fda's standards policy for medical devices
TRANSCRIPT

Richard A Stimson
FDA’s standards policy for medical devices
You as an operating room nurse can help develop and maintain good stan- dards for medical devices. On Feb 1, the Bureau of Medical Devices of the US Food and Drug Administration (FDA) issued new policies and procedures for developing standards for Class I1 medi- cal devices. Defining final procedures for implementing mandatory stan- dards, the agency also announced a pol- icy supporting development of volun- tary consensus standards in lieu of mandatory standards whenever feasi- ble. After an overview of these FDA policies, I will discuss roles the nursing profession might play in developing standards.
Richard A Stimson, PhD, is associate direc- tor for standards, Bureau of Medical Devices, Food and Drug Administration, Silver Spring, Md. He received a bachelor’s degree in me- chanical engineering from the University of Cincinnati and a master’s and doctorate in business administration from Ohio State Uni- versity, Columbus.
Under the 1976 amendments to the federal Food, Drug, and Cosmetic Act, the FDA is authorized to issue manda- tory standards for Class I1 devices and to define a process for their develop- ment. These amendments gave the FDA new authority to assure the safety and effectiveness of devices intended for human use. Device is broadly defined in the amendments as a “health care prod- uct that does not achieve any of its prin- cipal intended purposes by chemical ac- tion within or on the body or by being metabolized.” (In vitro diagnostic prod- ucts are included.)
The law provides that these products will be classified into three groups according to how difficult it is to assure their safety and effectiveness. In Class I, devices are subject to general controls. Class I1 includes all devices for which general controls are not sufficient. This is the classification that will be dis- cussed in this article. Class 111 consists of implants and life-supporting devices. These must be approved for safety and effectiveness before they can be mar- keted, unless the FDA determines this i s not necessary.
Before a mandatory standard for a medical device can be published, an ad- visory panel of experts must judge that a standard is required to assure reason- able safety and effectiveness of the de- vice. Such devices are placed in Class 11. Following classification, there are a number of steps for developing a stan-
2 14 AORN Journal, August 1980, Vol32, No 2

dard. When implemented, the resulting standard has the force of law. Final standards are published in the Federal Register, the government’s official pub- lication for rules and regulations.
Developing mandatory standards can be a long and costly process. Rather than rely solely on mandatory stan- dards, the Bureau intends to rely heav- ily on voluntary standards. Organiza- tions such as the American National Standards Institute (ANSI), the Associ- ation for the Advancement of Medical Instrumentation (AAMI), the National Committee for Clinical Laboratory Standards, and the American Society for Testing and Materials presently de- velop such standards. We plan to work closely with these organizations in car- rying out the FDA’s standards program.
As we see it, there will be a dual pro- gram, providing a balance between vol- untary and mandatory standards. This approach will encourage cooperation by and full participation of nongovern- ment interests, resulting in better stan- dards and making optimum use of available resources.
FDA plans to endorse voluntary standards that meet our approval after considering criteria relating to their content and development (Table 1).
FDA plans to provide support to vol- untary standards groups. This support can consist of:
technical assistance in preparing
assistance in determining the effec-
investigating the extent of volun-
development of test methods where necessary, monetary support to consumer representatives t o cover travel expenses.
The endorsement procedure FDA
a letter of endorsement to the de- veloper of the standard (if there are
the standard
tiveness of the standard
tary conformance
plans to use will include:
requirements in the standard be- yond safety and effectiveness is- sues, only those portions relating to safety and effectiveness will be en- dorsed) periodically publishing in the Fed- eral Register a listing of endorsed standards.
- distribution of a list of endorsed standards
- press releases - technical articles - encouraging manufacturers to
label their products, “meets fed- erally endorsed. . . standard. . .”
- encouraging purchasing agents such as hospitals and third-party payers to require endorsed stan- dards; the nursing profession’s influence in purchasing deci- sions can be of help in this re- gard.
If there is a published standard, we will review it in accordance with the FDA criteria. For standards developed prior to publication of our voluntary stan- dards policy and the criteria, a “grand- father” approach will be considered so preexisting worthwhile voluntary standards are not automatically re- jected. The Bureau of Medical Devices plans to review for endorsement approx- imately 40 existing voluntary stan- dards during Fiscal Year 1980.
