fast track into ob labor and delivery. lightening
TRANSCRIPT

Fast Track into OB
Labor and Delivery

Lightening

Five Ps of Labor
Passage
Passenger
Psyche
Powers
Pain
Passage: the bony pelvis and soft tissue
False pelvis (upper flaring part)True pelvis (lower part)
InletMiddleOutletShaped like a wide curved funnel
Soft TissueImpacted by previous birthsImpacted by scaring

More on the true and false pelvis
See text page 25Divided by false line: linea terminalis
Extends from sacroiliac joint to anterior iliopubic prominence
The upper false pelvis support the enlarging uterus and guides fetus into true pelvisThe TRUE pelvis however dictated the bony limits of the birth canal

Anatomical picture of pelvic inlet

Passage dimensions

Anatomical features of the pelvic outlet Page 25-26
Transverse diameter between the inner surfaces of the ischial tuberosities (spines) (bi ischial diameter)
Anterior posterior measurement of outlet is between lower border of symphysis pubis and tip of sacrum.
Passenger Page 122
Fetal skull page 123
Lie: orientation to Mom’s spine
Attitude: normally flexed
Presentation: part entering pelvis
Position: how a reference point on the fetal presenting part oriented within the mother’s pelvis
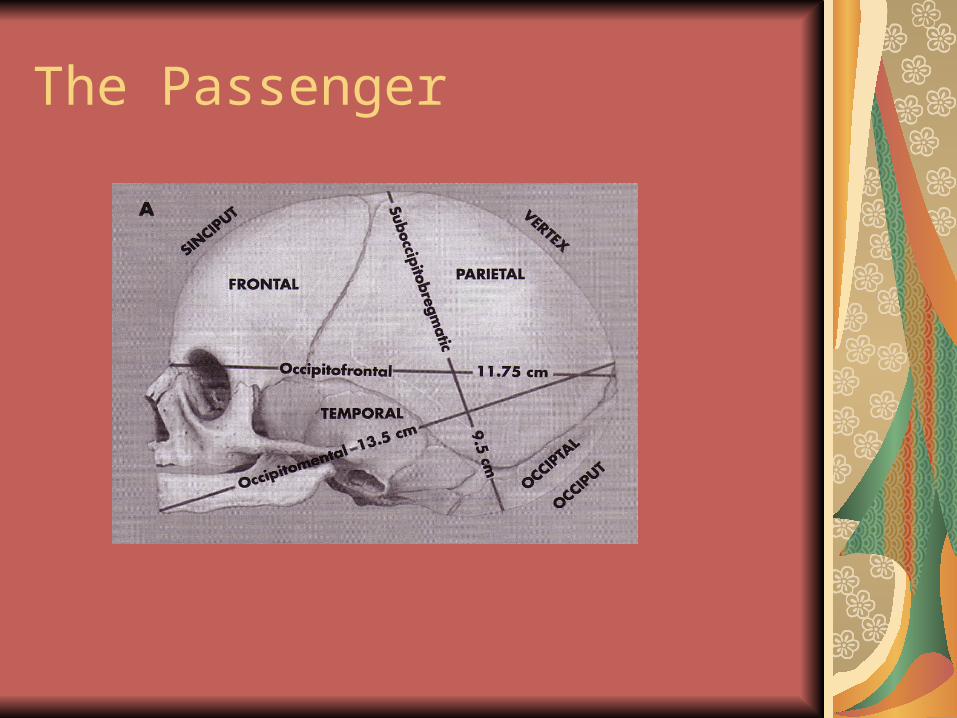
The Passenger
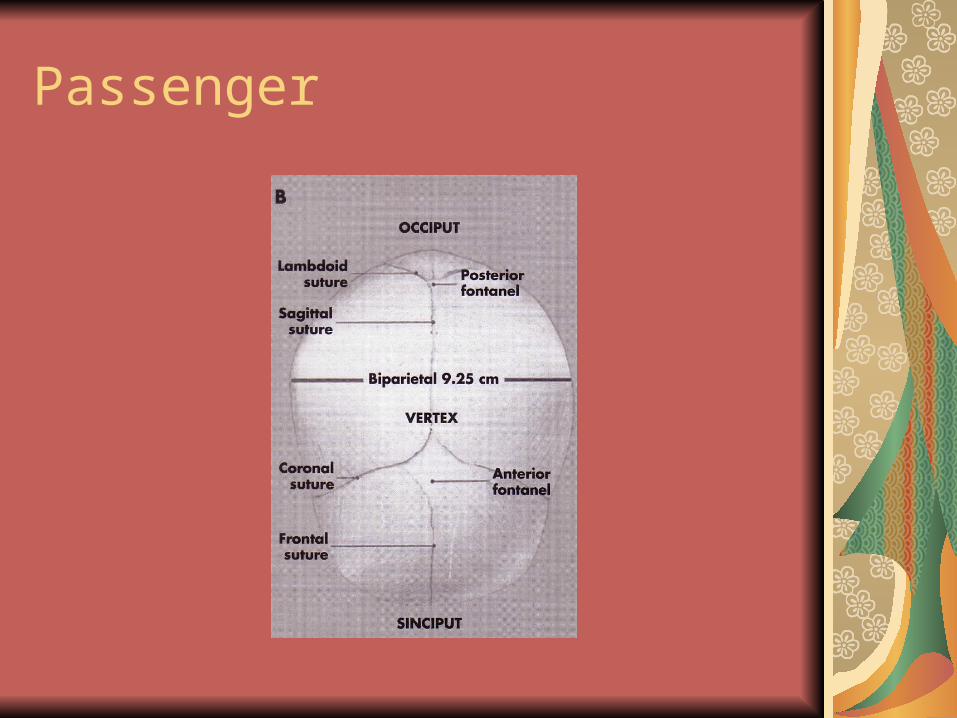
Passenger
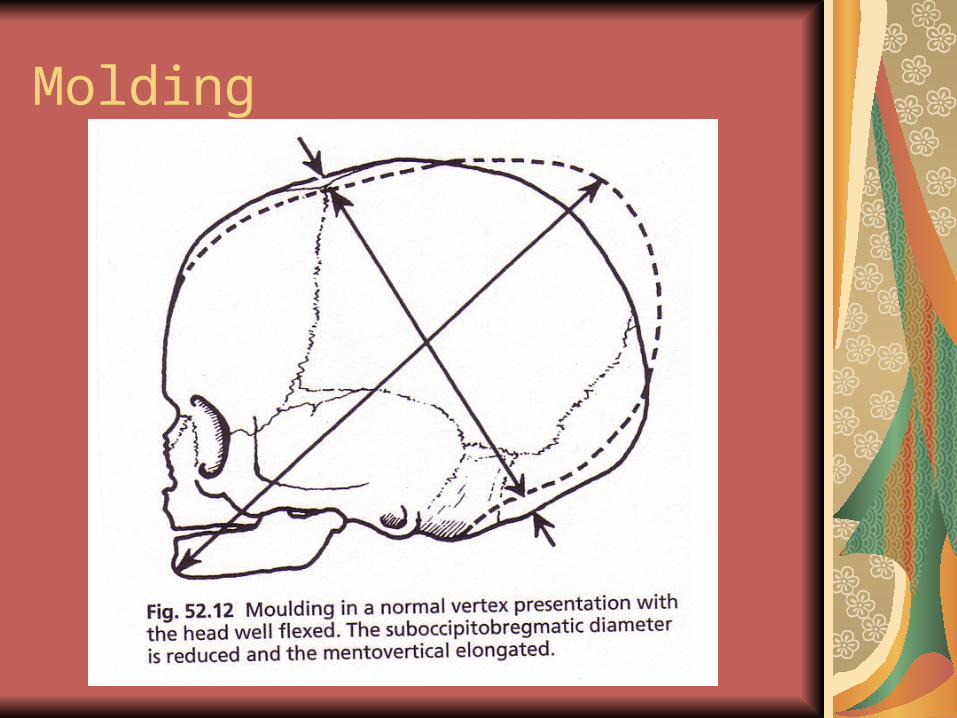
Molding
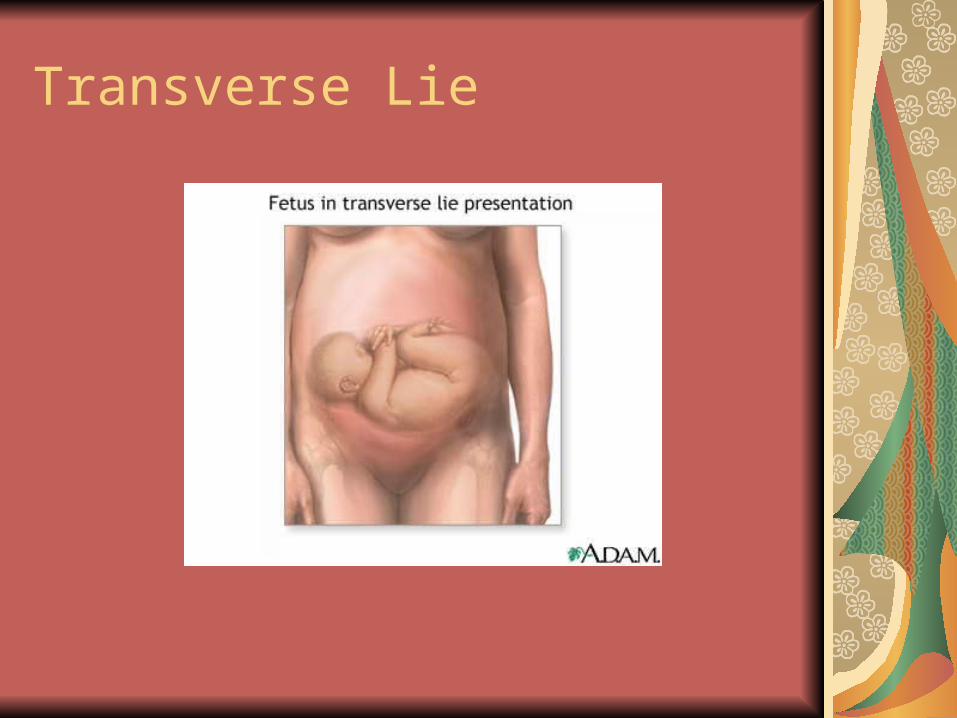
Transverse Lie

