sheets and
giving pens with these and the quiz
proved quite popular. We announced a
winner at 1pm with 18/20 and they
won a tin of chocolates that had been
kindly donated.
It was amazing when we start-
ed to count up the money people had
generously donated and we were so
shocked when we got the final figure
of £517.33 as this beats any amount
we have raised within our departments
in the past year. I think when people
are raising money for a charity that
touches someone’s heart and has af-
fected their family directly, people are
definitely more generous and it’s great
that we have been able to raise some
more awareness for the Scleroderma
Society.”
Celebrating Fundraising Success
Scleroderma News: Fundraising Page 9
If you would like to see your event covered in Scleroderma News, please email Hollie, [email protected]
Stamp Collecting Pulls in Pounds
Jason Burgh has once again taken on a challenge on behalf of
the Scleroderma Society, but this time it involves stamps.
Jason has been collecting stamps within his local community
and has gained huge support with his current total reaching
8,500 stamps. Jason’s collection has not only raised aware-
ness of scleroderma and the society but will bring in much
needed funds. Thank you Jason.
Going Dry for Scleroderma
We all like a nice glass of wine or something stronger on
a Friday but Chris Jones has gone dry this January. He is
getting sponsored to abstain from alcohol for the whole
month. Chris’s total has reached £250 but he has since
pledged that if he reaches £500 he won’t touch a single
drop in February either. Help to keep Chris dry: https://
www.justgiving.com/Chris-Jones91

Meet our Heroes:
Lianne Robertson and Jamie Forman “Jamie and I are taking on this challenge together and are really looking forward to it.
I’m an actor and events manager and Jamie works as a maintenance technician/Janitor in
a public school. We live in Glasgow and moved here together after meeting in our
hometown of Fraserburgh in the far north east of Scotland. I ran the London Marathon
in 2011 and since then Jamie has also taken a keen interest in running. I have always
told Jamie he must run the London Marathon at some point in life. Over the last few
years Jamie has done a few half marathons but this will be his first marathon. We chose
Scleroderma as we had a family member who suffered from an aggressive form and
unfortunately lost her battle with it. We hope that our funds can go towards more
research to find better treatments and even a cure.” Support Lianne and Jamie to reach
their target: uk.virginmoneygiving.com/LianneRobertson
The London Marathon 2014
Gareth Clifton “Since completing the London Marathon in 2011, I have secretly always wanted to do it
again and I was fortunate to be offered a place. I will be drawing on all my experiences of
previous marathons. This is a charity which is close to my heart especially as my mum suf-
fers from the condition. Having run for the charity previously and raised funds, I wanted to
do it again. I want to raise awareness and much needed donations to help the future treat-
ment.” Support Gareth on his London Marathon journey: www.justgiving.com/run-GC-run
Nicola Bowerman “I live in Bedfordshire with my husband Nick and my two children, Thomas, aged 8 and Sophie
aged 6. I never used to enjoy running. I think my dislike goes back to school P.E lessons where we
were made to run cross country in the freezing cold! However in 2012 I set myself a New Year’s
resolution to do something I struggled with and decided to take up running. I joined a local run-
ning club as I knew I would struggle to do this on my own and I have never looked back. I was
totally surprised to find out how much I absolutely love running and really wished I had started
running earlier. I was fortunate enough to gain a ballot place this year for the London Marathon
and I knew straight away I wanted to run in memory of my beloved dad (Bill Storey) for the Scle-
roderma Society. My dad was diagnosed in August 1998 with a very aggressive form of scleroder-
ma and was only given 3 months to live. Dame Black and Professor Denton gave my dad an op-
portunity to be part of a clinical trial and receive a stem cell transplant. His condition improved
and he was on top of his illness but unfortunately 7 years later he developed pulmonary hyper-
tension and died in December 2004. My dad was a wonderful man and I feel absolutely privileged
to call him my dad. He would be absolutely thrilled that I am raising money for the society and
giving something back for all the help and support they gave him and my family. As everyone
knows scleroderma is very rare, so I was completely shocked when one of my closest friends was
diagnosed with the disease last year. I am also running and raising funds for Katie Knight. I will
cross that finish line with the memory of my dad and celebrate with some bubbly with Katie!” If
you would like to sponsor me, my just giving website is www.justgiving.com/Nicola-Bowerman2
Scleroderma News: Fundraising Page 10

Scleroderma News: Fundraising Page 11
Fancy Getting Involved? Want to make a positive change in 2014? There are plenty of
ways you can help The Scleroderma Society:
Innovation Board The Innovation Board will discuss ideas
and ways in order to continue devel-
opment of the society. We will have
meetings both in person and via online
sources so even if you aren’t able to
travel please do get in touch if this
sounds like an opportunity you would
like to be a part of. You don’t have to
be a radical thinker to be on this
board. We are looking for individuals
who wish to see the society move for-
ward and progress and want to be a
part of that.
Newsletter Packing We are looking for volunteers who
can help us four times a year to pack-
age up our newsletters to be sent out
to our members. If you are able to
spare a day every three months or just
one day throughout the year then we
would love to have you on our team.
Live near London?
Love to make noise? Well this is perfect for you! We are
looking for volunteers to come down
and join us at the London Marathon on
13th April 2014 to cheer on our run-
ners! This year we have nine fundrais-
ers running and would love to give
them as much support as possible. If
you would like to support our fund-
raisers but don’t love to make noise
then we would love volunteers to hand
out goodie bags on our stall at the
finish line and raise awareness for the
society.
Refer a Friend for 2014 Included in this copy of Scleroderma
News is a ‘Join Us’ form. Why not pass
this form to a friend, and encourage
them to join the Scleroderma Society?
It’s only £5 a year and in return we’ll
send 4 copies of Scleroderma News!
Buddy/Befriender Would you like a scleroderma buddy?
Someone you can phone or have a cup
of tea with or even someone to help
you with your shopping. If you would
like to develop a friendship like this
then please get in touch so we can find
a buddy for you. Become a buddy! We
are always looking for individuals who
are happy to be added to our database
as a buddy. When another individual
seeks a buddy in your area we will get
in touch with you and support you in
your role.
If you are interested in any of our
volunteer opportunities please
contact Amy Baker: amybaker@
sclerodermasociety.co.uk or call
020 7000 1925 for a chat…
Fundraiser Stories Online: We
would love to feature all our fund-
raisers in our newsletter but un-
fortunately there just isn’t enough
space as we have so many won-
derful people fundraising for us.
