feature acne in childhood: an updatem3.wyanokecdn.com/b201c146e539ce04aa961dc8e276faaf.pdflescent or...
TRANSCRIPT

418 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:10 | OCTOBER 2013
FEATURE
Acne is the most common chron-ic skin disease affecting chil-dren and adolescents, with an
85% prevalence rate among those aged 12 to 24 years.1 However, recent data suggest a younger age of onset is com-mon and that teenagers only comprise 36.5% of patients with acne.2,3 This ar-ticle provides an overview of acne, its pathophysiology, and contemporary classification; reviews treatment op-tions; and reviews recently published algorithms for treating acne of differing levels of severity.
Acne can be classified based on le-sion type (morphology) and the age group affected.4 The contemporary classification of acne based on sev-eral recent reviews is addressed below. Acne lesions (see Table 1, page 419) can be divided into noninflammatory lesions (open and closed comedones, see Figure 1) and inflammatory lesions (papules, pustules, and nodules, see Figure 2). The comedone begins with
the microcomedone, which is a micro-scopic plug of the follicular ostia of the pilosebaceous unit. Four process-es are necessary for an acne lesion to evolve: 1) altered shedding of the ke-ratinocytes that line the pilosebaceous unit; 2) increased sebum production;
3) proliferation of Propionibacterium acnes (considered the “acne organ-ism”); and 4) the release of inflamma-tory mediators.5 The sequence of these events remains under investigation (ie, some recent studies suggest that even comedones may be preceded by inflam-
Acne in Childhood: An UpdateWendy Kim, DO; and Anthony J. Mancini, MD
Wendy Kim, DO, is Assistant Professor of In-
ternal Medicine and Pediatrics, Division of Der-
matology, Loyola University Medical Center,
Chicago. Anthony J. Mancini, MD, is Professor
of Pediatrics and Dermatology, Northwestern
University Feinberg School of Medicine, Ann
and Robert H. Lurie Children’s Hospital of Chi-
cago.Address correspondence to: Anthony J. Man-
cini, MD, Division of Dermatology Box #107, Ann and Robert H. Lurie Children’s Hospital of Chicago, 225 E. Chicago Avenue, Chicago, IL 60611; email: [email protected].
Disclosure: Dr. Kim is an advisory board par-ticipantfor Galderma. Dr. Mancini is a consul-tant, speaker, and advisory board participant for Galderma.
doi: 10.3928/00904481-20130924-13
Figure 1. Comedonal acne. This patient has numerous closed comedones (ie, “whiteheads”).
All i
mag
es c
ourte
sy o
f Ant
hony
J. M
anci
ni, M
D.
Figure 2. Moderate mixed acne. In this patient, a combination of closed comedones, inflammatory pap-ules, and pustules can be seen.
PEDIATRIC ANNALS 42:10 | OCTOBER 2013 Healio.com/Pediatrics | 419
FEATURE
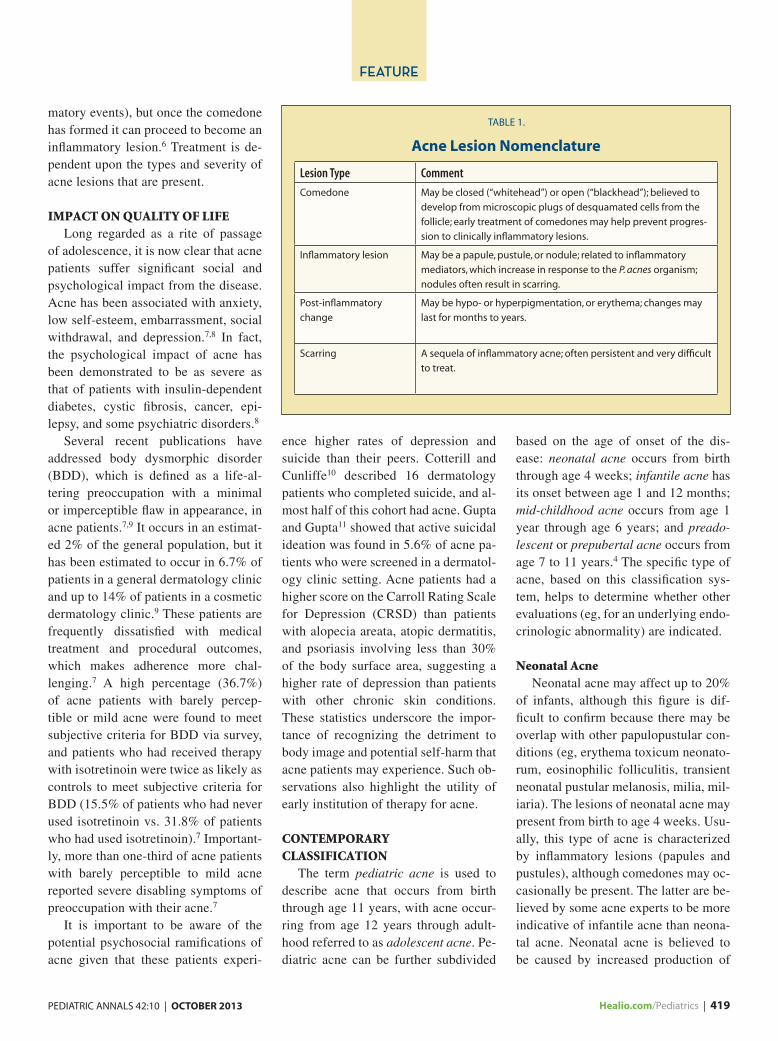
matory events), but once the comedone has formed it can proceed to become an inflammatory lesion.6 Treatment is de-pendent upon the types and severity of acne lesions that are present.