Fetal Lie

Fetal Lie LongitudinalFetal Presentation: Vertex

Attitude: Flexion/Extension

Fetal Attitude: a well flexed head
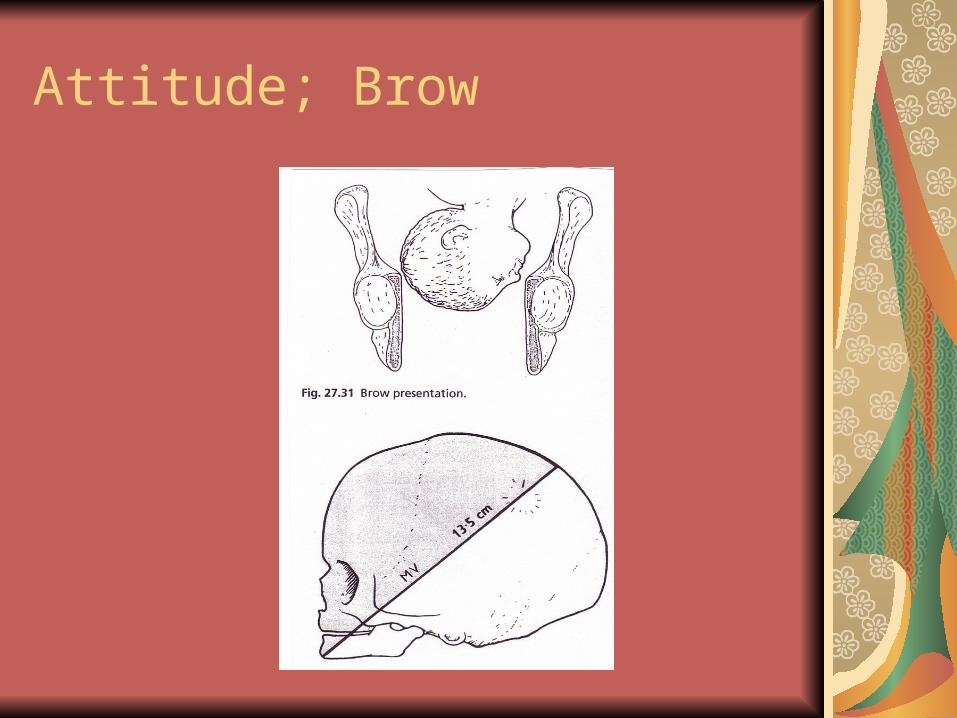
Attitude; Brow