So you can now read about our
fundraisers on our website under
Fundraiser Stories. Every time
you receive a newsletter from us
our Fundraiser Stories will be up-
dated so you can see our most
current fundraisers.
Could Your Employer
Help Fight Scleroderma?
Every year we are looking to increase awareness and raise
even more money to fund our vital work. Could your work help us this year? Nominate us for charity of the
year or hold a fundraiser within your work place to help raise awareness and funds. If you would like to know
more about how your workplace can support us email: [email protected]
Hi readers! Hollie here! I’m recruiting researchers,
writers, bloggers, photographers, illustrators, graphic
designers and more to get involved in producing Scle-
roderma News! Experience or no experience, if you
have an interest in print media and would like to get
your work published please get in touch! I’d love to
hear from you! Email [email protected]

Top Tips: Help is at Hand!
Scleroderma News: Top Tips Page 12
Below: Hot tip ! These little purses make it easy to find your change
especially if your hands are not working properly! - Helena
Trustee Helena Rozga shares her top tips for coping with Raynaud’s!
Left: Helena’s red hot tip! Always carry hand warmers! The Hot
Rox is rechargeable, Helena got hers from Amazon:
www.amazon.co.uk/hotrox+hand+warmers , but you can also find
them elsewhere on the internet, including at www.the hotrox.co.uk.
If you have a Costco near you then they are the cheapest place to
pick up Little Hotties, costing around £11 for 40 pairs!
“Does limited hand functionality and
Raynaud’s make it difficult for you
to take your cards from your wallet
or purse? My hot tip is punch a
whole in the cards away from the
magnetic strip or chip/signature area
in one corner and put them on a
key ring! It’s easy for you to single
out the card you want and pass the
key fob to the sales assistant so they
can be scanned while still on the
ring! Sales assistants smile and tell
me it’s “very clever” of course they
don’t know it’s to stop the embar-
rassment of my fumbling around in
my wallet!” - Helena Rozga

“I recommend
pain manage-
ment, try read-
ing or Googling
“Spoon Theo-
ry.” Kim Tat-
terfield
“I find it helps to put a fleece blanket
in the dryer, rolling up in it will stop a
Raynauds attack immediately.” - Lin-
da Ferri
“I use Little Hotties Hand warmers
and toe warmers. I also wear ther-
mals under my clothes.” - Teresa
LeBleu Rowland
“I refuse to be
beaten by stairs,
and use this
'mountaineering'
session as my
way of creaking
the body back
into some sort
of action in the morning” - Sandra
Branch –Burbridge
“We are what we think! I change my
sad thoughts to happy thoughts and it
does make a difference in my attitude
and everybody around me. It is not
easy to do when our bodies are in
pain and suffering but if we can make
ourselves laugh, it does work mira-
cles on our attitudes.” - Ann Have-
lock
“Mittens not gloves, and always carry
the instant heat packs.” - Diane
Begley
“A warm fuzzy robe. If I keep my
core very warm, my hands and feet
don't have Raynaud's attacks as often
or as bad. Stocking hats help a lot
too. I may look silly but I am saving
my fingers and toes!” - Polly Lay
“For an inexpen-
sive quick fix, cut
the top bands off
old socks, cut a
small hole about
1/2 down from
the top (for the
thumb to go
through) and you can wear as a hand/
wrist warmer. You can hem or use
stitch glue to keep ends from raveling
depending on the material.” - Elie
Salas
“I try to walk on the treadmill at least
10 minutes a day, especially if the
weather is too cold to go out to
walk.” – Michele Huntington
“I have just bought a down duvet,
UGGs are a must, as are sheep skin
mittens, why not try an electric un-
der blanket too?” – Liz Fitzpatrick
Leadbetter
“I work out on
my ab-doer twist,
it gives me energy
and stamina. Mu-
sic also gets me
moving!” - Mar-
garet Cole
“I love my heat lamp in my bathroom.
I can get out of a warm shower and
stay warm, which helps me so much...
I make sure my clothes have been in
the dryer and start the day warm,
then it's easier for me to stay warm.
Hot hands and feet warmers. Mittens
work better than gloves for me... and
good boots!” - Krystal Hovater
“I have 3 mischievous male dogs that
keep me alert and force me to go
outside to see what they're up to. I
am the alpha to my pack, and when I
step outside they are 'pretend' biting
into the air at each other's faces. Be-
cause my hands hurt they know that
when I put on my leather garden
gloves, Mommy is going to play with
them!” - Maria Saenz Leija
“Do something
for other peo-
ple! I find if I set
a goal of doing
something for
someone else it
takes away from
the bad of Scle-
roderma and I
am able to then make it through a
day DOING instead of letting it keep
me down and out.” - Karen Cyrus
“I always make a list of things I need
to do (brain fog) and mark things in
their priority. Anything not urgent
can wait to be tackled on a good or
better day.” – Caroline Adams
Reader’s Top Tips for improving
your Scleroderma Life!
Scleroderma News: Reader’s Top Tips Page 13
DO YOU HAVE A TOP TIP YOU WOULD LIKE TO SHARE? Share your top tips with readers of
Scleroderma News and lets all help each other! Email: [email protected]

LA Stone
My name is Georgia Davis and I have
been a fully qualified beauty therapist
since 1990.
It was during a placement in Switzerland
that I was shown and used LaStone Hot
& Cold stone massages. This highly effec-
tive way of massaging was so successful
with the skiers tired legs and bodies,
removing their lactic acid and preventing
the onset of muscle soreness.
I offer my clients a variety of
treatments, delivering a deeply
penetrating massage which ef-
fects chemical, physical and spir-
itual healing whilst bringing bal-
ance to mind, body and soul.
My first introduction to Sclero-
derma was though treating Hele-
na. After a full health assessment
I was able to tailor make a treat-
ment plan of varying tempera-
tures to enable Helena's body to
heal and re-energise itself with
out heavy or deep massage movements.
LaStone is a Geo-Thermal treatment,
where the circulatory system is stimulat-
ed by using hot and cold stones to enable
the body to do the work from the inside.
The hot Basalt stones are safely heated in
a controlled temperature unit whilst the
cold marble stones are placed on ice.