IMPACT ON QUALITY OF LIFELong regarded as a rite of passage
of adolescence, it is now clear that acne patients suffer significant social and psychological impact from the disease. Acne has been associated with anxiety, low self-esteem, embarrassment, social withdrawal, and depression.7,8 In fact, the psychological impact of acne has been demonstrated to be as severe as that of patients with insulin-dependent diabetes, cystic fibrosis, cancer, epi-lepsy, and some psychiatric disorders.8
Several recent publications have addressed body dysmorphic disorder (BDD), which is defined as a life-al-tering preoccupation with a minimal or imperceptible flaw in appearance, in acne patients.7,9 It occurs in an estimat-ed 2% of the general population, but it has been estimated to occur in 6.7% of patients in a general dermatology clinic and up to 14% of patients in a cosmetic dermatology clinic.9 These patients are frequently dissatisfied with medical treatment and procedural outcomes, which makes adherence more chal-lenging.7 A high percentage (36.7%) of acne patients with barely percep-tible or mild acne were found to meet subjective criteria for BDD via survey, and patients who had received therapy with isotretinoin were twice as likely as controls to meet subjective criteria for BDD (15.5% of patients who had never used isotretinoin vs. 31.8% of patients who had used isotretinoin).7 Important-ly, more than one-third of acne patients with barely perceptible to mild acne reported severe disabling symptoms of preoccupation with their acne.7
It is important to be aware of the potential psychosocial ramifications of acne given that these patients experi-
ence higher rates of depression and suicide than their peers. Cotterill and Cunliffe10 described 16 dermatology patients who completed suicide, and al-most half of this cohort had acne. Gupta and Gupta11 showed that active suicidal ideation was found in 5.6% of acne pa-tients who were screened in a dermatol-ogy clinic setting. Acne patients had a higher score on the Carroll Rating Scale for Depression (CRSD) than patients with alopecia areata, atopic dermatitis, and psoriasis involving less than 30% of the body surface area, suggesting a higher rate of depression than patients with other chronic skin conditions. These statistics underscore the impor-tance of recognizing the detriment to body image and potential self-harm that acne patients may experience. Such ob-servations also highlight the utility of early institution of therapy for acne.
CONTEMPORARY CLASSIFICATION
The term pediatric acne is used to describe acne that occurs from birth through age 11 years, with acne occur-ring from age 12 years through adult-hood referred to as adolescent acne. Pe-diatric acne can be further subdivided
based on the age of onset of the dis-ease: neonatal acne occurs from birth through age 4 weeks; infantile acne has its onset between age 1 and 12 months; mid-childhood acne occurs from age 1 year through age 6 years; and preado-lescent or prepubertal acne occurs from age 7 to 11 years.4 The specific type of acne, based on this classification sys-tem, helps to determine whether other evaluations (eg, for an underlying endo-crinologic abnormality) are indicated.
Neonatal AcneNeonatal acne may affect up to 20%
of infants, although this figure is dif-ficult to confirm because there may be overlap with other papulopustular con-ditions (eg, erythema toxicum neonato-rum, eosinophilic folliculitis, transient neonatal pustular melanosis, milia, mil-iaria). The lesions of neonatal acne may present from birth to age 4 weeks. Usu-ally, this type of acne is characterized by inflammatory lesions (papules and pustules), although comedones may oc-casionally be present. The latter are be-lieved by some acne experts to be more indicative of infantile acne than neona-tal acne. Neonatal acne is believed to be caused by increased production of
TABLE 1.
Acne Lesion Nomenclature
Lesion Type Comment
Comedone May be closed (“whitehead”) or open (“blackhead”); believed to
develop from microscopic plugs of desquamated cells from the
follicle; early treatment of comedones may help prevent progres-
sion to clinically inflammatory lesions.
Inflammatory lesion May be a papule, pustule, or nodule; related to inflammatory
mediators, which increase in response to the P. acnes organism;
nodules often result in scarring.
Post-inflammatory
change
May be hypo- or hyperpigmentation, or erythema; changes may
last for months to years.
Scarring A sequela of inflammatory acne; often persistent and very difficult
to treat.

420 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:10 | OCTOBER 2013
FEATURE
dehydroepiandrosterone (DHEA), in association with a large androgen-pro-ducing zona reticularis in the fetal adre-nal glands. There is also transplacental passage of androgens, which stimulate sebaceous glands, as well as testicular production of androgens. From birth through age 6 to 12 months, boys also have pubertal levels of testosterone, which might explain why acne is more common in male infants than in female infants.12
In recent years, a more pustular pre-sentation of neonatal acne has been de-scribed and termed neonatal cephalic pustulosis (see Figure 3). A relationship between this condition and increased colonization with (or hypersensitivity to) Malassezia furfur, M. sympodialis, or other species has been suggested. In a 1996 cohort of 13 neonates, pus-tule smears from the faces and necks were notable for M. furfur in eight pa-tients, whose skin all cleared rapidly following application of ketoconazole cream.13 Subsequent studies have been inconsistent in their findings, but many experts still recommend consideration of topical antifungal therapy in neo-nates with severe pustular acneiform eruptions.14-16
Infantile AcneInfantile acne begins sometime in
the first year of life, typically between ages 4 to 6 weeks and age 1 year. It is more common in boys than in girls and is more likely than neonatal acne to be predominantly comedonal (see Figure 4). Inflammatory lesions may or may not be present, but if present they may occasionally be severe. Nodules can also occur occasionally, and when in-fantile acne is moderate to severe, scar-ring may result (see Figure 5). In pa-tients with infantile acne, the physical examination should include a growth assessment as well as evaluation for any features of precocious puberty or an-drogen excess, including axillary odor,
Figure 3. Neonatal cephalic pustulosis. This newborn had numerous pustules over the forehead and cheeks, and improved dramatically following therapy with a topical antifungal cream.