Presentation: Breech
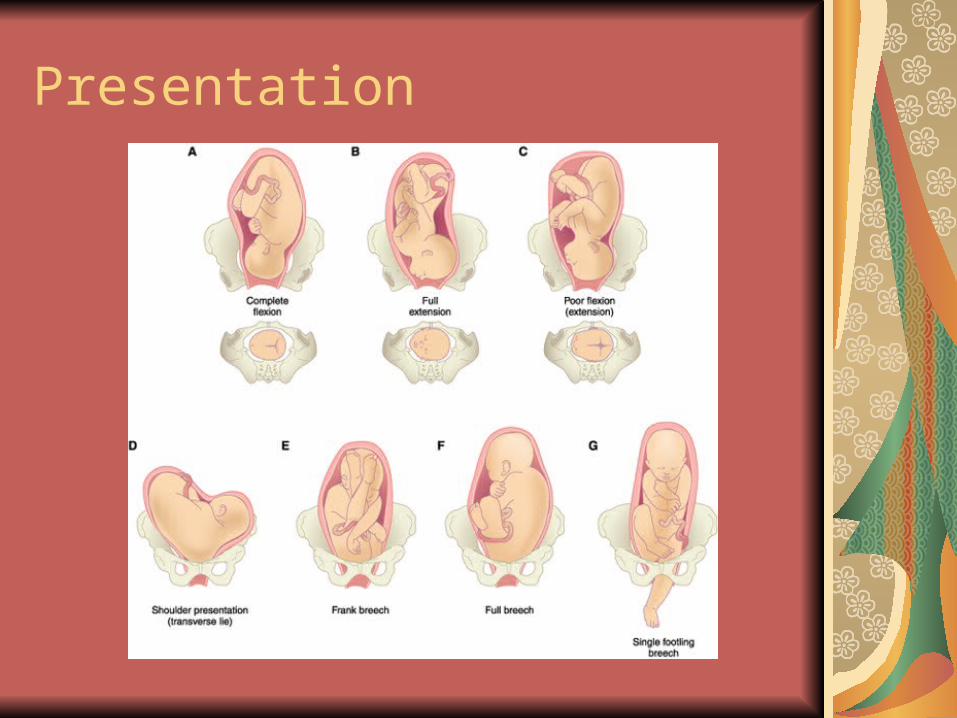
Presentation

Fetal Positions

Position: Posterior
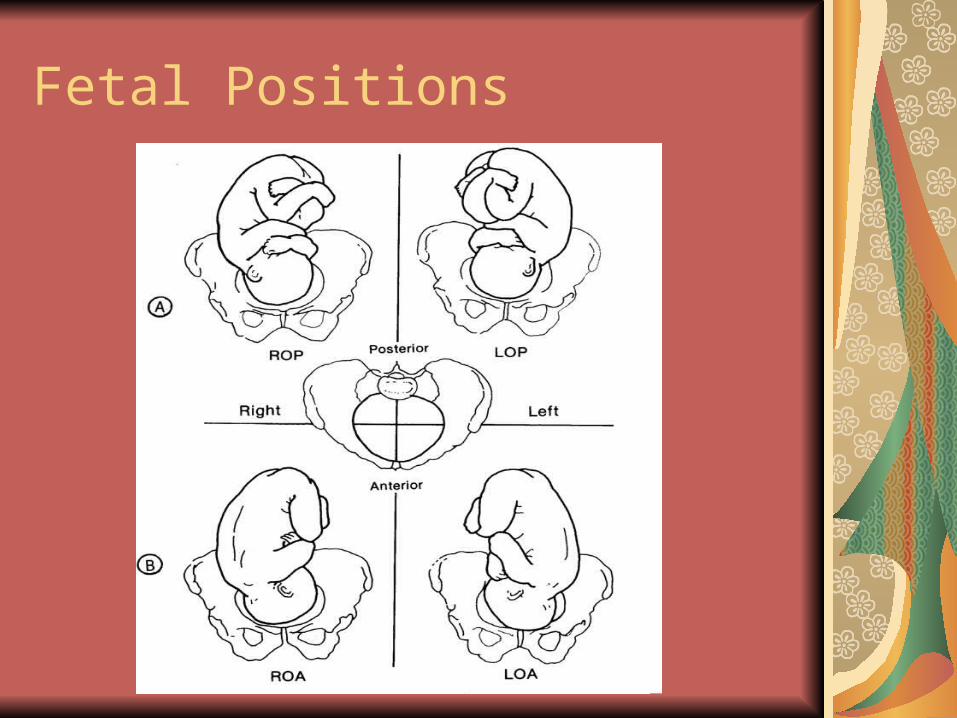
Fetal Positions

Using Fetal Heart Tones to Determine Position
Psyche
Woman’s mental state
Emotional; not described as surgical procedure
Mental State greatly impacts mothers ability to cope and tolerate discomfort
Perception of pain
Anxiety

Powers of Labor
Involuntary forces of labor
Contractions
Voluntary forces of labor
Mother’s pushing efforts