Learning about Scleroderma and the ef-
fects temperature can have on the body
especially if you’re also dealing with Ray-
naud's, I always keep the hands and feet
cocooned in warmth whilst using the
cold prescriptively on areas where there
is extra tension and stubborn aches and
pains. I also offer a alternative LaStone
treatment called CastleBuilding. Using
the stones to wrap up and cocoon the
body in an non- invasive therapy with the
client still fully clothed. This is excellent
for tension, stress and anxiety which is
often overlooked in today's world.
By Helena Rozga
“I have always tried to keep moving
throughout the various traumatic
stages of Scleroderma, ranging from
crawling up the stairs on all fours to
now doing Pilates and swimming. I
have always been determined not to
let Scleroderma get the better of me
and as you all know this is sometimes
really difficult. The things I have done
to maintain circulation and flexibility
have varied along with the degree of
involvement and pain.:
First off, I have always tried to mas-
sage my hands and feet. As soon as I
could tolerate body contact, I found
a lovely lady, Gill, at Bodykind, who
did the most wonderful aromathera-
py body massage and reflexology.
This was really beneficial along with
the wax baths and exercises for my
hands. I have progressed now to LA
stone massage, which eased my
aches and pains and helped to repair
my troublesome shoulder. I have
asked Georgia, my therapist to ex-
plain the LA stone technique to you.
Even when in hospital, I was able to
continue with the massage through
the wonderful Keith Hunt and team
of volunteers at the Royal Free.
When I was in Miami before my ill-
ness, I was in an hotel with a roof
top swimming pool. I thought it quite
bizarre to see people and particularly
ladies in full make up drinking cock-
tails in the pool and chatting. When
they were not drinking, they were
power striding up and down the
length of the pool. Obviously proper
swimming was uncool! I remembered
this years later and my second ven-
ture was to join a local pool. I just
walked up and down, hardly a power
walk but nonetheless the water was
supporting my movement and I was
able to exercise.
I had to deal with the Raynaud’s diffi-
culties but it worked for me. Eventu-
ally I was able to learn to swim again
which took time and discomfort as
my limbs were so constricted but I
am sure I am now in a much better
place because of it.
My posture and balance was affected
by the Scleroderma and friends kept
telling me to try Pilates but I was
afraid and embarrassed as I couldn’t
get down on the floor and my hands
do not flatten. I am sure you recog-
nise the difficulties here without me
writing about it. So my third venture
was to find Claire, a professional
Pilate’s teacher and amazingly I have
experienced all the benefits of Stott
Pilates, which I have asked Claire to
tell you about (on the next page.)
Friends tell me my posture is more
aligned and I am much more flexible.
Personally, if you give Pilates a go,
dependant on your level of stamina
and flexibility, it is better to start
with one to one tuition. Most places
do a free introductory session to
explain the basics and to see if it is
for you.”
Fixed or Flexible?
Scleroderma News: Reader’s Top Tips Page 14

Top Tips to Keep Moving: Pilates
Scleroderma News: Top Tips Page 15
By Clair Cornish, Manager of
Prime Pilates in Rayleigh, Essex.
“I was first introduced to Pilates after
I sustained a knee injury while train-
ing to become a professional dancer.
I was advised to undertake a course
of Pilates as part of a rehabilitation
programme, after undergoing knee
surgery which then allowed me to
complete my training and professional
dance career. After seeing such great
results through my own experience
and with my dance career coming to
an end I decided to train and become
a fully certified STOTT PILATES in-
structor.
I have worked with a diverse range of
clients and have helped them achieve
fantastic results: for example those
with injuries, postural problems, mul-
tiple sclerosis, pre and post natal cli-
ents and after meeting Helena, Scle-
roderma.
The STOTT PILATES method is a
contemporary approach to the origi-
nal exercise method pioneered by
the late Joseph Pilates. Co founders
Moira and Lindsay Merrithew, along
with a team of physical therapists,
sports medicine and fitness profes-
sionals have come together to refine
the STOTT PILATES method of exer-
cise, making it one of the safest and
effective method available. It is used
by rehab and prenatal clients, ath-
letes, celebrities and everyone in be-
tween.
Pilates is low impact exercise that is
designed to restore the neutral
curves of the spine and rebalance the
muscles around the joints. Exercises
can be modified to cater to many
different body types and abilities mak-
ing it applicable to everyday life.
The benefits of Pilates:
Increased strength without
unwanted bulk
Increased core strength, stabil-
ity and mobility
Improved posture and fitness
levels which may help prevent
injury
Greater ease of movement
Heightened body awareness
Low impact on the joints
Enhanced balance, coordina-
tion and circulation
Improved athletic perfor-
mance
If you are a beginner it may be best
to start off with a one to one session
and to always train with a qualified
instructor to ensure that you are
doing the movements correctly. An
experienced instructor will be able to
modify the exercises to accommo-
date your limitations, continually chal-
lenging your range and monitoring
your improvement.
People always ask what results they
should expect. Pilates will increase
your strength, flexibility, mobility,
balance and body awareness as well
as decreasing back pain and other
general aches and pains.
Stott Pilates can be done on both
equipment and on a mat. Most of the
- exercises are floor work, some-
times using small equipment such as
balls, fitness circles, roam rollers, flex
bands and pillows.
Pilates equipment is different. There
are several different pieces of equip-
ment that might be used in a lesson.
Some of the equipment uses spring
tension which doesn't always make
exercises harder as you would think
but actually helps you to isolate cer-
tain muscles.
Equipment found in a Pilates studio:
The reformer
Cadillac
Stability chair
Arc barrel
Spine corrector
Leader barrel
Regardless of age or fitness level, Pila-
tes is an ideal complement to any
cardiovascular exercise, athletic train-
ing or rehabilitation.
Scleroderma News: Scientific & Medical Page 16
DOC SPOT Chris Denton is a Professor in the Centre for Rheumatology at the Royal Free Hospital in London and
runs the Scleroderma Clinic. He also has a major research programme that spans both clinical and
laboratory trials related to scleroderma.
I have Raynaud's and scleroderma and
have been on the same medication
for some time. Recently, I have de-
veloped very painful mouth ulcers and
wonder if there is a connection? I
have reread all the patient infor-
mation leaflets but I can't find any
reference to mouth ulcers.
Mouth ulcers are common but can
occur as a side effect of some medica-
tions given for scleroderma such as
methotrexate (and other agents). I
would recommend discussing this
with your doctor - you may need a
blood test. Sometimes mouth ul-
cers due to methotrexate can be re-
duced by taking folic acid supple-
ments. However mouth ulcers can
occur for other reasons or as part of
an underlying connective tissue dis-
ease.