Figure 5. Infantile acne. The mild scarring present in this infant highlights the importance of considering early therapy for patients with moderate or severe involvement.
Figure 4. Infantile acne. This infant has numerous open comedones (“blackheads”) with occasional in-flammatory papules.
422 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:10 | OCTOBER 2013
FEATURE
breast development, clitoromegaly, presence of axillary and/or genital hair, and increased muscle mass. If concerns are present, laboratory workup and/or referral to a pediatric endocrinologist are recommended. Sidebar 1 (see page 423) lists the recommended laboratory evaluation when androgen excess is suspected.14,15,17
Mid-Childhood AcneAcne that begins in children aged 1
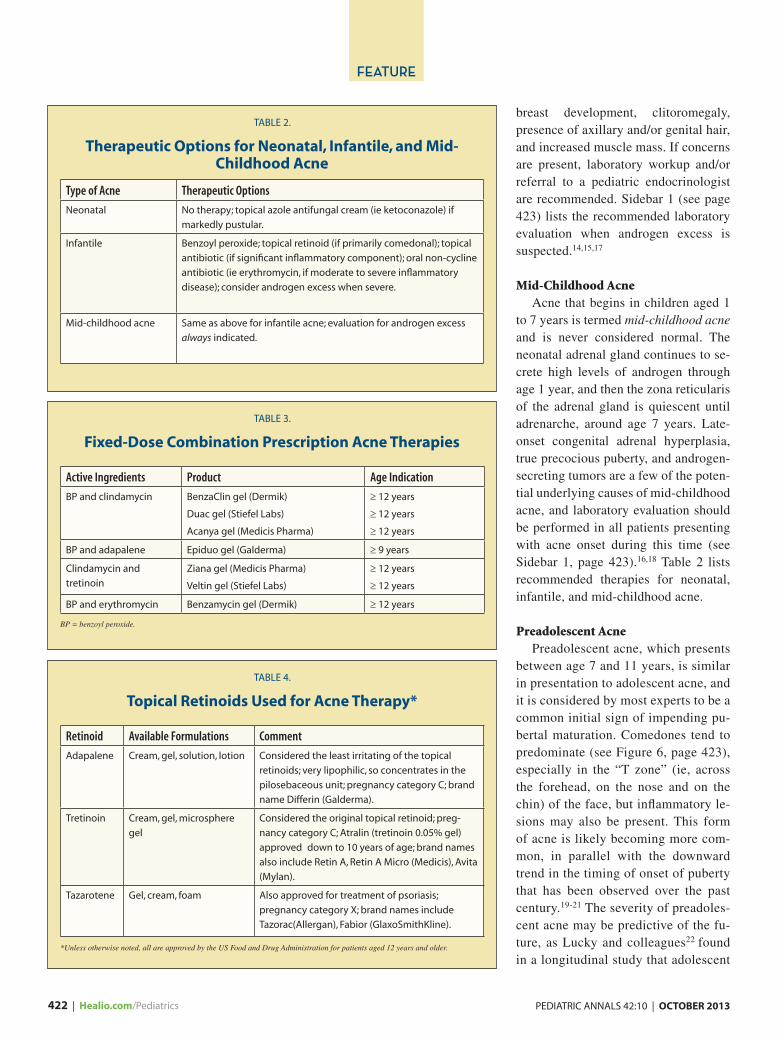
to 7 years is termed mid-childhood acne and is never considered normal. The neonatal adrenal gland continues to se-crete high levels of androgen through age 1 year, and then the zona reticularis of the adrenal gland is quiescent until adrenarche, around age 7 years. Late-onset congenital adrenal hyperplasia, true precocious puberty, and androgen-secreting tumors are a few of the poten-tial underlying causes of mid-childhood acne, and laboratory evaluation should be performed in all patients presenting with acne onset during this time (see Sidebar 1, page 423).16,18 Table 2 lists recommended therapies for neonatal, infantile, and mid-childhood acne.
Preadolescent AcnePreadolescent acne, which presents
between age 7 and 11 years, is similar in presentation to adolescent acne, and it is considered by most experts to be a common initial sign of impending pu-bertal maturation. Comedones tend to predominate (see Figure 6, page 423), especially in the “T zone” (ie, across the forehead, on the nose and on the chin) of the face, but inflammatory le-sions may also be present. This form of acne is likely becoming more com-mon, in parallel with the downward trend in the timing of onset of puberty that has been observed over the past century.19-21 The severity of preadoles-cent acne may be predictive of the fu-ture, as Lucky and colleagues22 found in a longitudinal study that adolescent
TABLE 3.
Fixed-Dose Combination Prescription Acne Therapies
Active Ingredients Product Age Indication
BP and clindamycin BenzaClin gel (Dermik)
Duac gel (Stiefel Labs)
Acanya gel (Medicis Pharma)
≥ 12 years
≥ 12 years
≥ 12 years
BP and adapalene Epiduo gel (Galderma) ≥ 9 years
Clindamycin and
tretinoin
Ziana gel (Medicis Pharma)
Veltin gel (Stiefel Labs)
≥ 12 years
≥ 12 years
BP and erythromycin Benzamycin gel (Dermik) ≥ 12 years
BP = benzoyl peroxide.