Contraction Cycle

Effects of contractions on the cervix
EffacementThins the cervix
Before labor approximately 2 cm long
Thinning of cervix is expressed in %
100% thin slick membrane at edge of fetal head
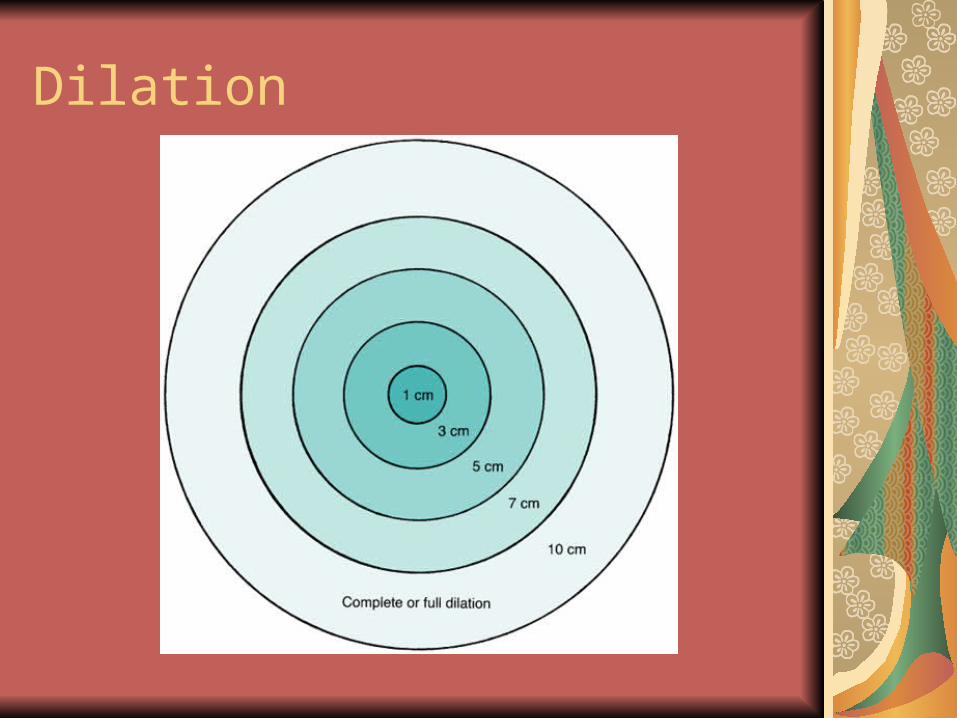
DilationOpening of the cervix
Described in cm of opening
Full dilation at 10 cms

Effacement and Dilation
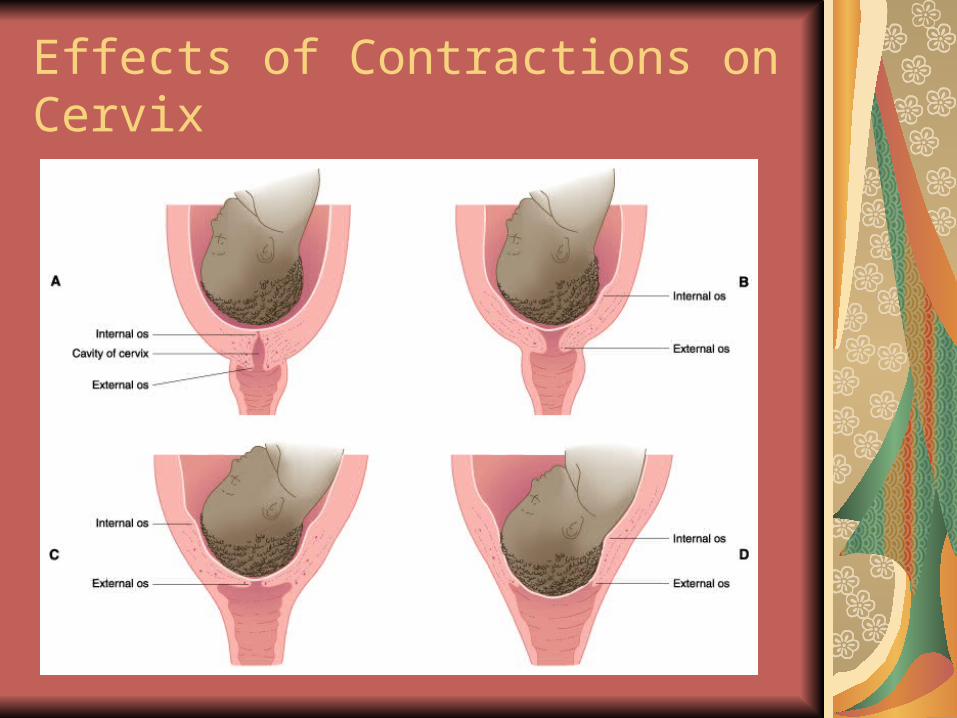
Effects of Contractions on Cervix

Effacement
Dilation

Mechanisms of Labor
Descent
Flexion
Rotation
Extension
Restitution
External Rotation

Engagement: Stations

Mechanisms of labor with effacement and dilation
Read to learn activity
Signs of impending labor (page 131)
Signs of True Labor (136)
Signs of False Labor (135-136)
Read those sections and then we will do a quiz together. RELAX!