My tongue swells up and goes blue at
times and I find it difficult to talk. It
feels like my tongue is shrinking. Can
Raynaud's affect the tongue?
It is certainly possible for the
tongue to be affected and this seems
to occur in both primary Raynaud’s
or in association with connective tis-
sue disease. Blood vessel spasm in
Raynaud’s can involve any of the ves-
sels that respond to or regulate tem-
perature and this includes the tongue
(it is an important cooling device in
dogs!) Raynaud's therapies may
improve these symptoms.
The tops of my hands are very itchy
and get tiny hard spots, which are not
visible but I can feel them, also the
tops of my feet, my big toe and
around my ankles are itchy too - no
spots but sometimes it looks like I
have a nettle rash on the top of my
toe and on the backs of my wrists.
The itching is always on both sides at
the same time. Any ideas please?
This symptom sounds like urticaria,
which is the result of release of hista-
mine and other factors in the skin - it
can be provoked by temperature
change, scratching or sometimes in
association with a poor circulation. It
can be helped by anti-histamine
creams or tablets (although these may
cause drowsiness). Some connective
tissue diseases are associated with
uticaria and so if this is a severe and
persistent problem you should con-
sult your doctor as specialist derma-
tology or rheumatology referral might
be appropriate.
I have read that one should have an
ANA (anti nuclear antibody) blood
test if Raynaud’s becomes severe or if
you develop Raynaud’s after the age
of 40. If this comes back positive does
it always that you have scleroderma
or can you have positive ANA and
not develop scleroderma?
Most patients with Raynaud’s phe-
nomenon (RP) have “primary RP”
that is not associated with any under-
lying disease, some patients do devel-
op a related condition such as sclero-
derma or another rheumatic or con-
nective tissue disease (secondary RP)
some cases of RP have positive ANA
and this is associated with increased
chance of developing an associated
disease over subsequent years, but
many patients do not develop sclero-
derma. Research studies suggest only
about 10% of such cases progress to
scleroderma.
I have just undergone my first
course of Iloprost and wonder how
long it takes before it kicks in?
lloprost is a synthetic form of the
natural substance prostacyclin that
opens up blood vessels and improves
circulation. There may be some im-
mediate benefit from Iloprost during
infusion but the maximum effect
seems to occur around 6 weeks after
treatment is complete. This is likely
to reflect the beneficial effect on
blood vessels and their lining cells
(the endothelium).
I saw a Rheumatologist recently about
my possible Raynaud’s, dry eyes, and
dry mouth. I have difficulty in swal-
lowing. He has referred me to a Gas-
troenterologist and an ENT specialist
about my swallowing problems. He
has also suggested to my GP that he
should put me on drug called Thy-
moxamine for my peripheral circula-
tion. Is this a common medication for
Raynaud’s?
Thymoxamine is one of a number of
drugs that can reduce blood vessel
spasm. It was originally developed for
high blood pressure and is a class of
drugs called “alpha adrenergic block-
ers” that block some of the effects of
adrenaline. It is sometimes used in
Raynaud’s although other agents such
as Nifedipine or losartan are also pre-
scribed. It is often necessary to try
several different medications to find
one that works and does not cause
significant side –effects. Many of the
common side effects relate to lower-
ing of blood pressure.
This article has been produced in association with The Raynaud’s & Scleroderma Association.

Scleroderma News: Scientific & Medical Page 17
This is the story of Maurice Raynaud - the
man who put the ‘ R’ in CREST
As someone who has scleroderma, or
someone who knows a person with scle-
roderma, you’ll be aware that nearly all
those with systemic sclerosis can have
Raynaud’s. Sometimes the symptoms of
Raynaud’s can pre-date the diagnosis of
scleroderma by some years. When the
onset of Raynaud’s is swift and severe –
particularly but not exclusively in women
in their 30s or 40s – it is worth further
investigation by a rheumatologist. Where
it is found to be associated with an auto-
immune disease – particularly scleroder-
ma – the Raynaud’s is said to be
‘secondary’. Where no rheumatic auto-
immune disease is detected, it is generally
‘primary’ Raynaud’s – something which up
to 10 million people are estimated to have
in the UK alone.
Maurice Raynaud is said to have
‘discovered’ the medical condition that
bears his name, although the issue which
has and continues to face thousands of
people – affecting blood flow to the
body’s extremities – has existed through-
out history. Raynaud's is today called a
‘phenomenon’ rather than ‘disease’ as it
was in the 19th century and is named after
Dr Maurice Raynaud who documented
the symptoms for modern medicine. The
son of a university professor, August Ga-
briel Maurice Raynaud was born in 1834
and started his medical studies at the
University of Paris helped by his uncle,
Vernois, a well known Paris physician. He
obtained his medical doctorate in 1862
and a PhD in 1863 and although he held
privileges working in various Paris hospi-
tals, he was never appointed to a senior
position.
The story has it that in the late 1850s, the
presentation of a 27 year old woman
posed a conundrum to the medics of the
day. The fingers of her hands repeatedly
became pale and cold. Over the next few
weeks the tips of some of her fingers
became black and shriveled and these
‘cold’ episodes were accompanied by pain
and great discomfort.
The doctor who attended her was a
young man called Maurice Raynaud. He
was perplexed at the situation – faced with a patient who had spontaneously
developed gangrene of her fingers with no
apparent cause. The young woman ap-
peared healthy, with a good pulse in her
wrists that suggested a normal supply of
blood to her hands, yet her fingers looked
starved of blood and the tips of her fin-
gers had become gangrenous. Maurice
Raynaud’s 19th century medical teaching
told him that such gangrene was due to
either blockage of a main artery in a limb,
diabetes, typhoid, or poisoning by a fungus
associated with mouldy rye. None of
these were relevant to his patient and her
medical history showed that colour
changes in her digits seemed associated
only with cold temperatures and stress.
He deduced that the colour changes were
due to some sort of intermittent block-
age of the blood supply and that the
spontaneous gangrene of her fingertips
was in some way connected.
Over the next few years Raynaud saw
patients with similar symptoms and
shared his observations with colleagues.
Subsequently he recorded 25 patients whose fingers, toes, or sometimes the
face and ears changed colour in the cold
in a similar manner, whilst some also de-
veloped areas of gangrene on the affected
parts. Raynaud was baffled by the cause of
the phenomenon whose symptoms he’d
recorded which included colour changes
of the extremities and the appearance of
‘flat’ nails.