From a regulatory point of view, an FDA-endorsed voluntary standard is still voluntary, not mandatory. FDA in- tends to promote voluntary con- formance to endorsed standards. It is hoped that these standards will become “accepted industry practice” and that conforming devices will have a competi- tive advantage over those that do not conform. If this happens, the intent of regulatory control will have been im- plemented through industry practice rather than being imposed by the FDA. The success of FDA’s program for en-
promotional actions such as:
AORN Journal, August 1980, Vol32 , No 2 215
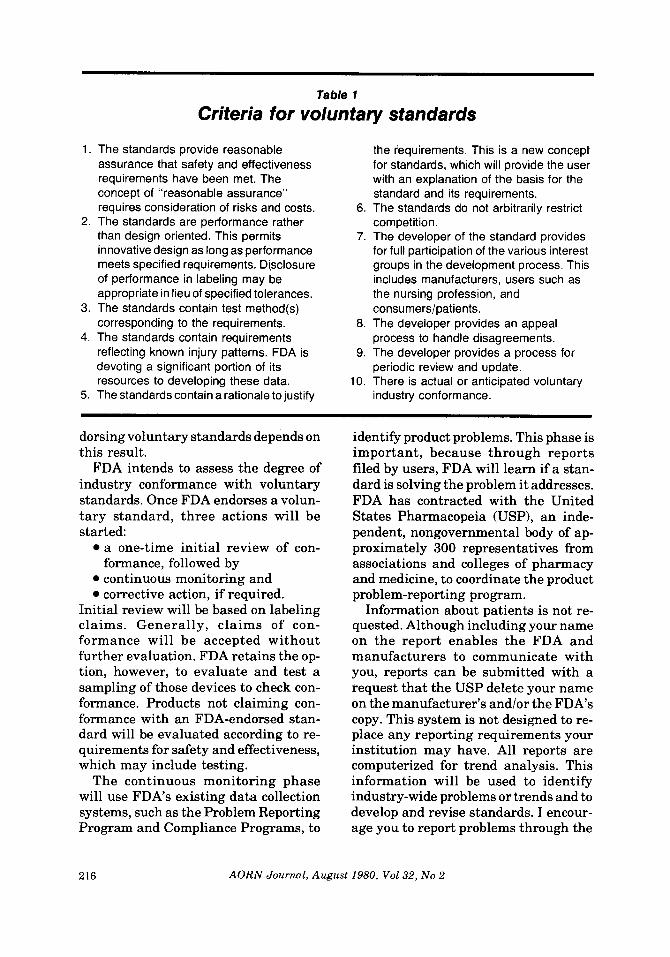
Table 1
Criteria for voluntary standards
1.
2.
3.
4.
5.
The standards provide reasonable assurance that safety and effectiveness requirements have been met. The concept of “reasonable assurance” requires consideration of risks and costs. The standards are performance rather
innovative design as long as performance meets specified requirements. Disclosure of performance in labeling may be appropriate in lieu of specified tolerances. The standards contain test method(s) corresponding to the requirements. 8. The standards contain requirements
9. devoting a significant portion of its
10. The standards contain a rationale to justify
6.
7. than design oriented. This permits
reflecting known injury patterns. FDA is
resources to developing these data.
the iequirements. This is a new concept for standards, which will provide the user with an explanation of the basis for the standard and its requirements. The standards do not arbitrarily restrict competition. The developer of the standard provides for full participation of the various interest groups in the development process. This includes manufacturers, users such as the nursing profession, and consumerslpatients. The developer provides an appeal process to handle disagreements. The developer provides a process for periodic review and update. There is actual or anticipated voluntary industry conformance.
dorsing voluntary standards depends on this result.
FDA intends to assess the degree of industry conformance with voluntary standards. Once FDA endorses a volun- tary standard, three actions will be started:
a one-time initial review of con-
continuous monitoring and corrective action, if required.
formance, followed by
Initial review will be based on labeling claims. Generally, claims of con- formance will be accepted without further evaluation. FDA retains the op- tion, however, to evaluate and test a sampling of those devices to check con- formance. Products not claiming con- formance with an FDA-endorsed stan- dard will be evaluated according to re- quirements for safety and effectiveness, which may include testing.
The continuous monitoring phase will use FDA’s existing data collection systems, such as the Problem Reporting Program and Compliance Programs, to
identify product problems. This phase is important, because through reports filed by users, FDA will learn if a stan- dard is solving the problem it addresses. FDA has contracted with the United States Pharmacopeia (USP), an inde- pendent, nongovernmental body of ap- proximately 300 representatives from associations and colleges of pharmacy and medicine, to coordinate the product problem-reporting program.
Information about patients is not re- quested. Although including your name on the report enables the FDA and manufacturers to communicate with you, reports can be submitted with a request that the USP delete your name on the manufacturer’s and/or the FDA’s copy. This system is not designed to re- place any reporting requirements your institution may have. All reports are computerized for trend analysis. This information will be used to identify industry-wide problems or trends and to develop and revise standards. I encour- age you to report problems through the
216 AORN Journal, August 1980, Vol32, No 2

USP system, although I understand that current AORN policy is not to par- ticipate in this program. I hope that you will reconsider this policy. Feedback on conformance to standards, especially voluntary standards, is absolutely nec- cessary if the program is to be effective.
In addition to this voluntary prob- lem-reporting system, the Bureau is de- veloping a mandatory experience re- porting regulation. The objective of this proposed regulation is to require that manufacturers provide FDA with in- formation concerning device-related deaths, injuries, defects, and recalls.
FDA also routinely inspects man- ufacturers. During this inspection, specific information will be collected re- garding product conformance to a specific standard(s).