Contractions; Page 120-21
Frequency
Duration
Interval
Increment/Peak/decrement
Intensity: Mild, moderate, strong

Contraction MonitoringThe basics
FrequencyFrom the beginning of one contraction to the beginning of the next contraction
Duration From the beginning of one contraction to the end of that contraction
IntervalThe space between two contractions; from the end of one contraction to the beginning of the next one

Rule of contractions
Based on infant getting adequate oxygenation
The frequency must not be less than two minutes
The duration must not be more than 90 seconds
The interval must not be less than 60 seconds

Fetal Heart monitoring
IntermittentAllows freedom of movement
Does not offer a continuous record
Obtain a baseline rate
Rule: any FHR outside the normal limits or slowing that persists after the contraction ends is promptly reported to the health care provider
See box 6-2 page 133
Continuous Fetal Heart Monitoring
Offers a written record
Allows collection of more data
May however run a strip on admission and then re run a strip at regular intervals during the labor
Referred to in terms of reassuring and non reassuring patterns.
Box 6-3 page 135

Fetal and Contraction MonitoringThe Basics
Top of strip is the fetal heart monitoring
Bottom of strip is the contraction pattern
Each small square is 10 seconds
Between each bold line is 60 seconds

Reassuring fetal heart/contraction pattern
110-160 bpm
Variability
Accelerations
Early decelerations
Contraction frequency greater than every 2 minutes, duration less than 90 seconds; relaxation interval of at least 60 seconds.
Non reassuring patterns
Fetal tachycardia
Fetal bradycardia
Variable decelerations
Late decelerations
Absences or decreased variability

Decelerations
Early Due to fetal head compression during contractions and are expected
LateDue to utero-placental insufficiency and are non reassuring
VariableDue to cord compression and are non reassuring.
Early decelerations
Reassuring pattern of deceleration during the early contraction due to fetal head compression
Always return to baseline before the end of the contraction
They often mirror a contraction
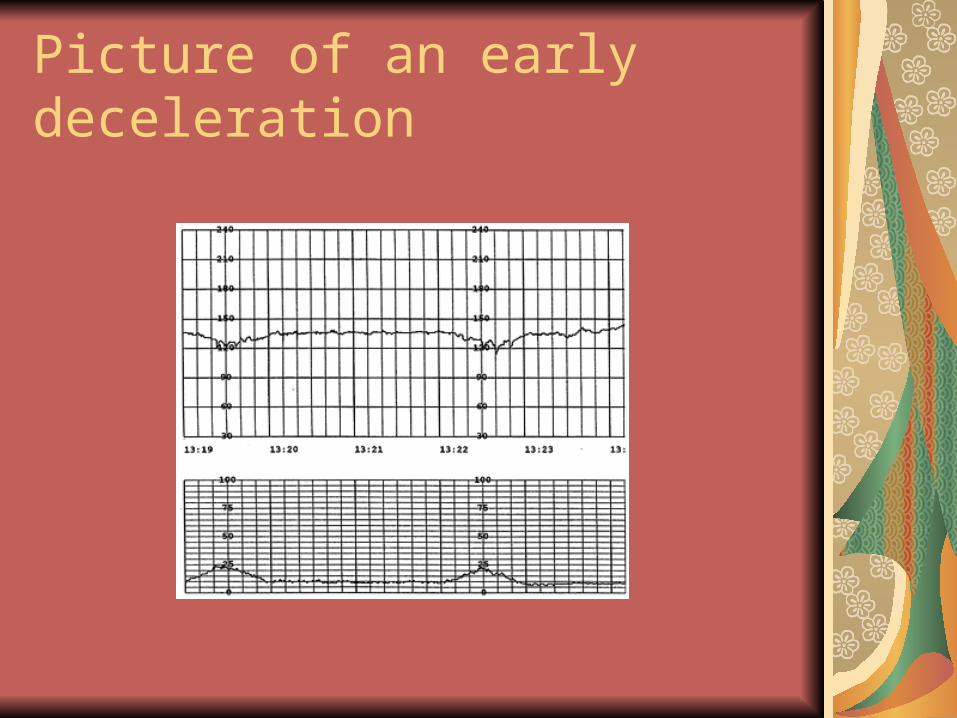
Picture of an early deceleration

Late deceleration
NON reassuring
Due to lack of oxygen to the baby
Uteroplacental insufficiency
Do NOT return to baseline FHR after the contraction ends