A breakthrough came when Raynaud
made a connection with the work his
contemporary, Claude Bernard, was un-
dertaking. Famous for his empirical ap-
proach to medicine, Bernard’s work in-
cluded experimentation on the body’s
blood flow. He had discovered that arter-
ies - the vessels carrying bright red blood
all around the body - are supplied by
nerves, which, when activated, cause the
arteries to constrict and hence carry less
blood. The nerves in question were called
the sympathetic nerves. Here at last was
Raynaud's answer! Raynaud believed that
these ‘sympathetic nerves’ must be over-
active, making the arteries so narrow that
not enough blood reached the extremities
to keep them alive. When the condition is
severe enough gangrene develops but in
its milder form the affected areas inter-
mittently turn white or blue and finally
red when the blood eventually returns. In
essence, the fingers and anywhere else
affected were being strangled or asphyxi-
ated by a lack of blood! Raynaud pub-
lished his thoughts in the form of a thesis
in 1862 called, "De I'asphyxie locale et de
la gangrene syrnetrique des extremites"
translated as "On Local Asphyxia and Symmetrical Gangrene of the Extremi-
ties".
Maurice Raynaud died at the age of only
47 in 1881 of a heart attack, having suf-
fered from cardiac disease in the preced-
ing years. He had become respected and
recognised as an excellent teacher, clini-
cian, researcher and writer.
When Raynaud discovered the condition
that would later carry his name, preven-
tion and treatment was little understood. However, the one recommendation that
is still relevant today is that patients
should try to stay warm and avoid con-
suming anything that might constrict their
blood vessels.
Today, so much more is now known
about Raynaud’s than in the 19th century –
it’s association with scleroderma and how
to manage moderate and severe cases.
Yet, awareness of its significance beyond ‘
that cold weather condition’ is still some-
thing the general population and some
clinicians need to consider seriously tak-
ing heed of the severity of symptoms and
investigating potential underlying causes.
Gloves On Please!
This February the Scleroderma Society
are getting their gloves on in support of
the RSA Raynaud’s awareness month

Scleroderma News: Scientific & Medical Page 18
By Frank van den Hoogen & Jaap
Fransen
Systemic sclerosis can be recognized
by an expert rather easily when the
disease is fully developed. But the
course of the disease can be different
between patients, and symptoms may
vary significantly especially in the be-
ginning of the disease. This makes it
sometimes difficult to establish a diag-
nosis of systemic sclerosis and it of-
ten depends on the expertise of the
physician.
The cause of systemic sclerosis is still
unknown, and there still is no therapy
that can cure the disease. Therefore
research is needed and to perform
research the participation of patients
is mandatory. In order to secure that
in studies of systemic sclerosis all
included patients indeed have system-
ic sclerosis, we need classification
criteria. Classification criteria are not
the same as diagnostic criteria, but
they should be very close to the way
physicians diagnose systemic sclerosis
in daily practice. To successfully apply
results from studies to patients in
practice, it is of course most relevant
that patients in studies resemble pa-
tients in practice.
In 1980, the American College of
Rheumatology developed criteria for
systemic sclerosis, the so called
“preliminary ACR-criteria for the
classification of systemic sclerosis”.
At that time, not much was known
about autoantibodies that are associ-
ated with systemic sclerosis, and we
did not know about the significance
of nailfold capillary changes. As a con-
sequence, autoantibodies and nailfold
capillary changes were not included in
the preliminary ACR-classification
criteria. Moreover, mostly patients
with definite and diffuse cutaneous
disease were included in the develop-
ment of these criteria.
Later, it appeared that
many patients with a
diagnosis of early or
limited cutaneous dis-
ease were not classified
as systemic sclerosis and
could not be included in
studies.
So it was time to devel-
op new classification
criteria. The European
League against Rheuma-
tism (EULAR) and the
American College of
Rheumatology (ACR)
assigned a task force
with the main goal to
develop new classification criteria for
systemic sclerosis that would per-
form better than the preliminary
ACR criteria. The task force consist-
ed of 4 Europeans (Frank van den
Hoogen, Jaap Fransen, Alan Tyndall,
Marco MatucciCerenic), and 4
Northern Americans (Janet Pope,
Dinesh Khanna, Sindhu Johnson, Mur-
ray Baron). The task force started in
2008. First we asked physicians who
treat many patients with systemic
sclerosis which symptoms or features
they thought could be attributed to
this disease. The results was an ex-
tensive list of 168 features, varying
form arthralgias and fatigue to thick-
ened skin, digital ulcers and autoanti-
bodies.
Next we started to reduce the num-
ber of features by having experts
rating their appropriateness for clas-
sifying systemic sclerosis. The fea-
tures and their combination was test-
ed with an expert panel. We exam-
ined in a specially collected database
with scleroderma patients and sclero-
derma-like patients what would hap-
pen if we omitted one feature and
how the features performed. All this
was done with the help of many scle-
roderma experts from Europe and
Northern America.