TABLE 4.
Topical Retinoids Used for Acne Therapy*
Retinoid Available Formulations Comment
Adapalene Cream, gel, solution, lotion Considered the least irritating of the topical
retinoids; very lipophilic, so concentrates in the
pilosebaceous unit; pregnancy category C; brand
name Differin (Galderma).
Tretinoin Cream, gel, microsphere
gel
Considered the original topical retinoid; preg-
nancy category C; Atralin (tretinoin 0.05% gel)
approved down to 10 years of age; brand names
also include Retin A, Retin A Micro (Medicis), Avita
(Mylan).
Tazarotene Gel, cream, foam Also approved for treatment of psoriasis;
pregnancy category X; brand names include
Tazorac(Allergan), Fabior (GlaxoSmithKline).
*Unless otherwise noted, all are approved by the US Food and Drug Administration for patients aged 12 years and older.
TABLE 2.
Therapeutic Options for Neonatal, Infantile, and Mid-Childhood Acne
Type of Acne Therapeutic Options
Neonatal No therapy; topical azole antifungal cream (ie ketoconazole) if
markedly pustular.
Infantile Benzoyl peroxide; topical retinoid (if primarily comedonal); topical
antibiotic (if significant inflammatory component); oral non-cycline
antibiotic (ie erythromycin, if moderate to severe inflammatory
disease); consider androgen excess when severe.
Mid-childhood acne Same as above for infantile acne; evaluation for androgen excess
always indicated.

PEDIATRIC ANNALS 42:10 | OCTOBER 2013 Healio.com/Pediatrics | 423
FEATURE
girls with more severe acne were more likely to have had more comedonal and inflammatory lesions as early as age 10 years. This cohort also was also more likely to undergo earlier men-arche than those girls who had had mild preadolescent comedonal acne.22
ACNE THERAPYThe following sections apply to ado-
lescent acne, although preadolescent acne is usually treated with similar agents (albeit often in “off-label” fash-ion). An exhaustive discussion of acne therapy is beyond the scope of this ar-ticle (for more information, the reader is directed to recent reviews12,16,23).
TOPICAL THERAPYProper skin cleansing should always
be discussed with acne patients. Al-though the patient may be under the im-pression that scrubbing to remove dirt and oil will improve the appearance of acne, such overmanipulation may actu-ally increase inflammation and, hence, should be discouraged. Cleansing once to twice daily with warm water and a gentle acne wash should be encour-aged.16 The use of scrubbing devices or abrasive sponges should be discour-aged for most patients.
Many over-the-counter products and “systems” for acne are available. The
active ingredients in these products are often benzoyl peroxide (BP) or salicylic acid. BP has been available since 1934 and works by creating free radicals that destroy the acne organism, P. acnes. Ad-ditionally, it reduces the release of reac-tive oxygen species from neutrophils, thereby reducing inflammation.24 BP has gained favor in recent years given its utility in acne therapy combined with the lack of development of resistance to this agent. It has also been shown to de-crease the development of resistance to concomitant antibiotics utilized as part of the acne regimen.25 BP is available in a variety of washes and “leave-on” gels, in strengths ranging from 2.5% to 10%. Although previously available by prescription, BP washes are now avail-able exclusively on an over-the-counter basis. However, it is also found in sev-eral fixed-dose combination products available by prescription (see Table 3, page 422). Patients should be warned about the potential bleaching of linens and clothing by BP. Salicylic acid is a keratolytic agent that may be beneficial for mild comedonal acne. It is available in washes, pads, and other over-the-counter products.
Topical retinoids play a paramount role in the treatment of acne. They are vitamin A derivatives (either natu-rally occurring or synthetic) that bind to retinoid receptors in the skin. They work within the nucleus to alter down-stream signals affecting inflammatory pathways and proliferation.26,27 Spe-cifically, retinoids normalize follicular keratinization and prevent the micro-comedone from forming; therefore, they play a preventive role in the treat-ment of acne in addition to their benefi-cial effects on the existing comedones. It is important to educate patients on proper use and expectations with topi-cal retinoids. These agents may result in some peeling, redness, and irritation, primarily with initial use.28 These side effects tend to decrease after 4 weeks of regular use and can be minimized by alternate-night (or every third night) application during initiation, if needed. It should be reiterated that topical reti-noids should be applied as a thin film at bedtime to all “fields” where the patient gets acne, and not as spot therapy. Table 4 (see page 422) lists the available topi-cal retinoids, along with their strengths, vehicles, and proprietary names.
SIDEBAR 1.
Recommended Laboratory Evaluations for the Child with Acne and Suspected
Androgen Excess• Luteinizing hormone
• Follicle-stimulating hormone
• Dehydroepiandrosterone sulfate
• 17-hydroxyprogesterone
• Free and total testosterone
• Prolactin
• Bone age
Figure 6. Preadolescent acne. This 9-year-old female has a combination of closed comedones and in-flammatory papules, which were limited to the “T zone” distribution on the forehead, nose, and chin.