Picture of late deceleration
Variable Deceleration
Due to cord compression
V, W, or U shaped
Do not exhibit a consistent pattern in relation to the contractions
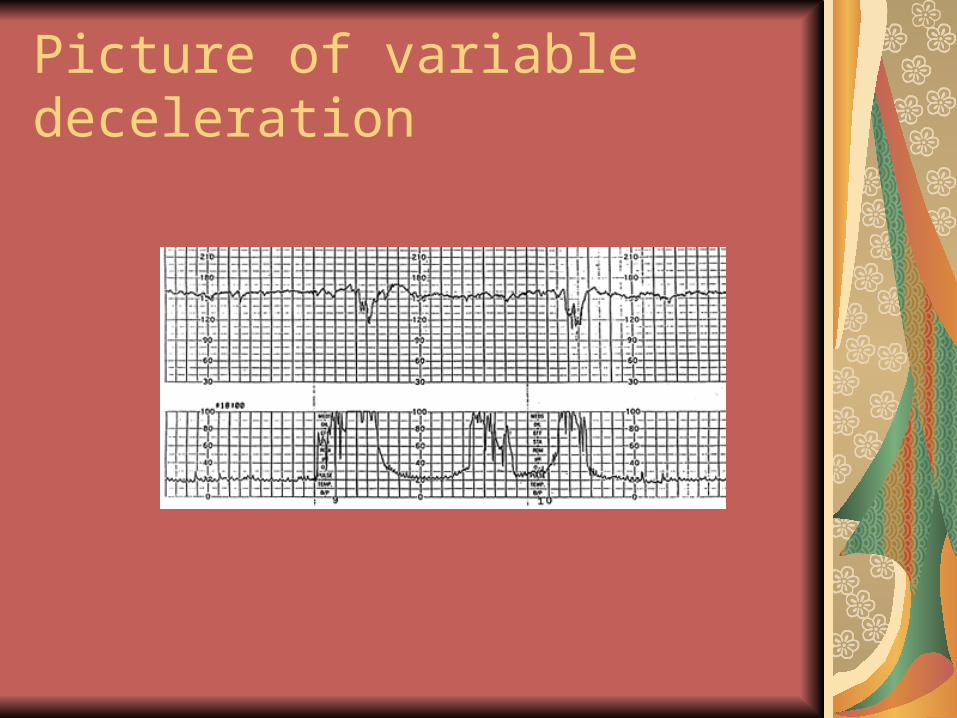
Picture of variable deceleration

Nursing responses to non reassuring patterns
Reposition mom, especially helpful in the variable decelerations
Oxygen 100% per tight face mask
IV fluids to expand blood volume and to dilute Pitocin (if given)
Stopping Pitocin
Giving tocolytic drugs to decrease uterine contractions

More FH patterns to look at

Stages of Labor
FirstOnset of labor until cervical effacement and dilation is complete (10 cm)
SecondFrom the completion of effacement and dilation until the baby is born
Third Expulsion of placenta
FourthRecovery phase

First stage divisions
Latent4-6 hours1-4 cmMild to moderate intensity
Active 2-6 hours4-7 cmModerate to firm intensity
Transition.5-2 hours7-10 cmFirm intensity
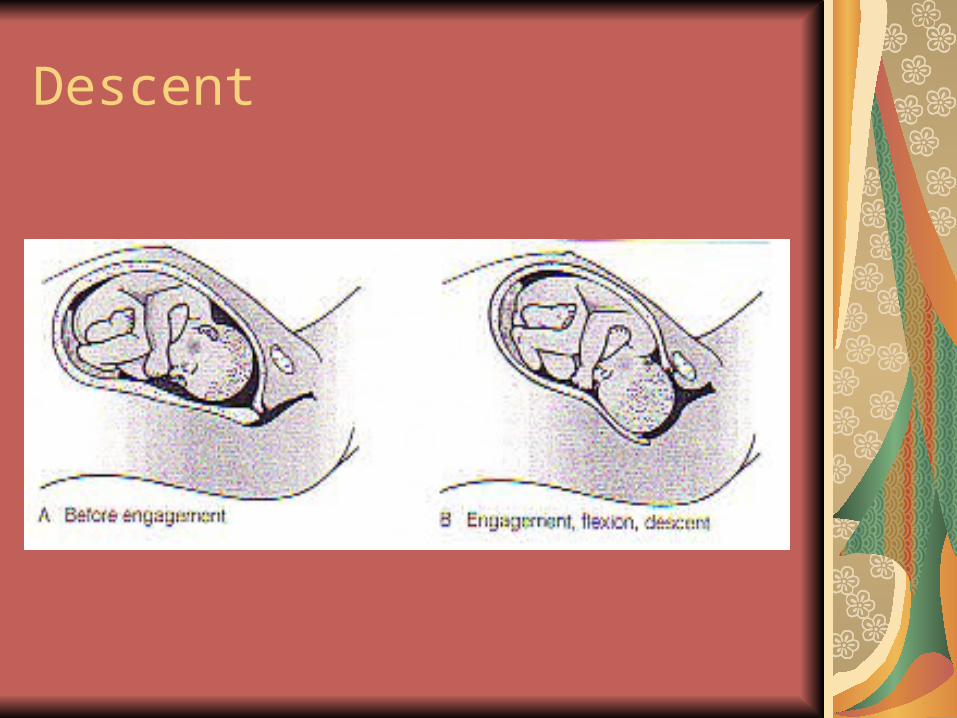
Descent

Mechanism of Labor, Continued

Mechanism of labor; continued

Delivery of shoulders

Second Stage
Second stage is also divided into three stages in other texts
Uncontrollable urge to push if no epidural
Exhaustion after each contraction
Unable to follow directions
“BABY IS COMING!!!”