We finally succeeded to develop clas-
sification criteria that perform better
than the 1980 preliminary ACR crite-
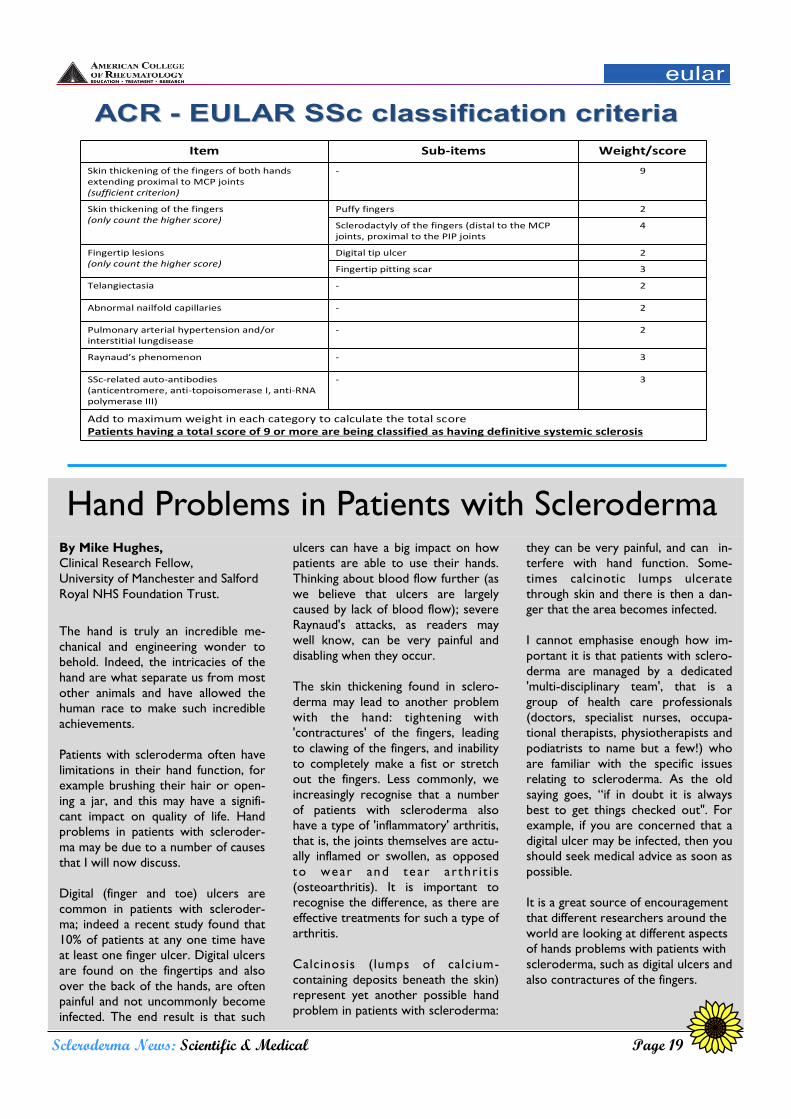
ria. The new ACR-EULAR classifica-
tion criteria are shown in the table
(shown across page) as well as to
whom the classification criteria
should be applied and to whom they
should not be applied.
It is of importance to know, that pa-
tients who fulfill the classification
criteria almost always will have sys-
temic sclerosis, but that patients who
not fulfill these criteria still may have
systemic sclerosis. The main reason is
that not all symptoms ascribed to
systemic sclerosis, could be included
in the classification criteria. The ex-
pertise of the physician will remain
necessary in these cases to establish a
diagnosis.
READ MORE::
ACR: www.rheumatology.org
EULAR: www.eular.org
ACR-EULAR NEWS: Classification
Criteria for Systemic Sclerosis
By Mike Hughes,
Clinical Research Fellow,
University of Manchester and Salford
Royal NHS Foundation Trust.
The hand is truly an incredible me-
chanical and engineering wonder to
behold. Indeed, the intricacies of the
hand are what separate us from most
other animals and have allowed the
human race to make such incredible
achievements.
Patients with scleroderma often have
limitations in their hand function, for
example brushing their hair or open-
ing a jar, and this may have a signifi-
cant impact on quality of life. Hand
problems in patients with scleroder-
ma may be due to a number of causes
that I will now discuss.
Digital (finger and toe) ulcers are
common in patients with scleroder-
ma; indeed a recent study found that
10% of patients at any one time have
at least one finger ulcer. Digital ulcers
are found on the fingertips and also
over the back of the hands, are often
painful and not uncommonly become
infected. The end result is that such
ulcers can have a big impact on how
patients are able to use their hands.
Thinking about blood flow further (as
we believe that ulcers are largely
caused by lack of blood flow); severe
Raynaud's attacks, as readers may
well know, can be very painful and
disabling when they occur.
The skin thickening found in sclero-
derma may lead to another problem
with the hand: tightening with
'contractures' of the fingers, leading
to clawing of the fingers, and inability
to completely make a fist or stretch
out the fingers. Less commonly, we
increasingly recognise that a number
of patients with scleroderma also
have a type of 'inflammatory' arthritis,
that is, the joints themselves are actu-
ally inflamed or swollen, as opposed
to wear and tear ar thr i t i s
(osteoarthritis). It is important to
recognise the difference, as there are
effective treatments for such a type of
arthritis.
Calcinosis (lumps of calcium-
containing deposits beneath the skin)
represent yet another possible hand
problem in patients with scleroderma:
they can be very painful, and can in-
terfere with hand function. Some-
times calcinotic lumps ulcerate
through skin and there is then a dan-
ger that the area becomes infected.
I cannot emphasise enough how im-
portant it is that patients with sclero-
derma are managed by a dedicated
'multi-disciplinary team', that is a
group of health care professionals
(doctors, specialist nurses, occupa-
tional therapists, physiotherapists and
podiatrists to name but a few!) who
are familiar with the specific issues
relating to scleroderma. As the old
saying goes, “if in doubt it is always
best to get things checked out". For
example, if you are concerned that a
digital ulcer may be infected, then you
should seek medical advice as soon as
possible.
It is a great source of encouragement
that different researchers around the
world are looking at different aspects
of hands problems with patients with
scleroderma, such as digital ulcers and
also contractures of the fingers.
Scleroderma News: Scientific & Medical Page 19
Item Sub-items Weight/score
Skin thickening of the fingers of both hands extending proximal to MCP joints(sufficient criterion)
- 9
Skin thickening of the fingers(only count the higher score)
Puffy fingers 2
Sclerodactyly of the fingers (distal to the MCP joints, proximal to the PIP joints
4
Fingertip lesions (only count the higher score)
Digital tip ulcer 2
Fingertip pitting scar 3
Telangiectasia - 2
Abnormal nailfold capillaries - 2
Pulmonary arterial hypertension and/or interstitial lungdisease
- 2
Raynaud’s phenomenon - 3
SSc-related auto-antibodies(anticentromere, anti-topoisomerase I, anti-RNA polymerase III)
- 3
Add to maximum weight in each category to calculate the total scorePatients having a total score of 9 or more are being classified as having definitive systemic sclerosis
ACR ACR -- EULAR SSc classification criteriaEULAR SSc classification criteria
Hand Problems in Patients with Scleroderma

Scleroderma News: Scientific & Medical Page 20
Telangiectatases are knot-like clusters
of blood vessels on the skin which
can occur in 30 to 50 per cent of
patients with systemic sclerosis, a
potentially serious and incurable au-
to-immune condition that affects con-
nective tissue. Telangiectases tend to
occur on the face, neck and upper
limbs and can cause psychological
issues for patients.
Currently, doctors use laser treat-
ment to blast the Telangiectases and
destroy them but this treatment can
be painful at the time and result in
bruising afterwards so researchers
have been looking for an alternative.