424 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:10 | OCTOBER 2013
FEATURE
Topical antibiotics, including eryth-romycin and clindamycin, are used in the treatment of inflammatory acne and are aimed at the reduction of P. acnes. These agents are typically applied once daily. Clindamycin is available as a 1% gel, solution, lotion, and foam, and erythromycin is available as a 5% gel and solution. Monotherapy with topi-cal antibiotics is not recommended be-cause of their prolonged onset of action and the likelihood of bacterial resis-tance.25 Since the 1970s, the resistance of P. acnes to erythromycin as well as clindamycin has increased dramati-cally.25 Concomitant use of BP, either as a wash or as part of a fixed-dose
combination product, is highly recom-mended when topical antibiotics are used. Dapsone 5% gel (Aczone, Aller-gan) was recently approved for acne. It has been shown to reduce inflammatory lesions in as early as 2 weeks, with the safety of twice-daily use being demon-strated for up to 1 year in patients aged 12 to 15 years.29,30 Hemolytic anemia can occur in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency when treated with oral dap-sone, but this effect seems very unlikely in G6PD-deficient patients treated with topical dapsone.31 Sulfur exhibits anti-bacterial and keratolytic properties, and it is often combined with sodium sulfa-
cetamide in acne products to mask its odor. Sodium sulfacetamide is available as a solution or lotion.
Several topical, fixed-dose combina-tion therapies have been approved for the treatment of mild-to-moderate acne vulgaris (see Table 3, page 422). The advantages of these therapies include the improved adherence they offer (via simplification of the treatment regimen) and the complementary mechanisms of action of the individual components. The fixed-dose combination products currently available include products containing BP and clindamycin, BP and adapalene, BP and erythromycin, and tretinoin and clindamycin. These agents are typically applied once to twice daily. To obtain US Food and Drug Administration (FDA) approval
SIDEBAR 2.
General Guidelines in Oral Antibiotic Therapy for Acne• Continue oral antibiotics for at least 2 to 3
months to assess for response
• Oral antibiotic therapy should be
combined with a topical regimen that
includes:
Benzoyl peroxide (either as part of a
“leave-on” regimen or as a wash), in an
effort to minimize the development of
bacterial resistance; and
Topical retinoid, to more effectively treat
comedones and for their role in preven-
tion of the development of new acne
• Educate patients to expect a 3- to
6-month period of therapy (occasionally
longer), with the goal of discontinuing the
oral treatment as early as feasible (while
continuing the topical maintenance
regimen).
• Discuss potential side effects and warn-
ings of oral antibiotic therapy.
• Routine laboratory monitoring is not
recommended in the absence of underly-
ing conditions that may predispose the
patient to toxicities (ie hepatic or renal
insufficiency)
Adapted from Eichenfield and Mancini,12 Eichenfield et al,16 Thiboutot et al,23 Tsankov et al,33 Webster and Graber,34 Zaenglein and Thiboutot,35 and Del Rosso and Kim36
TABLE 5.
Common Oral Antibiotics Used for Acne Therapy
Antibiotic Recommended Dose Potential Adverse Events / Comment
Doxycycline 50 mg-100 mg BID GI upset, pill esophagitis, sensitivity in the sun
(including photo-onycholysis), dental discol-
oration (not recommended < 8 years of age),
IBD, hepatitis, vaginal candidiasis; subantimicro-
bial dosing also used at 20 mg BID; available in
delayed-release formulation.
Minocycline 50 mg-100 mg BID Cutaneous and mucosal hyperpigmentation, drug
hypersensitivity with hepatitis and pneumonitis,
lupus-like syndrome, Stevens Johnson syndrome,
vaginal candidiasis, vestibular effects, dental
discoloration (not recommended < 8 years of
age), IBD, photosensitivity (less than doxycycline),
pseudotumor cerebri; available in extended-
release formulation.
Tetracycline 250 mg-500 mg BID GI upset, pill esophagitis, sensitivity in the sun,
hepatic dysfunction, dental discoloration (not
recommended < 8 years of age), IBD.
Erythromycin 250 mg-500 mg BID Marked GI upset, diarrhea, prolongation of QT
interval, increasing resistance in acne; no longer
recommended by most experts.
Cephalexin 250 mg-500 mg BID Vaginal candidiasis, rare drug reactions; routine
use for acne not recommended.
Trimethoprin-
sulfamethoxa-
zole
80 mg/400 mg to 160
mg/800 mg
Severe drug reactions, bone marrow suppression,
drug hypersensitivity syndrome; routine use for
acne strongly discouraged.
BID = twice daily; GI = gastrointestinal; IBD = inflammatory bowel disease.
PEDIATRIC ANNALS 42:10 | OCTOBER 2013 Healio.com/Pediatrics | 425
FEATURE
for these products, manufacturers need to show that the combination product demonstrates increased efficacy com-pared with the individual components (the “monads”) and the vehicle.
Oral TherapyAlthough only two oral antibiot-
ics (minocycline extended-release for moderate and severe acne and doxycy-cline delayed-release for severe acne) are FDA-approved for the treatment of acne, the use of oral antibiotics has been common practice for decades. The goal of antibiotic therapy is to reduce the P. acnes count and therefore the inflammatory stimulus. Oral antibiot-ics are typically viewed as “anti-in-flammatory” treatment for acne, rather than treatment for a true infection.32,33 By reducing the overall P. acnes load, bacterial lipases (and therefore triglyc-erides and subsequent free fatty acids) are reduced as well. Oral antibiotics are typically recommended when there is a suboptimal response to a topical thera-peutic regimen, when there is wide-spread disease (ie, extensive truncal disease) for which topical therapy alone may not be feasible, and when there is greater overall severity that seem un-likely to respond to topical treatments alone.16,23,34
Chlortetracycline, the first antibiotic in the cycline class, was introduced in 1948.33 Antibiotics in this class are still first-line therapy for patients older than 8 years with moderate-to-severe inflammatory acne. Tetracycline, how-ever, has become less desirable in the era of newer-generation cyclines, such as minocycline and doxycycline, given its limitations related to dosing on an empty stomach and gastrointestinal intolerance. Table 5 (see page 424) summarizes the oral antibiotics most commonly used for acne therapy. Some general guidelines in oral antibiotic therapy for acne are listed in Sidebar 2 (see page 424).