If action is required to correct a safety or effectiveness problem, several op- tions are available, depending on the circumstances:
0 notifying the manufacturer, who
revising the voluntary standard if it
instituting a compliance action 0 initiating development of a manda-
The February Federal Register also listed priority devices as candidates for standards and invited voluntary stan- dards organizations and other in- terested parties to indicate existing or planned standards development efforts for any of the devices on the lists. Based on this information, the Bureau of Med- ical Devices will develop a detailed vol- untary and a mandatory standards pro- gram for priority devices, indicating for each device what effort is underway and its schedule for completion.
First preference will be given to vol- untary standards. Mandatory stan- dards will be written if
corrects the problem
is deficient
tory standard.
0 no qualified offers are received 0 there is low probability of industry
For additional information These government publications provide information on the 1976 Medical Device Amendments.
The Health Professional and Medical Devices (Rockville, Md: US Food and Drug Administration, 1978). HEW Publication No (FDA) 78-401 1. 30-Point Summary: Medical Device Amendments of 1976 (Public Law 94-295) (Rockville, Md: U S Food and Drug Administration, 1977).
The publications may be ordered from the Bureau of Medical Devices, US Food and Drug Administration, HFK 120, 8757 Georgia Ave, Silver Spring, Md 20910.
voluntary conformance
needed. a strong regulatory approach is
There are several ways the nursing profession can play an important role in standards development and assess- ment. First, your knowledge of medical devices can be channeled to the volun- tary standards organizations through your representative on the Medical De- vice Standards Management Board of ANSI. This board coordinates the medi- cal device voluntary standards effort, and AORN is a member. AORN is also active on standards-writing committees such as AAMI. Your “hands-on” knowl- edge of many medical devices provides an essential contribution to stan- dards-writing committees.
Once a standard is developed and en- dorsed, FDA needs feedback on its effec- tiveness. Your evaluation of the effect of a medical device standard on the per- formance of a device is important to FDA and the voluntary standards or- ganizations. Your influence on procur- ing medical devices that meet FDA- endorsed standards is another area of impact. In summary, the nursing pro- fession can help assure safe and effec-?
AORN Journal, August 1980, Vol32, No 2 217

t i ve medical devices through: l e m repor t i ng p rog ram system 0 prov id ing FDA with any evaluat ion
of an endorsed s tandard y o u feel
0 selecting devices that meet appro-
invo lvement in writing standards repo r t i ng devices fa lsely c l a i m i n g con fo rmance t o F D A - e n d o r s e d war ran ts o u r a t tent ion standards
device t o t h e U n i t e d States Phar- macopeia (USP) th rough t h e prob-
repo r t i ng any defective o r problem p r ia te standards. 0
Federal policy helps, hinders HMO growth Federal intervention has helped and hindered growth and development of the health maintenance organization (HMO) concept, according to a new American Hospital Association (AHA) book.
Reform, by Joseph L Falkson, discusses the emergence and maturing of HMOs in the 1970s and describes the government's commitment to prepaid health care. Falkson, a political scientist, is president of Health Sector Management, Inc, a firm specializing in HMO management.
Referring to HMOs as the "centerpieces of national health policy in the 1970s," he notes the growth of HMOs from 39 in 1970 to 217 by mid-1979. HMO enrollment during this same period more than doubled from 3.6 million to 7.9 million persons.
The author concludes, however, that while helping to facilitate growth of the HMO movement, the federal government also inhibited the growth and development of the plans.
"On the one hand, federal dollars and publicity have stimulated HMO development," he says. "On the other hand, congressional insistence on shaping the emerging universe of HMOs to a set of rigid specifications, coupled with persistent executive branch difficulties in administering so complex a program, have inhibited the HMO industry's maturation."
Falkson is on the faculty of the George Washington University Medical Center's Department of Health Care Sciences and the Department of Community Medicine and International Health.
the Robert J Brady Co, a division of
HMOs and the Politics of Health System
The book, copublished by the AHA and
Prentice-Hall, Inc, discusses the problems encountered in establishing a federal role in HMOs, beginning with the Nixon Administration and concluding with the renewed efforts of the Carter Administration. Also chronicled are the major factors that constrained HMO policies over the past decade, including the conflicting priorities, splintered constituencies, and limited budgets.
Risk of skin cancer from tanning evaluated The older person who tans poorly is at increased risk of skin cancer from tanning. Excessive exposure to sunlight increases the risk of skin cancer. But some individuals are much more likely to get skin cancers from excessive tanning than others.
Skin cancer risk factors are tabulated in a report in Archives of Dermatology. Peter Paul Vitaliano, MD, of the University of Washington, Seattle, summarizes research findings:
1 . With enough exposure, anyone is at substantial risk for skin cancers.
2. The effects of sun exposure take 20 or more years to become evident. The young sun enthusiast should be made aware of the consequences of repeated exposures, especially if he or she does not tan easily.
3. Given the same amount of exposure, older subjects are more susceptible to skin cancers than younger subjects.
to skin cancer than a dark complexion. 4. The ability to tan is a greater deterrent
218 AORN Journal, August 1980, Vol32, No 2