Salford Royal is one of only a handful
of Trusts in the UK specialising in
systemic sclerosis, also known as
scleroderma, and Consultant Rheu-
matologist Ariane Herrick, also Pro-
fessor of Rheumatology at The Uni-
versity of Manchester, is a leading UK
expert in the condition. As part of
the Trust’s and University’s wide
range of studies to improve care of
scleroderma patients, researchers
tested using intense pulsed light (IPL)
instead of laser treatment. IPL is often
used cosmetically for treating birth-
marks and for hair removal.
Their pilot study treated 19 patients
with Telangiectases, using IPL on one
side of the face and laser treatment
on the other. They had three treat-
ments over the course of eight weeks
before the results were analysed us-
ing close-up photographs and special-
ist imaging. The research showed that
the effects were roughly comparable
but IPL had fewer side effects.
Salford Royal Rheumatology re-
searcher Dr Graham Dinsdale, who is
also a Research Associate at The Uni-
versity of Manchester, said: “While
this was only a small-scale pilot study,
it does suggest the potential for an
alternative, less painful, treatment for
Telangiectases. We will continue to
do all we can to find new and better
treatments for patients with systemic
sclerosis, which is a very serious and
debilitating condition.”
What is Telangiectasia?
Denise, a blogger from Michigan USA, explains: “Telangiectasia (Pictured above) are capil-
laries that have became dilated or enlarged which makes them visible on the surface of
the skin. Their appearance can vary from large pronounced red dots to very small dots.
More of a spidery broken vessel look may be what some experience. The specific reason
this happens is not yet known but scleroderma specialists view this as another aspect of
vascular damage caused by scleroderma. The spots when pressed will disappear only to
reappear once the pressure is released. They are flat and smooth on the skin with no
evidence of a raised spot or rash. Telangiectasia is the T in the acronym of CREST Syn-
drome. However, people with diffuse scleroderma can also get Telangiectasia. Telangiecta-
sia spots seem to more commonly appear on areas of the body which are exposed to the
sun. Therefore it has been stated by physicians that using a sunscreen of SPF 15 or great-
er is typically recommended. There are no proven preventative measure and efforts to
remove the spots by laser are not always successful. Many people choose cover-up cos-
metics such as a concealer or a foundation make-up as an alternative to the costly proce-
dure of laser which doesn't appear to bring long-term results.”
Read more of Denise’s blog: : http://sclerodermasupport.blogspot.co.uk
Researchers See the Light
Researchers at Salford Royal NHS Foundation Trust have
tested a new way to treat a disfiguring skin condition.

Scleroderma News: Scientific & Medical Page 21
By Lisa Elam
Patients with Scleroderma are part of
a minority of patients considered to
suffer with a ‘rare’ disease. Although
only a relatively small number of peo-
ple are affected by the disease
(approximately 1 in 10,000 people in
the UK) it is a disease that affects
multiple systems in the body and has
life-changing consequences for those
who are affected.
In my capacity as a medical student, I
was afforded the privilege of meeting
many patients with Scleroderma who
were lucky enough receive world
class treatment at my Rheumatology
p lacement with Professor K
Chakravarty, in May 2013. I was im-
pressed by the high standard of care
and was pleased indeed to see that
even patients with such a rare condi-
tion were being given the opportunity
to be seen and treated in their local
hospital, as opposed to travelling far
afield to other specialist centres.
This experience inspired me to sub-
mit an abstract to the International
Workshop for Scleroderma Research
in Boston, Masachussetts, in the
hope of broadcasting this excellent
work in the hope that the importance
of patients with rare conditions re-
ceiving specialist care in their local
area would be recognised by clinicians
globally. In order to quantify the ef-
fects of having such specialist care
provided locally, I conducted a survey
of all of the scleroderma patients
seen by Professor Chakravarty at
Queen’s hospital, Romford.
The results showed that 98% of pa-
tients were satisfied with the care
they received, 95% of patients stated
that attending their local hospital for
the same specialist care that they
could receive from further afield was
easier financially and from a conven-
ience perspective. 97% of patients felt
that their disease was well controlled
due to their attendance at the special-
ist clinic.
The poster was very well received at
the Scleroderma Workshop and
many clinicians and scientists alike
were interested to see how this mod-
el of care could be replicated on a
wider scale. The poster (pictured
above) included information on the
possibility of improving on this model
of care further still, by utilizing expert
patients in order to create a truly
holistic and supportive model of care
for patients with scleroderma.
I would like to thank the Scleroderma
Society for sponsoring my attendance
at the International Workshop for
Scleroderma Research and look for-
ward to working with them in the
future in order to raise awareness
amongst healthcare professionals
about Scleroderma.
Super-Specialist Clinics For All:
Introducing an exemplary model of care from North East London
Specialist Clinics
at the Royal Free
Hospital, London:
The rheumatology department is a major
centre for rheumatology y and connective
tissue diseases providing high quality care
for the full range of rheumatic diseases
including spinal pain through a physio-
therapy-led service. In addition to provid-
ing secondary care for rheumatic disease
to the local population, we have particu-
lar expertise in multisystem connective
tissue diseases, especially scleroderma
(systemic sclerosis).
Location: Lower ground floor, Royal Free
Hospital, London NW3 2QG
Appointments can be made following a
referral from a GP, and may be made
through the choose and book system, or
as tertiary referrals from other hospitals.
Cathy Can Help! Fight Scleroderma the fashionable way
Cathy Renwood, 44, from London,
has had Linear Morphea since the age
of 10. When she was 20 she had to
have major surgery after she lost all
movement in her right arm, due to
Morphea tightening her chest wall.
Cathy had her chest wall and right
breast rebuilt using skin grafts. After
the ordeal Cathy was left with scar-
ring and was forced to learn how to
dress around this. Cathy said: “Luckily
I am someone who loves shopping,
but this was still sometimes a chal-
lenge!
“Because of this I have recently start-
ed a Personal Shopping Business. I
specialise in Post-Mastectomy Fashion
and dressing around scars. I truly
believe that everyone should look and
feel their best. Some of us have a bit
more to dress around but this is al-
ways possible.”
“I am based in London and would like
to offer anyone with Scleroderma
20% off any of my services.
Also if anyone in the London area is
hosting/having a charity event, I would
like to donate a half day Personal
Shopping Session.”