Hormonal therapies, including spi-ronolactone and combined oral contra-ceptive pills, are potentially effective therapies in some patients with ado-lescent or young adult acne. Patients most likely to respond include females of childbearing age with acne accentu-ated on the neck and in the mandibular regions, those with perimenstrual flares in their acne, those with hirsutism or other features of androgen excess, and those with a poor response to conven-tional treatments.
Oral isotretinoin is an extremely ef-fective treatment for nodulocystic acne, and it was approved for use in 1982. It should be considered in patients with severe or resistant acne vulgaris in whom the likelihood for scarring is considered significant. Isotretinoin is a known teratogen, a fact that led to the development of the iPLEDGE program. iPLEDGE is an FDA-mandated regis-tration program for prospective patients as well as prescribing physicians and dispensing pharmacies. The goal of the
program is to reduce fetal exposure to isotretinoin by requiring monthly preg-nancy tests in females of childbearing age. Unfortunately, a recent retrospec-tive study of pregnancies occurring during isotretinoin use revealed that iPLEDGE has not made a significant impact in this regard.37 Isotretinoin is most appropriately prescribed by der-matologists (or other clinicians familiar with its use); further discussion of this topic is beyond the scope of this article.
DESIGNING A TREATMENT REGIMEN
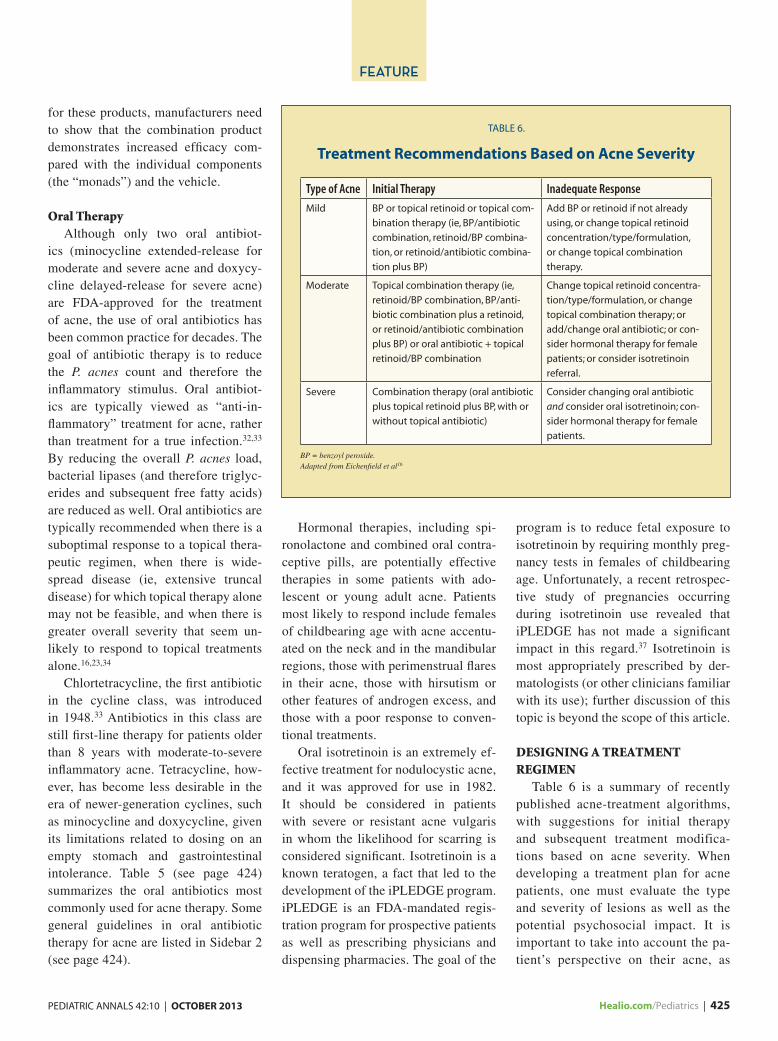
Table 6 is a summary of recently published acne-treatment algorithms, with suggestions for initial therapy and subsequent treatment modifica-tions based on acne severity. When developing a treatment plan for acne patients, one must evaluate the type and severity of lesions as well as the potential psychosocial impact. It is important to take into account the pa-tient’s perspective on their acne, as
TABLE 6.
Treatment Recommendations Based on Acne Severity
Type of Acne Initial Therapy Inadequate Response
Mild BP or topical retinoid or topical com-
bination therapy (ie, BP/antibiotic
combination, retinoid/BP combina-
tion, or retinoid/antibiotic combina-
tion plus BP)
Add BP or retinoid if not already
using, or change topical retinoid
concentration/type/formulation,
or change topical combination
therapy.
Moderate Topical combination therapy (ie,
retinoid/BP combination, BP/anti-
biotic combination plus a retinoid,
or retinoid/antibiotic combination
plus BP) or oral antibiotic + topical
retinoid/BP combination
Change topical retinoid concentra-
tion/type/formulation, or change
topical combination therapy; or
add/change oral antibiotic; or con-
sider hormonal therapy for female
patients; or consider isotretinoin
referral.
Severe Combination therapy (oral antibiotic
plus topical retinoid plus BP, with or
without topical antibiotic)
Consider changing oral antibiotic
and consider oral isotretinoin; con-
sider hormonal therapy for female
patients.