Baby is HERE!

Third stage
Expulsion of placenta
Elation and relief
Shivers and tremors
Signs of placental seperationLengthening of cord
Uterus rises and becomes firm
Fresh blood expelled from vagina

Recovery Period
Number one priority for the mother’s care is prevention of hemorrhageInfant care focuses on
airway, breathing and circulation maintaining body temperature maintaining blood glucose
Critical period of bonding and breast feeding.

Immediate care of Mother
Assessment and care bullets; Page 148
Observing for hemorrhage
Maintaining a firm fundus
Preventing bladder distention
Promoting comfortIce pack
Warm blanket
Assisting with breast feeding
Assessment of lower extremities
Immediate Care of the Infant
First hour infant is in “quiet alert” phase and this is critical time form bonding and breast feeding.
Unless the infant is in a medical emergency most of care can be done right at mother’s breast
Now let’s see what will happen when you observe a birth!!!!

Immediate Care of Infant
APGAR scoreKeep warm: dry and place on mothers chest: skin to skin with blanket over and cap onAssure that the nose is clean, bulb suction nose as well as mouth. Usually done at perineumClamp the cord.Vigilant observation of infants cardiorespiratory status

Later Needs of the Infant
Detailed examination
Bath
Erythromycin eye ointment
Aquamephyton (vitamin K injection)]
Hepatitis B vaccination

APGAR Score; Page 143
APGAR Score
Let’s take some time to score to do the critical thinking exercise on APGAR scoring found in your workbook
NCLEX Prep question
A client at 38 weeks gestation tells the nurse that it feels like her baby is sitting on her bladder causing her to urinate more frequently. However, the client states it has made it easier for her to breathe. The nurse recognizes that this is a sign of:
LighteningQuickeningContractionsFlexion

NCLEX Prep QuestionA client reports that her contractions started about 2 hr ago, did not go away when she had two glass of water and rested, and became stronger since she started walking. She thinks the contractions occur every 10 minutes and last about half a minute. She hasn’t had any fluid leak from her vagina, however, she did think she saw some blood when she wiped after voiding. The nurse should recognize that the client is experiencing:
Braxton Hick contractions
Rupture of membranes
Fetal descent
True Contractions

NCLEX Prep QuestionA nurse is monitoring the FHR and contractions of a client in labor. The FHR is in the 140s. Contractions are every 5 min and 45-50 sec in duration. The nurse performs a vaginal exam and finds the cervix is 2 cm dilated, 50% effaced and the fetus is at the -2 station. One hour later the dilation is still 2 cm, but now the effacement is 80% Which of the following stages and phases of labor is this client experiencing?
The first stage, latent phaseThe first stage, active phaseThe first stage, transition phaseThe second stage of labor

NCLEX Prep QuestionA nurse is admitting a client to the birthing unit. The client suddenly states, A”I think I urinated on myself. It’s all wet down there, I’m so embarrassed.” Which of the following actions should the nurse take at this time?
Test the fluid with Nitrazine paper, it will confirm urine by turning blueTest the fluid with Nitrazine paper, which will confirm urine by turning pink. Test the fluid with Nitrazine paper, which will confirm amniotic fluid by turning it blueTest the fluid with Nitrazine paper, which will confirm amniotic fluid by turning it yellow.
NCLEX Prep Question
A client experiences a large gush of fluid from her vagina while walking in the hallway of the birthing unit. The nurse’s first action should be to:
Test to see if the fluid is amnionic fluidMonitor fetal heart rate for distressDry the client and make her comfortableMonitor the client’s maternal contractions

NCLEX prep question
While conducting an admission history for a client at 39 weeks gestation, the client tells the nurse that she has been leaking water from her vagina for 2 days. The nurse knows that this client is at risk for:
Cord prolapse
Infection
Malpresentation.
hydramnios

NCLEX Prep Question
A client in active labor becomes nauseous with emesis, is very irritable, and feels she needs to have a bowel movement. She states, “I’ve had enough. I can’t do this anymore. I want to go home right now.” The nurse knows that these signs indicate the client is in the:
Second stage of laborFourth stage of laborTransition phase of labor.Active phase of labor