For more information on Cathy’s
work, take a look at her website
www.thestyleangel.co.uk.
Break Time Can you find all the Sclero-words?
Can You Solve
the Riddle?
A father and his son are in a car acci-
dent. The father dies instantly, and the
son is taken to the nearest hospital.
The doctor comes in and exclaims "I
can't operate on this boy."
"Why not?" the nurse asks.
"Because he's my son," the doctor
responds.
How is this possible?
Scleroderma News: Pharmacy Page 22
M E H O R E X A T E T T
O A S A M G O K S S R N
R H N M Y A H P I E U T
P F L D I L A X O A A R
H I S Y L I S N L G L O
E Z K T F Q P I S Y E O
A E R A R E I P P N D C
C H I S E N T O N L R D
T E Y I E N A M I N U L
D I R O P S L T U I G U

Notice board Local Contacts and support services
Inspirational Quote of the Season “I learned that courage was not the absence of fear, but the triumph over it. The brave man
is not he who does not feel afraid, but he who conquers that fear.” ― Nelson Mandela
Bedfordshire
Rita Boulton
01767 312544
Buckinghamshire &
Hertfordshire
Marilyn York
andrewandmarilyn@bt
internet.com 07702 592 387
Burton on Trent
Helen Nutland
[email protected] 01283 566333 x5247
Cornwall
Alex Pooley
alex@sclerodermasociety.
co.uk 01736 755845
Derbyshire, S.Yorkshire,
Staffordshire & Cheshire
Lynette Peters
lynette@sclerodermasociety.
co.uk 07947 350815
Derbyshire, S.Yorkshire,
Staffordshire & Cheshire
Diana Twigg
diana@sclerodermasociety.
co.uk 01298 24539
Devon
Anne Sheere
.co.uk 01752 338156
East Anglia
Jacky March
jacky@sclerodermasociety
.co.uk 01394 286637
East Midlands
Cheryl Darch
cheryl@sclerodermasociety
.co.uk 0116 2717180
East Sussex
Rosanna Clifton
rosanna@sclerodermasociety
.co.uk 01424 426738
East Yorkshire
Lynn Hind
01482 354312
Essex, Kent & East London
Amanda Thorpe
01702 344925
Hampshire
Tracey James
02392 677476
Lancashire & North West
Yorkshire
Sheila Procter
sheila@sclerodermasociety.
co.uk 01282 429004
Merseyside
Helen Lingwood
0151 2801194
North East England
Jessie Pickering
01388 527840
North East Scotland
Susan Wilson
077 40185627
North Wales
Kate Owen
angharad.owen48@btinternet.
com 01492 515834
Oxfordshire & Berkshire
Melanie Bowen
melanie@sclerodermasociety
.co.uk 01865 517033
Powys & Shropshire
Jennifer Ames
01544 267988
Scotland
Frances Bain
0131 477 1122
South London
Celia Bhinda
020 8698 6294
South Wales
Belinda Thompson
belinda@sclerodermasociety
.co.uk 02920 625056
South West England
Judith Foster
07985 335 336
Surrey
Nicky O'Shea
01483 764524
West Midlands
Jane Beach
01527 459552
West Sussex
Lesley Dodd
01903 753971
West Sussex
Jo Frowde
01403 741445
Wiltshire & North Hampshire
Lynn Morton
lynnm@sclerodermasociety
.co.uk 01980 863444
Local Group Co-ordinator: Liz Holloway
[email protected], 01243 539466
Join us on Facebook!
www.facebook.com/
sclerodermauk
Online Support
We have set up a new
and complementary
community powered by
Health Unlocked. If you
are a Facebook user you
may have seen advertise-
ments pop up on your
page. Why not give both
the forums a go? Have a
look around, meet and
get support from other
people with Scleroder-
ma.
Scleroderma News: Local Groups Page 23
Contacts
Steve Holloway
(Secretary) steve@
sclerodermasociety.co.uk
Susie Hoare susie@
sclerodermasociety.co.uk
Helena Rozga Helena@
sclerodermasociety.co.uk
Office & Administration
Manager: Amy Barrick
020 7000 1925, amy@
sclerodermasociety.co.uk
Local Group co-
ordinator: Liz Holloway,
uk
Helpline Manager: Helena
Rozga, Helena@
sclerodermasociety.co.uk
Event enquiries: Susie
Hoare, susie@
sclerodermasociety.co.uk
Events Calendar Calendar
@sclerodermasociety.co.uk
Helpline: Although The
Scleroderma Society can
not offer medical advice,
they operate a free helpline,
offering a kind ear. We will
help in any way we can be-
tween 9.00—21.00 every
day. Call 0800 311 2756.
Carers Support Group:
Michael Thorpe 01702 344
925, [email protected]
Specialist Nurses:
Nurse led lines for general
inquiries only, in non emer-
gencies. If the nurse is una-
vailable please leave a mes-
sage:
Liverpool Aintree Univer-
sity Hospital: Jan Lamb
0151 525 5980 bleep 2231
Bath Royal National Hospi-
tal for Rheumatic Diseases:
Sue Brown 01225 428 823
Belfast Ulster Hospital:
Audrey Hamilton 02890
561 310
Dundee Ninewells Hospi-
tal: Steve McSwiggan 01382
633 957
Leeds Chapel Allerton
Hospital: Elizabeth Tyas
0113 392 3035
London Royal Free
Hospital Scleroderma
queries: 020 783 02326
and Pulmonary
hypertension:
020 7472 6354
London Royal Brompton
Hospital Respiratory
queries: Lucy Pigram
07758 8943175
Manchester Hope
Hospita: Liz Wragg and
Catherine Lambe 0161
206 0192
Newcastle Freeman
Hospital Scleroderma
queries: Karen Walker
0191 223 1503 and
Pulmonary hypertension:
Rachael Crackett /
Julia De Soyza
0191 213 7418
Portsmouth Queen
Alexandra Hospital:
Paula White / Julie Ingold
02392 286935
Scleroderma News: Contacts Page 24
Connecting you to Scleroderma Professionals,
groups and nation wide support networks
Scleroderma
News
Write to:
The Scleroderma
Society
Bride House,
18-20 Bride Lane,
London
EC4Y 8EE
Phone us:
020 7000 1925
Email the editor:
Hollie@Scleroderma
society.co.uk
Printing &
Publishing:
Jarvis & Company
The Scleroderma Society is a registered charity: 286736