BP = benzoyl peroxide.Adapted from Eichenfield et al16

426 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:10 | OCTOBER 2013
FEATURE
some with even mild acne may be ex-periencing serious psychosocial com-promise. Patients and their parents should be warned if they are likely to have permanent scarring.
Before utilizing a treatment algo-rithm, the patient’s acne should be categorized as mild (predominantly comedonal or mixed comedonal and mildly inflammatory acne), moder-ate (more inflammatory lesions with a substantial comedonal component as well), or severe (even greater num-bers of inflammatory lesions and often comedones as well as nodules, and greater risk for scarring). Proper use and application of the treatment regi-men should be discussed, including a discussion of expected side effects of the medications. Written action plans are very beneficial and may increase adherence, which should be assessed at every visit, and the patient should be offered positive reinforcement when improvement is noted. It is also impor-tant to highlight changes that may not be clear to the patient, such as post-inflammatory hyperpigmentation as a sign of treatment response.
Adherence to therapy is a major is-sue in acne treatment in adolescents. Nonconfrontational but directed ques-tions such as “How many times per week do you forget to use your medi-cation?” rather than “Are you using your medication as directed?” may lead to more truthful answers. Other suggestions for increasing adherence with acne regimens include simplify-ing the number of medications pre-scribed (when feasible), setting re-alistic expectations, and reinforcing maintenance therapy once clinical im-provement is noted.12 Ease of use and choice of vehicle for topical medica-tions should be considered. For exam-ple, gels are traditionally more drying than creams, but may be appropriate for patients with oily skin. In addition, newer gel technologies are well toler-
ated and less drying than their prior formulations.
CONCLUSIONThe pathogenesis of acne is com-
plex and multifactorial, and our un-derstanding of it continues to evolve. Acne may be associated with signifi-cant psychosocial compromise and BDD, highlighting the importance of early therapy. Acne presenting in younger children may have other ram-ifications, and it can be categorized by the age of onset. In preadolescents and adolescents with acne, there are a vari-ety of traditional and newer treatment options. Use of a published treatment algorithm is helpful in guiding initial and subsequent therapeutic agents and combinations. Benzoyl peroxide is desirable as a component of any acne regimen, given its ability to help di-minish the development of resistance. Topical retinoids play an important role in acne therapy, both for their ef-fects on established lesions as well as their role in long-term maintenance. Adherence to an acne-treatment plan can be increased by appropriate edu-cation, anticipatory guidance, written action protocols, frequent follow-up, and simplification of the regimen, as feasible.
REFERENCES 1. Bhate K, Williams HC. Epidemiol-
ogy of acne vulgaris. Br J Dermatol. 2013;168(3):474-485.
2. Friedlander SF, Eichenfield LF, Fowler RF, Fried RG, Levy ML, Webster GF. Acne epidemiology and pathophysiology. Semin Cutan Med Surg. 2010;29(2 Suppl 1):2-4.
3. Yentzer BA, Hick J, Reese EL, Uhas A, Feldman SR, Balkrishnan R. Acne vulgaris in the United States: a descriptive epidemi-ology. Cutis. 2010;86(2):94-99.
4. Mancini AJ, Baldwin HE, Eichenfield LF, Friedlander SF, Yan AC. Acne life cycle: the spectrum of pediatric disease. Semin Cutan Med Surg. 2011;30(3 Suppl):S2-S5.
5. Williams HC, Dellevealle RP, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361-372.
6. Do TT, Zarkhin S, Orringer JS, et al. Computer assisted alignment and track-
ing of acne lesions indicate that most in-flammatory lesions arise from comedo-nes and de novo. J Am Acad Dermatol. 2008;58(4):603-608.
7. Bowe WP, Leyden JJ, Crerand CE, Sar-wer DB, Margolis DJ. Body dysmor-phic disorder symptoms among patients with acne vulgaris. J Am Acad Dermatol. 2007;57(2):222-230.
8. Pawin H, Chivot M, Beylot C, et al. Living with acne: a study of adolescents’personal ex-periences. Dermatology. 2007;215(4):308-314.
9. Conrado LA, Hounie AG, Diniz JB, et al. Body dysmorphic disorder among dermatologic patients: prevalence and clinical features. J Am Acad Dermatol. 2010;63(2):435-443.
10. Cotterill JA, Cunliffe WJ. Suicide in der-matological patients. Br J Dermatol. 1997;137(2):246-250.
11. Gupta MA, Gupta AK. Depression and sui-cidal ideation in patients with acne, alope-cia areata, atopic dermatitis and psoriasis. Br J Dermatol. 1998;139(5):846-850.
12. Eichenfield LF, Mancini AJ. PedAcne Re-source Guide: A Comprehensive Overview of Pediatric Acne & Companion to the On-line Self-Assessment Exam. New York, NY: Education Testing & Assessment Systems; 2013.
13. Rapelanoro R, Mortureux P, Couprie B, Maleville J, Taieb A. Neonatal Malas-sezia furfur pustulosis. Arch Dermatol. 1996;132(2):190-193.
14. Tom WL, Friedlander SF. Acne through the ages: case-based observations through childhood and adolescence. Clin Pediatr. 2008;47(7):639-651.
15. Friedlander SF, Baldwin HE, Mancini AJ, Yan AC, Eichenfield LF. The acne continu-um: age based approach to therapy. Semin Cutan Med Surg. 2011;30(3 Suppl):S6-S11.
16. Eichenfield LF, Krakowski AC, Piggott C, et al. Evidence based recommendations for the diagnosis and treatment of pediatric acne. Pediatrics. 2013;131(Suppl 3):S163-S186.
17. Mann MW, Ellis SS, Mallory SB. Infantile acne as the initial sign of an adrenocorti-cal tumor. J Am Acad Dermatol. 2007;56(2 Suppl):S15-S18.
18. Cantatore Francis JL, Glick SA. Childhood acne: evaluation and management. Derma-tol Ther. 2006;19(4)202-209.
19. Golub MS, Collman GW, Foster PM, et al. Public health implications of altered pu-berty timing. Pediatrics. 2008;121(Suppl 3):S218-S230.
20. Toppari J, Juul A. Trends in puberty timing in human and environmental modifiers. Mol Cell Endocrinol. 2010;324(1-2):39-44.
21. Euling SY, Herman-Giddens ME, Lee PA, et al. Examination of US puberty-timing data from 1940 to 1994 for secular trends:

PEDIATRIC ANNALS 42:10 | OCTOBER 2013 Healio.com/Pediatrics | 427
FEATURE
Panel findings. Pediatrics. 2008;121(Suppl 3):S172-S191.
22. Lucky AW, Biro FM, Sumbarti LA, Morrison JA, Sorg NW. Predictors of severity of acne vulgaris in young adolescent girls: results of a five year longitudinal study. J Pedatr. 1997;130(1):30-39.
23. Thiboutot D, Gollnick H, Bettoli V, et al. New insights into the management of acne: an update from the Global Alliance to Im-prove Outdomes in Acne group. J Am Acad Dermatol. 2009;60(5 Suppl):S1-S50.
24. Worret WI, Fluhr JW. Acne therapy with topical benzoyl peroxide, antibiotics, and azelaic acid. J Dtsch Dermatol Ges. 2006;4(4):293-300.
25. Humphrey S. Antibiotic resistance in acne treatment. Skin Therapy Lett. 2012;17(9):1-3.
26. Zaenglein AL. Topical retinoids in the treat-ment of acne vulgaris. Semin Cutan Med Surg. 2008;27(3):177-182.
27. Kligman AM, Fulton JE, Plewig G. Topical vitamin A acid in acne vulgaris. Arch Der-matol. 1969;99(4):469-476.
28. Cunliffe WJ, Danby FW, Dunlap F, Gold MH, Gratton D, Greenspan A. Randomised, controlled trial of the efficacy and safety of adapalene gel 0.1% and tretinoin cream 0.05% in patients with acne vulgaris. Eur J Dermatol. 2002;12(4):350-354.
29. Draelos ZD, Carter E, Maloney M, et al. Two randomized studies demonstrate the
efficacy and safety of dapsone gel, 5% for the treatment of acne vulgaris. J Am Acad Dermatol. 2007;56(3):439.
30. Lucky AW, Maloney JM, Roberts J, et al. Dapsone gel 5% for the treatment of acne vulgaris: safety and efficacy of long-term (1 year) treatment. J Drug Dermatol. 2007;6(10):981-987.
31. Piette WW, Taylor S, Pariser D, Jarratt M, Sheth P, Wilson D. Hematologic safety of dapsone gel, 5%, for topical treat-ment of acne vulgaris. Arch Dermatol. 2008;144(12):1564-1570.
32. Esterly NB, Koransky JS, Furey NL, Trev-isan M. Neutrophil chemotaxis in patients with acne receiving oral tetracycline ther-apy. Arch Dermatol. 1984;120(10):1308-1313.
33. Tsankov N, Broshtilova V, Kazandjieva J. Tetracyclines in dermatology. Clin Derma-tol. 2003;21(1):33-39.
34. Webster GF, Graber EM. Antibiotic treat-ment for acne vulgaris. Semin Cutan Med Surg. 2008;27(3):183-187.
35. Zaenglein AL, Thiboutot DM. Expert com-mittee recommendations for acne manage-ment. Pediatrics. 2006;118(3):1189-1199.
36. Del Rosso JQ, Kim G. Optimizing the use of oral antibiotics in acne vulgaris. Dermatol Clin. 2009;27(1):33-42.
37. Shin J, Cheetham TC, Wong L, et al. The impact of the iPLEDGE program on isotretinoin fetal exposure in an integrated health care system. J Am Acad Dermatol. 2011;65(6):1117-1125.
AD INDEX
ASSOCIATION AND MEETING SOLUTIONS, LLC6900 Grove Road, Thorofare, NJ 08086Infectious Diseases in Children® 2013 Symposium ................................................................................ C2-385
PFIZER INC235 East 42nd Street, New York, NY 10017Children’s Advil .......................................................................................................................................................... C4
SALIX PHARMACEUTICALS INC.8510 Colonnade Center Drive, Raleigh, NC 27615Vesicoureteral Reflux ...................................................................................................................................... 392A-D
SLACK INCORPORATED6900 Grove Road, Thorofare, NJ 08086Curbside Pediatrics ..................................................................................................................................................395Healio Experience ...................................................................................................................................................... C3Healio iPad Sweepstakes .......................................................................................................................................405Infectious Diseases in Children® Education Lab ........................................................................................... 421
While every precaution is taken to ensure accuracy, Pediatric Annals cannot guarantee against occasional changes or omissions in the preparation of this index.
Erratum:At the request of the authors, the online article by Linda Van Horn, PHD, RD
and Eileen Vincent, MS, RD, “The CHILD 1 and DASH Diets: Rationale and Translational Application” (September 2013) contains updated nutritional infor-mation in the Tables that differs from the print version. It can be seen at Healio.com/Pediatrics. Search the authors’ names to view those revisions.